The Bile Duct (and Pancreas) and the Physician
|
|
|
- Malcolm Dalton
- 5 years ago
- Views:
Transcription

1 The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester

2 Not so common?! Two weeks 38 ERCP s Physician Surgeon 5 0 Cholangitisstones Pancreatitis Cancer - Jaundice

3 Goals Introduction Assess severity and role of imaging Feeding modality Antibiotics When to intervene
4 Acute Biliary Pancreatitis Gallstones commonest cause worldwide Variable severity of presentation 10-20% life-threatening course 8-10% mortality Death associated with pancreatitis associated complications 2 phases (early <7 days, late >2 weeks)
5 Severe ABP ABP + organ failure and/or ABP + local complications APACHE II =/> 8 Ranson Criteria =/> 3 Low threshold for managing on HDU Crit Care Med 1999
6 APACHE II
7 Biliary 35-40% Alcohol 30% Metabolic Drugs Toxins Autoimune Causes Trauma Ischaemia Infection Genetic Idiopathic

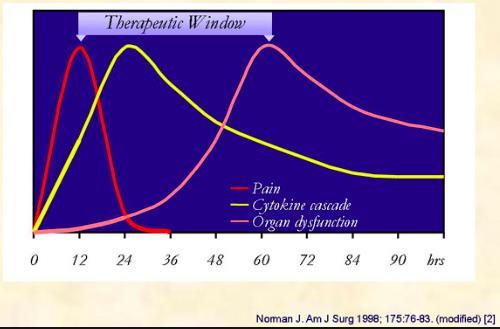
8 Inflammatory cascade Acute Pancreatitis Capillary Leak ARDS Shock ATN Hypovolaemia

9 Curr Med Chem 2006
10
11 Initial Ix Amylase - >3x ULN (if normal Creat) Lipase TG s Ca LFT s ALT/AST, ALKP, Bili Transaminases >3x ULN, 95% likelihood ABP CRP - >150 at 48 hours prognostication but more useful for its high NPV 86% Gastroenterology 2007
12 Q: 56 year old; Amylase 2500, ALT 330, WCC 16.5, Glucose 21, po2 7.4kpa. 1. Admit, USS, O2, antibiotics, glucose control 2. Admit, CT scan contrast, O2, glucose control, hydration 3. HDU admission, USS, O2, IV fluids, glucose control 4. HDU admission, O2, IV fluids, glucose control, antibiotics
13 Q: 56 year old; Amylase 2500, ALT 330, WCC 16.5, Glucose 21, po2 7.4kpa. 1. Admit, USS, O2, antibiotics, glucose control 2. Admit, CT scan contrast, O2, glucose control, hydration 3. HDU admission, USS, O2, IV fluids, glucose control 4. HDU admission, O2, IV fluids, glucose control, antibiotics
14 Ranson s Criteria PPV 49% NPV 91% Surg Gynaec Obstet 1974
15 CT scan To assess for severity and pancreatic necrosis Avoid in first 72 hours Lack of improvement in 72 hours Persistent fever in clinically severe ABP Acute deterioration after clinical improvement Diagnosis in doubt
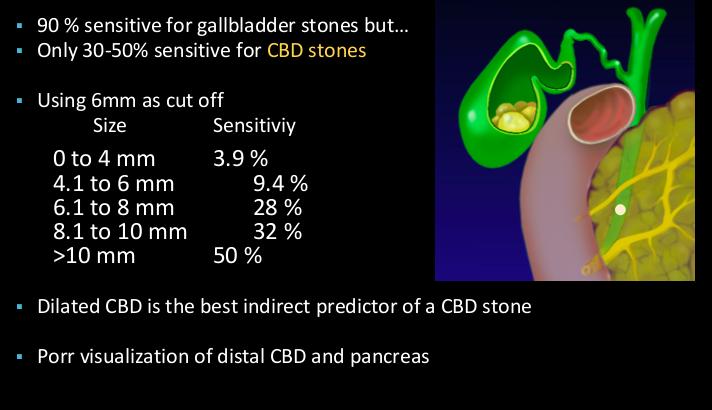
16 TAUSS
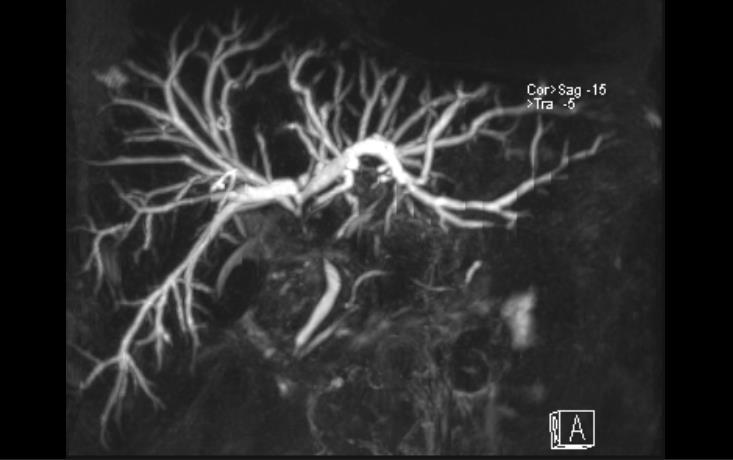
17 MRCP
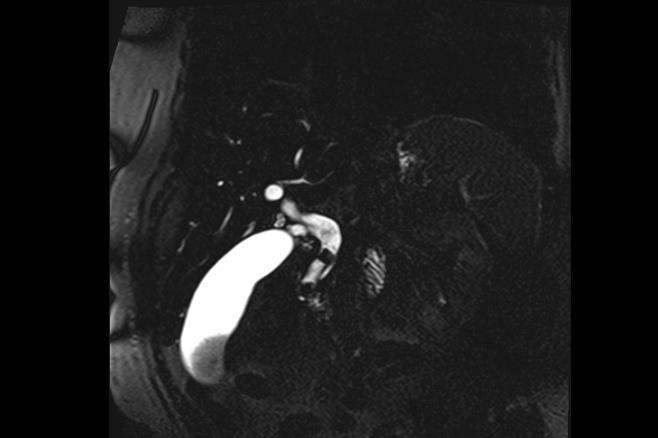
18 MRCP



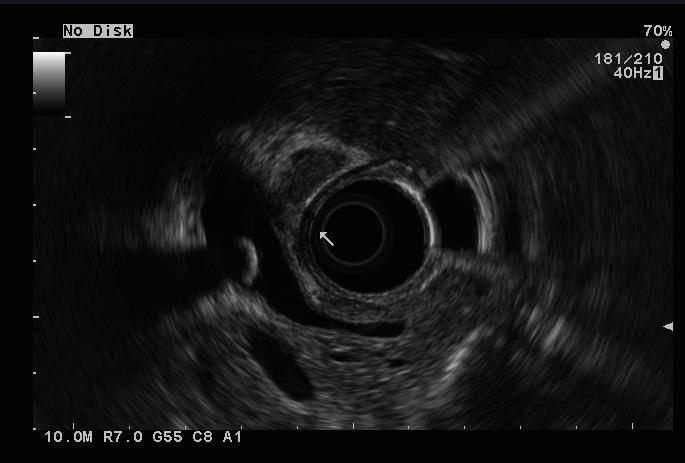
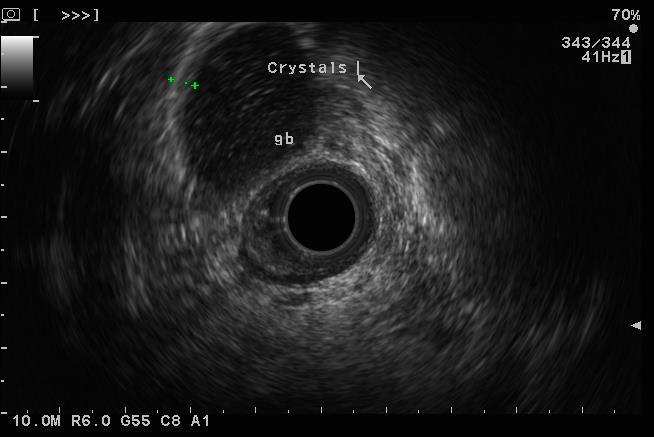
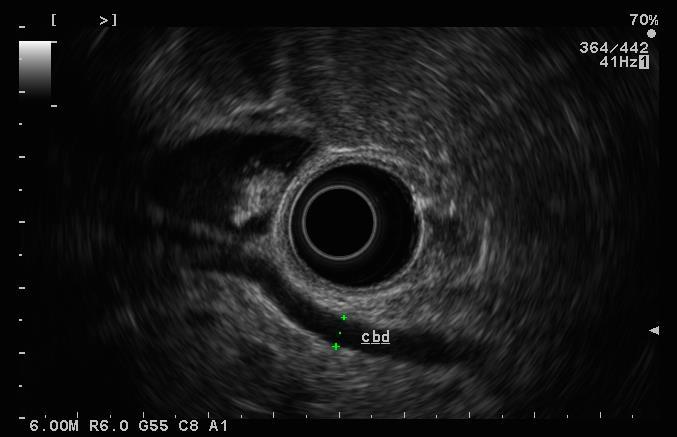
19 EUS Scope Electronic scanning Frequency: 5, 6, 7.5 and 10MHz Doppler facility ERCP was gold standard for ductal stones EUS sensitivity 89-94% specificity 95%

20
21

22 Management issues Elderly Obesity Can it influence the course of the disease? Pancreatology 2006
23 Hydration Cornerstone of medical therapy Stabilise capillary permeability Replace intravascular volume Maintains gut barrier function Can reduce pancreatic necrosis Which fluid? Crystalloid vs Colloid
24 Hydration Fluid resuscitation Aggressive 15ml/kg/hr vs Non-aggressive 5-10 ml/kg/hr Other regimes: 20mg/hr bolus then 3mg/kg/hr mls/hour for 48 hrs Equal number of studies favouring either approach
25 (Urgent) ERCP in ABP Severe ABP AND obstructive jaundice +/- Cholangitis YES Severe ABP AND CBD stones and not Jaundiced PROBABLY NOT Severe ABP AND no CBD stones and not jaundiced DEFINITELY NOT
26 Antibiotic Prophylaxis World Jour Gastro 2012 DO NOT ROUTINELY USE ANTIBIOTICS OR ANTIFUNGAL AGENTS IN NECROTISING PANCREATITIS Crit Care Med 2004
27 Potential role? Probiotics 298 pts with predicted severe pancreatitis multispecies probiotic (153) vs placebo (145) Combined infection endpoint Infections 30% in probiotic vs 28% in placebo 24 (16%) probiotics died vs 9 (6%) RR in probiotics developed bowel ischaemia vs 0 in placebo Lancet 2008
28 Nutrition Most patients with ABP will resolve in a few days and so no additional nutritional support needed. Pancreatic rest no longer accepted How soon to start feeding? TPN vs EN?
29 Dig Surg pt trial MOF Lower EN (20% vs 50%, p=0.02) Infected Necrosis and Surgery Lower in EN (20 vs 74%, p <0.001) Lower in EN (25% vs 88%, p<0.001) Mortality Lower in EN (6% vs 35 %, p<0.001)
30 Necrosis Sterile vs Infected Timing of intervention Type of intervention Surgical Percutaneous Endoscopic
31 Conclusion Recognise at risk patients for severe disease and use of imaging Provide aggressive monitoring and resuscitation Evidence-base does NOT support antibiotic prophlaxis Urgent ERCP in ABP with jaundice +/- cholangitis
32 Conclusion cont d No role for urgent ERCP in ABP without jaundice Establish early enteral feeding Historical surgical necrosectomy rare, with less invasive methods of treating necrosis step up approach
33 ACUTE CHOLANGITIS
34 Highlights Pathogenesis Microbiology Clinical features Lab findings Imaging Management
35 Highlights Cholangitis Potentially life threatening obstruction and infection of the biliary tree Charcoats triad Pain, Rigors, Jaundice 80% + from choledochlithiasis Rest strictures benign/malignant
36 Immediate Highlights Fluid resusucutation Broad Spectrum Antibiotics cover Correction of Coagulopathy Biliary Drainage
37 Pathogenesis Partial or Complete obstruction of the biliary tree Hallmark is raised intraductal biliary pressures Defence mechanisms overwhelmed Duodenum Portal venous system Infected gallbladder Periductal lymphatics
38 Microbiology 80%+ will have positive B/C Mostly Enteric bacteria E coli, Enterococcus, Enterobacter Polymicrobial bacteria Surgery or instrumentation
39 Clinical Features Charcoat triad (20-50%) Reynold Pentad (Hypotension/low GCS) Jaundice only 60-70% High index of suspicion Elderly Surgery/instr
40 CRP/WCC Lab findings/imaging LFT s may not necessarily be cholestatic. ALT/AST >250 is a good discriminator of gallstone aetiology. Relatively normal ALT/AST often indicates malignant aetiology Blood culture USS, CT, MRCP, EUS
41 Imaging USS biliary dilation, stones CT Malignancy / Staging / biliary dilation MRCP Stones, hilar stricture (after a CT), intra-hepatic stones EUS Never first line investigation
42 CT scan
43 MRCP

44 EUS

45 Tokyo 2013 guidleines Charcot triad TK13 Sensitivity 26% 92% Specificity 96% 78%
46 Management Antibiotics after blood cultures Fluid resuscitation and electrolyte correction Poor penetration into bile duct due to high intra-biliary pressures Correction of coagulopathy Biliary drainage vital. Can occur naturally or by intervention
47 Management Intervention decide on timing severe or moderate. Endoscopic Percutaneous (PTC) Advanced EUS techniques Open Surgery (T-tube drainage + later definitive care)

48
49 ERCP Superior to surgical drainage Mortality of ERCP vs surgical drainage 10% vs 32% in RCT NEJM 1992 Preferable to PTC Morbidity less, especially in presence of ascites and coagulopathy Arch Surg 197, AmJGastro 1998
50 Management PTC More accessible for an unstable patient May be available when ERCP isn t No RCT comparing ERCP vs PTC Higher M&M Useful for higher (hilar obstructions)
51 Conclusion High Index of suspicion Tokyo 13 guidelines Antibiotics May not be effective Close observation of mild cholangitis can become severe within hours Recognise severe cholangitis and arrange biliary drainage. Often < 24 hours. Prompt biliary drainage and modalities

52

53

54

55
56

57

58
59


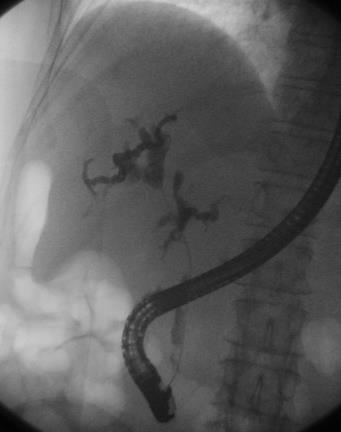
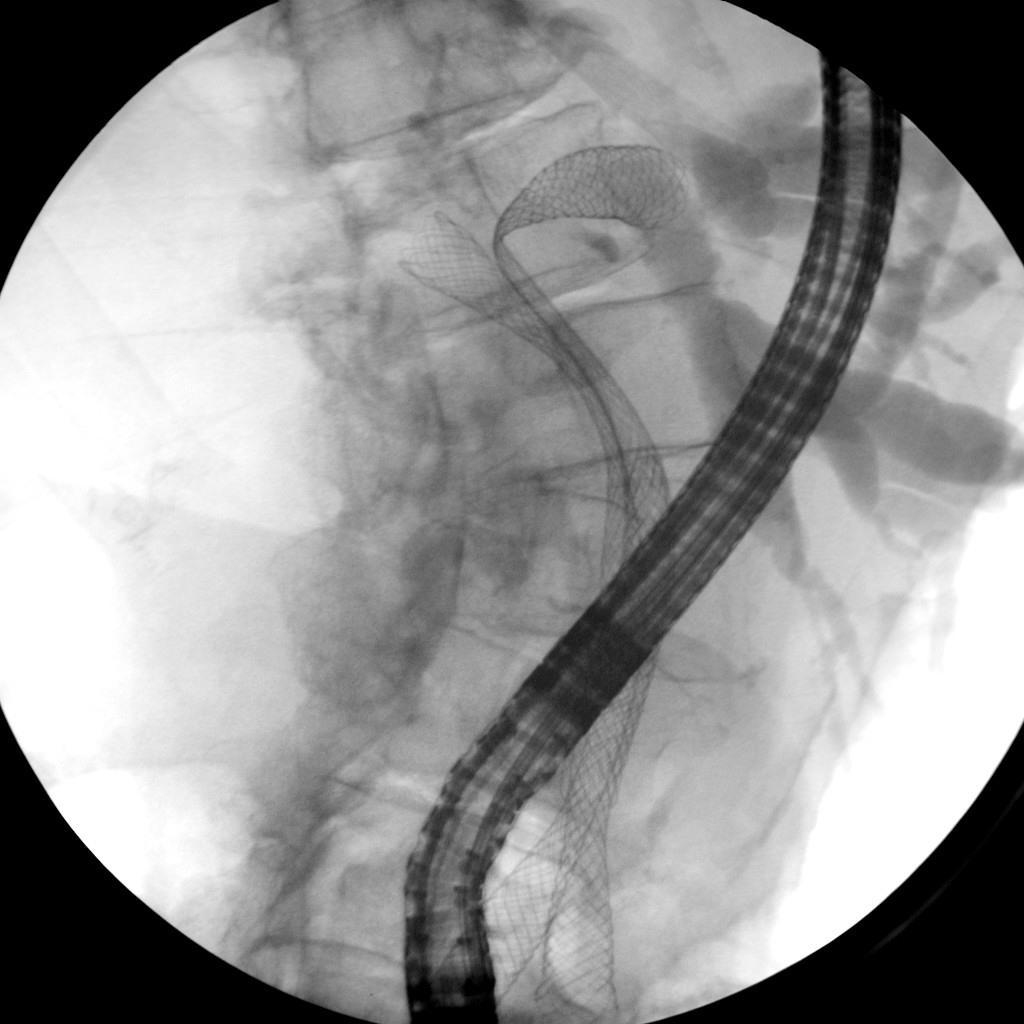
60 Hilar single colorectal metastasis [1]

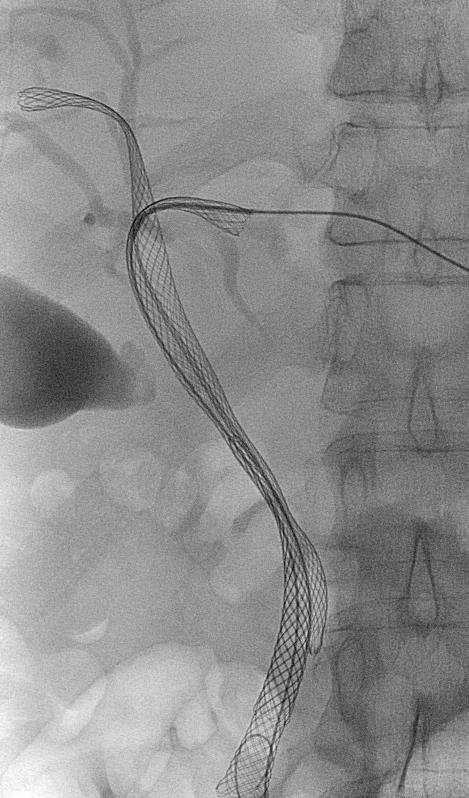

61 Hilar single colorectal metastasis (2)
Severe necrotizing pancreatitis. ICU Fellowship Training Radboudumc
 Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
ERCP / PTC Surgical Laparoscopic vs open Timing and order of approach
 Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Joint Trust Management of Acute Severe Pancreatitis in Adults
 A clinical guideline recommended for use For Use in: By: For: Division responsible for document: All clinical areas (as a reference for screening) ITU/HDU (for definitive care) All medical staff likely
A clinical guideline recommended for use For Use in: By: For: Division responsible for document: All clinical areas (as a reference for screening) ITU/HDU (for definitive care) All medical staff likely
Pancreatic Benign April 27, 2016
 Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Disclosures. Extra-hepatic Biliary Disease and the Pancreas. Objectives. Pancreatitis 10/3/2018. No relevant financial disclosures to report
 Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Acute Pancreatitis. Falk Symposium 161 Dresden
 Acute Pancreatitis Falk Symposium 161 Dresden 12.10.2007 Incidence of Acute Pancreatitis (Malmö) Lindkvist B, et al Clin Gastroenterol Hepatol 2004;2:831-837 Gallstones Alcohol AGA Medical Position Statement
Acute Pancreatitis Falk Symposium 161 Dresden 12.10.2007 Incidence of Acute Pancreatitis (Malmö) Lindkvist B, et al Clin Gastroenterol Hepatol 2004;2:831-837 Gallstones Alcohol AGA Medical Position Statement
Biliary Tree Ultrasound - In a nutshell. Pamela Parker Lead Sonographer
 Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Together, putting patients first
 The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
ERCP and EUS: What s New and What Should We Do?
 ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT
 GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT Name & Title Of Author: Dr Linda Jewes, Consultant Microbiologist Date Amended: December 2016 Approved by Committee/Group: Drugs & Therapeutics
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT Name & Title Of Author: Dr Linda Jewes, Consultant Microbiologist Date Amended: December 2016 Approved by Committee/Group: Drugs & Therapeutics
ACG Clinical Guideline: Management of Acute Pancreatitis
 ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
Management of Pancreatic Fistulae
 Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Management of Acute Pancreatitis and its Complications Aspirus Grand Rounds June 6, 2017 Eric A. Johnson MD
 Management of Acute Pancreatitis and its Complications Aspirus Grand Rounds June 6, 2017 Eric A. Johnson MD Disclosure: None In accordance with the Standards of the Wisconsin Medical Society, all those
Management of Acute Pancreatitis and its Complications Aspirus Grand Rounds June 6, 2017 Eric A. Johnson MD Disclosure: None In accordance with the Standards of the Wisconsin Medical Society, all those
Early management of complicated gallstones and acute pancreatitis
 Early management of complicated gallstones and acute pancreatitis A/Prof Richard Cade George Kalogeropoulos ( Fellow) HPB/Upper GI Unit Eastern Health, Melbourne biliary colic/acute cholecystitis common
Early management of complicated gallstones and acute pancreatitis A/Prof Richard Cade George Kalogeropoulos ( Fellow) HPB/Upper GI Unit Eastern Health, Melbourne biliary colic/acute cholecystitis common
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation
 and Endoscopic Ultrasound correlation") Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
CBD stones & strictures (Obstructive jaundice)
") 1 CBD stones & strictures (Obstructive jaundice) Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA), MHPE (Nl & Eg) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz
1 CBD stones & strictures (Obstructive jaundice) Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA), MHPE (Nl & Eg) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz
Management of Acute Pancreatitis
 Management of Acute Pancreatitis A Clinical Practice Guideline developed by the University of Toronto s Best Practice in Surgery JA Greenberg, M Bawazeer, J Hsu, J Marshall, JO Friedrich, A Nathens, N
Management of Acute Pancreatitis A Clinical Practice Guideline developed by the University of Toronto s Best Practice in Surgery JA Greenberg, M Bawazeer, J Hsu, J Marshall, JO Friedrich, A Nathens, N
Endoscopic Management of Acute Pancreatitis. Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018
 Endoscopic Management of Acute Pancreatitis Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018 Objectives Assessment of acute pancreatitis Early management Who needs an ERCP
Endoscopic Management of Acute Pancreatitis Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018 Objectives Assessment of acute pancreatitis Early management Who needs an ERCP
Acute pancreatitis Case reports. Clinical problems. Use of antibiotics? (P 1 & 2) Surgical treatment of AP? (P 3 & 4)
 Surgical treatment of AP? (P 3 & 4)") Case reports Clinical problems Use of antibiotics? (P 1 & 2) Surgical treatment of AP? (P 3 & 4) Case reports Case 1 Case 1 Patient KD History M, 63 y Obesity BMI 30.3 kg/m 2 Gallbladder stones No concomitant
Case reports Clinical problems Use of antibiotics? (P 1 & 2) Surgical treatment of AP? (P 3 & 4) Case reports Case 1 Case 1 Patient KD History M, 63 y Obesity BMI 30.3 kg/m 2 Gallbladder stones No concomitant
Primary Sclerosing Cholangitis and Cholestatic liver diseases. Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants
 Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
STRICTURES OF THE BILE DUCTS Session No.: 5. Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy
 STRICTURES OF THE BILE DUCTS Session No.: 5 Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy Drainage of biliary strictures. The history before 1980 Surgical bypass Percutaneous
STRICTURES OF THE BILE DUCTS Session No.: 5 Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy Drainage of biliary strictures. The history before 1980 Surgical bypass Percutaneous
9/21/15. Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015
 Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
Jaundice Chris Wells Regional CMT teaching 6 th June 2017
 Jaundice Chris Wells Regional CMT teaching 6 th June 2017 By the end you will Have a systematic approach to the patient with jaundice Be able to diagnose the cause of jaundice Have a framework for managing
Jaundice Chris Wells Regional CMT teaching 6 th June 2017 By the end you will Have a systematic approach to the patient with jaundice Be able to diagnose the cause of jaundice Have a framework for managing
Colangitis Esclerosante Primaria: Manejo Clínico y Endoscópico
 Colangitis Esclerosante Primaria: Manejo Clínico y Endoscópico Andrés Cárdenas, MD, MMSc, PhD, AGAF, FAASLD GI / Liver Unit, Hospital Clinic Institut de Malalties Digestives i Metaboliques Associate Professor
Colangitis Esclerosante Primaria: Manejo Clínico y Endoscópico Andrés Cárdenas, MD, MMSc, PhD, AGAF, FAASLD GI / Liver Unit, Hospital Clinic Institut de Malalties Digestives i Metaboliques Associate Professor
CrackCast Episode 28 Jaundice
 CrackCast Episode 28 Jaundice Episode overview: 1) Describe heme metabolism 2) List common pre-hepatic/hepatic/post-hepatic causes of jaundice Wisecracks: 1) What are clinical signs of liver disease? 2)
CrackCast Episode 28 Jaundice Episode overview: 1) Describe heme metabolism 2) List common pre-hepatic/hepatic/post-hepatic causes of jaundice Wisecracks: 1) What are clinical signs of liver disease? 2)
Biliary Tree Ultrasound - In a nutshell. Pamela Parker Lead Sonographer
 Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Surgical Management of CBD Injury Jin Seok Heo
 Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Biliary tree dilation - and now what?
 Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
EAST MULTICENTER STUDY PROPOSAL
 EAST MULTICENTER STUDY PROPOSAL (Proposal forms must be completed in its entirety, incomplete forms will not be considered) GENERAL INFORMATION Study Title: Prospective Multi-Institutional Evaluation of
EAST MULTICENTER STUDY PROPOSAL (Proposal forms must be completed in its entirety, incomplete forms will not be considered) GENERAL INFORMATION Study Title: Prospective Multi-Institutional Evaluation of
ESPEN Congress The Hague 2017
 ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
PANCREATIC CANCER GUIDELINES
 PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
Disclosures. Overview. Case 1. Common Bile Duct Sizes 10/14/2016. General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis
 Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
Quality & Safety Committee 17 th August 2017 Agenda item: 6.2
 SUMMARY REPORT ABM University Health Board Quality & Safety Committee 17 th August 2017 Agenda item: 6.2 Subject Improvements in the management of gallstone disease Prepared by Approved & presented by:
SUMMARY REPORT ABM University Health Board Quality & Safety Committee 17 th August 2017 Agenda item: 6.2 Subject Improvements in the management of gallstone disease Prepared by Approved & presented by:
Acute Pancreatitis. Encourage You to Read!
 Acute Pancreatitis Laith H. Jamil, MD, FACG Associate Director of Interventional Endoscopy Cedars Sinai Medical Center Los Angeles, CA Encourage You to Read! Copyright 2015 American College of Gastroenterology
Acute Pancreatitis Laith H. Jamil, MD, FACG Associate Director of Interventional Endoscopy Cedars Sinai Medical Center Los Angeles, CA Encourage You to Read! Copyright 2015 American College of Gastroenterology
Surgical Management of Acute Pancreatitis
 Surgical Management of Acute Pancreatitis Steven J. Hughes, MD, FACS Cracchiolo Family Professor of Surgery and Chief, General Surgery Overview Biliary pancreatitis a cost effective algorithm Key concepts
Surgical Management of Acute Pancreatitis Steven J. Hughes, MD, FACS Cracchiolo Family Professor of Surgery and Chief, General Surgery Overview Biliary pancreatitis a cost effective algorithm Key concepts
What can you expect after your ERCP?
 ERCP Explained and respond to bed rest, pain relief and fasting to rest the gut with the patient needing to stay in hospital for only a few days. Some patients develop severe pancreatitis and may require
ERCP Explained and respond to bed rest, pain relief and fasting to rest the gut with the patient needing to stay in hospital for only a few days. Some patients develop severe pancreatitis and may require
Overview of PSC Making the Diagnosis
 Overview of PSC Making the Diagnosis Tamar Taddei, MD Assistant Professor of Medicine Yale University School of Medicine Overview Definition Epidemiology Diagnosis Modes of presentation Associated diseases
Overview of PSC Making the Diagnosis Tamar Taddei, MD Assistant Professor of Medicine Yale University School of Medicine Overview Definition Epidemiology Diagnosis Modes of presentation Associated diseases
A Review of Liver Function Tests. James Gray Gastroenterology Vancouver
 A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
The role of ERCP in chronic pancreatitis
 The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
ESPEN Congress Brussels 2005
 ESPEN Congress Brussels 2005 Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition? Myriam Delhaye Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition?
ESPEN Congress Brussels 2005 Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition? Myriam Delhaye Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition?
Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno. Objectives. Why?
 Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno Objectives Discuss the goals of point-of-care biliary ultrasound Review the
Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno Objectives Discuss the goals of point-of-care biliary ultrasound Review the
Personal Profile. Name: 劉 XX Gender: Female Age: 53-y/o Past history. Hepatitis B carrier
 Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
Spleen indications of splenectomy complications OPSI
 Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
Bile Duct Injury during Lap Chole. Bile Duct Injury during cholecystectomy TOPICS. 1. Prevalence, mechanisms, prevention and diagnosis
 Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Exocrine functions: secretion of digestive enzymes (eg. lipase, amylase,
 Chapter 91 Pancreas Episode Overview: 1. List 10 differential diagnoses for acute pancreatitis 2. List 10 causes of pancreatitis. Which are most common in adults? Which one is most common in pediatrics?
Chapter 91 Pancreas Episode Overview: 1. List 10 differential diagnoses for acute pancreatitis 2. List 10 causes of pancreatitis. Which are most common in adults? Which one is most common in pediatrics?
Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
 Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
Frank Burton Memorial Update on Pancreato-biliary Cancers
 Frank Burton Memorial Update on Pancreato-biliary Cancers Diagnosis and management of pancreatic cancer: common dilemmas Moderators: Banke Agarwal, MD Paul Buse, MD Evaluation of patients with obstructive
Frank Burton Memorial Update on Pancreato-biliary Cancers Diagnosis and management of pancreatic cancer: common dilemmas Moderators: Banke Agarwal, MD Paul Buse, MD Evaluation of patients with obstructive
Tratamiento endoscópico de la CEP. En quien como y cuando?
 Tratamiento endoscópico de la CEP. En quien como y cuando? Andrés Cárdenas, MD, MMSc, PhD, AGAF, FAASLD GI / Liver Unit, Hospital Clinic Institut de Malalties Digestives i Metaboliques University of Barcelona
Tratamiento endoscópico de la CEP. En quien como y cuando? Andrés Cárdenas, MD, MMSc, PhD, AGAF, FAASLD GI / Liver Unit, Hospital Clinic Institut de Malalties Digestives i Metaboliques University of Barcelona
Lutheran Medical Center. Daniel H. Hunt, M.D. June 10 th, 2005
 Lutheran Medical Center Daniel H. Hunt, M.D. June 10 th, 2005 History xx y.o. pt with primary CBD stones s/p ERCP xx months earlier for attempted stone extraction resulting in post ERCP pancreatitis. Patient
Lutheran Medical Center Daniel H. Hunt, M.D. June 10 th, 2005 History xx y.o. pt with primary CBD stones s/p ERCP xx months earlier for attempted stone extraction resulting in post ERCP pancreatitis. Patient
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE. PRESENTED BY: Susan DePasquale, CGRN, MSN
 PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
Acute Pancreatitis:
 American College of Gastroenterology 2014 Acute Pancreatitis Scott Tenner, MD, MPH, FACG Clinical Professor of Medicine State University of New York Health Sciences Center Director, Brooklyn Gastroenterology
American College of Gastroenterology 2014 Acute Pancreatitis Scott Tenner, MD, MPH, FACG Clinical Professor of Medicine State University of New York Health Sciences Center Director, Brooklyn Gastroenterology
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
 Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Ambulatory Emergency Care Pathways. Painless Obstructive Jaundice
 Ambulatory Emergency Care Pathways Painless Obstructive Jaundice Effective Date: December 2011 Content Summary Ref Title Description 1 Condition Details Identifies pathway details and clinical sign-off
Ambulatory Emergency Care Pathways Painless Obstructive Jaundice Effective Date: December 2011 Content Summary Ref Title Description 1 Condition Details Identifies pathway details and clinical sign-off
Endoscopic Ultrasonography Clinical Impact. Giancarlo Caletti. Gastroenterologia Università di Bologna. Caletti
 Clinical Impact Giancarlo Gastroenterologia Università di Bologna AUSL di Imola,, Castel S. Pietro Terme (BO) 1982 Indications Diagnosis of Submucosal Tumors (SMT) Staging of Neoplasms Evaluation of Pancreato-Biliary
Clinical Impact Giancarlo Gastroenterologia Università di Bologna AUSL di Imola,, Castel S. Pietro Terme (BO) 1982 Indications Diagnosis of Submucosal Tumors (SMT) Staging of Neoplasms Evaluation of Pancreato-Biliary
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
ACUTE CHOLANGITIS AS a result of an occluded
 Digestive Endoscopy 2017; 29 (Suppl. 2): 88 93 doi: 10.1111/den.12836 Current status of biliary drainage strategy for acute cholangitis Endoscopic treatment for acute cholangitis with common bile duct
Digestive Endoscopy 2017; 29 (Suppl. 2): 88 93 doi: 10.1111/den.12836 Current status of biliary drainage strategy for acute cholangitis Endoscopic treatment for acute cholangitis with common bile duct
Controversies in the management of acute pancreatitis
 Kathmandu University Medical Journal (3) Vol., No. 3, Issue 7, 3-7 Controversies in the management of acute pancreatitis Singh DR 1, Mehta A, Dangol UMS 3 1 Lecturer, Medical Officer, 3 Lecturer, Dept.
Kathmandu University Medical Journal (3) Vol., No. 3, Issue 7, 3-7 Controversies in the management of acute pancreatitis Singh DR 1, Mehta A, Dangol UMS 3 1 Lecturer, Medical Officer, 3 Lecturer, Dept.
Evaluation and Management of Refractory Biliary Stricture. J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc.
 Evaluation and Management of Refractory Biliary Stricture J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc Outline What defines a refractory biliary stricture Endoscopic
Evaluation and Management of Refractory Biliary Stricture J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc Outline What defines a refractory biliary stricture Endoscopic
ENDOSCOPY IN COMPETITION DIAGNOSTICS. Dr. med. Dirk Hartmann Klinikum Ludwigshafen
 Falk Symposium 166 GI Endoscopy Standards and Innovations Mainz, 18. 19. September 2008 ENDOSCOPY IN COMPETITION DIAGNOSTICS Dr. med. Dirk Hartmann Klinikum Ludwigshafen ENDOSCOPY IN COMPETITION Competing
Falk Symposium 166 GI Endoscopy Standards and Innovations Mainz, 18. 19. September 2008 ENDOSCOPY IN COMPETITION DIAGNOSTICS Dr. med. Dirk Hartmann Klinikum Ludwigshafen ENDOSCOPY IN COMPETITION Competing
Presence of choledocholithiasis in patients undergoing cholecystectomy for mild biliary pancreatitis
 Original Article Presence of choledocholithiasis in patients undergoing cholecystectomy for mild biliary pancreatitis Pradhan S 1, Shah S 2, Maharjan S 2, Shah JN 3 1 2 2 3 Professor, Patan hospital Correspondence:
Original Article Presence of choledocholithiasis in patients undergoing cholecystectomy for mild biliary pancreatitis Pradhan S 1, Shah S 2, Maharjan S 2, Shah JN 3 1 2 2 3 Professor, Patan hospital Correspondence:
Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital
 in a District General Hospital") Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital Poster No.: C-1790 Congress: ECR 2012 Type: Authors: Scientific Exhibit J. A. Maguire 1, H. Kasem 2, M. Akhtar 2, M. Strauss
Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital Poster No.: C-1790 Congress: ECR 2012 Type: Authors: Scientific Exhibit J. A. Maguire 1, H. Kasem 2, M. Akhtar 2, M. Strauss
JAUNDICE. Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc
 JAUNDICE Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc Definition of Jaundice Icterus A yellowish staining of the skin, sclerae and deeper
JAUNDICE Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc Definition of Jaundice Icterus A yellowish staining of the skin, sclerae and deeper
Surveillance proposal consultation document
 Surveillance proposal consultation document 2018 surveillance of Gallstone disease: diagnosis and management (NICE guideline CG188) Proposed surveillance decision We propose to not update the NICE guideline
Surveillance proposal consultation document 2018 surveillance of Gallstone disease: diagnosis and management (NICE guideline CG188) Proposed surveillance decision We propose to not update the NICE guideline
Abnormal Liver Chemistries. Lauren Myers, MMsc. PA-C Oregon Health and Science University
 Abnormal Liver Chemistries Lauren Myers, MMsc. PA-C Oregon Health and Science University Disclosure 1. The speaker/planner Lauren Myers, MMSc, PA-C have no relevant financial relationships to disclose
Abnormal Liver Chemistries Lauren Myers, MMsc. PA-C Oregon Health and Science University Disclosure 1. The speaker/planner Lauren Myers, MMSc, PA-C have no relevant financial relationships to disclose
U Nordic Forum - Trauma & Emergency Radiology. Lecture Objectives. MDCT in Acute Pancreatitis. Acute Pancreatitis: Etiologies
 Nordic Forum - Trauma & Emergency Radiology Lecture Objectives MDCT in Acute Pancreatitis Borut Marincek Institute of Diagnostic Radiology niversity Hospital Zurich, Switzerland To describe the role of
Nordic Forum - Trauma & Emergency Radiology Lecture Objectives MDCT in Acute Pancreatitis Borut Marincek Institute of Diagnostic Radiology niversity Hospital Zurich, Switzerland To describe the role of
Complicated surgical infections
 Complicated surgical infections JASLYN DOSHI ID ADVANCED TRAINEE, WESTMEAD HOPC 46 F admitted 13 th March 2017 Epigastric pain Vomiting Diarrhoea Background Gastric banding 2009 Vomiting since last year
Complicated surgical infections JASLYN DOSHI ID ADVANCED TRAINEE, WESTMEAD HOPC 46 F admitted 13 th March 2017 Epigastric pain Vomiting Diarrhoea Background Gastric banding 2009 Vomiting since last year
ERCP complications and challenges in their diagnosis and management.
 ERCP complications and challenges in their diagnosis and management. Sandie R Thomson Chair of the Division of Gastroenterology, University of Cape Town ERCP Do I have a good Indication? . Algorithm for
ERCP complications and challenges in their diagnosis and management. Sandie R Thomson Chair of the Division of Gastroenterology, University of Cape Town ERCP Do I have a good Indication? . Algorithm for
Best of UEG week 2017 (Pancreas-biliary)
") Best of UEG week 2017 (Pancreas-biliary) Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
Best of UEG week 2017 (Pancreas-biliary) Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
Nothing to declare. Probable causes for the change
 acute pancreatitis March 25, 2017 C. S PITCHUMONI. MD,MACP,MACG,MPH.FRCP (c) Adjunct Professor of Medicine New York Medical College Professor of Medicine Rutgers university Nothing to declare Lesser sac?
acute pancreatitis March 25, 2017 C. S PITCHUMONI. MD,MACP,MACG,MPH.FRCP (c) Adjunct Professor of Medicine New York Medical College Professor of Medicine Rutgers university Nothing to declare Lesser sac?
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
The campaign on laboratory: focus on Gallstone Disease and ERCP
 The campaign on laboratory: focus on Gallstone Disease and ERCP Mauro Giuliani, MD, Specialist in Visceral Surgery, Vice Head Physician, Surgical Ward, Ospedale Regionale di Locarno Alberto Fasoli, MD,
The campaign on laboratory: focus on Gallstone Disease and ERCP Mauro Giuliani, MD, Specialist in Visceral Surgery, Vice Head Physician, Surgical Ward, Ospedale Regionale di Locarno Alberto Fasoli, MD,
7/11/2017. We re gonna help a lot of people today. Biliary/Pancreatic Endoscopy. AGS July 1-2, Kenneth M. Sigman, MD
 Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY
 A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer
 What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
What to do with abnormal LFTs? Andrew M Smith Hepatobiliary Surgeon
 What to do with abnormal LFTs? Andrew M Smith Hepatobiliary Surgeon "it looks like there's something wrong.with your television set. Matt Groenig, creator of The Simpsons Probability of an abnormal screening
What to do with abnormal LFTs? Andrew M Smith Hepatobiliary Surgeon "it looks like there's something wrong.with your television set. Matt Groenig, creator of The Simpsons Probability of an abnormal screening
Rokitansky-Aschoff sinuses are epithelial invaginations in the gallbladder wall that from as a result of increased gallbladder pressures.
 Anatomy The complexity of the biliary tree can be broken down into much simpler segments. The intrahepatic ducts converge to form the right and left hepatic ducts which exit the liver and join to become
Anatomy The complexity of the biliary tree can be broken down into much simpler segments. The intrahepatic ducts converge to form the right and left hepatic ducts which exit the liver and join to become
Sphincter of Oddi Dysfunction: What s the Verdict in 2014?
 SGNA March 2014 Sphincter of Oddi Dysfunction: What s the Verdict in 2014? Evan L. Fogel, M.D. Professor of Clinical Medicine ERCP Fellowship Director Division of Gastroenterology/Hepatology Indiana University
SGNA March 2014 Sphincter of Oddi Dysfunction: What s the Verdict in 2014? Evan L. Fogel, M.D. Professor of Clinical Medicine ERCP Fellowship Director Division of Gastroenterology/Hepatology Indiana University
