Dental materials and cements, and its use in children
|
|
|
- Willa Adams
- 5 years ago
- Views:
Transcription
1 Dental materials and cements, and its use in children
2 Study objectives Discuss amalgam restorations Discuss resin restorations Describe the history and evolution of use of silicate cement Discuss the role and importance of other cements in paediatric dentistry
3 Introduction The choice of a material to be used in a given situation in a child is usually not easy. There are a number of factors that affect the choice of material for use. These include the following:
4 Introduction Durability of material of choice: This affects the choice of the material vis a vis the length of time the tooth needs to stay in the mouth.
5 Introduction Age of the patient: This dictates cooperative ability and the length of time the material needs to stay in the mouth.
6 Introduction Caries risk: materials used in a child with high risk for caries would slightly differ from choices to be made in a child with low caries risk.
7 Introduction Techniques sensitivity of materials: one may choice to use a more forgiving material like amalgam in a less cooperative child than GIC for posterior restoration. Could GIC rather than composite as anterior restorative material in a less cooperative child.
8 Amalgam Dental amalgam is an alloy of mercury with another other metals in various composition. These are silver (69%), tin (17%), copper (13%) and zinc (1%). Long been used as restorative material for both the 1 0 and 2 0 teeth. It still remains the most commonly used material.
9 Amalgam - 2 The modern high copper amalgam alloys have better marginal integrity thereby reducing amalgam s tendency for marginal breakdown. This is because it creeps less. Also, surface corrosion is considerably reduced as gamma 2 particles are not produced. What is produced is Cu 6 Sn 5 which is also prone to corrosion but less so.
10 Setback of amalgam However the setback of amalgam continues to be lack of bond with tooth substance leading to marginal leakage and possibly secondary caries.
11 Setback of amalgam - 2 Amalgam toxicity for dental practitioners and the patient has continued to be stressed. Patient with large number of fillings may have incipient mercury leakage that could cause mercury toxicity. This reduces the interest of use of this material in patients who need large number of fillings.
12 Setback of amalgam - 3 Mercury have been demonstrated to leak into tooth structure causing discolouration; as well as into the pulp tissue.
13 Use of amalgam in children Amalgam needs a depth of at least 1.5mm to prevent its fracture. However in children, the thickness of enamel and dentine is less than that found in the permanent dentition, and the pulp horn is also high. Depth of 2mm to accommodate lining may result in pulpal exposure.
14 Use of amalgam in children - 2 In primary molars, the enamel rods are inclined occlusally. For this reason, the cavosurface margins of the cavity prepared on the primary molars should be sharp otherwise you have supported enamel.
15 Use of amalgam in children - 3 For best results, do not use amalgam in primary teeth requiring restorations on more than two surfaces. It is advisable to use cavity varnishes, and for deep cavities, cavity liners and varnishes before the placement of amalgam as this protects the exposed dentine and reduces subsequent trauma to the pulp.
16 Use of amalgam in children - 4 For best result, use dental amalgam alloys that are zinc free where moisture control may be a problem. This is because contamination with water before setting results in reaction with zinc, release of hydrogen, the pressure from released hydrogen causes amalgam flow and expansion evident a few days after insertion of restoration. This in turn, causes filling to protrude from the cavity resulting in failure.
17 Use of amalgam in children - 5 At the end of the restoration, burnish and polish the amalgam surface. You burnish to remove excess materials from the margins of the restoration. Your polishing amalgam increases resistance to corrosion and tarnish and reduces the tendency for recurrent caries and marginal failure.
18 Composite resin Composite resin are used for both anterior and posterior teeth restoration. While there are a lot of advocacy for the substitution of dental amalgam use composite, there are some peculiarities about composite that raises questions about the possibility of its routine use in primary teeth restoration.
19 Advantages of composite resin 1. Eliminates mercury in the dental environment 2. Improved appearance and aesthetics 3. Reduced thermal stimulation of the pulp 4. Colour matching potential 5. Bonds with tooth material (especially enamel) 6. Longevity (with proper technique, should last up to 10 years)
20 Idiosyncrasies with composite resin Composite is the material of choice for anterior restoration because of aesthetics. For posterior teeth, composite use should be limited to small cavities. Its use with larger cavities increases the shrinkage and possibility of marginal leakage resulting from intramaterial fracture.
21 Idiosyncrasies with composite resin - 2 Before material is inserted, the enamel margins should be etched as this increases the retention. However in primary dentition, the outer surface of the enamel is prismless and this does not respond well to etching. Retention is increased significantly if a diamond small round bur is used to remove the prismless surface and then the rest of the enamel is etched.
22 Idiosyncrasies with composite resin - 3 For the posterior teeth, because composite are not as condensable as amalgam, interproximal contacts are often open. To overcome this, the operator should prewedge the teeth before cavity preparation, and burnish the matrix band against the proximal surface of the adjacent teeth before insertion of the composite.
23 Idiosyncrasies with composite resin - 4 Use of a bonding or coupling agent increases the retention strength of composite. Postoperative sensitivity reported in permanent dentition which results from material shrinkage has not been reported in the primary dentition. Its use is difficult in class II cavities as it is difficult to etch the gingival margin of the proximal box. Thus defects at the gingival margin is common.
24 Idiosyncrasies with composite resin - 5 For posterior restoration, the use of intermediate or hybrid composite has addressed the issue of strength an occlusal wear that were problems in the past. However, there is a need to use a 45 o bevel at the cavosurface margin for good finishing.
25 Operator instructions The light cured composite have considerable handling advantage over the chemically activated form. It gives good working time. It is also more colour stable. The visible light cured resin, an advancement over the light cured composite, contains a photosensitive activator (ketones) which does not set unless activated by the ultraviolet light. Light cure also allows for incremental curing which reduces the tendency for shrinkage.
26 Operator instructions - 2 For deep cavities, apply a calcium hydroxide sublining to protect the pulp. With composite, use plastic instruments and not metal instruments to prevent changing the color of composite.
27 Disadvantages of composite resin 1. Shrinkage during polymerisation affecting marginal adaptation. 2. Pulpal protection with an appropriate liner necessary. 3. Appearance of microscopic voids which could cause recurrent caries if a rigid technique is not used.
28 Disadvantages of composite resin Possible open interproximal contacts. 5. Increased tendency to extensive abrasion of functional occlusal surfaces when used as a posterior restorative material.
29 Glass ionomer cement Glass ionomer cements are ion-leachable by aqueous polyacrylic acid. The cement powder is finely ground calcium aluminum fluorosilicate glass. The powder is combined with a solution of polyacrylic acid, maleic acid and tartaric acid. Its strength is increased with the addition of silver particles to the powder. This is known as cermet. Cermet however has low fracture toughness.
30 Uses of GIC in children dentistry Can be used a cavity liner for restorative materials like amalgam and composite. It serves as a thermal insulator. Can be used as a luting agent for orthodontic appliances, stainless steel crowns.
31 Uses of GIC in children dentistry - 2 Can be used along with composite in the restoration of deep cavities. The sandwich technique makes use of the greater bonding strength of GIC to dentine to increase the bond strength of composite. Used as fissure sealant in the management of caries. Its high viscosity limits its use as a fissure sealant.
32 Uses of GIC in children dentistry - 3 Good restorative material for class II and class III restorations in low stress-bearing areas. Can be used for indirect pulp capping in primary and permanent dentition. Can be used for direct pulp capping in the permanent dentition.
33 Uses of GIC in children dentistry - 4 It is a suitable restorative material in the primary teeth. Its survives for a period of 3 5years in the mouth with a medium survival rate of 3 years. Clinical success in primary molars shows that the GIC use should be limited to small lesions, and for teeth that will exfoliate within a year.
34 Uses of GIC in children dentistry - 5 When used in the primary teeth to restore marginal ridges, it is better to leave those restored ridges out of occlusion so as to ensure longevity. It is also important to make retention forms for GIC on the primary teeth so as to aid its retention
35 Uses of GIC in children dentistry - 6 Bulk placement of not less than 1mm is important in occlusal lesions so as to prevent fracture at the istmus, a common point of fracture because of the thin labio-lingual diameter. The fluoride leaching and fluoride absorbing properties makes its of great use as a caries prevention material.
36 Finishing GIC restorations After restoration, it is important to cover GIC with a glazing or bonding agent. This decreases the dehydration tendency that could cause creezing of the material due to shrinkage, crack formation and undue stress on the newly formed ionic exchange layer at the interphase between the material and the tooth structure. This crack is usually intra-material.
37 Finishing GIC restorations - 2 Polish after 24 hours. Where aesthetic is paramount, use sandwich technique.
38 Causes of failure of GIC restoration Dehydration. Early exposure of material to fluid. It is a technique sensitive material. Working of material into cavity after it has lost its gloss. Once gloss is loss, the tendency to bond to dentine is decreased. Easy wear when used in stress bearing areas.
39 Calcium hydroxide This is a colourless crystal or white powder prepared by reacting CaO (lime) with water through a process known as slaking. Ca(OH) 2 has a PH of 10 and thus would kill bacteria. Its beneficial effects is due to its high alkaline PH which makes it bacteriocidal. In the absence of infection, natural healing can take place.
40 Calcium hydroxide - 2 Ca(OH) 2 retains its antibacterial properties for about 2 months when placed under a restoration after which it degrades to calcium oxide and other less calcium salts eg calcium carbonate. Product has limited shelf-life.
41 Uses of calcium hydroxide Lining: when Ca(OH)2 is used as a lining, it is placed very thinly over the deepest part of cavity only.
42 Uses of calcium hydroxide - 2 Indirect pulp capping: when caries is deep such that excavation of soft dentine would result in pulpal exposure, indirect pulp is appropriate. The material is placed on the final layer of hard leathery infected dentine. The material sterilises the affected dentine and allows for formation of secondary dentine. It is important that the tooth is vital.
43 Uses of calcium hydroxide - 3 Direct pulp capping: when there is exposure of the pulp due to instrumentation NOT caries. Only done in permanent dentition. Such a tooth must not bleed spontaneously, no pain, no respond to hot and cold stimulus, no peri-radicular pathology.
44 Uses of calcium hydroxide - 4 Root dressing: can be used in inter-visit dressings of root canals especially weeping canals Root canal sealants: can be used as a canal sealant paste. This is no longer popular because it easily dissolves. Root canal filling material: for use following partial pulpectomy as this is a resorbable material Apical closure: use for apexification or apexogenesis eg hypocal
45 Limit of calcium hydroxide use a. It has poor compressive strength and thus unsuitable for use directly under amalgam. b. It does not bond to dentine and thus cannot prevent subsequent infection spreading pulpally. c. If used in conjunction with an acid-etch technique it will reduce the area available for bonding. d. Smears and contaminate the cavity when phosphoric acid is placed.
46 Mineral trioxide aggregate Mineral Trioxide Aggregate (MTA) is a mixture of a refined Portland cement and bismuth oxide Italso contains trace amounts of SiO2, CaO, MgO, K2SO4, and Na2SO4. MTA was first described for endodontic applications in the scientific literature in 1993.
47 Mineral trioxide aggregate - 2 Nowadays, there are two forms of MTA on the market, the traditional gray MTA (GMTA) and white MTA (WMTA), which was introduced in WMTA has less Al 2 O 3, MgO, and FeO and, also, smaller particles than GMTA.
48 Mineral trioxide aggregate - 3 Similar or less microleakage has been reported for MTA compared to traditional endodontic sealing materials [gutta-percha and pastes] when used as an apical restoration, furcation repair, and in the treatment of immature apices.
49 Mineral trioxide aggregate - 4 In vitro and in vivo studies support the biocompatibility of freshly mixed and set MTA when compared to other dental materials
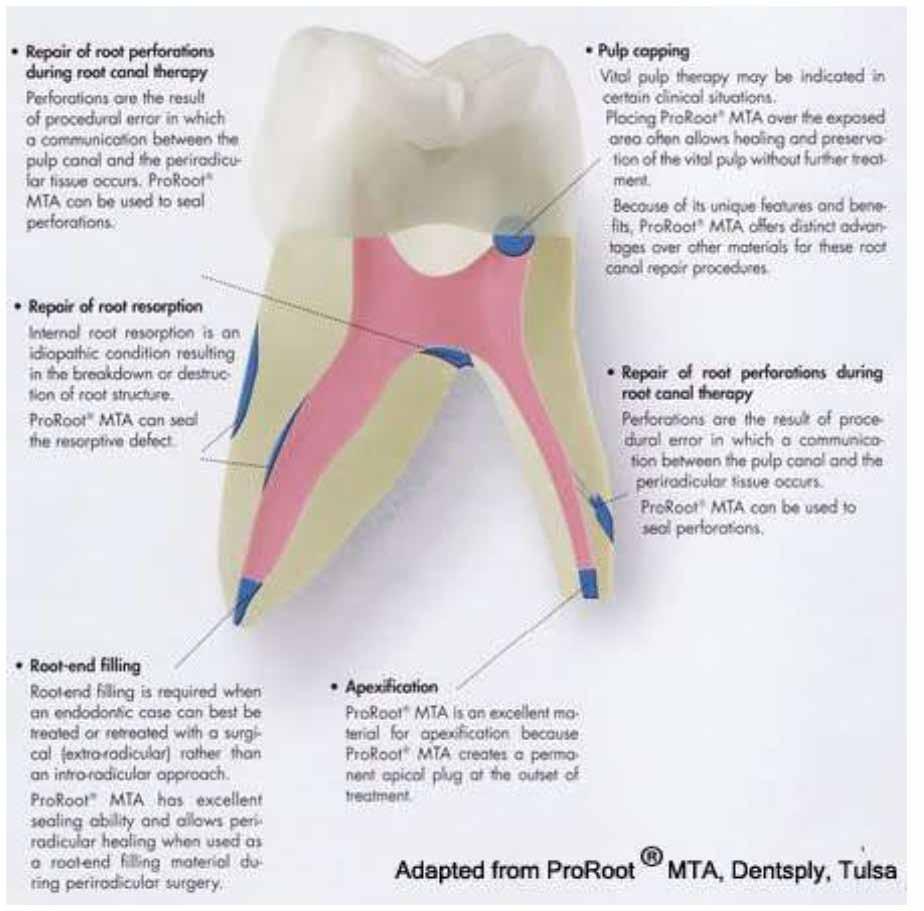
50 Uses of MTA Direct pulp capping Vital pulpotomy Root-end filling Root repair (resorption and perforations) Apexification.
51 Use of MTA for pulp capping Clinical prospective studies suggest that both GMTA and WMTA have similar results as traditional calcium hydroxide in non-carious mechanical pulp exposures in teeth with normal pulp tissue.
52 Use of MTA for pulp capping - 2 Histological analysis has suggested a more homogenous and continuous dentine bridge formation by MTA than calcium hydroxide at both 4 and 8 weeks after treatment and less inflammation associated with MTA than calcium hydroxide.
53 Use of MTA for vital pulpotomy Clinical prospective studies using MTA as pulpotomy dressings for primary and permanent teeth reported similar or better results for MTA materials compared to formocresol or calcium hydroxide with respect to the formation of dentine bridges and continued root development.
54 Use of MTA and root repair There are several case reports in which MTA has been successfully used to repair horizontal root fractures, root resorption, internal resorption, furcation perforations and apexification and/or apexogenesis which was confirmed clinically and radiographically.
55 Use of MTA and root repair - 2 3mm of MTA is recommended as the minimal amount when used as a root end filling and 5mm in apexogenesis.
56 Successes with MTA Overall results on the use of MTA in endodontics are favourable, but more well-designed and controlled clinical longitudinal studies are needed to allow systematic review and confirmation of all suggested clinical indications of MTA.
57
58 Quiz 1 Amalgam restorations in deciduous dentition: a. Appropriate depth of cavitiy is 2mm b. Bevel cavosurface margins because enamel rods are included occlusally c. Amalgam not appropriate for use in lesions with two surfaces d. Use amalgam with zinc for patients with moisture control
59 Quiz 2 Composite: a. Bond is good with deciduous molars once enamel is etched b. Important to remove outer enamel prior to etching c. Marginal leakage causes deciduous tooth sensitivity with use of material d. Zinc oxide eugenol lining appropriate for material e. Chemical cure composite more colour stable
60 Quiz 3 MTA: a. Known as Mineralised Trioxide Aggregate b. Can be used for vital pulpotomy in children c. Can be used as a root canal medicament d. Can be used for direct pulp capping e. Limited used due to associated toxicity
61 Question A six year old child comes into the clinic with multiple caries lesions. On examination, all the second deciduous molars are carious. The patient is dentally anxious. 1. Based on the four criteria for selection of dental restorative material, justify the material you will use for the final restoration for this child. 2. How may this be different if it is a second permanent molar? 3. Briefly outline your management plan for this child.
62 Reference reading material ent aterials#amalgam
63 Acknowledgement Slides were developed by Morenike Ukpong, Associate Professor in the Department of Paediatric Dentistry, Obafemi Awolowo University, Ile-Ife, Nigeria. The slides was developed and updated from multiple materials over the years. We have lost track of the various references used for the development of the slides We hereby acknowledge that many of the materials are not primary quotes of the group. We also acknowledge all those that were involved with the review of the slides.
Dental materials and cements, and its use in children
 Dental materials and cements, and its use in children Study objective Discuss the role and importance of cements in paediatric dentistry Calcium hydroxide This is a colourless crystal or white powder prepared
Dental materials and cements, and its use in children Study objective Discuss the role and importance of cements in paediatric dentistry Calcium hydroxide This is a colourless crystal or white powder prepared
Operative dentistry. Lec: 10. Zinc oxide eugenol (ZOE):
:") Operative dentistry Lec: 10 د.عبذالمنعم الخفاجي Zinc oxide eugenol (ZOE): There are 2 types: 1) Unreinforced ZOE (ordinary type): supplied as powder (zinc oxide + some additives like zinc acetate, white
Operative dentistry Lec: 10 د.عبذالمنعم الخفاجي Zinc oxide eugenol (ZOE): There are 2 types: 1) Unreinforced ZOE (ordinary type): supplied as powder (zinc oxide + some additives like zinc acetate, white
DH220 Dental Materials
 DH220 Dental Materials Lecture #5 Prof. Lamanna RDH, MS Restorative Dentistry: Glass Ionomer Bird & Robinson p.740-741 I. Use Liner Base Luting agent Restorative material: Class III, V, & eroded/abraded
DH220 Dental Materials Lecture #5 Prof. Lamanna RDH, MS Restorative Dentistry: Glass Ionomer Bird & Robinson p.740-741 I. Use Liner Base Luting agent Restorative material: Class III, V, & eroded/abraded
Pediatric endodontics. Diagnosis, Direct and Indirect pulp capping DR.SHANKAR
 Pediatric endodontics Diagnosis, Direct and Indirect pulp capping DR.SHANKAR WHY TO PRESERVE PRIMARY TEETH? The preservation of the primary dentition until their normal anticipated exfoliation can be justified
Pediatric endodontics Diagnosis, Direct and Indirect pulp capping DR.SHANKAR WHY TO PRESERVE PRIMARY TEETH? The preservation of the primary dentition until their normal anticipated exfoliation can be justified
Remaining dentin thickness Shallow cavity depth Preparation 0.5 mm into dentin (ideal depth) Moderate cavity depth Remaining dentin over pulp of at le
 Moderate cavity depth Remaining dentin over pulp of at le") Deep carious lesions management Remaining dentin thickness Shallow cavity depth Preparation 0.5 mm into dentin (ideal depth) Moderate cavity depth Remaining dentin over pulp of at least 1-2 mm Deep cavity
Deep carious lesions management Remaining dentin thickness Shallow cavity depth Preparation 0.5 mm into dentin (ideal depth) Moderate cavity depth Remaining dentin over pulp of at least 1-2 mm Deep cavity
Pulpal Protection: bases, liners, sealers, caries control Module D: Pulp capping-caries control
 Readings: Fundamentals of Operative Dentistry, 3 nd Edition; Summitt, et al Chapters 5, 6 and 8 Pulpal Protection: bases, liners, sealers, caries control Module D: Pulp capping-caries control REST 528A
Readings: Fundamentals of Operative Dentistry, 3 nd Edition; Summitt, et al Chapters 5, 6 and 8 Pulpal Protection: bases, liners, sealers, caries control Module D: Pulp capping-caries control REST 528A
Principle Investigators: Overview of Study Methods: Dr. John Burgess Dr. Carlos Muñoz
 Principle Investigators: Dr. John Burgess Dr. Carlos Muñoz Overview of Study Methods: Subjects in need of Class I and/or Class II restorations were enrolled in two clinical trials conducted in US dental
Principle Investigators: Dr. John Burgess Dr. Carlos Muñoz Overview of Study Methods: Subjects in need of Class I and/or Class II restorations were enrolled in two clinical trials conducted in US dental
RESTORATIVE MATERIALS
 Position Statement / Media Release RESTORATIVE MATERIALS Dental restorative materials are specially fabricated materials designed for use as dental restorations (fillings). Dental restorations are used
Position Statement / Media Release RESTORATIVE MATERIALS Dental restorative materials are specially fabricated materials designed for use as dental restorations (fillings). Dental restorations are used
Filling materials are used to replace missing parts of the tooth.
 Filling materials are used to replace missing parts of the tooth. 1- Dental caries. 2- Trauma. 3- Abrasion. Parts of teeth which require replacement by restorative materials vary in size of cavity, shape,
Filling materials are used to replace missing parts of the tooth. 1- Dental caries. 2- Trauma. 3- Abrasion. Parts of teeth which require replacement by restorative materials vary in size of cavity, shape,
CARIES STABILIZATION AND TEMPORARY RESTORATION
 CARIES STABILIZATION AND TEMPORARY RESTORATION LEARNING OUTCOMES Justify the importance of caries stabilisation procedure in operative care. List and discuss the methods to stabilise caries ( include preventive
CARIES STABILIZATION AND TEMPORARY RESTORATION LEARNING OUTCOMES Justify the importance of caries stabilisation procedure in operative care. List and discuss the methods to stabilise caries ( include preventive
General dentists in private practice place numerous
 PROACTIVE INTERVENTION DENTISTRY Incorporating Glass Ionomers into Everyday Dental Practice Todd Snyder, DDS, FAACD, FIADFE Introduction General dentists in private practice place numerous direct tooth
PROACTIVE INTERVENTION DENTISTRY Incorporating Glass Ionomers into Everyday Dental Practice Todd Snyder, DDS, FAACD, FIADFE Introduction General dentists in private practice place numerous direct tooth
riva helping you help your patients
 riva helping you help your patients what is a glass ionomer? how will a dentist benefit from using glass ionomers? how will a patient benefit from their glass ionomer? Glass ionomer is the generic name
riva helping you help your patients what is a glass ionomer? how will a dentist benefit from using glass ionomers? how will a patient benefit from their glass ionomer? Glass ionomer is the generic name
Primary Tooth Vital Pulp Therapy By: Aman Bhojani
 Primary Tooth Vital Pulp Therapy By: Aman Bhojani Introduction The functions of primary teeth are: mastication and function, esthetics, speech development, and maintenance of arch space for permanent teeth.
Primary Tooth Vital Pulp Therapy By: Aman Bhojani Introduction The functions of primary teeth are: mastication and function, esthetics, speech development, and maintenance of arch space for permanent teeth.
stabilisation and surface protection
 Guiding the way to caries stabilisation and surface protection Fissure sealing MI restorations Pulp capping Hypersensitivity Protection Caries stabilisation Fuji Triage from GC. Temporary restorations
Guiding the way to caries stabilisation and surface protection Fissure sealing MI restorations Pulp capping Hypersensitivity Protection Caries stabilisation Fuji Triage from GC. Temporary restorations
DPI Luting Cement. DPI Restorative Cement
 DPI Luting Cement DPI Luting Cement is Type I glass ionomer white luting cement. DPI glass ionomers are remarkably biocompatible and can be safely used in deep cavities provided the pulp is not exposed,
DPI Luting Cement DPI Luting Cement is Type I glass ionomer white luting cement. DPI glass ionomers are remarkably biocompatible and can be safely used in deep cavities provided the pulp is not exposed,
EQUIA. Self-Adhesive, Bulk Fill, Rapid Restorative System
 EQUIA EQUIA Fil EQUIA Coat + Self-Adhesive, Bulk Fill, Rapid Restorative System From the World Leader in Glass Ionomer Technology - A Complete Glass Ionomer Based Bulk Fill Rapid Restorative System Class
EQUIA EQUIA Fil EQUIA Coat + Self-Adhesive, Bulk Fill, Rapid Restorative System From the World Leader in Glass Ionomer Technology - A Complete Glass Ionomer Based Bulk Fill Rapid Restorative System Class
JMSCR Vol 4 Issue 06 Page June 2016
 www.jmscr.igmpublication.org Impact Factor 5.244 Index Copernicus Value: 5.88 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: http://dx.doi.org/10.18535/jmscr/v4i6.80 A Survey on Clinicians Choices of Restorative
www.jmscr.igmpublication.org Impact Factor 5.244 Index Copernicus Value: 5.88 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: http://dx.doi.org/10.18535/jmscr/v4i6.80 A Survey on Clinicians Choices of Restorative
Preparation and making fillings Class V., III., IV.
 Preparation and making fillings Class V., III., IV. Class V. Cervical defects - Dental caries - Non carious lesions (erosion, abrasion, V shaped defects) Types of defects Caries Erosion Abrasion V shaped
Preparation and making fillings Class V., III., IV. Class V. Cervical defects - Dental caries - Non carious lesions (erosion, abrasion, V shaped defects) Types of defects Caries Erosion Abrasion V shaped
Glass Ionomers. Reputable, Durable, Long Lasting
 Glass Ionomers Reputable, Durable, Long Lasting Conventional Glass Ionomer Restoratives Glass Ionomeres Technology more up-to-date than ever before! Successfull well proven material Exhibit biocompatibility
Glass Ionomers Reputable, Durable, Long Lasting Conventional Glass Ionomer Restoratives Glass Ionomeres Technology more up-to-date than ever before! Successfull well proven material Exhibit biocompatibility
Bonding to dentine: How it works. The future of restorative dentistry
 Bonding to dentine: How it works The future of restorative dentistry There are 82 adhesive systems on the market today! Are dentists confused about bonding? Michael Buonocore Buonocore MG. A simple method
Bonding to dentine: How it works The future of restorative dentistry There are 82 adhesive systems on the market today! Are dentists confused about bonding? Michael Buonocore Buonocore MG. A simple method
DENTAL MATERIALS STUDY GUIDE
 DENTAL MATERIALS STUDY GUIDE WORKSHEET Dentalelle Tutoring www.dentalelle.com Study Guide for Dental Materials Dentalelle Tutoring 1. When completing a large composite restoration, how should the composite
DENTAL MATERIALS STUDY GUIDE WORKSHEET Dentalelle Tutoring www.dentalelle.com Study Guide for Dental Materials Dentalelle Tutoring 1. When completing a large composite restoration, how should the composite
Direct composite restorations for large posterior cavities extended range of applications for high-performance materials
 Direct composite restorations for large posterior cavities extended range of applications for high-performance materials A case study by Ann-Christin Meier, Dr. med. dent., Stapelfeld, Germany When large
Direct composite restorations for large posterior cavities extended range of applications for high-performance materials A case study by Ann-Christin Meier, Dr. med. dent., Stapelfeld, Germany When large
MTA MIRACLE IN DENTISTRY Shikha Singh*,Rahul Maria**,AU Palekar***,Sweta Singh*.
 MTA MIRACLE IN DENTISTRY Shikha Singh*,Rahul Maria**,AU Palekar***,Sweta Singh*. Abstract MTA, is a new material developed for endodontics that appears to be a significant improvement over other materials
MTA MIRACLE IN DENTISTRY Shikha Singh*,Rahul Maria**,AU Palekar***,Sweta Singh*. Abstract MTA, is a new material developed for endodontics that appears to be a significant improvement over other materials
Part II National Board Review Operative Dentistry. Module 3D General Questions Answers in BOLD (usually the first answer)
") Part II National Board Review Operative Dentistry Module 3D General Questions Answers in BOLD (usually the first answer) Howard E. Strassler, DMD University of Maryland Dental School With special acknowledgements
Part II National Board Review Operative Dentistry Module 3D General Questions Answers in BOLD (usually the first answer) Howard E. Strassler, DMD University of Maryland Dental School With special acknowledgements
how to technique How to treat a cracked, but still inact, cusp. Disadvantages. 1 Issue Full coverage crown. >>
 Issue 37 2013 How to treat a cracked, but still inact, cusp. 1 Full coverage crown. >> Advantages. A full crown can splint all sections of the tooth together. 1 Disadvantages. 1 Encircles crown and acts
Issue 37 2013 How to treat a cracked, but still inact, cusp. 1 Full coverage crown. >> Advantages. A full crown can splint all sections of the tooth together. 1 Disadvantages. 1 Encircles crown and acts
The Dental Board of California Dental Materials Fact Sheet Adopted by the Board on October 17, 2001
 The following document is the Dental Board of California s Dental Materials Fact Sheet. The Department of Consumer Affairs has no position with respect to the language of the Dental Materials Fact Sheet;
The following document is the Dental Board of California s Dental Materials Fact Sheet. The Department of Consumer Affairs has no position with respect to the language of the Dental Materials Fact Sheet;
GUIDELINES FOR THE MANAGEMENT OF TRAUMATISED INCISORS
 GUIDELINES FOR THE MANAGEMENT OF TRAUMATISED INCISORS Dentists need to understand that the decision to remove or not reimplant an avulsed incisor must be made very carefully. The loss of such a tooth in
GUIDELINES FOR THE MANAGEMENT OF TRAUMATISED INCISORS Dentists need to understand that the decision to remove or not reimplant an avulsed incisor must be made very carefully. The loss of such a tooth in
The Facts About Fillings
 The Facts About Fillings DENTAL BOARD OF CALIFORNIA 1432 Howe Avenue Sacramento, California 95825 www.dbc.ca.gov Dental Materials Fact Sheet What About the Safety of Filling Materials? Patient health and
The Facts About Fillings DENTAL BOARD OF CALIFORNIA 1432 Howe Avenue Sacramento, California 95825 www.dbc.ca.gov Dental Materials Fact Sheet What About the Safety of Filling Materials? Patient health and
The Dental Board of California - Dental Materials Fact Sheet Adopted by the Board on October 17, 2001
 The Dental Board of California - Dental Materials Fact Sheet Adopted by the Board on October 17, 2001 As required by Chapter 801, Statutes of 1992, the Dental Board of California has prepared this fact
The Dental Board of California - Dental Materials Fact Sheet Adopted by the Board on October 17, 2001 As required by Chapter 801, Statutes of 1992, the Dental Board of California has prepared this fact
Fuji II LC. A Perfect Choice
 A Perfect Choice is a remarkable restorative material The world s first resin-reinforced glass ionomer has remained the benchmark for light cured glass ionomer cements, delivering more than 15 years of
A Perfect Choice is a remarkable restorative material The world s first resin-reinforced glass ionomer has remained the benchmark for light cured glass ionomer cements, delivering more than 15 years of
The Facts About Fillings
 Dental Board of California 2005 Evergreen Street, Suite 1550 Sacramento CA 95815 www.dbc.ca.gov Dental Materials Fact Sheet What About the Safety of Filling Materials? Patient health and the safety of
Dental Board of California 2005 Evergreen Street, Suite 1550 Sacramento CA 95815 www.dbc.ca.gov Dental Materials Fact Sheet What About the Safety of Filling Materials? Patient health and the safety of
Acknowledgments Introduction p. 1 Objectives p. 1 Goals p. 2 History of Dental Materials p. 3 The Oral Environment p. 4 Characteristics of the Ideal
 Preface p. v Acknowledgments p. vii Introduction p. 1 Objectives p. 1 Goals p. 2 History of Dental Materials p. 3 The Oral Environment p. 4 Characteristics of the Ideal Dental Material p. 5 Quality Assurance
Preface p. v Acknowledgments p. vii Introduction p. 1 Objectives p. 1 Goals p. 2 History of Dental Materials p. 3 The Oral Environment p. 4 Characteristics of the Ideal Dental Material p. 5 Quality Assurance
The Facts About Fillings
 Page 1 of 8 The Facts About Fillings DENTAL BOARD OF CALIFORNIA 1428 Howe Avenue Sacramento, California 95825 www.dbc.ca.gov Page 2 of 8 Dental Materials Fact Sheet What About the Safety of Filling Materials?
Page 1 of 8 The Facts About Fillings DENTAL BOARD OF CALIFORNIA 1428 Howe Avenue Sacramento, California 95825 www.dbc.ca.gov Page 2 of 8 Dental Materials Fact Sheet What About the Safety of Filling Materials?
