Remineralization effectiveness of MI Paste Plus - a clinical pilot study
|
|
|
- Baldwin Marsh
- 5 years ago
- Views:
Transcription

 thesis, University of Iowa, 2011. https://ir.uiowa.edu/etd/939. Follow this and additional works at: https://ir.uiowa.edu/etd Part of the Orthodontics and Orthodontology Commons")
1 University of Iowa Iowa Research Online Theses and Dissertations Spring 2011 Remineralization effectiveness of MI Paste Plus - a clinical pilot study Sarah Elizabeth Clark University of Iowa Copyright 2011 Sarah Clark This thesis is available at Iowa Research Online: Recommended Citation Clark, Sarah Elizabeth. "Remineralization effectiveness of MI Paste Plus - a clinical pilot study." MS (Master of Science) thesis, University of Iowa, Follow this and additional works at: Part of the Orthodontics and Orthodontology Commons
2 REMINERALIZATION EFFECTIVENESS OF MI PASTE PLUS TM A CLINICAL PILOT STUDY by Sarah Elizabeth Clark A thesis submitted in partial fulfillment of the requirements for the Master of Science degree in Orthodontics in the Graduate College of The University of Iowa May 2011 Thesis Supervisor: Professor Robert. N. Staley
3 Graduate College The University of Iowa Iowa City, Iowa CERTIFICATE OF APPROVAL MASTER'S THESIS This is to certify that the Master's thesis of Sarah Elizabeth Clark has been approved by the Examining Committee for the thesis requirement for the Master of Science degree in Orthodontics at the May 2011 graduation. Thesis Committee: Robert. N. Staley, Thesis Supervisor Clayton Parks James Wefel Fang Qian
4 To my loving husband, Tanner To my supportive parents, Dan and Karen To my inspirational sister and brother, Kristin and John ii
5 ACKNOWLEDGMENTS I would like to thank Drs. Robert Staley, Clayton Parks, James Wefel, and Fang Qian for serving on my thesis committee and for all the input and support during this project. I would also like to thank Jeff Harless for his patience, support, and insight into using the quantitative light-induced fluorescence unit. I would also like to thank Dr. Tom Southard and the rest of the faculty at the University of Iowa, Department of Orthodontics for giving me the opportunity to further my education and pursue a career in orthodontics. Lastly, I would like to thank Tanner for being an outstanding husband and friend, I know you will make a wonderful father. iii
6 TABLE OF CONTENTS LIST OF TABLES...v LIST OF FIGURES... viii INTRODUCTION...1 Purpose of this Study...3 LITERATURE REVIEW...4 Development of a White Spot Lesion...4 White Spot Lesions in Orthodontic Patients...6 Methods to Decrease Demineralization during Orthodontic Treatment...7 Mechanism of Action of Fluoride...9 Fluoride Dentrifice...10 Mechanism of Action of Casein Phosphopeptides...11 Casein Phosphopeptide Amorphous Calcium Phosphate (CPP-ACP)...11 Quantitative Light-induced Fluorescence (QLF)...15 MATERIALS AND METHODS...18 Sample...18 Patient Inclusion Criteria...18 Clinical Procedure...18 Measurement of Data...21 Statistical Analysis...23 Reliability of Intra- and Inter-Examiner Measurement of Lesion Area...24 RESULTS...31 DISCUSSION...60 Experimental Design...60 Limitations of the Study...61 Clinical Application...62 Future Projects...63 SUMMARY AND CONCLUSIONS...64 REFERENCES...65 iv
7 LIST OF TABLES Table 1. Descriptive statistics of measurement differences for intra- and inter-examiner for tooth # Descriptive statistics of measurement differences for intra- and inter-examiner for tooth # Descriptive statistics of measurement differences for intra- and inter-examiner for tooth # Descriptive statistics of measurement differences for intra- and inter-examiner for tooth # Descriptive statistics of measurement differences for intra- and inter-examiner for tooth # Descriptive statistics of measurement differences for intra- and inter-examiner for tooth # Descriptive statistics of measurement differences for intra- and inter-examiner for antimere teeth #6 and # Descriptive statistics of measurement differences for intra- and inter-examiner for antimere teeth #7 and # Descriptive statistics of measurement differences for intra- and inter-examiner for antimere teeth #8 and # Descriptive statistics of measurement differences for intra- and inter-examiner for all teeth Descriptive statistics of lesion area for tooth #6, control group Descriptive statistics of lesion area for tooth #7, control group Descriptive statistics of lesion area for tooth #8, control group Descriptive statistics of lesion area for tooth #9, control group Descriptive statistics of lesion area for tooth #10, control group Descriptive statistics of lesion area for tooth #11, control group Descriptive statistics of lesion area for tooth #6, treatment group Descriptive statistics of lesion area for tooth #7, treatment group Descriptive statistics of lesion area for tooth #8, treatment group...35 v
8 20. Descriptive statistics of lesion area for tooth #9, treatment group Descriptive statistics of lesion area for tooth #10, treatment group Descriptive statistics of lesion area for tooth #11, treatment group Descriptive statistics of lesion area for antimere teeth #6 and #11, control group Descriptive statistics of lesion area for antimere teeth #6 and #11, treatment group Descriptive statistics of lesion area for antimere teeth #7 and #10, control group Descriptive statistics of lesion area for antimere teeth #7 and #10, treatment group Descriptive statistics of lesion area for antimere teeth #8 and #9, control group Descriptive statistics of lesion area for antimere teeth #8 and #9, treatment group Descriptive statistics of lesion area for all teeth, control group Descriptive statistics of lesion area for all teeth, treatment group Descriptive statistics of F values for tooth #6, control group Descriptive statistics of F values for tooth #7, control group Descriptive statistics of F values for tooth #8, control group Descriptive statistics of F values for tooth #9, control group Descriptive statistics of F values for tooth #10, control group Descriptive statistics of F values for tooth #11, control group Descriptive statistics of F values for tooth #6, treatment group Descriptive statistics of F values for tooth #7, treatment group Descriptive statistics of F values for tooth #8, treatment group Descriptive statistics of F values for tooth #9, treatment group Descriptive statistics of F values for tooth #10, treatment group Descriptive statistics of F values for tooth #11, treatment group Descriptive statistics of F values for antimere teeth #6 and #11, control group...45 vi
9 44. Descriptive statistics of F values for antimere teeth #6 and #11, treatment group Descriptive statistics of F values for antimere teeth #7 and #10, control group Descriptive statistics of F values for antimere teeth #7 and #10, treatment group Descriptive statistics of F values for antimere teeth #8 and #9, control group Descriptive statistics of F values for antimere teeth #8 and #9, treatment group Descriptive statistics of F values for all teeth, control group Descriptive statistics of F values for all teeth, treatment group...47 vii
10 LIST OF FIGURES Figure 1. Example of white spot lesions (WSL) developed during orthodontic treatment Diagram illustrating the process of demineralization and remineralization Horizontal and vertical measurements used to calculate the area of the WSL Photographic images illustrating remineralization in the treatment group, T0 and T4 respectively Photographic images illustrating remineralization in the control group, T0 and T4 respectively QLF images illustrating remineralization in treatment group (above) and control group (below), T0 and T4 respectively QLF images illustrating no significant remineralization in treatment group (above) and control group (below), T0 and T4 respectively Treatment group QLF (above) and photographic (below) images, T0 and T4 respectively Control group QLF (above) and photographic (below) images, T0 and T4 respectively...57 viii
11 1 INTRODUCTION Orthodontic treatment does more than just straighten teeth, it gives a person their unique smile and provides them with a positive sense of self-esteem. However, this smile can be compromised by the development of demineralization around the brackets, bands, and wires during orthodontic treatment. Upon removal of appliances at the termination of treatment, the patient may exhibit straight, yet blemished teeth. These white, chalky areas of demineralization are evidence of a loss of calcified tooth structure and are termed white spot lesions (Figure 1). And if left untreated, further decalcification may cause these early lesions to develop into cavitations that will require tooth reduction or permanent restoration (Mitchell, 1992). Even with advances in materials and techniques over the years, enamel demineralization associated with fixed orthodontic appliances has been observed and continues to be a problem (Farhadian et al., 2008). Historically, topical fluoride application has been the most common method to prevent development of white spot lesions around orthodontic appliances. A study reported by Stratemann and Shannon (1974) used a stannous fluoride gel. Only 2% of the subjects using the fluoride gel exhibited decalcification compared with the 58% of the control group. Another study using a neutral sodium fluoride rinse reported a 25% reduction in the incidence of white spot lesions (Geiger et al., 1992). More recently, Farhadian et al. (2008) observed a 40% decrease in the depth of demineralization among teeth treated with fluoride varnish compared to untreated controls. Though the results of these studies are promising, it takes a compliant patient to achieve such results and compliance with these patients is difficult to attain. Unfortunately, patients with poor oral hygiene that could benefit the most from fluoride preventive measures are also the same patients that are least likely to comply with the required topical fluoride protocol.
, which are products of milk protein casein, are thought to have the ability to increase the level of calcium phosphate in dental plaque which would depress the")
12 2 Recently, Recaldent, which is a complex of casein phosphopeptides and amorphous calcium phosphate (CPP-ACP), has been proclaimed to prevent and even reverse white spot lesions. Casein phosphopeptides (CPP), which are products of milk protein casein, are thought to have the ability to increase the level of calcium phosphate in dental plaque which would depress the demineralization process and raise the remineralization process (Reynolds, 1998). Recaldent is the active ingredient in MI Paste and MI Paste Plus, which are preventive treatment products marketed by GC America (Alsip, IL, USA) to provide a wide variety of benefits. The products are advertised to help prevent dry mouth, reduce tooth sensitivity, help fight acid imbalance, prevent demineralization, and enhance remineralization. The FDA has approved the use of MI Paste TM and MI Paste Plus TM as a prophy paste and for treating hypersensitivity. Figure 1. Example of white spot lesions (WSL) developed during orthodontic treatment.
13 3 Purpose of this Study The purpose of this study is to evaluate the effectiveness of MI Paste Plus in increasing remineralization and improving the esthetic appearance of white spot lesions in patients who have been treated with fixed orthodontic appliances. Each patient must meet specific criteria in order to be included in the study. Those patients who are eligible and choose to participate in the study will undergo four in-office MI Paste Plus TM treatments as well as three months of at-home MI Paste Plus TM applications. Initial, progress and final photographs will be made, the area of the white spot lesions will be measured and size comparisons will be conducted. Quantitative light-induced fluorescence (QLF) will also be used to quantitatively monitor the remineralization effects of MI Paste Plus TM after orthodontic treatment and three months post-treatment.
14 4 LITERATURE REVIEW Development of a White Spot Lesion Dental caries, one of the most prevalent chronic diseases in adults and children worldwide (Featherstone, 2000), affects nearly 90% of youth and 95% of adults within the United States (García-Godoy et al., 2008). Dental caries is a preventable, multifactorial disease that involves bacteria (dental plaque), susceptible teeth (the host), and carbohydrates (the diet) (Keyes et al., 1963). These factors play a role in the dynamic demineralization-remineralization process that occurs at the surface of each tooth in the oral environment. As teeth erupt into the oral cavity, they are immediately covered by an acquired enamel pellicle that consists of an acellular base layer of protective proteins. This pellicle, which is continually present and immediately reforms after disruption from tooth brushing or professional prophylactic cleaning, serves as the base on which dental plaque builds (García-Godoy et al., 2008). Bacteria bind to the enamel pellicle and as dental plaque matures, additional bacteria adhere. Over 600 different bacteria colonize dental plaque, with aerobic, facultative anaerobic and anaerobic organisms coexisting (Marsh, 2006). Acidogenic bacteria within dental plaque produce acid when fermentable carbohydrates are metabolized. Once this acid decreases the ph surrounding the teeth past a critical level (ph = 5.5) it has the potential to diffuse into enamel and dissolve calcium phosphate mineral (Featherstone, 2000). During this demineralization process, less-soluble phases of dicalcium phosphate dihydrate (CaHPO 4 2H 2 O) and fluoridated hydroxyapatite (Ca 5 ( PO4 ) 3 (OH) x F (1-x) ) precipitate out of the enamel surface and into the saliva. This process continues until equilibrium is reached between the enamel and the oral environment. Demineralization can continue as long as the oral ph remains acidic (Margolis et al., 1990).
15 5 Once the oral ph rises above the acidic level and normalizes, the remineralization process of the tooth surface can start. Calcium and phosphate are both minerals in saliva and, with the help of fluoride, diffuse into the enamel and remineralize crystalline structures in demineralized areas. Fluoridated hydroxyapatite and fluorapatite are the constituents of the structures that are rebuilt and are much more resistant to acid attack than the original structure (Selwitz et al., 2007). The processes of demineralization and remineralization occur several times throughout the day and if balanced, will not result in carious lesions. If however, the multi-factorial disease is not kept in balance and the oral environment becomes acidic, demineralization rather than remineralization occurs and the lesion will progress and eventually become a frank cavitation (Featherstone, 2000). A diagrammatic representation of the demineralization and remineralization cycle is shown in Figure 2. Figure 2. Diagram illustrating the process of demineralization and remineralization.
16 6 The primary clinical presentation of dental caries in enamel is a white spot lesion. It is an area of demineralized enamel that usually develops because of prolonged plaque accumulation (Guzman-Armstrong, 2010). The white spot lesion s opaque appearance is a result of the loss of subsurface enamel, which results in the loss of enamel translucency (Zero, 1999). Over time when plaque accumulates and aciduric bacteria colonize, active white spot lesions are produced. If left untreated, a cavitated carious lesion can develop. The patient s modifying factors can also impact the development of white spot lesions, this includes medical, dental, and medication history; diet; levels of calcium, phosphate, and bicarbonate in saliva; fluoride levels; and genetic susceptibility (Chalmers, 2006; Mount, 2005). A continuous process of enamel demineralization and remineralization occurs that can progress from initial demineralization, to noncavitated lesions, and finally to cavitated lesions (Fejerskov, 2003). White Spot Lesions in Orthodontic Patients It is agreed upon that demineralization and the development of white spot lesions is a problem during orthodontic treatment; however, published literature shows great variation in the prevalence. Zachrisson et al. (1971) reported that 89% of patients developed white spot lesions, while Gorelick et al. (1982) observed that 49.6% of patients had white spot formation on at least one tooth at debanding. However, Sudjalim et al. (2006) reported overall prevalence of white spot lesions ranging widely between 2 and 96%. The differences in reported prevalence may be attributed to variation in incidence geographically or to the difference in the definition of a white spot lesion. However prevalent, it is established that white spot lesions may persist for years resulting in a permanent, unaesthetic result with the potential of worsening to the point of requiring permanent restoration (Øgaard, 1989; Sudjalim et al., 2006). Fixed orthodontic appliances create areas for plaque accumulation and make tooth cleaning difficult. The irregular surfaces of brackets, bands, and wires limit the naturally
17 7 occurring self-cleansing mechanisms of the oral musculature and saliva (Guzman- Armstrong, 2010), leading to increased plaque retention and subsequent white spot lesion formation. Due to the difficulty of effective daily cleaning around fixed appliances, patients without fluoride supplementation (Ogaard et al., 1988), those with poor oral hygiene (Zachrisson et al,. 1971), and those patients with a high Streptococcus mutans count (Ogaard, 1989) are at higher risk for enamel demineralization and white spot lesion formation. The degree of white spot lesion development is not completely apparent until the fixed orthodontic appliances are removed. Upon removal of appliances, white, opaque demarcations on the labial surface of the teeth where the brackets and bands once were may be evident. These white, unesthetic demarcations of decalcification detract from the smile and final esthetic result of straight teeth and good occlusion. Because these white spot lesions most often occur on maxillary anterior teeth, they pose a significant esthetic problem (Gorelick et al., 1982). Methods to Decrease Demineralization During Orthodontic Treatment Depending on the patient s risk factors, a number of suitable agents and therapies can be used to help prevent white spot lesions in orthodontic patients: fluoride toothpastes, gels, varnishes, and mouth rinses; antimicrobials; xylitol gum; diet counseling; and casein derivatives (Guzman-Armstrong, 2010). The critical component in preventing demineralization is patient compliance along with good oral hygiene. Reinforcing oral hygiene habits throughout orthodontic treatment has been shown to be effective in reducing demineralization (Artun et al., 1986). Exhaustive tooth brushing, daily flossing, and routine prophylactic cleanings will minimize the amount of dental plaque, thereby decreasing the probability of developing areas of decalcification (Øgaard, 1989).
18 8 Decreasing the amount of Streptococcus mutans has also been shown to limit the caries process (van Houte, 1994). Chlorhexidine is an antimicrobial agent that is effective at reducing levels of Streptococcus mutans (Ribeiro, 2007). Therefore, a before bedtime protocol utilizing a chlorhexidine rinse, gel, or varnish may assist in preventing demineralization. A drawback of the chlorhexidine products is their tendency to stain the teeth. Xylitol gum has been shown to be effective as a caries preventive agent. Xylitol is a polyol (a type of carbohydrate) that is not a metabolizable substrate for Streptococcus mutans and can be used as a low-calorie sugar substitute. It is noncariogenic and appears to have antimicrobial properties that help to inhibit the attachment of Streptococcus mutans to the teeth, decreasing the bacterial count. Makinen et al (1995) showed that the systematic use of xylitol chewing gum can significantly reduce the risk of caries. The consumption of chewing gum has also increased production of stimulated saliva containing more calcium and phosphate ionic concentrations when compared to non-stimulated saliva. Increasing the levels of topical fluoride in the oral cavity is fundamental in minimizing the risk of decalcification. Fluoride can be introduced via dentifrice, mouth rinses, foams, gels, varnishes, bonding agents, cements, and even elastomers. Several of these delivery systems are intended for home use, relying on patient cooperation. Patient compliance with these products is essential for these products to have a significant preventive effect. For instance, Geiger et al. (1992) reported that only 42% of patients rinsed with sodium fluoride mouth rinse at least every other day, but patients who were more compliant had fewer white spot lesions. It is difficult to have a high percentage of patients willing and able to follow hygiene instruction for an extended period of time. Due to the unpredictability of patient cooperation, fluoride products that do not rely on patient compliance have gained popularity. Brackets and bands can be cemented with fluoride-releasing materials, sealants can be placed to cover the facial surface of
19 9 each tooth, and a fluoride varnish containing high amounts of fluoride can be applied at office visits at least twice per year (Schmit et al., 2002; Todd et al., 1999; Ashcraft et al., 1997; Vorhies et al., 1998). Mechanism of Action of Fluoride Fluoride has the ability to aid in the prevention of dental caries. Topical fluoride has three principal mechanisms of action: 1) inhibiting bacterial metabolism, 2) inhibiting demineralization, and 3) enhancing remineralization (Featherstone, 2000). To inhibit bacterial metabolism, acidulated fluoride ions in the form HF are able to cross the cell wall and membrane of cariogenic bacteria, such as Streptococcus mutans (Whitford et al., 1977; Van Loveren et al., 1990). Once inside the cell, HF dissociates, acidifying the cell and inhibiting enzyme activity with the fluoride ion F -. Enolase, an enzyme involved in carbohydrate metabolism, is affected by such inhibitory activity. This activity limits the cariogenic potential of the cell (Featherstone, 2000). Fluoride also has the ability to protect the enamel surface from demineralization during an acid attack. If topical fluoride is present in the plaque fluid when the ph drops below the critical level (ph = 5.5), it will travel with the acid into the subsurface layer, absorb to the crystal surface of carbonated hydroxyapatite (CAP) and protect it from being dissolved (Featherstone, 2000). Thus, low levels of fluoride surrounding the enamel during an acid attack are able to inhibit demineralization. The third mechanism of action of fluoride is enhancing the remineralization process. Following the acid attack and the ph rising above 5.5, available calcium and phosphate are able to be attracted into the crystal structure by the presence of absorbed fluoride. Calcium and phosphate ions enhance and are required for this remineralization process. These three minerals are able to create a new crystalline structure between hydroxyapatite (HAP) and fluorapatite (FAP), which is stronger and more acid-resistant
20 10 than the previous structure (Featherstone, 2000; Moreno et al., 1977; ten Cate et al., 1991). Fluoride Dentifrice Fluoridated dentifrice is the most common method of topical fluoride delivery worldwide and is recognized as a major factor in reducing the prevalence of caries in many developed countries (Zero, 2006). In a meta-analysis of seventy studies by Marinho et al. (2003) and in a systematic review of fifty-four published studies by Twetman et al. (2003), it was concluded that there was clear evidence that fluoridated toothpastes are effective in preventing dental caries. Fluoride concentrations in dentifrice range from low (below 600 ppm) to high (5000 ppm), with the majority between ppm. The low and high concentrations of fluoride are intended for patients under the age of six and those with high caries risk, respectively (Ammari, 2003). Twetman et al. (2003) reported a superior preventive effect with toothpastes containing 1,500 ppm fluoride compared with those containing 1,000 ppm fluoride. Sources of fluoride in dentifrice include stannous fluoride (SnF 2 ), monofluorophosphate (MFP), and sodium fluoride (NaF). Of these, the majority of dentifrice marketed in the United States is in the form of NaF or MFP (Zero, 2006). High-fluoridated dentifrice, such as PreviDent 5000 Plus (Colgate-Palmolive Co., New York City, NY, USA), have few studies demonstrating efficacy over traditional 1,100 ppm fluoride dentifrice. Baysan et al. (2001) compared the ability of two fluoridated dentifrices, one containing 5,000 ppm (PreviDent 5000 Plus ) and the other 1,100 ppm (Winterfresh Gel ), to reverse primary root caries lesions. They concluded that the 5,000 ppm fluoride dentifrice was significantly better at preventing the lesions than the 1,100 ppm fluoride dentifrice.
21 11 Mechanism of Action of Casein Phosphopeptides Dairy products such as milk, milk concentrates, powders, and cheeses have been demonstrated to have anticariogenic properties (Reynolds et al., 1981; Rosen et al., 1984; Harper et al., 1986, 1987; Krobicka et al., 1987; Silva et al., 1987). Using in vitro, animal, and in situ caries models, the components responsible for this significant attribute have been identified as casein, calcium, and phosphate (Schweigert et al., 1946, Shaw, 1950; Bavetta et al., 1957; Holloway et al., 1961, Reynolds et al., 1984, 1987, 1989; Reynolds, 1987). A soluble form of casein, or caseinate, was shown to have anticariogenic potential in rats; however, due to the high amount required for effective caries control this form of casein was not ideal for commercial use (Reynolds et al., 1984). Researchers later discovered that digesting caseinate with trypsin did not destroy the protein s ability to prevent subsurface enamel demineralization (Reynolds, 1989). The resultant tryptic peptides were shown to be incorporated within dental plaque along with elevated concentrations of calcium and phosphate (Reynolds, 1998). The major tryptic peptides associated with the anticariogenic nature of casein are casein phosphopeptides (CPP). Through multiple phosphoseryl residues, CPP has the unique ability to stabilize calcium phosphate in a CPP-amorphous calcium phosphate (ACP) complex (Azarpazhooh et al., 2008). Casein Phosphopeptide-Amorphous Calcium Phosphate (CPP-ACP) The CPP-ACP complex was patented by the University of Melbourne, Australia, and the Victorian Dairy Industry Authority, Abbotsford, Australia. Bonlac Foods Limited (an Australian company owned by 2,300 dairy farmers in Victoria and Tasmania) has retained exclusive manufacturing and marketing rights for CPP-ACP and is the owner of the trademark Recaldent (Azarpazhooh et al., 2008). CPP-ACP
22 12 complexes have been shown to exhibit anticariogenic activity in laboratory, animal, and human in situ caries models (Morgan et al., 2008; Oshiro et al., 2007; Ramlingam et al., 2005; Reynolds et al., 1987, 1991, 1995, 1997, 1998, 1999, 2003; Shen et al., 2001). The anticariogenic mechanism of CPP-ACP is the localization of amorphous calcium phosphate at the tooth surface, where it buffers free calcium and phosphate ion activity during an acid challenge, and maintaining a state of supersaturation of calcium and phosphate ions on the enamel surface (ElSayad, 2009). This process results in a decrease in demineralization during a cariogenic challenge and an increase in the subsequent remineralization of the enamel (Azarpazhooh et al., 2008; Reynolds, 1987, 1991, Pulido et al., 2008). One of the benefits of this peptide compound is that it has been shown to incorporate well into the salivary pellicle thereby reducing the adherence of cariogenic bacteria, specifically S. sobrinus and S. mutans (Schupbach, 1996). In addition to reducing the amount of acid-producing bacteria within dental plaque, the incorporation of CPP-ACP within dental plaque is able to provide a reservoir of additional bio-available calcium and phosphate ions. These ions help buffer acidic challenges to the enamel and aid in rebuilding enamel structure (Aimutis, 2004). It has been shown that enamel remineralized by CPP-ACP is relatively more acid-resistant than normal tooth enamel (Yengopal, 2009). The most commonly tested (and used) mode of CPP-ACP application in the human oral environment is via sugar-free sorbitol or xylitol-based chewing gum. Other vehicles include milk, mouth rinses, lozenges, and dental cream/ MI Paste /Tooth Mousse (Yengopal, 2009). Morgan et al. (2008) compared the progression and regression of interproximal caries in adolescent subjects chewing a sugar-free gum containing 54 mg CPP-ACP to subjects chewing identical gum without CPP-ACP. The investigators reported a significantly slowed progression and enhanced regression of the lesions relative to the control group over a 24 month period. Similarily, Cai et al. (2007) showed that gum containing 18.8 mg and 56.4 mg of the CPP-ACP nanocomplexes, chewed for 20 minutes
23 13 four times per day for 14 days, increased enamel subsurface remineralization by 102% and 152%, respectively, relative to the control sugar-free gum. In a randomized, controlled trial Reynolds et al. (2003) observed an increase in plaque calcium and inorganic phosphate levels of 118% and 57%, respectively, using a 2% CPP-ACP mouth rinse. The increase of calcium and phosphate ions within dental plaque was consistent with the proposed anticariogenic mechanism of CPP-ACP by maintaining the supersaturated state of remineralizing ions on the enamel surface. The investigators also reported that mouth rinses containing ACP without CPP did not exhibit increased calcium and inorganic phosphate levels. This is significant in that it demonstrates that CPP is essential in stabilizing and delivering ACP to the tooth surface (Reynolds et al., 2003). Currently, CPP-ACP (Recaldent ) is commercially available in the United States in the form of sugar-free gum, Trident White (Cadbury North America, Parsippany, NJ), MI Paste, and MI Paste Plus (containing 900 ppm fluoride) (GC America, Alsip, IL, USA). The FDA has approved MI Paste for use primarily as an abrasive prophylactic paste, secondarily as treatment for dentin hypersensitivity, and thirdly for dry mouth. However, its use as a caries preventive and remineralization agent is considered off-label. Outside the United States, MI Paste and MI Paste Plus is marketed as GC Tooth Mousse and Tooth Mousse Plus (GC Europe N.V., Leuven, Belgium) (Azarpazhooh et al., 2008). While several articles have been published on the evidence of CPP-ACP as an anti-caries agent in its pure form, quality studies involving commercially-available MI Paste and MI Paste Plus (or Tooth Mousse TM and Tooth Mousse Plus TM ) are limited. The majority of reviews are found in abstracts presented at International Association for Dental Research (IADR) conferences and funded by GC Corporation (Paterson, 2008; Sakaguchi, 2005, 2006; Sato, 2003). Although CPP-ACP is the main active ingredient in these products (5-10% w/v) it is uncertain whether incorporation into the form of a paste
24 14 alters its effective ability. An IADR abstract presented by Sato et al., (2003) confirmed the ability of Tooth Mousse to prevent the formation of caries in a bovine tooth model. Using Knoop Hardness measurements to evaluate treatment groups, those treated with Tooth Mousse displayed a significantly less change in hardness reduction compared to a placebo paste and to a fluoridated paste. In addition, Sakaguchi et al., (2005) reported the ability of MI Paste to prevent acid-inducted demineralization in bovine tooth enamel compared with a placebo paste, a 900 ppm fluoride paste, and water. Samples were imaged using quantitative light-induced fluorescence (QLF) as well as x-ray CT. Researchers concluded that there was a significant protective effect of MI Paste in preventing the demineralization of enamel. Sakaguchi et al., (2006) later described a synergistic effect of CPP-ACP and fluoride, as found in Tooth Mousse Plus (MI Paste Plus ), in remineralizing subsurface enamel lesions in bovine teeth. Tooth Mousse Plus was compared with Tooth Mousse, a placebo containing no CPP-ACP or fluoride, and a paste containing 950 ppm fluoride. The remineralization potential of Tooth Mousse Plus (Tooth Mousse with 900 ppm fluoride) was greater than the additive effect of the Tooth Mousse and the 950 ppm fluoridated paste groups. It is important to note that GC Corporation appears on each of the author reference lists. Studies not associated with GC Corporation prove to be a bit more contradictory. For instance, a study attempting to remineralize subsurface enamel lesions on extracted human teeth using MI Paste, MI Paste with Crest toothpaste, Crest toothpaste alone, and PreviDent 5000 Plus reported no significant difference between groups except for the PreviDent 5000 Plus treatment group (Eberle, 2006). In addition, a recent study examining the ability of MI Paste in preventing the progression of artificial carious lesions in human enamel revealed no significant effect of the product (Pulido et al., 2008). The authors reported that no significant difference between MI Paste, 1100 ppm NaF, or a combined application of both products was detected from the study. On the other hand, Guilio et al. (2009) reported greater demineralization
25 15 resistance in teeth coated with Tooth Mousse than a control group after enamel stripping. In a clinical trial conducted by Bailey et al. (2009), 92% of white spot lesions had regressed or stabilized after using a remineralizing cream (Tooth Mousse TM ) containing 10% w/v CPP-ACP. Over 12 weeks, there were significantly (31%) more post-orthodontic white spot lesions regressed with the remineralizing cream compared with an identical cream not containing CPP-ACP. CPP-ACP promotes remineralzation of enamel subsurface lesion, restoring the white opaque appearance of the lesions to translucency, even in the presence of fluoride (Reynolds et al., 2003, 2008). A dentifrice formulation containing 2% CPP-ACP nanocomplexes plus 1100 ppm F (CPP-ACPF) has been shown to be superior (2.6 times) to a dentifrice containing only 1100 ppm F in remineralization of enamel subsurface lesions in situ with mineral that was more resistant to acid challenge (Reynolds et al., 2008). The CPP-ACP nanocomplexes-plus-fluoride dentifrices resulted in significantly greater incorporation of fluoride into the subsurface enamel as fluorapatite. These results indicate that the CPP is an excellent delivery vehicle to co-localize bioavailable calcium, fluoride, and phosphate ions at the tooth surface to remineralize subsurface enamel lesions with fluorapitite (Reynolds, 2009). Quantitative Light-induced Fluorescence (QLF) The quantitative light-induced fluorescence (QLF) method for quantitative assessment of early enamel lesions provides a fluorescence image of a smooth surface carious lesion that quantifies the mineral loss and size of the lesion. Accordingly, the method is suitable for quantitative assessment of early enamel lesions in visually accessible surfaces. It may be used for quantitative monitoring of mineral changes (regression or progression) over just a few months (Angmar-Mansson, 2001). QLF is based on fluorescent light which is induced by visible or near-ultraviolet radiation. There is an uncertainty regarding the cause of the decreased fluorescence of
26 16 incipient lesions. The generally accepted explanation is that the light scattering in the lesion, which is much stronger than in sound enamel, causes the light path in the lesion to be much shorter than in sound enamel, thus the light absorption per volume is much smaller in the lesion and thus the fluorescence is less strong. A second explanation is that the light scattering in the lesion is a barrier for excitation light to reach the underlying fluorescing dentin, and a barrier for fluorescence light from dentin to reach the surface (Angmar-Mansson, 2001). QLF is non-destructive and thus a suitable method for quantitative assessment of one and the same lesion at different times. This involves making a series of images at different times. Most often, the first image in the series is made of the sound tooth which serves as the baseline for all later images. A comparison of images yields values of the fluorescence decrease as a function of position (x,y) on the tooth surface at the location of the lesion, expressed as a percentage of the fluorescence in the sound situation (Angmar- Mansson, 2001). The accuracy of any measurement technique is affected by the equipment used and the skill of the operator. Ideally, the equipment should be able to compensate for any deficiencies in the operator. With the QLF equipment, the operator adjusts the camera to view the region of interest on a monitor screen and the light guide is attached to the camera requiring no separate adjustment. The camera amplifier is automatically adjusted and an image can be grabbed and stored by pressing a foot pedal. There is on-screen guidance for the operator to perform image analysis. Reference points that are seen on subsequent images, such as a cusp tip or gingival margin, are used and assist for correction due to irradiation geometry changes. After these adjustments, the program is able to analyze both images and calculate the ^F (fluorescence loss) for each image (Angmar-Mansson). The ^F % is used to calculate the change between the images.
27 17 The repeatability and reproducibility of QLF have been tested in vivo. The image-capturing stages were tested by three operators, each captured images of 15 incipient smooth surface lesions in vivo. The analytical stage of the method was also tested. The same three operators analysed the images of 15 in vivo incipient smooth surface lesions. For the image-capturing stage, interexaminer reliability showed an interclass correlation coefficient, r, between 0.95 and For the analytical stage, intra-examiner reliability for all three analysts showed an intraclass correlation coefficient, r, between 0.93 and Interexaminer reliability showed an interclass correlation coefficient, r, between 0.95 and It was concluded that the in vivo repeatability and reproducibility of the QLF method is excellent (Angmar-Mansson). An in vivo application of the QLF method of measurement of mineral changes in natural enamel lesions on smooth surfaces was demonstrated in a 12-month study monitoring remineralization of carious lesions, which had developed around orthodontic brackets during fixed appliance therapy. Removal of the orthodontic brackets and bands had disclosed active carious lesions, and caries preventive measures were intensified. The carious lesions were monitored with the QLF method immediately after removal of the orthodontic brackets and once a month thereafter. During a 1-year follow-up period, the areas of the lesions decreased, and the lost enamel fluorescence was partly regained, indicating remineralization. It was concluded that QLF is appropriate for in vivo monitoring of mineral changes in incipient enamel lesions and is useful for the evaluation of preventive measures in caries-susceptible individuals, such as orthodontic patients (Mattousch, 2007).
28 18 MATERIALS AND METHODS The study protocol was reviewed and approved by the Institutional Review Board at the University of Iowa. Sample A total of twelve subject participants aged twelve to twenty years were selected in this pilot study. All participants were recruited from patients treated with fixed edgewise orthodontic appliances in the Department of Orthodontics at the University of Iowa, College of Dentistry. The sample was comprised of 6 control and 6 treatment subjects. All 12 subjects were Caucasian, 7 were female and 5 were male. Patient Inclusion Criteria The patients must have been age 12 years or older, been in good general health with no proven or suspected milk protein allergy and/or with a sensitivity or allergy to benzoate preservatives, had a treatment period with fixed appliances of at least 1 year at the debonding appointment, had at least 1 clinically visible white spot lesion on the facial surface of a maxillary anterior tooth, had not undergone any type of remineralization/demineralization regimen, and have not had more than 2 failed appointments during orthodontic treatment. The patient could not have been a consent debond, and must have had an informed consent signed by the participant and for those under 18 years, signed in addition by their parents or guardians. Clinical Procedure The purpose of the clinical study was to evaluate the effectiveness of CPP-ACPF, MI Paste Plus (GC America, Alsip, Illinois, USA) to remineralize and improve the esthetic appearance of white spot lesions (WSL) after orthodontic treatment.
29 19 Twelve patients were selected based on the inclusion criteria and were randomly assigned to the treatment and control groups (n=6 per group). The first six patients who met the study criteria were selected for the treatment group. The following six patients who again met the study criteria were selected to be the control subjects. One to two weeks after fixed orthodontic appliances were removed (T0), both the treatment and control subjects returned for photographs. These photographs consisted of five intra-oral photos of the six maxillary anterior teeth made at a higher magnification than standard photographs. A standard intra-oral photographic camera was utilized and the photos were taken in a light controlled environment with pre-set photographic protocol. The first photo was centered on the maxillary central incisors, the second and third on the right and left lateral incisors, and the remaining two on the right and left canines. The treatment and control subjects also had initial QLF images made at this appointment. Initial QLF images were made of the facial surface of all six maxillary anterior teeth. The images were examined visually for signs of demineralization, which appears as dark areas surrounded by bright green fluorescing tooth structure. Once the photographs and QLF images were made, the treatment subjects only started their first round of the in-office MI Paste Plus TM application. Appropriate isolation was achieved with cheek retractors. A 35% phosphoric acid etch was applied to only the white spot lesions for 1 minute. The etch was rinsed off thoroughly after 1 minute. A small amount of MI Paste Plus TM was applied directly onto the WSL with an application swab. The MI Paste Plus TM was left undisturbed for 5 minutes. After the 5 minutes had expired, the patient was instructed to use their tongue to spread the remaining paste throughout the mouth. The patient was requested to avoid expectoration for an additional 1-2 minutes. The patient was then advised not to eat or drink for 30 minutes following application. They were instructed to return in three weeks
30 20 for their second in-office application. At-home application instruction and oral hygiene guidance were given to the patient at the end of the appointment. Both the control group and treatment group were given a 6.4 oz tube of cavity protection toothpaste (Colgate or Crest depending on patient preference) to use during morning and evening brushing for the next three months. They were both given identical oral hygiene instruction. The subjects were advised to brush with a soft toothbrush both morning and night with the toothpaste provided. They were encouraged to floss once daily. They also received their invisible retainers along with full time wear instructions. The treatment group retainers were made with a thin reservoir area around the WSL for the MI Paste Plus TM to settle during the overnight application. The treatment group was given additional instruction for their at-home application of the MI Paste Plus TM (provided for patient). After brushing their teeth in the evening, each patient applied a pea-sized amount of the paste to the facial surface of the maxillary six teeth with a clean dry finger. The patient immediately inserted their invisible retainer which remained in place overnight and was not removed until the next morning. In the morning when the tray was removed, the patient was allowed to expectorate, rinse and complete their regular morning brush. The invisible retainer was rinsed, brushed and reinserted for full time daily wear. Both groups were instructed to return to the office in three weeks. Upon return (T1), a set of progress photographs were made of both groups and the treatment subjects received their in-office application of the MI Paste Plus TM. The clinical trial ran for a total of 12 weeks (3 months). T0 (initial appointment) and four retention visits were scheduled; 3 weeks (T1), 6 weeks (T2), 9 weeks (T3), and 12 weeks/ 3 months or final appointment (T4). At each visit, the treatment subjects were given an at-home diary card. The card detailed at-home MI Paste Plus TM application instruction and oral hygiene guidance. There was a column in the table where the patient was able to write in how many hours
31 21 the retainer was worn overnight. A separate section was available for comments. On the final 3 month in-office visit (T4), the treatment group did not have an MI Paste Plus TM application, but both groups had their final photographs and QLF images made. T4 photographs were made in the same manner as T0 photographs. T4 QLF images were captured using the software s video-repositioning technique. Measurement of Data The remineralization effectiveness of MI Paste Plus TM was quantitively measured in two ways, photographs (Area in mm 2 ) and quantitative light-induced fluorescence (fluorescence loss in per cent). Five standard photographs were made at each three week interval, but only the initial and final photographs and QLF images were used for calculation. Each photograph was made with the same Nikon D1X/105mm/SB29 camera. The focal distance and magnification ratio were standardized at 1:2 and the aperture maintained at an f equal to 40. The first photo was centered on the two central incisors, the second and third on the left and right lateral incisors, and the fourth and fifth on the left and right canines. Each photograph was downloaded into Dolphin Imaging 11 orthodontic imaging software. From the models made at the debond appointment, actual mesial/distal measurements were made for each of the six maxillary anterior teeth with Mitutoyo Absolute Digimatic calipers. These measurements were used to calibrate the photographic image in order to be able to measure the white spot lesions accurately. Two measurements were made, one horizontal (mesial/distal) and one vertical (incisal/gingival). The maximum lesion dimensions in both directions were measured in millimeters. The area of the lesion was calculated and compared. Figure 3 illustrates the horizontal and vertical measurements which were made for each individual white spot lesion on the calibrated photo in order to calculate the area.
 on a personal computer using the image capturing")
32 22 Figure 3. Horizontal and vertical measurements used to calculate the area of the WSL. QLF images were captured at the initial appointment and at the final three month appointment using an intraoral fluorescence camera (Inspektor TM Pro) on a personal computer using the image capturing software (QLF Patient version ). The mineral change and size of the lesion was quantified. The fluorescence change between initial and final appointment was compared. To ensure that the images of the tooth surface are always captured with the same camera position and from the same angle, the software uses video-repositioning techniques. The video-repositioning technique displays the baseline and live image simultaneously and computes their correlation based on similar geometry of the fluorescence intensities. Images are stored in a list when the correlation is higher than 0.90 and the system automatically stops grabbing when the correlation reaches In this way, the images from the T0 and T4 should show the tooth surface from the same angle and at the same magnification. The system s analysis software determined the lesion extent. A patch was drawn surrounding the lesion site with its borders on sound enamel. Inside the patch, the fluorescent levels of sound tissue were reconstructed using the fluorescence radiance of the surrounding sound enamel.
33 23 The T0 stored patch was overlayed around the T4 lesion. The percentage difference between the reconstructed (T4) and original fluorescence levels was calculated. To ensure that the same area of a tooth surface was analyzed at each time point, the analysis patch and surface contour were copied and then matched for size, orientation, and location to this tooth surface in the final image. Statistical Analysis The two-sample t-test and nonparametric Wilcoxon rank-sum test were used to detect the differences in lesion area and in F values between control and treatment groups at baseline and at 3-month follow-up, as appropriate. Within each group, the paired samples t-test and nonparametric Wilcoxon signed rank test were used to assess the differences in change of lesion area and change in F values from baseline to three-month follow-up under different situations. The paired sample t-test was also used to assess the mean differences between pairs of measurements for intra- and inter- examiner. Additionally, intraclass correlation coefficients were computed as a measure of agreement between two measurements which were taken either by a single evaluator or two evaluators on the same tooth for each subject. The following is an approximate guide for interpreting an agreement between two measurements that corresponds to an intraclass and interclass correlation coefficient: 1) 1.0 = perfect agreement 2) 0.8 = strong agreement 3) 0.5 = moderate agreement 4) 0.2 = weak agreement 5) 0.0 = no agreement
34 24 All tests employed a 0.05 level of statistical significance. SAS for Windows (v9.2, SAS Institute Inc, Cary, NC, USA) was used for the data analysis. Reliability of Intra- and Inter-Examiner Measurements of Lesion Areas Each patient s teeth were evaluated by two examiners. To eliminate the possible bias, examiner A took two measurements on each tooth in two sessions with an interval of 7 days, and examiner B only took one measurement. Therefore, 3 recordings were obtained on each tooth for each subject. The intra- and inter-examiner measurement reliability was assessed for each tooth, for antimere teeth, and for all teeth. The descriptive statistics of mean measurement differences for intra- and inter-examiner are summarized in Tables Based on the paired samples t-test, intra-examiner duplicate measurements for examiner A showed no significant differences, whereas inter-examiner differences (i.e. differences between measurements made by examiner A and examiner B) were also not statistically significant. This is true for teeth numbers 6, 7, 8, 9, and 10; antimere teeth #6 and #11, #7 and #10, #8 and #9; and for all teeth. For tooth #11, the data showed significant difference (between 1 st measurements of examiner A and measurements of examiner B (p=0.0312) (Table 6). Additionally, intra- and inter-class correlation coefficients were computed to assess intra- and inter-observer agreement in measurements of lesion areas. All correlation coefficients ranged from 0.80 to These indicated a strong agreement between two measurements with a single evaluator and with two evaluators, except for one case, in which the corresponding values between measurements examined by A and B (inter-examiner) were r = 0.62 and r = 0.60 for 1 st and 2 nd measurements of examiner A vs. examiner B, respectively. The correlation coefficients of 0.62 and 0.60 indicated a moderate agreement between two measurements.
35 25 Table 1: Descriptive statistics of measurement differences for intra- and inter-examiner for tooth #6. Variable N Mean Std Dev Min Max Median P-value Lesion Lesion Lesion Table 2: Descriptive statistics of measurement differences for intra- and inter-examiner for tooth #7. Variable N Mean Std Dev Min Max Median P-value Lesion Lesion Lesion
36 26 Table 3: Descriptive statistics of measurement differences for intra- and inter-examiner for tooth #8. Variable N Mean Std Dev Min Max Median P-value Lesion Lesion Lesion Table 4: Descriptive statistics of measurement differences for intra- and inter-examiner for tooth #9. Variable N Mean Std Dev Min Max Median P-value Lesion Lesion Lesion
37 27 Table 5: Descriptive statistics of measurement differences for intra- and inter-examiner for tooth #10. Variable N Mean Std Dev Min Max Median P-value Lesion Lesion Lesion Table 6: Descriptive statistics of measurement differences for intra- and inter-examiner for tooth #11. Variable N Mean Std Dev Min Max Median P-value Lesion Lesion ** Lesion ** Significantly different (a paired-sample t-test).
38 28 Table 7: Descriptive statistics of measurement differences for intra- and inter-examiner for antimere teeth #6 and #11. Variable N Mean Std Dev Min Max Median P-value Lesion Lesion Lesion Table 8: Descriptive statistics of measurement differences for intra- and inter-examiner for antimere teeth #7 and #10. Variable N Mean Std Dev Min Max Median P-value Lesion Lesion Lesion
39 29 Table 9: Descriptive statistics of measurement differences for intra- and inter-examiner for antimere teeth #8 and #9. Variable N Mean Std Dev Min Max Median P-value Lesion Lesion Lesion Table 10: Descriptive statistics of measurement differences for intra- and inter-examiner for all teeth. Variable N Mean Std Dev Min Max Median P-value Lesion Lesion Lesion
40 30 Note: Lesion 1 = first measurements of Examiner A Lesion 2 = second measurements of Examiner A Lesion 3 = measurements of Examiner B Lesion 12 = first measurements of Examiner A minus second measurements of Examiner A Lesion 13 = first measurements of Examiner A minus measurements of Examiner B Lesion 23 = second measurements of Examiner A minus measurements of Examiner B
41 31 RESULTS The average lesion areas of two measurements of examiner A on the same tooth for the same patient were used for the statistical analysis in this study. Tables report descriptive statistics of lesion area by each tooth for each time period. No significant differences between control and treatment groups were found at baseline for teeth numbers 6, 7, 8, 9, 10, and 11; all antimere teeth; and for all teeth (p>0.05 in each instance). Similarly, no significant difference in the lesion area were found between control and treatment groups at 3-month follow-up for teeth numbers 6, 7, 8, 10, and 11; all antimere teeth; and for all teeth (p>0.05 in each instance). Due to insufficient data, a statistical test was unable to be conducted for tooth #9. To compare the change in lesion area from baseline to 3-month follow-up between control and treatment group, a new variable called Lesion_area_change was created, and this new variable is defined as lesion area at baseline minus lesion area at 3- month follow-up. Based on the two-sample t-test, there were no significant differences between control and treatment groups for the mean lesion area change from baseline to follow-up for teeth numbers 6, 7, 8, 10, and 11; all antimere teeth; and for all teeth (p>0.05 in each instance). Due to insufficient data, a statistical test was unable to be conducted for tooth #9. Within the control group, the data showed there were no significant differences in the lesion area measured between baseline and 3-month follow-up for teeth numbers 6, 7, 8, 10, and 11; antimere teeth #7 and #10, #8 and #9; and for all teeth (p>0.05 in each instance). Due to insufficient data, a statistical test was unable to be conducted for tooth #9. The data showed there was a significant difference in the lesion area measured between baseline and 3-month follow-up for antimere teeth #6 and #11 (p=0.0235) in the
42 32 control group. It revealed that the mean lesion measured at baseline was significantly greater than that at follow up (Table 23). Within the treatment group, the data showed that there were no significant differences in the lesion area measured between baseline and 3-month follow-up for teeth numbers 7, 8, 9, 10, 11 and antimere teeth #7 and #10. The data also showed there was a significant difference in the lesion area measured between baseline and 3-month follow up for tooth #6 (p=0.0434). It revealed that the mean lesion measured for tooth #6 at baseline was significantly greater than that at follow up (Table 17). The data also showed there was a significant difference in the lesion area measured between baseline and 3- month follow-up for antimere teeth #6 and #11 (p=0.0181) in treatment group. It revealed that the mean lesion measured at baseline was significantly greater than that at follow up (Table 24). Based on the Wilcoxon signed-rank test, the data showed there was a significant difference in the lesion area measured between baseline and 3-month followup for antimere teeth #8 and #9 (p=0.0331) in treatment group. It revealed that the mean lesion measured at baseline was significantly greater than that at follow up (Table 28). Additional analysis was conducted for combining all teeth. The results showed that there was a significant difference in the lesion areas measured between baseline and follow-up for all teeth (p=0.0219). It revealed that the mean lesion measured at baseline was significantly greater than that at follow-up for treatment group (Table 30).
43 33 Table 11: Descriptive statistics of lesion area for tooth #6, control group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months Table 12: Descriptive statistics of lesion area for tooth #7, control group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months Table 13: Descriptive statistics of lesion area for tooth #8, control group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months
44 34 Table 14: Descriptive statistics of lesion area for tooth #9, control group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months Table 15: Descriptive statistics of lesion area for tooth #10, control group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months Table 16: Descriptive statistics of lesion area for tooth #11, control group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months
45 35 Table 17: Descriptive statistics of lesion area for tooth #6, treatment group. Variable N Mean** Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months ** Significantly different (p=0.0434, a paired-sample t-test). Table 18: Descriptive statistics of lesion area for tooth #7, treatment group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months Table 19: Descriptive statistics of lesion area for tooth #8, treatment group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months
46 36 Table 20: Descriptive statistics of lesion area for tooth #9, treatment group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months Table 21: Descriptive statistics of lesion area for tooth #10, treatment group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months Table 22: Descriptive statistics of lesion area for tooth #11, treatment group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months
47 37 Table 23: Descriptive statistics of lesion area for antimere teeth #6 and #11, control group. Variable N Mean** Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months ** Significantly different (p=0.0235, a paired-sample t-test). *** Comparison was based on the available measurements on both baseline and followup. In this case, the mean difference between baseline and 3-month follow-up is 0.93 (std = 1.09). Table 24: Descriptive statistics of lesion area for antimere teeth #6 and #11, treatment group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months ** Significantly different (p=0.0181, a paired-sample t-test). Table 25: Descriptive statistics of lesion area for antimere teeth #7 and #10, control group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months
48 38 Table 26: Descriptive statistics of lesion area for antimere teeth #7 and #10, treatment group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months Table 27: Descriptive statistics of lesion area for antimere teeth #8 and #9, control group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months Table 28: Descriptive statistics of lesion area for antimere teeth #8 and #9, treatment group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months ** Significantly different (p=0.0331, a Wilcoxon signed-rank test).
49 39 Table 29: Descriptive statistics of lesion area for all teeth, control group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months Table 30: Descriptive statistics of lesion area for all teeth, treatment group. Variable N Mean Std Dev Min Max Median Lesion Area - Baseline Lesion Area 3 Months ** Significantly different (p=0.0219, a paired-sample t-test). Based on the two-sample t-test, the data showed that there was no significant difference in F value between control and treatment groups at baseline for teeth numbers 7, 8, 10, 11 and all antimere teeth (p>0.05 in each instance), except for tooth number 6. The significant difference in F values between control and treatment groups was found at baseline for tooth #6 (p=0.0240). Data showed that mean F values were significantly less negative in treatment group than control group (mean F: vs , respectively) (Table 31-42). Due to insufficient data, a statistical test was unable to be conducted for tooth #9.
50 40 Considering all the teeth at baseline, there was a significant difference in F values between control and treatment groups (p=0.0268, a Wilcoxon rank-sum test). Data showed that median or mean F values was significantly less negative in treatment group than control group (median F: -7.4 vs , respectively) (Table 49 and 50). At 3-month follow-up, no significant differences were found for teeth numbers 6, 7, 8, 10, 11, and all antimere teeth (p>0.05 in each instance). Due to insufficient data, a statistical test was unable to be conducted for tooth #9. The data showed that there was a significant difference in F values between control and treatment groups at 3-month follow-up for all teeth (p=0.0332, Wilcoxon rank-sum test). Data showed that median or mean F values were significantly less negative in treatment group than control group (median F: vs , respectively) (Table 49 and 50). To compare the changes in F values from baseline to 3-month follow-up between the two groups, a new variable called F_value_change was created, and this new variable is defined as F values at baseline minus F values at 3-month follow-up. Based on the two-sample t-test, there were no significant differences between control and treatment groups for the mean change in F values from baseline to 3-month follow-up for teeth numbers 6, 7, 8, 10, and 11; all antimere teeth; and for all teeth (p>0.05 for each instance). Due to insufficient data, a statistical test was unable to be conducted for tooth #9. For the control group, the data showed there was no significant difference in F values between baseline and 3-month follow-up for teeth numbers 6, 7, 8, 10, 11, and all antimere teeth (p>0.05 in each instance). Due to insufficient data, a statistical test was unable to be conducted for tooth #9. The results indicated that there was a significant difference in F values between baseline and 3-month follow-up for all teeth (p=0.0013, a Wilcoxon signed-rank test). Data showed that mean or median F values was significantly less negative at 3-month follow-up than at baseline (mean or median F: or vs or , respectively) (Table 49).
51 41 For the treatment group, no significant differences in F values between baseline and 3-month follow-up were found for teeth numbers 6, 7, 8, 9, 10, 11; and all antimere teeth (p>0.05 in each instance). The results indicated that there was a significant difference in F values between baseline and 3-month follow-up for all teeth (p=0.0288, a Wilcoxon signed-rank test). Data showed that median F values was significantly less negative at 3-month follow-up than at baseline (mean or median F: or vs or -7.40, respectively) (Table 50). Table 31: Descriptive statistics of F values for tooth #6, control group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months Table 32: Descriptive statistics of F values for tooth #7, control group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months
52 42 Table 33: Descriptive statistics of F values for tooth #8, control group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months Table 34: Descriptive statistics of F values for tooth #9, control group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months Table 35: Descriptive statistics of F values for tooth #10, control group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months
53 43 Table 36: Descriptive statistics of F values for tooth #11, control group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months Table 37: Descriptive statistics of F values for tooth #6, treatment group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months Table 38: Descriptive statistics of F values for tooth #7, treatment group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months
54 44 Table 39: Descriptive statistics of F values for tooth #8, treatment group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months Table 40: Descriptive statistics of F values for tooth #9, treatment group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months Table 41: Descriptive statistics of F values for tooth #10, treatment group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months
55 45 Table 42: Descriptive statistics of F values for tooth #11, treatment group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months Table 43: Descriptive statistics of F values for antimere teeth #6 and #11, control group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months Table 44: Descriptive statistics of F values for antimere teeth #6 and #11, treatment group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months
56 46 Table 45: Descriptive statistics of F values for antimere teeth #7 and #10, control group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months Table 46: Descriptive statistics of F values for antimere teeth #7 and #10, treatment group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months Table 47: Descriptive statistics of F values for antimere teeth #8 and #9, control group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months
57 47 Table 48: Descriptive statistics of F values for antimere teeth #8 and #9, treatment group. Variable N Mean Std Dev Min Max Median F Value - Baseline F Value 3 Months Table 49: Descriptive statistics of F values for all teeth, control group. Variable N Mean** Std Dev Min Max Median F Value - Baseline F Value 3 Months ** Significantly different between baseline and follow-up (p=0.0013, a Wilcoxon signedrank test). Table 50: Descriptive statistics of F values for all teeth, treatment group. Variable N Mean** Std Dev Min Max Median F Value - Baseline F Value 3 Months ** Significantly different between baseline and follow-up (p=0.0288, a Wilcoxon signedrank test).
58 48 White spot lesion area was measured from a photograph at baseline and 3-month follow-up. The photographic results show a significant difference in the lesion area for antimere teeth #6 and #11 (p=0.0235) in the control group. In the treatment group, tooth #6 (p=0.0434), antimere teeth #6 and #11 (p=0.0181) and #8 and #9 (p=0.0331), and all teeth (p=0.0219) showed a significant difference in the lesion areas measured between baseline and follow-up. QLF images were made at the same time and the white spot lesions were quantified using F values. When comparing the F values between baseline and 3-month follow-up within both the control group and treatment group for all teeth, the results indicate that there is a significant difference (p= and p= , respectively). There was no significant difference found when looking at each tooth or antimere teeth.



59 49 Figure 4. Photographic images illustrating remineralization in the treatment group, T0 and T4 respectively.



60 50 (Figure 4 Continued)



61 51 Figure 5. Photographic images illustrating remineralization in the control group, T0 and T4 respectively.

 and control group")
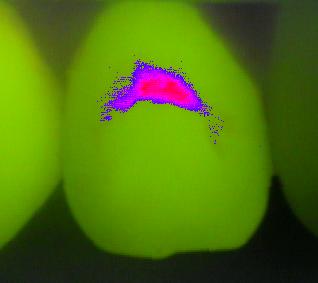
62 Figure 6. QLF images illustrating remineralization in treatment group (above) and control group (below), T0 and T4 respectively. 52

 and control")
63 Figure 7. QLF images illustrating no significant remineralization in treatment group (above) and control group (below), T0 and T4 respectively. 53
64 Figure 8. Treatment group QLF images (above) and photographic images (below), T0 and T4 respectively. 54


65 (Figure 8 Continued) 55
")
66 (Figure 8 Continued) 56
 and photographic")
67 57 Figure 9. Control group QLF images (above) and photographic images (below), T0 and T4 respectively.


68 (Figure 9 Continued) 58


69 (Figure 9 Continued) 59
This thesis is available at Iowa Research Online:
 University of Iowa Iowa Research Online Theses and Dissertations Spring 2012 Effectiveness of Mi PasteTM, Mi Paste PlusTM, and Topex RenewTM in remineralization and visible reduction of white spot lesions
University of Iowa Iowa Research Online Theses and Dissertations Spring 2012 Effectiveness of Mi PasteTM, Mi Paste PlusTM, and Topex RenewTM in remineralization and visible reduction of white spot lesions
GC Tooth Mousse Plus for Orthodontics. Helps keep you smiling. Made from milk
 GC Tooth Mousse Plus for Orthodontics Helps keep you smiling Made from milk Prevention Daily application of GC Tooth Mousse Plus with RECALDENT (CPP-ACP) throughout the full course of orthodontic treatment
GC Tooth Mousse Plus for Orthodontics Helps keep you smiling Made from milk Prevention Daily application of GC Tooth Mousse Plus with RECALDENT (CPP-ACP) throughout the full course of orthodontic treatment
Linking Research to Clinical Practice
 Prevention of Root Caries Denise M. Bowen, RDH, MS Linking Research to Clinical Practice The purpose of Linking Research to Clinical Practice is to present evidence based information to clinical dental
Prevention of Root Caries Denise M. Bowen, RDH, MS Linking Research to Clinical Practice The purpose of Linking Research to Clinical Practice is to present evidence based information to clinical dental
GC Tooth Mousse Plus. Made from milk. Perfect for teeth.
 GC Tooth GC Tooth Made from milk. Perfect for teeth. 1 We all brush our teeth everyday. But people who really want to care for their teeth are discovering the many benefits that come from moussing their
GC Tooth GC Tooth Made from milk. Perfect for teeth. 1 We all brush our teeth everyday. But people who really want to care for their teeth are discovering the many benefits that come from moussing their
Innovative Dental Therapies for the Aging Population
 Innovative Dental Therapies for the Aging Population By Daniel H Ward DDS 1080 Polaris Pkwy Ste 130 Columbus OH 43240 614-430-8990 dward@columbus.rr.com US Population is Aging 1970-28 million>60 14% of
Innovative Dental Therapies for the Aging Population By Daniel H Ward DDS 1080 Polaris Pkwy Ste 130 Columbus OH 43240 614-430-8990 dward@columbus.rr.com US Population is Aging 1970-28 million>60 14% of
Chapter 14 Outline. Chapter 14: Hygiene-Related Oral Disorders. Dental Caries. Dental Caries. Prevention. Hygiene-Related Oral Disorders
 Chapter 14 Outline Chapter 14: Hygiene-Related Oral Disorders Hygiene-Related Oral Disorders Dental caries Prevention Gingivitis Prevention Tooth hypersensitivity Pathophysiology Treatment 2 Hygiene-Related
Chapter 14 Outline Chapter 14: Hygiene-Related Oral Disorders Hygiene-Related Oral Disorders Dental caries Prevention Gingivitis Prevention Tooth hypersensitivity Pathophysiology Treatment 2 Hygiene-Related
Tooth Mousse. Plus from GC. and MI Paste. Remineralising protective crèmes with triple the benefit: Strengthen. Protect. Replenish.
 Tooth Mousse and MI Paste Plus from GC. Remineralising protective crèmes with triple the benefit: Strengthen. Protect. Replenish. A healthy balance in the mouth, inhibit demineralisation of dentin and
Tooth Mousse and MI Paste Plus from GC. Remineralising protective crèmes with triple the benefit: Strengthen. Protect. Replenish. A healthy balance in the mouth, inhibit demineralisation of dentin and
MI Varnish The ultimate fluoride varnish
 MI Varnish The ultimate fluoride varnish GC introduces MI Varnish, the first fluoride varnish with RECALDENT (CPP-ACP) MI Varnish is a 5% NaF varnish enhanced with 2% RECALDENT (CPP-ACP) to give an exceptional
MI Varnish The ultimate fluoride varnish GC introduces MI Varnish, the first fluoride varnish with RECALDENT (CPP-ACP) MI Varnish is a 5% NaF varnish enhanced with 2% RECALDENT (CPP-ACP) to give an exceptional
Iowa Research Online. University of Iowa. Andre Correia Jham University of Iowa. Theses and Dissertations. Spring 2010
 University of Iowa Iowa Research Online Theses and Dissertations Spring 2010 The efficacy of Novamin powered technology Oravive and TopexRenew, Crest and Prevident 5000 Plus in preventing enamel demineralization
University of Iowa Iowa Research Online Theses and Dissertations Spring 2010 The efficacy of Novamin powered technology Oravive and TopexRenew, Crest and Prevident 5000 Plus in preventing enamel demineralization
Management of ECC and Minimally Invasive Dentistry
 Management of ECC and Minimally Invasive Dentistry Ranbir Singh DMD MPH NYU-Lutheran Phoenix Pgy1 Pediatric Dental Resident Phoenix ECC Management Management of dental caries includes identification of
Management of ECC and Minimally Invasive Dentistry Ranbir Singh DMD MPH NYU-Lutheran Phoenix Pgy1 Pediatric Dental Resident Phoenix ECC Management Management of dental caries includes identification of
Dental caries prevention. Preventive programs for children 5DM
 Dental caries prevention Preventive programs for children 5DM Definition of Terms Preventive dentistry: usage of all the means to achieve and maintain the optimal oral health prevention of dental caries,
Dental caries prevention Preventive programs for children 5DM Definition of Terms Preventive dentistry: usage of all the means to achieve and maintain the optimal oral health prevention of dental caries,
White Spot Lesions: A Hygiene Perspective in the Orthodontic Practice. 16 MAY 2016 // hygienetown.com. clinical orthodontics // feature
 White Spot Lesions: A Hygiene Perspective in the Orthodontic Practice by Miranda Valenzuela, RDH Miranda Valenzuela, RDH, graduated in 2006 with an associate degree in dental hygiene, and has received
White Spot Lesions: A Hygiene Perspective in the Orthodontic Practice by Miranda Valenzuela, RDH Miranda Valenzuela, RDH, graduated in 2006 with an associate degree in dental hygiene, and has received
Restorative treatment The history of dental caries management consisted of many restorations placed as well as many teeth removed and prosthetic
 Restorative treatment The history of dental caries management consisted of many restorations placed as well as many teeth removed and prosthetic replacements provided. Paradigm shift towards a medical
Restorative treatment The history of dental caries management consisted of many restorations placed as well as many teeth removed and prosthetic replacements provided. Paradigm shift towards a medical
Linking Research to Clinical Practice
 Linking Research to Clinical Practice Non Fluoride Caries Preventive Agents Denise M. Bowen, RDH, MS The purpose of Linking Research to Clinical Practice is to present evidence based information to clinical
Linking Research to Clinical Practice Non Fluoride Caries Preventive Agents Denise M. Bowen, RDH, MS The purpose of Linking Research to Clinical Practice is to present evidence based information to clinical
Fluor Protector S. The protective fluoride varnish. Superior protection against dental caries and erosion
 Fluor Protector S The protective fluoride varnish Superior protection against dental caries and erosion Fluor Protector S The strong fluoride varnish In order to stay healthy and look good, teeth need
Fluor Protector S The protective fluoride varnish Superior protection against dental caries and erosion Fluor Protector S The strong fluoride varnish In order to stay healthy and look good, teeth need
The 4Cs in Solving the Caries Puzzle
 The 4Cs in Solving the Caries Puzzle CAMBRA Caries Detection & Assesment System (ICDAS) Case-based protocol Calcium/Phosphate & Fluoride Objectives: Engaging in this program, the participant will be able
The 4Cs in Solving the Caries Puzzle CAMBRA Caries Detection & Assesment System (ICDAS) Case-based protocol Calcium/Phosphate & Fluoride Objectives: Engaging in this program, the participant will be able
Copyright and Acknowledgements. Caries Management Course Module: Topical Therapies. Disclaimer 3/31/2015
 Caries Management Course Module: Topical Therapies Robert S Jones DDS PhD Assistant Professor Division of Pediatric Dentistry University of Minnesota Copyright and Acknowledgements This work is protected
Caries Management Course Module: Topical Therapies Robert S Jones DDS PhD Assistant Professor Division of Pediatric Dentistry University of Minnesota Copyright and Acknowledgements This work is protected
Prevention of white spot lesions in orthodontic practice: a contemporary review
 REVIEW Australian Dental Journal 2006;51:(4):284-289 Prevention of white spot lesions in orthodontic practice: a contemporary review TR Sudjalim,* MG Woods, DJ Manton Abstract The development of white
REVIEW Australian Dental Journal 2006;51:(4):284-289 Prevention of white spot lesions in orthodontic practice: a contemporary review TR Sudjalim,* MG Woods, DJ Manton Abstract The development of white
CAries Management By Risk Assessment"(CAMBRA) - a must in preventive dentistry
 - a must in preventive dentistry") CAries Management By Risk Assessment"(CAMBRA) - a must in preventive dentistry Nanda Kishor KM* *MDS, Reader, Department of Conservative and Endodontics Pacific Dental College, Udaipur, Rajasthan, India
CAries Management By Risk Assessment"(CAMBRA) - a must in preventive dentistry Nanda Kishor KM* *MDS, Reader, Department of Conservative and Endodontics Pacific Dental College, Udaipur, Rajasthan, India
Bacterial Plaque and Its Relation to Dental Diseases. As a hygienist it is important to stress the importance of good oral hygiene and
 Melissa Rudzinski Preventive Dentistry Shaunda Clark November 2013 Bacterial Plaque and Its Relation to Dental Diseases As a hygienist it is important to stress the importance of good oral hygiene and
Melissa Rudzinski Preventive Dentistry Shaunda Clark November 2013 Bacterial Plaque and Its Relation to Dental Diseases As a hygienist it is important to stress the importance of good oral hygiene and
Oral health education for caries prevention
 Oral health education for caries prevention Objective Understand the fundamentals that inform oral health education programmes. Understand how to segment oral health information for preventive purposes
Oral health education for caries prevention Objective Understand the fundamentals that inform oral health education programmes. Understand how to segment oral health information for preventive purposes
Uses of Fluoride in Dental Practices
 Uses of Fluoride in Dental Practices BY: Sulafa El-Samarrai Preventive &pedodontic department General Mechanisms of Action in Caries Reduction 1-Increase enamel resistance or reduction in enamel solubility
Uses of Fluoride in Dental Practices BY: Sulafa El-Samarrai Preventive &pedodontic department General Mechanisms of Action in Caries Reduction 1-Increase enamel resistance or reduction in enamel solubility
Root Surface Protection Simple. Effective. Important.
 GC Fuji VII / Fuji VII EP Root Surface Protection Simple. Effective. Important. Brush up your painting skills and help your patients Q&A Prof. Laurie Walsh University of Queensland lifestyle factors (frequency
GC Fuji VII / Fuji VII EP Root Surface Protection Simple. Effective. Important. Brush up your painting skills and help your patients Q&A Prof. Laurie Walsh University of Queensland lifestyle factors (frequency
Saliva. Introduction. Salivary Flow. Saliva and the Plaque Biofilm. The Minerals in Saliva
 Saliva Introduction Saliva is like a bloodstream to the mouth. As does blood, saliva helps build and maintain the health of the soft and hard tissues. Saliva removes waste products and provides disease-fighting
Saliva Introduction Saliva is like a bloodstream to the mouth. As does blood, saliva helps build and maintain the health of the soft and hard tissues. Saliva removes waste products and provides disease-fighting
Sealants First! Prioritizing Prevention through Same Day Sealants
 Sealants First! Prioritizing Prevention through Same Day Sealants Candace Owen, RDH, MS, MPH NNOHA Education Director Janine Musheno, DMD Project HOME Dental Director 2018 NNOHA Annual Conference Stephen
Sealants First! Prioritizing Prevention through Same Day Sealants Candace Owen, RDH, MS, MPH NNOHA Education Director Janine Musheno, DMD Project HOME Dental Director 2018 NNOHA Annual Conference Stephen
EFFICACY OF AMORPHOUS CALCIUM PHOSPHATE, G.C. TOOTH MOUSSE AND GLUMA DESENSITIZER IN TREATING DENTIN HYPERSENSITIVITY : A RANDOMIZED CLINICAL TRIAL
 Original Article International Journal of Dental and Health Sciences Volume 01,Issue 02 EFFICACY OF AMORPHOUS CALCIUM PHOSPHATE, G.C. TOOTH MOUSSE AND GLUMA DESENSITIZER IN TREATING DENTIN HYPERSENSITIVITY
Original Article International Journal of Dental and Health Sciences Volume 01,Issue 02 EFFICACY OF AMORPHOUS CALCIUM PHOSPHATE, G.C. TOOTH MOUSSE AND GLUMA DESENSITIZER IN TREATING DENTIN HYPERSENSITIVITY
Tooth hypersensitivity and Dental erosion DR. KÁROLY BARTHA
 Tooth hypersensitivity and Dental erosion DR. KÁROLY BARTHA 2 Why Is Erosion an Issue Now? Changing dietary habits Higher consumption of acidic beverages (colas, sport drinks) Higher incidence of xerostomia
Tooth hypersensitivity and Dental erosion DR. KÁROLY BARTHA 2 Why Is Erosion an Issue Now? Changing dietary habits Higher consumption of acidic beverages (colas, sport drinks) Higher incidence of xerostomia
Effect of Three Different Remineralizing Agents on Enamel Caries Formation An in vitro Study
 KATHMANDU UNIVERSITY MEDICAL JOURNAL Effect of Three Different Remineralizing Agents on Enamel Caries Formation An in vitro Study Sathe N, 1 Chakradhar Raju RVS, 1 Chandrasekhar V 2 Department of Conservative
KATHMANDU UNIVERSITY MEDICAL JOURNAL Effect of Three Different Remineralizing Agents on Enamel Caries Formation An in vitro Study Sathe N, 1 Chakradhar Raju RVS, 1 Chandrasekhar V 2 Department of Conservative
Early Childhood Caries (ECC) KEVIN ZIMMERMAN DMD
 KEVIN ZIMMERMAN DMD") Early Childhood Caries (ECC) KEVIN ZIMMERMAN DMD What Is Early Childhood Caries? Early Childhood Caries (ECC) is a transmissible infectious process that affects children younger than age 6 and results
Early Childhood Caries (ECC) KEVIN ZIMMERMAN DMD What Is Early Childhood Caries? Early Childhood Caries (ECC) is a transmissible infectious process that affects children younger than age 6 and results
Overview: The health care provider explores the health behaviors and preventive measures that enhance children s oral health.
 Lesson 5: Prevention Overview: The health care provider explores the health behaviors and preventive measures that enhance children s oral health. Goals: The health care provider will be able to describe:
Lesson 5: Prevention Overview: The health care provider explores the health behaviors and preventive measures that enhance children s oral health. Goals: The health care provider will be able to describe:
DEPOSITS. Dentalelle Tutoring 1
 DEPOSITS Dentalelle Tutoring WWW.DENTALELLE.COM 1 PH SCALE WWW.DENTALELLE.COM 2 DENTAL CARIES Dental caries is a dynamic process that involves a susceptible tooth, cariogenic bacteria in dental plaque
DEPOSITS Dentalelle Tutoring WWW.DENTALELLE.COM 1 PH SCALE WWW.DENTALELLE.COM 2 DENTAL CARIES Dental caries is a dynamic process that involves a susceptible tooth, cariogenic bacteria in dental plaque
Caries Clinical Guidelines. Low Caries Risk
 Caries Clinical Guidelines Clinical guidelines Low Caries Risk at LOW RISK for future dental caries. Your patient does not show any disease indicators or factors that predict dental caries in the immediate
Caries Clinical Guidelines Clinical guidelines Low Caries Risk at LOW RISK for future dental caries. Your patient does not show any disease indicators or factors that predict dental caries in the immediate
Health Promotion and Disease Prevention are the Foundation of Community Based Health Care
 Health Promotion and Disease Prevention are the Foundation of Community Based Health Care Joan I. Gluch, RDH, Ph.D. Director of Community Health Associate Dean for Academic Policies Renewed Perspective
Health Promotion and Disease Prevention are the Foundation of Community Based Health Care Joan I. Gluch, RDH, Ph.D. Director of Community Health Associate Dean for Academic Policies Renewed Perspective
EFFECT OF ACIDULATED PHOSPHATE FLUORIDE GEL ON THE PREVENTION OF WHITE SPOT LESIONS IN PATIENTS UNDERGOING ACTIVE ORTHODONTIC TREATMENT.
 EFFECT OF ACIDULATED PHOSPHATE FLUORIDE GEL ON THE PREVENTION OF WHITE SPOT LESIONS IN PATIENTS UNDERGOING ACTIVE ORTHODONTIC TREATMENT A Thesis by CORNEIL KIMBERLY HUTTO FRETTY Submitted to the Office
EFFECT OF ACIDULATED PHOSPHATE FLUORIDE GEL ON THE PREVENTION OF WHITE SPOT LESIONS IN PATIENTS UNDERGOING ACTIVE ORTHODONTIC TREATMENT A Thesis by CORNEIL KIMBERLY HUTTO FRETTY Submitted to the Office
Title:Is there a place for Tooth Mousse(R) in the prevention and treatment of early dental caries? A systematic review.
 in the prevention and treatment of early dental caries? A systematic review.") Author's response to reviews Title:Is there a place for Tooth Mousse(R) in the prevention and treatment of early dental caries? A systematic review. Authors: Sarah L Raphael (sarah.raphael@sydney.edu.au)
Author's response to reviews Title:Is there a place for Tooth Mousse(R) in the prevention and treatment of early dental caries? A systematic review. Authors: Sarah L Raphael (sarah.raphael@sydney.edu.au)
OMNII Oral Pharmaceuticals
 Fluoride Varnish in a Pediatric Practice Created by W. Edward Gonzalez D.M.D. OMNII Oral Pharmaceuticals The Preventive Care Consultants OMNII Firsts In Dentistry OMNII Gel PerioMed white & brite FlossRx
Fluoride Varnish in a Pediatric Practice Created by W. Edward Gonzalez D.M.D. OMNII Oral Pharmaceuticals The Preventive Care Consultants OMNII Firsts In Dentistry OMNII Gel PerioMed white & brite FlossRx
Examination and Treatment Protocols for Dental Caries and Inflammatory Periodontal Disease
 Examination and Treatment Protocols for Dental Caries and Inflammatory Periodontal Disease Dental Caries The current understanding of the caries process supports the shift in caries management from a restorative-only
Examination and Treatment Protocols for Dental Caries and Inflammatory Periodontal Disease Dental Caries The current understanding of the caries process supports the shift in caries management from a restorative-only
Teeth to Treasure. Grades: 4 to 6
 Teeth to Treasure Grades: 4 to 6 What is oral health? It s keeping your teeth, gums and mouth healthy! Why do you suppose this is important? Well, let s take a look at how we use and need our teeth. Appearance
Teeth to Treasure Grades: 4 to 6 What is oral health? It s keeping your teeth, gums and mouth healthy! Why do you suppose this is important? Well, let s take a look at how we use and need our teeth. Appearance
Fluoridens 133 Fluorosilicic acid 136 Fluorosis, see Dental fluorosis Foams 118 acute toxicity 71, 122 clinical efficacy 122 Free saliva 149, 150
 Subject Index Abrasive systems, dentifrices 123 Absorption 23, 24, 38, 78 Accidental poisonings 66, 67, 69, 70, see also Acute toxicity Acid-base status, see also ph metabolism effects 28, 29 toxicity
Subject Index Abrasive systems, dentifrices 123 Absorption 23, 24, 38, 78 Accidental poisonings 66, 67, 69, 70, see also Acute toxicity Acid-base status, see also ph metabolism effects 28, 29 toxicity
19/03/2018. Objectives
 Target group 10 to 14 years old Aims This presentation has been designed to provide those viewing it with information on how to maintain a good Oral Health Objectives At the end, the viewer will be able
Target group 10 to 14 years old Aims This presentation has been designed to provide those viewing it with information on how to maintain a good Oral Health Objectives At the end, the viewer will be able
CARIES RISK ASSESSMENT FORM FOR AGE 0 TO 5 YEARS Instructions on reverse Patient Name: I.D. # Age Date Initial/baseline exam date Recall/POE date
 CARIES RISK ASSESSMENT FORM FOR AGE 0 TO 5 YEARS Instructions on reverse Patient Name: I.D. # Age Date Initial/baseline exam date Recall/POE date Respond to each question in sections 1, 2, and 3 with a
CARIES RISK ASSESSMENT FORM FOR AGE 0 TO 5 YEARS Instructions on reverse Patient Name: I.D. # Age Date Initial/baseline exam date Recall/POE date Respond to each question in sections 1, 2, and 3 with a
Effect of addition of Fluoride on Enamel remineralization potential of CCP-ACP and Novamin: A comparative Study
 ENDODONTOLOGY Volume: 27 Issue 2 December 2015 ORIGINAL RESEARCH Effect of addition of Fluoride on Enamel remineralization potential of Sai Kalyan S. 1, Wagle Rahul 2, Chandki rita 3, Byakod Praveen 4,
ENDODONTOLOGY Volume: 27 Issue 2 December 2015 ORIGINAL RESEARCH Effect of addition of Fluoride on Enamel remineralization potential of Sai Kalyan S. 1, Wagle Rahul 2, Chandki rita 3, Byakod Praveen 4,
Management of Inadequate Margins and Gingival Recession Presenting as Tooth Sensitivity
 Management of Inadequate Margins and Gingival Recession Presenting as Tooth Sensitivity Nicolas Elian, DDS Private Practice Englewood Cliffs, New Jersey David Geon U Kim, DDS, MS Faculty and Research Coordinator
Management of Inadequate Margins and Gingival Recession Presenting as Tooth Sensitivity Nicolas Elian, DDS Private Practice Englewood Cliffs, New Jersey David Geon U Kim, DDS, MS Faculty and Research Coordinator
Fluor Protector Overview
 Fluor Protector Overview Superior protection against dental caries and erosion Fluoride Clinically proven Fluoride varnish Features and mechanism of action Application Intensive care gel Risks to teeth
Fluor Protector Overview Superior protection against dental caries and erosion Fluoride Clinically proven Fluoride varnish Features and mechanism of action Application Intensive care gel Risks to teeth
FRANK OSEI-BONSU UGDS/KBTH
 FRANK OSEI-BONSU UGDS/KBTH Definition Introduction G. V. Black s concept of Restoration New classification of Caries Principles & Concept of MID Conclusion An approach to the management of dental caries
FRANK OSEI-BONSU UGDS/KBTH Definition Introduction G. V. Black s concept of Restoration New classification of Caries Principles & Concept of MID Conclusion An approach to the management of dental caries
Effects of orthodontic treatment with a fixed appliance on the caries experience of patients with high and low risk of caries
 Journal of Dental Sciences (2011) 6, 195e199 Available online at www.sciencedirect.com journal homepage: www.e-jds.com ORIGINAL ARTICLE Effects of orthodontic treatment with a fixed appliance on the caries
Journal of Dental Sciences (2011) 6, 195e199 Available online at www.sciencedirect.com journal homepage: www.e-jds.com ORIGINAL ARTICLE Effects of orthodontic treatment with a fixed appliance on the caries
Comparative Evaluation of Two Remineralizing Agents on Enamel around Orthodontic /jp-journals
 JIOS Comparative Evaluation of Two Remineralizing Agents on Enamel around Orthodontic 10.5005/jp-journals-10021-1267 Brackets: An in vitro Study Original article Comparative Evaluation of Two Remineralizing
JIOS Comparative Evaluation of Two Remineralizing Agents on Enamel around Orthodontic 10.5005/jp-journals-10021-1267 Brackets: An in vitro Study Original article Comparative Evaluation of Two Remineralizing
JIOS ABSTRACT. Received on: 7/9/13 Accepted after Revision: 21/9/13
 JIOS Clinical Evaluation of Enamel Demineralization during Orthodontic Treatment: An in vivo 10.5005/jp-journals-10021-1251 Study using GC Tooth Mousse Plus Original Research Clinical Evaluation of Enamel
JIOS Clinical Evaluation of Enamel Demineralization during Orthodontic Treatment: An in vivo 10.5005/jp-journals-10021-1251 Study using GC Tooth Mousse Plus Original Research Clinical Evaluation of Enamel
The 21 st Century vision on. caries management, now brought into your. daily practice
 The 21 st Century vision on caries management, now brought into your daily practice Minimum Intervention A 21 st century vision on Patient Caries Management The concept of minimal intervention dentistry
The 21 st Century vision on caries management, now brought into your daily practice Minimum Intervention A 21 st century vision on Patient Caries Management The concept of minimal intervention dentistry
OliNano Seal Professional prophylaxis for long-term protection
 Professional prophylaxis for long-term protection NEW The patented formula of silicone polymer NANO Technology General information Dental health is one of the main factors to maintain overall health, and
Professional prophylaxis for long-term protection NEW The patented formula of silicone polymer NANO Technology General information Dental health is one of the main factors to maintain overall health, and
BioCoat Featuring SmartCap Technology
 R R Breakthrough! BioCoat Featuring SmartCap Technology The only bioactive pit and fissure sealant that provides relentless protection through daily release of fluoride, calcium and phosphate ions. Bioactive
R R Breakthrough! BioCoat Featuring SmartCap Technology The only bioactive pit and fissure sealant that provides relentless protection through daily release of fluoride, calcium and phosphate ions. Bioactive
3M Fast Release Varnish
 3M Fast Release Varnish 5% Sodium Fluoride Varnish Fast Release Formula Technical Data Sheet 2 3M Fast Release Varnish 3M Fast Release Varnish is a fluoride-containing varnish. It can be applied to enamel
3M Fast Release Varnish 5% Sodium Fluoride Varnish Fast Release Formula Technical Data Sheet 2 3M Fast Release Varnish 3M Fast Release Varnish is a fluoride-containing varnish. It can be applied to enamel
Ivoclar Vivadent. Professional Care Program. Oral health management A system of solutions
 Ivoclar Vivadent Professional Care Program Oral health management A system of solutions Ivoclar Vivadent Oral health management Contents CRT Bacteria Makes bacteria visible CRT Bacteria healthy mouth healthy
Ivoclar Vivadent Professional Care Program Oral health management A system of solutions Ivoclar Vivadent Oral health management Contents CRT Bacteria Makes bacteria visible CRT Bacteria healthy mouth healthy
Dental Health. This document includes 12 tips that can be used as part of a monthly year-long dental health campaign or as individual messages.
 Dental Health This document includes 12 tips that can be used as part of a monthly year-long dental health campaign or as individual messages. What is gingivitis? Gingivitis is the beginning stage of gum
Dental Health This document includes 12 tips that can be used as part of a monthly year-long dental health campaign or as individual messages. What is gingivitis? Gingivitis is the beginning stage of gum
PUBLISHED VERSION. This document has been archived with permission from the Australian Dental Association, received 18th January, 2007.
 PUBLISHED VERSION Saunders, J. G. C.; McIntyre, John Malcolm The ability of 1.23% acidulated phosphate fluoride gel to inhibit simulated endogenous erosion in tooth roots Australian Dental Journal, 2005;
PUBLISHED VERSION Saunders, J. G. C.; McIntyre, John Malcolm The ability of 1.23% acidulated phosphate fluoride gel to inhibit simulated endogenous erosion in tooth roots Australian Dental Journal, 2005;
NEW. Block plaque, calculus, and halitosis with the science of prevention
 NEW Block plaque, calculus, and halitosis with the science of prevention OraVet Dental Hygiene Chews Backed by Science You Can Believe In A New Way to Combat Plaque, Calculus, and Halitosis Where They
NEW Block plaque, calculus, and halitosis with the science of prevention OraVet Dental Hygiene Chews Backed by Science You Can Believe In A New Way to Combat Plaque, Calculus, and Halitosis Where They
RISK FACTORS BY AGE (Wandera et al. 2000)
") RISK ASSESSMENT Stacey Lubetsky DMD ST. BARNABAS HOSPITAL RISK ASSESSMENT The primary thrust of early risk assessment is to screen for parent-infant groups who are at risk of ECC and would benefit from
RISK ASSESSMENT Stacey Lubetsky DMD ST. BARNABAS HOSPITAL RISK ASSESSMENT The primary thrust of early risk assessment is to screen for parent-infant groups who are at risk of ECC and would benefit from
In vitro comparison of microabrasion, CPP-ACP, CPP-ACFP and combination therapies on the remineralization of white spot lesions
 Nova Southeastern University NSUWorks College of Dental Medicine Student Theses, Dissertations and Capstones College of Dental Medicine 1-1-2014 In vitro comparison of microabrasion, CPP-ACP, CPP-ACFP
Nova Southeastern University NSUWorks College of Dental Medicine Student Theses, Dissertations and Capstones College of Dental Medicine 1-1-2014 In vitro comparison of microabrasion, CPP-ACP, CPP-ACFP
Everyday Relief. Everyday Protection.
 Everyday Relief. Everyday Protection. CLINICAL RESULTS ON BACK! A Targeted Approach to Practice Building! Treats Sensitivity Soothes & Moisturizes Dry Mouth Tissues Helps to Prevent Caries & Gingivitis
Everyday Relief. Everyday Protection. CLINICAL RESULTS ON BACK! A Targeted Approach to Practice Building! Treats Sensitivity Soothes & Moisturizes Dry Mouth Tissues Helps to Prevent Caries & Gingivitis
Comparative Analysis of Remineralizing Potential of Three Commercially Available Agents- An in Vitro Study
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 2 Ver. III (February. 2017), PP 01-05 www.iosrjournals.org Comparative Analysis of Remineralizing
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 2 Ver. III (February. 2017), PP 01-05 www.iosrjournals.org Comparative Analysis of Remineralizing
OUR EXPERIENCE WITH GRADIA DIRECT IN THE RESTORATION OF ANTERIOR TEETH
 ISSN: 1312-773X (Online) Journal of IMAB - Annual Proceeding (Scientific Papers) 2006, vol. 12, issue 2 OUR EXPERIENCE WITH GRADIA DIRECT IN THE RESTORATION OF ANTERIOR TEETH Snezhanka Topalova-Pirinska,
ISSN: 1312-773X (Online) Journal of IMAB - Annual Proceeding (Scientific Papers) 2006, vol. 12, issue 2 OUR EXPERIENCE WITH GRADIA DIRECT IN THE RESTORATION OF ANTERIOR TEETH Snezhanka Topalova-Pirinska,
PERINATAL CARE AND ORAL HEALTH
 PERINATAL CARE AND ORAL HEALTH Lakshmi Mallavarapu, DDS Terry Reilly Health Services Boise, Idaho CE objectives Recognize the necessity of Oral Care during Perinatal Period Examine and assess teeth and
PERINATAL CARE AND ORAL HEALTH Lakshmi Mallavarapu, DDS Terry Reilly Health Services Boise, Idaho CE objectives Recognize the necessity of Oral Care during Perinatal Period Examine and assess teeth and
2012 Ph.D. APPLIED EXAM Department of Biostatistics University of Washington
 2012 Ph.D. APPLIED EXAM Department of Biostatistics University of Washington Background Dental caries is an infectious, transmissible bacterial disease that is a common childhood condition in the United
2012 Ph.D. APPLIED EXAM Department of Biostatistics University of Washington Background Dental caries is an infectious, transmissible bacterial disease that is a common childhood condition in the United
EVALUATION OF COLOR CHANGE IN WHITE SPOT LESIONS OF ENAMEL FLUOROSIS USING A RESIN INFILTRATE
 EVALUATION OF COLOR CHANGE IN WHITE SPOT LESIONS OF ENAMEL FLUOROSIS USING A RESIN INFILTRATE Monisha Singhal PG STUDENT DEPARTMENT OF PEDODONTICS & PREVENTIVE DENTISTRY CHANDRA DENTAL COLLEGE & HOSPITAL
EVALUATION OF COLOR CHANGE IN WHITE SPOT LESIONS OF ENAMEL FLUOROSIS USING A RESIN INFILTRATE Monisha Singhal PG STUDENT DEPARTMENT OF PEDODONTICS & PREVENTIVE DENTISTRY CHANDRA DENTAL COLLEGE & HOSPITAL
IJCPD INTRODUCTION ABSTRACT /jp-journals
 IJCPD Reshma Rajan et al RESEARCH ARTICLE 10.5005/jp-journals-10005-1281 A Polarized Light Microscopic Study to Comparatively evaluate Four Remineralizing Agents on Enamel viz CPP-ACPF, ReminPro, SHY-NM
IJCPD Reshma Rajan et al RESEARCH ARTICLE 10.5005/jp-journals-10005-1281 A Polarized Light Microscopic Study to Comparatively evaluate Four Remineralizing Agents on Enamel viz CPP-ACPF, ReminPro, SHY-NM
Casein is the predominant
 CLINICAL PRACTICE CRITICAL REVIEW Clinical efficacy of casein derivatives A systematic review of the literature Amir Azarpazhooh, DDS, MSc; Hardy Limeback, BSc, PhD, DDS Casein is the predominant phosphoprotein
CLINICAL PRACTICE CRITICAL REVIEW Clinical efficacy of casein derivatives A systematic review of the literature Amir Azarpazhooh, DDS, MSc; Hardy Limeback, BSc, PhD, DDS Casein is the predominant phosphoprotein
Food, Nutrition & Dental Health Summary
 By Liz Pearson, RD www.lizpearson.com Food, Nutrition & Dental Health Summary Canadian Health Measures Survey (2007 to 2009) 57% of 6 11 year olds have or have had a cavity 59% of 12 19 year olds have
By Liz Pearson, RD www.lizpearson.com Food, Nutrition & Dental Health Summary Canadian Health Measures Survey (2007 to 2009) 57% of 6 11 year olds have or have had a cavity 59% of 12 19 year olds have
Promoting Oral Health
 Promoting Oral Health Hope Saltmarsh, RDH, M.Ed. Doug Johnson, DMD October 2009 11/3/2009 12:14:04 PM 5864_ER_RED 1 Learning Objectives Identify Bright Futures recommendations for oral health. Describe
Promoting Oral Health Hope Saltmarsh, RDH, M.Ed. Doug Johnson, DMD October 2009 11/3/2009 12:14:04 PM 5864_ER_RED 1 Learning Objectives Identify Bright Futures recommendations for oral health. Describe
Course #:
 Welcome to Lesson 7: Indicators of Problems of the Dental Health for Individuals with Disabilities webcast series. Please adjust your computer volume so that it is at a comfortable listening level for
Welcome to Lesson 7: Indicators of Problems of the Dental Health for Individuals with Disabilities webcast series. Please adjust your computer volume so that it is at a comfortable listening level for
Iowa Research Online. University of Iowa. Tanner Jay Clark University of Iowa. Theses and Dissertations. Spring Copyright 2010 Tanner Jay Clark
 University of Iowa Iowa Research Online Theses and Dissertations Spring 2010 The efficacy of ProSeal, SeLECT Defense, OrthoCoat, and Biscover LV resin sealants on the prevention of enamel demineralization
University of Iowa Iowa Research Online Theses and Dissertations Spring 2010 The efficacy of ProSeal, SeLECT Defense, OrthoCoat, and Biscover LV resin sealants on the prevention of enamel demineralization
MODULE 15: ORAL HEALTH ACROSS THE LIFESPAN
 MODULE 15: ORAL HEALTH ACROSS THE LIFESPAN Oral Health Across the Lifespan MODULE 15: ORAL HEALTH ACROSS THE LIFESPAN Part 4: Oral Health and Older Adults Mark Wolff DDS, PhD Healthy People 2020 Objectives
MODULE 15: ORAL HEALTH ACROSS THE LIFESPAN Oral Health Across the Lifespan MODULE 15: ORAL HEALTH ACROSS THE LIFESPAN Part 4: Oral Health and Older Adults Mark Wolff DDS, PhD Healthy People 2020 Objectives
Management of initial caries lesions: Iowa survey
 University of Iowa Iowa Research Online Theses and Dissertations Spring 2017 Management of initial caries lesions: Iowa survey Amira Elgreatly University of Iowa Copyright 2017 Amira Elgreatly This thesis
University of Iowa Iowa Research Online Theses and Dissertations Spring 2017 Management of initial caries lesions: Iowa survey Amira Elgreatly University of Iowa Copyright 2017 Amira Elgreatly This thesis
Colgate-Palmolive Company, Piscataway, NJ. 2 Research Center, School of Dentistry, Medical Sciences Campus, University of Puerto Rico.
 Anticaries Efficacy of a Sodium Monofluorophosphate Dentifrice Containing Xylitol in a Dicalcium Phosphate Dihydrate Base: A 30-month caries clinical study in Costa Rica. J.L. Sintes 1, A. Elías-Boneta
Anticaries Efficacy of a Sodium Monofluorophosphate Dentifrice Containing Xylitol in a Dicalcium Phosphate Dihydrate Base: A 30-month caries clinical study in Costa Rica. J.L. Sintes 1, A. Elías-Boneta
NEW ZEALAND DATA SHEET
 1 PRODUCT NAME Clinpro 5000 anti-cavity toothpaste Vanilla Mint Clinpro 5000 anti-cavity toothpaste Spearmint Clinpro 5000 anti-cavity toothpaste Bubble Gum 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Thick
1 PRODUCT NAME Clinpro 5000 anti-cavity toothpaste Vanilla Mint Clinpro 5000 anti-cavity toothpaste Spearmint Clinpro 5000 anti-cavity toothpaste Bubble Gum 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Thick
Seniors Oral Care
 For information about oral health care, please contact the Ontario Dental Association at 416-922-3900 or visit www.youroralhealth.ca The Ontario Dental Association gratefully acknowledges UBC ELDERS Education,
For information about oral health care, please contact the Ontario Dental Association at 416-922-3900 or visit www.youroralhealth.ca The Ontario Dental Association gratefully acknowledges UBC ELDERS Education,
t. Purpose. Establishes policy and guidelines for identifying and managing oral disease risk in the Navy Military Health System.
 DEPARTMENT OF THE NAVY BUREAU OF MEDICINE AND SURGERY 2300 E STREET NW WASHINGTON DC 20372-5300 IN REPL V REFER TO BUMEDINST 6600.16A BUMED-M3/5 BUMED INSTRUCTION 6600.16A From: Chief, Bureau of Medicine
DEPARTMENT OF THE NAVY BUREAU OF MEDICINE AND SURGERY 2300 E STREET NW WASHINGTON DC 20372-5300 IN REPL V REFER TO BUMEDINST 6600.16A BUMED-M3/5 BUMED INSTRUCTION 6600.16A From: Chief, Bureau of Medicine
Remineralisation of Enamel Subsurface Lesions with Casein Phosphopeptide - Amorphous Calcium Phosphate in Patients with Fixed Orthodontic Appliances
 BALKAN JOURNAL OF STOMATOLOGY ISSN 1107-1141 STOMATOLOGICAL SOCIETY Remineralisation of Enamel Subsurface Lesions with Casein Phosphopeptide - Amorphous Calcium Phosphate in Patients with Fixed Orthodontic
BALKAN JOURNAL OF STOMATOLOGY ISSN 1107-1141 STOMATOLOGICAL SOCIETY Remineralisation of Enamel Subsurface Lesions with Casein Phosphopeptide - Amorphous Calcium Phosphate in Patients with Fixed Orthodontic
Our Teeth. Word List: find each word from the list below in the table above (just circle each word on the table and cross it off from your list)
") Your Teeth Our Teeth B I L L E V Q I Z Q Q V E J E U Q A L P S Q A V S R Q E D Y E E G L E M A N E Y R V J R R G R L E A I Y T I V A C E B R A B Q O A C A P N C X M I L K T E E T H L M X O L M I Z T E
Your Teeth Our Teeth B I L L E V Q I Z Q Q V E J E U Q A L P S Q A V S R Q E D Y E E G L E M A N E Y R V J R R G R L E A I Y T I V A C E B R A B Q O A C A P N C X M I L K T E E T H L M X O L M I Z T E
SOFT DRINKS & DENTAL HEALTH.
 SOFT DRINKS & DENTAL HEALTH www.giveuplovingpop.org.uk @gulpnow SOFT DRINKS & DENTAL HEALTH All text tables, copyright Health Equalities Group 2017 Primary authors: Alexandra Holt, MSc. Health Equalities
SOFT DRINKS & DENTAL HEALTH www.giveuplovingpop.org.uk @gulpnow SOFT DRINKS & DENTAL HEALTH All text tables, copyright Health Equalities Group 2017 Primary authors: Alexandra Holt, MSc. Health Equalities
Effects of miswak and nano calcium carbonate toothpastes on the hardness of demineralized human tooth surfaces
 Journal of Physics: Conference Series PAPER OPEN ACCESS Effects of miswak and nano calcium carbonate toothpastes on the hardness of demineralized human tooth surfaces To cite this article: F Dianti et
Journal of Physics: Conference Series PAPER OPEN ACCESS Effects of miswak and nano calcium carbonate toothpastes on the hardness of demineralized human tooth surfaces To cite this article: F Dianti et
DOSAGE FORMS AND STRENGTHS White toothpaste containing 1.1% sodium fluoride (3)
") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use 3M TM ESPE TM Clinpro TM 5000 Anti-Cavity Toothpaste safely and effectively. See full prescribing
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use 3M TM ESPE TM Clinpro TM 5000 Anti-Cavity Toothpaste safely and effectively. See full prescribing
Best Practices in Oral Health for Older Adults -How to Keep My Bite in My Life!
 Best Practices in Oral Health for Older Adults -How to Keep My Bite in My Life! Mr. has most of his natural teeth. Mr. JB Age 78. In for rehab from stroke; will return home. Non-dominant hand/arm paralyzed.
Best Practices in Oral Health for Older Adults -How to Keep My Bite in My Life! Mr. has most of his natural teeth. Mr. JB Age 78. In for rehab from stroke; will return home. Non-dominant hand/arm paralyzed.
Developing Dental Leadership. Fluoride varnish: How it works and how to apply it
 Fluoride varnish: How it works and how to apply it Fluoride Varnish It is the responsibility of the prescriber to ensure that a medicament is suitable for use A product licence indicates that the product
Fluoride varnish: How it works and how to apply it Fluoride Varnish It is the responsibility of the prescriber to ensure that a medicament is suitable for use A product licence indicates that the product
2 during treatment... how to technique. How to handle white spot lesions associated with orthodontic treatment. Issue
 Issue 17 2013 How to handle white spot lesions associated with orthodontic treatment. 1 background... It is well recognised that the placement of fixed orthodontic appliances increases a patient s risk
Issue 17 2013 How to handle white spot lesions associated with orthodontic treatment. 1 background... It is well recognised that the placement of fixed orthodontic appliances increases a patient s risk
stabilisation and surface protection
 Guiding the way to caries stabilisation and surface protection Fissure sealing MI restorations Pulp capping Hypersensitivity Protection Caries stabilisation Fuji Triage from GC. Temporary restorations
Guiding the way to caries stabilisation and surface protection Fissure sealing MI restorations Pulp capping Hypersensitivity Protection Caries stabilisation Fuji Triage from GC. Temporary restorations
SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT 2 QUALITATIVE AND QUANTITATIVE COMPOSITION
 SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Duraphat 5000 ppm Fluoride Toothpaste 2 QUALITATIVE AND QUANTITATIVE COMPOSITION 1 g of toothpaste contains 5 mg fluoride (as sodium fluoride),
SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Duraphat 5000 ppm Fluoride Toothpaste 2 QUALITATIVE AND QUANTITATIVE COMPOSITION 1 g of toothpaste contains 5 mg fluoride (as sodium fluoride),
PATIENT INFORMATION DIABETES AND ORAL HEALTH
 PATIENT INFORMATION DIABETES AND ORAL HEALTH www.dentalcareireland.ie DIABETES AND ORAL HEALTH People with poor diabetes control can be more prone to oral health problems such as gum disease, dry mouth,
PATIENT INFORMATION DIABETES AND ORAL HEALTH www.dentalcareireland.ie DIABETES AND ORAL HEALTH People with poor diabetes control can be more prone to oral health problems such as gum disease, dry mouth,
Topical versus systemic fluoride: which is more effective in preventing dental caries in high risk population?
 Boston University OpenBU Theses & Dissertations http://open.bu.edu Boston University Theses & Dissertations 2013 Topical versus systemic fluoride: which is more effective in preventing dental caries in
Boston University OpenBU Theses & Dissertations http://open.bu.edu Boston University Theses & Dissertations 2013 Topical versus systemic fluoride: which is more effective in preventing dental caries in
journal of dentistry 41s (2013) s35 s41 Available online at journal homepage:
 s35 s41 Available online at journal homepage:") Available online at www.sciencedirect.com journal homepage: www.intl.elsevierhealth.com/journals/jden Comparing the efficacy of a dentifrice containing 1.5% arginine and 1450 ppm fluoride to a dentifrice
Available online at www.sciencedirect.com journal homepage: www.intl.elsevierhealth.com/journals/jden Comparing the efficacy of a dentifrice containing 1.5% arginine and 1450 ppm fluoride to a dentifrice
WHY DENTAL SEALANTS MIGHT BE THE RIGHT CHOICE A GUIDE FOR YOU AND YOUR CHILDREN
 WHY DENTAL SEALANTS MIGHT BE THE RIGHT CHOICE A GUIDE FOR YOU AND YOUR CHILDREN We don t need to tell you why it is important to keep up with a healthy oral hygiene regimen for your child, mainly because
WHY DENTAL SEALANTS MIGHT BE THE RIGHT CHOICE A GUIDE FOR YOU AND YOUR CHILDREN We don t need to tell you why it is important to keep up with a healthy oral hygiene regimen for your child, mainly because
DENTAL CLINICS OF NORTH AMERICA. Emmiam. Incipient and Hidden Caries. GUEST EDITOR Daniel W. Boston, DMD. October 2005 Volume49 Number4
 DENTAL CLINICS OF NORTH AMERICA Incipient and Hidden Caries GUEST EDITOR Daniel W. Boston, DMD October 2005 Volume49 Number4 Emmiam An Imprint of Elsevier, Inc. PHILADELPHIA LONDON TORONTO MONTREAL SYDNEY
DENTAL CLINICS OF NORTH AMERICA Incipient and Hidden Caries GUEST EDITOR Daniel W. Boston, DMD October 2005 Volume49 Number4 Emmiam An Imprint of Elsevier, Inc. PHILADELPHIA LONDON TORONTO MONTREAL SYDNEY
Comparison of the Effect of Recaldent and Xylitol on the Amounts of Salivary Streptococcus Mutans
 Novelty in Biomedicine Original Article Comparison of the Effect of Recaldent and Xylitol on the Amounts of Salivary Streptococcus Mutans Shila Emamieh 1, Hossein Goudarzi 2, Alireza Akbarzadeh-Baghban
Novelty in Biomedicine Original Article Comparison of the Effect of Recaldent and Xylitol on the Amounts of Salivary Streptococcus Mutans Shila Emamieh 1, Hossein Goudarzi 2, Alireza Akbarzadeh-Baghban
Frequently Asked Questions. About Community Water Fluoridation. Overview. 1-What is fluoride?
 Frequently Asked Questions About Community Water Fluoridation Overview 1-What is fluoride? Fluoride is a naturally occurring mineral that protects teeth from tooth decay. 2-Why is fluoride added to water
Frequently Asked Questions About Community Water Fluoridation Overview 1-What is fluoride? Fluoride is a naturally occurring mineral that protects teeth from tooth decay. 2-Why is fluoride added to water
Margherita Fontana, DDS, PhD
 Chu et al., 2014 Margherita Fontana, DDS, PhD University of Michigan School of Dentistry Department of Cariology, Restorative Sciences and Endodontics mfontan@umich.edu Objectives Attendees will be able
Chu et al., 2014 Margherita Fontana, DDS, PhD University of Michigan School of Dentistry Department of Cariology, Restorative Sciences and Endodontics mfontan@umich.edu Objectives Attendees will be able
Oral Health. Links: Other articles related to this theme: Water and Natural Hazards; Water Scarcity; Water Challenges; Water for Positive Health
 Oral Health Water, Sanitation and Health Theme Article Links: Other articles related to this theme: Water and Natural Hazards; Water Scarcity; Water Challenges; Water for Positive Health Disease fact files:
Oral Health Water, Sanitation and Health Theme Article Links: Other articles related to this theme: Water and Natural Hazards; Water Scarcity; Water Challenges; Water for Positive Health Disease fact files:
TOOTH WHITENING. Why would you want your teeth whitened?
 COSMETIC DENTISTRY TOOTH WHITENING COMPOSITE FILLINGS CROWNS BRIDGES RESTORATIONS - INLAY AND ONLAY VENEERS IMPLANTS FIXED ORTHODONTIC BRACES REMOVABLE APPLIANCES TOOTH WHITENING Why would you want your
COSMETIC DENTISTRY TOOTH WHITENING COMPOSITE FILLINGS CROWNS BRIDGES RESTORATIONS - INLAY AND ONLAY VENEERS IMPLANTS FIXED ORTHODONTIC BRACES REMOVABLE APPLIANCES TOOTH WHITENING Why would you want your
Alabama Medicaid Agency. 1st Look Program
 Alabama Medicaid Agency 1st Look Program Overview 1 st Look Program goals Qualified Physicians Who qualifies for the program? Billing/Eligible Services Documentation Requirements Referrals Program Contacts
Alabama Medicaid Agency 1st Look Program Overview 1 st Look Program goals Qualified Physicians Who qualifies for the program? Billing/Eligible Services Documentation Requirements Referrals Program Contacts
Good Oral Health: The Path to Good Overall Health
 Good Oral Health: The Path to Good Overall Health Leading Age Spring Conference May 2, 2018 Carole Ferch, RDH Carol Van Aernam, RDH, BA Copyright 2018 IOWA CAREGIVERS All Rights Reserved Multi-stakeholder
Good Oral Health: The Path to Good Overall Health Leading Age Spring Conference May 2, 2018 Carole Ferch, RDH Carol Van Aernam, RDH, BA Copyright 2018 IOWA CAREGIVERS All Rights Reserved Multi-stakeholder
Policy Statement Community Oral Health Promotion: Fluoride Use (Including ADA Guidelines for the Use of Fluoride)
") Policy Statement 2.2.1 Community Oral Health Promotion: Fluoride Use (Including ADA Guidelines for the Use of Fluoride) Position Summary Water fluoridation is the safest and the most effective way to reduce
Policy Statement 2.2.1 Community Oral Health Promotion: Fluoride Use (Including ADA Guidelines for the Use of Fluoride) Position Summary Water fluoridation is the safest and the most effective way to reduce
Analysis of fluoride levels retained intraorally or ingested following routine clinical applications of topical fluoride products
 ADRF RESEARCH REPORT Australian Dental Journal 2001;46:(1):24-31 Analysis of fluoride levels retained intraorally or ingested following routine clinical applications of topical fluoride products K Heath,*
ADRF RESEARCH REPORT Australian Dental Journal 2001;46:(1):24-31 Analysis of fluoride levels retained intraorally or ingested following routine clinical applications of topical fluoride products K Heath,*