TB Special Situations Case Discussions
|
|
|
- Alison O’Brien’
- 5 years ago
- Views:
Transcription
1 TB Special Situations Case Discussions Chris Keh, MD TB Control, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, UCSF Curry International Tuberculosis Center, Clinical Intensive, September 16, 2016 Special Situations Diabetes Pregnancy Hepatic Disease Advanced Age Renal Disease Chris Keh, MD 1


2 Case 1 55 yo diabetic M, presents with cough, hemoptysis, weight loss x 3 months 55 yo diabetic M On three different oral DM medications HbA1c=10% Smear positive x 3, numerous GeneXpert- MTBC detected, rifampin resistance detected Next steps? Chris Keh, MD 2
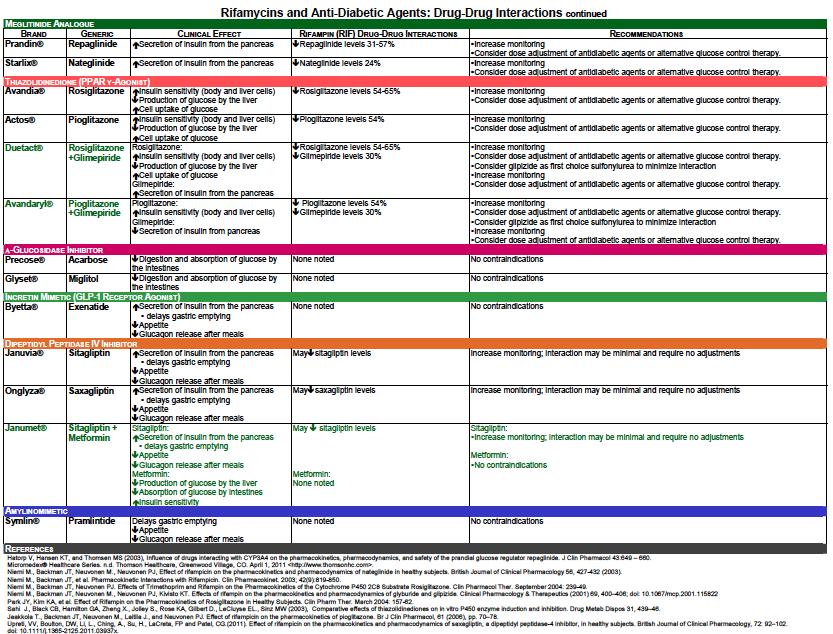
3 Diabetes + TB Patients with risk factors for DM should be screened with fasting glucose or HbA1c ADA risk factors include: Age >45, BMI >25, first-degree relative with DM, and race/ethnicity (African American, Asian, Hispanic, American Indian/Alaska Native, or Hawaiian Native/Pacific Islander Diabetes + TB Drug-drug interactions Sulfonylureas- RIF decreases concentration Thiazolidinedione- RIF decreases concentration Dipeptidyl peptidase inhibitor- RIF decreases concentration Rifampin alone has been associated with hyper/hypoglycemia in DM and non-dm patients Chris Keh, MD 3

4 Chris Keh, MD 4
 Yes Higher treatment failure ++/- Increased mortality / poor treatment outcome ++/- Chiang, et al. PLOS One, 2016 Dooley, et al. Lancet ID, 2009 Jimenez-Corona, Thorax, 2013 Baker, et al.")
5 Diabetes + TB Factors Evidence References Increased risk of progression to TB (Relative risk of progression to active TB 2-4.1) Yes Higher treatment failure ++/- Increased mortality / poor treatment outcome ++/- Chiang, et al. PLOS One, 2016 Dooley, et al. Lancet ID, 2009 Jimenez-Corona, Thorax, 2013 Baker, et al. BMC Medicine, 2011 Low drug levels (?clinical significance) Yes Hanneke, et al. CID, 2006 Ruslami, AAC, 2010 Heysel, 2010, 2013 Increased risk of drug-resistant TB +/- Jimenez-Corona, Thorax, 2013 Diabetes + TB Radiographic presentation may vary, but studies are mixed: More cavities Lower lung involvement CITC/FirlandTB Image Library; Masa Narita, MD, ThienkhaiVu, MD. Chris Keh, MD 5
6 55 yo diabetic M PSQ with no INH mutations detected; presence of RIF resistance DST confirms rifampin mono-resistance RIF d/c d, unable to tolerate PZA. Multiple med re-challenge due to GI side effects Complains of pill burden and ongoing GI distress Blood sugars Eventually on stable regimen of INH/EMB/FQ/injectable Remained numerous smear positive through month 2 Next steps? Diabetes- length of TB treatment Patients with DM and either cavitation on initial CXR OR positive culture at 2 months should be followed more closely with consideration to extend treatment. Some experts recommend extending treatment to 9 months in poorly controlled DM. Executive Summary: Official ATS/CDC/IDSA Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis. Clin Infect Dis Oct 1;63(7): Chris Keh, MD 6
 Controversial Unclear clinical significance in all-comers- reports of both no impact vs poor outcome on treatment cure/relapse Typically peak levels drawn (2-3 hours post-dose),")
7 Diabetes- treatment may be more difficult Peripheral neuropathy Diabetic Gastroparesis Diabetic retinopathy CKD Drug-drug interactions Rifampin increases intestinal absorption of glucose Therapeutic drug monitoring (TDM) Controversial Unclear clinical significance in all-comers- reports of both no impact vs poor outcome on treatment cure/relapse Typically peak levels drawn (2-3 hours post-dose), with later level (6 hours) if delayed absorption is suspected refer to the drug guide Samples need prompt processing (INH, ethionamide are unstable at room temp in whole blood/serum, followed by RIF, rest lkely stable x 24 hours) Peloquin CA.,et al. Drugs Jun;74(8): Chris Keh, MD 7
 Drug-Drug Interactions (e.g. ART) Diabetes 2 nd line drugs Peloquin CA.,et al. Drugs. 2014 Jun;74(8):839-54. Case 2 25 yo Chinese G1P0, PPD+ Chris Keh, MD 8")
8 Therapeutic drug monitoring (TDM) When might this be helpful? Poor response to MTB treatment (radiographic, microbiologic, or clinical) GI issues or suspected absorption issues (e.g. chronic diarrhea, gastroparesis, short bowel syndrome, IBD) Kidney disease (e.g. CKD, PD, CRRT) Drug-Drug Interactions (e.g. ART) Diabetes 2 nd line drugs Peloquin CA.,et al. Drugs Jun;74(8): Case 2 25 yo Chinese G1P0, PPD+ Chris Keh, MD 8


9 25 yo pregnant F CXR- left apical nodularity, scarring and volume loss which likely represent sequelae of old granulomatous disease. Recommend correlation with prior imaging. Immigrated from China in 2013 Chronic cough x month. Sore throat and hoarseness x 1 week. 36 weeks pregnant Next steps? 25 yo pregnant F Repeat CXR- unchanged left apical scarring consistent with sequelae of prior granulomatous disease Sputum- numerous smear positive (x3) GeneXpert- MTBC detected, no rifampin resistance detected Next steps? Chris Keh, MD 9
 Next steps? Pregnancy Pregnancy does not increase the risk for progression to active TB Routine screening not indicated unless high risk for infection (e.")
10 25 yo pregnant F Sputum- numerous smear positive GeneXpert- MTBC detected, no rifampin resistance detected CT- left apical scarring with bronchiectasis and calcification, likely sequelae of prior granulomatous disease (done after delivery) Next steps? Pregnancy Pregnancy does not increase the risk for progression to active TB Routine screening not indicated unless high risk for infection (e.g FB) or progression (e.g. recent contact, immunosuppressed) However, if screening is positive, CXR indicated as soon as possible. Abnormal CXR should have expedited evaluations Monitoring LFT baseline and ongoing monitoring due to risk for hepatoxicity, likely highest in 3 rd trimester and 1 st 3 months post-partum Frequent sputums to assess infectiousness * WHO Guidelines for treatment of tuberculosis, 4 th edition. Chris Keh, MD 10
11 Pregnancy- treatment PZA is controversial in the US due to lack of safety data More strongly considered if HIV+, extrapulmonary, severe TB, drug-resistant WHO* and IUATLD recommends all 4 drugs Some experts recommend all 4 drugs based on above and the fact that PZA has been used for years in high endemic countries All 4 first-line drugs are category C Administer pyridoxine given risk for neuropathy Aminoglycosides with known teratogenicity. Use of 2 nd line agentsseek consultation Duration of treatment is the same as in non-pregnant pansusceptible disease Executive Summary: Official ATS/CDC/IDSA Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis. Clin Infect Dis Oct 1;63(7): WHO Guidelines for treatment of tuberculosis, 4 th edition. 25 yo pregnant F, 37 weeks Patient was started on RIPE 1 week f/u: tolerating meds, LFT normal Home contacts include- 3 adults + 3 kids She participated in 3-hour pre-natal classes Next steps? Chris Keh, MD 11
12 Contact evaluation and Infection Control Home Outpatient OB clinic Inpatient delivery plan Mother Determination of isolation procedures- pre/peri/post Placenta for path and culture Baby Evaluation for congenital TB Physical exam- fever, irritability, HSM, LAD, cough, poor feeding CXR If concerns for congenital TB: gastric aspirates, LP, sepsis w/u, start RIPE Decision of window prophylaxis if congenital TB work-up negative 25 yo pregnant F, 39 weeks Household contacts 1 st test negative 4/10 outpatient OB providers TST neg Mom admitted for induction due to oligohydramnios Smear neg x 1 Next steps? Chris Keh, MD 12

13 Baby evaluation Baby evaluation Evidence of chorioamnionitis Baby required minimal Bipap/cpap due to stunning Initially started on window proph, then expanded to RIPE after sleepiness, hypoglycemia, and temp instability Started on amp/gent LP unremarkable Gastric aspirates done Mother: Smear neg x 3 Next steps? Chris Keh, MD 13
.")
14 Breastfeeding Small concentrations of TB medications (not enough to provide treatment) are detected in breast milk and have not been reported to cause toxicity to the nursing infant. Thus, breastfeeding is encouraged in non-infectious women on 1 st line medications. Exclusively breast-fed infants should receive supplementary pyridoxine (1-2 mg/kg/day). Case 3 44 yo Korean M, immigration evaluation Chris Keh, MD 14

15 44 yo Korean immigrant Screening labs include: HBV sag positive, sab negative HIV neg, HbA1c 6% LFT normal, INR normal Asymptomatic Sputum smear positive GeneXpert- MTBC detected, no rifampin resistance detected Next steps? CITC/FirlandTB Image Library; Masa Narita, MD, ThienkhaiVu, MD yo Korean immigrant You provide counseling and the patient has never been given a diagnosis of hepatitis B. Due to smear positivity, liver imaging will be delayed Patient does not have a PCP or insurance due to new immigration status. Next steps? Chris Keh, MD 15

:853-67.")
16 When do you consider an alternate regimen? ALT >3x ULN at baseline, not due to TB Prior history of hepatotoxicity to TB meds Advanced liver disease, e.g. cirrhosis/esld By ultrasound or CT By markers of end-stage liver disease (ESLD)- INR, bilirubin, AST/ALT, bilirubin Consider liver-sparing regimen Executive Summary: Official ATS/CDC/IDSA Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis. Clin Infect Dis Oct 1;63(7): Drug-induced Liver Injury (DILI) Causative: PZA (1%) INH Asymptomatic elevation <5x ULN in 10-20% Clinical hepatitis, % depending on combo Fatal hepatitis <0.023% RIF rare except in combination with other drugs Asymptomatic hyperbilirubinemia (0.6%) Cholestatic pattern of hepatitis Chris Keh, MD 16
17 44 yo Korean immigrant with chronic HBV RIPE is started 1 week later: AST 80, ALT 120 (asymptomatic) 2 weeks later: AST 250, ALT 300 (fatigue) Next steps? DILI (management) HOLD medications for the following or any GI complaint: abdominal pain, diarrhea, fatigue, nausea/vomiting, anorexia, malaise, jaundice, dark urine. Check LFT s If LFT <5x upper limit of normal (ULN) and asymptomatic, okay to restart but may need closer monitoring. If LFT <3x ULN and symptomatic, okay to restart with supportive measures, e.g. treatment of gastritis or nausea. May need closer monitoring. Chris Keh, MD 17
18 DILI (management) STOP medications for the following: Asymptomatic + LFT >5x upper limit of normal (ULN) Symptomatic + LFT >3x ULN Screen for hepatitis (A, B, C) or other underlying causes of liver disease (alcohol use, other hepatotoxic medications). Check INR. Determine if urgent evaluation or admission is needed (e.g. >10x ULN or any evidence of liver failure- asterixis, confusion, dehydration, coagulopathy) 44 yo Korean immigrant with chronic HBV, AST/ALT rise Meds are held Med list reviewed- none No ETOH reported Liver US- unremarkable 1 week follow-up: symptoms resolved and AST/ALT 50/40 Smears are still positive Next steps? Chris Keh, MD 18
19 DILI (re-challenge) Monitor LFTs weekly until 2x ULN (some programs completely normal), before re-challenging with medications. If severe TB disease, may need to start liver-sparing regimen. Seek consultation in re-introduction of medications Choice in med re-challenge depends on co-morbidities (cirrhosis), degree of hepatitis (mild vs severe), susceptibilities (pan-susceptible or pending), phase (initial or continuation), and most likely suspect (PZA/INH>RIF). Typically, start least suspect agent first (along w/ non-hepatotoxic meds), monitor LFTs in 3-7 days, and if remain normal then rechallenge with next agent. 44 yo Korean immigrant with chronic HBV, AST/ALT rise EMB restarted 3 days later, AST/ALT normal and rifampin restarted 1 week later, AST/ALT normal and INH restarted 1 week later, AST/ALT are 180/150 with nausea Next steps? What would be your potential alternate regimens? Chris Keh, MD 19
20 Hepatic Disease Most likely hepatotoxic medications: PZA, INH >> RIF If you avoid PZA Alternate treatment RIF + INH + EMB x 2 months, followed by 7 mo RIF + INH INH + PZA RIF + EMB + FQ/injectable/cycloserine x mo INH INH + PZA + RIF Little to no potential of DILI RIF + PZA + EMB x 6 mo EMB + FQ + cycloserine +/- injectable x mo Executive Summary: Official ATS/CDC/IDSA Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis. Clin Infect Dis Oct 1;63(7): Case 4 96 yo Indian F diagnosed with pulmonary TB Chris Keh, MD 20
21 96 yo F with pulm TB Numerous smear positive disease CXR- RUL cavity Weight 85 lbs Creatinine 1.0 How do you proceed? Advanced Age Risk of DILI (drug-induced livery injury) increases with age Some experts avoid PZA in pts >75 yo Risk / benefit decisions on RIPE vs RIE vs RIE+FQ Consider severity of disease and bacillary load Consider risk for drug resistance Consider risk for DILI Close medication review due to drug-drug interactions needed Executive Summary: Official ATS/CDC/IDSA Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis. Clin Infect Dis Oct 1;63(7): Chris Keh, MD 21
22 Advanced Age Low BMI / malnutrition is often an issue: Close monitoring of weight and dose adjustments May need nutritional supplementation Creatinine may not accurately reflect actual CrCl/GFR due to low muscle mass. Calculation recommended. Close medication review needed due to drug-drug interactions and an ever-changing polypharmaceutical list (often includes anti-htn, thyroid replacement, antidepressants, and blood thinners) Associated with higher mortality and poor outcomes. Yen, et al. Int J Tuberc Lung Dis Oct;17(10): Wang, et al. Infection Aug;36(4): Lin, et al. Age Ageing May;44(3): yo F with pulm TB- back to the case Calculated CrCl~19.9 She has a history of PE on coumadin, HTN, DM In addition, you find out that she lives at home with her daughter, son-in-law, and 4 grandchildren (ages 6 months, 4 yo, 7 yo, 10 yo) GeneXpert- MTBC detected, rifampin resistance not detected How do you proceed? Chris Keh, MD 22
23 Renal Disease Requires dose / frequency adjustment Pyrazinamide mg/kg TIW Ethambutol mg/kg TIW Levofloxacin mg TIW No adjustment Rifampin Isoniazid Moxifloxacin All TB medications should be ideally given after HD on HD days. Consider monitoring drug levels PD- no data available Executive Summary: Official ATS/CDC/IDSA Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis. Clin Infect Dis Oct 1;63(7): yo F with pulm TBdiscussion points EMB/PZA should be renally dosed Consideration of drug-drug interactions-?use rifabutin vs discuss with PCP need for interacting medications Risk / benefit discussion regarding 4 drugs- heavy burden of disease + high risk contacts at home vs. DDI and potential for toxicity Consider nutrition status and how to improve Chris Keh, MD 23
 Your")

24 Assistance is right around the corner CITC warmline: (toll-free) Your friendly neighborhood TB controller Turn around to those sitting next to you in the room Chris Keh, MD 24
TB Case Management Hepatitis
 TB Case Management Hepatitis Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
TB Case Management Hepatitis Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
Standard TB Treatment
 Standard TB Treatment Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
Standard TB Treatment Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
6/8/2018 TB TREATMENT. Bijan Ghassemieh, MD Seattle TB Clinical Intensive Disclosures. None
 TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
TB Grand Rounds. Reynard McDonald, MD & Henry Fraimow, MD January 30, Outline
 TB Grand Rounds Reynard McDonald, MD & Henry Fraimow, MD January 30, 2007 Outline Overview of 2006 ATS statement regarding hepatotoxicity of anti-tb therapy Case examples highlighting management of patients
TB Grand Rounds Reynard McDonald, MD & Henry Fraimow, MD January 30, 2007 Outline Overview of 2006 ATS statement regarding hepatotoxicity of anti-tb therapy Case examples highlighting management of patients
Treatment of Tuberculosis
 TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Tuberculosis and Diabetes Dec. 10, 2009 Dean Schillinger, M.D. and Gisela Schecter, M.D., M.P.H. 1 of 18
 Screening, Diagnosis, and Treatment of TB in Persons with Diabetes Dean Schillinger, M.D. University of California San Francisco CA Diabetes Program Gisela Schecter, M.D., M.P.H. TB Control Branch CA Department
Screening, Diagnosis, and Treatment of TB in Persons with Diabetes Dean Schillinger, M.D. University of California San Francisco CA Diabetes Program Gisela Schecter, M.D., M.P.H. TB Control Branch CA Department
Treatment of Latent TB Infection (LTBI)
") Treatment of Latent TB Infection (LTBI) Mahesh C. Patel, MD June 14, 2017 2014 MFMER slide-1 Mahesh C. Patel, MD Associate Professor Treatment of LTBI Department of Internal Medicine, Division of Infectious
Treatment of Latent TB Infection (LTBI) Mahesh C. Patel, MD June 14, 2017 2014 MFMER slide-1 Mahesh C. Patel, MD Associate Professor Treatment of LTBI Department of Internal Medicine, Division of Infectious
Pre-Treatment Evaluation. Treatment of Latent TB Infection (LTBI) Initiating Treatment: Patient Education. Before initiating treatment for LTBI:
 Initiating Treatment: Patient Education. Before initiating treatment for LTBI:") Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Drug Interactions Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Management of MDR TB in special situations. Dr Sarabjit Chadha The Union
 Management of MDR TB in special situations Dr Sarabjit Chadha The Union MDR TB in special situations Pregnancy Breastfeeding Contraception Renal Insufficiency Diabetes Pregnancy and TB Pregnancy is not
Management of MDR TB in special situations Dr Sarabjit Chadha The Union MDR TB in special situations Pregnancy Breastfeeding Contraception Renal Insufficiency Diabetes Pregnancy and TB Pregnancy is not
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Treatment of Tuberculosis
 Treatment of Tuberculosis, 1940 s Treatment of Tuberculosis ATS/CDC/IDSA Joint Statement 2003 Saskatchewan Lung Association Outline, 2012 Treatment of Tuberculosis Principles of treatment of tuberculosis
Treatment of Tuberculosis, 1940 s Treatment of Tuberculosis ATS/CDC/IDSA Joint Statement 2003 Saskatchewan Lung Association Outline, 2012 Treatment of Tuberculosis Principles of treatment of tuberculosis
Treating TB What Happened? All the Patients Have Challenging Co-Morbid Conditions Now!
 EXCELLENCE EXPERTISE INNOVATION Treating TB What Happened? All the Patients Have Challenging Co-Morbid Conditions Now! Barbara J Seaworth, MD, Medical Director, Heartland National TB Center Professor,
EXCELLENCE EXPERTISE INNOVATION Treating TB What Happened? All the Patients Have Challenging Co-Morbid Conditions Now! Barbara J Seaworth, MD, Medical Director, Heartland National TB Center Professor,
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Disclosures. Outline. No disclosures or conflicts of interest to report. Special LTBI situations. H t it d id ff t
 Selected Topics in LTBI June 2, 2015 Bijan Ghassemieh, MD Senior Fellow UW Division of Pulmonary/Critical Care Disclosures No disclosures or conflicts of interest to report Outline Special LTBI situations
Selected Topics in LTBI June 2, 2015 Bijan Ghassemieh, MD Senior Fellow UW Division of Pulmonary/Critical Care Disclosures No disclosures or conflicts of interest to report Outline Special LTBI situations
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
Managing Complex TB Cases Diana M. Nilsen, MD, RN
 Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB and Comorbidities Adriana Vasquez, MD April 12, 2018
 TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
Treatment of Active Tuberculosis
 Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015
 Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 Initiation Phase Part 1 Ginny Dowell, RN, BSN February 4, 2015 Ginny Dowell RN, BSN has the following disclosures to make:
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 Initiation Phase Part 1 Ginny Dowell, RN, BSN February 4, 2015 Ginny Dowell RN, BSN has the following disclosures to make:
Chapter 5 Treatment for Latent Tuberculosis Infection
 Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Managing the Patients Response to TB Treatment
 Managing the Patients Response to TB Treatment Barbarah Martinez, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Barbarah Martinez, RN, BSN has
Managing the Patients Response to TB Treatment Barbarah Martinez, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Barbarah Martinez, RN, BSN has
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Latent TB Infection Treatment
 Latent TB Infection Treatment Douglas B. Hornick, MD Pulmonologist w/ Infectious Attitude Division of Pulmonary/Critical Care/Occ Med UI Carver College of Medicine 2014 MFMER slide-1 Disclosures: None
Latent TB Infection Treatment Douglas B. Hornick, MD Pulmonologist w/ Infectious Attitude Division of Pulmonary/Critical Care/Occ Med UI Carver College of Medicine 2014 MFMER slide-1 Disclosures: None
Treatment of Tuberculosis
 Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
SA TB Guidelines The interface with Advanced Clinical Care
 SA TB Guidelines The interface with Advanced Clinical Care Dr Kogie Naidoo (MBCHB, PHD) Head: CAPRISA Treatment Research Programme Honorary Lecturer - UKZN Department of Public Heath Medicine Annual Workshop
SA TB Guidelines The interface with Advanced Clinical Care Dr Kogie Naidoo (MBCHB, PHD) Head: CAPRISA Treatment Research Programme Honorary Lecturer - UKZN Department of Public Heath Medicine Annual Workshop
Anti Tuberculosis Medications: Side Effects & adverse Events
 Anti Tuberculosis Medications: Side Effects & adverse Events Diana Fortune, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Diana Fortune, RN,
Anti Tuberculosis Medications: Side Effects & adverse Events Diana Fortune, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Diana Fortune, RN,
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Tuberculosis Intensive November 17 20, 2015 San Antonio, TX
 Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
MANAGEMENT OF DILI in TB/HIV coinfected patients. Chimoio 31 August 2017 by Dr Ndiviwe Mphothulo
 MANAGEMENT OF DILI in TB/HIV coinfected patients Chimoio 31 August 2017 by Dr Ndiviwe Mphothulo ANTI-TB drugs Groups Drugs Group 1: First-line oral drugs Ethambutol (Emb) Pyrazinamide(PZA) Isoniazid (INH)
MANAGEMENT OF DILI in TB/HIV coinfected patients Chimoio 31 August 2017 by Dr Ndiviwe Mphothulo ANTI-TB drugs Groups Drugs Group 1: First-line oral drugs Ethambutol (Emb) Pyrazinamide(PZA) Isoniazid (INH)
Utilizing All the Tools in the TB Toolbox
 Utilizing All the Tools in the TB Toolbox Sandra Morano, B.A., R.N. Public Health Nurse, City of Stamford, CT TB Talk The New England TB Consortium March 18, 2010 Background TB Program, City of Stamford,
Utilizing All the Tools in the TB Toolbox Sandra Morano, B.A., R.N. Public Health Nurse, City of Stamford, CT TB Talk The New England TB Consortium March 18, 2010 Background TB Program, City of Stamford,
MEDICAL MANAGEMENT OF TB
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE MEDICAL MANAGEMENT OF TB LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the recommended treatment
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE MEDICAL MANAGEMENT OF TB LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the recommended treatment
Debbie Onofre, RN, BSN March 18, TB Nurse Case Management March 17 19, 2015 San Antonio, Texas
 Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Debbie Onofre, RN, BSN March 18, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION
Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Debbie Onofre, RN, BSN March 18, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION
LTBI Videos-Treatment
 LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012
 TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012 Challenges of TB Treatment in Special Populations in Corrections Marcos Burgos, MD November 28, 2012 Marcos Burgos, MD has the following
TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012 Challenges of TB Treatment in Special Populations in Corrections Marcos Burgos, MD November 28, 2012 Marcos Burgos, MD has the following
Treatment: First Line Drugs TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS TREATMENT: GENERAL PRINCIPLES MECHANISM OF ACTION MID 27
 TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS Treatment: First Line Drugs 1. ISONIAZID = INH Bacteriocidal against dividing organisms Dose = 300mg = one pill = well absorbed Good CNS penetration Can be
TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS Treatment: First Line Drugs 1. ISONIAZID = INH Bacteriocidal against dividing organisms Dose = 300mg = one pill = well absorbed Good CNS penetration Can be
Substance Abuse and Tuberculosis Springfield, IL April 27, 2011
 Substance Abuse and Tuberculosis Springfield, IL April 27, 2011 Co-morbidities in Substance Abuse that Impact Managing TB Lisa Armitige, MD, PhD April 27, 2011 Lisa Armitige, MD, PhD has the following
Substance Abuse and Tuberculosis Springfield, IL April 27, 2011 Co-morbidities in Substance Abuse that Impact Managing TB Lisa Armitige, MD, PhD April 27, 2011 Lisa Armitige, MD, PhD has the following
TB Intensive San Antonio, Texas May 7-10, 2013
 TB Intensive San Antonio, Texas May 7-10, 2013 TB and Diabetes Barbara Seaworth, MD May 09, 2013 Barbara Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial
TB Intensive San Antonio, Texas May 7-10, 2013 TB and Diabetes Barbara Seaworth, MD May 09, 2013 Barbara Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB Nurse Assessment. Ginny Dowell, RN, BSN October 21, 2015
 TB Nurse Assessment Ginny Dowell, RN, BSN October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19-22, 2015 Wichita, KS EXCELLENCE EXPERTISE INNOVATION Ginny Dowell,
TB Nurse Assessment Ginny Dowell, RN, BSN October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19-22, 2015 Wichita, KS EXCELLENCE EXPERTISE INNOVATION Ginny Dowell,
TB in Foreign Born and High Risk Populations
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 TB in Foreign Born and High Risk Populations John J. Nava, M.D. December 9, 2009 Tuberculosis in High Risk Populations and the Foreign Born
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 TB in Foreign Born and High Risk Populations John J. Nava, M.D. December 9, 2009 Tuberculosis in High Risk Populations and the Foreign Born
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
LTBI in Special Populations John Nava, MD October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
5. HIV-positive individuals treated with INH should receive Pyridoxine (B6) 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH
 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH") V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
Dosage and Administration
 SIRTURO product information for healthcare providers 2 WARNINGS: An increased risk of death was seen in the SIRTURO (bedaquiline) treatment group (9/79, 11.4%) compared to the placebo treatment group (2/81,
SIRTURO product information for healthcare providers 2 WARNINGS: An increased risk of death was seen in the SIRTURO (bedaquiline) treatment group (9/79, 11.4%) compared to the placebo treatment group (2/81,
Treatment of Tuberculosis, 2017
 Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 TB and Diabetes Barbara Seaworth, MD November 13, 2014 Barbara Seaworth, MD has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas November 11 14, 2014 TB and Diabetes Barbara Seaworth, MD November 13, 2014 Barbara Seaworth, MD has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas April 9-11, 2013
 TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
Dose Counting Exercise Elizabeth Foy, RN, BSN September 8, 2016
 Dose Counting Exercise Elizabeth Foy, RN, BSN September 8, 2016 TB Nurse Case Management September 7-9, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Jessica Quintero, M.Ed., has the following disclosures
Dose Counting Exercise Elizabeth Foy, RN, BSN September 8, 2016 TB Nurse Case Management September 7-9, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Jessica Quintero, M.Ed., has the following disclosures
MDR TB/HIV INTEGRATION MDR TB WORKSHOP 18 SEPTEMBER 2015
 MDR TB/HIV INTEGRATION MDR TB WORKSHOP 18 SEPTEMBER 2015 HIV & MDR :Impact of early ART initiation Adjusted HR: 0.14; p = 0.042 86% reduction in mortality with ART Initiation during MDR-TB treatment 2015
MDR TB/HIV INTEGRATION MDR TB WORKSHOP 18 SEPTEMBER 2015 HIV & MDR :Impact of early ART initiation Adjusted HR: 0.14; p = 0.042 86% reduction in mortality with ART Initiation during MDR-TB treatment 2015
TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION
 TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION Michelle Haas, M.D. Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION Michelle Haas, M.D. Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
TB Classification (ATS/CDC)
") bits and pieces Lisa Chen, MD UCSF Pulmonary/Critical Care Curry International Tuberculosis Center 10/2017 TB Classification (ATS/CDC) TB0 No tuberculosis exposure, not infected TB1 Tuberculosis exposure,
bits and pieces Lisa Chen, MD UCSF Pulmonary/Critical Care Curry International Tuberculosis Center 10/2017 TB Classification (ATS/CDC) TB0 No tuberculosis exposure, not infected TB1 Tuberculosis exposure,
My heart is racing. Managing Complex Cases. Case 1. Case 1
 Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer
 Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Treatment and Monitoring
 Treatment and Monitoring Disclosures We have no actual or potential conflicts of interest in relation to this presentations. We have no financial relationships to disclose. Learning Objectives After this
Treatment and Monitoring Disclosures We have no actual or potential conflicts of interest in relation to this presentations. We have no financial relationships to disclose. Learning Objectives After this
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
Case 1: Clinical Presentation
 Impostors and Preconceived Notions: Lessons Learned in TB Diagnosis & Treatment Tuberculosis Nursing Workshop June 1, 2015 Christopher Spitters, MD, MPH Tuberculosis Clinic Public Health Seattle & King
Impostors and Preconceived Notions: Lessons Learned in TB Diagnosis & Treatment Tuberculosis Nursing Workshop June 1, 2015 Christopher Spitters, MD, MPH Tuberculosis Clinic Public Health Seattle & King
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas April 6-8, 2011 TB Disease: ATS/CDC/IDSA Guidelines Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received
TB Intensive San Antonio, Texas April 6-8, 2011 TB Disease: ATS/CDC/IDSA Guidelines Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received
Rehuka Khurana, MD, MPH has the following disclosures to make:
 Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric TB: Treatment of Tuberculosis Disease Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [with help from Andrea Cruz, M.D.] Objectives At the end
Advanced Concepts in Pediatric TB: Treatment of Tuberculosis Disease Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [with help from Andrea Cruz, M.D.] Objectives At the end
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
Treatment of Tuberculosis Disease. Treatment of Tuberculosis. Decision to Treat Initiation of Therapy 1
 Treatment of Tuberculosis Some Highlights of Most Recent Update Treatment of Tuberculosis Disease Germaine Jacquette, MD Physician Specialist NJMS Global Tuberculosis Institute September 15, 2010 The provider
Treatment of Tuberculosis Some Highlights of Most Recent Update Treatment of Tuberculosis Disease Germaine Jacquette, MD Physician Specialist NJMS Global Tuberculosis Institute September 15, 2010 The provider
Pediatric Tuberculosis: The Essentials October 8, 2014
 Pediatric Tuberculosis: The Essentials Ann M Loeffler, MD Randall Children s Hospital at Legacy Emanuel Portland, Oregon Curry International TB Center Disclosures Nothing to disclose Learning Objectives
Pediatric Tuberculosis: The Essentials Ann M Loeffler, MD Randall Children s Hospital at Legacy Emanuel Portland, Oregon Curry International TB Center Disclosures Nothing to disclose Learning Objectives
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
TB Nurse Case Management San Antonio, TX. TB Medications and Adverse Effects
 TB Nurse Case Management San Antonio, TX April 1 3, 2014 TB Medications and Adverse Effects Debbie Onofre RN, BSN Nurse Consultant/ Nurse Educator Heartland National TB Center April 1, 2014 Debbie Onofre,
TB Nurse Case Management San Antonio, TX April 1 3, 2014 TB Medications and Adverse Effects Debbie Onofre RN, BSN Nurse Consultant/ Nurse Educator Heartland National TB Center April 1, 2014 Debbie Onofre,
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 TB and Diabetes Barbara Seaworth, MD July 19, 2012 Barbara Seaworth, MD, FIDSA, FACP has the following disclosures to make: Has an advisory
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 TB and Diabetes Barbara Seaworth, MD July 19, 2012 Barbara Seaworth, MD, FIDSA, FACP has the following disclosures to make: Has an advisory
Tips and Tricks for Diagnosing and Treating Tuberculosis
 Tips and Tricks for Diagnosing and Treating Tuberculosis Bob Belknap M.D. Director, Denver Metro TB Program December 6, 2017 DenverPublicHealth.org @DenverPublicHealth @DenPublicHealth Disclosures No conflicts
Tips and Tricks for Diagnosing and Treating Tuberculosis Bob Belknap M.D. Director, Denver Metro TB Program December 6, 2017 DenverPublicHealth.org @DenverPublicHealth @DenPublicHealth Disclosures No conflicts
TB is Global. Latent TB Infection (LTBI) Sharing the Care: Working Together. September 24, 2014
 Sharing the Care: Working Together. September 24, 2014") Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Laboratory Diagnosis for MDR TB
 Laboratory Diagnosis for MDR TB Neha Shah MD MPH Centers for Disease Control and Prevention Division of Tuberculosis Elimination California Department of Public Health Guam March 07 Objectives Describe
Laboratory Diagnosis for MDR TB Neha Shah MD MPH Centers for Disease Control and Prevention Division of Tuberculosis Elimination California Department of Public Health Guam March 07 Objectives Describe
TB Clinical Guidelines: Revision Highlights March 2014
 TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
PROBLEMS IN TX CASE STUDY. JB is a 42 yo BM who was admitted to
 Why TB Drugs Fail Part 2 Why TB Drugs Fail OR How We Fail TB Drugs (and Tb Patients) 1 PROBLEMS IN TX FAILURE TO RESPOND TB MENINGITIS RENAL FAILURE HEPATITIS CAN T SWALLOW PILLS GI INTOLERANCE ADVERSE
Why TB Drugs Fail Part 2 Why TB Drugs Fail OR How We Fail TB Drugs (and Tb Patients) 1 PROBLEMS IN TX FAILURE TO RESPOND TB MENINGITIS RENAL FAILURE HEPATITIS CAN T SWALLOW PILLS GI INTOLERANCE ADVERSE
MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS
 MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS A Bekker FIDSSA Conference, 2017 OUTLINE Case Perinatal TB Approach to the TB-exposed newborn MOM AND BABY S Born by NVD at peripheral hospital
MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS A Bekker FIDSSA Conference, 2017 OUTLINE Case Perinatal TB Approach to the TB-exposed newborn MOM AND BABY S Born by NVD at peripheral hospital
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
TB & HIV CO-INFECTION IN CHILDREN. Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012
 TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
Therapeutic Drug Monitoring for Improving TB Treatment Outcomes: A Concept for a Randomized Clinical Trial before Clinical Implementation
 Therapeutic Drug Monitoring for Improving TB Treatment Outcomes: A Concept for a Randomized Clinical Trial before Clinical Implementation Randall Reves, MD, MSc TB Consultant Professor of Medicine and
Therapeutic Drug Monitoring for Improving TB Treatment Outcomes: A Concept for a Randomized Clinical Trial before Clinical Implementation Randall Reves, MD, MSc TB Consultant Professor of Medicine and
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
TB Nurse Case Management
 TB Nurse Case Management San Antonio, Texas March 2-4, 2011 TB Medications and Adverse Effects Debbie Onofre, RN, BSN March 3, 2011 Debbie Onofre, RN, BSN has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas March 2-4, 2011 TB Medications and Adverse Effects Debbie Onofre, RN, BSN March 3, 2011 Debbie Onofre, RN, BSN has the following disclosures to make: No conflict
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011
 ART Treatment Guideline Training 31 st January to 4 th February, 2011") TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
Focus on LTBI October 17, 2017
 APPROACHES TO LTBI TREATMENT Chris Keh, MD Director, TB Prevention and Control Program, SFDPH HS Assistant Clinical Professor, Infectious Diseases, UCSF Curry International TB Center, LTBI, October 17,
APPROACHES TO LTBI TREATMENT Chris Keh, MD Director, TB Prevention and Control Program, SFDPH HS Assistant Clinical Professor, Infectious Diseases, UCSF Curry International TB Center, LTBI, October 17,
TB BASICS: PRIORITIES AND CLASSIFICATIONS
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.