Complication of Laparoscopic Cholecystectomy
 Complication of Laparoscopic Cholecystectomy R.K.Mishra What to do if something goes wrong There is not a single laparoscopic surgeon in the world who has not damaged CBD Complications Early Common bile
Complication of Laparoscopic Cholecystectomy R.K.Mishra What to do if something goes wrong There is not a single laparoscopic surgeon in the world who has not damaged CBD Complications Early Common bile
Management of Gallbladder Disease. Cory Buschmann, MD PGY-5 11/28/2017
 Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Prophylactic Antibiotics in Severe Acute Pancreatitis: Antibiotics are good. Karen Lo R 3 University of Colorado Oct 11, 2010
 Prophylactic Antibiotics in Severe Acute Pancreatitis: Antibiotics are good Karen Lo R 3 University of Colorado Oct 11, 2010 Overview Pancreas: The History Pancreas: The Organ The Disease Pathogenesis
Prophylactic Antibiotics in Severe Acute Pancreatitis: Antibiotics are good Karen Lo R 3 University of Colorado Oct 11, 2010 Overview Pancreas: The History Pancreas: The Organ The Disease Pathogenesis
Endoscopic treatment of primary sclerosing cholangitis: Is there something new?
 Endoscopic treatment of primary sclerosing cholangitis: Is there something new? Arnaud Lemmers, MD, PhD Gastroenterology Department, Erasme Hospital, ULB, Brussels BASL December 1st 2017 AGENDA Introduction
Endoscopic treatment of primary sclerosing cholangitis: Is there something new? Arnaud Lemmers, MD, PhD Gastroenterology Department, Erasme Hospital, ULB, Brussels BASL December 1st 2017 AGENDA Introduction
PowerPoint Made Easy(er)
") PowerPoint Made Easy(er) Teachers of Tomorrow November 2017 The Problem Objectives The participant will be able to: 1. Select appropriate structural features in PowerPoint to enhance content delivery &
PowerPoint Made Easy(er) Teachers of Tomorrow November 2017 The Problem Objectives The participant will be able to: 1. Select appropriate structural features in PowerPoint to enhance content delivery &
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
Does Sphincter of Oddi Dysfunction Even Exist Anymore?
 Does Sphincter of Oddi Dysfunction Even Exist Anymore? Grace H. Elta, MD, FACG Professor of Medicine University of Michigan Sphincter of Oddi Dysfunction Best studied clinical association: Biliary pain
Does Sphincter of Oddi Dysfunction Even Exist Anymore? Grace H. Elta, MD, FACG Professor of Medicine University of Michigan Sphincter of Oddi Dysfunction Best studied clinical association: Biliary pain
Diagnosis of chronic Pancreatitis. Christoph Beglinger, University Hospital Basel, Switzerland
 Diagnosis of chronic Pancreatitis Christoph Beglinger, University Hospital Basel, Switzerland Pancreatitis Pancreas Pancreas - an organ that makes bicarbonate to neutralize gastric acid, enzymes to digest
Diagnosis of chronic Pancreatitis Christoph Beglinger, University Hospital Basel, Switzerland Pancreatitis Pancreas Pancreas - an organ that makes bicarbonate to neutralize gastric acid, enzymes to digest
Biliary Tract Disease NIKI TADAYON GENERAL & VASCULAR SURGEON SHOHADA TAJRISH HOSPITAL
 Biliary Tract Disease NIKI TADAYON GENERAL & VASCULAR SURGEON SHOHADA TAJRISH HOSPITAL Differential Diagnosis of RUQ pain Gallstone disease (and its related complications) Gastritis/duodenitis Peptic ulcer
Biliary Tract Disease NIKI TADAYON GENERAL & VASCULAR SURGEON SHOHADA TAJRISH HOSPITAL Differential Diagnosis of RUQ pain Gallstone disease (and its related complications) Gastritis/duodenitis Peptic ulcer
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013
 Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
CLINICAL GUIDELINE FOR MANAGEMENT OF GALLSTONES PATHOLOGY IN ADULTS
 CLINICAL GUIDELINE FOR MANAGEMENT OF GALLSTONES PATHOLOGY IN ADULTS 1. Aim/Purpose of this Guideline This guideline is for the management of gallstones pathology in adults. It has been benchmarked against
CLINICAL GUIDELINE FOR MANAGEMENT OF GALLSTONES PATHOLOGY IN ADULTS 1. Aim/Purpose of this Guideline This guideline is for the management of gallstones pathology in adults. It has been benchmarked against
Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine
 Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine Endoscopy & Chronic Pancreatitis Diagnosis EUS ERCP Exocrine Function
Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine Endoscopy & Chronic Pancreatitis Diagnosis EUS ERCP Exocrine Function
6 th August 2018 Day 1 - Gallbladder & Bile duct Topic
 Venue: Sterling Hospital Auditorium, Sterling Hospitals, Gurukul Road Ahmedabad, Gujarat 6 th August 2018 Day 1 - Gallbladder & Bile duct Registration(8:00am-8:15am) Inauguration(8:15am-8:30am) Welcome
Venue: Sterling Hospital Auditorium, Sterling Hospitals, Gurukul Road Ahmedabad, Gujarat 6 th August 2018 Day 1 - Gallbladder & Bile duct Registration(8:00am-8:15am) Inauguration(8:15am-8:30am) Welcome
Emergency Surgery Course Graz, March ACUTE PANCREATITIS. Carlos Mesquita Coimbra
 ACUTE PANCREATITIS Carlos Mesquita Coimbra ESSENTIALS (1) AP occurs when digestive enzymes become activated while still in the pancreas, causing inflammation repeated bouts of AP can lead to chronic pancreatitis
ACUTE PANCREATITIS Carlos Mesquita Coimbra ESSENTIALS (1) AP occurs when digestive enzymes become activated while still in the pancreas, causing inflammation repeated bouts of AP can lead to chronic pancreatitis
Chronic Pancreatitis. Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture
 Chronic Pancreatitis Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture What is Chronic Pancreatitis Progressive inflammatory disease Pancreatic parenchyma replaced w/fibrous tissue Destruction
Chronic Pancreatitis Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture What is Chronic Pancreatitis Progressive inflammatory disease Pancreatic parenchyma replaced w/fibrous tissue Destruction
GALLBLADDER CANCER. Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011
 GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
Pathophysiology ACUTE PANCREATITIS
 Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation