What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital
|
|
|
- Joan Singleton
- 5 years ago
- Views:
Transcription



1 What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital
2 Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning

3 Nolan CJ et al. Lancet 2011;378:
4 Tahrani A et al. Lancet 2011;378: Therapeutic targets

5 Nolan CJ et al. Lancet 2011;378:
6
7 ADA and EASD algorithm Reinforce lifestyle interventions at every visit and check HbA 1C every 3 months until HbA 1C is <7% and then at least every 6 months. The interventions should be changed if HbA 1C is 7%. Tier 1: Well validated core therapies At diagnosis: Lifestyle + metformin Lifestyle and metformin + basal insulin Lifestyle and metformin + sulphonylurea a Lifestyle and metformin + intensive insulin Step 1 Step 2 Step 3 Tier 2: Less well validated studies Lifestyle and metformin + pioglitazone No hypoglycaemia Oedema/CHF Bone loss Lifestyle and metformin + pioglitazone + sulphonylurea a Lifestyle and metformin + GLP-1 agonist b No hypoglycaemia Weight loss Nausea/vomiting Lifestyle and metformin + basal insulin a Sulfonylureas other than glybenclamide (glyburide) or chlorpropamide. b Insufficient clinical use to be confident regarding safety. Nathan et al. Diabetes Care 2008;31:1 11
8
9

10 There is no place for pioglitazone in the management of type 2 diabetes
11 Pioglitazone pros and cons Bladder cancer: RR Avoid if active or PH of bladder ca, or if have uninvestigated haematuria Consider risk factors: smoking, age Osteoporosis PROACTIVE study: 16% RR in all-cause mortality, non-fatal MI and stroke MHRA Safety Update August 2011
12 Pioglitazone case study PH, 78 M Jan 11: wt 90.1 kg, HbA1c 72 mmol/mol (8.7%) Glargine 20 u am, 50 u pm Metformin 850 mg tds Sitagliptin 100 mg od Added pioglitazone 30 mg od Glargine dose reduced to 16 u am, 44 u pm July 11: wt 98.1 kg, HbA1c 57.5 mmol/mol (7.4%) Lows during the night
 Beta-cell mass* Brain Energy intake* Liver Hepatic glucose output GI tract Decreased motility *in animal")
13 Physiological effects of GLP1 Pancreas Insulin secretion (glucose-dependent) and beta-cell sensitivity Insulin synthesis Glucagon secretion (glucose-dependent) Beta-cell mass* Brain Energy intake* Liver Hepatic glucose output GI tract Decreased motility *in animal studies

14 The family of incretin-based therapies Human GLP-1 analogues, e.g. liraglutide Exendin-based therapies, e.g. exenatide GLP-1 receptor agonists DPP-4 inhibitors, e.g. sitagliptin, vildagliptin Incretin-based therapies
15 DPP IV inhibitors Comparable improvement in glycaemic control to SUs but with much less hypoglycaemia and weight neutral Useful in renal failure Saxagliptin: renal dose 2.5 mg od Linagliptin: biliary excretion, no dose adjustment needed CV outcome trials in progress
16 Exenatide national audit 10 5 HbA1c change (%) Weight change (Kg) months after exenatide start in 1959 patients
17 Exenatide in real clinical use - conclusion 60% of patients achieve the ideal of both weight loss and fall in HbA1c However many patients experience a predominant response to only one of weight or HbA1c with more minimal response to the other Hence only 28% achieve the NICE guideline The NICE guideline should change to acknowledge that significant weight loss or significant HbA1c response may represent a beneficial response
18 Composite end points that matter HbA 1c <7.0% + No weight gain + No hypoglycaemia
 40 35 30 25 20 15 10 39% 32%* 15%** 8%**, 6%**, 24%* 8%**, 35%* 14%**, 5 0 Liraglutide 1.8 mg (n=1363) Liraglutide 1.")
19 Composite endpoint: HbA 1c <7.0%, no weight gain and no hypos LEAD studies No head-to-head comparison in the LEAD programme between liraglutide 1.2mg and glargine or exenatide 46% Lira vs Sita Patients reaching target (%) % 32%* 15%** 8%**, 6%**, 24%* 8%**, 35%* 14%**, 5 0 Liraglutide 1.8 mg (n=1363) Liraglutide 1.2 mg (n=896) SU (n=490) TZD (n=231) Glargine (n=232) Exenatide Placebo (n=231) (n=524) Liraglutide 1.8 mg (n=214) Liraglutide 1.2 mg (n=210) Sitagliptin (n=210) Liraglutide 1.8 mg is superior (*p<0.01; ** p<0.0001) Liraglutide 1.2 mg is superior ( p<0.0001) Percentages are from logistic regression model adjusted for trial, previous treatment and with baseline HbA 1c and weight as covariates Zinman B et al. Diabetologia 2009; 52(Suppl 1): S292 (A743); Prately RE et al. Lancet 2010; 375:

20 Comparative odds ratio for achieving the composite endpoint HbA 1c <7.0%, no weight gain, no minor or major hypoglycaemia Comparison Odds ratio favouring liraglutide Liraglutide 1.8 mg vs TZD 10.3 *** Liraglutide 1.2 mg vs. TZD 7.5 *** Liraglutide 1.8 mg vs SU 7.3 *** Liraglutide 1.2 mg vs. SU 5.3 *** Liraglutide 1.8 mg vs glargine 3.7 *** Liraglutide 1.8 mg vs sitagliptin 3.4 *** Liraglutide 1.2 mg vs sitagliptin 2.6 *** Liraglutide 1.8 mg vs exenatide 2.0 ** **p<0.005; ***p< in favour of liraglutide 1.8 mg Based on meta-analysis of LEAD 1 6. Adjusted for previous treatment, baseline values and randomisation. LOCF, ITT Zinman B et al. Diabetologia 2009; 52(Suppl 1): S292 (A743); Prately RE et al. Lancet 2010; 375:

21 DeYoung MB et al. Diab Tech Ther 2011;13: Exenatide ER

22 Exenatide ER (Bydureon)
23 Microsphere deposits DeYoung MB et al. Diab Tech Ther 2011;13:
24 Exenatide ER vs Glargine DURATION 3 Lancet 2010;375:
25 Exenatide ER vs glargine: targets DURATION 3 Lancet 2010;375:
26 Exenatide ER vs BD DURATION 5 J Clin End Met 2011;96:
27 Exenatide ER vs BD: targets DURATION 5 J Clin End Met 2011;96:
28 Long vs short-acting GLP 1 agonists Advantages: Better glycaemic control Better tolerated?better adherence Disadvantages:?Less weight loss Slower onset of action More difficult to stop
29 GLP1 agonists and insulin Buse JB et al. Ann Intern Med 2011;154:103-12
30 GLP1 and insulin case study PC, 52 M Jan 10: wt kg HbA1c 86 mmol/mol (10.0%) On 256 units insulin/d Started liraglutide: titrated to 1.8 mg od Treatment costs injectable therapy 5.84/day April 11: wt kg HbA1c 62 mmol/mol (7.8%) On 68 units insulin/d Treatment costs injectable therapy 5.69/day

31 NPH/isophane insulin should be first choice for initiation in type 2 diabetes
32 Waugh N et al. HTA assessment 2010;14:No 6 Glycaemic control
33 ACCORD intensive BG lowering The ACCORD study group. N Eng J Med 2008;358:
 3.0 2.5 2.0 1.5 1.0 1.2% 2.8% 0.")

34 Hypoglycaemia and mortality: The ACCORD experience 3.5 Overall mortality (%) % 2.8% Never experienced severe hypoglycaemia Experienced severe hypoglycaemia Bonds DE et al. BMJ 2010; 340: b4909
35 Hypoglycaemia and mortality: The ADVANCE experience Zoungas S et al. N Engl J Med 2010; 363:



36 Pathophysiological cardiovascular consequences of hypoglycaemia CRP, C reactive protein; IL 6, interleukin 6; VEGF, vascular endothelial growth factor Desouza et al. Diabetes Care 2010;33:

