SKIN HISTOLOGY AND FUNCTION
|
|
|
- Joseph Todd
- 5 years ago
- Views:
Transcription

1 SKIN HISTOLOGY AND FUNCTION
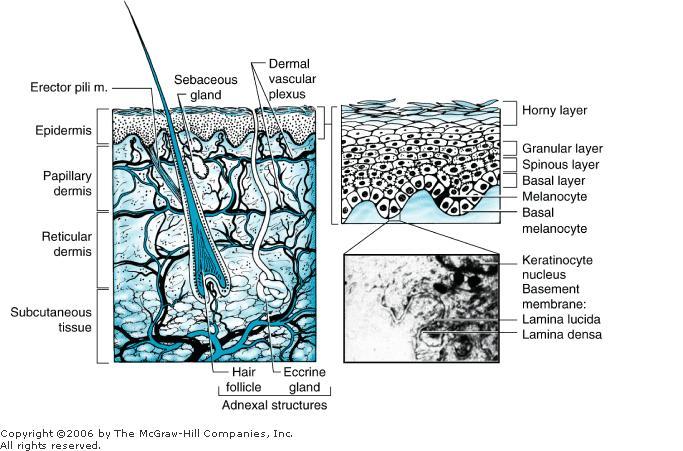
2 THREE LAYERS : EPIDERMIS BASEMENT MEMBRANE DERMIS EPIDERMIS : COMPOSED OF KERATINOCYTES NO MATRIX DEEP BASAL LAYER MITOTICALLY ACTIVE SPINOUS LAYER MATURE HYALIN HORNY LAYER AGED CELLS SHED TRANSIT TIME: 40 TO 56 DAYS KERAINS 5 & 14 MELANOCYTES ORIGIN FROM NEURA CREST 1:35 MELANIN TYROSINE & CYSTEINE MELANOSOME TO KERATINOCYTES DENSITY OF MELANOCYTES CONSTANT MELANIN PRODUCTION INFLUENCED BY MSH, ACTH, UV RAYS etc
3 BASEMENT MEMBRANE ZONE ANCHOR EPIDERMIS TO DERMIS BY PROTEIN STRUCTURES DERMIS : 70% OF WEIGHT COLLAGEN TYPE I TENSILE STRENGTH ELASTIC FIBRES GROUND SUBSTANCE POLYSACCHARIDE, POLYPEPTIDES FIBROBLASTS THROUGHOUT DERMIS PROTEIN MATRIX NET WORK OF BLOOD VESSELS PAPILLARY DERMIS GLOMUS BODIES: TORTUOUS A V SHUNTS REGULATES BODY TEMPERATURE SENSORY NERVE ENDINGS RECEPTORS, PACINIAN, MEISSNER, RUFFINI FREE NERVE ENDINGS MERKEL S CELLS, HAIR FOLLICLE ADENEXCAL : SWEAT GLANDS PALMS, SOLE, AXILLA APPOCRINE GLANDS AXILLA, PERINEUM SCENT
4
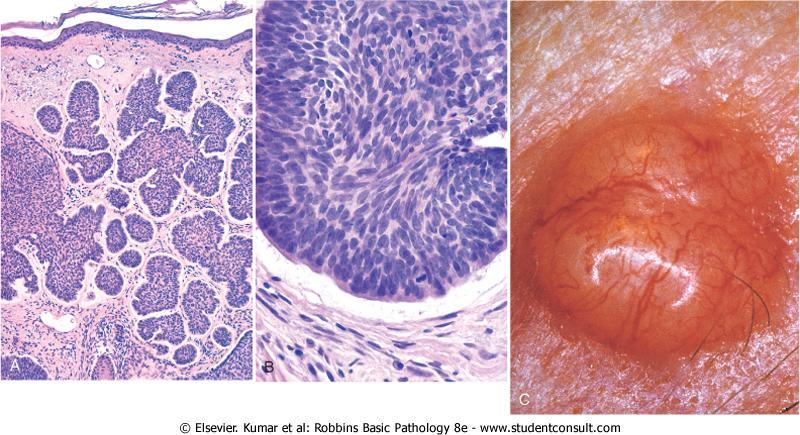
5 MALIGNANT TUMOURS EPIDEMIOLOGY EXPOSURE TO UV RADIATION CHEMICAL CARCINOGEN TAR, ARSENIC, NITROGEN MUSTARD HPV SQUAMOUS CELL CA RADIATION DERMATITIS CHRONIC IRRITATION MARJOLIN S ULCER etc IMMUNO SUPPRESSION HIV BASAL CELL CARCINOMA SLOW GROWING RARELY METASTASIS LOCALLY DESTRUCTIVE SITES FACE, SCALP, NOSE, CHEEK
6 PRE DISPOSING FACTORS FAIR COMPLEXION RADIOATION EXPOSURE SUN BURNS IMMUNO SURESSION PATHOLOGY ARISE FROM BASAL LAYER OF EPIDERMIS PILOSEBACEOUS ADENEXA TYPES: a) NODULAR b) SUPERFICIAL c) MICRONODULAR d) INFILTRATING e) SCLEROSING INFILTRATING AND SCLEROSING TYPES MOST AGGRESSIVE 10 %

7

8
9 CLINICAL FEATURES PEARLY, TRANSLUCENT MASS RAISED BORDERS ULCERATE ERYTHMATOUS PATCHES, SCALY SCARING, (DD.PSORIASIS, EZEMA) ISLANDS OF TUMOUR EXTENDING SURROUNDING DIAGNOSIS BIOPSY SHAVE, PUNCH, INCISION, EXCISION TREATMENT ELECTRO DESICCATION CURETTAGE NODULAR TYPE LESS THAN 2 cm SUPERFICIAL ANY SIZE % CURE RATE
10 CRYOTHERAPY: LESION 2 cm Scarring, HYPOPIGMENTATION NO HISTELOGICAL CONFIRMATION USED ONLY LESS AGGRESSIVE LESIONS NOT USED IN PERI ORAL, ORBITAL AREAS SURGICAL EXCISION CURE RATE 90 % MARGIN 2 5 mm DEPEND ON SIZE MOH S MICROGRAPHIC SURGERY PERI ORAL AREA 99 % PRIMARY 96 % RECURRENT NASAL ALA LESIONS
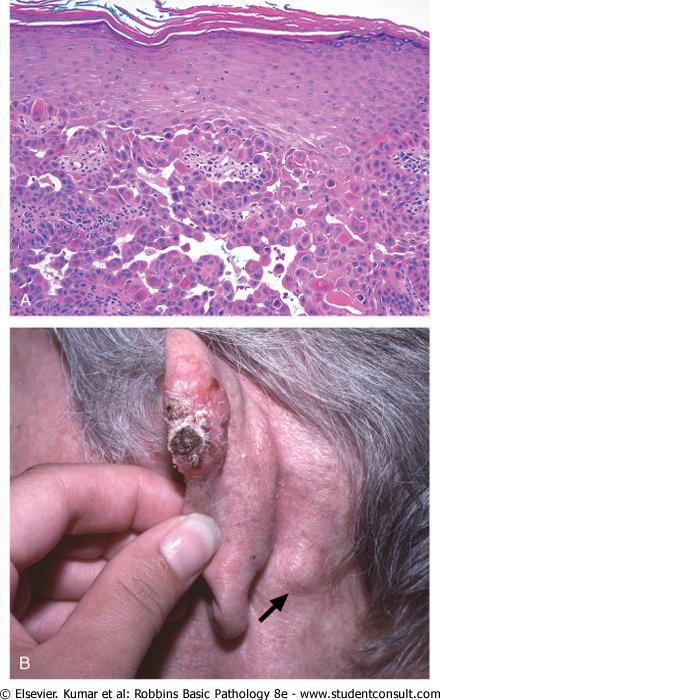
11 SQUAMOUS CELL CARCINOMA MORE COMMON THAN BCC ARISE FROM KERATINOCYTES EPIDERMIS ARISE FROM ACTINIC KERATOSIS, LEUKOPLAKIA, RADIATION DERMATITIS, SCARS, CHRONIC ULCER, BOWEN DISEASE INSITU SKIN PATCHES, NODULE CENTRAL INFLAMATION INDURATION, NECROSIS OOZING METASTASES DIRECT INFILTARTION, LYMPHATIC HAEMATOGENOUS AUSTRALIA: HIGH UV EXPOSURE RACE : WHITE COMPLEXION SEX : MALE / FEMALE 2:1 AGE : ABOVE 60 years RISK FACTORS: IONIZING RADIATION, ARSENIC etc
12 DIFFERENTIAL DIAGNOSIS ACTINIC KERATOSIS BCC MELANOMA KERATOACANTHOMA PYODERMA GANGRENOSUM WARTS INVESTIGATIONS CT, MRI, DEPTH OF INVASION BIOPSY : PUNCH, SHAVE, INCISIONAL, EXCISIONAL HISTOLOGY NEST OF EPIDERMAL CELLS MIXTURE OF NORMAL AND ANAPLASTIC CELLS WELL DIFFERENTIATED EPITHELIAL PEARL CONCENTRIC LAYERS OF SQUAMOUS CELLS WITH CENTRAL KERANTINIZATION POORLY DIFFERENTIATED LACKS HORN PEARLS SPECIAL STAINS : S100 NEGATIVE FOR SCC POSITIVE FOR MELANOMA
13 STAGING TNM PRIMARY TUMOUR Tx PRIMARY TUMOUR CANNOT BE ASSESSED To NO EVDIENCE OF PRIMARY TUMOUR T 1 TUMOUR 2 cm T 2 TUMOUR 2 4 cm T3 TUMOUR LARGER THAN 4 cm T4 TUMOUR INVADES DEEPER STRUCTURES REGIONAL NODES N X NODES CANNOT BE ASSESSED N0 NO NODES N1 SINGLE IPSILATERAL NODE 3 cm N2 a) SINGLE b) MULTIPLE c) BILATERAL METASTASIS M X DISTANT METASTASIS CANNOT BE ASSESSED M0 NO DISTANT METASTASIS M1 DISTANT METASTASIS PRESENT
14 TREATMENT : DRUG THERAPY ACTINIC KERATOSIS 5 FLUORORACIL TOPICAL DICLOFENAC GEL BIOPSY CONFIRMATION SCC/BCC IMIQUIMOD 5 % CREAM SUPERFICIAL IMMUNE MODIFIER THROUGH LESIONS ONLY INTERFERON, CYTOKINES PHOTODYNAMIC THERPAY (PDT) PHOTOSENSITIZING DRUGS LIGHT ACTIVATES OXYGEN, FREE RADICALS DESTROY, TARGETED TISSUE. ALA AMINOLEVULINIC ACID SKIN TUMOURS ACTIVE PROTOPORPHYRIN IX ACTINIC KERATOSIS, FACIAL LESION 90 %
15 SURGICAL TREATMENT CURETTAGE AND ELECTROSURGERY REPEATED SEVERAL TIMES NO SPECIMEN AVAILABLE FOR HPE 96 % CURE CRYOSURGERY LIQUID NITROGEN CURE 97 % EXCISION LOCAL EXCISION HPE 92 % CURE 4 mm MARGIN RECURRENCE 5 8 % WELL DIFFERENTIATED LESIONS MOH S MICROGRAPHIC SURGERY LESIONS ARE REMOVED IN STAGES HORIZONTAL FROZEN SECTIONING PERIPHERAL AND DEEP MARGINS
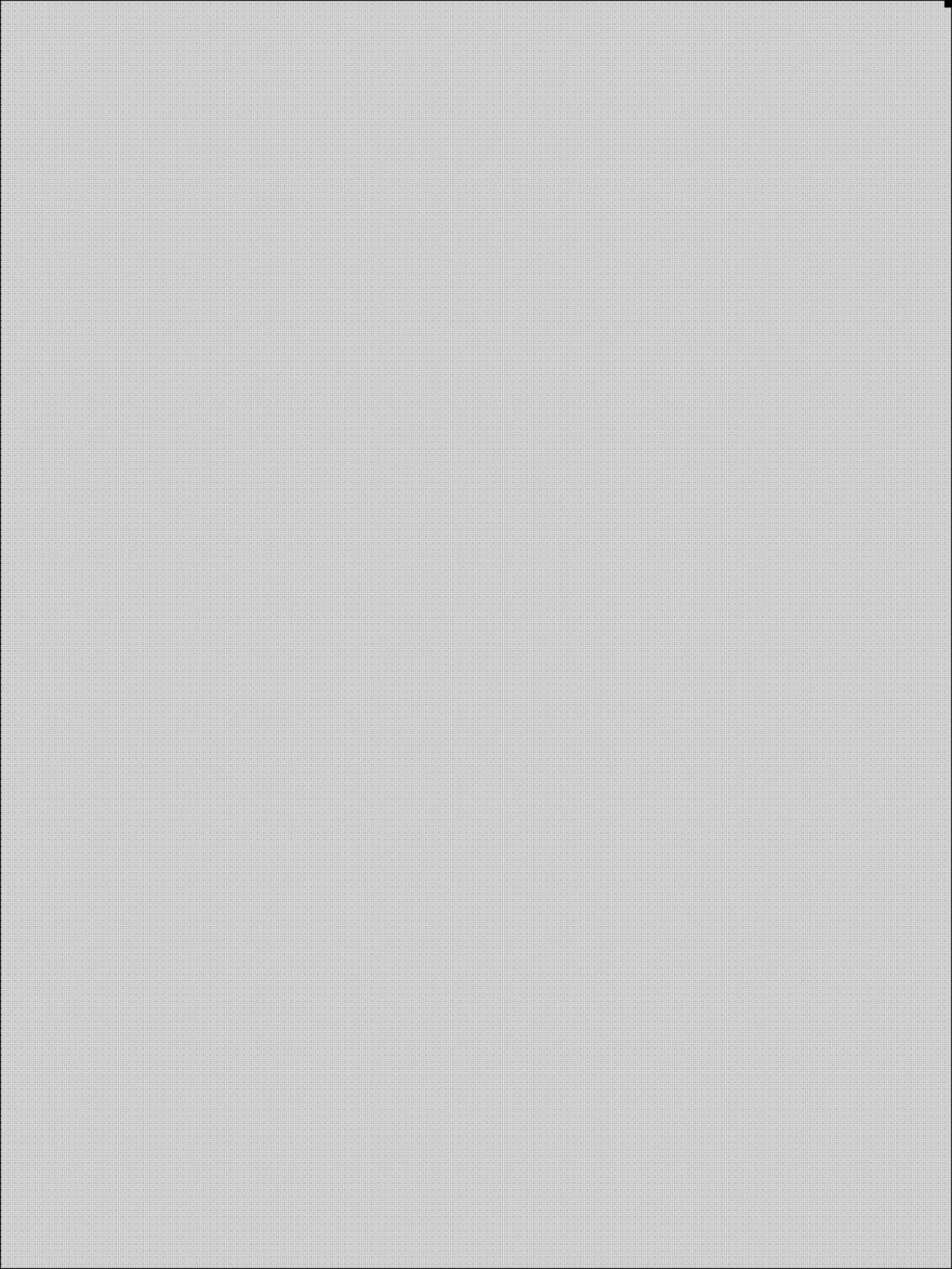
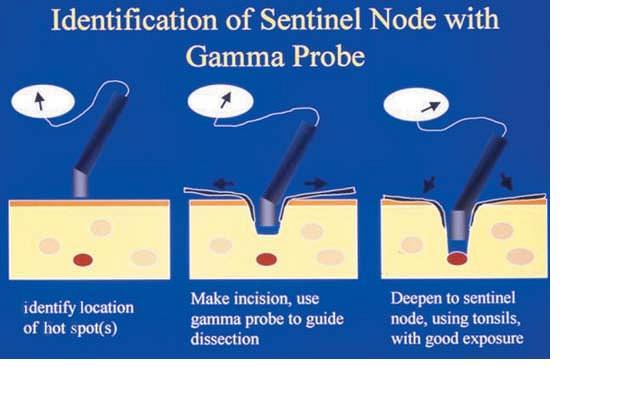
16 CURE RATE SCC 96 % IN 5 YEARS FOR RECURRENT SCC 90 % CURE RATE TISSUE SPARING DISFIGUREMENT IN DISTINCT MARGIN, GENITAL PENILE SHAFT LOCAL ANAESTHESIA, SAY CASE OF SURGERY COST EFFECTIVE MOH S SURGERY NOT USEFUL IN INVASIVE LESIONS SENTINEL NODE BIOPSY LASER SURGERY RADIATION THERAPY OLDER PATIENT, NO HPE PREVENTION SPF SUN PROTECTING FACTOR CLOTHING SUNSCREEN S SPR 30 ZINC OXIDE, TITANIUM OXIDE APPLIED EVERY 30 MINTS DURING EXPOSURE
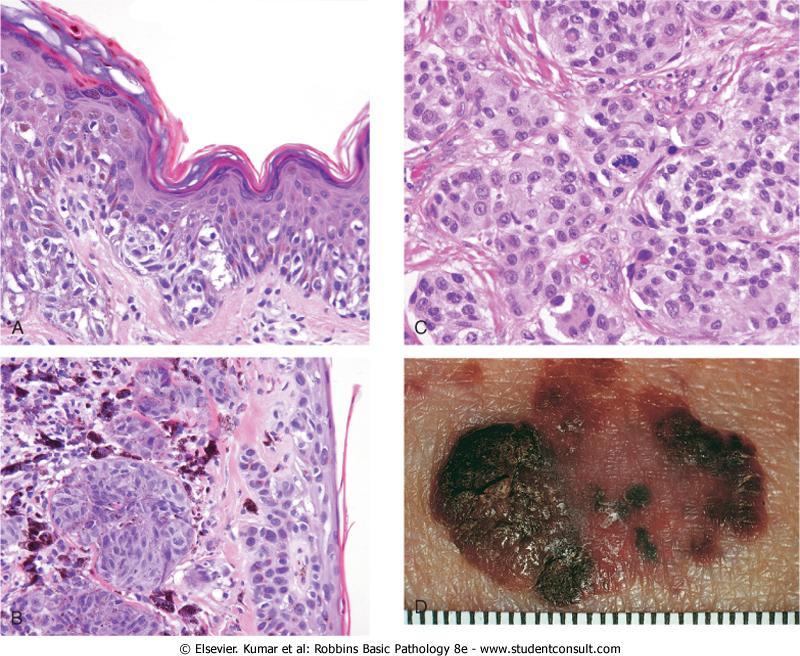
17 MALIGNANT MELANOMA MALIGNANT TRANFORMATION OF MELANOCYTES MELANOCYTES DERIVED FROM NEURAL CREST SKIN, GIT, BRAIN ADULTS WHITE POPULATION HIGHEST ASIAN S LOWEST ETIOLOGY FAMILY HISTORY POSITIVE IN 5 10 % PERSONAL BLUE EYES, FAIR SUN BURN FRECKLING NEVI DYSPLASTIC IMMUNOSUPPRESSIVE STATE
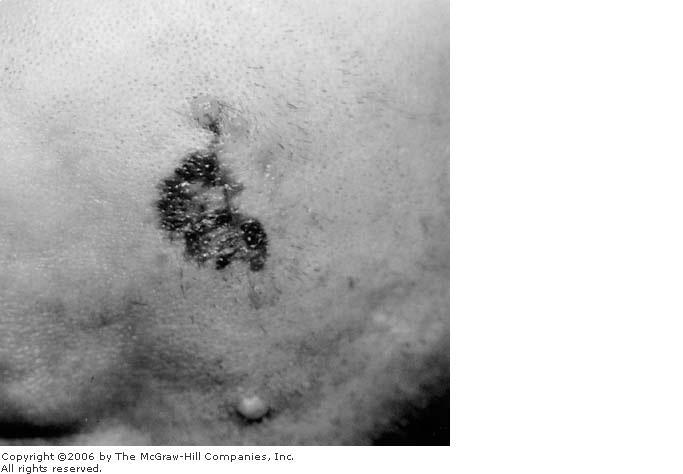
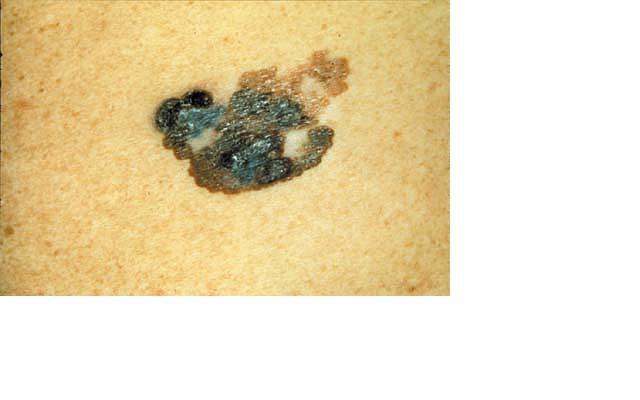
18 SUN EXPOSURE HIGH U V RADIATION LOW LATITUDE BLISTERING SUN BURNS DYSPLASTIC NEVI OVER A TIME MELANOMA CLINICAL PRESENTATION ABCDE A ASYMMETRY B BORDER IRREGULAR C COLOUR VARIATION D DIAMETER > 6 cm E ELEVATED SURFACE ITCHING, BLEED, ULCERATION, SATELITE LESIONS BIOPSY: EXCISION / INCISION, 2 mm MARGIN FULL THICKNESS SKIN
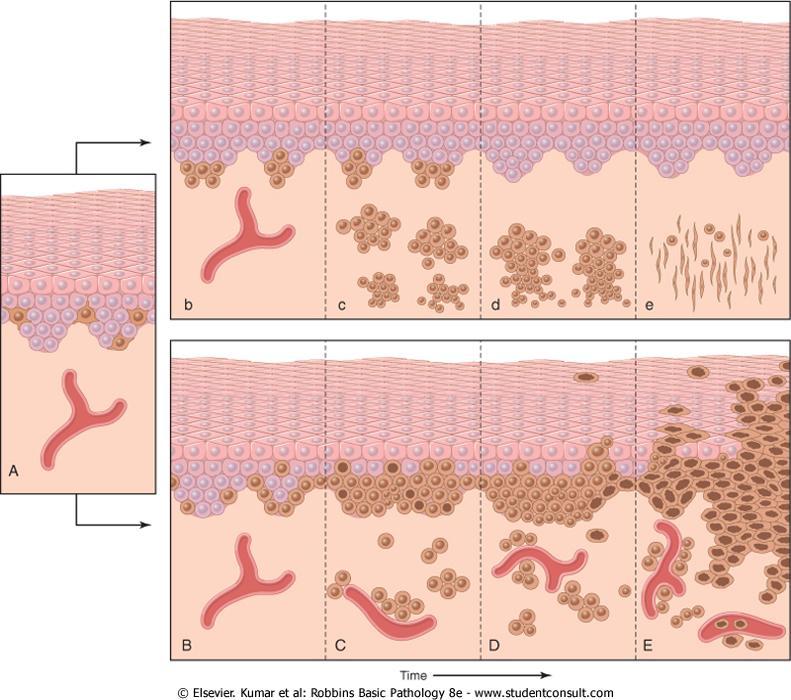
19 SAPPEY : LYMPHATIC DRAINAGE DEPEND ON ANATOMICAL LOCATION LYMPHATIC OVER LAP HISTOLOGICAL CLASSIFICATION GROWTH PATTERN SUPERFICIAL SPREADING 70 % OF MELANOMA CELLS AT DERMS EPIDERAL JUNCTION MIGRATE TO S.GRANULOSUM & CORNEUM PAPPILARY DERMIS FROM DYSPLATIC NEVUS FLAT, ELEVATED LATTER 2 cm DIAMETER, VARIGATED COLOURS NODULAR MELANOMA EXTENSIVE VERTICAL GROWTH INTO DERMIS THAN RADIAL
20
21
22
23
24

25
26
27
28 15 30 % BLUE BLACK OCCUR WITHOUT PRE EXISTING LESION LENTIGO MALGNA MELANOMA 4 10 % MELANOMA SPINDLE SHAPE HYPERCHROMATIC CELLS EPIDERMIS ATROPHIC SIZE 3 cms, FLAT, FRECKLE, FACE, NECK ARISE IN HUTCHINSON S FRECKLE (LENTIGO MALIGNA) ACRAL LENTIGINOUS MELANOMA 2 8% IN WHITE 30 60% IN DARK SKINNED PEOPLE DERMO EPIODERMAL JUNCTION INVASION PAPILLAR DERMIS PALMS, SOLES, FLAT IRREGULAR BORDERS ULCERATIONS
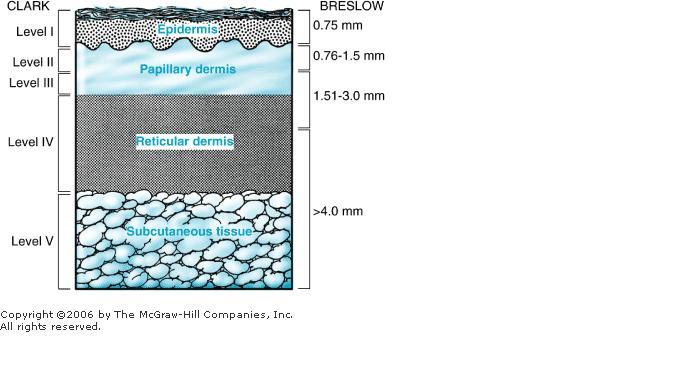
29 DESMOPLASTIC MELANOMA 1% RARE PERI NEURAL INVASION HIGHER LOCAL RECURRENCE LOWER REGIONAL METASTASIS CLASSIFICATION AND STAGING BRESLOW S THICKNESS 0.75 mm or LESS THICKNESS mm THICKNESS mm THICKNESS > 4 mm
30 CLARK LEVEL I INVOLVES EPIDERMIS ONLY IN SITU LEVEL II INVADES PAPILLARY DERMIS ONLY LEVEL II INVADES PAPILLART & INTERFACE LEVEL IV INVADER RETICULAR DERMIS NOT SUB CUTANEOUS TISSUE LEVEL V INVADES INTO SUB CUTAEOUS TISSUE TNM STAGING T X PRIMARY TUMOUR CANNOT BE ASSESSED
31
32 T0 NO EVIDENCE TUMOUR T15 IN SITU INVOLVES ONLY EPIDERMIS T1 1 mm LESS THICKNESS T mm LESS THICKNESS T3 2 4 mm LESS THICKNESS T4 > 4 mm, INVADES SUB CUTANEOUS TISSUE SATELLITE TUMOURS WITHIN 2 cm a) TUMOUR > 4 mm b) WITHOUT ULCERATION c) ULERATION REGIONAL NODES NX CANNOT BE ASSESSED N0 NO REGIONAL NODE METS
33 N1 ONE NODE N2 2 3 NODES N3 4 OR MORE DISTANT METASTASIS MX DISTANT METASTASIS CANNOT BE ASSESSED M0 NO DISTANT METS M1 DISTANT METASTASIS a) SUB CUTANEOUS TISSUE, NODES b) METASTASIS TO LUNG c) METASTASIS TO OTHER ORGANS
34 MEDICAL MANAGEMENT INTERFERON (α 2BIFN) STAGE III MELANOMA TOXIC RELAPSE REDUCED GM CSF (GRANULOCYTE STIMULATING FACTOR) STIMULATES IMMUNE SYSTEM NOT TOXIC AND OVER ALL SURVIVAL STAGE III & IV PALLIATION ONLY CYTOKINE AND VACCINE THERAPY TUMOUR SPECIFIC TARGETS ONCOGENE
35 CDK4, TRP 2, MART 1 AUTOLOGOUS (ALLOGENIC) CHEMOTHERAPY TEMOZOLOMIDE DACARBAZINE SURGICAL TREATMENT STAGE O : 0.5 % TO 1.5 % cm MARGIN EXCISION IN SITU/OBSERVATION STAGE I : T₁ LESION 1 TO 2 cms MARGIN SENTINEL NODE BIOPSY CLOSURE PRIMARY, SKIN GRAFTING
36 STAGE II 2 cms MARGIN NO ADVANTAGE IN 4 6 cms MARGINS LYMPH ADENCTOMY SENTINEL NODE BIOPSY IN NO NODES CLINICALLY HYPERTHERMIC ARTERIAL LIMB PERFUSION MELPHALAN ADJUVANT THERPAY STAGE III 2 cm MARGIN REGIONAL LYMPHADENOCTOMY STAGE IV REFRACTORY CONSIDER FOR CLINICAL TRIALS DTC, BCNU RADIATION
37
38

39 THANK YOU
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Clinical characteristics
 Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer. 5 Warning Signs. American Osteopathic College of Occupational and Preventive Medicine OMED 2012, San Diego, Monday, October 8, 2012 C-1
 Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Learning Objectives. Tanning. The Skin. Classic Features. Sun Reactive Skin Type Classification. Skin Cancers: Preventing, Screening and Treating
 Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Periocular Malignancies
 Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY
 IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Cutaneous Malignancies: A Primer COPYRIGHT. Marissa Heller, M.D.
 Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012
 Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Living Beyond Cancer Skin Cancer Detection and Prevention
 Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
Skin Cancer 101: Diagnosis and Management of the Most Common Cancer
 Skin Cancer 101: Diagnosis and Management of the Most Common Cancer Sarah Patton, PA-C, MSHS Skin Surgery Center www.skinsurgerycenter.com Seattle/Bellevue, WA Skin cancer Skin cancer is by far the most
Skin Cancer 101: Diagnosis and Management of the Most Common Cancer Sarah Patton, PA-C, MSHS Skin Surgery Center www.skinsurgerycenter.com Seattle/Bellevue, WA Skin cancer Skin cancer is by far the most
 Page 1 of 15 Title Authored By Course No Contact Hours 2 Skin Cancer the Real Picture for Early Detection and Treatment Cheryl Sommer RN, MSN, ARNP SC120604 Purpose The purpose of this course is to provide
Page 1 of 15 Title Authored By Course No Contact Hours 2 Skin Cancer the Real Picture for Early Detection and Treatment Cheryl Sommer RN, MSN, ARNP SC120604 Purpose The purpose of this course is to provide
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Malignant Melanoma Early Stage. A guide for patients
 This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
Melanoma: The Basics. What is a melanocyte?
 Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
SKIN CANCER. Most common cancer diagnosis 40% of all cancers
 SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT
 LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
Dermatological Manifestations in the Elderly. Sanjay Siddha Staff Dermatologist UHN & MSH
 Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
General information about skin cancer
 Skin Cancer General information about skin cancer Key points Skin cancer is a disease in which malignant (cancer) cells form in the tissues of the skin. There are different types of cancer that start in
Skin Cancer General information about skin cancer Key points Skin cancer is a disease in which malignant (cancer) cells form in the tissues of the skin. There are different types of cancer that start in
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Glenn D. Goldman, MD. University of Vermont Medical Center. University of Vermont College of Medicine
 Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Skin Cancer - Non-Melanoma
 Skin Cancer - Non-Melanoma Introduction Each year, millions of people find out that they have skin cancer. Skin cancer is almost 100% curable if found early and treated right away. It is possible to prevent
Skin Cancer - Non-Melanoma Introduction Each year, millions of people find out that they have skin cancer. Skin cancer is almost 100% curable if found early and treated right away. It is possible to prevent
Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest risk.
 Basics of Skin Cancer Detection and Treatment of Non- Melanoma Skin Cancers Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest
Basics of Skin Cancer Detection and Treatment of Non- Melanoma Skin Cancers Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Skin Cancers Emerging Trends and Treatment Approaches
 Skin Cancers Emerging Trends and Treatment Approaches Andrei Metelitsa, MD, FRCPC, FAAD Clinical Associate Professor, Dermatology, U of C Co-Director, Institute for Skin Advancement Copyright 2017 by Sea
Skin Cancers Emerging Trends and Treatment Approaches Andrei Metelitsa, MD, FRCPC, FAAD Clinical Associate Professor, Dermatology, U of C Co-Director, Institute for Skin Advancement Copyright 2017 by Sea
Common Benign Lesions and Skin Cancers. 22nd May 2015 Dr Mark Foley
 Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee
 I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee Some thoughts Is this skin cancer? How common is this? How likely is this in this patient? What happens next if it s something
I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee Some thoughts Is this skin cancer? How common is this? How likely is this in this patient? What happens next if it s something
Glenn D. Goldman, MD. Fletcher Allen Health Care. University of Vermont College of Medicine
 Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses
 Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
An Overview of Melanoma. Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center
 An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Malignant tumors of melanocytes : Part 3. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Malignant tumors of melanocytes: Part 1. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Technicians & Nurses Program
 ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
Periocular skin cancer
 Periocular skin cancer Information for patients Skin cancer involving the skin of the eyelid or around the eye is called a periocular skin cancer. Eyelid skin cancers occur most often on the lower eyelid,
Periocular skin cancer Information for patients Skin cancer involving the skin of the eyelid or around the eye is called a periocular skin cancer. Eyelid skin cancers occur most often on the lower eyelid,
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
NAACCR Hospital Registry Webinar Series
 NAACCR Hospital Registry Webinar Series October 4, 2007 Abstracting Melanoma Cancer Incidence and Treatment Data Image source: commons.wikimedia.org/wiki/image.melanoma.jpg Sites include Melanoma Skin
NAACCR Hospital Registry Webinar Series October 4, 2007 Abstracting Melanoma Cancer Incidence and Treatment Data Image source: commons.wikimedia.org/wiki/image.melanoma.jpg Sites include Melanoma Skin
1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter.
 Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CH 05 THE INTEGUMENTARY SYSTEM
 CH 05 THE INTEGUMENTARY SYSTEM This system consists of skin and its derivatives. The skin is one of the largest organs of the body in terms of surface area. The functions of the integumentary system include:
CH 05 THE INTEGUMENTARY SYSTEM This system consists of skin and its derivatives. The skin is one of the largest organs of the body in terms of surface area. The functions of the integumentary system include:
Disclosures. I have no conflicts of interest to disclose
 Disclosures I have no conflicts of interest to disclose Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco 2
Disclosures I have no conflicts of interest to disclose Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco 2
Skin lesions The Good and the Bad. Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry
 Skin lesions The Good and the Bad Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry Case 1 32 year old woman Australian Lesion on back New hair growing
Skin lesions The Good and the Bad Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry Case 1 32 year old woman Australian Lesion on back New hair growing
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 12, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Integumentary System
 Integumentary System The integumentary system is commonly known as the Skin Largest organ of human body 10% total body weight and would cover over 20 square feet Functions of Skin 1. Protection Barrier
Integumentary System The integumentary system is commonly known as the Skin Largest organ of human body 10% total body weight and would cover over 20 square feet Functions of Skin 1. Protection Barrier
Disclosures. Melanoma and Non melanoma Skin Cancer: What You Need to Know. I have no conflicts of interest to disclose
 Disclosures Melanoma and Non melanoma Skin Cancer: What You Need to Know I have no conflicts of interest to disclose Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department
Disclosures Melanoma and Non melanoma Skin Cancer: What You Need to Know I have no conflicts of interest to disclose Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department
Springer Healthcare. Staging and Diagnosing Cutaneous Melanoma. Concise Reference. Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone
 Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Mohs surgery for the nail unit
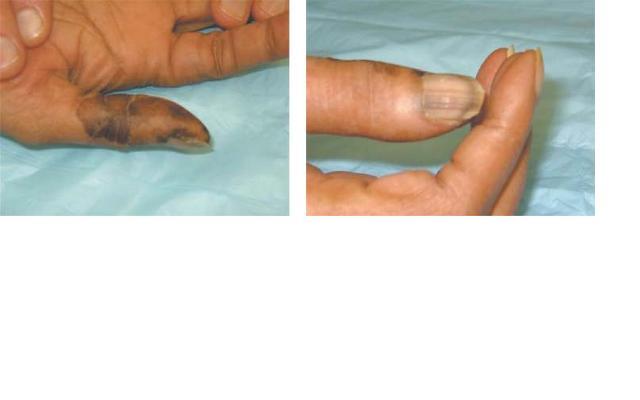
 Mohs surgery for the nail unit olivier.cogrel@chu-bordeaux.fr Dermatologic surgery, Mohs surgery and lasers unit CHU Bordeaux, France Squamous cell carcinoma +++ Acral lentiginous melanoma Lichte et al.
Mohs surgery for the nail unit olivier.cogrel@chu-bordeaux.fr Dermatologic surgery, Mohs surgery and lasers unit CHU Bordeaux, France Squamous cell carcinoma +++ Acral lentiginous melanoma Lichte et al.
Lumps and Bumps: An Organized Approach to Diagnosis and Management. Disclosure. Introduction. References. Structure of Skin.
 Lumps and Bumps: An Organized Approach to Diagnosis and Management Nothing to disclose Disclosure Tammy Pifer Than, MS, OD, FAAO Carl Vinson VAMC tammythan@bellsouth.net References Fitzpatrick's Color
Lumps and Bumps: An Organized Approach to Diagnosis and Management Nothing to disclose Disclosure Tammy Pifer Than, MS, OD, FAAO Carl Vinson VAMC tammythan@bellsouth.net References Fitzpatrick's Color
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Subject Index. Dry desquamation, see Skin reactions, radiotherapy
 Subject Index Actinic keratosis disseminated disease 42 surgical excision 42 AIDS, see Kaposi s sarcoma Amifostine, skin reaction prophylaxis 111 Basal cell carcinoma, superficial X-ray therapy Bowen s
Subject Index Actinic keratosis disseminated disease 42 surgical excision 42 AIDS, see Kaposi s sarcoma Amifostine, skin reaction prophylaxis 111 Basal cell carcinoma, superficial X-ray therapy Bowen s
Identifying Benign and Malignant Skin Lesions. No Disclosures. Common Benign Lesions. Benign Lesions 2/25/2018. Stucco Keratoses.
 Dermatology in Primary Care Identifying Benign and Malignant Skin Lesions Christy Quire Baker, APRN, FNP-BC, DCNP Dermatology Certified Nurse Practitioner No Disclosures Common Benign Lesions Seborrheic
Dermatology in Primary Care Identifying Benign and Malignant Skin Lesions Christy Quire Baker, APRN, FNP-BC, DCNP Dermatology Certified Nurse Practitioner No Disclosures Common Benign Lesions Seborrheic
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 13, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Human Anatomy & Physiology
 PowerPoint Lecture Slides prepared by Barbara Heard, Atlantic Cape Community College Ninth Edition Human Anatomy & Physiology C H A P T E R 5 Annie Leibovitz/Contact Press Images 2013 Pearson Education,
PowerPoint Lecture Slides prepared by Barbara Heard, Atlantic Cape Community College Ninth Edition Human Anatomy & Physiology C H A P T E R 5 Annie Leibovitz/Contact Press Images 2013 Pearson Education,
Interesting Case Series. Aggressive Tumor of the Midface
 Interesting Case Series Aggressive Tumor of the Midface Adrian Frunza, MD, Dragos Slavescu, MD, and Ioan Lascar, MD, PhD Bucharest Emergency Clinical Hospital, Bucharest University School of Medicine,
Interesting Case Series Aggressive Tumor of the Midface Adrian Frunza, MD, Dragos Slavescu, MD, and Ioan Lascar, MD, PhD Bucharest Emergency Clinical Hospital, Bucharest University School of Medicine,
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial
 Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Non-melanoma Skin Cancer
 Non-melanoma Skin Cancer Understanding your diagnosis 1 888 939-3333 cancer.ca Non-melanoma Skin Cancer Understanding your diagnosis When you first hear that you have cancer, you may feel alone and afraid.
Non-melanoma Skin Cancer Understanding your diagnosis 1 888 939-3333 cancer.ca Non-melanoma Skin Cancer Understanding your diagnosis When you first hear that you have cancer, you may feel alone and afraid.
NAACCR Webinar Series 1
 Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES OCULAR ONCOLOGY PERIOCULAR CUTANEOUS MALIGNANCY Site Group: Ocular Periocular Cutaneous Malignancies Prepared by: Harmeet S. Gill MD, FRCSC
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES OCULAR ONCOLOGY PERIOCULAR CUTANEOUS MALIGNANCY Site Group: Ocular Periocular Cutaneous Malignancies Prepared by: Harmeet S. Gill MD, FRCSC
Exenteration. Introduction. The skin. Epidermal malignancies 8/3/2017. Neglected basal cell carcinoma
 Jeremiah Tao, MD, FACS Director, Oculoplastic and Orbital Surgery Associate Professor, UC Irvine Neglected basal cell carcinoma Exenteration Introduction Chief question with any eyelid lesion: Suspicious
Jeremiah Tao, MD, FACS Director, Oculoplastic and Orbital Surgery Associate Professor, UC Irvine Neglected basal cell carcinoma Exenteration Introduction Chief question with any eyelid lesion: Suspicious
Metastatic Melanoma. Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds
 Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
MOHS MICROGRAPHIC SURGERY: AN OVERVIEW
 MOHS MICROGRAPHIC SURGERY: AN OVERVIEW SKIN CANCER: Skin cancer is far and away the most common malignant tumor found in humans. The most frequent types of skin cancer are basal cell carcinoma, squamous
MOHS MICROGRAPHIC SURGERY: AN OVERVIEW SKIN CANCER: Skin cancer is far and away the most common malignant tumor found in humans. The most frequent types of skin cancer are basal cell carcinoma, squamous
Nonmelanoma skin cancers
 Skin cancer Philip Clarke Nonmelanoma skin cancers Treatment options Background Australia has one of the highest skin cancer rates in the world. Early detection and treatment of skin cancer is vital to
Skin cancer Philip Clarke Nonmelanoma skin cancers Treatment options Background Australia has one of the highest skin cancer rates in the world. Early detection and treatment of skin cancer is vital to
Clinical Pathological Conference. Malignant Melanoma of the Vulva
 Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Dual Wavelength Phototherapy System
 Dual Wavelength Phototherapy System The AKLARUS Blue and Red Combination System is an effective, drugfree alternative for treating acne & photodamaged skin. The non-invasive Aklarus treatment has been
Dual Wavelength Phototherapy System The AKLARUS Blue and Red Combination System is an effective, drugfree alternative for treating acne & photodamaged skin. The non-invasive Aklarus treatment has been
Describe the functions of the vertebrate integumentary system. Discuss the structure of the skin and how it relates to function.
 Chapter 5 Describe the functions of the vertebrate integumentary system. Discuss the structure of the skin and how it relates to function. Explain the basis for different skin colors. Describe the structure
Chapter 5 Describe the functions of the vertebrate integumentary system. Discuss the structure of the skin and how it relates to function. Explain the basis for different skin colors. Describe the structure
Malignant Cutaneous Neoplasms
 Malignant Cutaneous Neoplasms Kathleen Haycraft, DNP, FNP/PNP-BC, DCNP All slides Kathleen Haycraft Objectives: 1. Identify common cutaneous malignant neoplasms. 2. Identify the etiology, pathophysiology
Malignant Cutaneous Neoplasms Kathleen Haycraft, DNP, FNP/PNP-BC, DCNP All slides Kathleen Haycraft Objectives: 1. Identify common cutaneous malignant neoplasms. 2. Identify the etiology, pathophysiology
SKIN. 3. How is the skin structured around the finger joints to allow for flexible movement of the fingers?
 SKIN Objectives for Exam #1: 1. List various skin structures and describe their functions. 2. Describe skin responses to increases and decreases in body temperature. 3. Provide examples of various skin
SKIN Objectives for Exam #1: 1. List various skin structures and describe their functions. 2. Describe skin responses to increases and decreases in body temperature. 3. Provide examples of various skin
Pathology. Skin Tumor. Bayan N. Mohammad 15/10/2015. Mohammad al-orjani. Page 0 of 23
 #7 35 Pathology Skin Tumor Bayan N. Mohammad 15/10/2015 Mohammad al-orjani Page 0 of 23 بسم هللا الرحمن الرحيم GREETINGS This lecture is about skin tumors, all the slides are included and every slide will
#7 35 Pathology Skin Tumor Bayan N. Mohammad 15/10/2015 Mohammad al-orjani Page 0 of 23 بسم هللا الرحمن الرحيم GREETINGS This lecture is about skin tumors, all the slides are included and every slide will
The Integumentary System
 The Integumentary System The Integumentary System Integument is skin Skin and its appendages make up the integumentary system (See if you can name some appendages) A fatty layer (hypodermis) lies deep
The Integumentary System The Integumentary System Integument is skin Skin and its appendages make up the integumentary system (See if you can name some appendages) A fatty layer (hypodermis) lies deep
Index. Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, Anorectal melanoma RT for, 1035
 Index Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, 947 948 Anorectal melanoma RT for, 1035 B Bacille Calmette-Guerin (BCG) in melanoma, 1008 BCG. See Bacille
Index Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, 947 948 Anorectal melanoma RT for, 1035 B Bacille Calmette-Guerin (BCG) in melanoma, 1008 BCG. See Bacille
CHAPTER 5 INTEGUMENTARY
 CHAPTER 5 INTEGUMENTARY skin under the skin other stuff cutaneous layer hypodermis (subcutaneous) accessory structures Cutaneous layer = skin epithelial layers = connective tissue layer = dermis Subcutaneous
CHAPTER 5 INTEGUMENTARY skin under the skin other stuff cutaneous layer hypodermis (subcutaneous) accessory structures Cutaneous layer = skin epithelial layers = connective tissue layer = dermis Subcutaneous
Skin and Body Membranes Body Membranes Function of body membranes Cover body surfaces Line body cavities Form protective sheets around organs
 Skin and Body Membranes Body Membranes Function of body membranes Cover body surfaces Line body cavities Form protective sheets around organs Classification of Body Membranes Epithelial membranes Cutaneous
Skin and Body Membranes Body Membranes Function of body membranes Cover body surfaces Line body cavities Form protective sheets around organs Classification of Body Membranes Epithelial membranes Cutaneous
Skin and Body Membranes
 4 Skin and Body Membranes PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB Skin and Body Membranes
4 Skin and Body Membranes PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB Skin and Body Membranes
Skin Cancer of the Nose: Common and Uncommon
 Skin Cancer of the Nose: Common and Uncommon Mark Russell, M.D. Associate Professor of Dermatology, Otolaryngology, and Pathology University of Virginia Objectives Review clinical presentations of select
Skin Cancer of the Nose: Common and Uncommon Mark Russell, M.D. Associate Professor of Dermatology, Otolaryngology, and Pathology University of Virginia Objectives Review clinical presentations of select
Oral and Maxillofacial Surgery Department
 Oral and Maxillofacial Surgery Department This leaflet explains: Lentigo Maligna What are the aims of this leaflet? This leaflet has been written to help you understand more about lentigo maligna and melanoma
Oral and Maxillofacial Surgery Department This leaflet explains: Lentigo Maligna What are the aims of this leaflet? This leaflet has been written to help you understand more about lentigo maligna and melanoma
WHAT DOES THE PATHOLOGY REPORT MEAN?
 Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Skin Cancer. There are many types of diseases. From a simple cold to the deadly disease
 Skin Cancer Skin Cancer 1 There are many types of diseases. From a simple cold to the deadly disease Mesothelioma. Some diseases are almost harmless and some can kill you in less than a year. There are
Skin Cancer Skin Cancer 1 There are many types of diseases. From a simple cold to the deadly disease Mesothelioma. Some diseases are almost harmless and some can kill you in less than a year. There are
Histopathology of Melanoma
 THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
Skin Malignancies. Presented by Dr. Douglas Paauw
 Skin Malignancies Presented by Dr. Douglas Paauw Disclosure: Dr. Paauw has no significant financial interest in any of the products or manufacturers mentioned. How Common Is Skin Cancer? *½ of all White
Skin Malignancies Presented by Dr. Douglas Paauw Disclosure: Dr. Paauw has no significant financial interest in any of the products or manufacturers mentioned. How Common Is Skin Cancer? *½ of all White
Patient Guide. The precise answer for tackling skin cancer. Brachytherapy: Because life is for living
 Patient Guide Brachytherapy: The precise answer for tackling skin cancer Because life is for living Overview of skin cancer Skin cancer is the most common cancer worldwide. In fact more people are diagnosed
Patient Guide Brachytherapy: The precise answer for tackling skin cancer Because life is for living Overview of skin cancer Skin cancer is the most common cancer worldwide. In fact more people are diagnosed
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
Due next week in lab - Scientific America Article Select one article to read and complete article summary
 Due in Lab 1. Skeletal System 33-34 2. Skeletal System 26 3. PreLab 6 Due next week in lab - Scientific America Article Select one article to read and complete article summary Cell Defenses and the Sunshine
Due in Lab 1. Skeletal System 33-34 2. Skeletal System 26 3. PreLab 6 Due next week in lab - Scientific America Article Select one article to read and complete article summary Cell Defenses and the Sunshine
SKIN HISTOLOGY the microscopic anatomy of the Integument. Mikrogeo. com
 SKIN HISTOLOGY the microscopic anatomy of the Integument Mikrogeo. com Hair follicles, sweat glands, sebaceous glands (even teeth) are products of the epidermis,embryologically speaking ectododerm, that
SKIN HISTOLOGY the microscopic anatomy of the Integument Mikrogeo. com Hair follicles, sweat glands, sebaceous glands (even teeth) are products of the epidermis,embryologically speaking ectododerm, that
4 Skin and Body Membranes Study Guide
 Name: SKIN AND BODY MEMBRANES: 4 Skin and Body Membranes Study Guide Period: Body membranes, which cover body surfaces, line its cavities, and form protective sheets around organs, fall into two major
Name: SKIN AND BODY MEMBRANES: 4 Skin and Body Membranes Study Guide Period: Body membranes, which cover body surfaces, line its cavities, and form protective sheets around organs, fall into two major
Unit 4 - The Skin and Body Membranes 1
 Unit 4 - The Skin and Body Membranes 1 I. Unit 4: Skin and Body Membranes A. Body Membranes 1. Function of body membranes a) Cover body surfaces b) Line body cavities c) Form protective sheets around organs
Unit 4 - The Skin and Body Membranes 1 I. Unit 4: Skin and Body Membranes A. Body Membranes 1. Function of body membranes a) Cover body surfaces b) Line body cavities c) Form protective sheets around organs
Review of Cutaneous Malignancies
 Review of Cutaneous Malignancies Tanya Nino, MD Department of Dermatology Did You Know? More than 3.5 million skin cancers are diagnosed in the US annually Melanoma incidence rates have been increasing
Review of Cutaneous Malignancies Tanya Nino, MD Department of Dermatology Did You Know? More than 3.5 million skin cancers are diagnosed in the US annually Melanoma incidence rates have been increasing
Integumentary System-Skin and Body Coverings
 Integumentary System-Skin and Body Coverings List the four types of epithelial or connective membranes. The epithelial cutaneous includes your and is exposed to the. Its function is to. An example is..
Integumentary System-Skin and Body Coverings List the four types of epithelial or connective membranes. The epithelial cutaneous includes your and is exposed to the. Its function is to. An example is..
Melanoma and Dermoscopy. Disclosure Statement: ABCDE's of melanoma. Co-President, Usatine Media
 Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas