JCO INTERVIEWS Richard P. McLaughlin, DDS on Facial and Dental Planning
|
|
|
- Claire Dalton
- 5 years ago
- Views:
Transcription


1 2004 JCO, Inc. May not be distributed without permission. JCO INTERVIEWS on Facial and Dental Planning DR. KEIM Dr. McLaughlin, your new book, Facial and Dental Planning for Orthodontists and Oral Surgeons, co-authored with Dr. Bill rnett, 1 focuses on diagnosis and treatment planning. What do you see as the new, unique, and different aspects of the philosophy of diagnosis and treatment planning? Dr. McLaughlin Dr. Keim Dr. McLaughlin is a Contributing Editor of the Journal of Clinical Orthodontics and in the private practice of orthodontics at 1831 Sunset Cliffs Blvd., San Diego, C 92107; rpmclaugh@aol. com. Dr. Keim is Editor of the Journal of Clinical Orthodontics. DR. MCLUGHLIN Emphasis is on three areas of evaluation the temporomandibular joints, the face, and the dentition with new and easier-to-use information in each area. In addition to the traditional methods of TMJ evaluation and treatment, there is the challenging area of TMJ remodeling with emphasis on stabilization and medical management. Important contributions are made in the book by Dr. Tom Eggleton (physical therapy), Dr. Richard Gevirtz (biofeedback), and Dr. Steve Milam (medical management and TMJ lavage). Next there are more thorough and objective methods of facial planning. In the past, due to incomplete clinical examination and inadequate information from cephalometric x-rays, more subjective facial planning decisions have been made. While this may produce adequate results, there is a greater chance of error. In my opinion, the above areas are two of Dr. rnett s great contributions to both orthodontics and oral surgery. Finally, once a decision has been made concerning the angulation and the anteroposterior and vertical position of the incisors from the facial analysis, specific information is provided for calculating the orthodontic movements required for the midlines, cuspids, and molars. This, too, reduces errors in the dental alignment of our cases. DR. KEIM What do you see as the appropriate goals for treatment planning? DR. MCLUGHLIN The goals of treatment include: Healthy musculature and temporomandibular joints Facial balance Correct static and functional occlusion Periodontal health Resolving the patient s chief complaints Stability of dental and skeletal changes Improved airway DR. KEIM What are the requirements for a systematized and objective approach to diagnosis and treatment planning? DR. MCLUGHLIN It is important that very specific methods and techniques be carried out from the initial contact with the patient to the presentation of the treatment plan. Important steps cannot be eliminated along the way, and VOLUME XXXVIII NUMBER JCO, Inc. 199
2 JCO INTERVIEWS checks and balances need to occur as the process proceeds. In addition, objective methods rather than subjective opinions should accompany the process. DR. KEIM Where is the patient s chief complaint addressed in this protocol? DR. MCLUGHLIN fter obtaining personal information from the patient, a Chief Complaint Form, as developed by Dr. rnett, is completed. 2 The original form has been modified into two forms: a basic orthodontic form for routine cases, and a surgical form for more complex cases. Each form is in three sections, asking questions concerning the face, the teeth, and symptoms (the TMJs). This form is reviewed with the patient at the initial examination and once again at the consultation to insure that the patient s concerns are being addressed. DR. KEIM What are the essential elements of a clinical patient exam? DR. MCLUGHLIN The clinical exam consists of three parts: the TMJ exam, the facial exam (frontal view and profile view), and the intraoral exam. screening TMJ examination is indicated for all patients, whether they do or do not describe symptoms. Two palpation positions (over the condyles externally and using the small fingers in the ear canal) are used during three mandibular movements (opening and closing, left and right lateral, and protrusion). These provide information concerning the patient s range of movement, deviation from normal movements, any pain during movement, and joint sounds. The protocol for the facial examination was published by Dr. rnett and Dr. Robert Bergman, 3 but both the frontal and profile facial exams have been modified slightly since the original publication. Lastly, the intraoral exam is completed, recording necessary information. DR. KEIM What do you see as the main areas of diagnosis? DR. MCLUGHLIN The main areas of diagnosis follow the main areas of the clinical exam. Concerning the temporomandibular joints, it is important to determine if the problem is purely muscular, strictly limited to the joints, or, more commonly, a combination of the two. It is critical to determine the location and extent of TMJ damage in other words, local or total remodeling of the condyle. main emphasis of the book is to evaluate the face three-dimensionally and objectively determine and quantify the areas of facial deformity. By doing this, we can be more accurate in determining the best method of treatment as well as alternative options. In the past, this has been an area of subjective estimates, and mistakes are possible with such an approach. Concerning the dentition, accurate determinations need to be made of molar relationships, midlines, occlusal cants, arch widths, arch crowding, and planes of occlusion. This can then be combined with information on ideal incisor positioning from the facial plan. With this information, a more accurate determination can be made concerning tooth movements needed and anchorage requirements. DR. KEIM How is facial planning different from traditional orthodontic treatment planning? DR. MCLUGHLIN Facial planning involves two key components that have not been as thoroughly addressed as possible in the past. The first key is a thorough clinical facial examination. This provides us with important soft-tissue, dental, and skeletal information in the frontal (transverse and vertical) dimension and the sagittal (vertical and horizontal) dimension. This information can be developed and objectified by the second key, which is Soft Tissue Cephalometric nalysis (STC) and Cephalometric Treatment Planning (CTP). These two methods help us to minimize the weaknesses inherent in cranial base references and provide us with significantly greater soft-tissue information. DR. KEIM How does facial planning differ from traditional facial planning based on cranial base measurements? 200 JCO/PRIL 2004
3 DR. MCLUGHLIN Utilizing cranial base landmarks to evaluate difficult cases has always been problematic, since these landmarks vary in position from patient to patient, and are often hard to locate on the head film. lso, traditional cephalometric treatment planning has focused on dentoskeletal factors, with only minimal emphasis on soft tissues. Surgeons in the 1980s (Epker, Wolford, and others) began focusing more on soft tissue by utilizing a line perpendicular to Frankfort horizontal and through subnasale. Such a method provided a greater focus on soft tissue; however, it was still subject to the problems associated with the cranial base landmark, Frankfort horizontal. Studies by various authors in the 1980s and 1990s (for example, Lundstrom and Lundstrom 4 ) suggested that utilizing natural head posture was a more accurate reference than cranial base references. The True Vertical Line is a vertical line through subnasale with the patient in natural head posture. Dr. rnett used this line to develop his analysis, 5 which provides us with thorough information on virtually all of the important dentoskeletal and soft-tissue measurements in the vertical and horizontal planes. DR. KEIM What kind of standards are used in an objective treatment-planning system? DR. MCLUGHLIN We have had objective standards relative to static occlusion, such as Dr. ndrews s six keys, and functional occlusion, such as the goals described by Dr. Roth. dmittedly, we are unable to achieve these goals in every case, and the reasons are multiple. This does not mean that we discard them as irrelevant. They continue to serve as objective references and reasonable goals to achieve whenever possible. In the same way, we can benefit from objective standards relative to facial planning, even though we are unable to achieve such results in each case. More research is needed so that objective standards are established for different ethnic groups. In addition to the rnett norms (essentially a Caucasian Southern California group), the Japanese are well on the way to completing and publishing their norms. Studies are also ongoing in Korea and India to my knowledge. This is a very exciting project, and the minor differences are enlightening. DR. KEIM What role does condylar position play in this method of case documentation? DR. MCLUGHLIN Consistent condyle positioning is critical in the case documentation process. If this is not done, critical errors can be made in treatment planning. wax bite with proper condyle positioning is placed when taking facial photographs and cephalometric x-rays and when mounting study models. In this way, there is a consistency of records when evaluating the case. DR. KEIM Where should the condyle be placed during record taking? DR. MCLUGHLIN The condyle needs to be seated superiorly in the fossa in an uncompressed position during record taking. The position may vary slightly from patient to patient and is probably a very small area vs. a pinpoint position. This perspective is not a license to be sloppy during record taking, but a realistic awareness. The importance of the seated condyle position is well documented with extensive literature on condylar sag in surgical cases, relapse with functional appliances, mandibular positional changes with rheumatoid and degenerative arthritis, and generally unstable occlusions associated with unseated condyles. Treating patients to unseated condyle positions has consistently led to treatment failure. We do not need to beat this subject to death any longer. On the other hand, in our zeal to provide a seated condyle position, we have at times placed the condyle in a compressed position. There is a growing body of evidence showing that condylar compression leads to local or even total condylar remodeling. Therefore, the goal is to place the condyle in a seated but uncompressed position. This is not the easiest of tasks. DR. KEIM How do you assure that the condyles are in this position during record taking? VOLUME XXXVIII NUMBER 4 201
4 JCO INTERVIEWS DR. MCLUGHLIN For bite registration, the patient is seated in the chair at approximately a 45 angle. The mandible is manipulated with gentle seating pressure, using the thumb on the chin and two fingers under each side of the mandible. Once this has been practiced with the patient, the initial wax bite is taken. The selected wax is a sheet of medium-hardness pink baseplate wax, folded in half and then folded again to 1cm width in the incisor area (open bites need more thickness in the anterior area). The wax is then trimmed to the general shape of the patient s upper arch. With the wax in place, the patient is closed in the seated condyle position to first tooth contact. The wax bite is removed, and a sharp pair of scissors is used to accurately trim just behind the most distal molars, through the upper buccal cusps, and along the edge of the incisors. This avoids soft-tissue distortion during the next two wax-bite checks and when mounting the models. The wax bite is then repositioned onto the maxillary teeth, and the bite is retaken in the same way. The lower incisors must fit precisely into the incisor indentations. If not, the wax bite is discarded and the process is begun again. This repeated wax bite is removed and chilled in cold water. It is then repositioned and taken a third time. Once again, the lower incisors must fit accurately, or the entire process is repeated. If it is not possible to obtain repeated incisor positioning, then the patient is most likely in need of a phase of splint therapy. lso, if the TMJ examination reveals joint or muscle symptoms, then the patient should undergo a phase of splint therapy. Using the above technique has proven to be the best method of avoiding mandibular positioning errors. DR. KEIM The role of condylar remodeling in the long-term instability of many cases has only recently been fully understood. Could you speak to this issue? DR. MCLUGHLIN The work of Dr. rnett, Dr. Milam, and others has been very helpful in this area. They often refer to condylar remodeling as the last frontier in the TMJ management issue. The book presents an up-to-date discussion of this subject. In summary, condylar remodeling can be local (confined to smaller areas on the head of the condyle) or total (involving the entire head of the condyle). Local remodeling is also being referred to as functional remodeling, since it is observed in nearly everyone as a result of normal functioning. With this type of remodeling, ramus height is not affected and the occlusion remains stable. Total remodeling, which fortunately occurs in a small number of patients, is referred to as dysfunctional remodeling. This is the orthodontist s and surgeon s nightmare, since the ramus height is affected and the bite is unstable. It is also significant for the orthodontist, since it can disturb normal growth and development. Joint stabilization with splint therapy is important for these patients. lso, protocols for medical management of the joint are being developed, and, hopefully, this will allow us to begin improving our ability to help these patients. DR. KEIM You define three groups of cases: Group 1 is non-surgical, Group 3 is surgical, and Group 2 is borderline cases that could be treated surgically or non-surgically. Where do you draw the line between a Group 2 and a Group 3 case, one that definitely requires surgery? DR. MCLUGHLIN It is impossible to draw a clear line between surgical and non-surgical cases. This is due to cultural differences, personal patient preferences, the orthodontist s biases and preferences, financial factors, and availability of surgical treatment. Having said this, the more we can objectively evaluate our cases, the better our decision making will be. The rnett STC and CTP protocol allows us to do this. In addition, computerized access to these programs allows us to quickly evaluate cases as orthodontic and/or surgical. lso, options can be presented to the patient in a clear and concise manner, allowing them to participate more fully in these important decisions. DR. KEIM What do you mean by double 202 JCO/PRIL 2004
5 assessment of the difficult borderline surgical cases? DR. MCLUGHLIN Group 1 cases are evaluated only for orthodontic treatment, as they do not present with skeletal disharmonies that require a surgical assessment. Group 3 cases present with such severe skeletal disharmonies that it is readily apparent that an acceptable result cannot be achieved non-surgically. Therefore, these cases are evaluated for surgical-orthodontic treatment. Group 2 borderline cases, which can make up a fairly large group in the orthodontic practice, can benefit from a double assessment. That is, they can be evaluated for orthodontic treatment only and also for surgical-orthodontic treatment. In the past, this has been a tedious process, and has not been fully completed for most cases. However, the computerized STC and CTP allow the clinician to do it quickly and accurately. DR. KEIM Do you handle a Group 2 borderline case that opts for non-surgical treatment differently from a Group 1 non-surgical case? DR. MCLUGHLIN These patients are frequently our most difficult cases to manage orthodontically. It is often necessary to move teeth long distances, with added anchorage, periodontal, and instability concerns. Long-term retention is often required. These factors should be carefully explained to the patient, who may alternatively reconsider the surgical option. judgment can be coordinated with the patient s concerns to fine-tune and guide the case to a satisfactory completion. The two patients shown on the following pages are examples of how we used facial and dental planning in borderline cases one Class II and one Class III. DR. KEIM Rick, on behalf of our readers, I d like to thank you for this discussion. CKNOWLEDGMENTS: Dr. McLaughlin would like to thank Dr. John Bennett for his help in writing the book, as well as his completion of the line drawings and coordination with the publishers. He would also like to thank Michaele Carnahan and Patty Knecht for their assistance in his and Dr. rnett s office. REFERENCES 1. rnett, G.W. and McLaughlin, R.P.: Facial and Dental Planning for Orthodontists and Oral Surgeons, Mosby, St. Louis, rnett, G.W. and Worley, C.M. Jr.: The treatment motivation survey: Defining patient motivation for treatment, m. J. Orthod. 115: , rnett, G.W.; Jelic, J.S.; Kim, J.; Cummings, D.R.; Beress,.; Worley, C.M. Jr.; Chung, B.; and Bergman, R.: Soft tissue cephalometric analysis: Diagnosis and treatment planning of dentofacial deformity, m. J. Orthod. 116: , Lundstrom, F. and Lundstrom,.: Clinical evaluation of maxillary and mandibular prognathism, Eur. J. Orthod. 11: , rnett, G.W. and Bergman, R.T.: Facial keys to orthodontic diagnosis and treatment planning, Parts I and II, m. J. Orthod. 103: , , DR. KEIM What is the role of the doctor s subjective artistic and clinical judgment in such a system? DR. MCLUGHLIN Clinical judgment comes into play with each part of the clinical examination: the TMJs, the face three-dimensionally, and the condition of the dentition in its entirety. This judgment is also critical in the analysis of all of the records, and is essential in treatment planning of all aspects of the case. Objective norms serve as points of reference to improve our clinical judgment. lso, the doctor s subjective artistic VOLUME XXXVIII NUMBER 4 203







6 B C D 204 JCO/PRIL 2004








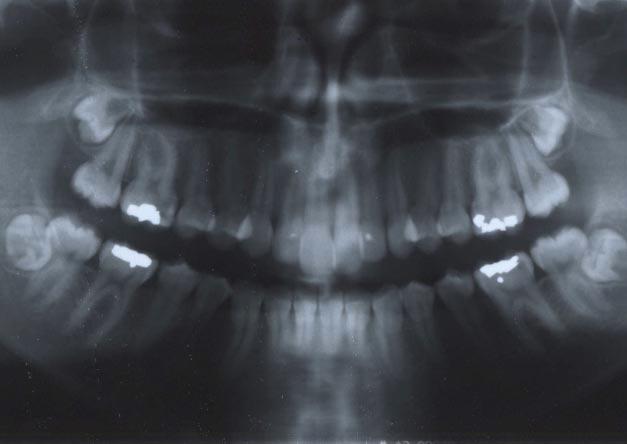
7 E Patient Z.D.. 15-year-old female patient with Class II skeletal and dental pattern. Maxillary molars were 6mm Class II on each side. Lower midline was symmetrical, with upper midline 1.5mm left. Lower arch showed minimal crowding, but upper anterior segment was moderately crowded. Panoramic radiograph showed all four third molars impacted. Evaluation indicated that patient could benefit from double assessment for surgical-orthodontic treatment and orthodontics only. B. rnett nalysis indicated maxilla in normal horizontal and vertical position, upper lip normal in thickness and length, and upper incisors in normal vertical and anteroposterior position, but slightly undertorqued. Mandible was severely retrusive, and lower incisors were proclined. C. Surgical-orthodontic analysis. Both arches could be aligned without extractions using interproximal reduction. Upper incisors could be slightly advanced, and lower incisors uprighted. fter orthodontic preparation, mandible could be surgically advanced approximately 6mm. D. Orthodontic analysis. Lower incisors could be left in original positions to contact lower anterior teeth, leaving molars in Class II relationship. This would result in some flattening of upper lip, but with average lip thickness, effect would be minimal. Patient elected orthodontic treatment only, following extraction of upper first bicuspids. E. Patient after 28 months of treatment; note small spaces remaining in upper extraction sites due to small upper lateral incisors and second bicuspids. E VOLUME XXXVIII NUMBER 4 205








8 B C D 206 JCO/PRIL 2004








9 E Patient R.C.. 14-year-old female patient with Class III skeletal and dental pattern. Posterior segments were about 4mm Class III on each side. Patient had narrow maxilla and bilateral crossbite. Lower anterior segment showed 7mm of crowding. Only lower third molars were present. Evaluation indicated that patient could benefit from double assessment for surgical-orthodontic treatment and orthodontics only. B. rnett nalysis indicated slight midface deficiency and slight mandibular prominence. Maxillary occlusal plane was steep, and lower incisors were extremely upright. C. Surgical-orthodontic analysis. Presurgical orthodontics would consist of rapid palatal expansion, followed by arch alignment without extractions, along with advancement of lower incisors and some interproximal reduction in lower anterior segment. When patient s growth was complete, two-jaw surgery would be performed with slight maxillary advancement, flattening of maxillary occlusal plane, and mandibular setback. D. Orthodontic analysis. Maxillary arch would be expanded and upper incisors advanced, allowing alignment without extractions. Mandibular crowding and lack of overbite created greatest challenge. Nonextraction treatment would result in lower incisor advancement and unacceptable overbite and overjet. Extraction of lower bicuspids was considered, but would create 14mm of space to offset 7mm of crowding, limiting need for Class III elastics. Decision was made to extract second molars, allowing Class III elastics to be used to retract lower dentition and extrude lower incisors. E. Patient after 38 months of treatment. E VOLUME XXXVIII NUMBER 4 207
Facial planning for orthodontists and oral surgeons
 ADVANCES IN ORTHODONTICS & DENTOFACIAL SURGERY Facial planning for orthodontists and oral surgeons G. William Arnett, DDS, FACD, a and Michael J. Gunson, DDS, MD b Santa Barbara, Calif The bite indicates
ADVANCES IN ORTHODONTICS & DENTOFACIAL SURGERY Facial planning for orthodontists and oral surgeons G. William Arnett, DDS, FACD, a and Michael J. Gunson, DDS, MD b Santa Barbara, Calif The bite indicates
Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction
 Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
The ASE Example Case Report 2010
 The ASE Example Case Report 2010 The Requirements for Case Presentation in The Angle Society of Europe are specified in the Appendix I to the Bylaws. This example case report exemplifies how these requirements
The ASE Example Case Report 2010 The Requirements for Case Presentation in The Angle Society of Europe are specified in the Appendix I to the Bylaws. This example case report exemplifies how these requirements
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER:44 CASE NUMBER: 2 Year: 2010 ESLO 01 RÉSUMÉ OF CASE 5 CASE CATEGORY: CLASS II DIVISION 1 MALOCCLUSION A MALOCCLUSION WITH SIGNIFICANT MANDIBULAR
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER:44 CASE NUMBER: 2 Year: 2010 ESLO 01 RÉSUMÉ OF CASE 5 CASE CATEGORY: CLASS II DIVISION 1 MALOCCLUSION A MALOCCLUSION WITH SIGNIFICANT MANDIBULAR
Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics
 Case Report Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics Isao Saito, DDS, PhD a ; Masaki Yamaki, DDS, PhD b ; Kooji Hanada,
Case Report Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics Isao Saito, DDS, PhD a ; Masaki Yamaki, DDS, PhD b ; Kooji Hanada,
AD2 MEASURES CONDYLE DISPLACEMENT (MCD) MANUAL
 MANUAL") AD2 MEASURES CONDYLE DISPLACEMENT (MCD) MANUAL Dr. Jorge Ayala Puente, DDS* Dr. Gonzalo Gutiérrez Álvarez, DDS* Dr. José Miguel Obach M., DDS Translation: Dr. Barbara Fernández Lübbert, DDS Edited: Dr.
AD2 MEASURES CONDYLE DISPLACEMENT (MCD) MANUAL Dr. Jorge Ayala Puente, DDS* Dr. Gonzalo Gutiérrez Álvarez, DDS* Dr. José Miguel Obach M., DDS Translation: Dr. Barbara Fernández Lübbert, DDS Edited: Dr.
Sample Case #1. Disclaimer
 ABO Sample Cases Disclaimer Sample Case #1 The following sample questions and answers were composed and vetted by a panel of experts in orthodontics and are intended to provide an example of the types
ABO Sample Cases Disclaimer Sample Case #1 The following sample questions and answers were composed and vetted by a panel of experts in orthodontics and are intended to provide an example of the types
Gentle-Jumper- Non-compliance Class II corrector
 15 CASE REPORT Gentle-Jumper- Non-compliance Class II corrector Amit Prakash 1,O.P.Mehta 2, Kshitij Gupta 3 Swapnil Pandey 4 Deep Kumar Suryawanshi 4 1 Senior lecturer Bhopal - INDIA 2 Professor Bhopal
15 CASE REPORT Gentle-Jumper- Non-compliance Class II corrector Amit Prakash 1,O.P.Mehta 2, Kshitij Gupta 3 Swapnil Pandey 4 Deep Kumar Suryawanshi 4 1 Senior lecturer Bhopal - INDIA 2 Professor Bhopal
2008 JCO, Inc. May not be distributed without permission. Correction of Asymmetry with a Mandibular Propulsion Appliance
 2008 JCO, Inc. May not be distributed without permission. www.jco-online.com CASE REPORT Correction of Asymmetry with a Mandibular Propulsion Appliance JOSÉ AUGUSTO MENDES MIGUEL, DDS, MSC, PHD GUSTAVO
2008 JCO, Inc. May not be distributed without permission. www.jco-online.com CASE REPORT Correction of Asymmetry with a Mandibular Propulsion Appliance JOSÉ AUGUSTO MENDES MIGUEL, DDS, MSC, PHD GUSTAVO
Mesial Step Class I or Class III Dependent upon extent of step seen clinically and patient s growth pattern Refer for early evaluation (by 8 years)
") Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Ortho-surgical Management of Severe Vertical Dysplasia: A Case Report
 Case Report Ortho-surgical Management of Severe Vertical Dysplasia: A Case Report 1 Vinni Arora, 2 Rekha Sharma, 3 Sachin Parashar 1 Senior Resident, 2 Professor and Head of Department, 3 Former Resident
Case Report Ortho-surgical Management of Severe Vertical Dysplasia: A Case Report 1 Vinni Arora, 2 Rekha Sharma, 3 Sachin Parashar 1 Senior Resident, 2 Professor and Head of Department, 3 Former Resident
Removable appliances
 Removable appliances Melinda Madléna DMD, PhD associate professor Department of Pedodontics and Orthodontics Faculty of Dentistry Semmelweis University Budapest Classification of the orthodontic anomalies
Removable appliances Melinda Madléna DMD, PhD associate professor Department of Pedodontics and Orthodontics Faculty of Dentistry Semmelweis University Budapest Classification of the orthodontic anomalies
KJLO. A Sequential Approach for an Asymmetric Extraction Case in. Lingual Orthodontics. Case Report INTRODUCTION DIAGNOSIS
 KJLO Korean Journal of Lingual Orthodontics Case Report A Sequential Approach for an Asymmetric Extraction Case in Lingual Orthodontics Ji-Sung Jang 1, Kee-Joon Lee 2 1 Dream Orthodontic Clinic, Gimhae,
KJLO Korean Journal of Lingual Orthodontics Case Report A Sequential Approach for an Asymmetric Extraction Case in Lingual Orthodontics Ji-Sung Jang 1, Kee-Joon Lee 2 1 Dream Orthodontic Clinic, Gimhae,
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 RÉSUMÉ
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 RÉSUMÉ
System Orthodontic Treatment Program By Dr. Richard McLaughlin, Dr. John Bennett and Dr. Hugo Trevisi
 A Clinical Review of the MBT Versatile+ Appliance System Orthodontic Treatment Program By Dr. Richard McLaughlin, Dr. John Bennett and Dr. Hugo Trevisi Treatment Philosophy of the MBT Appliance System
A Clinical Review of the MBT Versatile+ Appliance System Orthodontic Treatment Program By Dr. Richard McLaughlin, Dr. John Bennett and Dr. Hugo Trevisi Treatment Philosophy of the MBT Appliance System
2007 JCO, Inc. May not be distributed without permission.
 2007 JCO, Inc. May not be distributed without permission. www.jco-online.com CSE REPORT Correction of an symmetrical Class II Malocclusion Using Predictable Force Systems PIERO PLCIOS, DDS, MDS FLVIO URIBE,
2007 JCO, Inc. May not be distributed without permission. www.jco-online.com CSE REPORT Correction of an symmetrical Class II Malocclusion Using Predictable Force Systems PIERO PLCIOS, DDS, MDS FLVIO URIBE,
Class III malocclusion occurs in less than 5%
 CDABO CASE REPORT Orthodontic correction of a Class III malocclusion in an adolescent patient with a bonded RPE and protraction face mask Steven W. Smith, DDS, a and Jeryl D. English, DDS, MS b Dallas,
CDABO CASE REPORT Orthodontic correction of a Class III malocclusion in an adolescent patient with a bonded RPE and protraction face mask Steven W. Smith, DDS, a and Jeryl D. English, DDS, MS b Dallas,
The practice of orthodontics is faced with new
 CLINICIAN S CORNER A new approach to correction of crowding William Randol Womack, DDS, a Jae H. Ahn, DDS, MSD, b Zahra Ammari, DDS, MDSc, c and Anamaría Castillo, DDS, MS c Phoenix, Ariz, and Santa Clara,
CLINICIAN S CORNER A new approach to correction of crowding William Randol Womack, DDS, a Jae H. Ahn, DDS, MSD, b Zahra Ammari, DDS, MDSc, c and Anamaría Castillo, DDS, MS c Phoenix, Ariz, and Santa Clara,
THE MBT VERSATILE+ APPLIANCE SYSTEM
 THE MBT VERSATILE+ APPLIANCE SYSTEM McLaughlin, Bennett, Trevisi The MBT Versatile+ Appliance System THE DEVELOPMENT OF A TREATMENT MECHANICS AND APPLIANCE PHILOSOPHY The first fully programmed preadjusted
THE MBT VERSATILE+ APPLIANCE SYSTEM McLaughlin, Bennett, Trevisi The MBT Versatile+ Appliance System THE DEVELOPMENT OF A TREATMENT MECHANICS AND APPLIANCE PHILOSOPHY The first fully programmed preadjusted
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS Dr. Masatoshi Sana Year: ESLO 01 RÉSUMÉ OF CASE 8 CASE CATEGORY: TRANS / VERTICAL DISCREPANCY NAME: Akiko T. BORN : 15/03/1973 SEX: F PRE-TREATMENT RECORDS: AGE:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS Dr. Masatoshi Sana Year: ESLO 01 RÉSUMÉ OF CASE 8 CASE CATEGORY: TRANS / VERTICAL DISCREPANCY NAME: Akiko T. BORN : 15/03/1973 SEX: F PRE-TREATMENT RECORDS: AGE:
Class II Correction with Invisalign Molar rotation.
 Tips from your peers to help you treat with confidence. Class II Correction with Invisalign Molar rotation. Dr. Mazyar Moshiri. Class II Correction with Invisalign Molar Rotation. Dr. Mazyar Moshiri. Orthodontic
Tips from your peers to help you treat with confidence. Class II Correction with Invisalign Molar rotation. Dr. Mazyar Moshiri. Class II Correction with Invisalign Molar Rotation. Dr. Mazyar Moshiri. Orthodontic
Significant improvement with limited orthodontics anterior crossbite in an adult patient
 VARIA Significant improvement with limited orthodontics anterior crossbite in an adult patient Arzu Ari-Demirkaya Istanbul, Turkey Summary Objectives. Orthodontic treatment is known to last as long as
VARIA Significant improvement with limited orthodontics anterior crossbite in an adult patient Arzu Ari-Demirkaya Istanbul, Turkey Summary Objectives. Orthodontic treatment is known to last as long as
A SIMPLE METHOD FOR CORRECTION OF BUCCAL CROSSBITE OF MAXILLARY SECOND MOLAR
 Short Communication International Journal of Dental and Health Sciences Volume 01,Issue 03 A SIMPLE METHOD FOR CORRECTION OF BUCCAL CROSSBITE OF MAXILLARY SECOND MOLAR Sumit Yadav 1,Davender Kumar 2,Achla
Short Communication International Journal of Dental and Health Sciences Volume 01,Issue 03 A SIMPLE METHOD FOR CORRECTION OF BUCCAL CROSSBITE OF MAXILLARY SECOND MOLAR Sumit Yadav 1,Davender Kumar 2,Achla
Arrangement of the artificial teeth:
 Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER: 44 CASE NUMBER: 1 Year: ESLO 01 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME: K.N BORN: 03/03/1980 SEX: Male PRE-TREATMENT RECORDS:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER: 44 CASE NUMBER: 1 Year: ESLO 01 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME: K.N BORN: 03/03/1980 SEX: Male PRE-TREATMENT RECORDS:
Definition and History of Orthodontics
 In the name of GOD Definition and History of Orthodontics Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 1 William R. Proffit, Henry W. Fields, David M.Sarver.
In the name of GOD Definition and History of Orthodontics Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 1 William R. Proffit, Henry W. Fields, David M.Sarver.
Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report
 Case Report Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/506 Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report Ahmed Alassiry Assistant
Case Report Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/506 Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report Ahmed Alassiry Assistant
Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient
 Case Report Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient Masayoshi Kawakami, DDS, PhD a ; Takakazu Yagi, DDS, PhD b ; Kenji
Case Report Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient Masayoshi Kawakami, DDS, PhD a ; Takakazu Yagi, DDS, PhD b ; Kenji
Anterior Open Bite Correction with Invisalign Anterior Extrusion and Posterior Intrusion.
 Tips from your peers to help you treat with confidence. Anterior Open Bite Correction with Invisalign Anterior Extrusion and Posterior Intrusion. Dr. Linda Crawford DDS, MS, P.C. Anterior Open Bite Correction
Tips from your peers to help you treat with confidence. Anterior Open Bite Correction with Invisalign Anterior Extrusion and Posterior Intrusion. Dr. Linda Crawford DDS, MS, P.C. Anterior Open Bite Correction
ADOLESCENT TREATMENT. Thomas J. Cangialosi. Stella S. Efstratiadis. CHAPTER 18 Pages CLASS II DIVISION 1 WHY NOW?
 ADOLESCENT By Thomas J. Cangialosi and Stella S. Efstratiadis From Riolo, M. and Avery, J. Eds., Essentials for Orthodontic Practice, EFOP Press of EFOP, LLC. Ann Arbor and Grand Haven, Michigan, U.S.A.,
ADOLESCENT By Thomas J. Cangialosi and Stella S. Efstratiadis From Riolo, M. and Avery, J. Eds., Essentials for Orthodontic Practice, EFOP Press of EFOP, LLC. Ann Arbor and Grand Haven, Michigan, U.S.A.,
CASE: EXTRACTION Dr. TRAINING M (CA) Caucasian AGE: 8.6 VISUAL NORMS RMO X: 02/06/ R: 02/21/2003 MISSING PERMANENT TEETH RMO 2003
 Caucasian AGE: 8.6 VISUAL NORMS RMO X: 02/06/ R: 02/21/2003 MISSING PERMANENT TEETH RMO 2003") O C RMO CASE: EXTRACTION Dr. TRAINING M (CA) Caucasian AGE:. X: // - R: // MISSING PERMANENT TEETH VISUAL NORMS RMO R L RMO Diagnostic Services RMO, Inc. ()- Post Office Box ()- Canoga Park, CA - EXTRACTION
O C RMO CASE: EXTRACTION Dr. TRAINING M (CA) Caucasian AGE:. X: // - R: // MISSING PERMANENT TEETH VISUAL NORMS RMO R L RMO Diagnostic Services RMO, Inc. ()- Post Office Box ()- Canoga Park, CA - EXTRACTION
SURGICAL MODEL ACCURACY DEVICE. 25 years - manufacturing and distribution - around the globe research - design - manufacturing - distribution
 SURGICAL MODEL ACCURACY DEVICE 25 years - manufacturing and distribution - around the globe research - design - manufacturing - distribution 2 SMAD - SURGICAL MODEL ACCURACY DEVICE SMAD has be designed
SURGICAL MODEL ACCURACY DEVICE 25 years - manufacturing and distribution - around the globe research - design - manufacturing - distribution 2 SMAD - SURGICAL MODEL ACCURACY DEVICE SMAD has be designed
ORTHODONTICS Treatment of malocclusion Assist.Lec.Kasem A.Abeas University of Babylon Faculty of Dentistry 5 th stage
 Lec: Treatment of class I malocclusion Class I occlusion can be defined by Angles, classification as the mesiobuccal cusp of the upper 1 st permanent molar occlude with the developmental groove of the
Lec: Treatment of class I malocclusion Class I occlusion can be defined by Angles, classification as the mesiobuccal cusp of the upper 1 st permanent molar occlude with the developmental groove of the
OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 2 Year: 2010 WBLO 01 RESUME OF CASE 2 CASE CATEGORY: ADULT MALOCCLUSION NAME : MARIA A. BORN: 18.04.1983 SEX:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 2 Year: 2010 WBLO 01 RESUME OF CASE 2 CASE CATEGORY: ADULT MALOCCLUSION NAME : MARIA A. BORN: 18.04.1983 SEX:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS KANARELIS PANAGIOTIS (TAKIS) CASE NUMBER: 1 Year: 2012 WBLO 1 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS KANARELIS PANAGIOTIS (TAKIS) CASE NUMBER: 1 Year: 2012 WBLO 1 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME:
Concepts of occlusion Balanced occlusion. Monoplane occlusion. Lingualized occlusion. Figure (10-1)
") Any contact between teeth of opposing dental arches; usually, referring to contact between the occlusal surface. The static relationship between the incising or masticatory surfaces of the maxillary or
Any contact between teeth of opposing dental arches; usually, referring to contact between the occlusal surface. The static relationship between the incising or masticatory surfaces of the maxillary or
MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D
 by Masatada Koga, D.D.S., Ph.D") MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D Dr. Masatada Koga, D.D.S., Ph.D, is an assistant professor in the Department of Orthodontics
MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D Dr. Masatada Koga, D.D.S., Ph.D, is an assistant professor in the Department of Orthodontics
ortho case report Sagittal First international magazine of orthodontics By Dr. Luis Carrière Special Reprint
 Cover image courtesy of K Line Europe GmbH (www.kline-europe.de) ortho Special Reprint international magazine of orthodontics 1 2017 case report Sagittal First By Dr. Luis Carrière Sagittal First Author:
Cover image courtesy of K Line Europe GmbH (www.kline-europe.de) ortho Special Reprint international magazine of orthodontics 1 2017 case report Sagittal First By Dr. Luis Carrière Sagittal First Author:
Correction of Crowding using Conservative Treatment Approach
 Case Report Correction of Crowding using Conservative Treatment Approach Dr Tapan Shah, 1 Dr Tarulatha Shyagali, 2 Dr Kalyani Trivedi 3 1 Senior Lecturer, 2 Professor, Department of Orthodontics, Darshan
Case Report Correction of Crowding using Conservative Treatment Approach Dr Tapan Shah, 1 Dr Tarulatha Shyagali, 2 Dr Kalyani Trivedi 3 1 Senior Lecturer, 2 Professor, Department of Orthodontics, Darshan
An Evaluation of the Use of Digital Study Models in Orthodontic Diagnosis and Treatment Planning
 Original Article An Evaluation of the Use of Digital Study in Orthodontic Diagnosis and Treatment Planning Brian Rheude a ; P. Lionel Sadowsky b ; Andre Ferriera c ; Alex Jacobson d Abstract: The purpose
Original Article An Evaluation of the Use of Digital Study in Orthodontic Diagnosis and Treatment Planning Brian Rheude a ; P. Lionel Sadowsky b ; Andre Ferriera c ; Alex Jacobson d Abstract: The purpose
Crowded Class II Division 2 Malocclusion
 Class II Division 2 Malocclusion Crowded Class II Division 2 Malocclusion Clinicians: Drs. Chris Chang, Hsin-Yin Yeh, Sophia Pei-Wen Shu, W. Eugene Roberts Patient: Miss Jhan Pre-treatment Diagnosis An
Class II Division 2 Malocclusion Crowded Class II Division 2 Malocclusion Clinicians: Drs. Chris Chang, Hsin-Yin Yeh, Sophia Pei-Wen Shu, W. Eugene Roberts Patient: Miss Jhan Pre-treatment Diagnosis An
Ibelieve the time has come for the general dentists to
 EARLY ORTHODONTIC TREATMENT Brock Rondeau, D.D.S. I.B.O., D.A.B.C.P., D-A.C.S.D.D., D.A.B.D.S.M., D.A.B.C.D.S.M. Ibelieve the time has come for the general dentists to get serious and educated in an effort
EARLY ORTHODONTIC TREATMENT Brock Rondeau, D.D.S. I.B.O., D.A.B.C.P., D-A.C.S.D.D., D.A.B.D.S.M., D.A.B.C.D.S.M. Ibelieve the time has come for the general dentists to get serious and educated in an effort
TWO PHASE FOR A BETTER FACE!! TWIN BLOCK AND HEADGEAR FOLLOWED BY FIXED THERAPY FOR CLASS II CORRECTION
 Case Report NUJHS Vol. 5, No.2, June 2015, ISSN 2249-7110 TWO PHASE FOR A BETTER FACE!! TWIN BLOCK AND HEADGEAR FOLLOWED BY FIXED THERAPY FOR CLASS II CORRECTION 1 2 3 4 U S Krishna Nayak, Ashutosh Shetty,
Case Report NUJHS Vol. 5, No.2, June 2015, ISSN 2249-7110 TWO PHASE FOR A BETTER FACE!! TWIN BLOCK AND HEADGEAR FOLLOWED BY FIXED THERAPY FOR CLASS II CORRECTION 1 2 3 4 U S Krishna Nayak, Ashutosh Shetty,
ISW for the treatment of adult anterior crossbite with severe crowding combined facial asymmetry case
 International Research Journal of Medicine and Biomedical Sciences Vol.3 (2),pp. 15-29, November 2018 Available online at http://www.journalissues.org/irjmbs/ https://doi.org/10.15739/irjmbs.18.004 Copyright
International Research Journal of Medicine and Biomedical Sciences Vol.3 (2),pp. 15-29, November 2018 Available online at http://www.journalissues.org/irjmbs/ https://doi.org/10.15739/irjmbs.18.004 Copyright
Compromised nonsurgical treatment of a patient with a severe Class III malocclusion
 Clinical Compromised nonsurgical treatment of a patient with a severe Class III malocclusion Eric B Lowenhaupt Abstract: This case report describes the orthodontic diagnosis and treatment of a 13y10m Caucasian
Clinical Compromised nonsurgical treatment of a patient with a severe Class III malocclusion Eric B Lowenhaupt Abstract: This case report describes the orthodontic diagnosis and treatment of a 13y10m Caucasian
Early Mixed Dentition Period
 REVIEW ARTIC CLE AODMR The Effects of a Prefabricated Functional Appliance in Early Mixed Dentition Period Toshio Iwata 1, Takashi Usui 2, Nobukazu Shirakawa 2, Toshitsugu Kawata 3 1 Doctor of Philosophy
REVIEW ARTIC CLE AODMR The Effects of a Prefabricated Functional Appliance in Early Mixed Dentition Period Toshio Iwata 1, Takashi Usui 2, Nobukazu Shirakawa 2, Toshitsugu Kawata 3 1 Doctor of Philosophy
You. Fix. Could. This? Treatment solutions for typical and atypical adult relapse. 78 SEPTEMBER 2017 // orthotown.com
 by Dan Grob, DDS, MS, editorial director, Orthotown magazine You Could Fix This? Treatment solutions for typical and atypical adult relapse 78 SEPTEMBER 2017 // orthotown.com OT0917_Mechanics_AG.indd 78
by Dan Grob, DDS, MS, editorial director, Orthotown magazine You Could Fix This? Treatment solutions for typical and atypical adult relapse 78 SEPTEMBER 2017 // orthotown.com OT0917_Mechanics_AG.indd 78
The Tip-Edge appliance and
 Figure 1: Internal surfaces of the edgewise archwire slot are modified to create the Tip-Edge archwire slot. Tipping surfaces (T) limit crown tipping during retraction. Uprighting surfaces (U) control
Figure 1: Internal surfaces of the edgewise archwire slot are modified to create the Tip-Edge archwire slot. Tipping surfaces (T) limit crown tipping during retraction. Uprighting surfaces (U) control
Research & Reviews: Journal of Dental Sciences
 Research & Reviews: Journal of Dental Sciences Orthodontic Camouflage of Skeletal Class I, Class II and Class III Malocclusion in Borderline Cases Report of Three Cases Dr. Seema Kapil Lahoti 1 *, Dr.
Research & Reviews: Journal of Dental Sciences Orthodontic Camouflage of Skeletal Class I, Class II and Class III Malocclusion in Borderline Cases Report of Three Cases Dr. Seema Kapil Lahoti 1 *, Dr.
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER : 13 Dr. Masatoshi Sana CASE NUMBER : Year : ESLO 01 RÉSUMÉ OF CASE 2 CASE CATEGORY: CLASS I MALOCCLUSION NAME: BORN: SEX: Yukari K. 08/03/1979
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER : 13 Dr. Masatoshi Sana CASE NUMBER : Year : ESLO 01 RÉSUMÉ OF CASE 2 CASE CATEGORY: CLASS I MALOCCLUSION NAME: BORN: SEX: Yukari K. 08/03/1979
The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain
 Welcome Ron Not Ron? Click here. My Account The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain VOLUME 26 : NUMBER 03 : PAGES (165-178) 1992 CHRISTOPHER K. KESLING, DDS, MS Tooth movement in
Welcome Ron Not Ron? Click here. My Account The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain VOLUME 26 : NUMBER 03 : PAGES (165-178) 1992 CHRISTOPHER K. KESLING, DDS, MS Tooth movement in
Case Report. Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System and MatrixORTHOGNATHIC Plating System.
 Case Report Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System and MatrixORTHOGNATHIC Plating System. Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System
Case Report Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System and MatrixORTHOGNATHIC Plating System. Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System
The America Association of Oral and Maxillofacial Surgeons classify occlusion/malocclusion in to the following three categories:
 Subject: Orthognathic Surgery Policy Effective Date: 04/2016 Revision Date: 07/2018 DESCRIPTION Orthognathic surgery is an open surgical procedure that corrects anomalies or malformations of the lower
Subject: Orthognathic Surgery Policy Effective Date: 04/2016 Revision Date: 07/2018 DESCRIPTION Orthognathic surgery is an open surgical procedure that corrects anomalies or malformations of the lower
Angle Class II, division 2 malocclusion with severe overbite and pronounced discrepancy*
 O C a s e R e p o r t ngle Class II, division 2 malocclusion with severe overbite and pronounced discrepancy* Daniela Kimaid Schroeder** bstract This article reports the treatment of a young patient at
O C a s e R e p o r t ngle Class II, division 2 malocclusion with severe overbite and pronounced discrepancy* Daniela Kimaid Schroeder** bstract This article reports the treatment of a young patient at
JCO INTERVIEWS Drs. G. William Arnett and Michael J. Gunson on Esthetic Treatment Planning for Orthognathic Surgery
 2010 JCO, Inc. May not be distributed without permission. www.jco-online.com JCO INTERVIEWS Drs. G. William Arnett and Michael J. Gunson on Esthetic Treatment Planning for Orthognathic Surgery DR. CHUDASAMA
2010 JCO, Inc. May not be distributed without permission. www.jco-online.com JCO INTERVIEWS Drs. G. William Arnett and Michael J. Gunson on Esthetic Treatment Planning for Orthognathic Surgery DR. CHUDASAMA
Evaluation of maxillary protrusion malocclusion treatment effects with prosth-orthodontic method in old adults
 Evaluation of maxillary protrusion malocclusion treatment effects with prosth-orthodontic method in old adults Peicheng Xu, DDS, MSD, a and Honghu Liu, DDS, PhD b a Shanghai Xuhui Dental Hospital and b
Evaluation of maxillary protrusion malocclusion treatment effects with prosth-orthodontic method in old adults Peicheng Xu, DDS, MSD, a and Honghu Liu, DDS, PhD b a Shanghai Xuhui Dental Hospital and b
Fixed Twin Blocks. Guidelines for case selection are similar to those for removable Twin Block appliances.
 Fixed Twin Blocks Development of Fixed Twin Blocks Dr Clark has enjoyed the cooperation of Dynaflex in developing the Fixed Twin Block. Six years of clinical testing has confirmed that this technique produces
Fixed Twin Blocks Development of Fixed Twin Blocks Dr Clark has enjoyed the cooperation of Dynaflex in developing the Fixed Twin Block. Six years of clinical testing has confirmed that this technique produces
Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results.
 SM 3M Health Care Academy Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results. Christopher S. Riolo, DDS, M.S, Ph.D. Dr. Riolo received his DDS
SM 3M Health Care Academy Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results. Christopher S. Riolo, DDS, M.S, Ph.D. Dr. Riolo received his DDS
Forsus Class II Correctors as an Effective and Efficient Form of Anchorage in Extraction Cases
 Forsus Class II Correctors as an Effective and Efficient Form of Anchorage in Extraction Cases by Lisa Alvetro, DDS, MSD After receiving her DDS summa cum laude from Ohio State University, Dr. Alvetro
Forsus Class II Correctors as an Effective and Efficient Form of Anchorage in Extraction Cases by Lisa Alvetro, DDS, MSD After receiving her DDS summa cum laude from Ohio State University, Dr. Alvetro
SURGICAL - ORTHODONTIC TREATMENT OF CLASS II DIVISION 1 MALOCCLUSION IN AN ADULT PATIENT: A CASE REPORT
 Case Report International Journal of Dental and Health Sciences Volume 02, Issue 02 SURGICAL - ORTHODONTIC TREATMENT OF CLASS II DIVISION 1 MALOCCLUSION IN AN ADULT PATIENT: A CASE REPORT Amit Dahiya 1,Minakshi
Case Report International Journal of Dental and Health Sciences Volume 02, Issue 02 SURGICAL - ORTHODONTIC TREATMENT OF CLASS II DIVISION 1 MALOCCLUSION IN AN ADULT PATIENT: A CASE REPORT Amit Dahiya 1,Minakshi
ORTHODONTIC INITIAL ASSESSMENT FORM (OIAF) w/ INSTRUCTIONS
 w/ INSTRUCTIONS") Use the accompanying Tip Sheet and How to Score the Orthodontic Initial Assessment Form for guidance in completion of the assessment form. You will need this score sheet and a disposable ruler (or a Boley
Use the accompanying Tip Sheet and How to Score the Orthodontic Initial Assessment Form for guidance in completion of the assessment form. You will need this score sheet and a disposable ruler (or a Boley
OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 1 Year: 2010 WBLO 01 RESUME OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME : IOANNIS.G BORN: 03.01.1989 SEX:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 1 Year: 2010 WBLO 01 RESUME OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME : IOANNIS.G BORN: 03.01.1989 SEX:
Interview with Vincent KOKICH
 DOI: 10.1051/odfen/2010302 J Dentofacial Anom Orthod 2010;13:218-222 Ó RODF / EDP Sciences Interview with Vincent KOKICH Conducted by and translated by Sophie ROZENCWEIG Dr. Kokich, it has always been
DOI: 10.1051/odfen/2010302 J Dentofacial Anom Orthod 2010;13:218-222 Ó RODF / EDP Sciences Interview with Vincent KOKICH Conducted by and translated by Sophie ROZENCWEIG Dr. Kokich, it has always been
SPECIAL. The effects of eruption guidance and serial extraction on the developing dentition
 SPECIAL The effects of eruption guidance and serial extraction on the developing dentition Robert M. Little, DDS, MSD, PhD Clinical practice is a balance of our collective experience and intuitive clinical
SPECIAL The effects of eruption guidance and serial extraction on the developing dentition Robert M. Little, DDS, MSD, PhD Clinical practice is a balance of our collective experience and intuitive clinical
An Innovative Treatment Approach with Atypical Orthodontic Extraction Pattern in Bimaxillary Protrusion Case
 10.5005/jp-journals-10021-1127 CASE REPORT An Innovative Treatment Approach with Atypical Orthodontic Extraction Pattern in Bimaxillary Protrusion Case 1 Anil Miglani, 2 Reena R Kumar, 3 Ashish Chopra,
10.5005/jp-journals-10021-1127 CASE REPORT An Innovative Treatment Approach with Atypical Orthodontic Extraction Pattern in Bimaxillary Protrusion Case 1 Anil Miglani, 2 Reena R Kumar, 3 Ashish Chopra,
The conservative treatment of Class I malocclusion with maxillary transverse deficiency and anterior teeth crowding
 B B O C a s e R e p o r t The conservative treatment of Class I malocclusion with maxillary transverse deficiency and anterior teeth crowding Lincoln I. Nojima* Abstract This report describes the treatment
B B O C a s e R e p o r t The conservative treatment of Class I malocclusion with maxillary transverse deficiency and anterior teeth crowding Lincoln I. Nojima* Abstract This report describes the treatment
Treatment of Long face / Open bite
 In the name of GOD Treatment of Long face / Open bite in preadolescent children Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 13 William R. Proffit, Henry W.
In the name of GOD Treatment of Long face / Open bite in preadolescent children Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 13 William R. Proffit, Henry W.
Treatment of a severe class II division 1 malocclusion with twin-block appliance
 2018; 4(5): 167-171 ISSN Print: 2394-7500 ISSN Online: 2394-5869 Impact Factor: 5.2 IJAR 2018; 4(5): 167-171 www.allresearchjournal.com Received: 27-03-2018 Accepted: 28-04-2018 Dr. Sheetal Bohra Resident
2018; 4(5): 167-171 ISSN Print: 2394-7500 ISSN Online: 2394-5869 Impact Factor: 5.2 IJAR 2018; 4(5): 167-171 www.allresearchjournal.com Received: 27-03-2018 Accepted: 28-04-2018 Dr. Sheetal Bohra Resident
AUSTRALASIAN ORTHODONTIC BOARD
 AUSTRALASIAN ORTHODONTIC BOARD CASE IDENTIFICATION 18 - ST AUSTRALASIAN ORTHODONTIC BOARD CASE DETAILS (Form 2) After you have received your AOB Number, you must submit to your State Convenor 1 : Form
AUSTRALASIAN ORTHODONTIC BOARD CASE IDENTIFICATION 18 - ST AUSTRALASIAN ORTHODONTIC BOARD CASE DETAILS (Form 2) After you have received your AOB Number, you must submit to your State Convenor 1 : Form
Correction of Class II Division 2 Malocclusion by Fixed Functional Class II Corrector Appliance: Case Report
 Case Report To cite: Kumar M, Sharma H, Bohara P. Correction of class II division 2 malocclusion by fixed functional class II corrector appliance: case report. Journal of contemporary orthodontics, February
Case Report To cite: Kumar M, Sharma H, Bohara P. Correction of class II division 2 malocclusion by fixed functional class II corrector appliance: case report. Journal of contemporary orthodontics, February
Combined use of digital imaging technologies: ortho-surgical treatment
 DOI: 10.1051/odfen/2018059 J Dentofacial Anom Orthod 2018;21:210 The authors Combined use of digital imaging technologies: ortho-surgical treatment L. Petitpas Private practice, 54700 Pont-à-Mousson Are
DOI: 10.1051/odfen/2018059 J Dentofacial Anom Orthod 2018;21:210 The authors Combined use of digital imaging technologies: ortho-surgical treatment L. Petitpas Private practice, 54700 Pont-à-Mousson Are
Archived SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS
 SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS 14.1 CERTIFICATE OF MEDICAL NECESSITY...2 14.2 OPERATIVE REPORT...2 14.2.A PROCEDURES REQUIRING A REPORT...2 14.3 PRIOR AUTHORIZATION REQUEST...2 14.3.A
SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS 14.1 CERTIFICATE OF MEDICAL NECESSITY...2 14.2 OPERATIVE REPORT...2 14.2.A PROCEDURES REQUIRING A REPORT...2 14.3 PRIOR AUTHORIZATION REQUEST...2 14.3.A
ALTERNATE OCCLUSAL SCHEMES
 ALTERNATE OCCLUSAL SCHEMES The same basic concepts need to be applied to all occlusal schemes. Some challenges include missing teeth, transposed teeth, crossbites, and anterior open bites. POSTERIOR CROSSBITES
ALTERNATE OCCLUSAL SCHEMES The same basic concepts need to be applied to all occlusal schemes. Some challenges include missing teeth, transposed teeth, crossbites, and anterior open bites. POSTERIOR CROSSBITES
Orthodontic and Orthognathic Surgical Correction of a Skeletal Class III Malocclusion
 Dental Medicine Research 30 2) 161 166, 2010 161 Case Report Orthodontic and Orthognathic Surgical Correction of a Skeletal Class III Malocclusion Tetsutaro Yamaguchi, Yoko Tomoyasu, Tatsuo Shirota*, Masashi
Dental Medicine Research 30 2) 161 166, 2010 161 Case Report Orthodontic and Orthognathic Surgical Correction of a Skeletal Class III Malocclusion Tetsutaro Yamaguchi, Yoko Tomoyasu, Tatsuo Shirota*, Masashi
A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
 Dhaval Ranjitbhai Lekhadia, Gautham Hegde RESEARCH ARTICLE 10.5005/jp-journals-10029-1149 A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
Dhaval Ranjitbhai Lekhadia, Gautham Hegde RESEARCH ARTICLE 10.5005/jp-journals-10029-1149 A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
Treatment of Class II non-extraction using the Bioprogressive method
 DOI: 10.1051/odfen/2014013 J Dentofacial Anom Orthod 2014;17:407 Ó RODF / EDP Sciences Treatment of Class II non-extraction using the Bioprogressive method P. Guezenec CD SQODF, membre titulaire de la
DOI: 10.1051/odfen/2014013 J Dentofacial Anom Orthod 2014;17:407 Ó RODF / EDP Sciences Treatment of Class II non-extraction using the Bioprogressive method P. Guezenec CD SQODF, membre titulaire de la
Changes of the Transverse Dental Arch Dimension, Overjet and Overbite after Rapid Maxillary Expansion (RME)
") Dental Journal Changes of the Transverse Dental Arch Dimension, Overjet and Overbite after Rapid Maxillary Expansion (RME) Department of Advanced General Dentistry Faculty of Dentistry, Mahidol University.
Dental Journal Changes of the Transverse Dental Arch Dimension, Overjet and Overbite after Rapid Maxillary Expansion (RME) Department of Advanced General Dentistry Faculty of Dentistry, Mahidol University.
CASE: HISPANIC SAMPLE Dr. TRAINING F (LA) Latin AGE: 10.5 VISUAL NORMS RMO X: 06/23/ R: 02/21/2003 MISSING PERMANENT TEETH RMO 2003
 Latin AGE: 10.5 VISUAL NORMS RMO X: 06/23/ R: 02/21/2003 MISSING PERMANENT TEETH RMO 2003") O C RMO CASE: HISPANIC SAMPLE Dr. TRAINING F (LA) Latin AGE:. X: // - R: // MISSING PERMANENT TEETH VISUAL NORMS RMO R L RMO Diagnostic Services RMO, Inc. ()- Post Office Box 7 ()7- Canoga Park, CA -7
O C RMO CASE: HISPANIC SAMPLE Dr. TRAINING F (LA) Latin AGE:. X: // - R: // MISSING PERMANENT TEETH VISUAL NORMS RMO R L RMO Diagnostic Services RMO, Inc. ()- Post Office Box 7 ()7- Canoga Park, CA -7
Volume 22 No. 14 September Dentists, Federally Qualified Health Centers and Health Maintenance Organizations For Action
 State of New Jersey Department of Human Services Division of Medical Assistance & Health Services Volume 22 No. 14 September 2012 TO: Dentists, Federally Qualified Health Centers and Health Maintenance
State of New Jersey Department of Human Services Division of Medical Assistance & Health Services Volume 22 No. 14 September 2012 TO: Dentists, Federally Qualified Health Centers and Health Maintenance
APPENDIX A. MEDICAID ORTHODONTIC INITIAL ASSESSMENT FORM (IAF) You will need this scoresheet and a disposable ruler (or a Boley Gauge)
 You will need this scoresheet and a disposable ruler (or a Boley Gauge)") APPENDIX A MEDICAID ORTHODONTIC INITIAL ASSESSMENT FORM (IAF) You will need this scoresheet and a disposable ruler (or a Boley Gauge) Name: _ I. D. Number: Conditions: 1. Cleft palate deformities 2. Deep
APPENDIX A MEDICAID ORTHODONTIC INITIAL ASSESSMENT FORM (IAF) You will need this scoresheet and a disposable ruler (or a Boley Gauge) Name: _ I. D. Number: Conditions: 1. Cleft palate deformities 2. Deep
Treatment of Angle Class III. Department of Paedodontics and Orthodontics Dr. habil. Melinda Madléna associate professor
 Department of Paedodontics and Orthodontics Dr. habil. Melinda Madléna associate professor Disorders in Angle Class III The position of the lower jaw is foreward regarding to the upper jaw Mesialocclusion
Department of Paedodontics and Orthodontics Dr. habil. Melinda Madléna associate professor Disorders in Angle Class III The position of the lower jaw is foreward regarding to the upper jaw Mesialocclusion
Reliability of A and B point for cephalometric analysis
 Reliability of A and B point for cephalometric analysis Angle East Washington DC March, 2015 Carl P Roy, DDS, MS 1 History Orthodontic profession has always attempted to classify malocclusions. A-P relationship
Reliability of A and B point for cephalometric analysis Angle East Washington DC March, 2015 Carl P Roy, DDS, MS 1 History Orthodontic profession has always attempted to classify malocclusions. A-P relationship
RMO VISUAL NORMS. CASE: CHINESE SAMPLE Dr. TRAINING F (CH) Chinese AGE: 12.4 X: 09/30/ R: 02/21/2003 MISSING PERMANENT TEETH
 Chinese AGE: 12.4 X: 09/30/ R: 02/21/2003 MISSING PERMANENT TEETH") O C RMO CASE: CHINESE SAMPLE Dr. TRAINING F (CH) Chinese AGE:. X: // - R: // MISSING PERMANENT TEETH VISUAL NORMS RMO R L RMO Diagnostic Services RMO, Inc. ()- Post Office Box ()- Canoga Park, CA - CHINESE
O C RMO CASE: CHINESE SAMPLE Dr. TRAINING F (CH) Chinese AGE:. X: // - R: // MISSING PERMANENT TEETH VISUAL NORMS RMO R L RMO Diagnostic Services RMO, Inc. ()- Post Office Box ()- Canoga Park, CA - CHINESE
Case Report. profile relaxed relaxed smiling. How would you treat this malocclusion?
 Pre-Treatment profile relaxed relaxed smiling How would you treat this malocclusion? Case R. C. 16 years, 9 months introduction This female adolescent with bilabial protrusion and flared upper anterior
Pre-Treatment profile relaxed relaxed smiling How would you treat this malocclusion? Case R. C. 16 years, 9 months introduction This female adolescent with bilabial protrusion and flared upper anterior
PH-04A: Clinical Photography Production Checklist With A Small Camera
 PH-04A: Clinical Photography Production Checklist With A Small Camera Operator Name Total 0-49, Passing 39 Your Score Patient Name Date of Series Instructions: Evaluate your Series of photographs first.
PH-04A: Clinical Photography Production Checklist With A Small Camera Operator Name Total 0-49, Passing 39 Your Score Patient Name Date of Series Instructions: Evaluate your Series of photographs first.
Low-Force Mechanics Nonextraction. Estimated treatment time months (Actual 15 mos 1 week). Low-force mechanics.
. Low-force mechanics.") T.S. Age: 43 Years 1 Month Diagnosis: Class I Nonextraction Adult (severe crowding, very flat profile with tissue-grafting indications) Background: This case is very similar to the previous case of a 14-year-old.
T.S. Age: 43 Years 1 Month Diagnosis: Class I Nonextraction Adult (severe crowding, very flat profile with tissue-grafting indications) Background: This case is very similar to the previous case of a 14-year-old.
Surgical-Orthodontic Treatment of Gummy Smile with Vertical Maxillary Excess
 Case Report 10.5005/jp-journals-10021-1219 Surgical-Orthodontic Treatment of Gummy Smile with Vertical Maxillary Excess 1 Sumit Kumar Yadav, 2 Vikas Sehgal, 3 Sanjay Mittal ABSTRACT Vertical maxillary
Case Report 10.5005/jp-journals-10021-1219 Surgical-Orthodontic Treatment of Gummy Smile with Vertical Maxillary Excess 1 Sumit Kumar Yadav, 2 Vikas Sehgal, 3 Sanjay Mittal ABSTRACT Vertical maxillary
Invisalign technique in the treatment of adults with pre-restorative concerns
 Mampieri and Giancotti Progress in Orthodontics 2013, 14:40 REVIEW Open Access Invisalign technique in the treatment of adults with pre-restorative concerns Gianluca Mampieri * and Aldo Giancotti Abstract
Mampieri and Giancotti Progress in Orthodontics 2013, 14:40 REVIEW Open Access Invisalign technique in the treatment of adults with pre-restorative concerns Gianluca Mampieri * and Aldo Giancotti Abstract
The following standards and procedures apply to the provision of orthodontic services for children in the Medicaid/NJ FamilyCare (NJFC) programs.
 programs.") B.4.2.11 Orthodontic Services The following standards and procedures apply to the provision of orthodontic services for children in the Medicaid/NJ FamilyCare (NJFC) programs. Orthodontic Consultation
B.4.2.11 Orthodontic Services The following standards and procedures apply to the provision of orthodontic services for children in the Medicaid/NJ FamilyCare (NJFC) programs. Orthodontic Consultation
Severe Malocclusion: Appropriately Timed Treatment. This article discusses challenging issues clinicians face when treating
 Severe Malocclusion: The Importance of Appropriately Timed Treatment A Synchronized and Simultaneous Interdisciplinary Plan Using Cosmetic Dentistry Principles David M. Sarver, DMD, MS Abstract This article
Severe Malocclusion: The Importance of Appropriately Timed Treatment A Synchronized and Simultaneous Interdisciplinary Plan Using Cosmetic Dentistry Principles David M. Sarver, DMD, MS Abstract This article
PREDICTABILITY IN COMPREHENSIVE RECONSTRUCTION Bite registration and recovery process for comprehensive reconstructive cases.
 PREDICTABILITY IN COMPREHENSIVE RECONSTRUCTION Bite registration and recovery process for comprehensive reconstructive cases. By Matt Roberts The most predictable comprehensive restorative techniques revolve
PREDICTABILITY IN COMPREHENSIVE RECONSTRUCTION Bite registration and recovery process for comprehensive reconstructive cases. By Matt Roberts The most predictable comprehensive restorative techniques revolve
MEDICAL ASSISTANCE BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE
 MEDICAL ASSISTANCE BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE ISSUE DATE EFFECTIVE DATE NUMBER October 21,1996 October 28,1996 03-96-06 SUBJECT BY Information on New Procedures
MEDICAL ASSISTANCE BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE ISSUE DATE EFFECTIVE DATE NUMBER October 21,1996 October 28,1996 03-96-06 SUBJECT BY Information on New Procedures
#45 Ortho-Tain, Inc PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT
 #45 Ortho-Tain, Inc. 1-800-541-6612 PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT Analysis and Diagnosis of Occlusion: The ideal child of 5 y ears of age that probably has the best chance
#45 Ortho-Tain, Inc. 1-800-541-6612 PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT Analysis and Diagnosis of Occlusion: The ideal child of 5 y ears of age that probably has the best chance
Case Report Unilateral Molar Distalization: A Nonextraction Therapy
 Case Reports in Dentistry Volume 2012, Article ID 846319, 4 pages doi:10.1155/2012/846319 Case Report Unilateral Molar Distalization: A Nonextraction Therapy M. Bhanu Prasad and S. Sreevalli Department
Case Reports in Dentistry Volume 2012, Article ID 846319, 4 pages doi:10.1155/2012/846319 Case Report Unilateral Molar Distalization: A Nonextraction Therapy M. Bhanu Prasad and S. Sreevalli Department
Response Type axium Adult Comprehensive Oral Examination (COE)
") Page 1 1. RADIOGRAPHIC EVALUATION 1001 Panoramic image (PAN) Maxillary sinuses Nasal cavity TMJ complex Mandibular canal visualization?bone anomalies (eg. radiopacity/radiolucency) Soft tissue abnormalities
Page 1 1. RADIOGRAPHIC EVALUATION 1001 Panoramic image (PAN) Maxillary sinuses Nasal cavity TMJ complex Mandibular canal visualization?bone anomalies (eg. radiopacity/radiolucency) Soft tissue abnormalities
Preventive Orthodontics
 Semmelweis University Faculty of Dentistry Department in Community Dentistry director: Dr. Kivovics Péter assoc.prof. http://semmelweis-egyetem.hu/fszoi/ https://www.facebook.com/fszoi Preventive Orthodontics
Semmelweis University Faculty of Dentistry Department in Community Dentistry director: Dr. Kivovics Péter assoc.prof. http://semmelweis-egyetem.hu/fszoi/ https://www.facebook.com/fszoi Preventive Orthodontics
S.H. Age: 15 Years 3 Months Diagnosis: Class I Nonextraction Severe crowding, very flat profile. Background:
 S.H. Age: 15 Years 3 Months Diagnosis: Class I Nonextraction Severe crowding, very flat profile Background: This case was selected to illustrate the long-term impact of treatment planning on the face and
S.H. Age: 15 Years 3 Months Diagnosis: Class I Nonextraction Severe crowding, very flat profile Background: This case was selected to illustrate the long-term impact of treatment planning on the face and
Class II correction with Invisalign - Combo treatments. Carriere Distalizer.
 Tips from your peers to help you treat with confidence. Class II correction with Invisalign - Combo treatments. Carriere Distalizer. Dr. Clark D. Colville. Carriere Distalizer and Invisalign Combo. A distalization
Tips from your peers to help you treat with confidence. Class II correction with Invisalign - Combo treatments. Carriere Distalizer. Dr. Clark D. Colville. Carriere Distalizer and Invisalign Combo. A distalization
The Modified Twin Block Appliance in the Treatment of Class II Division 2 Malocclusions
 Journal of Orthodontics/Vol. 28/2001/271 280 The Modified Twin Block Appliance in the Treatment of Class II Division 2 Malocclusions F. M. V. DYER H. F. MCKEOWN P. J. SANDLER Department of Orthodontics,
Journal of Orthodontics/Vol. 28/2001/271 280 The Modified Twin Block Appliance in the Treatment of Class II Division 2 Malocclusions F. M. V. DYER H. F. MCKEOWN P. J. SANDLER Department of Orthodontics,
Non-surgical management of skeletal malocclusions: An assessment of 100 cases
 Non-surgical management of skeletal malocclusions: An assessment of 100 cases In early 1970 s reduced risks associated with surgical procedures allowed the treatment planning process for skeletal malocclusions
Non-surgical management of skeletal malocclusions: An assessment of 100 cases In early 1970 s reduced risks associated with surgical procedures allowed the treatment planning process for skeletal malocclusions