37 Hypoglycaemia in clinical practice 3% of people with type 2 diabetes experienced severe hypoglycaemia over a 12 month period People of all ages who experienced severe hypoglycaemia had a 79% increased risk of suffering an acute cardiovascular event Hypoglycaemia directly preceded an acute cardiovascular event in over 25% of people People who experienced severe hypoglycaemia incurred a 2 fold greater health related expenditure Johnston et al. Diabetes care March 2011
38 Nocturnal hypoglycaemia Almost 50% of all episodes of severe hypoglycaemia occur at night during sleep 1 Nocturnal hypoglycaemia is a major concern to patients and family, and is a particular barrier to insulin dose titration 2,3 Nocturnal hypoglycaemia has a major detrimental effect on mood and well being the following day 1 Nocturnal hypoglycaemia is linked to dead in bed syndrome 4 Recurrent nocturnal hypoglycaemia is linked to development of hypoglycaemia unawareness 5 Avoiding nocturnal hypoglycaemia is a key clinical imperative 1. Allen KV. Endocr Pract 2003; 9: Frier BM. Diabetes Metab Res Rev 2008; 24: Yale JF. Diabetes Res Clin Pract 2004; 65 Suppl 1: S Tanenburg RJ et al. Endocr Pract 2010; 16: Veneman T et al. Diabetes 1993; 42:
39 Consequences of hypoglycaemia for driving in the UK Patients managed by insulin, must inform the DVLA of their treatment and also if the following apply: You suffer more than one episode of disabling hypoglycaemia (low blood sugar) within 12 months, or if you or your carer feels you are at high risk of developing disabling hypoglycaemia You develop impaired awareness of hypoglycaemia (difficulty in recognising the warning symptoms of low blood sugar) You suffer disabling hypoglycaemia while driving DVLA guidance. Available at:
40 Higher rate of severe hypoglycaemia with intensive glycaemic control* UKPDS 1 ADVANCE 2 ACCORD 3 VADT p<0.001 vs. conventional HR 1.86 ( ) p<0.001 p<0.001 p=0.001 Annualised rate of severe hypoglycaemia (%) Conv Gly Ins Std Int Std Int Std Int HbA 1C = 7.9% 7.1% 7.2% 7.3% 6.5% 7.5% 6.4% 8.4% 6.9% *Intensive glycaemic control was defined differently in these trials. Hypoglycaemia requiring any assistance in glucose lowering trials. Conv, conventional therapy; Gly, glibenclamide; HbA 1c, glycated haemoglobin; HR, hazard ratio; Ins, insulin; Int, intensive therapy; Std, standard therapy 1 UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998;352:837 53; 2 Patel et al; ADVANCE Collaborative Group [ADVANCE]. N Engl J Med 2008;358: ; 3 Gerstein et al; Action to Control Cardiovascular Risk in Diabetes Study Group [ACCORD]. N Engl J Med 2008;358: ; 4 Duckworth et al. N Engl J Med 2009;360:129 39
41 Myth 1: hypoglycaemia does not occur in T2DM Severe hypoglycaemia 1 Mild hypoglycaemia 1 Proportion reporting at least one hypoglycaemic episode SU <2 yr >5 yr <5 yr >15 yr SU <2 yr >5 yr <5 yr >15 yr T1D SU, sulphonylurea T2D T1D 55% of severe and 43% of all hypoglycaemic episodes occur during sleep in T1D 2 36% of severe episodes that occurred while awake had no warning signs 2 T2D T1D 1 UK Hypoglycaemia Study Group Diabetologia 2007;50:1140 7; 2 DCCT. Am J Med 1991;90:450 9
42 Myth 2: hypoglycaemia does not have major consequences in T2DM Similar clinical (CV and neurological) consequences to T1D However: T2D population is older Symptoms can be different Hypoglycaemia unawareness More comorbidities high frequency of CVD osteoporosis higher fracture risk longer hospital stay duration Event rate increases with disease duration progressive disease CV, cardiovascular; CVD, CV disease Chelliah et al. Drugs Aging 2004;21:511 30; Lebovitz Diab Rev 1999;7:139 53
43 Hypoglycaemic event rates are reduced with basal analogue insulins vs. NPH in T2DM 1.0 p<0.001 p<0.001 p<0.05 p<0.05 p=0.018 p= Insulin detemir NPH Insulin glargine Relative risk hour Nocturnal Hermansen weeks, n= hour* Nocturnal Philis Tsimikas weeks, n= hour Nocturnal Home 2010 Meta analysis, n=2711 * PM dose Threshold of <3.1 mmol/l for confirmed hypoglycaemia Threshold of <3.9 mmol/l for confirmed hypoglycaemia Home et al. Diabetes Obes Metab 2010;12;772 9; Hermansen et al. Diabetes Care 2006;29: ; Philis Tsimikas et al. Clin Ther 2006;28:
44 Hypoglycaemia and basal analogues Waugh N et al. HTA assessment 2010;14:No 6
45 Tahrani A et al. Lancet 2011;378:
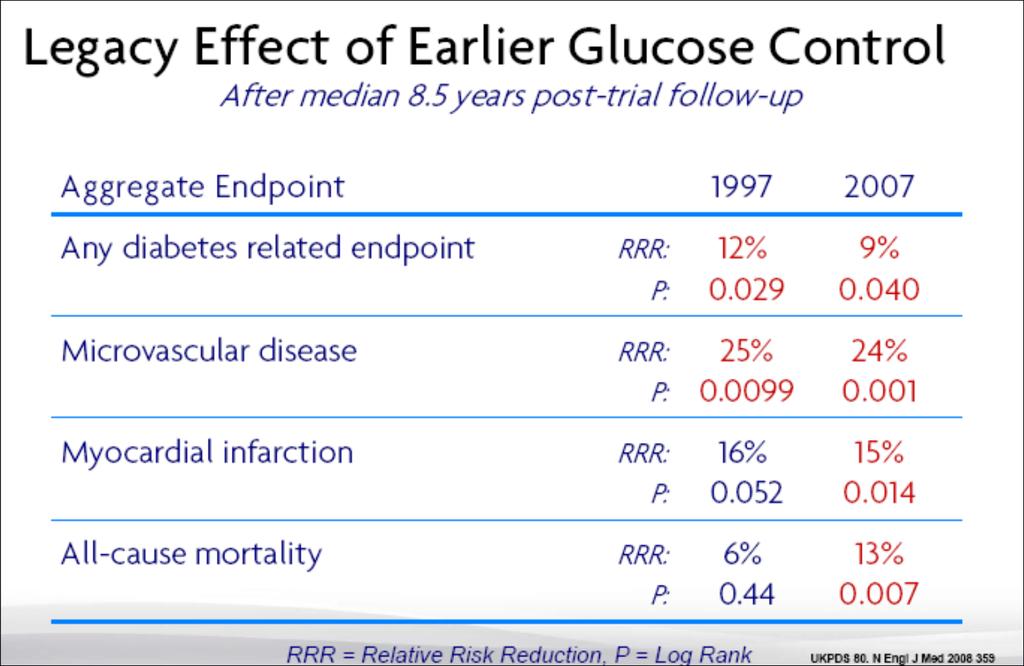
46 Bullet Points for New Clinical Solutions There is a legacy effect of good glycaemic control so NICE targets are essential and combination drug therapy is inevitable The ideal drug combination therapy for glucose control combines low risk of hypoglycaemia, weight reduction and CV safety Newer agents, particularly those targeting the GLP1 receptor show potential but CV safety data is awaited
47
48
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Management of Type 2 Diabetes
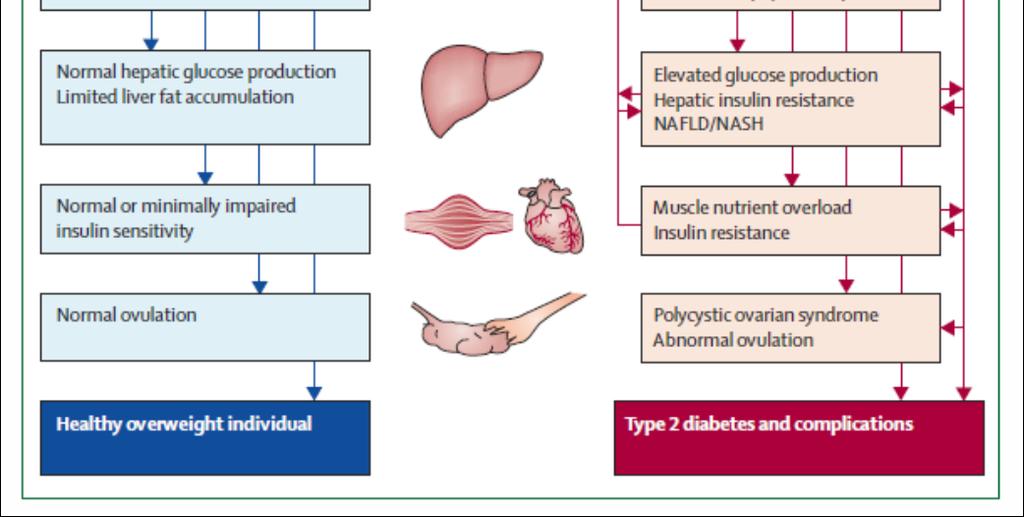
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
Hypoglycemic Therapy :What to start & stop
 The Cork Diabetes & Endocrinology Clinic CDEC.IE Bon Secours Hospital, Cork Hypoglycemic Therapy :What to start & stop Maeve C. Durkan MBBS.FACP, Mmed.Ed Consultant in Diabetes, Endocrinology & Metabolism
The Cork Diabetes & Endocrinology Clinic CDEC.IE Bon Secours Hospital, Cork Hypoglycemic Therapy :What to start & stop Maeve C. Durkan MBBS.FACP, Mmed.Ed Consultant in Diabetes, Endocrinology & Metabolism
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
MANAGEMENT OF TYPE 2 DIABETES
 MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
Newer and Expensive treatment of diabetes. Endocrinology Visiting Associate Professor Institute of Medicine TUTH
 Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
Dr Tahseen A. Chowdhury Royal London Hospital. New Guidelines in Diabetes: NICE or Nasty?
 Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Treatment Options for Diabetes: An Update
 Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Diabetes new challenges, new agents, new order
 Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
T2DM is a global epidemic with
 : a new option for the management of type 2 diabetes Marc Evans MRCP, MD, Consultant Diabetologist, Llandough Hospital, Cardiff Incretin-based therapies for the treatment of diabetes mellitus (T2DM) present
: a new option for the management of type 2 diabetes Marc Evans MRCP, MD, Consultant Diabetologist, Llandough Hospital, Cardiff Incretin-based therapies for the treatment of diabetes mellitus (T2DM) present
Glycemic control a matter of life and death
 Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Glucose Control drug treatments
 Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
COPYRIGHT. Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely?
 Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
Scottish Medicines Consortium
 Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
Alia Gilani Health Inequalities Pharmacist
 Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
GLP-1RA and insulin: friends or foes?
 Tresiba Expert Panel Meeting 28/06/2014 GLP-1RA and insulin: friends or foes? Matteo Monami Careggi Teaching Hospital. Florence. Italy Dr Monami has received consultancy and/or speaking fees from: Merck
Tresiba Expert Panel Meeting 28/06/2014 GLP-1RA and insulin: friends or foes? Matteo Monami Careggi Teaching Hospital. Florence. Italy Dr Monami has received consultancy and/or speaking fees from: Merck
Real World Evidence: From Efficacy to Effectiveness
 Real World Evidence: From Efficacy to Effectiveness Professor Kamlesh Khunti University of Leicester, UK Leicester Diabetes Centre at University Hospitals of Leicester NHS Trust, 2015. Not to be reproduced
Real World Evidence: From Efficacy to Effectiveness Professor Kamlesh Khunti University of Leicester, UK Leicester Diabetes Centre at University Hospitals of Leicester NHS Trust, 2015. Not to be reproduced
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
YOU HAVE DIABETES. Angie O Connor Community Diabetes Nurse Specialist 25th September 2013
 YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
Dept of Diabetes Main Desk
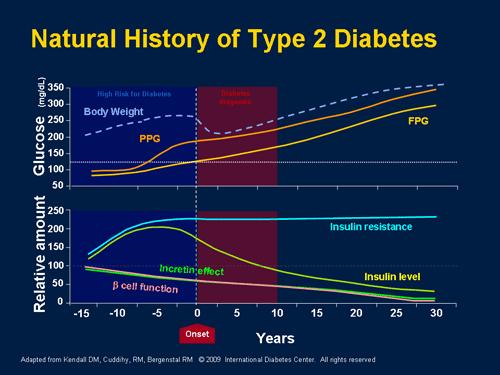
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Update on Cardiovascular Outcome Trials in Diabetes. Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013
 Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Glucose Control and Prevention of Cardiovascular Disease
 Glucose Control and Prevention of Cardiovascular Disease Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Diabetes Update+, March
Glucose Control and Prevention of Cardiovascular Disease Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Diabetes Update+, March
New Treatments for Type 2 diabetes. Nandini Seevaratnam April 2016 Rushcliffe Patient Forum
 New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and Diabetes Atlas -sixth Edition: IDF 2013
, 2013 and Diabetes Atlas -sixth Edition: IDF 2013") IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
NMQF. Washington DC 2014
 NMQF Washington DC 2014 ACE/AACE Treatment Algorithm Jaime A. Davidson, MD, FACP, MACE Prof. of Medicine Division of Endocrinology, Diabetes and Metabolism President WorldWIDE Diabetes Advisor to the AACE
NMQF Washington DC 2014 ACE/AACE Treatment Algorithm Jaime A. Davidson, MD, FACP, MACE Prof. of Medicine Division of Endocrinology, Diabetes and Metabolism President WorldWIDE Diabetes Advisor to the AACE
Metabolic Karma. - Essential Solution in Type2 DM - Eun Gyoung Hong, M.D., Ph.D
 2014 ICDM Breakfast Symposium. Oct 18, 2014 Grand Hilton, Seoul Metabolic Karma - Essential Solution in Type2 DM - Eun Gyoung Hong, M.D., Ph.D Department of Endocrinology and Metabolism, Hallym University
2014 ICDM Breakfast Symposium. Oct 18, 2014 Grand Hilton, Seoul Metabolic Karma - Essential Solution in Type2 DM - Eun Gyoung Hong, M.D., Ph.D Department of Endocrinology and Metabolism, Hallym University
Management of Diabetes Mellitus: A Primary Care Perspective
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
UKPDS: Over Time, Need for Exogenous Insulin Increases
 UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
DPP-4/SGLT2 inhibitor combined therapy for type 2 diabetes
 THERAPY REVIEW DPP-4/SGLT2 inhibitor combined therapy for type 2 diabetes STEVE CHAPLIN SPL DPP-4 inhibitors and SGLT2 inhibitors lower blood glucose by complementary mechanisms of action, and two fixeddose
THERAPY REVIEW DPP-4/SGLT2 inhibitor combined therapy for type 2 diabetes STEVE CHAPLIN SPL DPP-4 inhibitors and SGLT2 inhibitors lower blood glucose by complementary mechanisms of action, and two fixeddose
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Role of incretins in the treatment of type 2 diabetes
 Role of incretins in the treatment of type 2 diabetes Jens Juul Holst Department of Medical Physiology Panum Institute University of Copenhagen Denmark Diabetes & Obesity Spanish Society of Internal Medicine
Role of incretins in the treatment of type 2 diabetes Jens Juul Holst Department of Medical Physiology Panum Institute University of Copenhagen Denmark Diabetes & Obesity Spanish Society of Internal Medicine
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Management of Diabetes Mellitus: A Primary Care Perspective. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Sulfoniluree e glinidi: pro e contro
 Sulfoniluree e glinidi: pro e contro Giorgio Sesti Università Magna Graecia di Catanzaro ITALY T2DM anti-hyperglycaemic therapy: general recommendations Diabetes Care 35:1364-1379, 2012; Diabetologia 55:1577-1596,
Sulfoniluree e glinidi: pro e contro Giorgio Sesti Università Magna Graecia di Catanzaro ITALY T2DM anti-hyperglycaemic therapy: general recommendations Diabetes Care 35:1364-1379, 2012; Diabetologia 55:1577-1596,
Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy
 Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy Melpomeni Peppa Assistant Professor of Endocrinology 2 nd Dept of Internal Medicine-Propaedeutic, Athens
Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy Melpomeni Peppa Assistant Professor of Endocrinology 2 nd Dept of Internal Medicine-Propaedeutic, Athens
Should Psychiatrists be diagnosing (and treating) metabolic syndrome
 metabolic syndrome") Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Multiple Small Feedings of the Mind: Diabetes. Sonja K Fredrickson, MD, BC-ADM March 7, 2014
 Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
Hypoglyceamia and Exercise
 Hypoglyceamia and Exercise Noreen Barker Diabetes Specialist Nurse May 2016 Hypoglyceamia What is a hypo? Why are we concerned? Signs and symptoms Treatments Causes Hypo unawareness Managing diabetes and
Hypoglyceamia and Exercise Noreen Barker Diabetes Specialist Nurse May 2016 Hypoglyceamia What is a hypo? Why are we concerned? Signs and symptoms Treatments Causes Hypo unawareness Managing diabetes and
Efficacy and Safety of Sitagliptin in Various Clinical Settings of T2DM
 Efficacy and Safety of Sitagliptin in arious Clinical Settings of T2DM Young Min Cho, MD, PhD Division of Endocrinology and Metabolism Department of Internal Medicine Seoul National University College
Efficacy and Safety of Sitagliptin in arious Clinical Settings of T2DM Young Min Cho, MD, PhD Division of Endocrinology and Metabolism Department of Internal Medicine Seoul National University College
Individualising Insulin Regimens: Premixed or basal plus/bolus?
 Individualising Insulin Regimens: Premixed or basal plus/bolus? Dr. Ted Wu Director, Diabetes Centre, Hospital Sydney, Australia Turkey, April 2015 Centre of Health Professional Education Optimising insulin
Individualising Insulin Regimens: Premixed or basal plus/bolus? Dr. Ted Wu Director, Diabetes Centre, Hospital Sydney, Australia Turkey, April 2015 Centre of Health Professional Education Optimising insulin
Liraglutide (Victoza) in combination with basal insulin for type 2 diabetes
 in combination with basal insulin for type 2 diabetes") Liraglutide (Victoza) in combination with basal insulin for type 2 diabetes May 2011 This technology summary is based on information available at the time of research and a limited literature search. It
Liraglutide (Victoza) in combination with basal insulin for type 2 diabetes May 2011 This technology summary is based on information available at the time of research and a limited literature search. It
Ipoglicemia: trattamento e strategie di prevenzione
 Ipoglicemia: trattamento e strategie di prevenzione Antonio Ceriello Insititut d'investigacions Biomèdiques August Pi i Sunyer (IDIBAPS) Barcelona Spain Frequency of Hypoglycemia Increases as HbA1c Declines
Ipoglicemia: trattamento e strategie di prevenzione Antonio Ceriello Insititut d'investigacions Biomèdiques August Pi i Sunyer (IDIBAPS) Barcelona Spain Frequency of Hypoglycemia Increases as HbA1c Declines
exenatide 2mg powder and solvent for prolonged-release suspension for injection (Bydureon ) SMC No. (748/11) Eli Lilly and Company Limited
 SMC No. (748/11) Eli Lilly and Company Limited") exenatide 2mg powder and solvent for prolonged-release suspension for injection (Bydureon ) SMC No. (748/11) Eli Lilly and Company Limited 09 December 2011 The Scottish Medicines Consortium (SMC) has completed
exenatide 2mg powder and solvent for prolonged-release suspension for injection (Bydureon ) SMC No. (748/11) Eli Lilly and Company Limited 09 December 2011 The Scottish Medicines Consortium (SMC) has completed
T2 Diabetes in Sep-16. Stephen Leow Disclosures. Why do we treat diabetes? Agenda. Targets
 Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Single Technology Appraisal. Canagliflozin in combination therapy for treating type 2 diabetes
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
sitagliptin, 25mg, 50mg and 100mg film-coated tablets (Januvia ) SMC No. (1083/15) Merck Sharp and Dohme UK Ltd
 SMC No. (1083/15) Merck Sharp and Dohme UK Ltd") sitagliptin, 25mg, 50mg and 100mg film-coated tablets (Januvia ) SMC No. (1083/15) Merck Sharp and Dohme UK Ltd 07 August 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the
sitagliptin, 25mg, 50mg and 100mg film-coated tablets (Januvia ) SMC No. (1083/15) Merck Sharp and Dohme UK Ltd 07 August 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Management of Diabetes
 Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Current principles of diabetes management
 Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
STEP 3: Add or Substitute with one of
 Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes
 Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Mr Rab Burtun. Dr David Kim. 8:30-10:30 WS #2: Diabetes Basic 11:00-13:00 WS #9: Diabetes Basic (Repeated)
") Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
An Update on Guidelines and Evidence of the Treatment of Type 2 Diabetes Mellitus
 Nevada Academy of Family Physicians 29 th Annual Summer CME Meeting August 3 5, 2018 An Update on Guidelines and Evidence of the Treatment of Type 2 Diabetes Mellitus Presented by: James D. Honeycutt,
Nevada Academy of Family Physicians 29 th Annual Summer CME Meeting August 3 5, 2018 An Update on Guidelines and Evidence of the Treatment of Type 2 Diabetes Mellitus Presented by: James D. Honeycutt,
Beyond A1C. Non-glycemic Effects of GLP-1 Receptor Agonists. Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows
 Beyond A1C Non-glycemic Effects of GLP-1 Receptor Agonists Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows Disclosures No conflicts of interest. Learning Objectives 1. Understand the physiological
Beyond A1C Non-glycemic Effects of GLP-1 Receptor Agonists Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows Disclosures No conflicts of interest. Learning Objectives 1. Understand the physiological
insulin degludec/liraglutide 100 units/ml / 3.6mg/mL solution for injection pre-filled pen (Xultophy ) SMC No. (1088/15) Novo Nordisk A/S
 SMC No. (1088/15) Novo Nordisk A/S") insulin degludec/liraglutide 100 units/ml / 3.6mg/mL solution for injection pre-filled pen (Xultophy ) SMC No. (1088/15) Novo Nordisk A/S 4 September 2015 The Scottish Medicines Consortium (SMC) has completed
insulin degludec/liraglutide 100 units/ml / 3.6mg/mL solution for injection pre-filled pen (Xultophy ) SMC No. (1088/15) Novo Nordisk A/S 4 September 2015 The Scottish Medicines Consortium (SMC) has completed
CONTROLLO GLICEMICO E RISCHIO CARDIOVASCOLARE. AGOSTINO CONSOLI DMSI - Università d Annunzio CHIETI ITALY. sul Paziente ad alto rischio CV*
 CONTROLLO GLICEMICO E RISCHIO CARDIOVASCOLARE AGOSTINO CONSOLI DMSI - Università d Annunzio CHIETI ITALY sul Paziente ad alto rischio CV* Does reducing hyperglycemia protect against cardiovascular risk?
CONTROLLO GLICEMICO E RISCHIO CARDIOVASCOLARE AGOSTINO CONSOLI DMSI - Università d Annunzio CHIETI ITALY sul Paziente ad alto rischio CV* Does reducing hyperglycemia protect against cardiovascular risk?
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetic Management of the Cardiac Patient
 Diabetic Management of the Cardiac Patient Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Disclosures Grants/Research Support:
Diabetic Management of the Cardiac Patient Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Disclosures Grants/Research Support:
Francesca Porcellati
 XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
The Alphabet Soup of Diabetes. Egils Bogdanovics M.D. Hungerford Diabetes Center
 The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
No Increased Cardiovascular Risk for Lixisenatide in ELIXA
 ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017
 TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
Drug Therapy for Diabetes Mellitus. Adj A/Prof Daniel Chew Dept of Endocrinology 8 th July 2017
 Drug Therapy for Diabetes Mellitus Adj A/Prof Daniel Chew Dept of Endocrinology 8 th July 2017 Diabetes Subtypes Optimal Treatment Ominous Octet DeFronzo. DIABETES, VOL. 58, APRIL 2009 Schematic Overview
Drug Therapy for Diabetes Mellitus Adj A/Prof Daniel Chew Dept of Endocrinology 8 th July 2017 Diabetes Subtypes Optimal Treatment Ominous Octet DeFronzo. DIABETES, VOL. 58, APRIL 2009 Schematic Overview
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
Optimal glucose control. DM Treatment. Glucose Control one out of many. Many guidelines: Confusing. Theorectically easy
 DM Treatment How to Achieve Optimal Glycaemic Control The Tung Wah Eastern Hospital Experience of DM Share Care Experience Optimal glucose control Theorectically easy More challenging in the real world
DM Treatment How to Achieve Optimal Glycaemic Control The Tung Wah Eastern Hospital Experience of DM Share Care Experience Optimal glucose control Theorectically easy More challenging in the real world
효과적인경구혈당강하제의조합은? 대한당뇨병학회제 17 차연수강좌 ( ) 가천의대길병원내분비대사내과
 가천의대길병원내분비대사내과") 효과적인경구혈당강하제의조합은? 대한당뇨병학회제 17 차연수강좌 (2011.10.30.) 가천의대길병원내분비대사내과 박이병 내용 배경 경구혈당강하제의병합이왜필요한가? (WHY?) 경구혈당강하제의병합은언제시작하나? (WHEN?) 경구혈당강하제의병합은어떻게하는것이좋은가?(HOW) 맺음말 배경 : drugs for treating diabetes In 1995 :
효과적인경구혈당강하제의조합은? 대한당뇨병학회제 17 차연수강좌 (2011.10.30.) 가천의대길병원내분비대사내과 박이병 내용 배경 경구혈당강하제의병합이왜필요한가? (WHY?) 경구혈당강하제의병합은언제시작하나? (WHEN?) 경구혈당강하제의병합은어떻게하는것이좋은가?(HOW) 맺음말 배경 : drugs for treating diabetes In 1995 :
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
How can we improve outcomes in Type 2 diabetes?
 How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
New Drug Evaluation: Insulin degludec, subcutaneous injection
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
The first stop for professional medicines advice
 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1 receptor analogues The first stop for professional medicines advice 1 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1
London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1 receptor analogues The first stop for professional medicines advice 1 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville
 Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus. Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre
 Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Clinical Overview of Combination Therapy with Sitagliptin and Metformin
 Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
There have been important changes in diabetes care which may not be covered in undergraduate textbooks.
 Diabetes Clinical update There have been important changes in diabetes care which may not be covered in undergraduate textbooks. Changes in the diagnosis of diabetes a) HbA1C Since 2011, World Health Organisation
Diabetes Clinical update There have been important changes in diabetes care which may not be covered in undergraduate textbooks. Changes in the diagnosis of diabetes a) HbA1C Since 2011, World Health Organisation
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies. Module D
 Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Noninsulin Treatment of Diabetes: What the PCP Needs to Know
 Non Insulin Treatment of Type 2 Diabetes: What the PCP Needs to Know Martin J. Abrahamson, MD Senior Vice President for Medical Affairs Joslin Diabetes Center Associate Professor of Medicine Harvard Medical
Non Insulin Treatment of Type 2 Diabetes: What the PCP Needs to Know Martin J. Abrahamson, MD Senior Vice President for Medical Affairs Joslin Diabetes Center Associate Professor of Medicine Harvard Medical
GLP-1. GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4.
 GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
insulin degludec (Tresiba ) is not recommended for use within NHS Scotland.
 is not recommended for use within NHS Scotland.") insulin degludec (Tresiba ) 100units/mL solution for injection in pre-filled pen or cartridge and 200units/mL solution for injection in pre-filled pen SMC No. (856/13) Novo Nordisk 08 March 2013 The Scottish
insulin degludec (Tresiba ) 100units/mL solution for injection in pre-filled pen or cartridge and 200units/mL solution for injection in pre-filled pen SMC No. (856/13) Novo Nordisk 08 March 2013 The Scottish
TYP 2 DIABETES. Marc Donath
 TYP 2 DIABETES Marc Donath Treatment of Typ 2 Diabetes GLP-1 Anti-IL-1β Insulin sulfonylureas Metformin UCP-1 IL-1β Sport SGLT2i Bariatric surgery Cardiomyocytes Control Glucose Dyntar et al. Diabetes
TYP 2 DIABETES Marc Donath Treatment of Typ 2 Diabetes GLP-1 Anti-IL-1β Insulin sulfonylureas Metformin UCP-1 IL-1β Sport SGLT2i Bariatric surgery Cardiomyocytes Control Glucose Dyntar et al. Diabetes
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Type 2 diabetes: recent advances in diagnosis and management
 DRUG REVIEW n Type 2 diabetes: recent advances in diagnosis and management Sudesna Chatterjee MD, FRCP and Melanie Davies MD, FRCP, FRCGP The expanding array of new type 2 diabetes agents and how to combine
DRUG REVIEW n Type 2 diabetes: recent advances in diagnosis and management Sudesna Chatterjee MD, FRCP and Melanie Davies MD, FRCP, FRCGP The expanding array of new type 2 diabetes agents and how to combine
Safety profile of Liraglutide: Recent Updates. Mohammadreza Rostamzadeh,M.D.
 Safety profile of Liraglutide: Recent Updates Mohammadreza Rostamzadeh,M.D. Pancreatitis: Victoza post-marketing experience: spontaneous reports of pancreatitis For the majority of the cases, there is
Safety profile of Liraglutide: Recent Updates Mohammadreza Rostamzadeh,M.D. Pancreatitis: Victoza post-marketing experience: spontaneous reports of pancreatitis For the majority of the cases, there is
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment