Dr. Jahnavi Kedare Associate Professor Dept. of Psychiatry, T. N. Medical College B. Y. L. Nair Hospital, Mumbai.
|
|
|
- Stanley Carter
- 5 years ago
- Views:
Transcription

1 Dr. Jahnavi Kedare Associate Professor Dept. of Psychiatry, T. N. Medical College B. Y. L. Nair Hospital, Mumbai.
2 A 60 year old male patient came to the opd with h/o loss of interest in pleasurable activities Sadness of mood, h/o helplessness, hopelessness and worthlessness Following retirement 3-4 months ago. h/o financial stressors following daughter s wedding h/o 3 previous episodes of similar nature in the last 20 years Family h/o depression in father.
3 Diagnosis- Major depressive disorder, intermittent major depressive episodes with current episode depression Treated with T. Sertraline each time with good recovery.

4 A 65 year old male patient comes with h/o lack of sleep, loss of appetite, weight loss since 3-4 months. h/o forgetfulness since 2 months h/o social withdrawal, psychomotor retardation since 2 months h/o financial stressors following daughter s marriage On enquiry, h/o sadness of mood, helplessness, hopelessness, worthlessness Crying spells Easy fatigability No past or family h/o depression
5 Diagnosis- Major depressive disorder Treated with T. Mirtazapine 30 mg. After 3months of treatment 50% recovery.
6 What is the difference between these two patients? Young/early onset Vs. Late onset. Late onset depression or late-life depression is defined as an episode of clinical depression occurring after the age of 60 in an individual who previously had never experienced clinical depression. What are the differences? Why are the differences?
7 Clinically distinct Etiologically different Comorbidity- medical and psychological Risk factors Protective factors Treatment response Depression to dementia
8 an increased chance of experiencing thinking and memory problems (often more pronounced than feelings of sadness) a greater likelihood of experiencing higher rates of fatigue and agitation. an increased likelihood of a concurrent medical illness. more likely to have vascular risk factors including history of cerebrovascular disease
9 more likely to have concomitant cognitive deficits, especially executive functioning, Structural changes in the brain more likely to develop dementia subsequently in early onset depression an increased chance of a family history of mood disorders Early onset associated with personality disorders or traits like neuroticism
10 it is treatable, 40 and 60% show sustained recovery with standard treatment, 15 20%of cases may relapse, Remaining 20-35% do not recover as well following treatment. LLD is untreated very often because, a) older adults do not mention depressive symptoms to their physician, or do not recognize the signs of depression in themselves, b) the health professional does not recognise the depressive symptoms, mistaking them as symptoms of medical illness or side effect of medication.

11 In old age, major depressive disorder and clinically significant depressive symptoms. The prevalence of major depressive disorder ranges from 1-5% in most large-scale epidemiological studies. Clinically significant depressive symptoms are present in approximately 15% of community-dwelling older adults. Indian studies: Community-based studies involving 70 to 7,150 elderly subjects report prevalence rate varying from 8.9% to 62.16%. Clinic-based studies involving 50 to 5,260 participants report prevalence rates ranging from 42.4% to 72%. Significant decline in Prevalence of major depression as compared to midlife, however an increase in clinically significant depressive symptoms among older adults than in midlife.
12 LLD is associated with increased risk of morbidity, increased risk of suicide, decreased physical, cognitive and social functioning, and greater self-neglect, and hence an increased mortality. cognitive-affective symptoms of depression, including dysphoria and worthlessness/guilt are reported less often. Sleep disturbance, fatigue, psychomotor retardation, loss of interest and hopelessness more prevalent. Subjective complaints of poor memory and concentration Slower cognitive processing speed and executive dysfunction are frequent findings.
13 In contrast to depressive disorders in younger adults, LLD is associated with cerebrovascular comorbidities and microvascular lesions. Represented in particular by white matter hyperintensities (WMHs) on structural magnetic resonance imaging (MRI), subcortical lacunes, microinfarcts and microbleeds, also frontal and temporal (hippocampal) gray matter changes/atrophy, neurodegenerative pathologies, and related biochemical changes.
14 Old concept of atherosclerotic depression More recent term of vascular depression (VaDep). VaDep hypothesis, by Alexopoulos, In 1997 :Cerebrovascular disease (CVD), including small vessel ischemic changes, structural damage to frontal subcortical circuits, with disruption of cortico striato pallido thalamo cortical pathways. may predispose, precipitate, or perpetuate some geriatric depressive symptoms.
15 Newer MRI based studies : VaDep accounts for up to 50 % of MDD cases in the elderly. MRI-defined VaDep, Krishnan et al, by definition includes CVD findings on MRI. Patients with VaDep : a distinct clinical and neuropsychological profile and a positive association with hypertension. The MRI literature supporting the VaDep hypothesis shows that loss of brain volume and white matter integrity are associated with poor clinical treatment outcomes.
16 based on adequate criteria, such as: (1) Evidence of vascular pathology in elderly subjects with or without cognitive impairment. (2) Absence of previous depressive episodes preceding obvious cerebrovascular disease. (3) Presence of cerebrovascular risk factors. (4) Co-incidence of depression with cerebrovascular risk factors. (5) Clinical symptoms characteristic of VaDep such as executive dysfunction, decrease in processing speed, and lethargy. (6) Neuroimaging data confirming CVD.
17 VaDap when associated with greater disability, poorer outcomes and executive dysfunction- Depression executive dysfunction syndrome / Depression-cognitive impairment disease Cognitive impairment- Verbal fluency, naming and initiation/ perseveration Psychomotor retardation, anhedonia Less severe vegetative symptoms, agitation, guilt.

18
19
20 Depression of Alzheimer disease is diagnosed in the presence of three or more symptoms of major depression, not including difficulty concentrating, but including additional nonsomatic symptoms such as irritability and social withdrawal. Individuals with VaDep are at greater risk to develop cognitive impairment, more likely related to vascular dementia than to Alzheimer s disease (AD). Recent data showed that VaDep is not a risk factor for AD. Cognitively unimpaired patients with depressive episodes may have more underlying AD pathology, in particular β-amyloid deposition.
21 specific syndrome, depression of Parkinson's disease, recommends an inclusive approach in which all symptoms are counted towards a diagnosis of major depression even if they overlap with PD symptoms (Marsh et al., 2006).

22 Biological vulnerabilities including genetic vulnerability. Age associated and medical illness associated neurobiological changes. Stressful life events including bereavement reduced engagement with the environment including taking up meaningful activities and roles.
23 Genetic risk: twin studies e.g. Swedish twin registry- heritability more in younger onset depression, genes- polymorphism in 5HT transporter gene associated with depressed mood, APOE4 carriers having poorer cognitive performance, DCP1 MTHRF affecting lipid metabolism and homocysteine levels Other biological factors: include endocrine, inflammatory or immune, cardiovascular, and neuroanatomical factors. Endocrine dys-regulation: diabetes? Cause or effect? DIABETES Prevalence estimates for depression in patients with Type II diabetes are as high as 15% for major depression and approximately 20% for elevated depressive symptoms. Evidence appears to be stronger for depression as a risk factor for diabetes than the reverse. Depression associated with hypo and hyperthyroidism
24 Late life depression is also associated with bone loss; this may be due to the role of inflammatory markers in both conditions (Alexopoulos, 2005). A number of biological variables such as increased adrenocortical activity, elevated insulin growth factor-1, and inflammatory markers, associated both with accelerated aging on the cellular level and with depression in later life (Alexopoulos, 2005). Inflammatory risk factors are associated with appetite and sleep disturbance, loss of energy, concentration disturbance, and thoughts of death. Minor depression appears more closely related to inflammatory risk factors than to vascular or degenerative changes Medications as a cause of depression: Certain medications (such as beta blockers, CNS medications,, calcium channel blockers, digitalis, corticosteroids, hormones, anti-parkinson agents, respiratory or gastrointestinal medications, certain cancer medications, benzodiazepines and interferon) (Alexopoulos, 2005; Djernes, 2006.) Diastolic hypotension is associated with low positive affect, which may explain why depression can be a side effect of certain anti- hypertensive drugs such as betablockers (Blazer, 2003).
25 Conditions believed to be most strongly associated with depression include cardiac and cerebrovascular disease and neurological conditions. Depression may be the consequence of vascular disease. Depression appears independently from vascular disease, but vascular brain disease may stimulate the development and course of depression. Cerebrovascular pathology and depression may appear without obvious connection as two manifestations of the same genetic predisposition and pathobiological mechanisms. Depression may cause cardiovascular and/or cerebrovascular disease and there may be a bidirectional relationship between depression and vascular disease. Cardiovascular disorders- Consequences of depression in heart disease patients include rehospitalization, slower recovery, disability, mortality, and increased health care costs.
26 OTHER NEUROLOGICAL DISORDERS Rates of major depression are highest among stroke patients (20-25%; Park et al., 2007) and intermediate among those with PD (15-20%; Reijnders, Ehrt, Weber, Aarsland, & Leentjens, 2008), compared to 10-15% among those with AD (Park et al., 2007). Co-morbid depression is associated with functional impairment symptoms appear to be a risk factor for incident stroke (Wouts et al., 2008) and PD (Ishiara & Brayne, 2006).
27 Major depression with cognitive impairment- Pseudodementia, Reversible dementia Major depression with cognitive impairment 40% develope dementia within 3-5 years. Is depression a precursor of dementia? Depression can be both an early or midlife risk factor for dementia and also an early sign of incipient dementia. Both dementia and depression resulting from the same neuropathological changes. Dementia itself can lead to depression due to psychological reaction to the cognitive and behavioral changes of dementia.
28 anxiety typically precedes depression suggesting that anxiety disorders may be a risk factor for late life depression. insomnia is a risk factor for both onset and persistence of depression.
29 High scores on personality scales measuring neuroticism are strongly related to depression ruminative coping style and avoidant coping style has been associated with depression. Stressful life events Stressful life events- financial difficulties, bereavement, new interpersonal conflict. Cognitive style also influences a person's response to stressful events.
30 A meta-analysis of prospective studies of depressive symptoms and disorders in adults aged 50 or older found that bereavement more than tripled the risk of depression, with the largest effect size of any risk factors examined (Cole & Dendukuri, 2003). PROBLEMS WITH SOCIAL SUPPORT Deficits in social support, negative aspects of the social network, and even excessive amounts of support have been studied as risk factors for depression in late life,. quality not quantity, of social support is important in the development of depression. Deterioration in financial status leads to persistent depressive symptoms, Socioeconomic disadvantage early in life may increase vulnerability to depression throughout the lifespan through the effects of poor nutrition, reduced opportunities for education, less access to health care, or other mechanisms.
31 Importance of resources health, cognitive function, socioeconomic status. use of social support to manage their health-related stresses. Role of meaningful engagement, whether in social activities, volunteer work, or religion. Improvements in emotion regulation with age. Older adults are less reactive to stressors, particularly those of an interpersonal nature, than are younger adults. Have less negative affect and demonstrated less reactivity to daily stressors than younger adults. Cognitive strategy of positive reappraisal. Focus on positive and emotionally meaningful experiences
32 Factors associated with resiliency in late life include a positive self- concept, a sense of mastery or self-efficacy. sense of control and self-esteem. Perceived social support buffers the effect of stressful events in older adults Religious involvement. Factors thought to buffer the effects of biological vulnerability to depression in late life : physical exercise, stress reduction strategies, and hormone replacement therapy. Efforts to promote vascular health

33
34 78 year old widowed male patient History of stoke 3 months ago Not doing physiotherapy since 2 months Crying spells Refusing to get up from bed Not taking self care Relatives C/O memory problems History of hypertension and DM since 20 years Living in a joint family Running a business till 3 months ago
35 Risk factors History of hypertension Stroke Age DM Widowed Protective factors Joint family Working till 3 months ago

36 Suicidal behaviour in late life differs in several ways from that observed earlier in the lifespan. More lethal means, Suicidal behaviour is fatal. Higher level of intent and detailed planning Less likely to verbalize suicidal thoughts Higher rates of death ideation, like pervasive wish to die They visit a physician shortly before death.
37 Depression in 85% of suicides. Physical illnesses, including cancer, seizure disorder, chronic pulmonary disorder, renal failure, vision or hearing impairment, and even incontinence. Personality traits: High scores on neurotocism and low scores on openness to experience In rigid personalitiies Alcohol abuse Long term placement in nursing home
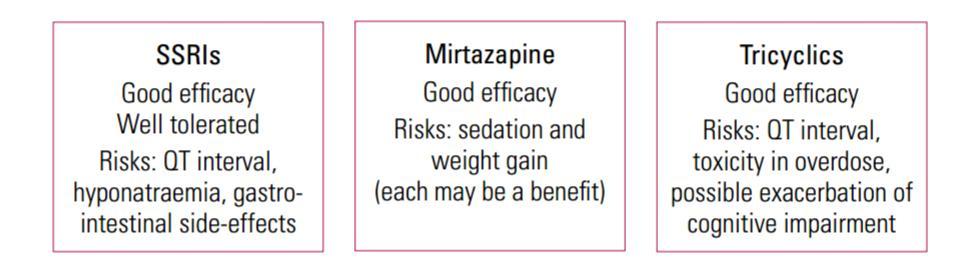
38 Treatment for late-life depression requires a distinct approach because of age-related physiological changes, which alter pharmacokinetics and pharmacodynamics. Drug distribution within the body changes as a result of increased body fat and reduced volume of water. Renal excretion is reduced, so there may be increased concentrations of active compounds that are renally excreted. Lower doses, slow titration and careful monitoring. The increased prevalence of comorbid medical conditions in this age group means that patients are more vulnerable to medication side-effects. Polypharmacy is a risk, and care is needed to minimise the effects of drug interactions
39
40
41 Electroconvulsive therapy (ECT), an evidence-based treatment alternative for depression. Treatment efficacy is impressive, with improvement seen in more than 80% of patients in most trials. Adverse events such as cardiac complications, memory loss, and delirium, ECT is the oldest, most studied and most effective treatment for TRLLD with remission rates around 60 %. Recent studies in ECT for LLD focus on speed of remission in non-trd patients, stimulus pulse width and maintenance protocols to address issues of neurocognitive side effects and relapse rates.
42 behavioral therapy, cognitive behavioral therapy, cognitive bibliotherapy, problemsolving therapy, brief psychodynamic therapy and life review therapy Most of these treatments have a behavioral activation component, which directly addresses the problem of activity limitation; some focus on meaningfulness of the activity. Engage therapy, Mindfulness cognitive therapy
43 rtms : FDA approved rtms as a treatment for depression for patients not responding to at least one antidepressant medication with a maximum age of 69. Other stimulation therapies include : transcranial direct current stimulation (tdcs), magnetic seizure therapy (MST), vagus nerve stimulation (VNS) and deep brain stimulation (DBS). Physical exercise.
44 Factors associated with improved chance of recovery from late-life depression Having a family history of depression Being female Having an extroverted personality Having no history of substance abuse or a psychotic illness Not having to be hospitalised for the depression Having high levels of social support*.
45
46 70 year old male patient Interpersonal stressors with daughter-in-law and property issues with nephew Precipitating event- police complaint by nephew History of withdrawn behaviour, sadness of mood, hopelessness, helplessness, continuous suicidal ideation Not sleeping, not eating History of auditory hallucinations, visual hallucinations Delusion of persecution reference Diagnosis- Depression with psychotic features
47 Treatment given T. Escitalopram, T. Haloperidol 12ECTs Poor response Relapsed within 2 months Added T. Valproate Poor response At present, patient responding to C. Fluoxetine.
48 Treating older adults with subsyndromal depressive symptoms. According to the Amsterdam Study of the Elderly, treatment of all patients with subsyndromal depressive symptoms could prevent 24.6% of new depression onsets in that period. Treatment of comorbid insomnia or other sleep disturbance. Other prevention interventions target older adults at risk of depression due to physical illness and bereavement and caregiver status. individual therapy for atrisk bereaved older adults, educational interventions for subjects with chronic illness, cognitive-behavioral interventions to reduce negative thinking, and life review.
49 Older adults go to primary physicians more often with somatic symptoms. So educating professional and lay audiences regarding recognition of depression in older adults, stressing particularly that depression is not a normal part of aging is important.
50 THANK YOU!
Geriatric Depression; Not a Normal Part of Growing Older. Cherie Warriner, LCSW
 1 Geriatric Depression; Not a Normal Part of Growing Older Cherie Warriner, LCSW What is Depression? While it is normal to feel sad or blue on occasion, these feelings are often transient. Depression is
1 Geriatric Depression; Not a Normal Part of Growing Older Cherie Warriner, LCSW What is Depression? While it is normal to feel sad or blue on occasion, these feelings are often transient. Depression is
GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES
 FACULTY DEVELOPMENT MASTERWORKS SERIES") UNIVERSITY OF SOUTH FLORIDA GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES Kathryn Hyer, PhD, MPP Principal Investigator h Providers of Continuing Education For additional
UNIVERSITY OF SOUTH FLORIDA GERIATRIC WORKFORCE ENHANCEMENT PROGRAM (GWEP) FACULTY DEVELOPMENT MASTERWORKS SERIES Kathryn Hyer, PhD, MPP Principal Investigator h Providers of Continuing Education For additional
Depression in the Eldery Handout Package
 Depression in the Eldery Handout Package Depression in the Elderly 1 Learning Objectives Upon completion of this module, you should be able to: 1. State the prevalence and describe the consequences of
Depression in the Eldery Handout Package Depression in the Elderly 1 Learning Objectives Upon completion of this module, you should be able to: 1. State the prevalence and describe the consequences of
Depression in Late Life
 Depression in Late Life Robert Madan MD FRCPC Geriatric Psychiatrist Key Learnings Robert Madan MD FRCPC Key Learnings By the end of the session, participants will be able to List the symptoms of depression
Depression in Late Life Robert Madan MD FRCPC Geriatric Psychiatrist Key Learnings Robert Madan MD FRCPC Key Learnings By the end of the session, participants will be able to List the symptoms of depression
A Basic Approach to Mood and Anxiety Disorders in the Elderly
 A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
Depressive, Bipolar and Related Disorders
 Depressive, Bipolar and Related Disorders Robert Kelly, MD Assistant Professor of Psychiatry Weill Cornell Medical College White Plains, New York Lecture available at www.robertkelly.us Financial Conflicts
Depressive, Bipolar and Related Disorders Robert Kelly, MD Assistant Professor of Psychiatry Weill Cornell Medical College White Plains, New York Lecture available at www.robertkelly.us Financial Conflicts
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
Depression: Assessment and Treatment For Older Adults
 Tool on Depression: Assessment and Treatment For Older Adults Based on: National Guidelines for Seniors Mental Health: the Assessment and Treatment of Depression Available on line: www.ccsmh.ca www.nicenet.ca
Tool on Depression: Assessment and Treatment For Older Adults Based on: National Guidelines for Seniors Mental Health: the Assessment and Treatment of Depression Available on line: www.ccsmh.ca www.nicenet.ca
Recognizing Depression and Restoring Mood and Well- Being in the Older Patient
 Recognizing Depression and Restoring Mood and Well- Being in the Older Patient Andreea L. Seritan, MD UC Davis Mini Medical School February 22, 2014 Objectives Review late life depression symptoms Review
Recognizing Depression and Restoring Mood and Well- Being in the Older Patient Andreea L. Seritan, MD UC Davis Mini Medical School February 22, 2014 Objectives Review late life depression symptoms Review
DEPRESSION VS. DEMENTIA IN THE ELDERLY PART I 9 CE hours
 DEPRESSION VS. DEMENTIA IN THE ELDERLY PART I 9 CE hours About the author Dr. Jassin M. Jouria is a medical doctor, professor of academic medicine, and medical author. He graduated from Ross University
DEPRESSION VS. DEMENTIA IN THE ELDERLY PART I 9 CE hours About the author Dr. Jassin M. Jouria is a medical doctor, professor of academic medicine, and medical author. He graduated from Ross University
Mental Health Problems in Older Adults: Signs & Symptoms Addressing Illness, Injury, & Loss
 Mental Health Problems in Older Adults: Signs & Symptoms Addressing Illness, Injury, & Loss Tobi A. Abramson, PhD September 22, 2013 Myths, Misperceptions, & Stereotypes Questions to consider Who has misperceptions
Mental Health Problems in Older Adults: Signs & Symptoms Addressing Illness, Injury, & Loss Tobi A. Abramson, PhD September 22, 2013 Myths, Misperceptions, & Stereotypes Questions to consider Who has misperceptions
A new Anatomy of Melancholy: rethinking depression and resilience
 A new Anatomy of Melancholy: rethinking depression and resilience Prof Declan McLoughlin Dept of Psychiatry & Trinity College Institute of Neuroscience Trinity College Dublin St Patrick s University Hospital
A new Anatomy of Melancholy: rethinking depression and resilience Prof Declan McLoughlin Dept of Psychiatry & Trinity College Institute of Neuroscience Trinity College Dublin St Patrick s University Hospital
Handout 3: Mood Disorders
 Handout 3: Mood Disorders Mood disorders are called affective (emotional) disorders. There are two categories of mood disorders: Depressive Disorders Bipolar Affective Disorders Depressive Disorders Minor
Handout 3: Mood Disorders Mood disorders are called affective (emotional) disorders. There are two categories of mood disorders: Depressive Disorders Bipolar Affective Disorders Depressive Disorders Minor
Depression Workshop 26 January 2007
 Depression Workshop 26 January 2007 Leslie G Walker Professor of Cancer Rehabilitation Donald M Sharp Senior Lecturer in Behavioural Oncology Mary B Walker Senior Clinical and Research Nurse Specialist
Depression Workshop 26 January 2007 Leslie G Walker Professor of Cancer Rehabilitation Donald M Sharp Senior Lecturer in Behavioural Oncology Mary B Walker Senior Clinical and Research Nurse Specialist
Aging with Bipolar Disorder. Neha Jain, MD, FAPA Assistant Professor of Psychiatry, UConn Health
 Aging with Bipolar Disorder Neha Jain, MD, FAPA Assistant Professor of Psychiatry, UConn Health Objectives Define bipolar disorder in the elderly Review comorbidities How does it differ from bipolar in
Aging with Bipolar Disorder Neha Jain, MD, FAPA Assistant Professor of Psychiatry, UConn Health Objectives Define bipolar disorder in the elderly Review comorbidities How does it differ from bipolar in
Depression among Older Adults. Prevalence & Intervention Strategies
 Depression among Older Adults Prevalence & Intervention Strategies Definition Depression is a complex syndrome complex characterized by mood disturbance plus variety of cognitive, psychological, and vegetative
Depression among Older Adults Prevalence & Intervention Strategies Definition Depression is a complex syndrome complex characterized by mood disturbance plus variety of cognitive, psychological, and vegetative
SECTION 1. Children and Adolescents with Depressive Disorder: Summary of Findings. from the Literature and Clinical Consultation in Ontario
 SECTION 1 Children and Adolescents with Depressive Disorder: Summary of Findings from the Literature and Clinical Consultation in Ontario Children's Mental Health Ontario Children and Adolescents with
SECTION 1 Children and Adolescents with Depressive Disorder: Summary of Findings from the Literature and Clinical Consultation in Ontario Children's Mental Health Ontario Children and Adolescents with
Guilt Suicidality. Depression Co-Occurs with Medical Illness The rate of major depression among those with medical illness is significant.
 1-800-PSYCH If you are obsessive-compulsive, dial 1 repeatedly If you are paranoid-delusional, dial 2 and wait, your call is being traced If you are schizophrenic, a little voice will tell you what number
1-800-PSYCH If you are obsessive-compulsive, dial 1 repeatedly If you are paranoid-delusional, dial 2 and wait, your call is being traced If you are schizophrenic, a little voice will tell you what number
Depression and cognitive decline in later life: cause, consequence or co-morbidity?
 Depression and cognitive decline in later life: cause, consequence or co-morbidity? Damien Gallagher MB MD MRCPsych Geriatric Psychiatrist, Sunnybrook Health Sciences Centre, Assistant Professor, University
Depression and cognitive decline in later life: cause, consequence or co-morbidity? Damien Gallagher MB MD MRCPsych Geriatric Psychiatrist, Sunnybrook Health Sciences Centre, Assistant Professor, University
Session outline. Introduction to depression Assessment of depression Management of depression Follow-up Review
 Depression 1 Session outline Introduction to depression Assessment of depression Management of depression Follow-up Review 2 Activity 1: Person s story followed by group discussion Present the first person
Depression 1 Session outline Introduction to depression Assessment of depression Management of depression Follow-up Review 2 Activity 1: Person s story followed by group discussion Present the first person
Depression. Content. Depression is common. Depression Facts. Depression kills. Depression attacks young people
 Content Depression Dr. Anna Lam Associate Consultant Department of Psychiatry, Queen Mary Hospital Honorary Clinical Assistant Professor Li Ka Shing Faculty of Medicine, The University of Hong Kong 1.
Content Depression Dr. Anna Lam Associate Consultant Department of Psychiatry, Queen Mary Hospital Honorary Clinical Assistant Professor Li Ka Shing Faculty of Medicine, The University of Hong Kong 1.
Primary Care: Referring to Psychiatry
 Primary Care: Referring to Psychiatry Carol Capitano, PhD, APRN-BC Assistant Professor, Clinical Educator University of New Mexico College of Nursing University of New Mexico Psychiatric Center Objectives
Primary Care: Referring to Psychiatry Carol Capitano, PhD, APRN-BC Assistant Professor, Clinical Educator University of New Mexico College of Nursing University of New Mexico Psychiatric Center Objectives
Symptoms Duration Impact on functioning
 Dr. Lori Triano- Antidormi Dr. Jane Storrie OPA Annual Conference February 21, 2015 Symptoms Duration Impact on functioning Numbness, shock, disbelief, denial Sadness Apathy, lack of interest, enthusiasm
Dr. Lori Triano- Antidormi Dr. Jane Storrie OPA Annual Conference February 21, 2015 Symptoms Duration Impact on functioning Numbness, shock, disbelief, denial Sadness Apathy, lack of interest, enthusiasm
Geriatric Depression Diagnosis and Treatment. Disclosures. Objectives 11/4/2018. None
 Geriatric Depression Diagnosis and Treatment David Mansoor, MD Assistant Professor of Psychiatry OHSU/PVAMC March 2018 Disclosures None Objectives Introduction / Epidemiology Assessment Differential Diagnosis
Geriatric Depression Diagnosis and Treatment David Mansoor, MD Assistant Professor of Psychiatry OHSU/PVAMC March 2018 Disclosures None Objectives Introduction / Epidemiology Assessment Differential Diagnosis
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults
 Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
Pharmaceutical Interventions. Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007
 Pharmaceutical Interventions Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007 Outline Overview Overview of initial workup and decisions in elderly depressed individual
Pharmaceutical Interventions Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007 Outline Overview Overview of initial workup and decisions in elderly depressed individual
9/24/2012. Amer M Burhan, MBChB, FRCP(C)
") Depression and Dementia Amer M Burhan MBChB, FRCPC Head of CAMH Memory Clinic, Toronto Geriatric Neuropsychiatrist Assistant Prof Psychiatry at U of T Objectives Discuss the prevalence and impact of depression
Depression and Dementia Amer M Burhan MBChB, FRCPC Head of CAMH Memory Clinic, Toronto Geriatric Neuropsychiatrist Assistant Prof Psychiatry at U of T Objectives Discuss the prevalence and impact of depression
4. Definition, clinical diagnosis and diagnostic criteria
 4. Definition, clinical diagnosis and diagnostic criteria 4.1. Definition Major depression is a mood disorder consisting of a set of symptoms, which include a predominance of the affective type (pathological
4. Definition, clinical diagnosis and diagnostic criteria 4.1. Definition Major depression is a mood disorder consisting of a set of symptoms, which include a predominance of the affective type (pathological
Delirium, Depression and Dementia
 Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Life is a miserable thing. I have decided to spend my life thinking about it. Irvin D. Yalom, The Schopenhauer Cure
 Life is a miserable thing. I have decided to spend my life thinking about it. Irvin D. Yalom, The Schopenhauer Cure GERIATRIC DEPRESSION Samir Patel, MD Geriatrics and Palliative Medicine and Geriatric
Life is a miserable thing. I have decided to spend my life thinking about it. Irvin D. Yalom, The Schopenhauer Cure GERIATRIC DEPRESSION Samir Patel, MD Geriatrics and Palliative Medicine and Geriatric
Depression and Suicide in Older Adults. William T. Regenold, M.D.C.M. Associate Professor of Psychiatry Director, Geriatric Psychiatry Division
 Depression and Suicide in Older Adults William T. Regenold, M.D.C.M. Associate Professor of Psychiatry Director, Geriatric Psychiatry Division What is depression in older adults like? A syndrome in people
Depression and Suicide in Older Adults William T. Regenold, M.D.C.M. Associate Professor of Psychiatry Director, Geriatric Psychiatry Division What is depression in older adults like? A syndrome in people
Some newer, investigational approaches to treating refractory major depression are being used.
 CREATED EXCLUSIVELY FOR FINANCIAL PROFESSIONALS Rx FOR SUCCESS Depression and Anxiety Disorders Mood and anxiety disorders are common, and the mortality risk is due primarily to suicide, cardiovascular
CREATED EXCLUSIVELY FOR FINANCIAL PROFESSIONALS Rx FOR SUCCESS Depression and Anxiety Disorders Mood and anxiety disorders are common, and the mortality risk is due primarily to suicide, cardiovascular
Measure #106 (NQF 0103): Adult Major Depressive Disorder (MDD): Comprehensive Depression Evaluation: Diagnosis and Severity
: Adult Major Depressive Disorder (MDD): Comprehensive Depression Evaluation: Diagnosis and Severity") Measure #106 (NQF 0103): Adult Major Depressive Disorder (MDD): Comprehensive Depression Evaluation: Diagnosis and Severity 2014 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: Percentage
Measure #106 (NQF 0103): Adult Major Depressive Disorder (MDD): Comprehensive Depression Evaluation: Diagnosis and Severity 2014 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: Percentage
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia
 Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
Depressive and Bipolar Disorders
 Depressive and Bipolar Disorders Symptoms Associated with Depressive and Bipolar Disorders Characteristics of mood symptoms Affects a person s well being, school, work, or social functioning Continues
Depressive and Bipolar Disorders Symptoms Associated with Depressive and Bipolar Disorders Characteristics of mood symptoms Affects a person s well being, school, work, or social functioning Continues
Mental Health: Subjective evaluation of overall quality of life (QOL) Happiness, life satisfaction, morale, trait effect, etc. Quality of Life (QOL)
 Happiness, life satisfaction, morale, trait effect, etc. Quality of Life (QOL)") Mental Health: Subjective evaluation of overall quality of life (QOL) Happiness, life satisfaction, morale, trait effect, etc. Quality of Life (QOL) Multidimensional concept Includes: Physical health Cognitive
Mental Health: Subjective evaluation of overall quality of life (QOL) Happiness, life satisfaction, morale, trait effect, etc. Quality of Life (QOL) Multidimensional concept Includes: Physical health Cognitive
8/15/14. Julie Wood, MD Southwestern Behavioral Healthcare & Mulberry Memory Clinic
 Julie Wood, MD Southwestern Behavioral Healthcare & Mulberry Memory Clinic SILVER TSUNAMI DEPRESSION STATS DIAGNOSTIC CRITERIA ASSESSMENT OF GERIATRIC DEPRESSION RISK FACTORS TREATMENT OPTIONS FOR GERIATRIC
Julie Wood, MD Southwestern Behavioral Healthcare & Mulberry Memory Clinic SILVER TSUNAMI DEPRESSION STATS DIAGNOSTIC CRITERIA ASSESSMENT OF GERIATRIC DEPRESSION RISK FACTORS TREATMENT OPTIONS FOR GERIATRIC
DEPRESSION An introduction to aging science brought to you by the American Federation for Aging Research
 infoaging guides DISEASES OF AGING DEPRESSION An introduction to aging science brought to you by the American Federation for Aging Research WHAT IS DEPRESSION AND WHY IS IT IMPORTANT? Depression is a mood
infoaging guides DISEASES OF AGING DEPRESSION An introduction to aging science brought to you by the American Federation for Aging Research WHAT IS DEPRESSION AND WHY IS IT IMPORTANT? Depression is a mood
Contemporary Psychiatric-Mental Health Nursing Third Edition. Introduction. Introduction 9/10/ % of US suffers from Mood Disorders
 Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Introduction 12% of US suffers from Mood Disorders MD are a group of psychiatric DO characterized by physical, emotional
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Introduction 12% of US suffers from Mood Disorders MD are a group of psychiatric DO characterized by physical, emotional
Psychosocial Problems In Reproductive Health Of Elders
 Psychosocial Problems In Reproductive Health Of Elders Dr. Sonia Oveisi Maternity and Child Health Assistant Professor of Qazvin University of Medical Science 6/2/2014 1 Goals 1. Definition 2. Epidemiology
Psychosocial Problems In Reproductive Health Of Elders Dr. Sonia Oveisi Maternity and Child Health Assistant Professor of Qazvin University of Medical Science 6/2/2014 1 Goals 1. Definition 2. Epidemiology
Behavioral Aspects of Parkinson s Disease
 Behavioral Aspects of Parkinson s Disease Joseph H. Friedman, MD Director, Movement Disorders Program Butler Hospital Dept of Neurology Alpert Medical School of Brown University 1 Disclosures Drugs will
Behavioral Aspects of Parkinson s Disease Joseph H. Friedman, MD Director, Movement Disorders Program Butler Hospital Dept of Neurology Alpert Medical School of Brown University 1 Disclosures Drugs will
Mood Disorders. Gross deviation in mood
 Mood Disorders Gross deviation in mood Depression u Affective: Depressed mood (kids-irritability), or anhedonia for 2 weeks minimum. u Cognitive: worthlessness/ guilt, hopelessness, indecisiveness/ concentration,
Mood Disorders Gross deviation in mood Depression u Affective: Depressed mood (kids-irritability), or anhedonia for 2 weeks minimum. u Cognitive: worthlessness/ guilt, hopelessness, indecisiveness/ concentration,
Comparative Health Care Analysis of Depression in the Elderly
 Comparative Health Care Analysis of Depression in the Elderly Julie Breazeale & Norma Bono Oregon Health & Science University Klamath Falls April 29 th, 2016 Depression Overview www.thedigitalfa.com According
Comparative Health Care Analysis of Depression in the Elderly Julie Breazeale & Norma Bono Oregon Health & Science University Klamath Falls April 29 th, 2016 Depression Overview www.thedigitalfa.com According
Managing Pain. in Marfan Syndrome. Traci J. Speed, MD PhD Assistant Professor, Department of Psychiatry and Behavioral Sciences
 Managing Pain in Marfan Syndrome Traci J. Speed, MD PhD Assistant Professor, Department of Psychiatry and Behavioral Sciences No financial disclosures Objectives Define pain Discuss the role of comorbid
Managing Pain in Marfan Syndrome Traci J. Speed, MD PhD Assistant Professor, Department of Psychiatry and Behavioral Sciences No financial disclosures Objectives Define pain Discuss the role of comorbid
Chapter 15: Late Life and Psychological Disorders
 \ Chapter 15: Late Life and Psychological Disorders 1. Ageism refers to a. the physical deterioration that accompanies old age. b. the intellectual deterioration that frequently occurs as a person ages.
\ Chapter 15: Late Life and Psychological Disorders 1. Ageism refers to a. the physical deterioration that accompanies old age. b. the intellectual deterioration that frequently occurs as a person ages.
More Than Just Moody Blaise Aguirre, MD Child and Adolescent Psychiatrist McLean Hospital Assistant Professor of Psychiatry Harvard Medical School
 More Than Just Moody Blaise Aguirre, MD Child and Adolescent Psychiatrist McLean Hospital Assistant Professor of Psychiatry Harvard Medical School Keep in Mind In the U.S., approximately 10-15% of children/adolescents
More Than Just Moody Blaise Aguirre, MD Child and Adolescent Psychiatrist McLean Hospital Assistant Professor of Psychiatry Harvard Medical School Keep in Mind In the U.S., approximately 10-15% of children/adolescents
Drugs for Emotional and Mood Disorders Chapter 16
 Drugs for Emotional and Mood Disorders Chapter 16 NCLEX-RN Review Question 1 Choices Please note Question #1 at the end of Ch 16 pg 202 & Key pg 805 answer is #4 1. Psychomotor symptoms 2. Tachycardia,
Drugs for Emotional and Mood Disorders Chapter 16 NCLEX-RN Review Question 1 Choices Please note Question #1 at the end of Ch 16 pg 202 & Key pg 805 answer is #4 1. Psychomotor symptoms 2. Tachycardia,
Bipolar disorder. Paz García-Portilla
 Bipolar disorder Paz García-Portilla BD I: Epidemiology Life-time prevalence 1% (0.7 1.8%) 30% with diagnosis and without treatment, or with erroneous diagnosis (major unipolar depression, borderline PD)
Bipolar disorder Paz García-Portilla BD I: Epidemiology Life-time prevalence 1% (0.7 1.8%) 30% with diagnosis and without treatment, or with erroneous diagnosis (major unipolar depression, borderline PD)
depression and anxiety in later life clinical challenges and creative research
 2 nd Annual MARC Symposium Critical Themes in Ageing Melbourne, 10 th August 2018 depression and anxiety in later life clinical challenges and creative research Nicola T Lautenschlager, MD, FRANZCP Professor
2 nd Annual MARC Symposium Critical Themes in Ageing Melbourne, 10 th August 2018 depression and anxiety in later life clinical challenges and creative research Nicola T Lautenschlager, MD, FRANZCP Professor
Chapter 6 Mood Disorders and Suicide An Overview of Mood Disorders
 Page 1 Extremes in Normal Mood Chapter 6 Mood Disorders and Suicide An Overview of Mood Disorders Nature of depression Nature of mania and hypomania Types of DSM-IV Depressive Disorders Major depressive
Page 1 Extremes in Normal Mood Chapter 6 Mood Disorders and Suicide An Overview of Mood Disorders Nature of depression Nature of mania and hypomania Types of DSM-IV Depressive Disorders Major depressive
Randall Espinoza, MD, MPH Clinical Professor of Psychiatry Geffen School of Medicine at UCLA
 Randall Espinoza, MD, MPH Clinical Professor of Psychiatry Geffen School of Medicine at UCLA Research and academic support: Prior K01 (GACA) from BHPr R01 Neuroimaging Biomarkers of ECT Response in Major
Randall Espinoza, MD, MPH Clinical Professor of Psychiatry Geffen School of Medicine at UCLA Research and academic support: Prior K01 (GACA) from BHPr R01 Neuroimaging Biomarkers of ECT Response in Major
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
DEPRESSION IN CHILDHOOD AND ADOLECENCE
 DEPRESSION IN CHILDHOOD AND ADOLECENCE Bob Salo Mood Disorders Childhood Depression Major Depressive Disorder Disruptive Mood Dysregulation Disorder Bipolar Affective Disorder Mainly Depressive Mainly
DEPRESSION IN CHILDHOOD AND ADOLECENCE Bob Salo Mood Disorders Childhood Depression Major Depressive Disorder Disruptive Mood Dysregulation Disorder Bipolar Affective Disorder Mainly Depressive Mainly
Treating Childhood Depression in Pediatrics. Martha U. Barnard, Ph.D. University of Kansas Medical Center Pediatrics/Behavioral Sciences
 Treating Childhood Depression in Pediatrics Martha U. Barnard, Ph.D. University of Kansas Medical Center Pediatrics/Behavioral Sciences Objectives The learner will: Describe the signs and symptoms of childhood
Treating Childhood Depression in Pediatrics Martha U. Barnard, Ph.D. University of Kansas Medical Center Pediatrics/Behavioral Sciences Objectives The learner will: Describe the signs and symptoms of childhood
Psychosis, Mood, and Personality: A Clinical Perspective
 Psychosis, Mood, and Personality: A Clinical Perspective John R. Chamberlain, M.D. Assistant Director, Psychiatry and the Law Program Assistant Clinical Professor University of California San Francisco
Psychosis, Mood, and Personality: A Clinical Perspective John R. Chamberlain, M.D. Assistant Director, Psychiatry and the Law Program Assistant Clinical Professor University of California San Francisco
DEMOGRAPHICS. Old Age for DD. Dual Diagnosis: Mental Illness & Developmental Disabilities. Peggy A. Szwabo, Ph.D. 314/647/4488
 Dual Diagnosis: Mental Illness & Developmental Disabilities Peggy A. Szwabo, Ph.D. 314/647/4488 pszwabo@sbcglobal.net DEMOGRAPHICS 10-15% of DD are 65+ 40-70% mental disorder 40% not in formal delivery
Dual Diagnosis: Mental Illness & Developmental Disabilities Peggy A. Szwabo, Ph.D. 314/647/4488 pszwabo@sbcglobal.net DEMOGRAPHICS 10-15% of DD are 65+ 40-70% mental disorder 40% not in formal delivery
Mood Disorders Workshop Dr Andrew Howie / Dr Tony Fernando Psychological Medicine Faculty of Medical and Health Sciences University of Auckland
 Mood Disorders Workshop 2010 Dr Andrew Howie / Dr Tony Fernando Psychological Medicine Faculty of Medical and Health Sciences University of Auckland Goals To learn about the clinical presentation of mood
Mood Disorders Workshop 2010 Dr Andrew Howie / Dr Tony Fernando Psychological Medicine Faculty of Medical and Health Sciences University of Auckland Goals To learn about the clinical presentation of mood
Mood Disorders. Dr. Vidumini De Silva
 Mood Disorders Dr. Vidumini De Silva Depression - Lowering of mood Mania - Heightening of mood Depressive Disorder Overview Introduction Clinical Features Aetiology Course and prognosis What s your management
Mood Disorders Dr. Vidumini De Silva Depression - Lowering of mood Mania - Heightening of mood Depressive Disorder Overview Introduction Clinical Features Aetiology Course and prognosis What s your management
Mental Health Rotation Educational Goals & Objectives
 Mental Health Rotation Educational Goals & Objectives Mental illness is prevalent in the general population and is commonly seen and treated in the office of the primary care provider. Educational experiences
Mental Health Rotation Educational Goals & Objectives Mental illness is prevalent in the general population and is commonly seen and treated in the office of the primary care provider. Educational experiences
POST-STROKE DEPRESSION
 POST-STROKE DEPRESSION Stroke Annual Review March 7 th & 8 th, 2018 Justine Spencer, PhD, CPsych OVERVIEW What is Post-Stroke Depression (PSD)? Risk factors/predictors Impact of PSD Treatment and Management
POST-STROKE DEPRESSION Stroke Annual Review March 7 th & 8 th, 2018 Justine Spencer, PhD, CPsych OVERVIEW What is Post-Stroke Depression (PSD)? Risk factors/predictors Impact of PSD Treatment and Management
Depression in Older Adults. Key Issues
 Depression in Older Adults Key Issues Depression and Older Adults: Key Issues is an overview of important information that you should know about depression in older adults. Depression is one of the most
Depression in Older Adults Key Issues Depression and Older Adults: Key Issues is an overview of important information that you should know about depression in older adults. Depression is one of the most
Depression in Older Adults. Paul Boulware, MD Arizona Neurological Institute April 22, 2012
 Depression in Older Adults Paul Boulware, MD Arizona Neurological Institute April 22, 2012 What is it? Major depressive disorder is a syndrome, a collection of symptoms Presentation is variable among individuals
Depression in Older Adults Paul Boulware, MD Arizona Neurological Institute April 22, 2012 What is it? Major depressive disorder is a syndrome, a collection of symptoms Presentation is variable among individuals
 DEPRESSION Depression is a major public health problem around the world Affects 1:5 older people living in the community Affects 2:5 older people living in care homes Various treatment options available,
DEPRESSION Depression is a major public health problem around the world Affects 1:5 older people living in the community Affects 2:5 older people living in care homes Various treatment options available,
KEY MESSAGES. It is often under-recognised and 30-50% of MDD cases in primary care and medical settings are not detected.
 KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
Major Depression Major Depression
 Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Major Depression Major Depression Characterized by a change in several aspects of a person s life and emotional state
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Major Depression Major Depression Characterized by a change in several aspects of a person s life and emotional state
Understanding Psychiatry & Mental Illness
 Understanding Psychiatry & Steve Ellen Mental Illness MB, BS. M.Med. MD. FRANZCP Head, Consultation, Liaison & Emergency Psychiatry, Alfred Health. Associate Professor, Monash Alfred Psychiatry Research
Understanding Psychiatry & Steve Ellen Mental Illness MB, BS. M.Med. MD. FRANZCP Head, Consultation, Liaison & Emergency Psychiatry, Alfred Health. Associate Professor, Monash Alfred Psychiatry Research
Depression in the Medically Ill
 Mayo School of Continuous Professional Development Psychiatry in Medical Settings February 9 th, 2017 Depression in the Medically Ill David Katzelnick, M.D. Professor of Psychiatry, Mayo Clinic College
Mayo School of Continuous Professional Development Psychiatry in Medical Settings February 9 th, 2017 Depression in the Medically Ill David Katzelnick, M.D. Professor of Psychiatry, Mayo Clinic College
DEPRESSION. Dr. Jonathan Haverkampf, M.D.
 Dr., M.D. Depression is one of the most common medical conditions, which can interfere with a person s quality of life, relationships and ability to work significantly. Fortunately, there are a number
Dr., M.D. Depression is one of the most common medical conditions, which can interfere with a person s quality of life, relationships and ability to work significantly. Fortunately, there are a number
Aging and Mental Health Current Challenges in Long Term Care
 Aging and Mental Health Current Challenges in Long Term Care Stephanie Saur & Christina Pacheco Acute Care Behavioural Consultants Alzheimer Society Peel What is Mental Health? Mental health includes our
Aging and Mental Health Current Challenges in Long Term Care Stephanie Saur & Christina Pacheco Acute Care Behavioural Consultants Alzheimer Society Peel What is Mental Health? Mental health includes our
DIAGNOSTIC CRITERIA (ICD 10)
") DEPRESSION Depression is a major public health problem around the world Affects 1:5 older people living in the community Affects 2:5 older people living in care homes Various treatment options available,
DEPRESSION Depression is a major public health problem around the world Affects 1:5 older people living in the community Affects 2:5 older people living in care homes Various treatment options available,
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Geriatric Depression 李淑花醫師林口長庚醫院精神科 10:20-11:10, Outlines
 Geriatric Depression 李淑花醫師林口長庚醫院精神科 10:20-11:10, 2013.06.22 1 Outlines Introduction Clinical presentation Cognitive impairment in old age depressive disorder Vascular depression hypothesis Pharmacotherapy
Geriatric Depression 李淑花醫師林口長庚醫院精神科 10:20-11:10, 2013.06.22 1 Outlines Introduction Clinical presentation Cognitive impairment in old age depressive disorder Vascular depression hypothesis Pharmacotherapy
Chapter 7 - Mood Disorders
 Chapter 7 - Mood Disorders I. DEPRESSION A. Description Symptoms: 5+ constant over 2 weeks - sadness/depressed mood - guilt/remorse/worthlessness - suicidal thoughts - anhedonia (lack of pleasure) - fatigue/lethargy
Chapter 7 - Mood Disorders I. DEPRESSION A. Description Symptoms: 5+ constant over 2 weeks - sadness/depressed mood - guilt/remorse/worthlessness - suicidal thoughts - anhedonia (lack of pleasure) - fatigue/lethargy
PSYCHIATRIC CO-MORBIDITY STEVE SUGDEN MD MPH
 PSYCHIATRIC CO-MORBIDITY STEVE SUGDEN MD MPH OVERVIEW: PSYCHIATRIC DISORDERS Mood Disorders Anxiety Disorders Psychotic Disorders Personality Disorders PTSD Eating Disorders EXAMPLE What is the diagnosis?
PSYCHIATRIC CO-MORBIDITY STEVE SUGDEN MD MPH OVERVIEW: PSYCHIATRIC DISORDERS Mood Disorders Anxiety Disorders Psychotic Disorders Personality Disorders PTSD Eating Disorders EXAMPLE What is the diagnosis?
DEMENTIA AND MEDICATION
 DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
Mental Disorders in Older Adults, by George W. Rebok, is available under a Creative Commons Attribution-NonCommercial-ShareAlike 2.5 Generic license.
 Mental Disorders in Older Adults, by George W. Rebok, is available under a Creative Commons Attribution-NonCommercial-ShareAlike 2.5 Generic license. 2007, The Johns Hopkins University and George W. Rebok.
Mental Disorders in Older Adults, by George W. Rebok, is available under a Creative Commons Attribution-NonCommercial-ShareAlike 2.5 Generic license. 2007, The Johns Hopkins University and George W. Rebok.
Guidelines MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD)
") MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
Women, Aging and Mental Health. Dr Cathy Shea Associate Professor Head, Division of Geriatric Psychiatry University of Ottawa
 Women, Aging and Mental Health Dr Cathy Shea Associate Professor Head, Division of Geriatric Psychiatry University of Ottawa Objectives To discuss the course of early onset mental illness and issues to
Women, Aging and Mental Health Dr Cathy Shea Associate Professor Head, Division of Geriatric Psychiatry University of Ottawa Objectives To discuss the course of early onset mental illness and issues to
Mild Cognitive Impairment (MCI)
") October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Bipolar Disorder 4/6/2014. Bipolar Disorder. Symptoms of Depression. Mania. Depression
 Bipolar Disorder J. H. Atkinson, M.D. Professor of Psychiatry HIV Neurobehavioral Research Programs University of California, San Diego KETHEA, Athens Slides courtesy of John Kelsoe, M.D. Bipolar Disorder
Bipolar Disorder J. H. Atkinson, M.D. Professor of Psychiatry HIV Neurobehavioral Research Programs University of California, San Diego KETHEA, Athens Slides courtesy of John Kelsoe, M.D. Bipolar Disorder
Arizona Geriatrics Society 5th Annual Spring Geriatrics Multi-Disciplinary Conference EXPANDING YOUR GERIATRIC TOOLBOX Saturdays, May 5, 12, 19
 Arizona Geriatrics Society 5th Annual Spring Geriatrics Multi-Disciplinary Conference Teri Kennedy, PhD, MSW, LCSW, ACSW Director, Office of Gerontological Social Work Initiatives Arizona State University/School
Arizona Geriatrics Society 5th Annual Spring Geriatrics Multi-Disciplinary Conference Teri Kennedy, PhD, MSW, LCSW, ACSW Director, Office of Gerontological Social Work Initiatives Arizona State University/School
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Major Depressive Disorder. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Major Depressive Disorder. These podcasts are designed to give medical students an overview of key topics in pediatrics.
Our Senior Clients Clinical Issues Treatment Implications Interventions
 Our Senior Clients Clinical Issues Treatment Implications Interventions Presented by Dr. Christine A. Cauffield, CEO, LSF Health Systems Learning Objectives Identify key characteristics of Major Depressive
Our Senior Clients Clinical Issues Treatment Implications Interventions Presented by Dr. Christine A. Cauffield, CEO, LSF Health Systems Learning Objectives Identify key characteristics of Major Depressive
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
PSYCH 235 Introduction to Abnormal Psychology. Agenda/Overview. Mood Disorders. Chapter 11 Mood/Bipolar and Related disorders & Suicide
 PSYCH 235 Introduction to Abnormal Psychology Chapter 11 Mood/Bipolar and Related disorders & Suicide 1 Agenda/Overview Mood disorders Major depression Persistent Depressive Disorder (Dysthymia) Bipolar
PSYCH 235 Introduction to Abnormal Psychology Chapter 11 Mood/Bipolar and Related disorders & Suicide 1 Agenda/Overview Mood disorders Major depression Persistent Depressive Disorder (Dysthymia) Bipolar
Mental Health Disorders Civil Commitment UNC School of Government
 Mental Health Disorders 2017 Civil Commitment UNC School of Government Edward Poa, MD, FAPA Chief of Inpatient Services, The Menninger Clinic Associate Professor, Baylor College of Medicine NC statutes
Mental Health Disorders 2017 Civil Commitment UNC School of Government Edward Poa, MD, FAPA Chief of Inpatient Services, The Menninger Clinic Associate Professor, Baylor College of Medicine NC statutes
Mental Health Counseling for mood, aging, and coping with life transitions and chronic illness.
 Mental Health Counseling for mood, aging, and coping with life transitions and chronic illness. Silver Linings for Seniors Silver Linings for Seniors, Inc. offers on-site confidential Mental Health Counseling
Mental Health Counseling for mood, aging, and coping with life transitions and chronic illness. Silver Linings for Seniors Silver Linings for Seniors, Inc. offers on-site confidential Mental Health Counseling
Repetitive transcranial magnetic stimulation for depression
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Repetitive transcranial magnetic stimulation for depression Depression causes low mood or sadness that can
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Repetitive transcranial magnetic stimulation for depression Depression causes low mood or sadness that can
ACOEM Commercial Driver Medical Examiner Training Program
 ACOEM Commercial Driver Medical Examiner Training Program Module 7: Psychological Psychological 49 CFR 391.41(b)(9) "A person is physically qualified to drive a commercial motor vehicle if that person
ACOEM Commercial Driver Medical Examiner Training Program Module 7: Psychological Psychological 49 CFR 391.41(b)(9) "A person is physically qualified to drive a commercial motor vehicle if that person
DSM5: How to Understand It and How to Help
 DSM5: How to Understand It and How to Help Introduction: The DSM5 is a foreign language! Three Questions: I. The first was, What the key assumptions made to determine the organization of the DSM5? A. Mental
DSM5: How to Understand It and How to Help Introduction: The DSM5 is a foreign language! Three Questions: I. The first was, What the key assumptions made to determine the organization of the DSM5? A. Mental
Depression and Bipolar Disorder
 The Canadian Mental Health Association (CMHA) is a nation-wide, charitable organization that promotes the mental health of all and supports the resilience and recovery of people experiencing mental illness.
The Canadian Mental Health Association (CMHA) is a nation-wide, charitable organization that promotes the mental health of all and supports the resilience and recovery of people experiencing mental illness.
GENI Jeopardy: Geriatric Mental Health. Part of the brain responsible for executive functioning
 GENI Jeopardy: Geriatric Mental Health Part of the brain responsible for executive functioning Dementia: It is not just forgetfulness GENI February 20, 2008 Marcia Carr - CNS Dementia Dementia means brain
GENI Jeopardy: Geriatric Mental Health Part of the brain responsible for executive functioning Dementia: It is not just forgetfulness GENI February 20, 2008 Marcia Carr - CNS Dementia Dementia means brain
Dr M Suresh Kumar MD DPM MPH (USA) Director Psymed hospital Chennai NAMSCON 2018 October Puducherry
 Director Psymed hospital Chennai NAMSCON 2018 October Puducherry") MENTAL HEALTH IN ELDERLY Dr M Suresh Kumar MD DPM MPH (USA) Director Psymed hospital Chennai www.drmsureshkumar.com NAMSCON 2018 October 26 2018 Puducherry Mental health in elderly Source: Elderly in India.
MENTAL HEALTH IN ELDERLY Dr M Suresh Kumar MD DPM MPH (USA) Director Psymed hospital Chennai www.drmsureshkumar.com NAMSCON 2018 October 26 2018 Puducherry Mental health in elderly Source: Elderly in India.
Alcoholism. Psychiatry. Alcoholism. Alcoholism. Certification. Certification
 Alcoholism Psychiatry Liz Clark, D.O., MPH & TM FAOCOPM MY-2012 Except where absolute criteria exist (i.e., a current clinical diagnosis of alcoholism), as a medical examiner, you make the final determination
Alcoholism Psychiatry Liz Clark, D.O., MPH & TM FAOCOPM MY-2012 Except where absolute criteria exist (i.e., a current clinical diagnosis of alcoholism), as a medical examiner, you make the final determination
Mental Health Issues and Treatment
 Mental Health Issues and Treatment Mental health in older age Depression Causes of depression Effects of depression Suicide Newsom, Winter 2017, Psy 462/562 Psychology of Adult Development and Aging 1
Mental Health Issues and Treatment Mental health in older age Depression Causes of depression Effects of depression Suicide Newsom, Winter 2017, Psy 462/562 Psychology of Adult Development and Aging 1
Caring for the Mind: Managing Depression and Anxiety. Highlights from 2017 ONS Congress
 Caring for the Mind: Managing Depression and Anxiety Highlights from 2017 ONS Congress Mood and Anxiety Disorders: Symptoms of mood disorders Non-reactive mood, worthlessness, guilt, loss of interest,
Caring for the Mind: Managing Depression and Anxiety Highlights from 2017 ONS Congress Mood and Anxiety Disorders: Symptoms of mood disorders Non-reactive mood, worthlessness, guilt, loss of interest,
Management of a HIV-infected patient with a psychiatric disorder
 Management of a HIV-infected patient with a psychiatric disorder Maria Ferrara, Modena, Italia Guida Da Ponte, Lisboa, Portugal Jordi Blanch, Barcelona Main complaint Mr M is a 30-year-old HIV+ man In
Management of a HIV-infected patient with a psychiatric disorder Maria Ferrara, Modena, Italia Guida Da Ponte, Lisboa, Portugal Jordi Blanch, Barcelona Main complaint Mr M is a 30-year-old HIV+ man In
Mending the Mind: treatment of the severely mentally ill
 Mending the Mind: treatment of the severely mentally ill First, the bad news Mental Illness Prevalence: putting things in perspective --More than 54 million Americans have a mental disorder in any given
Mending the Mind: treatment of the severely mentally ill First, the bad news Mental Illness Prevalence: putting things in perspective --More than 54 million Americans have a mental disorder in any given
Malaysian Healthy Ageing Society
 { Organised by: Co-Sponsored: Malaysian Healthy Ageing Society Promoting Healthy Ageing in Depressed Elderly Patients Ist World Congress On Healthy Ageing Evolution: Holistic Ageing in an Age of change
{ Organised by: Co-Sponsored: Malaysian Healthy Ageing Society Promoting Healthy Ageing in Depressed Elderly Patients Ist World Congress On Healthy Ageing Evolution: Holistic Ageing in an Age of change