Treatment Options for the Compromised Tooth
 New Edition Treatment Options for the Compromised Tooth A Decision Guide American Association of Endodontists www.aae.org/treatmentoptions TREATMENT PLANNING CONSIDERATIONS The Treatment Options for the
New Edition Treatment Options for the Compromised Tooth A Decision Guide American Association of Endodontists www.aae.org/treatmentoptions TREATMENT PLANNING CONSIDERATIONS The Treatment Options for the
Pediatrics. Biodentine. Dentin Substitute
 Pediatrics Biodentine Dentin Substitute Biodentine : Therapeutic care for your younger patients teeth (5) 1 2 Maintain pulp vitality Biodentine is bioactive and promotes the pulp s self healing capacity
Pediatrics Biodentine Dentin Substitute Biodentine : Therapeutic care for your younger patients teeth (5) 1 2 Maintain pulp vitality Biodentine is bioactive and promotes the pulp s self healing capacity
Danville Family Dentist Dental Practice of Shailaja Singh DDS
 Danville Family Dentist Dental Practice of Shailaja Singh DDS The Facts About Dental Materials DENTAL BOARD OF CALIFORNIA 1432 Howe Avenue Sacramento, California 95825 www.dbc.ca.gov Dental Materials Fact
Danville Family Dentist Dental Practice of Shailaja Singh DDS The Facts About Dental Materials DENTAL BOARD OF CALIFORNIA 1432 Howe Avenue Sacramento, California 95825 www.dbc.ca.gov Dental Materials Fact
Howard E. Strassler, DMD University of Maryland School of Dentistry
 Part II National Board Review Operative Dentistry-Biomaterials Structures, chemical properties, physical properties BASIC CONCEPTS ON HOW DENTAL MATERIALS WORK! Howard E. Strassler, DMD University of Maryland
Part II National Board Review Operative Dentistry-Biomaterials Structures, chemical properties, physical properties BASIC CONCEPTS ON HOW DENTAL MATERIALS WORK! Howard E. Strassler, DMD University of Maryland
Two Year Findings- Kalona Trial
 Medical Management of Caries Using Silver Nitrate and Fluoride Varnish Two Year Findings- Kalona Trial Michael Kanellis, DDS, MS & Arwa Owais, BDS, MS The University of Iowa College of Dentistry Background
Medical Management of Caries Using Silver Nitrate and Fluoride Varnish Two Year Findings- Kalona Trial Michael Kanellis, DDS, MS & Arwa Owais, BDS, MS The University of Iowa College of Dentistry Background
FRACTURES AND LUXATIONS OF PERMANENT TEETH
 FRACTURES AND LUXATIONS OF PERMANENT TEETH 1. Treatment guidelines and alveolar bone Followup Procedures INFRACTION Clinical findings Radiographic findings Treatment Follow-Up Favorable Outcome Unfavorable
FRACTURES AND LUXATIONS OF PERMANENT TEETH 1. Treatment guidelines and alveolar bone Followup Procedures INFRACTION Clinical findings Radiographic findings Treatment Follow-Up Favorable Outcome Unfavorable
Pulpal Protection: bases, liners, sealers, caries control Module A: Basic Concepts
 Readings: Fundamentals of Operative Dentistry, 3 nd Edition; Summitt, et al Chapters 5, 6 and 8 Pulpal Protection: bases, liners, sealers, caries control Module A: Basic Concepts REST 528A Operative #3A
Readings: Fundamentals of Operative Dentistry, 3 nd Edition; Summitt, et al Chapters 5, 6 and 8 Pulpal Protection: bases, liners, sealers, caries control Module A: Basic Concepts REST 528A Operative #3A
Essentials of. Dental Assisting. Edition 6. Debbie S. Robinson Doni L. Bird
 Essentials of Dental Assisting Edition 6 Debbie S. Robinson Doni L. Bird CHAPTER21 Restorative Procedures http://evolve.elsevier.com/robinson/essentials/ LEARNING OBJECTIVES KEY TERMS 1. Pronounce, define,
Essentials of Dental Assisting Edition 6 Debbie S. Robinson Doni L. Bird CHAPTER21 Restorative Procedures http://evolve.elsevier.com/robinson/essentials/ LEARNING OBJECTIVES KEY TERMS 1. Pronounce, define,
Practice Impact Questionnaire
 Practice Impact Questionnaire Your practitioner identifier is: XXXXXXXX It is very important that ONLY YOU complete this questionnaire because your responses will be compared to responses that you provided
Practice Impact Questionnaire Your practitioner identifier is: XXXXXXXX It is very important that ONLY YOU complete this questionnaire because your responses will be compared to responses that you provided
FIVE THINGS YOU NEED TO KNOW ABOUT GLASS IONOMERS
 FIVE THINGS YOU NEED TO KNOW ABOUT GLASS IONOMERS FIVE THINGS YOU NEED TO KNOW ABOUT GLASS IONOMERS Glass Ionomers Solve Clinicians Quandaries Amalgam fillings have been around for almost two centuries,
FIVE THINGS YOU NEED TO KNOW ABOUT GLASS IONOMERS FIVE THINGS YOU NEED TO KNOW ABOUT GLASS IONOMERS Glass Ionomers Solve Clinicians Quandaries Amalgam fillings have been around for almost two centuries,
Endodontics Cracked Tooth: How to manage it in daily practice
 Calogero Bugea Endodontics Cracked Tooth: How to manage it in daily practice 5 Feb 2016 Tooth Fractures are not rare, surface cracks, or craze lines, are relatively common in teeth. In most of cases they
Calogero Bugea Endodontics Cracked Tooth: How to manage it in daily practice 5 Feb 2016 Tooth Fractures are not rare, surface cracks, or craze lines, are relatively common in teeth. In most of cases they
Lec11 يجافخلا معنملاذبع د 0 Dental Amalgam:- Advantages:- Disadvantages:- Composition: -
 Operative dentistry Lec11 د 0 عبذالمنعم الخفاجي Dental Amalgam:-Is a union of mercury (liquid) with amalgam alloys (powder) to give a plastic mass, which, hardens in the cavity. Amalgam alloy:- Is a combination
Operative dentistry Lec11 د 0 عبذالمنعم الخفاجي Dental Amalgam:-Is a union of mercury (liquid) with amalgam alloys (powder) to give a plastic mass, which, hardens in the cavity. Amalgam alloy:- Is a combination
CONTENTS. Endodontic therapy Permanent open apex teeth Intracanal Medication. A. Introduction I. Problems II. III. IV. B. Research C.
 CONTENTS A. Introduction I. Problems II. III. IV. Endodontic therapy Permanent open apex teeth Intracanal Medication B. Research C. Conclusion INTRODUCTION A. Problems 1. In permanent teeth with open apex
CONTENTS A. Introduction I. Problems II. III. IV. Endodontic therapy Permanent open apex teeth Intracanal Medication B. Research C. Conclusion INTRODUCTION A. Problems 1. In permanent teeth with open apex
Restorative Dentistry for the Primary Dentition. References : pinkham, chapter 21
 In The Name Of God Restorative Dentistry for the Primary Dentition References : pinkham, chapter 21 INSTRUMENTATION High speed Handpiece(100,000 to 300,000 rpm) Low speed handpiece(500 to 15,000 rpm) hand
In The Name Of God Restorative Dentistry for the Primary Dentition References : pinkham, chapter 21 INSTRUMENTATION High speed Handpiece(100,000 to 300,000 rpm) Low speed handpiece(500 to 15,000 rpm) hand
dental fillings facts About the brochure:
 dental fillings facts About the brochure: Your dentist is dedicated to protecting and improving oral health while providing safe dental treatment. This fact sheet provides information you need to discuss
dental fillings facts About the brochure: Your dentist is dedicated to protecting and improving oral health while providing safe dental treatment. This fact sheet provides information you need to discuss
NON-SURGICAL ENDODONTICS
 NON-SURGICAL ENDODONTICS UnitedHealthcare Dental Coverage Guideline Guideline Number: DCG009.02 Effective Date: February 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE...1 BENEFIT CONSIDERATIONS...1
NON-SURGICAL ENDODONTICS UnitedHealthcare Dental Coverage Guideline Guideline Number: DCG009.02 Effective Date: February 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE...1 BENEFIT CONSIDERATIONS...1
2. Gap closure and replacement of the missing tooth 35 with directly modelled bridge region 34-36
 GrandTEC Test Kit Dear User, This Test Kit has been put together to enable you to test GrandTEC on the model before using it in a clinical situation. GrandTEC is a resin-impregnated glass fibre strip.
GrandTEC Test Kit Dear User, This Test Kit has been put together to enable you to test GrandTEC on the model before using it in a clinical situation. GrandTEC is a resin-impregnated glass fibre strip.
NON-SURGICAL ENDODONTICS
 NON-SURGICAL ENDODONTICS UnitedHealthcare Dental Coverage Guideline Guideline Number: DCG009.03 Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...1 BENEFIT CONSIDERATIONS...1
NON-SURGICAL ENDODONTICS UnitedHealthcare Dental Coverage Guideline Guideline Number: DCG009.03 Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...1 BENEFIT CONSIDERATIONS...1
lec: Dental material dr. Aseel Mohammed Filling material
 Filling material Filling material: the material that is used to replace a missing part of the tooth which may result from dental caries, trauma or abrasion. It can be divided in to: 1. Direct filling materials:
Filling material Filling material: the material that is used to replace a missing part of the tooth which may result from dental caries, trauma or abrasion. It can be divided in to: 1. Direct filling materials:
Dowel restorations Treatment with a post and core
 Dowel restorations Treatment with a post and core A post and core is a dental restoration used to sufficiently buildup tooth structure for future restoration with a crown when there is not enough tooth
Dowel restorations Treatment with a post and core A post and core is a dental restoration used to sufficiently buildup tooth structure for future restoration with a crown when there is not enough tooth
PROPAEDEUTICS OF CONSERVATIVE DENTISTRY
 MEDICAL UNIVERSITY VARNA FACULTY OF DENTAL MEDICINE DEPARTMENT OF CONSERVATIVE DENTISTRY AND ORAL PATHOLOGY QUESTIONNAIRE OF PROPAEDEUTICS OF CONSERVATIVE DENTISTRY Academic year 2016/2017 Questions for
MEDICAL UNIVERSITY VARNA FACULTY OF DENTAL MEDICINE DEPARTMENT OF CONSERVATIVE DENTISTRY AND ORAL PATHOLOGY QUESTIONNAIRE OF PROPAEDEUTICS OF CONSERVATIVE DENTISTRY Academic year 2016/2017 Questions for
Questions for final state exam
 Questions for final state exam 1. 1. Estetic filling in operative dentistry 2. Pulp-dentin organ, morphology and functions, pulp-periodontal complex 3. The process(es) of tooth eruption, disorders linked
Questions for final state exam 1. 1. Estetic filling in operative dentistry 2. Pulp-dentin organ, morphology and functions, pulp-periodontal complex 3. The process(es) of tooth eruption, disorders linked
If you re still using a powder-liquid liner. Like VITREBOND...
 If you re still using a powder-liquid liner 1 Like VITREBOND... FORGET ABOUT IT. Introducing GC Fuji LINING LC Paste Pak GC Fuji LINING LC Paste Pak GC Fuji LINING LC Paste Pak Radiopaque Light-Cured Glass
If you re still using a powder-liquid liner 1 Like VITREBOND... FORGET ABOUT IT. Introducing GC Fuji LINING LC Paste Pak GC Fuji LINING LC Paste Pak GC Fuji LINING LC Paste Pak Radiopaque Light-Cured Glass
ASSIGNMENT 16. Book Assignment: Operative Dentistry, pages 16-1 to 16-33
 ASSIGNMENT 16 Book Assignment: Operative Dentistry, pages 16-1 to 16-33 16-1. Operative dentistry is concerned with the prevention and treatment of defects of what tooth surfaces? 1. Enamel and cementum
ASSIGNMENT 16 Book Assignment: Operative Dentistry, pages 16-1 to 16-33 16-1. Operative dentistry is concerned with the prevention and treatment of defects of what tooth surfaces? 1. Enamel and cementum
Staywell FL Child Medicaid Plan Benefits
 The following is a complete list of dental procedures for which benefits are payable under this Plan. For beneficiaries under age 21, additional coverage may be available with documentation of medical
The following is a complete list of dental procedures for which benefits are payable under this Plan. For beneficiaries under age 21, additional coverage may be available with documentation of medical
Fee Schedule Detail Procedure Procedure Description Code Fee
 Fee Schedule Detail Procedure Procedure Description Code Fee D0120 PERIODIC ORAL EVALUATION - ESTABLISHED PATIENT $ 32.29 D0140 LIMITED ORAL EVALUATION-PROBLEM FOCUSED $ 53.02 D0150 COMPREHENSIVE ORAL
Fee Schedule Detail Procedure Procedure Description Code Fee D0120 PERIODIC ORAL EVALUATION - ESTABLISHED PATIENT $ 32.29 D0140 LIMITED ORAL EVALUATION-PROBLEM FOCUSED $ 53.02 D0150 COMPREHENSIVE ORAL
Treatment Options for the Compromised Tooth: A Decision Guide
 Treatment Options for the Compromised Tooth: A Decision Guide www.aae.org/treatmentoptions ROOT AMPUTATION, HEMISECTION, BICUSPIDIZATION Case One Hemisection of the distal root of tooth #19. 13 mo. Recall
Treatment Options for the Compromised Tooth: A Decision Guide www.aae.org/treatmentoptions ROOT AMPUTATION, HEMISECTION, BICUSPIDIZATION Case One Hemisection of the distal root of tooth #19. 13 mo. Recall
DiaDent Group International DIA.DENT DiaRoot BioAggregate. Root Canal Repair Material
 DiaDent Group International 1.877.DIA.DENT www.diadent.com DiaRoot BioAggregate Root Canal Repair Material PRECISION. PURITY. RESULTS ABOUT DIAROOT... DiaRoot BioAggregate Root Canal Repair Material is
DiaDent Group International 1.877.DIA.DENT www.diadent.com DiaRoot BioAggregate Root Canal Repair Material PRECISION. PURITY. RESULTS ABOUT DIAROOT... DiaRoot BioAggregate Root Canal Repair Material is
Management of ECC and Minimally Invasive Dentistry
 Management of ECC and Minimally Invasive Dentistry Ranbir Singh DMD MPH NYU-Lutheran Phoenix Pgy1 Pediatric Dental Resident Phoenix ECC Management Management of dental caries includes identification of
Management of ECC and Minimally Invasive Dentistry Ranbir Singh DMD MPH NYU-Lutheran Phoenix Pgy1 Pediatric Dental Resident Phoenix ECC Management Management of dental caries includes identification of
أ.م. هدى عباس عبد اهلل CROWN AND BRIDGE جامعة تكريت كلية. Lec. (2) طب االسنان
 طب االسنان") Lec. (2) CROWN AND BRIDGE أ.م. هدى عباس عبد اهلل Patient selection and examination A thorough diagnosis must first be made of the patient's dental condition, considering both hard and soft tissues. this
Lec. (2) CROWN AND BRIDGE أ.م. هدى عباس عبد اهلل Patient selection and examination A thorough diagnosis must first be made of the patient's dental condition, considering both hard and soft tissues. this
MDG Dental Plan Comparison
 D0999 Office visit during regular hours, general dentist only Evaluations D0120 Periodic oral examination - established patient D0140 Limited oral evaluation - problem focused D0145 Oral evaluation for
D0999 Office visit during regular hours, general dentist only Evaluations D0120 Periodic oral examination - established patient D0140 Limited oral evaluation - problem focused D0145 Oral evaluation for
Restoring Deep Cavity Preparations
 Restoring Deep Cavity Preparations Townies share techniques and discuss restoring posterior teeth with composites Dentaltown.com > Message Boards > Cosmetic Dentistry > Restoring Deep Cavity Preparations
Restoring Deep Cavity Preparations Townies share techniques and discuss restoring posterior teeth with composites Dentaltown.com > Message Boards > Cosmetic Dentistry > Restoring Deep Cavity Preparations
SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental SCHEDULE OF BENEFITS
 SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental SCHEDULE OF BENEFITS COST-SHARING PEDIATRIC DENTAL CARE ESSENTIAL HEALTH BENEFIT Deductible One (1) Member under age 19 Two (2) or more Members
SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental SCHEDULE OF BENEFITS COST-SHARING PEDIATRIC DENTAL CARE ESSENTIAL HEALTH BENEFIT Deductible One (1) Member under age 19 Two (2) or more Members
MTA PULPOTOMY ASSOCIATED APEXOGENESIS OF HUMAN PERMANENT MOLAR WITH IRREVERSIBLE PULPITIS: A CASE REPORT
 Case Report International Journal of Dental and Health Sciences Volume 02, Issue 05 MTA PULPOTOMY ASSOCIATED APEXOGENESIS OF HUMAN PERMANENT MOLAR WITH IRREVERSIBLE PULPITIS: A CASE REPORT Nabi Shahnaz
Case Report International Journal of Dental and Health Sciences Volume 02, Issue 05 MTA PULPOTOMY ASSOCIATED APEXOGENESIS OF HUMAN PERMANENT MOLAR WITH IRREVERSIBLE PULPITIS: A CASE REPORT Nabi Shahnaz
Polymers in everyday things dentistry
 HOTOCOY olymers in everyday things dentistry (Background information) olymers are a part of everyday life and examples can be found almost anywhere. Many people think of polymers simply as plastics used
HOTOCOY olymers in everyday things dentistry (Background information) olymers are a part of everyday life and examples can be found almost anywhere. Many people think of polymers simply as plastics used
Dental material for filling the root canals "AUREOSEAL M.T.A."
 Dental material for filling the root canals "AUREOSEAL M.T.A." Highly biocompatible root canal cement without eugenol. 1. Composition: Powder: Mineral-trioxide-agregat (М.Т.А.) based on Portland cement,
Dental material for filling the root canals "AUREOSEAL M.T.A." Highly biocompatible root canal cement without eugenol. 1. Composition: Powder: Mineral-trioxide-agregat (М.Т.А.) based on Portland cement,
CLASS II AMALGAM RESTORATION 36MO
 INTERNATIONAL PEER REVIEW CLASS II AMALGAM RESTORATION 36MO Leung Kwan Yu, Steve BDS II - Class 2019, The University of Hong Kong instruments Mirror Periodontal probe Hatchets Gingival margin trimmers
INTERNATIONAL PEER REVIEW CLASS II AMALGAM RESTORATION 36MO Leung Kwan Yu, Steve BDS II - Class 2019, The University of Hong Kong instruments Mirror Periodontal probe Hatchets Gingival margin trimmers
Indications The selection of amalgam as a restorative material for class V cavity should involve the following considerations:
 1 Lec.7 د.عبد املنعم اخلفاجي CLASS V CAVITY PREPARATION FOR AMAGLAM Indications The selection of amalgam as a restorative material for class V cavity should involve the following considerations: 1- Caries:
1 Lec.7 د.عبد املنعم اخلفاجي CLASS V CAVITY PREPARATION FOR AMAGLAM Indications The selection of amalgam as a restorative material for class V cavity should involve the following considerations: 1- Caries:
Journal of Dental & Oro-facial Research Vol. 14 Issue 01 Jan. 2018
 Journal of Dental & Oro-facial Research Vol. 14 Issue 01 Jan. 2018 Management of Non-Vital Teeth with Open Apices using MTA: Two Case Reports *Karan Narang 1, Mohini Nayak 2, Abdul Wahed, 3 John V. George
Journal of Dental & Oro-facial Research Vol. 14 Issue 01 Jan. 2018 Management of Non-Vital Teeth with Open Apices using MTA: Two Case Reports *Karan Narang 1, Mohini Nayak 2, Abdul Wahed, 3 John V. George
how to technique Issue How to improve the longevity of porcelain veneers.
 Issue 4 2013 How to improve the longevity of porcelain veneers. 1. Avoid finishing on a resin composite restoration. longer term weak spot Although tempting in the interests of minimal tooth removal, finishing
Issue 4 2013 How to improve the longevity of porcelain veneers. 1. Avoid finishing on a resin composite restoration. longer term weak spot Although tempting in the interests of minimal tooth removal, finishing
21 NCAC 16G.0101 FUNCTIONS THAT MAY BE DELEGATED
 1 1 1 1 1 1 1 1 0 1 0 1 1 NCAC 1G.01is proposed for amendment as follows: 1 NCAC 1G.01 FUNCTIONS THAT MAY BE DELEGATED A dental hygienist may be delegated functions to be performed under the control and
1 1 1 1 1 1 1 1 0 1 0 1 1 NCAC 1G.01is proposed for amendment as follows: 1 NCAC 1G.01 FUNCTIONS THAT MAY BE DELEGATED A dental hygienist may be delegated functions to be performed under the control and
Stainless Steel Crowns
 Stainless Steel Crowns Objectives Indications for use of stainless steel crowns Technique used in preparing and placing a stainless steel crown restoration on a primary molar. Indications for SSC Restoration
Stainless Steel Crowns Objectives Indications for use of stainless steel crowns Technique used in preparing and placing a stainless steel crown restoration on a primary molar. Indications for SSC Restoration
Ceramic Based Aesthetic CAD/CAM Restorative
 Ceramic Based Aesthetic CAD/CAM Restorative Create Natural Aesthetics with High-Strength Materials SHOFU Block HC and Disk HC are the latest generation of hybrid-ceramic restorative materials for use with
Ceramic Based Aesthetic CAD/CAM Restorative Create Natural Aesthetics with High-Strength Materials SHOFU Block HC and Disk HC are the latest generation of hybrid-ceramic restorative materials for use with
SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental Schedule of Benefits
 COST-SHARING SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental Schedule of Benefits Members can search for a Network Provider at www.solsticecare.com/provider-search.aspx Member Services:
COST-SHARING SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental Schedule of Benefits Members can search for a Network Provider at www.solsticecare.com/provider-search.aspx Member Services:
Peninsula Dental Social Enterprise (PDSE)
") Peninsula Dental Social Enterprise (PDSE) Paediatric Pathway - Restorative Version 2.0 Date approved: May 2018 Approved by: The Board Review due: May 2020 Page 1 of 7 Routine assessment: Clinical Examination
Peninsula Dental Social Enterprise (PDSE) Paediatric Pathway - Restorative Version 2.0 Date approved: May 2018 Approved by: The Board Review due: May 2020 Page 1 of 7 Routine assessment: Clinical Examination
For the Perfect Class V and All Cervical Area Gingival Margins when Placing Direct Composites, Create an Injection Molding Matrix
 Cronicon OPEN ACCESS EC DENTAL SCIENCE Case Report For the Perfect Class V and All Cervical Area Gingival Margins when Placing Direct Composites, Create an Injection Molding Paul C Belvedere* Adjunct Professor,
Cronicon OPEN ACCESS EC DENTAL SCIENCE Case Report For the Perfect Class V and All Cervical Area Gingival Margins when Placing Direct Composites, Create an Injection Molding Paul C Belvedere* Adjunct Professor,
INDIANA HEALTH COVERAGE PROGRAMS
 INDIANA HEALTH COVERAGE PROGRAMS PROVIDER CODE TABLES Note: Due to possible changes in Indiana Health Coverage Programs (IHCP) policy or national coding updates, inclusion of a code on the code tables
INDIANA HEALTH COVERAGE PROGRAMS PROVIDER CODE TABLES Note: Due to possible changes in Indiana Health Coverage Programs (IHCP) policy or national coding updates, inclusion of a code on the code tables
Polycarbonate Crowns for Primary teeth Revisited. Restorative options, Technique & Case reports
 Polycarbonate Crowns for Primary teeth Revisited Restorative options, Technique & Case reports Karthik Venkataraghavan 1, John Chan 2 1 Pediatric Dentist, Vibha Dental Care Centre, Bangalore, India. 2
Polycarbonate Crowns for Primary teeth Revisited Restorative options, Technique & Case reports Karthik Venkataraghavan 1, John Chan 2 1 Pediatric Dentist, Vibha Dental Care Centre, Bangalore, India. 2
Clinical report. Drs Paul and Alexandre MIARA and F. CONNOLLY COMPOSITE POSTERIOR FILLINGS. How to control. layering? 8 - Dentoscope n 124
 COMPOSITE POSTERIOR FILLINGS How to control layering? 8 - Dentoscope n 124 CV FLASH Dr Paul MIARA Dental surgeon Dr Alexandre MIARA Dental surgeon Dr F. CONNOLLY Dental surgeon Thanks to continuous improvements
COMPOSITE POSTERIOR FILLINGS How to control layering? 8 - Dentoscope n 124 CV FLASH Dr Paul MIARA Dental surgeon Dr Alexandre MIARA Dental surgeon Dr F. CONNOLLY Dental surgeon Thanks to continuous improvements
Practical vital pulp treatment: MTA or calcium hydroxide?
 Practical vital pulp treatment: MTA or calcium hydroxide? Hal Duncan, Division of Restorative Dentistry and Periodontology, Dublin Dental University Hospital, Trinity College Dublin, Ireland NVvE Voorjaarscongres,
Practical vital pulp treatment: MTA or calcium hydroxide? Hal Duncan, Division of Restorative Dentistry and Periodontology, Dublin Dental University Hospital, Trinity College Dublin, Ireland NVvE Voorjaarscongres,
Clinical UM Guideline
 Clinical UM Guideline Subject: Endodontic Therapy Guideline #: 03-001 Current Effective Date: 03/24/2017 Status: New Last Review Date: 02/08/2017 Description This document addresses the procedure of endodontic
Clinical UM Guideline Subject: Endodontic Therapy Guideline #: 03-001 Current Effective Date: 03/24/2017 Status: New Last Review Date: 02/08/2017 Description This document addresses the procedure of endodontic
Restoration of the worn dentition
 Clin Dent Rev (2017) 1:4 https://doi.org/10.1007/s41894-017-0003-3 TREATMENT Restoration of the worn dentition Paul King 1 Received: 16 March 2017 / Accepted: 31 May 2017 / Published online: 30 June 2017
Clin Dent Rev (2017) 1:4 https://doi.org/10.1007/s41894-017-0003-3 TREATMENT Restoration of the worn dentition Paul King 1 Received: 16 March 2017 / Accepted: 31 May 2017 / Published online: 30 June 2017
Get in front of the 8 ball with the new Fuji VIII GP. The first auto-cure, resin reinforced glass ionomer restorative
 Get in front of the 8 ball with the new Fuji VIII GP The first auto-cure, resin reinforced glass ionomer restorative 8 reasons to choose Fuji VIII GP Auto-cure, resin reinforced glass ionomer restorative
Get in front of the 8 ball with the new Fuji VIII GP The first auto-cure, resin reinforced glass ionomer restorative 8 reasons to choose Fuji VIII GP Auto-cure, resin reinforced glass ionomer restorative
Ketac Universal Aplicap
 Ketac Universal Aplicap Technical Data Sheet 2 Introduction Ketac Universal Aplicap is the latest development in a long history of proven glass ionomer technology from 3M. It s designed to save steps for
Ketac Universal Aplicap Technical Data Sheet 2 Introduction Ketac Universal Aplicap is the latest development in a long history of proven glass ionomer technology from 3M. It s designed to save steps for
Educational Training Document
 Educational Training Document Table of Contents Part 1: Resource Document Disclaimer Page: 2 Part 2: Line Item Grade Sheets Page: 3 Release: 11/2016 Page 1 of 6 Part 1: Resource Document Disclaimer The
Educational Training Document Table of Contents Part 1: Resource Document Disclaimer Page: 2 Part 2: Line Item Grade Sheets Page: 3 Release: 11/2016 Page 1 of 6 Part 1: Resource Document Disclaimer The
Newport News Public Schools Summary Schedule of Services Delta Dental PPO EPO Plan
 Newport News Public Schools Summary of Services Delta Dental PPO EPO Plan Services In-Network Out-of-Network PPO Premier All Other Diagnostic & Preventive Oral Exams & Teeth Cleanings Fluoride Applications
Newport News Public Schools Summary of Services Delta Dental PPO EPO Plan Services In-Network Out-of-Network PPO Premier All Other Diagnostic & Preventive Oral Exams & Teeth Cleanings Fluoride Applications
New Nano-Hybrid Technology for your everyday Use
 New Nano-Hybrid Technology for your everyday Use NEW New NANO-HYBRID TECHNOLOGY For Your every Day USE You need a composite that allows you to easily achieve high quality restorations? Polofil NHT, the
New Nano-Hybrid Technology for your everyday Use NEW New NANO-HYBRID TECHNOLOGY For Your every Day USE You need a composite that allows you to easily achieve high quality restorations? Polofil NHT, the
values is of great interest.
 User Report Dr. Ralph Schönemann, May 21, 2008 There are numerous self-etchbonding systems on the market that sometimes differ very much from one another with regards to their chemical composition. It
User Report Dr. Ralph Schönemann, May 21, 2008 There are numerous self-etchbonding systems on the market that sometimes differ very much from one another with regards to their chemical composition. It
Jordi Manauta. Shadeguides Composite onlays. Page 1 of Apr 2012
 Jordi Manauta Shadeguides Composite onlays 25 Apr 2012 Indirect composite restorations in posterior teeth give us advantages to enhance the quality, durability and supreme aesthetics. An Article byâ Jordi
Jordi Manauta Shadeguides Composite onlays 25 Apr 2012 Indirect composite restorations in posterior teeth give us advantages to enhance the quality, durability and supreme aesthetics. An Article byâ Jordi
Continually Fluoride Releasing Aesthetic Dental Restorative Material
 Continually Fluoride Releasing Aesthetic Dental Restorative Material Research is our best product Image provided by Dr. Sushil Koirala BEAUTIFIL II More than just filling BEAUTIFIL II stands out for its
Continually Fluoride Releasing Aesthetic Dental Restorative Material Research is our best product Image provided by Dr. Sushil Koirala BEAUTIFIL II More than just filling BEAUTIFIL II stands out for its
Here are some frequently asked questions about Endodontic treatment:
 Here are some frequently asked questions about Endodontic treatment: What is an "Endodontist"? Endodontists are dentists who specialize in treating the soft inner tissue of your tooth's roots. After they
Here are some frequently asked questions about Endodontic treatment: What is an "Endodontist"? Endodontists are dentists who specialize in treating the soft inner tissue of your tooth's roots. After they
LOUISIANA MEDICAID PROGRAM ISSUED: 08/18/14 REPLACED: 09/15/13 CHAPTER 16: DENTAL SERVICES APPENDIX A: EPSDT DENTAL PROGRAM FEE SCHEDULE PAGE(S) 16
 16") APPENDIX A: FEE SCHEDULE DENTAL PROGRAM FEE SCHEDULE Provided in the table on the following pages are the reimbursable dental procedure codes and fees for the Medicaid of Louisiana, EPSDT Dental Program.
APPENDIX A: FEE SCHEDULE DENTAL PROGRAM FEE SCHEDULE Provided in the table on the following pages are the reimbursable dental procedure codes and fees for the Medicaid of Louisiana, EPSDT Dental Program.
DELTA DENTAL PPO EPO PLAN DESIGN CP070
 DELTA DENTAL PPO EPO PLAN DESIGN CP070 SCHEDULE OF BENEFITS AND The benefits shown below are performed as deemed appropriate by the attending Dentist subject to the limitations and exclusions of the program.
DELTA DENTAL PPO EPO PLAN DESIGN CP070 SCHEDULE OF BENEFITS AND The benefits shown below are performed as deemed appropriate by the attending Dentist subject to the limitations and exclusions of the program.
RESTORING ENDODONTICALLY TREATED TEETH POST RESTORATIONS CROWNS. Dr. Szabó Enikő associate professor
 RESTORING ENDODONTICALLY TREATED TEETH POST RESTORATIONS CROWNS Dr. Szabó Enikő associate professor Why is the risk of fracture greater? loss of tooth structure large caries trepanation cavity access to
RESTORING ENDODONTICALLY TREATED TEETH POST RESTORATIONS CROWNS Dr. Szabó Enikő associate professor Why is the risk of fracture greater? loss of tooth structure large caries trepanation cavity access to
LOUISIANA MEDICAID PROGRAM ISSUED: 09/15/13 REPLACED: 03/28/13 CHAPTER 16: DENTAL SERVICES APPENDIX A: EPSDT DENTAL PROGRAM FEE SCHEDULE PAGE(S) 16
 16") APPENDIX A: FEE SCHEDULE DENTAL PROGRAM FEE SCHEDULE Provided in the table on the following pages are the reimbursable dental procedure codes and fees for the Medicaid of Louisiana, EPSDT Dental Program.
APPENDIX A: FEE SCHEDULE DENTAL PROGRAM FEE SCHEDULE Provided in the table on the following pages are the reimbursable dental procedure codes and fees for the Medicaid of Louisiana, EPSDT Dental Program.