PROBLEMS IN TX CASE STUDY. JB is a 42 yo BM who was admitted to
|
|
|
- Brianne Hall
- 6 years ago
- Views:
Transcription
1 Why TB Drugs Fail Part 2 Why TB Drugs Fail OR How We Fail TB Drugs (and Tb Patients) 1
2 PROBLEMS IN TX FAILURE TO RESPOND TB MENINGITIS RENAL FAILURE HEPATITIS CAN T SWALLOW PILLS GI INTOLERANCE ADVERSE DRUG REACTIONS ALLERGIES DRUG INTERACTIONS CASE STUDY JB is a 42 yo BM who was admitted to hospital following a new onset seizure. He complains of persistent headaches over the past month and a history of 30 lb weight loss and chronic cough. He is diabetic and has a history of alcoholism. He has a negative PPD but an abnormal chest x-ray and AFB positive sputum smears and culture. 2
3 CASE STUDY JB is started on 4-drug TB therapy and referred to his CHD. JB does well and is smear and culture negative at 2 months. EMB and PZA are stopped. However, at 3 months he is again loosing weight, his headaches have returned and he is now smear and culture positive. Question 1 The most likely reason for JB s treatment failure is: 1. Non compliance 2. Resistance 3. Low serum drug levels 4. Inadequate tissue penetration 3
4 Diabetes Reduced immunity Changes in gi emptying/absorption Effects of severe hyperglycemia Altered protein binding TB and TB drugs can make diabetes more difficult to control Some antidiabetic drugs can contribute to hepatitis Alcohol/Drug Abuse Gastritis Effect on metabolism Malnutrition Decreased immunity Increased risk of side effects Hepatitis Peripheral neuropathy Non-compliance 4

5 THICK WALLED CAVITY QUESTION #2 JB had an MRI and his CNS TB has gotten worse. Which drug would NOT be a good choice to cross the BBB in therapeutic quantities? 1. INH 2. RIFAMPIN 4. ETHAMBUTOL 4. PZA 5. STREPTOMYCIN 5
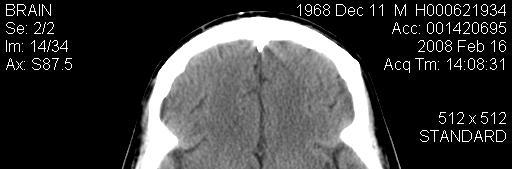
6 TB MENINGITIS Tuberculomabiopsy proven-with surrounding edema 6
7 MIC Versus Concentration DRUG PK [ ] MCG/ML MCG/ML MIC INH RIF PZA EMB STM CAP OFLOX CNS PENETRATION INH % RIF 10-25% PZA % EMB 10-50% STM <10% QUINILONES 10-50% CYCLOSERINE % 7
8 Protein Binding Aminoglycoside ~30% Cipro/Floxin i 20-40% EMB 10-15% INH 10-15% PZA 50% PAS 50-60% RIF 84-90% CNS PENETRATION DRUG EXPECTED SERUM [ ] MCG/ML PB EFFECTIVE SERUM [ ] MCG/ML % CSF normal Effective conc norm % CSF inflamed EFFECTIVE CSF [ ] INFLAMED MIC INH 3-5 (4) 10-15% % 4 100% RIF 8-24 (10) 85% % 1 20% EMB 2-6 (4) 25% % % 2 5 PZA (40) 50% 20 75% % LEVOFLOXACIN 8-12 (10) 30% % 2 45% 4.5 MOXIFLOXACIN 3-5 (4) 40% % 2 CYCLOSERINE (25) 0% 25 90% % 25 8
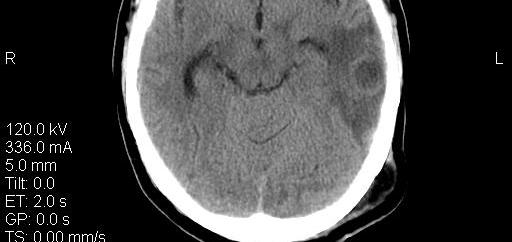
9 Smiling Face Brain CT LOW SERUM DRUG LEVELS WRONG DOSE REDUCED ABSORPTION DIABETES/HIV GI DISEASE/SURGERY MALNUTRITION LAXATIVE ABUSE DRUG-FOOD INTERACTIONS DRUG-DRUG INTERACTIONS INCREASED METABOLISM / EFLUX VOMITING NON-COMPLIANCE 9


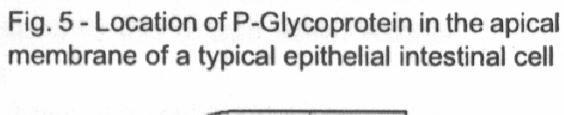
10 INTESTINAL WALL SMALL INTESTINE PAPILLI P-Glycoproteins 10


11 CYP 450 System QUESTION #3 WHICH OF THE FOLLOWING CAN BE TAKEN WITHOUT REGARD TO MEALS? 1. INH 2. RIFAMPIN 3. MOXIFLOXACIN 4. ETHAMBUTOL 11
12 Bioavailability RIF 100%(FASTING) 70% (FED) NFV 20%(FASTING) 80% (FED) Absorption Food/Drug Interactions Most often caused by Iron Calcium Magnesium Aluminum Zinc Fat Low/high ph Protein Most effected INH, EMB, RIF Ofloxacin/ciprofloxacin Indinavir, saquinavir, nelfinavir, lopinavir, ddi, tenofovir 12
13 BEWARE OF FLUIDS DAIRY PRODUCTS Ca FORMS INSOLUABLE COMPLEXES WITH RX FOOD SUPPLEMENTS Protein, Ca and other minerals ORANGE JUICE MG AND CA APPLE JUICE CA AND FE TUBE FEEDINGS STOP FEEDING FOR 2 HOURS BEFORE AND AFTER TB DRUGS 13
14 TAKE ON AN EMPTY STOMACH (1 HR BEFORE OR 2 HRS AFTER A MEAL) INH RIF,RBT EMB PZA QUINOLONES TAKE WITH FOOD ETHIONAMIDE / PAS TO REDUCE GI SIDE EFFECTS CLOFAZAMINE TO MAXIMZE ABSORPTION 14
15 WITHOUT REGARD TO MEALS PZA CYCLOSERINE RIFAPENTINE MOXIFLOXACIN Dusty in Basket 15
16 Resistance Primary mixed resistance Secondary resistance Risk factors Patient non-compliance Improper prescription Inadequate tissue penetration Heavy burden of disease RESISTANCE LOW DRUG LEVELS IN SERUM vs AT SITE OF INFECTION DRUG INTERACTION VOMITING 16
17 RESISTANCE POTENTIAL PROB. OF RESISTANCE NO ACTIVITY MAXIMUM EFFECT INCREASING POTENCY Population Curve 17
18 Question #4 Shortly after his MRI, JB s lab work shows rapidly deteriorating renal function. His CL cr is currently 20 ml/min. Which drug may need to have its dose modified? 1. INH 2. RIF 3. EMB 4. PZA DRUGS NEEDING ADJUSTMENT IN RENAL FAILURE EXCRETED RENALLY AS ACTIVE DRUG ACTIVE METABOLITE POTENTIALLY TOXIC METABOLITE HOW ADJUST DOSING? REDUCE DOSE EXTEND DOSING INTERVAL WHEN ADJUST? 50, 30, 10 ML/MIN AND SOMETIMES AT 80 18
19 ISONIAZID RENAL DOSING ACUTE RENAL FAILURE IN OVER DOSE CL CR <10, REDUCE DOSE BY 50% RIFAMPIN CAN CAUSE ACUTE RENAL FAILURE CL CR < 10, REDUCE DOSE BY 50% RENAL DOSING AMINOGLYCOSIDES SM, AMK, KAN, CAP CAUSE RENAL TOXICITY REDUCE DOSE AT 80 ML/MIN, 50, AND 10 OR EXTEND DOSING INTERVAL EMB EMB RENALLY EXCRETED AS ACTIVE DRUG REDUCE DOSE AT 50 ML/MIN, 10 ML/MIN 19
20 PZA RENAL DOSING DOSE CHANGES NOT GENERALLY REQUIRED BUT - CL CR < 50 REDUCE DOSE TO MG/KG/D EXTEND INTERVAL AT 10 ML/MIN DIALYSIS AVOID USE RIFABUTIN CL < 30 ML/MIN REDUCE DOSE BY 50% QUINALONES RENAL DOSING OFLOXACIN, LEVOFLOXACIN REDUCE DOSES AT 50 ML/MIN EXTEND INTERVAL AT 10 ML/MIN MOXIFLOXACIN NO DOSAGE ADJUSTMENT NEEDED CYCLOSERINE REDUCE DOSE AT 80, 50, 10 ML 20
21 HEMODIALYSIS CAN GENERALLY GIVE STANDARD DAILY DOSES 3 TIMES A WEEK AFTER DIALYSIS MAY GET DIALYSIS UNIT TO DO DOT FOR YOU DO DRUG LEVELS RENAL FAILURE USE DRUGS METABOLIZED BY LIVER INH, RIF, PZA MOXIFLOXACIN VS LEVOFLOXACIN GIVE LOWER DOSES OF DRUGS RENALLY EXCRETED AS ACTIVE AGENTS GIVE SAME DOSE LESS FREQUENTLY DAILY DOSE 2 OR 3 TIMES A WEEK GIVE AFTER DIALYSIS MONITOR 21
22 CASE JB is successfully treated with steroids for his contrast t related renal failure. Three weeks later he develops elevated AST and ALT (>5x uln) and his total billi is at 4 and increasing. HEPATIC DYSFUNCTION ALLOW LIVER TO COOL OFF USE RENALLY EXCRETED DRUGS EMB, QUINALONE, AMG RESTART SUSPECT DRUGS ONE AT A TIME RIFABUTIN VS RIFAMPIN GIVE TWICE WEEKLY DOSES LEVOFLOXCIN VS MOXIFLOXACIN ADJUNCT AGENTS ACTIGALL INTERFERON ALFA MONITOR 22
23 Pixel PROBLEMS IN TX FAILURE TO RESPOND TB MENINGITIS RENAL FAILURE HEPATITIS NON-COMPLIANCE PSYCHIATRIC ISSUES/ SUBSTANCE ABUSE CAN T SWALLOW P ILLS GI INTOLERANCE ADVERSE DRUG REACTIONS ALLERGIES DRUG INTERACTIONS 23
24 DOT DIRECTLY OBSERVE PATIENT TAKING THE MEDICATION DOD DOT - OR - DOD? DIRECTLY OBSERVED DELIVERY 24
25 CAN T SWALLOW PILLS CRUSH OR USE ORAL LIQUIDS INH SYRUP RIF SIMPLE SYRUP JAM, HONEY, APPLESAUCE, ETC STABILITY? PZA, EMB SIMPLE SYRUP CRUSH IN JELLY, APPLE JUICE INJECTABLES CAN T SWALLOW INH RIF AMINOGLYCOSIDES and CAPREOMYCIN QUINILONES EMB SUPPOSITORIES 25
26 GI INTOLERANCE DIVIDE DOSES START WITH LOW DOSE AND INCREASE OVER SEVERAL DAYS GIVE AFTER MEALS MEDICATE H2 ANTAGONIST/ PPI METOCLOPRAMIDE PROMETHAZINE ZOFRAN LORAZEPAM PEJ TUBE ADR HIGH URIC ACID LEVELS ALLOPURINOL, COLCHICINE, PROBENECID MYALGIAS, ARTHRALGIAS NSAIDS EXERCISE 26
27 ADR GIVE AT BEDTIME SWITCH TO A DIFFERENT DRUG ALLERGY/ITCHING ANTIHISTAMINES STEROIDS DESENSITIZATION DESENSITIZATION ALLERGIES LOW DOSES GIVEN FREQUENTLY AND IN GRADUALLY INCREASING DOSES DO ONLY WHERE EMERGENCY TX IS AVAILABLE 27
28 DRUG INTERACTIONS PHENYTOIN WARFARIN HORMONE BASED CONTRACEPTIVES EFAVIRENZ HIV PROTEASE INHIBITORS QUESTION #5 Which team is going to win the SEC championship? hi Florida Gators Alabama Tide The what? 28
29 Jenifur waiting for the big game to start TB Hotline TB-INFO 29
30 THE END A.G. HOLLEY TB HOTLINE TB-INF0 30
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Drug Interactions Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Treatment: First Line Drugs TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS TREATMENT: GENERAL PRINCIPLES MECHANISM OF ACTION MID 27
 TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS Treatment: First Line Drugs 1. ISONIAZID = INH Bacteriocidal against dividing organisms Dose = 300mg = one pill = well absorbed Good CNS penetration Can be
TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS Treatment: First Line Drugs 1. ISONIAZID = INH Bacteriocidal against dividing organisms Dose = 300mg = one pill = well absorbed Good CNS penetration Can be
Debbie Onofre, RN, BSN March 18, TB Nurse Case Management March 17 19, 2015 San Antonio, Texas
 Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Debbie Onofre, RN, BSN March 18, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION
Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Debbie Onofre, RN, BSN March 18, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION
Anti Tuberculosis Medications: Side Effects & adverse Events
 Anti Tuberculosis Medications: Side Effects & adverse Events Diana Fortune, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Diana Fortune, RN,
Anti Tuberculosis Medications: Side Effects & adverse Events Diana Fortune, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Diana Fortune, RN,
Drug Side Effects and Toxicity
 Drug Side Effects and Toxicity Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Toxicity Nausea and vomiting Any Drug Can Cause
Drug Side Effects and Toxicity Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Toxicity Nausea and vomiting Any Drug Can Cause
Treatment of Tuberculosis
 TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
DRUG SIDE EFFECTS AND TOXICITY
 DRUG SIDE EFFECTS AND TOXICITY Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Objectives After participating in this lecture,
DRUG SIDE EFFECTS AND TOXICITY Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Objectives After participating in this lecture,
5. HIV-positive individuals treated with INH should receive Pyridoxine (B6) 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH
 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH") V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
Standard TB Treatment
 Standard TB Treatment Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
Standard TB Treatment Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Pre-Treatment Evaluation. Treatment of Latent TB Infection (LTBI) Initiating Treatment: Patient Education. Before initiating treatment for LTBI:
 Initiating Treatment: Patient Education. Before initiating treatment for LTBI:") Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric TB: Treatment of Tuberculosis Disease Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [with help from Andrea Cruz, M.D.] Objectives At the end
Advanced Concepts in Pediatric TB: Treatment of Tuberculosis Disease Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [with help from Andrea Cruz, M.D.] Objectives At the end
TB Nurse Case Management San Antonio, TX. TB Medications and Adverse Effects
 TB Nurse Case Management San Antonio, TX April 1 3, 2014 TB Medications and Adverse Effects Debbie Onofre RN, BSN Nurse Consultant/ Nurse Educator Heartland National TB Center April 1, 2014 Debbie Onofre,
TB Nurse Case Management San Antonio, TX April 1 3, 2014 TB Medications and Adverse Effects Debbie Onofre RN, BSN Nurse Consultant/ Nurse Educator Heartland National TB Center April 1, 2014 Debbie Onofre,
Pharmacology and Pharmacokinetics of TB Drugs Part I
 Pharmacology and Pharmacokinetics of TB Drugs Part I Charles A. Peloquin, Pharm. D. Professor, and Director Infectious Disease Pharmacokinetics Laboratory College of Pharmacy and The Emerging Pathogens
Pharmacology and Pharmacokinetics of TB Drugs Part I Charles A. Peloquin, Pharm. D. Professor, and Director Infectious Disease Pharmacokinetics Laboratory College of Pharmacy and The Emerging Pathogens
Managing Complex TB Cases Diana M. Nilsen, MD, RN
 Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
TB Grand Rounds. Reynard McDonald, MD & Henry Fraimow, MD January 30, Outline
 TB Grand Rounds Reynard McDonald, MD & Henry Fraimow, MD January 30, 2007 Outline Overview of 2006 ATS statement regarding hepatotoxicity of anti-tb therapy Case examples highlighting management of patients
TB Grand Rounds Reynard McDonald, MD & Henry Fraimow, MD January 30, 2007 Outline Overview of 2006 ATS statement regarding hepatotoxicity of anti-tb therapy Case examples highlighting management of patients
Treatment of Tuberculosis
 Treatment of Tuberculosis, 1940 s Treatment of Tuberculosis ATS/CDC/IDSA Joint Statement 2003 Saskatchewan Lung Association Outline, 2012 Treatment of Tuberculosis Principles of treatment of tuberculosis
Treatment of Tuberculosis, 1940 s Treatment of Tuberculosis ATS/CDC/IDSA Joint Statement 2003 Saskatchewan Lung Association Outline, 2012 Treatment of Tuberculosis Principles of treatment of tuberculosis
Treatment of Active Tuberculosis
 Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Managing Anti-TB Therapy Side Effects and Complications Lisa Armitige, MD, PhD May 9, 2012 Lisa Armitige, MD, PhD has the following
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Managing Anti-TB Therapy Side Effects and Complications Lisa Armitige, MD, PhD May 9, 2012 Lisa Armitige, MD, PhD has the following
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
Treatment of Tuberculosis Disease. Treatment of Tuberculosis. Decision to Treat Initiation of Therapy 1
 Treatment of Tuberculosis Some Highlights of Most Recent Update Treatment of Tuberculosis Disease Germaine Jacquette, MD Physician Specialist NJMS Global Tuberculosis Institute September 15, 2010 The provider
Treatment of Tuberculosis Some Highlights of Most Recent Update Treatment of Tuberculosis Disease Germaine Jacquette, MD Physician Specialist NJMS Global Tuberculosis Institute September 15, 2010 The provider
SA TB Guidelines The interface with Advanced Clinical Care
 SA TB Guidelines The interface with Advanced Clinical Care Dr Kogie Naidoo (MBCHB, PHD) Head: CAPRISA Treatment Research Programme Honorary Lecturer - UKZN Department of Public Heath Medicine Annual Workshop
SA TB Guidelines The interface with Advanced Clinical Care Dr Kogie Naidoo (MBCHB, PHD) Head: CAPRISA Treatment Research Programme Honorary Lecturer - UKZN Department of Public Heath Medicine Annual Workshop
Pediatric TB Intensive San Antonio, Texas October 14, 2013
 Pediatric TB Intensive San Antonio, Texas October 14, 2013 Treatment of Tuberculosis in Children Jeffrey R. Starke, M.D. Professor of Pediatrics October 14, 2013 Jeffrey R. Starke, M.D. has the following
Pediatric TB Intensive San Antonio, Texas October 14, 2013 Treatment of Tuberculosis in Children Jeffrey R. Starke, M.D. Professor of Pediatrics October 14, 2013 Jeffrey R. Starke, M.D. has the following
6/8/2018 TB TREATMENT. Bijan Ghassemieh, MD Seattle TB Clinical Intensive Disclosures. None
 TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
Case presentation. Dr Connie Haley, MD, MPH Dr Gautam Kalyatanda, MD
 Case presentation Dr Connie Haley, MD, MPH Dr Gautam Kalyatanda, MD History of presenting illness 20 Year old woman from Nigeria who came to study at Montgomery in August 2013 About 2 weeks after arriving,
Case presentation Dr Connie Haley, MD, MPH Dr Gautam Kalyatanda, MD History of presenting illness 20 Year old woman from Nigeria who came to study at Montgomery in August 2013 About 2 weeks after arriving,
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Mitnick CD, Shin SS, Seung KJ, et al. Comprehensive treatment
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Mitnick CD, Shin SS, Seung KJ, et al. Comprehensive treatment
Pediatric TB Intensive Houston, Texas
 Pediatric TB Intensive Houston, Texas November 13, 2009 Treatment of Pediatric TB Jeffrey R. Starke, M.D. November 13, 2009 MANAGEMENT OF CHILDHOOD TUBERCULOSIS Jeffrey R. Starke, M.D. Professor of Pediatrics
Pediatric TB Intensive Houston, Texas November 13, 2009 Treatment of Pediatric TB Jeffrey R. Starke, M.D. November 13, 2009 MANAGEMENT OF CHILDHOOD TUBERCULOSIS Jeffrey R. Starke, M.D. Professor of Pediatrics
LTBI in Special Populations John Nava, MD October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
Official ATS/CDC/IDSA Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis (Nahid et al, CID 2016)
") Official ATS/CDC/IDSA Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis (Nahid et al, CID 2016) APPENDIX C: DRUGS IN CURRENT USE The U.S. Food and Drug Administration (FDA) has approved
Official ATS/CDC/IDSA Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis (Nahid et al, CID 2016) APPENDIX C: DRUGS IN CURRENT USE The U.S. Food and Drug Administration (FDA) has approved
LTBI Videos-Treatment
 LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
Managing the Patients Response to TB Treatment
 Managing the Patients Response to TB Treatment Barbarah Martinez, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Barbarah Martinez, RN, BSN has
Managing the Patients Response to TB Treatment Barbarah Martinez, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Barbarah Martinez, RN, BSN has
Dosage and Administration
 SIRTURO product information for healthcare providers 2 WARNINGS: An increased risk of death was seen in the SIRTURO (bedaquiline) treatment group (9/79, 11.4%) compared to the placebo treatment group (2/81,
SIRTURO product information for healthcare providers 2 WARNINGS: An increased risk of death was seen in the SIRTURO (bedaquiline) treatment group (9/79, 11.4%) compared to the placebo treatment group (2/81,
Tuberculosis medications: adverse drug reactions
 Tuberculosis medications: adverse drug reactions Rajesh M. Prabhu, M.D. Infectious Diseases Essentia Health, Duluth, MN July 25, 2017 2014 MFMER slide-1 No Finanial Disclosures Learning Objectives 1. Describe
Tuberculosis medications: adverse drug reactions Rajesh M. Prabhu, M.D. Infectious Diseases Essentia Health, Duluth, MN July 25, 2017 2014 MFMER slide-1 No Finanial Disclosures Learning Objectives 1. Describe
Treatment of Tuberculosis
 TB Intensive Tyler, Texas June 1-3, 2009 Treatment of Tuberculosis Barbara Seaworth, MD June 3, 2009 Treatment of Tuberculosis Barbara J Seaworth MD Medical Director Heartland National TB Center 1 Purpose
TB Intensive Tyler, Texas June 1-3, 2009 Treatment of Tuberculosis Barbara Seaworth, MD June 3, 2009 Treatment of Tuberculosis Barbara J Seaworth MD Medical Director Heartland National TB Center 1 Purpose
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Case Management of the TB/HIV Infected Patient
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Nurse Case Management
 TB Nurse Case Management San Antonio, Texas March 2-4, 2011 TB Medications and Adverse Effects Debbie Onofre, RN, BSN March 3, 2011 Debbie Onofre, RN, BSN has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas March 2-4, 2011 TB Medications and Adverse Effects Debbie Onofre, RN, BSN March 3, 2011 Debbie Onofre, RN, BSN has the following disclosures to make: No conflict
Analysis. Answers. Action. Saturday Night Fever. Shaka Brown Capital Congress
 Saturday Night Fever Shaka Brown Capital Congress Shaka Zulu October 31, 2012 SICK SUCKS How my illness started October 2013 August to October 2013 Symptoms: Severe fatigue Night sweats Low grade fever
Saturday Night Fever Shaka Brown Capital Congress Shaka Zulu October 31, 2012 SICK SUCKS How my illness started October 2013 August to October 2013 Symptoms: Severe fatigue Night sweats Low grade fever
Treatment of Tuberculosis, 2017
 Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Management of MDR TB in special situations. Dr Sarabjit Chadha The Union
 Management of MDR TB in special situations Dr Sarabjit Chadha The Union MDR TB in special situations Pregnancy Breastfeeding Contraception Renal Insufficiency Diabetes Pregnancy and TB Pregnancy is not
Management of MDR TB in special situations Dr Sarabjit Chadha The Union MDR TB in special situations Pregnancy Breastfeeding Contraception Renal Insufficiency Diabetes Pregnancy and TB Pregnancy is not
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Shu-Hua Wang, MD, MPH &TM Assistant Professor of Medicine The Ohio State University
 Shu-Hua Wang, MD, MPH &TM Assistant Professor of Medicine The Ohio State University For anti-tuberculosis medications: Describe clinical monitoring for adverse drug reactions Review specific drug side
Shu-Hua Wang, MD, MPH &TM Assistant Professor of Medicine The Ohio State University For anti-tuberculosis medications: Describe clinical monitoring for adverse drug reactions Review specific drug side
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014
 Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Monitoring Patients for TB Adverse Reactions and Managing Side Effects Catalina Navarro, RN, BSN April 11, 2014 Catalina Navarro, RN,
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Monitoring Patients for TB Adverse Reactions and Managing Side Effects Catalina Navarro, RN, BSN April 11, 2014 Catalina Navarro, RN,
Treatment and Monitoring
 Treatment and Monitoring Disclosures We have no actual or potential conflicts of interest in relation to this presentations. We have no financial relationships to disclose. Learning Objectives After this
Treatment and Monitoring Disclosures We have no actual or potential conflicts of interest in relation to this presentations. We have no financial relationships to disclose. Learning Objectives After this
Dana G. Kissner, MD Detroit Department of Health & Wellness Promotion Wayne State University
 Dana G. Kissner, MD Detroit Department of Health & Wellness Promotion Wayne State University I reply to those who urge me to take medicine that they should wait at least until I am restored to my strength
Dana G. Kissner, MD Detroit Department of Health & Wellness Promotion Wayne State University I reply to those who urge me to take medicine that they should wait at least until I am restored to my strength
104 MMWR December 17, 2004
 104 MMWR December 17, 2004 TABLE 8. Substantial pharmacokinetic drug-drug interactions for drugs used in the treatment of opportunistic Drugs Interacting with Mechanism/effects Recommendations Acyclovir
104 MMWR December 17, 2004 TABLE 8. Substantial pharmacokinetic drug-drug interactions for drugs used in the treatment of opportunistic Drugs Interacting with Mechanism/effects Recommendations Acyclovir
Antimycobacterial drugs. Dr.Naza M.Ali lec Dec 2018
 Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015
 Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 Initiation Phase Part 1 Ginny Dowell, RN, BSN February 4, 2015 Ginny Dowell RN, BSN has the following disclosures to make:
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 Initiation Phase Part 1 Ginny Dowell, RN, BSN February 4, 2015 Ginny Dowell RN, BSN has the following disclosures to make:
Patient History 1. Patient History 2. Social History. The Role of Surgery in the Management of TB. Reynard McDonald, MD & Paul Bolanowski, MD
 Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
Early Identification and Prevention of Drug-to-Drug Interactions in a tertiary care hospital. RadhikaSoanker*, SubbalaxmiMVS $.
 Early Identification and Prevention of Drug-to-Drug Interactions in a tertiary care hospital. RadhikaSoanker*, SubbalaxmiMVS $. * Dept of Clinical Pharmacology & Therapeutics, $ Dept of General Medicine,
Early Identification and Prevention of Drug-to-Drug Interactions in a tertiary care hospital. RadhikaSoanker*, SubbalaxmiMVS $. * Dept of Clinical Pharmacology & Therapeutics, $ Dept of General Medicine,
Antituberculous Agents
 Antituberculous Agents Primary or First Line Drugs: Isoniazid (INH) Rifampin Rifadin or Rimactane Ethambutal Streptomycin Pyrazinamide Isoniazid(INH) Most active. Small molecule, water soluble, Structurally
Antituberculous Agents Primary or First Line Drugs: Isoniazid (INH) Rifampin Rifadin or Rimactane Ethambutal Streptomycin Pyrazinamide Isoniazid(INH) Most active. Small molecule, water soluble, Structurally
Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)
") Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)-750-5496 Local health care providers, including physicians offices, labs and hospitals, are required by law to
Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)-750-5496 Local health care providers, including physicians offices, labs and hospitals, are required by law to
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Drugs David Griffith, MD August 13, 2014 David Griffith, MD has the following disclosures to make: No conflict
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Drugs David Griffith, MD August 13, 2014 David Griffith, MD has the following disclosures to make: No conflict
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
Dose Counting Exercise Elizabeth Foy, RN, BSN September 8, 2016
 Dose Counting Exercise Elizabeth Foy, RN, BSN September 8, 2016 TB Nurse Case Management September 7-9, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Jessica Quintero, M.Ed., has the following disclosures
Dose Counting Exercise Elizabeth Foy, RN, BSN September 8, 2016 TB Nurse Case Management September 7-9, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Jessica Quintero, M.Ed., has the following disclosures
Management of MDR TB. Dr Priscilla Rupali MD; DTM&H Professor and Head Department of Infectious Diseases Christian Medical College Vellore
 Management of MDR TB Dr Priscilla Rupali MD; DTM&H Professor and Head Department of Infectious Diseases Christian Medical College Vellore Outline Global epidemiology of Tuberculosis Epidemiology of Tuberculosis
Management of MDR TB Dr Priscilla Rupali MD; DTM&H Professor and Head Department of Infectious Diseases Christian Medical College Vellore Outline Global epidemiology of Tuberculosis Epidemiology of Tuberculosis
Anti Tuberculosis Medications
 Anti Tuberculosis Medications Mary Ann Rodriguez, MD March 8, 2017 TB Nurse Case Management March 7 9, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Mary Ann Rodriguez, MD has the following disclosures
Anti Tuberculosis Medications Mary Ann Rodriguez, MD March 8, 2017 TB Nurse Case Management March 7 9, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Mary Ann Rodriguez, MD has the following disclosures
Pharmacokinetics (PK) and Pharmacodynamics (PD) in the Treatment of Tuberculosis
 and Pharmacodynamics (PD) in the Treatment of Tuberculosis") Pharmacokinetics (PK) and Pharmacodynamics (PD) in the Treatment of Tuberculosis Shaun E. Gleason, PharmD, MGS Associate Professor, Department of Clinical Pharmacy Director, Distance Degrees and Programs
Pharmacokinetics (PK) and Pharmacodynamics (PD) in the Treatment of Tuberculosis Shaun E. Gleason, PharmD, MGS Associate Professor, Department of Clinical Pharmacy Director, Distance Degrees and Programs
MANAGEMENT OF DILI in TB/HIV coinfected patients. Chimoio 31 August 2017 by Dr Ndiviwe Mphothulo
 MANAGEMENT OF DILI in TB/HIV coinfected patients Chimoio 31 August 2017 by Dr Ndiviwe Mphothulo ANTI-TB drugs Groups Drugs Group 1: First-line oral drugs Ethambutol (Emb) Pyrazinamide(PZA) Isoniazid (INH)
MANAGEMENT OF DILI in TB/HIV coinfected patients Chimoio 31 August 2017 by Dr Ndiviwe Mphothulo ANTI-TB drugs Groups Drugs Group 1: First-line oral drugs Ethambutol (Emb) Pyrazinamide(PZA) Isoniazid (INH)
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
TB and Comorbidities Adriana Vasquez, MD April 12, 2018
 TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
TB Intensive San Antonio, Texas August 7-10, 2012
 TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
Peter Mere Latham English physician & educator
 Poisons and medicine are oftentimes the same substance given with different intents Dana G. Kissner, MD Detroit Department of Health & Wellness Promotion Wayne State University Peter Mere Latham 1789-1875
Poisons and medicine are oftentimes the same substance given with different intents Dana G. Kissner, MD Detroit Department of Health & Wellness Promotion Wayne State University Peter Mere Latham 1789-1875
Tuberculosis: update 2013
 Tuberculosis: update 2013 William R. Bishai, MD, PhD Center for TB Research Division of Infectious Diseases Department of Medicine Johns Hopkins School of Medicine Question 1 A TB speaker at a major conference
Tuberculosis: update 2013 William R. Bishai, MD, PhD Center for TB Research Division of Infectious Diseases Department of Medicine Johns Hopkins School of Medicine Question 1 A TB speaker at a major conference
Concomitant antiretroviral therapy : Avifanz must be given in combination with other antiretroviral medications.
 Avifanz Tablet Description Avifanz is the brand name for Efavirenz. Efavirenz, a synthetic antiretroviral agent, is a non-nucleoside reverse transcriptase inhibitor. While Efavirenz is pharmacologically
Avifanz Tablet Description Avifanz is the brand name for Efavirenz. Efavirenz, a synthetic antiretroviral agent, is a non-nucleoside reverse transcriptase inhibitor. While Efavirenz is pharmacologically
Medication Administration and Adverse Reactions Alisha Blair, LVN September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Medication Administration and Adverse Reactions Alisha Blair, LVN September 28, 2011 Alisha Blair, LVN, has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Medication Administration and Adverse Reactions Alisha Blair, LVN September 28, 2011 Alisha Blair, LVN, has the following disclosures to make:
Overcoming the Challenges in Access to TB Drugs for Children
 Overcoming the Challenges in Access to TB Drugs for Children Gregory L. Kearns, PharmD, PhD Professor of Pediatrics and Pharmacology, University of Missouri Marion Merrell Dow / Missouri Chair in Pediatric
Overcoming the Challenges in Access to TB Drugs for Children Gregory L. Kearns, PharmD, PhD Professor of Pediatrics and Pharmacology, University of Missouri Marion Merrell Dow / Missouri Chair in Pediatric
MDR TB/HIV INTEGRATION MDR TB WORKSHOP 18 SEPTEMBER 2015
 MDR TB/HIV INTEGRATION MDR TB WORKSHOP 18 SEPTEMBER 2015 HIV & MDR :Impact of early ART initiation Adjusted HR: 0.14; p = 0.042 86% reduction in mortality with ART Initiation during MDR-TB treatment 2015
MDR TB/HIV INTEGRATION MDR TB WORKSHOP 18 SEPTEMBER 2015 HIV & MDR :Impact of early ART initiation Adjusted HR: 0.14; p = 0.042 86% reduction in mortality with ART Initiation during MDR-TB treatment 2015
Etiological Agent: Pulmonary Tuberculosis. Debra Mercer BSN, RN, RRT. Definition
 Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Outline 8/2/2013. PK/PD PK/PD first-line drug กก PK/PD กก
 Pharmacokinetic and pharmacodynamic of anti- tuberculosis drugs Outline PK/PD PK/PD first-line drug กก PK/PD กก Concentration vs time in tissue and other body fluids Pharmacologic or toxicologic effect
Pharmacokinetic and pharmacodynamic of anti- tuberculosis drugs Outline PK/PD PK/PD first-line drug กก PK/PD กก Concentration vs time in tissue and other body fluids Pharmacologic or toxicologic effect
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015
 Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 TB Medications and Adverse Drug Events Presented by Evelyn Drzymala, RN, BSN February 11, 2015 Evelyn Drzymala, RN, BSN has
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 TB Medications and Adverse Drug Events Presented by Evelyn Drzymala, RN, BSN February 11, 2015 Evelyn Drzymala, RN, BSN has
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
What He Said: Rifampin versus Rifapentine
 What He Said: Rifampin versus Rifapentine Charles A. Peloquin, Pharm.D. Director Infectious Disease Pharmacokinetics Laboratory Professor, College of Pharmacy & The Emerging Pathogens Institute University
What He Said: Rifampin versus Rifapentine Charles A. Peloquin, Pharm.D. Director Infectious Disease Pharmacokinetics Laboratory Professor, College of Pharmacy & The Emerging Pathogens Institute University
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Therapeutic Drug Monitoring for Improving TB Treatment Outcomes: A Concept for a Randomized Clinical Trial before Clinical Implementation
 Therapeutic Drug Monitoring for Improving TB Treatment Outcomes: A Concept for a Randomized Clinical Trial before Clinical Implementation Randall Reves, MD, MSc TB Consultant Professor of Medicine and
Therapeutic Drug Monitoring for Improving TB Treatment Outcomes: A Concept for a Randomized Clinical Trial before Clinical Implementation Randall Reves, MD, MSc TB Consultant Professor of Medicine and
Marcos Burgos, MD has the following disclosures to make:
 Guidelines for the Treatment of Tuberculosis Marcos Burgos, MD May 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures
Guidelines for the Treatment of Tuberculosis Marcos Burgos, MD May 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures
TB Special Situations Case Discussions
 TB Special Situations Case Discussions Chris Keh, MD TB Control, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, UCSF Curry International Tuberculosis
TB Special Situations Case Discussions Chris Keh, MD TB Control, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, UCSF Curry International Tuberculosis
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Treatment of Tuberculosis
 Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
Co-morbidities & Special Situations
 7 Co-morbidities & Special Situations 3rd edition contributors: GISELA F. SCHECTER, MD, MPH & AMIT S. CHITNIS, MD, MPH Extrapulmonary TB....................................... 174 Central nervous system
7 Co-morbidities & Special Situations 3rd edition contributors: GISELA F. SCHECTER, MD, MPH & AMIT S. CHITNIS, MD, MPH Extrapulmonary TB....................................... 174 Central nervous system
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas April 6-8, 2011 TB Disease: ATS/CDC/IDSA Guidelines Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received
TB Intensive San Antonio, Texas April 6-8, 2011 TB Disease: ATS/CDC/IDSA Guidelines Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
TB BASICS: PRIORITIES AND CLASSIFICATIONS
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.
Treatment of Tuberculosis
 Treatment of Tuberculosis American Thoracic Society, CDC, and Infectious Diseases Society of America Please note: An erratum has been published for this article. To view the erratum, please click here.
Treatment of Tuberculosis American Thoracic Society, CDC, and Infectious Diseases Society of America Please note: An erratum has been published for this article. To view the erratum, please click here.
Anri Uys (MSc Pharmacology, BPharm NWU) Medicines Information Centre, Division of Clinical Pharmacology University of Cape Town
 Medicines Information Centre, Division of Clinical Pharmacology University of Cape Town") Anri Uys (MSc Pharmacology, BPharm NWU) Medicines Information Centre, Division of Clinical Pharmacology University of Cape Town Since March 2008 26 700 Queries to date 450 Queries per month South Africa:
Anri Uys (MSc Pharmacology, BPharm NWU) Medicines Information Centre, Division of Clinical Pharmacology University of Cape Town Since March 2008 26 700 Queries to date 450 Queries per month South Africa:
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Chapter 5 Treatment for Latent Tuberculosis Infection
 Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Tuberculosis Intensive November 17 20, 2015 San Antonio, TX
 Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2013
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
TB Nurse Case Management. March 7-9, Diagnosis of TB: Ken Jost Wednesday March 7, 2012
 TB Nurse Case Management San Antonio, Texas March 7-9, 2012 Diagnosis of TB: Laboratory Ken Jost Wednesday March 7, 2012 Ken Jost has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 7-9, 2012 Diagnosis of TB: Laboratory Ken Jost Wednesday March 7, 2012 Ken Jost has the following disclosures to make: No conflict of interests No relevant
Introduction to. Pharmacokinetics. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Introduction to 1 Pharmacokinetics University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 2 Learning objectives Understand compartment models and how they effects
Introduction to 1 Pharmacokinetics University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 2 Learning objectives Understand compartment models and how they effects
Pediatric Tuberculosis: The Essentials October 8, 2014
 Pediatric Tuberculosis: The Essentials Ann M Loeffler, MD Randall Children s Hospital at Legacy Emanuel Portland, Oregon Curry International TB Center Disclosures Nothing to disclose Learning Objectives
Pediatric Tuberculosis: The Essentials Ann M Loeffler, MD Randall Children s Hospital at Legacy Emanuel Portland, Oregon Curry International TB Center Disclosures Nothing to disclose Learning Objectives