Galafold (migalastat) or Fabrazyme (agalsidase beta) Prior Authorization Criteria:
|
|
|
- Daisy Washington
- 5 years ago
- Views:
Transcription
1 Request for Prior Authorization for Fabry Disease Medications Website Form Submit request via: Fax All requests for Galafold (migalastat) or Fabrazyme (agalsidase beta) require a Prior Authorization and will be screened for medical necessity and appropriateness using the criteria listed below. Galafold (migalastat) or Fabrazyme (agalsidase beta) Prior Authorization Criteria: Disclaimer: All requests for Galafold (migalastat) or Fabrazyme (agalsidase beta) require a prior authorization and will be screened for medical necessity and appropriateness using the criteria listed below. For all requests for Fabrazyme (agalsidase beta) all of the following criteria must be met: Coverage may be provided with a diagnosis of Fabry Disease and the following criteria is met: Member is age 8 years of age or older Diagnosis has been confirmed by biochemical/genetic confirmation by ONE of the following: o α-galactosidase A (α-gal A) activity in plasma, isolated leukocytes, and/or cultured cells. o Plasma or urinary globotriaosylceramide(gb3/gl-3) or globotriaosylsphingosine (lyso-gb3). o Detection of pathogenic mutations in the GALA/GLA gene by molecular genetic testing. Medication must be prescribed by or in association with a dermatologist, neurologist, nephrologist, rheumatologist, or cardiologist. The requested dose and frequency is in accordance with FDA-approved labeling, nationally recognized compendia, and/or evidence-based practice guidelines Member has medical history of at least ONE of the following: o Intermittent episodes of burning pain in the extremities (acroparesthesias) o Cutaneous vascular lesions (angiokeratomas) o Diminished perspiration (hypo- or anhidrosis) o Characteristic corneal and lenticular opacities o Abdominal pain, nausea, and/or diarrhea of unknown etiology in young adulthood o Left ventricular hypertrophy (LVH) or hypertrophic cardiomyopathy of unknown etiology, particularly in young adults o Arrhythmias of unknown etiology, particularly in young adults o Stroke of unknown etiology at any age o Chronic kidney disease (CKD) and/or proteinuria of unknown etiology o Multiple renal sinus cysts discovered incidentally o Family history suggestive of the disorder (ie, history of unexplained gastrointestinal symptoms, extremity pain, and/or kidney disease, ischemic stroke, or cardiac disease in one or more family members) Initial Duration of Approval: 12 months
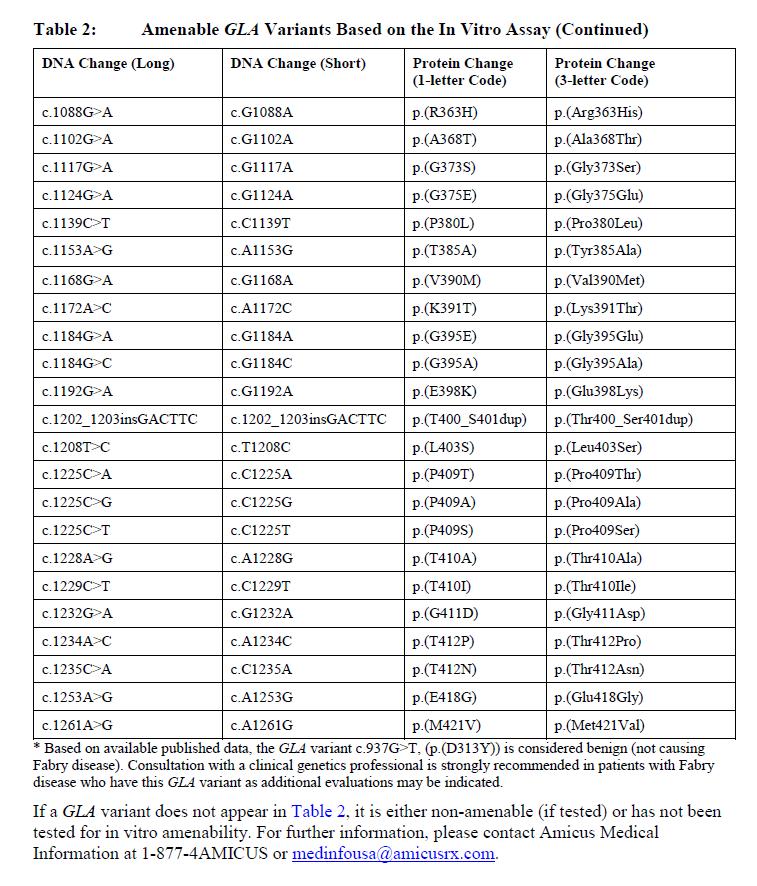
2 Updated: 09/2018 o Documentation of baseline values for plasma GL-3 and/or GL-3 inclusions o Documentation of improved values for plasma GL-3 and/or GL-3 inclusions defined by a reduction in plasma GL-3 and/or GL-3 inclusion compared to pretreatment baseline. Reauthorization Duration of approval: 12 months For all requests for Galafold (migalastat) all of the following criteria must be met: Coverage may be provided with a diagnosis of a confirmed diagnosis of Fabry disease and the following criteria is met: Member must be 18 years or older Member must have amenable GLA variant that is interpreted by a clinical genetics professional as causing Fabry disease (pathogenic, likely pathogenic) in the clinical context of the patient. (see attachment 1) Prescriber must provide documentation showing the member has tried and failed (which will be verified via pharmacy claims if available) or had an intolerance or contraindication to Fabrazyme (agalsidase beta). Baseline number of GL-3 inclusions per kidney interstitial capillary must be provided. The requested dose and frequency is in accordance with FDA-approved labeling, nationally recognized compendia, and/or evidence-based practice guidelines Exclusion criteria o Member must not have severe renal impairment (egfr <30 ml/minute/1.73 m 2 ) o Member must not have end-stage renal disease requiring dialysis Initial Duration of Approval: 6 months Reauthorization criteria o There must be 50% reduction from baseline in the number of GL-3 inclusions per kidney interstitial capillary. Reauthorization Duration of Approval: 12 months Coverage may be provided for any non-fda labeled indication if it is determined that the use is a medically accepted indication supported by nationally recognized pharmacy compendia or peer-reviewed medical literature for treatment of the diagnosis(es) for which it is prescribed. These requests will be reviewed on a case by case basis to determine medical necessity.
3 Fabrazyme (agalsidase beta) PRIOR AUTHORIZATION FORM Please complete and fax all requested information below including any progress notes, laboratory test results, or chart documentation as applicable to Highmark Health Options Pharmacy Services. FAX: (855) If needed, you may call to speak to a Pharmacy Services Representative. PHONE: (844) Monday through Friday 8:30am to 5:00pm PROVIDER INFORMATION Requesting Provider: NPI: Provider Specialty: Office Address: Office Contact: Office Phone: Office Fax: MEMBER INFORMATION Member Name: DOB: Health Options ID: Member weight: pounds or kg REQUESTED DRUG INFORMATION Medication: Strength: Frequency: Duration: Is the member currently receiving requested medication? Yes No Date Medication Initiated: Is this medication being used for a chronic or long-term condition for which the medication may be necessary for the life of the patient? Yes No Billing Information This medication will be billed: at a pharmacy OR medically (if medically please provide a JCODE: Place of Service: Hospital Provider s office Member s home Other Place of Service Information Name: NPI: Address: Phone: MEDICAL HISTORY (Complete for ALL requests) 1. Is member age 8 years of age or older? Yes No 2. Has member s diagnosis been confirmed by biochemical/genetic confirmation by ONE of the following: a. α-galactosidase A (α-gal A) activity in plasma, isolated leukocytes, and/or cultured cells. Yes No b. Plasma or urinary globotriaosylceramide(gb3/gl-3) or globotriaosylsphingosine (lyso-gb3). Yes No c. Detection of pathogenic mutations in the GALA/GLA gene by molecular genetic testing. Yes No 3. Is the medication been prescribed by or in association with a dermatologist, neurologist, nephrologist, rheumatologist, or cardiologist? Yes No 4. Does the member have medical history of at least ONE of the following: Yes No a. Intermittent episodes of burning pain in the extremities (acroparesthesias)
4 b. Cutaneous vascular lesions (angiokeratomas) c. Diminished perspiration (hypo- or anhidrosis) d. Characteristic corneal and lenticular opacities e. Abdominal pain, nausea, and/or diarrhea of unknown etiology in young adulthood f. Left ventricular hypertrophy (LVH) or hypertrophic cardiomyopathy of unknown etiology, particularly in young adults g. Arrhythmias of unknown etiology, particularly in young adults h. Stroke of unknown etiology at any age i. Chronic kidney disease (CKD) and/or proteinuria of unknown etiology j. Multiple renal sinus cysts discovered incidentally k. Family history suggestive of the disorder (ie, history of unexplained gastrointestinal symptoms, extremity pain, and/or kidney disease, ischemic stroke, or cardiac disease in one or more family members) CURRENT or PREVIOUS THERAPY Medication Name Strength/ Frequency Dates of Therapy Status (Discontinued & Why/Current) REAUTHORIZATION Please provide baseline values for plasma GL-3 and/or GL-3 inclusions. (Please provide documentation): Please provide improved values for plasma GL-3 and/or GL-3 inclusions defined by a reduction in plasma GL-3 and/or GL-3 inclusion compared to pre-treatment baseline. (Please provide documentation): Has the member experienced a significant improvement with treatment? Yes No Please describe: SUPPORTING INFORMATION or CLINICAL RATIONALE Prescribing Provider Signature Date
5 GALAFOLD (MIGALASTAT) PRIOR AUTHORIZATION FORM Please complete and fax all requested information below including any progress notes, laboratory test results, or chart documentation as applicable to Highmark Health Options Pharmacy Services. FAX: (855) If needed, you may call to speak to a Pharmacy Services Representative. PHONE: (844) Monday through Friday 8:30am to 5:00pm PROVIDER INFORMATION Requesting Provider: NPI: Provider Specialty: Office Address: Office Contact: Office Phone: Office Fax: MEMBER INFORMATION Member Name: DOB: Health Options ID: Member weight: pounds or kg REQUESTED DRUG INFORMATION Medication: Strength: Frequency: Duration: Is the member currently receiving requested medication? Yes No Date Medication Initiated: Is this medication being used for a chronic or long-term condition for which the medication may be necessary for the life of the patient? Yes No Billing Information This medication will be billed: at a pharmacy OR medically (if medically please provide a JCODE: Place of Service: Hospital Provider s office Member s home Other Place of Service Information Name: NPI: Address: Phone: MEDICAL HISTORY (Complete for ALL requests) 1) Is member 18 years of age or older? Yes No 2) Does the member have amenable GLA variant that has been interpreted by a clinical genetics professional as causing Fabry disease (pathogenic, likely pathogenic) in the clinical context of the patient? Yes No Please provide variant: 3) Has member tried and failed or had an intolerance or contraindication to Fabrazyme (agalsidase beta)? Yes No 4) What is the baseline number of GL-3 inclusions per kidney interstitial capillary? 5) Does the member have severe renal impairment (egfr <30 ml/minute/1.73 m 2 )? Yes No 6) Does the member have end-stage renal disease requiring dialysis? Yes No
6 CURRENT or PREVIOUS THERAPY Medication Name Strength/ Frequency Dates of Therapy Status (Discontinued & Why/Current) REAUTHORIZATION Please provide number of GL-3 inclusions per kidney interstitial capillary : Has the member experienced a significant improvement with treatment? Yes No Please describe: SUPPORTING INFORMATION or CLINICAL RATIONALE Prescribing Provider Signature Date

7 Attachment 1 Updated: 09/2018
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
Calcitonin Gene Related Peptide Receptor Inhibitors Prior Authorization Criteria:
 Request for Prior Authorization for Calcitonin Gene Related Peptide Receptor Inhibitors Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Calcitonin Gene
Request for Prior Authorization for Calcitonin Gene Related Peptide Receptor Inhibitors Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Calcitonin Gene
For all requests for Multiple Sclerosis Medications all of the following criteria must be met:
 Request for Prior Authorization for Multiple Sclerosis Medications Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Multiple Sclerosis Medications require
Request for Prior Authorization for Multiple Sclerosis Medications Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Multiple Sclerosis Medications require
GALAFOLD (migalastat) oral capsule
 oral capsule") GALAFOLD (migalastat) oral capsule Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
GALAFOLD (migalastat) oral capsule Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
REQUESTED DRUG INFORMATION
 Request for Prior Authorization for Lumizyme (alglucosidase alfa) Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Lumizyme (alglucosidase alfa) require
Request for Prior Authorization for Lumizyme (alglucosidase alfa) Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Lumizyme (alglucosidase alfa) require
Request for Prior Authorization for PCSK9 inhibitor therapy Website Form Submit request via: Fax
 Request for Prior Authorization for PCSK9 inhibitor therapy Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 PCSK9 is a protein that reduces the hepatic removal of low-density
Request for Prior Authorization for PCSK9 inhibitor therapy Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 PCSK9 is a protein that reduces the hepatic removal of low-density
Medication Policy Manual. Topic: Fabrazyme, agalsidase beta Date of Origin: February 17, 2015
 Medication Policy Manual Policy No: dru391 Topic: Fabrazyme, agalsidase beta Date of Origin: February 17, 2015 Committee Approval Date: March 13, 2015 Next Review Date: March 2016 Effective Date: July
Medication Policy Manual Policy No: dru391 Topic: Fabrazyme, agalsidase beta Date of Origin: February 17, 2015 Committee Approval Date: March 13, 2015 Next Review Date: March 2016 Effective Date: July
* Note: please reference the Highmark Health Options Gender Transition Services (MP- 033-MD-DE) policy for all gender dysphoria requests.
 policy for all gender dysphoria requests.") Request for Prior Authorization for Lupron, Lupron Depot (leuprolide acetate) Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Lupron (leuprolide acetate)
Request for Prior Authorization for Lupron, Lupron Depot (leuprolide acetate) Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Lupron (leuprolide acetate)
Section I. Short-acting opioid Prior Authorization Criteria
 Request for Prior Authorization for Opioid analgesics Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 Requests for opioid analgesics may be subject to prior authorization
Request for Prior Authorization for Opioid analgesics Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 Requests for opioid analgesics may be subject to prior authorization
Prior Authorization Conditions for Approval of Enbrel (etanercept) Website Form Submit request via: Fax
 Website Form Submit request via: Fax") Prior Authorization Conditions for Approval of Enbrel (etanercept) Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Enbrel (etanercept) require a prior
Prior Authorization Conditions for Approval of Enbrel (etanercept) Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Enbrel (etanercept) require a prior
Updated: 08/2017 DMMA Approved: 11/2017
 Request for Prior Authorization for Therapy to Treat Binge Eating Disorder Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for medications to treat Binge
Request for Prior Authorization for Therapy to Treat Binge Eating Disorder Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for medications to treat Binge
This presentation contains forward looking statements within the meaning of the Private Securities Litigation Reform Act of 1995 relating to business,
 American Society of Nephrology (ASN) Migalastat Monotherapy Phase 3 Data N November b 15 15, 2014 Safe Harbor This presentation contains forward looking statements within the meaning of the Private Securities
American Society of Nephrology (ASN) Migalastat Monotherapy Phase 3 Data N November b 15 15, 2014 Safe Harbor This presentation contains forward looking statements within the meaning of the Private Securities
Prior Authorization Conditions for Approval of Humira (adalimumab) Website Form Submit request via: Fax
 Website Form Submit request via: Fax") Prior Authorization Conditions for Approval of Humira (adalimumab) Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Humira (adalimumab) require a prior
Prior Authorization Conditions for Approval of Humira (adalimumab) Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Humira (adalimumab) require a prior
2. Does the patient have a diagnosis of Crohn s disease? Y N
 Pharmacy Prior Authorization MERC CARE PLA (MEDICAID) Stelara (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Pharmacy Prior Authorization MERC CARE PLA (MEDICAID) Stelara (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
TARCEVA (erlotinib) oral tablet
 oral tablet") TARCEVA (erlotinib) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
TARCEVA (erlotinib) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
SAVAYSA (edoxaban tosylate) oral tablet
 oral tablet") SAVAYSA (edoxaban tosylate) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
SAVAYSA (edoxaban tosylate) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
Request for Prior Authorization Growth Hormone (Norditropin
 Request for Prior Authorization Growth Hormone (Norditropin, Nutropin/AQ ) Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Growth Hormone require a
Request for Prior Authorization Growth Hormone (Norditropin, Nutropin/AQ ) Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Growth Hormone require a
Phase 3 investigation of lucerastat for patients with Fabry disease. Investor Webcast May 2018
 Phase 3 investigation of lucerastat for patients with Fabry disease Investor Webcast May 2018 The following information contains certain forward-looking statements, relating to the company s business,
Phase 3 investigation of lucerastat for patients with Fabry disease Investor Webcast May 2018 The following information contains certain forward-looking statements, relating to the company s business,
NEXAVAR (sorafenib tosylate) oral tablet
 oral tablet") NEXAVAR (sorafenib tosylate) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
NEXAVAR (sorafenib tosylate) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
Stage I: Rule-Out Dashboard
 Stage I: Rule-Out Dashboard GENE/GENE PANEL: GLA DISORDER: Fabry disease HGNC ID: 4296 OMIM ID: 301500 ACTIONABILITY PENETRANCE 1. Is there a qualifying resource, such as a practice guideline or systematic
Stage I: Rule-Out Dashboard GENE/GENE PANEL: GLA DISORDER: Fabry disease HGNC ID: 4296 OMIM ID: 301500 ACTIONABILITY PENETRANCE 1. Is there a qualifying resource, such as a practice guideline or systematic
Cardiomyopathy in Fabry s disease
 Cardiomyopathy in Fabry s disease Herzinsuffizienzlunch Basel, 11.09.2018 Christiane Gruner Kardiologie, UniversitätsSpital Zürich Content Background / epidemiology Differential diagnosis Clinical presentations
Cardiomyopathy in Fabry s disease Herzinsuffizienzlunch Basel, 11.09.2018 Christiane Gruner Kardiologie, UniversitätsSpital Zürich Content Background / epidemiology Differential diagnosis Clinical presentations
Fabry Disease and the Kidneys
 Department of Human Genetics Division of Medical Genetics Lysosomal Storage Disease Center www.genetics.emory.edu Fabry Disease and the Kidneys What is Fabry Disease? Fabry disease (FD) is an X-linked
Department of Human Genetics Division of Medical Genetics Lysosomal Storage Disease Center www.genetics.emory.edu Fabry Disease and the Kidneys What is Fabry Disease? Fabry disease (FD) is an X-linked
GILOTRIF (afatinib) oral tablet
 oral tablet") GILOTRIF (afatinib) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
GILOTRIF (afatinib) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
APIDRA (insulin glulisine) injection vial APIDRA SOLOSTAR (insulin glulisine) subcutaneous solution pen-injector
 injection vial APIDRA SOLOSTAR (insulin glulisine) subcutaneous solution pen-injector") APIDRA SOLOSTAR (insulin glulisine) subcutaneous solution pen-injector Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
APIDRA SOLOSTAR (insulin glulisine) subcutaneous solution pen-injector Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Pharmacy Prior Authorization
 Pharmacy Prior Authorization AETA BETTER HEALTH VIRGIIA Multiple Sclerosis Agents (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Pharmacy Prior Authorization AETA BETTER HEALTH VIRGIIA Multiple Sclerosis Agents (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
2. Has this plan authorized this medication in the past for this member (i.e., previous authorization is on file under this plan)?
?") Pharmacy Prior Authorization MERC CARE (MEDICAID) Multiple Sclerosis (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and
Pharmacy Prior Authorization MERC CARE (MEDICAID) Multiple Sclerosis (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and
The use of pathology surrogate markers in Fabry Disease. Beth L. Thurberg MD PhD Vice President of Pathology Genzyme
 Disclaimer: Presentation slides from the Rare Disease Workshop Series are posted by the EveryLife Foundation for Rare Diseases for educational purposes only. They are for use by drug development professionals
Disclaimer: Presentation slides from the Rare Disease Workshop Series are posted by the EveryLife Foundation for Rare Diseases for educational purposes only. They are for use by drug development professionals
3. Has the patient had a sustained improvement in Pain or Function (e.g. PEG scale with a 30 percent response from baseline)?
?") Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 Metformin tablet SR 24-hour modified release oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
Metformin tablet SR 24-hour modified release oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 Ezetimibe-simvastatin 10-80 mg oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
Ezetimibe-simvastatin 10-80 mg oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
3. Does the member continue to receive nutritional or psychological counseling?
 Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS CS Stimulants (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS CS Stimulants (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
2. Has this plan authorized this medication in the past for this member (i.e., previous authorization is on file under this plan)?
?") Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Multiple Sclerosis Agents (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Multiple Sclerosis Agents (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
2. Did the member receive this medication during a recent hospitalization? Y N
 Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Antipsychotics (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Antipsychotics (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
2. Did the patient receive this medication during a recent hospitalization? Y N
 Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Antipsychotics (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Antipsychotics (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
2. Is this request for a preferred medication? Y N
 Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
LOKELMA (sodium zirconium cyclosilicate) oral suspension
 oral suspension") LOKELMA (sodium zirconium cyclosilicate) oral suspension Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
LOKELMA (sodium zirconium cyclosilicate) oral suspension Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
REQUEST FOR MEDICARE PRESCRIPTION DRUG COVERAGE DETERMINATION This form may be sent to us by mail or fax:
 REQUEST FOR MEDICARE PRESCRIPTION DRUG COVERAGE DETERMINATION This form may be sent to us by mail or fax: Address: Fax Number: Anthem Blue Cross Cal MediConnect Plan 1-844-493-9213 Medicare Prior Authorization
REQUEST FOR MEDICARE PRESCRIPTION DRUG COVERAGE DETERMINATION This form may be sent to us by mail or fax: Address: Fax Number: Anthem Blue Cross Cal MediConnect Plan 1-844-493-9213 Medicare Prior Authorization
THIOLA (tiopronin) oral tablet
 oral tablet") THIOLA (tiopronin) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
THIOLA (tiopronin) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
2. Has this plan authorized this medication in the past for this member (i.e., previous authorization is on file under this plan)?
?") Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Multiple Sclerosis (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Multiple Sclerosis (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
TIBSOVO (ivosidenib) oral tablet
 oral tablet") TIBSOVO (ivosidenib) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
TIBSOVO (ivosidenib) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
Circle Yes or No Y N. [If no, skip to question 8.] 2. Has the patient been compliant with therapy as verified by the prescriber?
![Circle Yes or No Y N. [If no, skip to question 8.] 2. Has the patient been compliant with therapy as verified by the prescriber?](/thumbs/92/109743083.jpg "Circle Yes or No Y N. [If no, skip to question 8.] 2. Has the patient been compliant with therapy as verified by the prescriber?") 06/01/2016 Prior Authorization AETA BETTER HEALTH OF MICHIGA (MEDICAID) Tecfidera (MI88) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
06/01/2016 Prior Authorization AETA BETTER HEALTH OF MICHIGA (MEDICAID) Tecfidera (MI88) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
2. Does the patient have chronic urticaria? Y N
 Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Xolair (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Xolair (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Heterozygous Fabry Disease Females Are Not Just Carriers, But Suffer From
 Heterozygous Fabry Disease Females Are Not Just Carriers, But Suffer From Significant Burden of Disease And Impaired Quality of Life Raymond Wang, M.D. Children s Hospital of Orange County Division of
Heterozygous Fabry Disease Females Are Not Just Carriers, But Suffer From Significant Burden of Disease And Impaired Quality of Life Raymond Wang, M.D. Children s Hospital of Orange County Division of
VELTASSA (patiromer) oral suspension
 oral suspension") VELTASSA (patiromer) oral suspension Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
VELTASSA (patiromer) oral suspension Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
PHARMACY COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 11/16/17 SECTION: DRUGS LAST REVIEW DATE: 11/16/17 LAST CRITERIA REVISION DATE: ARCHIVE DATE:
 LEVALBUTEROL HFA (levalbuterol tartrate) inhalation aerosol Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
LEVALBUTEROL HFA (levalbuterol tartrate) inhalation aerosol Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
Drafting a Coverage Authorization Request Letter
 Drafting a Coverage Authorization Request Letter The following information is presented for informational purposes only and is not intended to provide reimbursement or legal advice. Laws, regulations,
Drafting a Coverage Authorization Request Letter The following information is presented for informational purposes only and is not intended to provide reimbursement or legal advice. Laws, regulations,
Fabry disease: a review of current management strategies
 Fabry disease: a review of current management strategies A. MEHTA 1, M. BECK 2, F. EYSKENS 3, C. FELICIANI 4, I. KANTOLA 5, U. RAMASWAMI 6, A. ROLFS 7, A. RIVERA 8, S. WALDEK 9, D.P. GERMAIN 10 1 Lysosomal
Fabry disease: a review of current management strategies A. MEHTA 1, M. BECK 2, F. EYSKENS 3, C. FELICIANI 4, I. KANTOLA 5, U. RAMASWAMI 6, A. ROLFS 7, A. RIVERA 8, S. WALDEK 9, D.P. GERMAIN 10 1 Lysosomal
3. Does the patient continue to receive nutritional or psychological counseling? Y N
 Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS CS Stimulants (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS CS Stimulants (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
ZURAMPIC (lesinurad) oral tablet
 oral tablet") ZURAMPIC (lesinurad) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
ZURAMPIC (lesinurad) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
Fabry disease: when to suspect it and how to treat it
 Fabry disease: when to suspect it and how to treat it Catalina Martín Cleary Alberto Ortiz Arduán, MD, PhD IIS-Fundacion Jimenez Diaz, UAM IRSIN, REDINREN Madrid, Spain Conflict of interest Consultant:
Fabry disease: when to suspect it and how to treat it Catalina Martín Cleary Alberto Ortiz Arduán, MD, PhD IIS-Fundacion Jimenez Diaz, UAM IRSIN, REDINREN Madrid, Spain Conflict of interest Consultant:
2. Does the patient have a diagnosis of ulcerative colitis or Crohn s? Y N
 Pharmacy Prior Authorization AETA BETTER HEALTH LOUISIAA (MEDICAID) Remicade (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
Pharmacy Prior Authorization AETA BETTER HEALTH LOUISIAA (MEDICAID) Remicade (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
Pharmacy Prior Authorization
 Pharmacy Prior Authorization AETA BETTER HEALTH ILLIOIS (MEDICAID) CS Stimulants (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Pharmacy Prior Authorization AETA BETTER HEALTH ILLIOIS (MEDICAID) CS Stimulants (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Inborn Errors of Metabolism. Landi Lombard Endocrinologist Kuilsrivier
 Inborn Errors of Metabolism Landi Lombard Endocrinologist Kuilsrivier Classification of Inborn Errors of Metabolism Amino acid disorders eg Phenylketonuria Organic acidemias eg Maple syrup urine disease
Inborn Errors of Metabolism Landi Lombard Endocrinologist Kuilsrivier Classification of Inborn Errors of Metabolism Amino acid disorders eg Phenylketonuria Organic acidemias eg Maple syrup urine disease
RAYOS (prednisone tablet delayed release) oral tablet
 oral tablet") RAYOS (prednisone tablet delayed release) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan.
RAYOS (prednisone tablet delayed release) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan.
Prior Authorization. Drug Name (select from list of drugs shown) Gilenya (fingolomid) Quantity Frequency Strength. Physician Name:
 Gilenya (fingolomid) Quantity Frequency Strength. Physician Name:") 06/01/2016 Prior Authorization Aetna Better Health Michigan Gilenya This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax signed
06/01/2016 Prior Authorization Aetna Better Health Michigan Gilenya This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax signed
Priority Health Medicare prior authorization form Fax completed form to: toll free, or
 Priority Health Medicare prior authorization form Fax completed form to: 877.974.4411 toll free, or 616.942.8206 This form applies to: Medicare Part B Medicare Part D This request is: Expedited request
Priority Health Medicare prior authorization form Fax completed form to: 877.974.4411 toll free, or 616.942.8206 This form applies to: Medicare Part B Medicare Part D This request is: Expedited request
KEVEYIS (dichlorphenamide) oral tablet
 oral tablet") KEVEYIS (dichlorphenamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
KEVEYIS (dichlorphenamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
Pharmacy Prior Authorization
 Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Anticoagulant Injectable (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Anticoagulant Injectable (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
3. Does the patient meet ALL of the following requirements? Y N
 Pharmacy Prior Authorization AETA BETTER HEALTH FLORIDA Procrit - Retacrit (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
Pharmacy Prior Authorization AETA BETTER HEALTH FLORIDA Procrit - Retacrit (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
SAMPLE IgE: ESR: CRP: # Joints: %BSA: Height: Weight: BMI:
 Please Note: Medical Necessity Prior Authorization may be overrided for both formulary coverage and benefit design restrictions. They are issued at the full discretion of the benefit manager. PRIOR AUTHORIZATION
Please Note: Medical Necessity Prior Authorization may be overrided for both formulary coverage and benefit design restrictions. They are issued at the full discretion of the benefit manager. PRIOR AUTHORIZATION
LEVEMIR (insulin detemir) subcutaneous solution LEVEMIR FLEXTOUCH (insulin detemir) subcutaneous solution pen-injector
 subcutaneous solution LEVEMIR FLEXTOUCH (insulin detemir) subcutaneous solution pen-injector") LEVEMIR FLEXTOUCH (insulin detemir) subcutaneous solution pen-injector Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
LEVEMIR FLEXTOUCH (insulin detemir) subcutaneous solution pen-injector Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
3. Does the patient have a diagnosis of rheumatoid arthritis (RA) with moderate to high disease activity?
 with moderate to high disease activity?") Pharmacy Prior Authorization MERC CARE PLA (MEDICAID) Enbrel (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Pharmacy Prior Authorization MERC CARE PLA (MEDICAID) Enbrel (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
ALUNBRIG (brigatinib) oral tablet
 oral tablet") ALUNBRIG (brigatinib) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
ALUNBRIG (brigatinib) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
Circle Yes or No Y N. [If yes, skip to question 30.] 2. Is this request for a child? Y N. [If no, skip to question 20.]
![Circle Yes or No Y N. [If yes, skip to question 30.] 2. Is this request for a child? Y N. [If no, skip to question 20.]](/thumbs/89/99261437.jpg "Circle Yes or No Y N. [If yes, skip to question 30.] 2. Is this request for a child? Y N. [If no, skip to question 20.]") 05/20/2015 Prior Authorization MERC CARE PLA (MEDICAID) Growth Hormone (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and
05/20/2015 Prior Authorization MERC CARE PLA (MEDICAID) Growth Hormone (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and
Highly specialised technologies guidance Published: 22 February 2017 nice.org.uk/guidance/hst4
 Migalastat for treating Fabry disease Highly specialised technologies guidance Published: 22 February 2017 nice.org.uk/guidance/hst4 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Migalastat for treating Fabry disease Highly specialised technologies guidance Published: 22 February 2017 nice.org.uk/guidance/hst4 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
A Unique Disease Uniquely Experienced
 A Unique Disease Uniquely Experienced Understanding Fabry disease a serious, progressive disorder with complex pathology 1 Fabry disease is an X-linked lysosomal storage disorder. 1 Caused by a deficiency
A Unique Disease Uniquely Experienced Understanding Fabry disease a serious, progressive disorder with complex pathology 1 Fabry disease is an X-linked lysosomal storage disorder. 1 Caused by a deficiency
LONSURF (trifluridine-tipiracil) oral tablet
 oral tablet") LONSURF (trifluridine-tipiracil) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
LONSURF (trifluridine-tipiracil) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
ALECENSA (alectinib) oral capsule
 oral capsule") ALECENSA (alectinib) oral capsule Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
ALECENSA (alectinib) oral capsule Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
FABRY DISEASE: Phenotypic Spectrum Genotype/Phenotype Correlations Enzyme Replacement Therapy (ERT) R. J. Desnick, Ph.D., M.D.
 R. J. Desnick, Ph.D., M.D.") FABRY DISEASE: Phenotypic Spectrum Genotype/Phenotype Correlations Enzyme Replacement Therapy (ERT) R. J. Desnick, Ph.D., M.D. Director, International Center for Fabry Disease Dean for Genetic & Genomic
FABRY DISEASE: Phenotypic Spectrum Genotype/Phenotype Correlations Enzyme Replacement Therapy (ERT) R. J. Desnick, Ph.D., M.D. Director, International Center for Fabry Disease Dean for Genetic & Genomic
Clinical Diversity in Patients with Anderson-Fabry Disease with the R301Q Mutation
 doi: 10.2169/internalmedicine.0959-18 Intern Med Advance Publication http://internmed.jp CASE REPORT Clinical Diversity in Patients with Anderson-Fabry Disease with the R301Q Mutation Saori Yamamoto 1,
doi: 10.2169/internalmedicine.0959-18 Intern Med Advance Publication http://internmed.jp CASE REPORT Clinical Diversity in Patients with Anderson-Fabry Disease with the R301Q Mutation Saori Yamamoto 1,
Pharmacy Prior Authorization
 Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Enbrel (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Enbrel (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Molina Healthcare of Texas
 Texas Standard Prior Authorization Form Addendum Molina Healthcare of Texas Ingrezza (Marketplace) This fax machine is located in a secure location as required by HIPAA Regulations. Complete / Review information,
Texas Standard Prior Authorization Form Addendum Molina Healthcare of Texas Ingrezza (Marketplace) This fax machine is located in a secure location as required by HIPAA Regulations. Complete / Review information,
FLUOXETINE 60 MG oral tablet FLUOXETINE 90 MG oral delayed release (once weekly) capsule
 capsule") FLUOXETINE 90 MG oral delayed release (once weekly) capsule Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
FLUOXETINE 90 MG oral delayed release (once weekly) capsule Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
Medical History Form
 Medical History Form Name: ; Birth date: / / ; Date: / / Person filling out form: ; Relationship: Thank you for taking the time to fill out this valuable information. This allows us to provide the best
Medical History Form Name: ; Birth date: / / ; Date: / / Person filling out form: ; Relationship: Thank you for taking the time to fill out this valuable information. This allows us to provide the best
1. Has this plan authorized this medication in the past for this patient (i.e., previous authorization is on file under this plan)?
?") 09/07/2016 Prior Authorization AETA BETTER HEALTH OF KETUCK (MEDICAID) PCSK9 Inhibitors (K88) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
09/07/2016 Prior Authorization AETA BETTER HEALTH OF KETUCK (MEDICAID) PCSK9 Inhibitors (K88) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
3. Has the patient shown improvement in signs and symptoms of the disease? Y N
 Pharmacy Prior Authorization MERC CARE (MEDICAID) Orencia (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax signed
Pharmacy Prior Authorization MERC CARE (MEDICAID) Orencia (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax signed
XATMEP (methotrexate) oral solution
 oral solution") XATMEP (methotrexate) oral solution Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
XATMEP (methotrexate) oral solution Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
IMBRUVICA (ibrutinib) oral capsule and tablet
 oral capsule and tablet") IMBRUVICA (ibrutinib) oral capsule and tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
IMBRUVICA (ibrutinib) oral capsule and tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
Circle Yes or No Y N. [If no, then no further questions.]
![Circle Yes or No Y N. [If no, then no further questions.]](/thumbs/89/100976446.jpg "Circle Yes or No Y N. [If no, then no further questions.]") 01/04/2016 Prior Authorization MERC MARICOPA ITEGRATED CARE - TXIX/XXI SMI (MEDICAID) Multiple Sclerosis Agents (AZ88) This fax machine is located in a secure location as required by HIPAA regulations.
01/04/2016 Prior Authorization MERC MARICOPA ITEGRATED CARE - TXIX/XXI SMI (MEDICAID) Multiple Sclerosis Agents (AZ88) This fax machine is located in a secure location as required by HIPAA regulations.
BLOOD GLUCOSE METER TEST STRIP STEP THERAPY CRITERIA
 BLOOD GLUCOSE METER TEST STRIP STEP THERAPY CRITERIA Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan.
BLOOD GLUCOSE METER TEST STRIP STEP THERAPY CRITERIA Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan.
2. Is the patient responding to medication? Y N
 Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS ADD-ADHD Stimulants (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS ADD-ADHD Stimulants (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
ADMELOG, NOVOLIN, NOVOLOG, and FIASP
 ADMELOG, NOVOLIN, NOVOLOG, and FIASP Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
ADMELOG, NOVOLIN, NOVOLOG, and FIASP Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
IBRANCE (palbociclib) oral capsule
 oral capsule") IBRANCE (palbociclib) oral capsule Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
IBRANCE (palbociclib) oral capsule Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
Authorization and appeals kit: Psoriatic arthritis
 1 Authorization and appeals kit: Psoriatic arthritis Resources for healthcare providers INDICATIONS COSENTYX is indicated for the treatment of moderate to severe plaque psoriasis in adult patients who
1 Authorization and appeals kit: Psoriatic arthritis Resources for healthcare providers INDICATIONS COSENTYX is indicated for the treatment of moderate to severe plaque psoriasis in adult patients who
Assessment report. for
 Assessment report for FABRAZYME agalsidase beta Assessment report on the shortage of Fabrazyme Overview of Shortage Period: Spontaneous Reports from June 2009 through 15 September and Registry Data from
Assessment report for FABRAZYME agalsidase beta Assessment report on the shortage of Fabrazyme Overview of Shortage Period: Spontaneous Reports from June 2009 through 15 September and Registry Data from
TEXAS MEDICAID Clinical Edit Prior Authorization Growth Hormones: HUMATROPE, NUTROPIN AQ, OMNITROPE, SAIZEN
 TEXAS MEDICAID Clinical Edit Prior Authorization Growth Hormones: HUMATROPE, NUTROPIN AQ, OMNITROPE, SAIZEN STEP 1: CLEARLY PRINT AND COMPLETE TO EXPEDITE PROCESSING Date: Prescriber First & Last Name:
TEXAS MEDICAID Clinical Edit Prior Authorization Growth Hormones: HUMATROPE, NUTROPIN AQ, OMNITROPE, SAIZEN STEP 1: CLEARLY PRINT AND COMPLETE TO EXPEDITE PROCESSING Date: Prescriber First & Last Name:
TEXAS MEDICAID Clinical Edit Prior Authorization Growth Hormones: GENOTROPIN & NORDITROPIN Texas Children s Health Plan Only
 TEXAS MEDICAID Clinical Edit Prior Authorization Growth Hormones: GENOTROPIN & NORDITROPIN Texas Children s Health Plan Only STEP 1: CLEARLY PRINT AND COMPLETE TO EXPEDITE PROCESSING Date: Prescriber First
TEXAS MEDICAID Clinical Edit Prior Authorization Growth Hormones: GENOTROPIN & NORDITROPIN Texas Children s Health Plan Only STEP 1: CLEARLY PRINT AND COMPLETE TO EXPEDITE PROCESSING Date: Prescriber First
SUMAVEL DOSEPRO (sumatriptan succinate) solution for injection
 solution for injection") SUMAVEL DOSEPRO (sumatriptan succinate) solution for injection Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
SUMAVEL DOSEPRO (sumatriptan succinate) solution for injection Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
9/9/2016. Drug Name (select from list of drugs shown) Bunavail Buccal Film (buprenorphinenaloxone) Suboxone Sublingual Film (buprenorphine-naloxone)
 Bunavail Buccal Film (buprenorphinenaloxone) Suboxone Sublingual Film (buprenorphine-naloxone)") 9/9/2016 Prior Authorization Form PASSPORT HEALTH PLAN KENTUCKY MEDICAID Buprenorphine Products This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
9/9/2016 Prior Authorization Form PASSPORT HEALTH PLAN KENTUCKY MEDICAID Buprenorphine Products This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Authorization and appeals kit: Moderate to severe plaque psoriasis coexisting with psoriatic arthritis
 Authorization and appeals kit: Moderate to severe plaque psoriasis coexisting with psoriatic arthritis Resources for healthcare providers INDICATIONS COSENTYX is indicated for the treatment of moderate
Authorization and appeals kit: Moderate to severe plaque psoriasis coexisting with psoriatic arthritis Resources for healthcare providers INDICATIONS COSENTYX is indicated for the treatment of moderate
LYNPARZA (olaparib) oral capsule and tablet
 oral capsule and tablet") LYNPARZA (olaparib) oral capsule and tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
LYNPARZA (olaparib) oral capsule and tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
3. Has the patient shown improvement in signs and symptoms of the disease? Y N
 Pharmacy Prior Authorization MERC CARE (MEDICAID) Renflexis (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Pharmacy Prior Authorization MERC CARE (MEDICAID) Renflexis (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Drug Prior Authorization Form Opdivo (nivolumab)
") This document contains both information and form fields. To read information, use the Down Arrow from a form field. Drug Prior Authorization Form The purpose of this form is to obtain information required
This document contains both information and form fields. To read information, use the Down Arrow from a form field. Drug Prior Authorization Form The purpose of this form is to obtain information required
2. Has this plan authorized this medication in the past for this member (i.e., previous authorization is on file under this plan)?
?") Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Growth Hormone (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and
Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Growth Hormone (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and
CYSTARAN (cysteamine hydrochloride) ophthalmic solution
 ophthalmic solution") CYSTARAN (cysteamine hydrochloride) ophthalmic solution Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
CYSTARAN (cysteamine hydrochloride) ophthalmic solution Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit
PHARMACY COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 5/18/17 SECTION: DRUGS LAST REVIEW DATE: 5/17/18 LAST CRITERIA REVISION DATE: ARCHIVE DATE:
 KARBINAL ER (carbinoxamine maleate) extended release oral suspension Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
KARBINAL ER (carbinoxamine maleate) extended release oral suspension Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Pharmacy Prior Authorization
 Pharmacy Prior Authorization MERC CARE PLA (MEDICAID) Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Pharmacy Prior Authorization MERC CARE PLA (MEDICAID) Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax