Data Exchange Workgroup Dental Subworkgroup Dental Claims White Paper
|
|
|
- Sherman Nichols
- 5 years ago
- Views:
Transcription
 to the ASC X12N 005010X224A2 Health Care Claim: Dental (837D) June 13,")
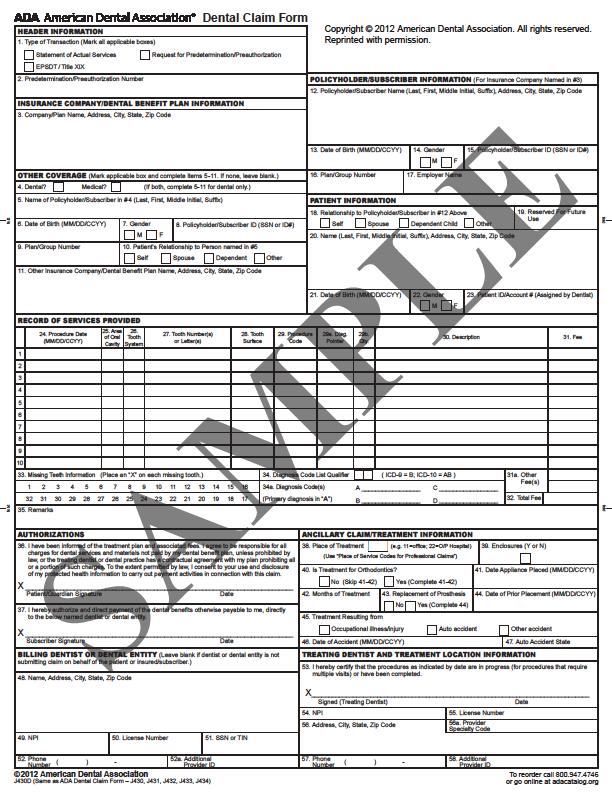
1 Data Exchange Workgroup Dental Subworkgroup Dental Claims White Paper White Paper: Mapping of the ADA Dental Claim Form ( 2012 American Dental Association) to the ASC X12N X224A2 Health Care Claim: Dental (837D) June 13, 2018
2 Workgroup for Electronic Data Interchange 1984 Isaac Newton Square, Suite 304, Reston, VA T: /F: Workgroup for Electronic Data Interchange, All Rights Reserved CONTENT Disclaimer I. Purpose II. III. IV. Scope Description of Mapping Acknowledgements List of Appendices Appendix A. ADA Dental Claim Form ( 2012 American Dental Association Appendix B. Mapping of the ADA Dental Claim Form to the ASC X12N X224A2 Health Care Claim: Dental (837D) 1
3 Disclaimer This document is Copyright 2018 by The Workgroup for Electronic Data Interchange (WEDI). It may be freely redistributed in its entirety provided that this copyright notice is not removed. It may not be sold for profit or used in commercial documents without the written permission of the copyright holder. This document is provided as is without any express or implied warranty. While all information in this document is believed to be correct at the time of writing, this document is for educational purposes only and does not purport to provide legal advice. If you require legal advice, you should consult with an attorney. The information provided here is for reference use only and does not constitute the rendering of legal, financial, or other professional advice or recommendations by the Workgroup for Electronic Data Interchange. The listing of an organization does not imply any sort of endorsement and the Workgroup for Electronic Data Interchange takes no responsibility for the products, tools, and Internet sites listed. The existence of a link or organizational reference in any of the following materials should not be assumed as an endorsement by the Workgroup for Electronic Data Interchange (WEDI), or any of the individual workgroups or subworkgroups of the WEDI Strategic National Implementation Process (WEDI SNIP). Document is for Education and Awareness Use Only Intellectual Property Citations The intellectual property in Appendix B (the mapping appendix) of this document belongs to X12. The link to X12 s Intellectual Property (IP) use can be found at: The intellectual property in the Appendix A (the dental claim form) belongs to the American Dental Association ( 2012 American Dental Association). The form illustrated in full in this Appendix, and portions illustrated in other chapters, are used with permission. This form is cited as the ADA Dental Claim Form or ADA Form within this White Paper. 2
4 Mapping of the ADA Dental Claim Form ( 2012 American Dental Association) to the ASC X12N X224A2 Health Care Claim: Dental (837D) I. Purpose The purpose of this white paper is to provide guidance on how to populate the ASC X12N X224A2 Health Care Claim: Dental (837D) electronic transaction from the data reported on the ADA Dental Claim Form ( 2012 American Dental Association). The ASC X12N X224A2 Health Care Claim: Dental (837D) is the current HIPAA adopted version of the electronic dental claim transaction. II. Scope The scope of this paper is to identify the mapping of the ADA Dental Claim Form to the ASC X12N X224A2 Health Care Claim: Dental (837D). III. Description of Mapping The ADA Dental Claim Form (Appendix A) was developed for dental providers and office staff to submit claims to be reimbursed by payers for services rendered. With today s focus on conducting claims and other administrative transactions electronically, it is important to have the ability to map the data from the ADA Dental Claim Form ( 2012 American Dental Association) to the ASC X12N X224A2 Health Care Claim: Dental (837D) electronic transaction. The Mapping of the ADA Dental Claim Form to the ASC X12N X224A2 Health Care Claim: Dental (837D) (Appendix B) provides the information a user needs to populate the electronic transaction with the data from the ADA Dental Claim Form. 3

5 Instructional Guide: In order to use this white paper, use Appendix A as a starting reference point. For example, under the Header box in the top left corner of Appendix A there is the Number 1. Number 2 for Predetermination/Preauthorization Number is immediately under Number 1. The chart in Appendix B maps the data elements on the ADA Dental Claim Form to the corresponding loops and segments in the ASC X12N X224A2 Health Care Claim: Dental (837D) electronic transaction. 4
6 For more information, refer to: The ADA Dental Claim Form ( 2012 American Dental Association) ( (The ASC X12N X224A2 Health Care Claim: Dental (837D) Technical Report Type 3 ( IV. Acknowledgements The co-chairs would like to extend our special thanks to all members of the WEDI Dental Workgroup with particular note to the following individuals. Tom Drinkard, Delta Dental of Virginia Frank Pokorny, American Dental Association Eric Kirnbauer, Tesia Clearinghouse, LLC. 5
7 Appendix A: ADA Dental Claim Form ( 2012 American Dental Association). In order to preserve the user-friendliness of the document, a title Appendix A does not appear in any of the margins. Consider this page as a cover page. The ADA Dental Claim Form is reprinted with the permission of the American Dental Association. See the American Dental Association s requested form name and copyright citations at the top and bottom right-hand side of the form image. 6
8 7
9 Appendix B: Mapping of the ADA Dental Claim Form ( 2012 American Dental Association) to the ASC X12N X224 Health Care Claim: Dental (837D) The following is the mapping of the ADA Dental Claim Form to the ASC X12N X224A2 Health Care Claim: Dental (837D). Location on ADA Dental Claim Form ADA Dental Claim Form Header Statement of actual services Request for Predetermination/Preauthorization EPSDT / Title XIX Predetermination/Preauthorization Number Insurance Company/Dental Benefit Plan Company/Plan Name, Address, City, State, Zip Code Dental? Medical? D Electronic Transaction Loop, Segment, and Element 2300 CLM / (empty) 2300 CLM / PB 2300 CLM REF (REF01 = 'G1') Prior Authorization ID 2300 REF (REF01 = 'G3') Predetermination ID 2010BB NM BB N BB N BB N BB N BB N SBR (is present) 2320 SBR (is present) 8
10 Location on ADA Dental Claim Form ADA Dental Claim Form Header Name of Policyholder/Subscriber in #4 (Last, First, Middle Initial, Suffix) Date of Birth Gender Policyholder/Subscriber ID (SSN or ID#) Plan / Group Number Patient's Relationship to Person named in #5 Other Insurance Company/Dental Benefit Plan Name, Address, City, State, Zip Code Policyholder/Subscriber (For Insurance Company Named in #3) Policyholder/Subscriber Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code Policyholder/Subscriber (For Insurance Company Named in #3) Policyholder/Subscriber (For Insurance Company Named in #3) Gender D Electronic Transaction Loop, Segment, and Element 2330A NM A NM A NM A NM N/A N/A 2330A NM SBR SBR B NM B N B N B N B N B N BA NM BA NM BA NM BA NM BA N BA N BA N BA N BA N Date of Birth 2010BA DMG BA DMG
11 Location on ADA Dental Claim Form ADA Dental Claim Form Header Policyholder/Subscriber (For Insurance Company Named in #3) Policyholder/Subscriber ID (SSN or ID#) Policyholder/Subscriber (For Insurance Company Named in #3) Plan / Group Number Policyholder/Subscriber (For Insurance Company Named in #3) Employer Name Patient Relationship to Primary Policyholder/Subscriber in #12 Above D Electronic Transaction Loop, Segment, and Element 2010BA NM BA SBR N/A 19 Reserved for Future Use N/A Patient Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code Patient Date of Birth Patient Gender Patient Patient ID/Account # (Assigned by Dentist) Procedure Date Area of Oral Cavity 2010CA PAT BA SBR CA NM CA NM CA NM CA NM CA N CA N CA N CA N CA N CA DMG CA DMG CLM DTP (DTP01 = 472) 2400 DTP (DTP01 = 472) 2400 SV
12 Location on ADA Dental Claim Form a 29b ADA Dental Claim Form Header Tooth System Tooth Number(s) or Letter(s) Tooth Surface Procedure Code Sales Tax Note when using CDT Code D9985: CDT Code D9985 is recorded on any unused line (1 through 10) in the ' section of the form. NOTE: Billing entities may record sales tax in different Diag Pointer Qty Description Sales Tax Note when using CDT Code D9985: Enter Sales Tax. Fee D Electronic Transaction Loop, Segment, and Element 2400 TOO TOO TOO TOO TOO TOO TOO SV Sales Tax Note when using CDT Code D9985: CDT Code D9985 is recorded on any unused line (1 through 10) in the Record of Services Provided' section of the form. NOTE: Billing entities may record sales tax in different 2400 SV SV SV SV SV SV SV
13 Location on ADA Dental Claim Form 31a 32 ADA Dental Claim Form Header Other Fees NOTE: Do not include sales tax in 31a when reported on a separate service line with CDT Code D9985. Total Fee 33 Missing Teeth 34 Diagnosis Code List Qualifier 34a (A) 34a (B,C, or D) Diagnosis Code (Primary Diagnosis) Diagnosis Code D Electronic Transaction Loop, Segment, and Element 2300 CLM DN (DN202 = M) 2300 HI HI HI HI HI HI HI HI Remarks 2300 NTE Authorizations - Release of Patient/Guardian 2300 CLM Signature Authorizations - Release of N/A Date Authorizations - Assignment of Benefits 2300 CLM Subscriber Signature Authorizations - Assignment of Benefits Date N/A CLM Place of Treatment 39 Enclosures (Y or N) 2300 PWK
14 Location on ADA Dental Claim Form ADA Dental Claim Form Header Is Treatment for Orthodontics? (No) Is Treatment for Orthodontics? (Yes) Date Appliance Placed Orthodontic Treatment Months Count Replacement of Prosthesis? (Yes) Replacement of Prosthesis? (No) Date of Prior Placement Treatment Resulting From Occupational illness/injury Treatment Resulting From Auto Accident Treatment Resulting From Other Accident Date of Accident Auto Accident State D Electronic Transaction Loop, Segment, and Element 2300 DN1 (is absent) 2300 DN1 (is present) 2300 DTP (DTP01 = 452) 2300 DN SV (SV305 = 'R') 2400 SV (SV305 = 'I') 2400 DTP (DTP01 = 441) 2300 CLM (CLM11-1 = 'EM') 2300 CLM (CLM11-2 = 'EM') 2300 CLM (CLM11-1 = 'AA') 2300 CLM (CLM11-2 = 'AA') 2300 CLM (CLM11-1 = 'OA') 2300 CLM (CLM11-2 = 'OA') 2300 DTP (DTP01 = '439') 2300 CLM
15 Location on ADA Dental Claim Form a ADA Dental Claim Form Header Billing Dentist or Dental Entity Name, Address, City, State, Zip Code Billing Dentist or Dental Entity NPI Billing Dentist or Dental Entity License Number Billing Dentist or Dental Entity SSN or TIN Billing Dentist or Dental Entity Phone Number Billing Dentist or Dental Entity Additional Provider ID Treating Dentist and Treatment Location Signed (Treating Dentist) Treating Dentist and Treatment Location Date Treating Dentist and Treatment Location NPI D Electronic Transaction Loop, Segment, and Element 2010AA NM AA NM AA NM AA NM AA N AA N AA N AA N AA N AA NM AA REF (REF01 = '0B') 2010AA REF (REF01 = 'EI') 2010AA REF (REF01 = 'SY') 2010AA PER (PER03 = 'TE') 2010AA PER (PER05 = 'TE') 2010AA PER (PER07 = 'TE') 2010AA REF (REF01 = '1G') 2010BB REF (REF01 = 'G2') 2010BB REF (REF01 = 'LU') 2300 CLM (CLM06 = 'Y') N/A 2310B NM
16 Location on ADA Dental Claim Form a ADA Dental Claim Form Header Treating Dentist and Treatment Location License Number Treating Dentist and Treatment Location Address, City, State, Zip Code Treating Dentist and Treatment Location Provider Specialty Code Treating Dentist and Treatment Location Phone Number Treating Dentist and Treatment Location Additional Provider ID D Electronic Transaction Loop, Segment, and Element 2310B REF (REF01 = '0B') 2310C NM C NM C NM C NM C N C N C N C N C N A PRV B PRV AA PER (PER03 = 'TE') 2010AA PER (PER05 = 'TE') 2010AA PER (PER07 = 'TE') 2310B PRV A PRV
SAMPLE. Dental Claim Form. X Patient/Guardian Signature. X Subscriber Signature. X Signed (Treating Dentist) 54. NPI 55.
 54. NPI 55.") HEADER INFORMATION 1. Type of Transaction (Mark all applicable boxes) Dental Claim Form fold fold Statement of Actual Services EPSDT / Title XIX 2. Predetermination/Preauthorization Number RECORD OF SERVICES
HEADER INFORMATION 1. Type of Transaction (Mark all applicable boxes) Dental Claim Form fold fold Statement of Actual Services EPSDT / Title XIX 2. Predetermination/Preauthorization Number RECORD OF SERVICES
ADA 2012 Claim Form Instructions
 Alaska Medical Assistance ADA 2012 laim Form Instructions This document is intended to provide Alaska Medicaid-specific instructions for completion of the ADA 2012 claim form. Each number listed in the
Alaska Medical Assistance ADA 2012 laim Form Instructions This document is intended to provide Alaska Medicaid-specific instructions for completion of the ADA 2012 claim form. Each number listed in the
ADA 2012 Dental Claim Form
 Claim Form Effective April 1, 2014, the West Virginia Medicaid and WVCHIP Program s claims processing system will begin accommodating the national version of the Claim Form. For Dental claim filing purposes,
Claim Form Effective April 1, 2014, the West Virginia Medicaid and WVCHIP Program s claims processing system will begin accommodating the national version of the Claim Form. For Dental claim filing purposes,
Clicking on the New Patient button allows the user to enter or edit patient and subscriber information to be stored for future use.
 Manual Claim Entry: Allows user to enter and submit claims manually. Clicking on the New Patient button allows the user to enter or edit patient and subscriber information to be stored for future use.
Manual Claim Entry: Allows user to enter and submit claims manually. Clicking on the New Patient button allows the user to enter or edit patient and subscriber information to be stored for future use.
Chapter 10 Billing on the ADA Claim Form
 10 Billing on the ADA Claim Form Reviewed/Revised: 10/10/2017, 02/01/2017, 02/15/2016, 09/16/2015, 09/18/2014 INTRODUCTION AHCCCS requires the reporting of all patient treatment provided by the dental
10 Billing on the ADA Claim Form Reviewed/Revised: 10/10/2017, 02/01/2017, 02/15/2016, 09/16/2015, 09/18/2014 INTRODUCTION AHCCCS requires the reporting of all patient treatment provided by the dental
Revised - See 09/24/2015 Version
 Dental Claim Form Instructions Claim Field Identification 1. Type of Transaction Statement of Actual Services EPSDT/Title XIX Request for Predetermination 2. Predetermination/ Prior Authorization Code
Dental Claim Form Instructions Claim Field Identification 1. Type of Transaction Statement of Actual Services EPSDT/Title XIX Request for Predetermination 2. Predetermination/ Prior Authorization Code
ADA Dental Claim Form (2018 American Dental Association) Completion Instructions Version 2 Effective January 1, 2019 Page 1 of 17
 Completion Instructions Version 2 Effective January 1, 2019 Page 1 of 17") Page 1 of 17 Introduction The ADA s Council on Dental Benefit Programs has responsibility for electronic and paper dental claim content and completion instructions. Staff from the Center for Dental Benefits,
Page 1 of 17 Introduction The ADA s Council on Dental Benefit Programs has responsibility for electronic and paper dental claim content and completion instructions. Staff from the Center for Dental Benefits,
Archived SECTION 15 - BILLING INSTRUCTIONS. Section 15 - Billing Instructions
 SECTION 15 - BILLING INSTRUCTIONS 15.1 ELECTRONIC DATA INTERCHANGE... 2 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION... 2 15.3 DENTAL CLAIM FORM... 3 15.4 PROVIDER RELATIONS COMMUNICATION UNIT... 3 15.5 RESUBMISSION
SECTION 15 - BILLING INSTRUCTIONS 15.1 ELECTRONIC DATA INTERCHANGE... 2 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION... 2 15.3 DENTAL CLAIM FORM... 3 15.4 PROVIDER RELATIONS COMMUNICATION UNIT... 3 15.5 RESUBMISSION
LIBERTY DENTAL PLAN LIBERTY QUARTERLY PROVIDER NEWS PROVIDER DIRECTORY VALIDATION LIBERTY DENTAL PLAN GROW YOUR BUSINESS UTILIZATION REVIEW
 GROW YOUR BUSINESS UTILIZATION REVIEW PROVIDER DIRECTORY VALIDATION LIBERTY DENTAL PLAN LIBERTY DENTAL PLAN VOLUME 4 Q1 SPRING 2018 LIBERTY QUARTERLY PROVIDER NEWS BUSINESS2BUSINESS LIBERTY DENTAL PLAN
GROW YOUR BUSINESS UTILIZATION REVIEW PROVIDER DIRECTORY VALIDATION LIBERTY DENTAL PLAN LIBERTY DENTAL PLAN VOLUME 4 Q1 SPRING 2018 LIBERTY QUARTERLY PROVIDER NEWS BUSINESS2BUSINESS LIBERTY DENTAL PLAN
Yale University - Group No. 4630
 Yale University - Group No. 4630 Dental Plan For Clerical & Technical Service & Maintenance & Yale Police Benevolent Association (YPBA) & Security Staff 1 Advancing Solutions For Great Oral Health January
Yale University - Group No. 4630 Dental Plan For Clerical & Technical Service & Maintenance & Yale Police Benevolent Association (YPBA) & Security Staff 1 Advancing Solutions For Great Oral Health January
D9995 and D9996 ADA Guide to Understanding and Documenting Teledentistry Events
 D9995 and D9996 ADA Guide Version 1 July 17, 2017 Page 1 of 10 D9995 and D9996 ADA Guide to Understanding and Documenting Teledentistry Events Developed by the ADA, this guide is published to educate dentists
D9995 and D9996 ADA Guide Version 1 July 17, 2017 Page 1 of 10 D9995 and D9996 ADA Guide to Understanding and Documenting Teledentistry Events Developed by the ADA, this guide is published to educate dentists
Dental Benefits Summary Delta Dental PPO plus Premier. Group # 9387
 Dental Benefits Summary Delta Dental PPO plus Premier Group # 9387 Topics Covered in This Booklet Page 1 About This Brochure 1 About Delta Dental 1 How to Use Your Program 2 Locating a Dentist 2-3 Why
Dental Benefits Summary Delta Dental PPO plus Premier Group # 9387 Topics Covered in This Booklet Page 1 About This Brochure 1 About Delta Dental 1 How to Use Your Program 2 Locating a Dentist 2-3 Why
New Patient Information
 Patient's Street Address: Home Phone: Cell Phone: of Birth: / / New Patient Information State: Name of Person Responsible for This Account: E-Mail Address: Zip Code: Work Phone: SSN: Do You Have Dental
Patient's Street Address: Home Phone: Cell Phone: of Birth: / / New Patient Information State: Name of Person Responsible for This Account: E-Mail Address: Zip Code: Work Phone: SSN: Do You Have Dental
EDITION SPECIAL INSIDE
 SUMMER 2008 Increase in Utilization of Crown Build-ups and Changes in Utilization Following an Audit Credentialing Tips and Reminders Online Fee Filing SPECIAL DELTA DENTAL OF MINNESOTA EDITION INSIDE
SUMMER 2008 Increase in Utilization of Crown Build-ups and Changes in Utilization Following an Audit Credentialing Tips and Reminders Online Fee Filing SPECIAL DELTA DENTAL OF MINNESOTA EDITION INSIDE
White Paper. Redefining Policies, Rules and Categories in ICD-10
 WEDI Strategic National Implementation Process (SNIP) WEDI SNIP ICD-10 Workgroup ICD-10 Crosswalks Sub Workgroup White Paper Redefining Policies, Rules and Categories in ICD-10 Published March 30, 2011
WEDI Strategic National Implementation Process (SNIP) WEDI SNIP ICD-10 Workgroup ICD-10 Crosswalks Sub Workgroup White Paper Redefining Policies, Rules and Categories in ICD-10 Published March 30, 2011
Dental Benefits Summary Delta Dental Premier/Delta Dental PPO/ Advantage Program
 Dental Benefits Summary Delta Dental Premier/Delta Dental PPO/ Advantage Program Group # 3196 Effective July 1, 2013 Topics Covered in This Booklet About This Brochure About Delta Dental How to Use Your
Dental Benefits Summary Delta Dental Premier/Delta Dental PPO/ Advantage Program Group # 3196 Effective July 1, 2013 Topics Covered in This Booklet About This Brochure About Delta Dental How to Use Your
DQA Measure Technical Specifications: Administrative Claims-Based Measures Per Member Per Month Cost of Clinical Services, Dental Services
 DQA Measure CCS-CH-A, Dental Services **Please read the DQA Measures User Guide prior to implementing this measure.** DQA Measure Technical Specifications: Administrative Claims-Based Measures Per Member
DQA Measure CCS-CH-A, Dental Services **Please read the DQA Measures User Guide prior to implementing this measure.** DQA Measure Technical Specifications: Administrative Claims-Based Measures Per Member
Guide to Dental Benefit Plans
 Guide to Dental Benefit Plans 211 E. Chicago Ave. Suite 1100 Chicago, IL 60611-2691 aae.org 2017 Patients often assume that dental coverage is similar to medical insurance, and they are shocked and angry
Guide to Dental Benefit Plans 211 E. Chicago Ave. Suite 1100 Chicago, IL 60611-2691 aae.org 2017 Patients often assume that dental coverage is similar to medical insurance, and they are shocked and angry
DQA Measure Technical Specifications: Administrative Claims-Based Measures Per Member Per Month Cost of Clinical Services, Dental Services
 DQA Measure CCS-CH-A, Dental Services **Please read the DQA Measures User Guide prior to implementing this measure.** DQA Measure Technical Specifications: Administrative Claims-Based Measures Per Member
DQA Measure CCS-CH-A, Dental Services **Please read the DQA Measures User Guide prior to implementing this measure.** DQA Measure Technical Specifications: Administrative Claims-Based Measures Per Member
Introduction to the Dental Blue Network and Other Products With Dental Benefits
 Introduction to the Dental Blue Network and Other Products With Dental Benefits An independent licensee of the Blue Cross and Blue Shield Association. U7430b, 2/11 BCBSNC Dental Products Dental Blue Products
Introduction to the Dental Blue Network and Other Products With Dental Benefits An independent licensee of the Blue Cross and Blue Shield Association. U7430b, 2/11 BCBSNC Dental Products Dental Blue Products
Services provided beyond a Member s benefit limit are not covered unless a BLE is requested and approved by Avesis.
 April 1, 2012 Dear Provider: Avesis would like to thank you for your continued participation in the Avesis UPMC for You dental network. This notice is to inform you of some upcoming changes to benefits
April 1, 2012 Dear Provider: Avesis would like to thank you for your continued participation in the Avesis UPMC for You dental network. This notice is to inform you of some upcoming changes to benefits
DQA Measure Technical Specifications: Administrative Claims-Based Measures Preventive Services for Children at Elevated Caries Risk, Dental Services
 DQA Measure PRV-CH-A, Dental Services **Please read the DQA Measures User Guide prior to implementing this measure.** DQA Measure Technical Specifications: Administrative Claims-Based Measures Preventive
DQA Measure PRV-CH-A, Dental Services **Please read the DQA Measures User Guide prior to implementing this measure.** DQA Measure Technical Specifications: Administrative Claims-Based Measures Preventive
Access Endodontics Marat Tselnik, DDS -PRACTICE LIMITED TO ENDODONTICS-
 Access Endodontics Marat Tselnik, DDS -PRACTICE LIMITED TO ENDODONTICS- REFERRED BY: TODAY S DATE: PATIENT NAME HOME PHONE (LAST) (FIRST) (MIDDLE) E-MAIL CELL PHONE HOME ADDRESS (STREET) (CITY) (STATE)
Access Endodontics Marat Tselnik, DDS -PRACTICE LIMITED TO ENDODONTICS- REFERRED BY: TODAY S DATE: PATIENT NAME HOME PHONE (LAST) (FIRST) (MIDDLE) E-MAIL CELL PHONE HOME ADDRESS (STREET) (CITY) (STATE)
Initial Clinical History and Physical Form
 601 E FM 544, Suite 400, Murphy, TX, 75094 TEL: 972-442-4700 Initial Clinical History and Physical Form Patient Information Name: Age: of Birth: / / Sex: Male / Female Marital Status: Single Married Divorced
601 E FM 544, Suite 400, Murphy, TX, 75094 TEL: 972-442-4700 Initial Clinical History and Physical Form Patient Information Name: Age: of Birth: / / Sex: Male / Female Marital Status: Single Married Divorced
Liberty Chiropractic Clinic Scarsdale Blvd., Houston, TX
 Liberty Chiropractic Clinic, -6154 Patient's Name Patient's Address City State Zip Code Age D.O.B. Single Married Divorced Widowed No. of children Occupation Employer Home Phone Work Phone Cell Phone Email
Liberty Chiropractic Clinic, -6154 Patient's Name Patient's Address City State Zip Code Age D.O.B. Single Married Divorced Widowed No. of children Occupation Employer Home Phone Work Phone Cell Phone Email
Dental Updates. Presentation by EDS Provider Field Consultants
 Dental Updates Presentation by EDS Provider Field Consultants October 2007 Agenda Objectives Provider Search National Provider Identifier New Dental Claim Form Dental Billing and Rendering Provider Information
Dental Updates Presentation by EDS Provider Field Consultants October 2007 Agenda Objectives Provider Search National Provider Identifier New Dental Claim Form Dental Billing and Rendering Provider Information
Child s Legal Name: Nickname: Male Female. Birth Date: Age: School: Grade: FATHER STEPMOTHER GUARDIAN? Insured s Name: D.O.B. Social Security #:
 Welcome Welcome to our practice! We strive to make each of your child s visits pleasant and comfortable. Our goal is to teach your child oral habits which will help keep their smile beautiful for their
Welcome Welcome to our practice! We strive to make each of your child s visits pleasant and comfortable. Our goal is to teach your child oral habits which will help keep their smile beautiful for their
Prior Authorization for Level 4 Deep Sedation and General Anesthesia Provided in Conjunction with Therapeutic Dental Treatment
 16.1.25.2 Prior Authorization for Level 4 Deep Sedation and General Anesthesia Provided in Conjunction with Therapeutic Dental Treatment Notice: MM/DD/YYYY Effective: July 1, 2017 Impacted Programs Health
16.1.25.2 Prior Authorization for Level 4 Deep Sedation and General Anesthesia Provided in Conjunction with Therapeutic Dental Treatment Notice: MM/DD/YYYY Effective: July 1, 2017 Impacted Programs Health
International Emergency and Expatriate Dental Program Instructions For Dentists
 International Emergency and Expatriate Dental Program Instructions For Dentists DeCare Dental is a leading dental benefit management company, serving a variety of dental benefit brand names across the
International Emergency and Expatriate Dental Program Instructions For Dentists DeCare Dental is a leading dental benefit management company, serving a variety of dental benefit brand names across the
2014 Rates. About Delta Dental networks BENEFITS OVERVIEW. Employee Only: $ Employee & Spouse: $ Employee & Child(ren): $83.
: $83.") BENEFITS OVERVIEW Benefit Summary for: Denny s, Inc. Effective Date: January 1, 2014 Plan Option: HIGH PLAN Delta Dental PPO Dentacare M Delta Dental PPO & Premier Non- Participating Providers Part-Time
BENEFITS OVERVIEW Benefit Summary for: Denny s, Inc. Effective Date: January 1, 2014 Plan Option: HIGH PLAN Delta Dental PPO Dentacare M Delta Dental PPO & Premier Non- Participating Providers Part-Time
New Patient Information
 New Patient Information Bloomfield Children s Dentistry 6405 Telegraph Road Bloomfield Hills, MI 48301 In order to get to know your family better, and to provide you with the best service, we ask that
New Patient Information Bloomfield Children s Dentistry 6405 Telegraph Road Bloomfield Hills, MI 48301 In order to get to know your family better, and to provide you with the best service, we ask that
NEW PATIENT PAPERWORK
 NEW PATIENT PAPERWORK Welcome! Please fill out the necessary paperwork provided. It is our pleasure to serve you and your family. How did you find out about us? If It was a friend or doctor, please list
NEW PATIENT PAPERWORK Welcome! Please fill out the necessary paperwork provided. It is our pleasure to serve you and your family. How did you find out about us? If It was a friend or doctor, please list
Contracting for Dental Services: Increase Access to Care
 Contracting for Dental Services: Increase Access to Care Irene V. Hilton, DDS, MPH Donald A. Simila, MSW, FACHE June 19, 2017 Objectives List scenarios in which health centers contract for dental services
Contracting for Dental Services: Increase Access to Care Irene V. Hilton, DDS, MPH Donald A. Simila, MSW, FACHE June 19, 2017 Objectives List scenarios in which health centers contract for dental services
Addiction Recovery Treatment Services (ARTS): Billing Best Practices. December 2017
: Billing Best Practices. December 2017") Addiction Recovery Treatment Services (ARTS): Billing Best Practices December 2017 Substance Use Billing Best Practices Following the guidelines, requirements, and protocols for billing substance use services
Addiction Recovery Treatment Services (ARTS): Billing Best Practices December 2017 Substance Use Billing Best Practices Following the guidelines, requirements, and protocols for billing substance use services
Idaho MMIS Provider Handbook
 Table of Contents 1. Section Modifications... 1 2. Guidelines... 2 2.1. General Policy... 2 2.2. Participant Eligibility... 2 2.2.1. Medicaid Basic Plan and Pregnant Women (PW) Program... 2 2.2.2. Medicaid
Table of Contents 1. Section Modifications... 1 2. Guidelines... 2 2.1. General Policy... 2 2.2. Participant Eligibility... 2 2.2.1. Medicaid Basic Plan and Pregnant Women (PW) Program... 2 2.2.2. Medicaid
Upperman Family Dental NEW PATIENT REGISTRATION
 Date Upperman Family Dental NEW PATIENT REGISTRATION First Name Middle Initial Last Name Patient is: Policy Holder Responsible Party Preferred Name Address Address 2 City, State, Zip Home Phone Cell Phone
Date Upperman Family Dental NEW PATIENT REGISTRATION First Name Middle Initial Last Name Patient is: Policy Holder Responsible Party Preferred Name Address Address 2 City, State, Zip Home Phone Cell Phone
**Please read the DQA Measures User Guide prior to implementing this measure.**
 **Please read the DQA Measures User Guide prior to implementing this measure.** DQA Measure Technical Specifications: Administrative Claims-Based Measures Prevention: Sealants for 6 9 year-old Children
**Please read the DQA Measures User Guide prior to implementing this measure.** DQA Measure Technical Specifications: Administrative Claims-Based Measures Prevention: Sealants for 6 9 year-old Children
**Please read the DQA Measures User Guide prior to implementing this measure.**
 **Please read the DQA Measures User Guide prior to implementing this measure.** DQA Measure Technical Specifications: Administrative Claims-Based Measures Prevention: Sealants for 6 9 year-old Children
**Please read the DQA Measures User Guide prior to implementing this measure.** DQA Measure Technical Specifications: Administrative Claims-Based Measures Prevention: Sealants for 6 9 year-old Children
Dental Benefits. Glossary. Delta Dental of Virginia DeltaDentalVA.com 1
 Dental Benefits Glossary Delta Dental of Virginia DeltaDentalVA.com 1 Table of Contents Dental Benefits Terms... 4 16 A Annual Maximum... 5 B Balance Billing... 5 Benefit Year... 5 Benefit Levels... 6
Dental Benefits Glossary Delta Dental of Virginia DeltaDentalVA.com 1 Table of Contents Dental Benefits Terms... 4 16 A Annual Maximum... 5 B Balance Billing... 5 Benefit Year... 5 Benefit Levels... 6
Florida Medicaid. Dental Services Coverage Policy. Agency for Health Care Administration
 Florida Medicaid Agency for Health Care Administration Table of Contents 1.0 Introduction... 1 1.1 Description... 1 1.2 Legal Authority... 1 1.3 Definitions... 1 2.0 Eligible Recipient... 2 2.1 General
Florida Medicaid Agency for Health Care Administration Table of Contents 1.0 Introduction... 1 1.1 Description... 1 1.2 Legal Authority... 1 1.3 Definitions... 1 2.0 Eligible Recipient... 2 2.1 General
International Emergency and Expatriate Dental Program
 International Emergency and Expatriate Dental Program Instructions for Dentists Program Outline We want to ensure you have the information you need to assist our members. Members of Delta Dental of Minnesota,
International Emergency and Expatriate Dental Program Instructions for Dentists Program Outline We want to ensure you have the information you need to assist our members. Members of Delta Dental of Minnesota,
Who is responsible for this account Relationship to patient. How did you hear about us (referral, facebook, etc.)?
?") EMERGENCY CONTACT INSURANCE PATIENT INFORMATION Name of Minor/Child SSN Sex: M F Age Birthdate Nickname Mailing Address City, State, Zip Physical Address City, State, Zip Home Phone Work Cell Email Address
EMERGENCY CONTACT INSURANCE PATIENT INFORMATION Name of Minor/Child SSN Sex: M F Age Birthdate Nickname Mailing Address City, State, Zip Physical Address City, State, Zip Home Phone Work Cell Email Address
Have you registered for the Arkansas Prescription Drug Monitoring Program?
 DENTAL BULLETIN WINTER 2016 Have you registered for the Arkansas Prescription Drug Monitoring Program? Any new provider coming into the Arkansas Blue Cross and Blue Shield networks must be registered with
DENTAL BULLETIN WINTER 2016 Have you registered for the Arkansas Prescription Drug Monitoring Program? Any new provider coming into the Arkansas Blue Cross and Blue Shield networks must be registered with
Family First Chiropractic
 Personal Information Title: (Check one) Mr. Mrs. Ms. Miss Other First Name Middle Initial Last Name Street City State Zip Code Email Home Phone ( ) - Cell Phone ( ) - Date of Birth / / Sex: Male Female
Personal Information Title: (Check one) Mr. Mrs. Ms. Miss Other First Name Middle Initial Last Name Street City State Zip Code Email Home Phone ( ) - Cell Phone ( ) - Date of Birth / / Sex: Male Female
GDA Coronal Polishing Enrollment Packet
 GDA Coronal Polishing Saturday, March 30, 2019 8 am to 5 pm 8200 Roberts Drive GDA Coronal Polishing Enrollment Packet Thank you for requesting information on the Georgia Dental Association s Coronal Polishing
GDA Coronal Polishing Saturday, March 30, 2019 8 am to 5 pm 8200 Roberts Drive GDA Coronal Polishing Enrollment Packet Thank you for requesting information on the Georgia Dental Association s Coronal Polishing
Family First Chiropractic
 Family First Chiropractic Personal Information Title: (Check one) Mr. Mrs. Ms. Miss Other First Name Middle Initial Last Name Street City State Zip Code Email Home Phone ( ) - Cell Phone ( ) - Date of
Family First Chiropractic Personal Information Title: (Check one) Mr. Mrs. Ms. Miss Other First Name Middle Initial Last Name Street City State Zip Code Email Home Phone ( ) - Cell Phone ( ) - Date of
Patient Registration (Please fill out one per family)
") Patient Registration (Please fill out one per family) Child s First and Last Name: Date of Birth: Child s Preferred Name: Gender: Male Female Child s Address: Child s City, Zip Code: Additional Children
Patient Registration (Please fill out one per family) Child s First and Last Name: Date of Birth: Child s Preferred Name: Gender: Male Female Child s Address: Child s City, Zip Code: Additional Children
plus DENTAL Willamette Dental of Idaho, Inc W. Emerald St., Suite 108, Boise, ID DENTAL INSURANCE Idaho
 Summary of Exclusions Coverage does not include: Conscious sedation/general anesthesia Any condition resulting from military service or war Injuries sustained while practicing or competing in a professional
Summary of Exclusions Coverage does not include: Conscious sedation/general anesthesia Any condition resulting from military service or war Injuries sustained while practicing or competing in a professional
Orthodontic Questionnaire. Please tell us why you have presented for evaluation and possible treatment. Dental History
 Orthodontic Consultation file:///c:/programdata/nierman/dentalwriternet/reports/out.html Version: ORTHOQ Orthodontic Questionnaire OFFICE USE Patient ID: NAME: -' Crowding ' Overbite CURRENT DATE: / /
Orthodontic Consultation file:///c:/programdata/nierman/dentalwriternet/reports/out.html Version: ORTHOQ Orthodontic Questionnaire OFFICE USE Patient ID: NAME: -' Crowding ' Overbite CURRENT DATE: / /
PATIENT MEDICAL HISTORY
 Patients Name: PATIENT MEDICAL HISTORY Address: Date of Last Visit: Date of Med History City: State: Zip: Email: Home Phone: Work Phone: Birth Date: Social Security No: Marital Status: Primary Dental Guarantor:
Patients Name: PATIENT MEDICAL HISTORY Address: Date of Last Visit: Date of Med History City: State: Zip: Email: Home Phone: Work Phone: Birth Date: Social Security No: Marital Status: Primary Dental Guarantor:
Welcome to Skyline Pediatric Dentistry!
 Welcome to Skyline Pediatric Dentistry! Patient Information Patient Name: Preferred Name: Today s Date: Birth Date: Age: Social Security #: Male Female Names of siblings: Responsible Party Information
Welcome to Skyline Pediatric Dentistry! Patient Information Patient Name: Preferred Name: Today s Date: Birth Date: Age: Social Security #: Male Female Names of siblings: Responsible Party Information
Jason A Boch DMD LLC Jason A. Boch, DMD DMSc Diplomate of the American Board of Periodontology
 Jason A Boch DMD LLC Jason A. Boch, DMD DMSc Diplomate of the American Board of Periodontology Patient Information Patient Name: of Birth: Gender (M/F): Name of Parent (if patient is a minor): Home Address:
Jason A Boch DMD LLC Jason A. Boch, DMD DMSc Diplomate of the American Board of Periodontology Patient Information Patient Name: of Birth: Gender (M/F): Name of Parent (if patient is a minor): Home Address:
Rhode Island Board of Examiners in Dentistry Room Capitol Hill Providence, RI Instructions and License Application for:
 CHECK LIST Application License Verification Employment letter Con. Ed. Compliance Tax Addendum **FOR OFFICE USE ONLY** Receipt # ID # Issue Date License # Rhode Island Board of Examiners in Dentistry Room
CHECK LIST Application License Verification Employment letter Con. Ed. Compliance Tax Addendum **FOR OFFICE USE ONLY** Receipt # ID # Issue Date License # Rhode Island Board of Examiners in Dentistry Room
Go the Extra Smile! How did you hear about Smile for a Lifetime?
 APPLICATION FORM Please print all pages and assure all fields are completed and each item below is included with this application. [ ] Applicant Questionnaire [ ] Copy of Report Card or Transcript [ ]
APPLICATION FORM Please print all pages and assure all fields are completed and each item below is included with this application. [ ] Applicant Questionnaire [ ] Copy of Report Card or Transcript [ ]
DQA Measure Technical Specifications: Administrative Claims-Based Measures Care Continuity, Dental Services
 **Please read the DQA Measures User Guide prior to implementing this measure.** DQA Measure Technical Specifications: Administrative Claims-Based Measures Care Continuity, Dental Services Description:
**Please read the DQA Measures User Guide prior to implementing this measure.** DQA Measure Technical Specifications: Administrative Claims-Based Measures Care Continuity, Dental Services Description:
Coding and Insurance. Manual A Comprehensive Resource For reporting Pediatric Dental Services
 Coding and Insurance Manual 2016 A Comprehensive Resource For reporting Pediatric Dental Services Table of Contents Coding and Insurance Manual 2016 1 Table of Contents Preface Introduction Acknowledgements
Coding and Insurance Manual 2016 A Comprehensive Resource For reporting Pediatric Dental Services Table of Contents Coding and Insurance Manual 2016 1 Table of Contents Preface Introduction Acknowledgements
PATIENT INFORMATION SHEET PERSON RESPONSIBLE FOR PAYMENT OF THIS ACCOUNT
 PATIENT INFORMATION SHEET Referred By: Patient s Name: SSN: Date of Birth: Address: City/Zip: Phone #: Sex: M / F Marital Status: M / S / W / D No. of Dependents: Email Address: Emergency Contact Person:
PATIENT INFORMATION SHEET Referred By: Patient s Name: SSN: Date of Birth: Address: City/Zip: Phone #: Sex: M / F Marital Status: M / S / W / D No. of Dependents: Email Address: Emergency Contact Person:
Additional Information Specification 0003: Rehabilitation Services Attachment
 Additional Information Specification 0003: Rehabilitation Services Attachment (This specification replaces Additional Information Message 0003: Rehabilitation Services Attachment September 1, 2002) Release
Additional Information Specification 0003: Rehabilitation Services Attachment (This specification replaces Additional Information Message 0003: Rehabilitation Services Attachment September 1, 2002) Release
SUMMARY OF BENEFITS 2017 PLAN INFORMATION
 SUMMARY OF BENEFITS 2017 PLAN INFORMATION Cigna Dental Insurance The Cigna Pediatric Dental Plan is included with the purchase of a Cigna Medical plan off Marketplace and covers dependents up to age 19.
SUMMARY OF BENEFITS 2017 PLAN INFORMATION Cigna Dental Insurance The Cigna Pediatric Dental Plan is included with the purchase of a Cigna Medical plan off Marketplace and covers dependents up to age 19.
DQA Measure Technical Specifications: Administrative Claims-Based Measures Treatment Services, Dental Services
 **Please read the DQA Measures User Guide prior to implementing this measure.** DQA Measure Technical Specifications: Administrative Claims-Based Measures Treatment Services, Dental Services Description:
**Please read the DQA Measures User Guide prior to implementing this measure.** DQA Measure Technical Specifications: Administrative Claims-Based Measures Treatment Services, Dental Services Description:
Written Protocol. Moving Tennessee Forward in Access to Care
 Written Protocol Moving Tennessee Forward in Access to Care Skilled Nursing Facilities Nursing Homes Public Health Programs Non- Profit Clinics History of the Legislation for Written Protocol Diana Saylor
Written Protocol Moving Tennessee Forward in Access to Care Skilled Nursing Facilities Nursing Homes Public Health Programs Non- Profit Clinics History of the Legislation for Written Protocol Diana Saylor
PATIENT INFORMATION SCHOOL/LOCATION
 PATIENT INFORMATION WWW.FAMILYCAREDENTISTRY.NET Date: NEW PATIENT UPDATE Patient: LAST FIRST MI PREFERRED TITLE MALE FEMALE CHILD* STUDENT** SINGLE MARRIED DIVORCED WIDOWED *IF CHILD, PROVIDE PARENT/GUARDIAN
PATIENT INFORMATION WWW.FAMILYCAREDENTISTRY.NET Date: NEW PATIENT UPDATE Patient: LAST FIRST MI PREFERRED TITLE MALE FEMALE CHILD* STUDENT** SINGLE MARRIED DIVORCED WIDOWED *IF CHILD, PROVIDE PARENT/GUARDIAN
Your Smile, Your Choice
 Your Smile, Your Choice Delta Dental PPO SM & DeltaCare USA Your company lets you choose between two dental plans from Delta Dental. Either way, you ll get reliable dentist networks and affordable preventive
Your Smile, Your Choice Delta Dental PPO SM & DeltaCare USA Your company lets you choose between two dental plans from Delta Dental. Either way, you ll get reliable dentist networks and affordable preventive
Affordable dental plan options for Blue Shield members
 Affordable dental plan options for Blue Shield members January 1 December 31, 2018 Blue Shield offers two optional supplemental dental plans to Blue Shield 65 Plus SM (HMO), Blue Shield 65 Plus Choice
Affordable dental plan options for Blue Shield members January 1 December 31, 2018 Blue Shield offers two optional supplemental dental plans to Blue Shield 65 Plus SM (HMO), Blue Shield 65 Plus Choice
Sample page. Relative Values for Dentists Relative values based on survey data from Relative Value Studies, Inc.
 2019 Relative Values for Dentists Relative values based on survey data from Relative Value Studies, Inc. Power up your coding optum360coding.com Contents Introduction...1 Getting Started... 1 Definitions
2019 Relative Values for Dentists Relative values based on survey data from Relative Value Studies, Inc. Power up your coding optum360coding.com Contents Introduction...1 Getting Started... 1 Definitions
NEW REQUIREMENT FOR THE SCHOOL YEAR:
 Dear Parent/Guardian There are new immunization requirements for students that are entering the 7 th grade AND those entering the 12 th grade. NEW REQUIREMENT FOR THE 2016-2017 SCHOOL YEAR: Starting in
Dear Parent/Guardian There are new immunization requirements for students that are entering the 7 th grade AND those entering the 12 th grade. NEW REQUIREMENT FOR THE 2016-2017 SCHOOL YEAR: Starting in
Tell Us About Your Child. Who is Accompanying Your Child Today? Parent Information. Primary Dental Insurance
 1 Today s Date: 2 (225) 664-2646 (225) 664-2640 (fax) 245 VETERANS BLVD. DENHAM SPRINGS, LA 70726 Who is Accompanying Your Child Today? Name: Relation: Do you have legal custody of this child? Yes No Tell
1 Today s Date: 2 (225) 664-2646 (225) 664-2640 (fax) 245 VETERANS BLVD. DENHAM SPRINGS, LA 70726 Who is Accompanying Your Child Today? Name: Relation: Do you have legal custody of this child? Yes No Tell
Patient Registration. First Name: Last Name: Middle Initial: Address: City, State, Zip: First Name: Last Name: Middle Initial:
 Patient Registration First Name: Last Name: Middle Initial: Preferred Name: DOB: Sex: Male Female Address: City, State, Zip: Home#: Cell#: Soc. Sec. #: Referred By: Previous Dentist: Responsible Party
Patient Registration First Name: Last Name: Middle Initial: Preferred Name: DOB: Sex: Male Female Address: City, State, Zip: Home#: Cell#: Soc. Sec. #: Referred By: Previous Dentist: Responsible Party
Welcome to South 40 Dental! Tell Us About Yourself
 Welcome to South 40 Dental! Tell Us About Yourself Name: Last First MI Title Preferred Name: Male Female Parent/Guardian Name if Under 18 Years Old: Address: City Prov. Postal Code Date of Birth (day)
Welcome to South 40 Dental! Tell Us About Yourself Name: Last First MI Title Preferred Name: Male Female Parent/Guardian Name if Under 18 Years Old: Address: City Prov. Postal Code Date of Birth (day)
Colorado Summit. Updates for Providers in the Colorado Medicaid Dental Program. This issue of the Colorado Summit will cover the following:
 Colorado Summit Updates for Providers in the Colorado Medicaid Dental Program Vol. 3 February 2015 Dear Dental Provider, DentaQuest is pleased to be working with the Department on the important job of
Colorado Summit Updates for Providers in the Colorado Medicaid Dental Program Vol. 3 February 2015 Dear Dental Provider, DentaQuest is pleased to be working with the Department on the important job of
Dear Patients, We have good news to share with you!
 Dear Patients, We have good news to share with you! It gives us great pleasure to introduce the Grand Marais Family Dentistry Benefits Plan. This in-house dental savings plan offers affordable care for
Dear Patients, We have good news to share with you! It gives us great pleasure to introduce the Grand Marais Family Dentistry Benefits Plan. This in-house dental savings plan offers affordable care for
2017 FAQs. Dental Plan. Frequently Asked Questions from employees
 2017 FAQs Dental Plan Frequently Asked Questions from employees September 2016 Dental plan Questions we ve heard our employees ask Here are some commonly asked questions about the Dental plan that our
2017 FAQs Dental Plan Frequently Asked Questions from employees September 2016 Dental plan Questions we ve heard our employees ask Here are some commonly asked questions about the Dental plan that our
Kids Dental Care Adult Patient Registration
 Kids Dental Care Adult Patient Registration To be updated every two years Patient's Name: DOB: SS# Sex: Male / Female Address: Apt/Unit/Floor: City: State: Zip Code: Home Phone #: ( ) - Cell Phone #: (
Kids Dental Care Adult Patient Registration To be updated every two years Patient's Name: DOB: SS# Sex: Male / Female Address: Apt/Unit/Floor: City: State: Zip Code: Home Phone #: ( ) - Cell Phone #: (
International Emergency and Expatriate Dental Program Claim Form and Instructions for Members
 International Emergency and Expatriate Dental Program Claim Form and Instructions for Members How to Complete the Claim Form The dental claim form is designed to capture the information that is essential
International Emergency and Expatriate Dental Program Claim Form and Instructions for Members How to Complete the Claim Form The dental claim form is designed to capture the information that is essential
POLICY TRANSMITTAL NO April 5, 2011 OKLAHOMA HEALTH CARE AUTHORITY
 POLICY TRANSMITTAL NO. 11-10 April 5, 2011 HEALTH POLICY OKLAHOMA HEALTH CARE AUTHORITY TO: SUBJECT: STAFF LISTED MANUAL MATERIAL CHAPTER 30. MEDICAL PROVIDERS-FEE FOR SERVICE OAC 317:30-5-700 and 30-5-700.1.
POLICY TRANSMITTAL NO. 11-10 April 5, 2011 HEALTH POLICY OKLAHOMA HEALTH CARE AUTHORITY TO: SUBJECT: STAFF LISTED MANUAL MATERIAL CHAPTER 30. MEDICAL PROVIDERS-FEE FOR SERVICE OAC 317:30-5-700 and 30-5-700.1.
APPLICATION FOR CLASS 3B DENTAL ANESTHESIA PERMIT WEST VIRGINIA BOARD OF DENTISTRY 1319 Robert C. Byrd Drive PO Box 1447 Crab Orchard, WV 25827
 BOARD OFFICE USE ONLY FEE PERMIT # EVALUATION DATE APPLICATION FOR CLASS 3B DENTAL ANESTHESIA PERMIT WEST VIRGINIA BOARD OF DENTISTRY 1319 Robert C. Byrd Drive PO Box 1447 Crab Orchard, WV 25827 I hereby
BOARD OFFICE USE ONLY FEE PERMIT # EVALUATION DATE APPLICATION FOR CLASS 3B DENTAL ANESTHESIA PERMIT WEST VIRGINIA BOARD OF DENTISTRY 1319 Robert C. Byrd Drive PO Box 1447 Crab Orchard, WV 25827 I hereby
Joint ADA and Health Level 7 Collaboration On Electronic Dental Attachments
 Joint ADA and Health Level 7 Collaboration On Electronic Dental Attachments Jean Narcisi, Director, Department of Dental Informatics Patrick Cannady, Manager, Department of Dental Informatics ADA Practice
Joint ADA and Health Level 7 Collaboration On Electronic Dental Attachments Jean Narcisi, Director, Department of Dental Informatics Patrick Cannady, Manager, Department of Dental Informatics ADA Practice
Reimbursement Guide. ATRIDOX Insurance Reimbursement Guide for the submission of insurance claims
 Reimbursement Guide Insurance Reimbursement Guide f the submission of insurance claims General reimbursement & submission infmation Reimbursement infmation Submission of insurance claims Pre-determination
Reimbursement Guide Insurance Reimbursement Guide f the submission of insurance claims General reimbursement & submission infmation Reimbursement infmation Submission of insurance claims Pre-determination
General Dental Treatment Consent Form
 General Dental Treatment Consent Form I authorize dental treatment including necessary or advisable examination, radiographs (x-rays), diagnostic aids or local anesthesia. In general terms, dental treatment
General Dental Treatment Consent Form I authorize dental treatment including necessary or advisable examination, radiographs (x-rays), diagnostic aids or local anesthesia. In general terms, dental treatment
Natural Health Center
 Natural Health Center 420 Yucca Lane - Turpin, OK 73950 Tel. No. (580) 778-3310 / Cell No. (620) 391-5520 / Fax No. (580) 778-3340 Today s Date / / Application for Treatment Name: Birthdate: SS# Address:
Natural Health Center 420 Yucca Lane - Turpin, OK 73950 Tel. No. (580) 778-3310 / Cell No. (620) 391-5520 / Fax No. (580) 778-3340 Today s Date / / Application for Treatment Name: Birthdate: SS# Address:
Healthcare Eligibility Benefit Inquiry and Response. 270/271 Companion Guide
 Healthcare Eligibility Benefit Inquiry and Response 270/271 Companion Guide Table of Contents Purpose...1 Preparation and Testing Requirements...1 Contact Information...1 System Availability...1 Batch
Healthcare Eligibility Benefit Inquiry and Response 270/271 Companion Guide Table of Contents Purpose...1 Preparation and Testing Requirements...1 Contact Information...1 System Availability...1 Batch
International Emergency Dental Program Claim Form and Instructions for Members
 International Emergency Dental Program Claim Form and Instructions for Members How to Complete the Claim Form The dental claim form is designed to capture the information that is essential for an accurate
International Emergency Dental Program Claim Form and Instructions for Members How to Complete the Claim Form The dental claim form is designed to capture the information that is essential for an accurate
Step by Step: How to maximize your benefits
 Step by Step: How to maximize your benefits Learn how to access your ID card, search for a dentist near you, download the Delta Dental mobile app and more! Click on a topic below to learn more: Subscriber
Step by Step: How to maximize your benefits Learn how to access your ID card, search for a dentist near you, download the Delta Dental mobile app and more! Click on a topic below to learn more: Subscriber
(City, State, Zip Code)
") This Partner Agency Agreement, dated this day of, 2015, is between COMMUNITY FOOD SHARE, INC. (CFS), whose address is 650 South Taylor Avenue, Louisville, CO 80027, and (Partner Agency) whose address is
This Partner Agency Agreement, dated this day of, 2015, is between COMMUNITY FOOD SHARE, INC. (CFS), whose address is 650 South Taylor Avenue, Louisville, CO 80027, and (Partner Agency) whose address is
Choosing your plan. City of Sacramento. We ll do whatever it takes and then some. Your Two Delta Dental Plan Options
 City of Sacramento Choosing your plan Your Two Delta Dental Plan Options The choice is yours. When it comes to dental health, you want benefits that provide you with the best balance of value and coverage.
City of Sacramento Choosing your plan Your Two Delta Dental Plan Options The choice is yours. When it comes to dental health, you want benefits that provide you with the best balance of value and coverage.
DQA Measure Technical Specifications: Administrative Claims-Based Measures Preventive Services for Children at Elevated Caries Risk, Dental Services
 **Please read the DQA Measures User Guide prior to implementing this measure.** DQA Measure Technical Specifications: Administrative Claims-Based Measures Preventive Services for Children at Elevated Caries
**Please read the DQA Measures User Guide prior to implementing this measure.** DQA Measure Technical Specifications: Administrative Claims-Based Measures Preventive Services for Children at Elevated Caries
HIPAA FOR THE DENTAL PRACTICE
 HIPAA FOR THE DENTAL PRACTICE Catherine C. Cownie Adam J. Freed E-mail: cownie@brownwinick.com E-mail: freed@brownwnick.com Telephone: 515-242-2490 Telephone: 515-242-2402 BrownWinick Law Firm 666 Grand
HIPAA FOR THE DENTAL PRACTICE Catherine C. Cownie Adam J. Freed E-mail: cownie@brownwinick.com E-mail: freed@brownwnick.com Telephone: 515-242-2490 Telephone: 515-242-2402 BrownWinick Law Firm 666 Grand
RE-CREDENTIALING PROFILE
 RE-CREDENTIALING PROFILE ATTESTATION: All information on this profile is required for continued membership. Failure to provide required information will impact your membership status with Delta Dental
RE-CREDENTIALING PROFILE ATTESTATION: All information on this profile is required for continued membership. Failure to provide required information will impact your membership status with Delta Dental
The following chart provides an illustration of the dental coverage provided under the Plan. Summary of Dental Care Benefits
 DENTAL CARE You or your eligible dependents may incur reasonable and customary charges for services and supplies provided by or under the supervision of a licensed, certified or registered oral surgeon
DENTAL CARE You or your eligible dependents may incur reasonable and customary charges for services and supplies provided by or under the supervision of a licensed, certified or registered oral surgeon
Welcome. In case of emergency, contact: Is condition due to an accident? [ ] Yes [ ] No
![Welcome. In case of emergency, contact: Is condition due to an accident? [ ] Yes [ ] No](/thumbs/89/99616722.jpg "Welcome. In case of emergency, contact: Is condition due to an accident? [ ] Yes [ ] No") Patient Information Welcome Who is responsible for this account? SSN Relationship to Patient Patient Name Insurance Co. Name: Preferred First Name Group #: ID #: Sex [ ] M [ ] F Age: Birthdate SS# Birthdate
Patient Information Welcome Who is responsible for this account? SSN Relationship to Patient Patient Name Insurance Co. Name: Preferred First Name Group #: ID #: Sex [ ] M [ ] F Age: Birthdate SS# Birthdate
Dr. Charles E. Copeland, DC Highland Chiropractic
 Highland Chiropractic Name: Birth Date: / / Gender M / F Occupation: Address: Employer: City: State: Zip: How did you hear about us? Home Phone: ( ) - Preferred Phone to Contact Work Phone: ( ) - Home
Highland Chiropractic Name: Birth Date: / / Gender M / F Occupation: Address: Employer: City: State: Zip: How did you hear about us? Home Phone: ( ) - Preferred Phone to Contact Work Phone: ( ) - Home
COOPERATIVE AGREEMENT FOR DENTAL SERVICES
 COOPERATIVE AGREEMENT FOR DENTAL SERVICES (Community Dental Provider) This agreement dated by and between (Name of Head Start/Early Head Start Program) (Address of Head Start/Early Head Start Program)
COOPERATIVE AGREEMENT FOR DENTAL SERVICES (Community Dental Provider) This agreement dated by and between (Name of Head Start/Early Head Start Program) (Address of Head Start/Early Head Start Program)
MOBILE PREMIER PEDIATRIC DENTISTRY Maureen T. Baldy, D.M.D.
 MOBILE PREMIER PEDIATRIC DENTISTRY Maureen T. Baldy, D.M.D. 3920 Airport Blvd, Mobile, AL 36608 251-342-3323 www.mobilekidsdentist.com Welcome! We would like to welcome you to our practice. Our goal is
MOBILE PREMIER PEDIATRIC DENTISTRY Maureen T. Baldy, D.M.D. 3920 Airport Blvd, Mobile, AL 36608 251-342-3323 www.mobilekidsdentist.com Welcome! We would like to welcome you to our practice. Our goal is
Who may we thank for referring you? Office Only LIST YOUR HEALTH CONCERNS BELOW. If you had the condition before, when? When did this episode start?
 Name Date / / Age Male / Female Address City State Zip Phone: Home Cell Cell Phone Provider Date of Birth / / Email Address Occupation Employer s Name Single / Married / Divorced / Widowed Spouse s Name
Name Date / / Age Male / Female Address City State Zip Phone: Home Cell Cell Phone Provider Date of Birth / / Email Address Occupation Employer s Name Single / Married / Divorced / Widowed Spouse s Name
NCAA, NAIA, or NJCAA Intercollegiate Football: Traumatic Brain Injury Supplemental Warranty Application for New and Renewal Policies
 NCAA, NAIA, or NJCAA Intercollegiate Football: Traumatic Brain Injury Supplemental Warranty Application for New and Renewal Policies INSTRUCTIONS Instructions for the Educational Organization (Applicant)
NCAA, NAIA, or NJCAA Intercollegiate Football: Traumatic Brain Injury Supplemental Warranty Application for New and Renewal Policies INSTRUCTIONS Instructions for the Educational Organization (Applicant)
Address (if different from above):
:") Lee H. Baker, DDS 1243 Augusta West Pkwy Augusta, GA 30909 (706) 855-8989-Phone (706) 855-0321-Fax www.drleebaker.com Welcome to our practice! In order to know you and your child better, please complete
Lee H. Baker, DDS 1243 Augusta West Pkwy Augusta, GA 30909 (706) 855-8989-Phone (706) 855-0321-Fax www.drleebaker.com Welcome to our practice! In order to know you and your child better, please complete
SUMMARY OF BENEFITS PLAN INFORMATION
 SUMMARY OF BENEFITS PLAN INFORMATION Cigna Dental Preventive Plan With Cigna there is more to smile about. You get flexible benefits and premium levels to meet your needs and budget, plus: Access to over
SUMMARY OF BENEFITS PLAN INFORMATION Cigna Dental Preventive Plan With Cigna there is more to smile about. You get flexible benefits and premium levels to meet your needs and budget, plus: Access to over
APPLICATION TO EMPLOY A
 STATE OF CALIFORNIA - STATE AND CONSUMER SERVICES AGENCY ARNOLD SCHWARZENEGGER, Governor BOARD OF PSYCHOLOGY 2005 Evergreen Street, SUITE 1400 SACRAMENTO, CA 95815-3831 (916) 263-2699 ext. 3303 www.psychboard.ca.gov
STATE OF CALIFORNIA - STATE AND CONSUMER SERVICES AGENCY ARNOLD SCHWARZENEGGER, Governor BOARD OF PSYCHOLOGY 2005 Evergreen Street, SUITE 1400 SACRAMENTO, CA 95815-3831 (916) 263-2699 ext. 3303 www.psychboard.ca.gov