TB and Co-Morbidities Lisa Armitige, MD, PhD September 27, 2011
|
|
|
- Bertha Perry
- 6 years ago
- Views:
Transcription
1 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 TB and Co-Morbidities Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest. No relevant financial relationships with any commercial companies pertaining to this educational activity. 1
2 Tuberculosis and Co-Morbidities Lisa Armitige, MD, PhD Medical Consultant Heartland National TB Center Associate Professor of Medicine/Pediatrics University of Texas at Tyler Diabetes 2
3 Type 2 Diabetes Increased risk has been noted in many racial and ethnic populations African Americans Hispanic/Latino Americans Native Americans Asian Americans Globally urbanization has fueled an increasing incidence in Africa, India, Asia Areas of world with high rates of tuberculosis Prevalence of Diagnosed Diabetes by Race/Ethnicity and Age in Persons 18 & Older AGE White, Black, Hispanic Other non-hispanic non-hispanic Overall Texas Diabetes Fact Sheet,
4 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) No Data <14.0% % % % >26.0% Diabetes No Data <4.5% % % % >9.0% CDC s Division of Diabetes Translation. National Diabetes Surveillance System available at updated 11/09 Does Diabetes Predispose to TB? DOES TB INCREASE THE RISK OF DIABETES? 4
5 Diabetes: a Moderate to Strong Risk Factor for TB 2008 Meta analysis 13 studies many areas of world showed increased risk of TB in persons with diabetes 3 prospective cohort studies showed RR case-control studies and 2 other types- OR Association of Diabetes and TB stronger With higher background TB incidence In younger age groups In Central America, Asia, Europe Among North Americans the RR for Hispanics 2.69 Jeon, PLoS Medicine, 2008 Diabetes Predisposes to TB Hong Kong prospective study of 4661 close contacts of active TB cases RR 3.4 in diabetics for both early primary progressive disease ( 3month) and late- reactivation ( within 5 years) disease Lee MS, Int J Tuberc Lung

 6")
6 The Growing Diabetic Epidemic Will Have a Significant Impact on TB Control Global Prevalence of Tuberculosis and Diabetes, 2008 (9.4 WHO 2010) 95% in developing countries (285 WHO 2010) 70% in developing countries (Source: World Health Organization, 2008) 6



7 Projected prevalent DM incidence & TB Incidence Dooley, & Chaisson, Lancet ID, Dec, 2009 At Risk Populations and Behaviors for TB and Diabetes TB Diabetes HIV/AIDS Immune Suppression Alcohol and Drug Abuse Homeless Population Refugees Prisoners Migrant Farm Workers Health Care Workers Native Americans Hispanics Asian / Pacific Islanders Blacks Older Age Unhealthy Diet Smoking Vitamin D deficiency Overweight / Obesity Cardiovascular Disease Family History Polycystic Ovary Syndrome (PCOS) 7


8 Linkage Between Tuberculosis and Diabetes Latent TB Infection (LTBI) in Diabetic Patients Persons with diabetes should be screened for TB with an IGRA or TST Communicate risk of progression to disease to community physicians caring for diabetics If LTBI is found, treat for latent infection INH for 9 months is best approach Be sure to include Vitamin B6 Neuropathy is complication of diabetes and a side effect of INH 8

9 Presentation of TB in Diabetics Various reports of more severe disease Varying findings as to the radiographic presentation? More cavities? Isolated lower lung involvement Classic Article Prior to Availability of TB Medications Howard Root MD, Deaconess Hospital, Boston NEJM, 1934 Dooley, & Chaisson, Lancet ID, Dec

10 TB and Diabetes, CXR Findings 50% each Dooley, & Chaisson, Lancet ID, Dec, 2009 Does Diabetes Impact TB Treatment and Cure? Previously thought not to affect treatment Four new studies from Baltimore, Texas, Taiwan and Indonesia reveal: Delayed culture conversion Higher mortality Dooly, 2009; Restrepo 2008; Wang 2008; Alisahlanda,
11 Response to Treatment Relapse may be more frequent Recent Shanghai study 203 diabetics with TB followed for 2 years after standard treatment 20% relapse rate in patients with DM (most Type 2) 5% relapse rate in patients without DM Zhang et al. Jpn J Infect Dis, 2009 Hyperglycemia in Patients with TB Blood glucose control may worsen while patients are taking Rifampin Rifampin augments intestinal absorption of glucose Does so in both diabetics and non-diabetics Infections impair glucose tolerance early in disease in both diabetics and non-diabetics Independent of rifampin, infection can lead to poor glucose control 11
12 Does Diabetes Increase the Risk of TB? DOES TB INCREASE THE RISK OF DIABETES? No evidence to suggest that having tuberculosis or taking medications for tuberculosis increases the risk for diabetes Increased hyperglycemia with active disease and with rifampininduced medicine interactions, does not lead to development of diabetes 12
13 Low Blood Levels of Rifampin in Diabetics: Indonesia 17 Patients with Diabetes and Tuberculosis Rifampin levels decreased 50% Perhaps related to higher BMI in diabetics Is a different dose of rifampin needed? Mg/kg? Hanneke M. J. Nijland Clinical Infectious Diseases, Treatment Issues Rifampin Rifampin induces CYP450 enzyme system increasing production of enzymes that metabolize many drugs Increased metabolism results in lower blood levels of drug (20 40+%) Affects many classes of diabetic medications 13
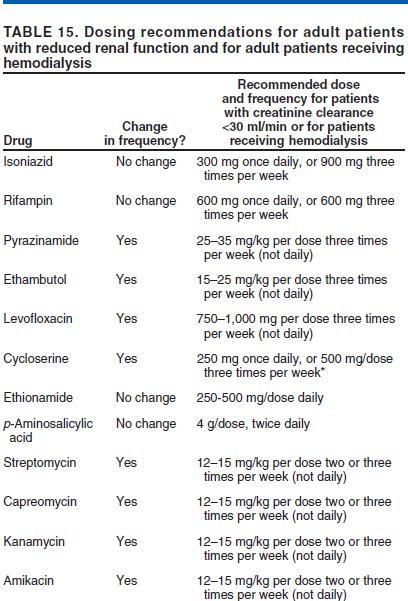
14 Effects of Rifampin on Anti-diabetic Drugs (Prandin) TB and Diabetes -Treatment Issues Diabetic neuropathy at baseline complicates therapy due to INH-related neuropathy Baseline assessment of neuropathy Vitamin B 6 (pyridoxine) to all diabetics on INH or ethionamide Renal insufficiency is associated with diabetes, especially long standing or poorly controlled diabetes Adjust dose and dosing interval of EMB & PZA in those with Creatinine Cl < 30 14
15 TB and Diabetes -Treatment Issues Diabetics have an increased risk of hepatotoxicity Multiple medications Fatty liver Monitoring and education are very important Baseline and monthly liver enzymes Educate regarding risk of liver toxicity, symptoms to watch for, and what to do should these occur Contact provider Hold TB medications until liver injury excluded What Can We Offer in TB Clinics? Include glucose or HB A1C on blood work. Educate on need to follow a healthy eating plan. Encourage physical activity for 30 to 60 minutes/ day. Stress the importance of taking medicines as directed. Encourage patients to quit smoking. Refer for regular physician visits Educate on need for daily foot check for cuts, blisters, sores, swelling, redness, or sore toenails. 15
16 TNF-α Antagonists TB in Patients treated with TNF-α Antagonists TNF-α: key role in control of latent TB Animal models Clinical disease in recipients Current agents: Infliximab (Remicade) Etanercept (Enbrel) Adalimumab (Humira) Certolizumab (Cimzia) Treatment with these associated with the development of active TB, often disseminated with aggressive progression TB reported more frequently than other opportunistic infections (OI) 16
 TB developed after median of 12 weeks 48 developed disease after 3 or less infusions 48/70 (69%) had extra pulmonary disease 17 disseminated 11 lymphatic, 4 peritoneal, 2 pleural 1 each")
17 * * * Per 100,000 treated patients Wallis, Lancet Inf Dis, 2008 TB in Patients treated with TNF-α Monoclonal Antibodies 70 cases of active TB reported in patients treated with infliximab (up to 5/29/01) TB developed after median of 12 weeks 48 developed disease after 3 or less infusions 48/70 (69%) had extra pulmonary disease 17 disseminated 11 lymphatic, 4 peritoneal, 2 pleural 1 each meningeal, enteric, paravertebral, bone, genital and bladder Confirmed by biopsy in 33 patients 12 patients died despite stopping TNF-α antagonist Keane N Engl J Med 2001; 345:
18 TB in Rheumatoid Arthritis and Effect of TNF-α Antagonists TB incidence in 6,460 infliximab treated patients followed prospectively in Spanish data base 61.9/100,000 No cases with other agents TB incidence in 10,782 patients prior to widespread use of infliximab 6.2/100,000 Marked decrease in TB with use of screening Gomez-Reino Arthritis Rheum 2003; 48: Warning: Risk Of Infections :Infliximab Tuberculosis (frequently disseminated or extrapulmonary at clinical presentation), and other opportunistic infections have been observed in patients receiving Remicade some of these infections have been fatal Patients should be evaluated for LTBI with a TST Treatment of LTBI should be initiated prior to therapy with Remicade SEE WARNINGS PDR

19 Etanercept All Anti-TNF Wallis, Lancet Inf Dis, 2008 Development of Active TB by Drug New infections shortly after start of TNF alpha antagonist - Reactivation TB Infliximab 20%/month 12 to 1 times greater than with etanercept Both drugs caused an equally high proportion of new infections that progressed directly to TB disease Excess cases of TB with Infliximab due to more efficient reactivation of latent TB infection. Wallis, Lancet Inf Dis,
20 Management of Patients with Suspected Infection Receiving TNF- Antagonists Stop TNF- antagonist if fever and other signs/symptoms consistent with an infectious process occur in a patient at possible risk for tuberculosis Aggressive evaluation Start empiric therapy for suspected pathogens while waiting cultures Dual infections have been reported Disagreement about when or whether TNF- antagonist can be restarted Paradoxical Upgrading in TNF-α Blocker Recipients Reactions similar or worse in intensity to those noted in HIV infected individuals Anti-inflammatory treatment important therapeutic intervention Steroids reported beneficial by Garcia et al in CID, 2005 Steroid use controversial by others 20
21 TB and Renal Disease TB in Chronic Kidney Disease Increased risk of progression from latent to active TB with chronic kidney disease (CKD) Difficulty diagnosing & treating dialysis patient Symptoms often mistaken for complications of dialysis Cough (congestive heart failure, fluid overload), fever (bacterial infection) Atypical presentation Extrapulmonary TB, especially abdominal TB common Contact investigation in a dialysis center is challenging Interpretation of TST and/or IGRA (BCG vaccinated persons) Excluding active TB Interpretation of symptoms Interpretation of chest x-ray ( heart failure, chronic infiltrates) 21
22 California TB Controller Association (CTCA) Recommendations TB skin test or IGRA At diagnosis of CKD When diagnosed with DM Thirty days prior to admission to HD Unit Thirty days prior to scheduled renal transplant Annual/periodic If TST Two step should be done TB Presentation in Dialysis Patient Pulmonary Atypical presentation Fever most common sign! Weight Loss Anorexia Cough (may be present) TB Disease considered in ANY patient with Recurrent pneumonia Pneumonia not improved within 2 weeks of antibiotics avoid fluoroquinolones, they may mask TB! 22
23 TB Presentation in Dialysis patients Extra pulmonary TB More common in dialysis patients Don t forget to do SPUTUMS!! Abdominal (Peritoneal, liver, bowel, adenopathy) TB peritonitis can be difficult to distinguish from bacterial Any other site possible, evaluate if abnormal TB Screening for CKD Patients TB Risk Assessment Questionnaire (RAQ) Rule Out - Active TB! Use Standardized risk assessment tool (RAQ) 23
24 CXR Findings of TB in CKD Cavitations, typical nodules and upper lobe infiltrates less common in late stage CKD Dialysis patients and transplant patients are immunocompromised and may have atypical findings on chest x-rays Any lung region, especially lower lobes, miliary, diffuse, resembling pulmonary edema, or NORMAL Pleural effusions 24
25 Pleural Effusions Delay in TB Diagnosis can occur If assumed that pleural effusions reflect volume overload or under dialyzed Consider diagnostic thoracentesis Pleural fluid or specimen biopsy Expert consultation with TB doctor Treatment Regimen: Active TB Initial Phase (first two months): INH 300mg po daily or 900 mg thrice weekly Rifampin 600mg po daily or thrice weekly Ethambutol 15-25mg/kg po thrice weekly PZA 25-35mg/kg po thrice weekly Vitamin B6 50mg thrice weekly Continuation INH and Rifampin x 4 7 months All doses should be given AFTER DIALYSIS 25
26 HIV 26
27 Outcomes of Exposure to M. tuberculosis Inhalation of Droplet Nuclei Regional replication in lungs, dissemination ~90% ~5% ~5% Killing, clearance of organisms Latent disease Active disease Outcomes of Exposure to M. tuberculosis in HIV-negative and HIV-positive patients Inhalation of Droplet Nuclei Regional replication in lungs, dissemination ~90% 10% reactivation ~5% reactivation per year lifetime Up to 36% active disease ~5% Killing, clearance of organisms Latent disease Active disease 27
28 Clinical Presentation HIV-positive vs. HIV-negative patients Driven mostly by degree of immunity HIV-positive patients are more likely to have: Isolated extrapulmonary localization (53-63% in some studies) Primary infection Pulmonary basilar involvement Tuberculous pneumonia Hilar or mediastinal lymphadenopathies Miliary or disseminated TB Normal CXR (8-20% in some studies) Clinical Microbiology and Infection, Volume 10 Number 5, May 2004 Classifying the Tuberculin Reaction 5 mm is classified as positive in HIV-positive persons Recent contacts of TB case Persons with fibrotic changes on chest radiograph consistent with old healed TB Patients with organ transplants and other immunosuppressed patients 28
29 Role of interferon-gamma release assays in the diagnosis of pulmonary tuberculosis in patients with advanced HIV infection Cattamanchi et al. BMC Infectious Diseases 2010, 10:75 ** Risk reduction by treatment of Latent TB Infection (LTBI) in HIV-infected patients Churchyard et al. JID 2007:196 (Suppl 1) S52 29
30 LTBI treatment MMWR August 8, 2003 / Vol. 52 / No. 31 An Algorithm for Tuberculosis Screening and Diagnosis in People with HIV N Engl J Med 2010;362:
 and enfuvirtide Once or twice weekly regimens show high rate of rifampin resistance in HIV")
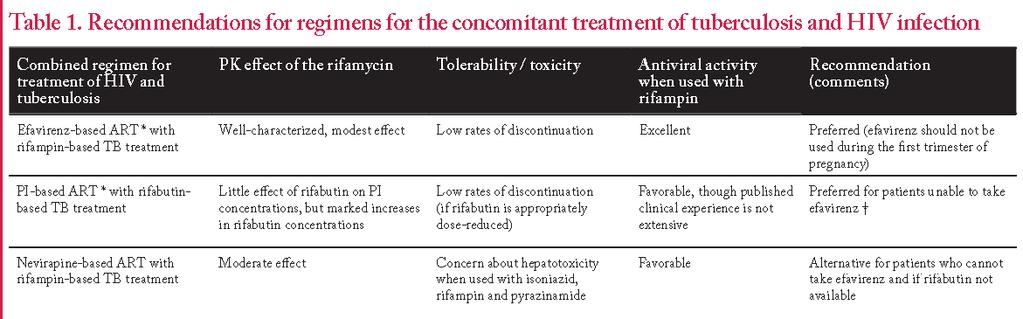
31 ATS recommendations for treatment of tuberculosis * * Morbidity and Mortality Weekly Report June 20, 2003 / Vol. 52 / No. RR-11 Rifamycins Have significant interaction with all ARVs except nucleoside analogues (other than AZT) and enfuvirtide Once or twice weekly regimens show high rate of rifampin resistance in HIV patients with CD4 cell count <100 Most common locus of interaction is the cytochrome P450 system As inducers, rifampin > rifapentine > rifabutin 31
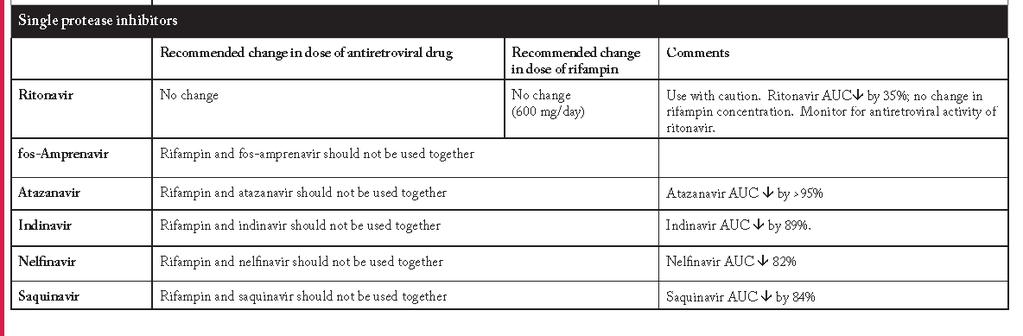
32 Rifampin and PIs Note: Decrease in serum protease inhibitor level is NOT overcome by low dose ritonavir Clinical Microbiology and Infection, Volume 10 Number 5, May 2004 Rifabutin Has much less effect than rifampin on drugs metabolized by CYP3A Requires dosage adjustment due to effects by many other drugs (such as ritonavir). PIs (especially if boosted with ritonavir) cause a marked increase in serum rifabutin serum concentrations and toxicity Rifabutin dose should be decreased when using PI-based regimens. Concerns regarding adequate dosing if patient is not compliant with PI medication 32
33 33
34 34

35 Remember Rifamycins can be safely added to almost any regimen. TB treatment regimens that do not contain rifampin have an unacceptably high failure rate Every effort should be made to treat within the CDC guidelines to increase the chances of treatment success, decrease the chances of relapse and minimize the length of time with toxicities. 35

36 Overall Treatment Outcomes * * Ronan. A. M. JID 2006:193 (15 May) 1439 When should treatment be started when patient is being treated for TB? Considerations Treatment of HIV improves outcomes in patients with TB Decreased death or relapse Multiple medications with multiple potential toxicities that are overlapping If the CD4 count is < 200, generally most ID physicians would treat for HIV with treatment for TB If the CD4 count is > 200 Arguments to start both treatments concurrently Arguments to delay the start of HAART 36

37 National Institute of Allergy and Infectious Diseases (NIAID) Embargoed for Release Thursday, July 22, a.m. EDT Contact: Laura Sivitz Leifman NIH-Funded Study Finds Early HAART during TB Treatment Boosts Survival Rate in People Co-Infected with HIV and TB When should treatment be started when patient is being treated for TB? ACTG 5221 STRIDE Study 806 individuals from 26 sites on 4 continents Conclusions: Overall, immediate ART did not reduce AIDS and death compared to early ART. For persons with CD4 50 cells/mm3 immediate ART resulted in lower rates of AIDS and death compared to early ART. Findings of the SAPiT Trial Findings support integration of TB and HIV treatment Recommend: Patients with CD4+ counts <50 cells/mm 3 Early ART initiation as soon as possible after TB treatment initiation Patients with CD4 counts 50 cells/mm 3 ART initiation can be deferred to start of the continuation phase of TB treatment Decision on early or late initiation: use clinical judgment of capacity to manage IRIS & toxicities 37

38 IRIS Meintjes et al Lancet ID 8: THEY ALWAYS COME BACK Do It Right The First Time! Barbara Seaworth 38
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas August 2-5, 2011 Tuberculosis andco- Morbidities Barbara Seaworth, MD August 3, 2011 Barbara Seaworth, MD has the following disclosures to make: Is on the HHSC advisory
TB Intensive San Antonio, Texas August 2-5, 2011 Tuberculosis andco- Morbidities Barbara Seaworth, MD August 3, 2011 Barbara Seaworth, MD has the following disclosures to make: Is on the HHSC advisory
TB Nurse Case Management
 TB Nurse Case Management San Antonio, Texas March 2-4, 2011 TB and Co Morbidities Barbara Seaworth, MD March 3, 2011 Barbara Seaworth, MD has the following disclosures to make: Has receives research funding
TB Nurse Case Management San Antonio, Texas March 2-4, 2011 TB and Co Morbidities Barbara Seaworth, MD March 3, 2011 Barbara Seaworth, MD has the following disclosures to make: Has receives research funding
Substance Abuse and Tuberculosis Springfield, IL April 27, 2011
 Substance Abuse and Tuberculosis Springfield, IL April 27, 2011 Co-morbidities in Substance Abuse that Impact Managing TB Lisa Armitige, MD, PhD April 27, 2011 Lisa Armitige, MD, PhD has the following
Substance Abuse and Tuberculosis Springfield, IL April 27, 2011 Co-morbidities in Substance Abuse that Impact Managing TB Lisa Armitige, MD, PhD April 27, 2011 Lisa Armitige, MD, PhD has the following
TB Intensive San Antonio, Texas. TB/HIV Co-Infection. Lisa Armitige, MD, PhD has the following disclosures to make:
 TB Intensive San Antonio, Texas August 2-5, 2011 TB/HIV Co-Infection Lisa Armitige, MD, PhD August 4, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas August 2-5, 2011 TB/HIV Co-Infection Lisa Armitige, MD, PhD August 4, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 TB in the HIV Patient Lisa Armitige, MD, PhD April 6, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 TB in the HIV Patient Lisa Armitige, MD, PhD April 6, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 TB and Diabetes Barbara Seaworth, MD July 19, 2012 Barbara Seaworth, MD, FIDSA, FACP has the following disclosures to make: Has an advisory
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 TB and Diabetes Barbara Seaworth, MD July 19, 2012 Barbara Seaworth, MD, FIDSA, FACP has the following disclosures to make: Has an advisory
TB Intensive San Antonio, Texas December 1-3, 2010
 TB Intensive San Antonio, Texas December 1-3, 2010 TB & Diabetes Barbara Seaworth, MD; HNTC December 3, 2010 Dual Epidemic Diabetes - Tuberculosis Barbara J. Seaworth MD Medical Director, Heartland NTBC
TB Intensive San Antonio, Texas December 1-3, 2010 TB & Diabetes Barbara Seaworth, MD; HNTC December 3, 2010 Dual Epidemic Diabetes - Tuberculosis Barbara J. Seaworth MD Medical Director, Heartland NTBC
TB Intensive San Antonio, Texas May 7-10, 2013
 TB Intensive San Antonio, Texas May 7-10, 2013 TB in the HIV Patient Lisa Armitige, MD, PhD May 09, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas May 7-10, 2013 TB in the HIV Patient Lisa Armitige, MD, PhD May 09, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas May 7-10, 2013
 TB Intensive San Antonio, Texas May 7-10, 2013 TB and Diabetes Barbara Seaworth, MD May 09, 2013 Barbara Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial
TB Intensive San Antonio, Texas May 7-10, 2013 TB and Diabetes Barbara Seaworth, MD May 09, 2013 Barbara Seaworth, MD has the following disclosures to make: No conflict of interests No relevant financial
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
TB and Comorbidities Adriana Vasquez, MD April 12, 2018
 TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
TB Intensive Tyler, Texas December 2-4, Tuberculosis and HIV Co-Infection. Lisa Y. Armitige, MD, PhD. December 4, 2008.
 TB Intensive Tyler, Texas December 2-4, 2008 Tuberculosis and HIV Co-Infection Lisa Y. Armitige, MD, Ph.D. December 4, 2008 Tuberculosis and HIV Co Infection Lisa Y. Armitige, MD, PhD Assistant Professor
TB Intensive Tyler, Texas December 2-4, 2008 Tuberculosis and HIV Co-Infection Lisa Y. Armitige, MD, Ph.D. December 4, 2008 Tuberculosis and HIV Co Infection Lisa Y. Armitige, MD, PhD Assistant Professor
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
TB/HIV Co-Infection. Tuberculosis and HIV
 TB Intensive Tyler, Texas June 2-4, 2010 TB/HIV Co-Infection Lisa Y Armitige, MD, PhD June 3, 2010 Tuberculosis and HIV Co-Infection Lisa Y Armitige, MD, PhD Medical Consultant Heartland National TB Center
TB Intensive Tyler, Texas June 2-4, 2010 TB/HIV Co-Infection Lisa Y Armitige, MD, PhD June 3, 2010 Tuberculosis and HIV Co-Infection Lisa Y Armitige, MD, PhD Medical Consultant Heartland National TB Center
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Treatment of Tuberculosis
 TB Intensive Tyler, Texas June 1-3, 2009 Treatment of Tuberculosis Barbara Seaworth, MD June 3, 2009 Treatment of Tuberculosis Barbara J Seaworth MD Medical Director Heartland National TB Center 1 Purpose
TB Intensive Tyler, Texas June 1-3, 2009 Treatment of Tuberculosis Barbara Seaworth, MD June 3, 2009 Treatment of Tuberculosis Barbara J Seaworth MD Medical Director Heartland National TB Center 1 Purpose
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 TB and Diabetes Barbara Seaworth, MD November 13, 2014 Barbara Seaworth, MD has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas November 11 14, 2014 TB and Diabetes Barbara Seaworth, MD November 13, 2014 Barbara Seaworth, MD has the following disclosures to make: No conflict of interests No relevant
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
Co-morbidities that Impact Managing TB Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Co-morbidities that Impact Managing TB Lisa Armitige, MD, PhD November 17, 2010 Co-morbidities in Substance Abuse that Impact
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Co-morbidities that Impact Managing TB Lisa Armitige, MD, PhD November 17, 2010 Co-morbidities in Substance Abuse that Impact
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
TB in the Correctional Setting Florence, Arizona October 7, 2014
 TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
Treating TB What Happened? All the Patients Have Challenging Co-Morbid Conditions Now!
 EXCELLENCE EXPERTISE INNOVATION Treating TB What Happened? All the Patients Have Challenging Co-Morbid Conditions Now! Barbara J Seaworth, MD, Medical Director, Heartland National TB Center Professor,
EXCELLENCE EXPERTISE INNOVATION Treating TB What Happened? All the Patients Have Challenging Co-Morbid Conditions Now! Barbara J Seaworth, MD, Medical Director, Heartland National TB Center Professor,
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
A look at medical factors that increase the risk for TB disease
 A look at medical factors that increase the risk for TB disease Mark Lobato, MD New England TB Consultant Division of Tuberculosis Elimination CDC Overview The spectrum of M. tuberculosis infection Immune
A look at medical factors that increase the risk for TB disease Mark Lobato, MD New England TB Consultant Division of Tuberculosis Elimination CDC Overview The spectrum of M. tuberculosis infection Immune
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Tuberculosis and Diabetes Mellitus. Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant
 Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Disclosures. TB and CoMorbidities Challenges and Opportunities. Burden of TB. Outline of the lecture. Target testing for TB Infection TB HIV 3/25/2012
 Disclosures TB and CoMorbidities Challenges and Opportunities E. Jane Carter, M.D. Associate Professor of Medicine Alpert School of Medicine, Brown University Providence, Rhode Island No financial disclosures
Disclosures TB and CoMorbidities Challenges and Opportunities E. Jane Carter, M.D. Associate Professor of Medicine Alpert School of Medicine, Brown University Providence, Rhode Island No financial disclosures
Approach to Co-infection with TB and HIV: 2011 Henry Fraimow, MD
 Approach to Co-infection with TB and HIV: 2011 Henry Fraimow, MD Consultant, Southern N.J. Regional Chest Clinic New Jersey State TB Physician Advisory Board Cooper Univ. Hospital EIP Program TB and HIV
Approach to Co-infection with TB and HIV: 2011 Henry Fraimow, MD Consultant, Southern N.J. Regional Chest Clinic New Jersey State TB Physician Advisory Board Cooper Univ. Hospital EIP Program TB and HIV
5. HIV-positive individuals treated with INH should receive Pyridoxine (B6) 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH
 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH") V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Drug Interactions Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
TUBERCULOSIS AND THE TNF-α INHIBITORS. Lloyd Friedman, M.D. Yale University Milford Hospital
 TUBERCULOSIS AND THE TNF-α INHIBITORS Lloyd Friedman, M.D. Yale University Milford Hospital Outline TNF-α Anti-TNF-α medications Rates of tuberculosis Lower rates with etanercept Screening for latent tuberculosis
TUBERCULOSIS AND THE TNF-α INHIBITORS Lloyd Friedman, M.D. Yale University Milford Hospital Outline TNF-α Anti-TNF-α medications Rates of tuberculosis Lower rates with etanercept Screening for latent tuberculosis
8/28/2017. Learning Objectives. After attending this presentation, learners will be able to:
 New and Noteworthy in Tuberculosis Diagnostics and Treatment Susan Swindells, MBBS Professor of Internal Medicine University of Nebraska Medical Center Omaha, Nebraska San Antonio, Texas: August 21 to
New and Noteworthy in Tuberculosis Diagnostics and Treatment Susan Swindells, MBBS Professor of Internal Medicine University of Nebraska Medical Center Omaha, Nebraska San Antonio, Texas: August 21 to
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Tuberculosis and Diabetes Dec. 10, 2009 Dean Schillinger, M.D. and Gisela Schecter, M.D., M.P.H. 1 of 18
 Screening, Diagnosis, and Treatment of TB in Persons with Diabetes Dean Schillinger, M.D. University of California San Francisco CA Diabetes Program Gisela Schecter, M.D., M.P.H. TB Control Branch CA Department
Screening, Diagnosis, and Treatment of TB in Persons with Diabetes Dean Schillinger, M.D. University of California San Francisco CA Diabetes Program Gisela Schecter, M.D., M.P.H. TB Control Branch CA Department
LTBI: Who to Test & When to Treat
 LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, TB Nurse Case Management September 12 14, 2017
 Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas April 6-8, 2011 TB Disease: ATS/CDC/IDSA Guidelines Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received
TB Intensive San Antonio, Texas April 6-8, 2011 TB Disease: ATS/CDC/IDSA Guidelines Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received
TB & HIV CO-INFECTION IN CHILDREN. Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012
 TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
Tuberculosis Intensive November 17 20, 2015 San Antonio, TX
 Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
The Epidemiology of Tuberculosis in Minnesota,
 The Epidemiology of Tuberculosis in Minnesota, 2011 2015 Minnesota Department of Health Tuberculosis Prevention and Control Program (651) 201-5414 Tuberculosis surveillance data for Minnesota are available
The Epidemiology of Tuberculosis in Minnesota, 2011 2015 Minnesota Department of Health Tuberculosis Prevention and Control Program (651) 201-5414 Tuberculosis surveillance data for Minnesota are available
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Case Management of the TB/HIV Infected Patient
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014
 TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Chapter 5 Treatment for Latent Tuberculosis Infection
 Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Tuberculosis Pathogenesis
 Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
ESCMID Online Lecture Library. by author
 Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
CLINICAL VIGNETTE: Patient 1. Approach to Co-infection with TB and HIV: TB and HIV Co-infection: Some Resources. Goals and Objectives
 TB and HIV Co-infection: Some Resources http://www.cdc.gov/tb http://www.umdnj.edu/globaltb/coretbresources.htm Approach to Co-infection with TB and HIV: 2011 Henry Fraimow, MD Consultant, Southern N.J.
TB and HIV Co-infection: Some Resources http://www.cdc.gov/tb http://www.umdnj.edu/globaltb/coretbresources.htm Approach to Co-infection with TB and HIV: 2011 Henry Fraimow, MD Consultant, Southern N.J.
Clinical Vignette: Patient 1. Approach to Co-infection with TB. TB and HIV Co-infection: Some Resources. Objectives.
 TB and HIV Co-infection: Some Resources http://www.cdc.gov/tb AETC Natl Resource Center: http://www.aidsetc.org Approach to Co-infection with TB and HIV: 2012 Henry Fraimow, MD Consultant, Southern N.J.
TB and HIV Co-infection: Some Resources http://www.cdc.gov/tb AETC Natl Resource Center: http://www.aidsetc.org Approach to Co-infection with TB and HIV: 2012 Henry Fraimow, MD Consultant, Southern N.J.
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
TB is Global. Latent TB Infection (LTBI) Sharing the Care: Working Together. September 24, 2014
 Sharing the Care: Working Together. September 24, 2014") Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Tuberculosis: update 2013
 Tuberculosis: update 2013 William R. Bishai, MD, PhD Center for TB Research Division of Infectious Diseases Department of Medicine Johns Hopkins School of Medicine Question 1 A TB speaker at a major conference
Tuberculosis: update 2013 William R. Bishai, MD, PhD Center for TB Research Division of Infectious Diseases Department of Medicine Johns Hopkins School of Medicine Question 1 A TB speaker at a major conference
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011
 ART Treatment Guideline Training 31 st January to 4 th February, 2011") TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012
 TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012 Challenges of TB Treatment in Special Populations in Corrections Marcos Burgos, MD November 28, 2012 Marcos Burgos, MD has the following
TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012 Challenges of TB Treatment in Special Populations in Corrections Marcos Burgos, MD November 28, 2012 Marcos Burgos, MD has the following
11/1/2017. Disclosures. Update In Tuberculosis, Indiana Outline/Objectives. Pathogenesis of M.tb Global/U.S. TB Burden, 2016
 Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal
 Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal Civil surgeons are required to report tuberculosis (TB) screening outcomes that result in latent TB
Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal Civil surgeons are required to report tuberculosis (TB) screening outcomes that result in latent TB
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
TB Update: March 2012
 TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
TB Update: March 2012 David Schlossberg, MD, FACP Medical Director, TB Control Program Philadelphia Department of Public Health 1 TB Update: March 2012 IGRAs vs TST LTBI A New Regimen NAATs What is Their
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
Guidelines for. Tuberculosis (TB) Screening and. Treatment of Patients with. Chronic Kidney Disease(CKD), Patients Receiving Hemodialysis (HD),
 Screening and. Treatment of Patients with. Chronic Kidney Disease(CKD), Patients Receiving Hemodialysis (HD),") C T C A G U I D E L I N E S Guidelines for Tuberculosis (TB) Screening and Treatment of Patients with Chronic Kidney Disease(CKD), Patients Receiving Hemodialysis (HD), Patients Receiving Peritoneal Dialysis
C T C A G U I D E L I N E S Guidelines for Tuberculosis (TB) Screening and Treatment of Patients with Chronic Kidney Disease(CKD), Patients Receiving Hemodialysis (HD), Patients Receiving Peritoneal Dialysis
Immune Reconstitution Inflammatory Syndrome. Dr. Lesego Mawela
 Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
Treatment of Tuberculosis, 2017
 Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
Latent Tuberculosis Best Practices
 Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
TB and Diabetes Intersection of Two Diseases
 TB and Diabetes Intersection of Two Diseases E. Jane Carter, M.D. Associate Professor of Medicine Alpert School of Medicine at Brown University Providence, Rhode Island Disclosures No financial disclosures
TB and Diabetes Intersection of Two Diseases E. Jane Carter, M.D. Associate Professor of Medicine Alpert School of Medicine at Brown University Providence, Rhode Island Disclosures No financial disclosures
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Tuberculosis, HIV, and Corrections James B. McAuley, MD, MPH April 22, 2009
 TB in the Correctional Setting Collinsville, Illinois April 22, 2009 Tuberculosis, HIV, and Corrections James B. McAuley, MD, MPH April 22, 2009 Tuberculosis, HIV, and Corrections James B. McAuley, MD
TB in the Correctional Setting Collinsville, Illinois April 22, 2009 Tuberculosis, HIV, and Corrections James B. McAuley, MD, MPH April 22, 2009 Tuberculosis, HIV, and Corrections James B. McAuley, MD
Treatment of Latent TB Infection (LTBI)
") Treatment of Latent TB Infection (LTBI) Mahesh C. Patel, MD June 14, 2017 2014 MFMER slide-1 Mahesh C. Patel, MD Associate Professor Treatment of LTBI Department of Internal Medicine, Division of Infectious
Treatment of Latent TB Infection (LTBI) Mahesh C. Patel, MD June 14, 2017 2014 MFMER slide-1 Mahesh C. Patel, MD Associate Professor Treatment of LTBI Department of Internal Medicine, Division of Infectious
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
Tuberculosis Education for the Medical Professional
 Tuberculosis Education for the Medical Professional North Dakota Diagnosis and Medical Management of Latent TB Infection Dawn Farrell, RN, BSN, PHN Maria Robles, BSN July 10, 2007 Tuberculosis Education
Tuberculosis Education for the Medical Professional North Dakota Diagnosis and Medical Management of Latent TB Infection Dawn Farrell, RN, BSN, PHN Maria Robles, BSN July 10, 2007 Tuberculosis Education
TB Nurse Assessment. Ginny Dowell, RN, BSN October 21, 2015
 TB Nurse Assessment Ginny Dowell, RN, BSN October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19-22, 2015 Wichita, KS EXCELLENCE EXPERTISE INNOVATION Ginny Dowell,
TB Nurse Assessment Ginny Dowell, RN, BSN October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19-22, 2015 Wichita, KS EXCELLENCE EXPERTISE INNOVATION Ginny Dowell,
Latent TB Infection (LTBI) Strategies for Detection and Management
 Strategies for Detection and Management") Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Tuberculosis: Where Are We Now?
 Tuberculosis: Where Are We Now? Amee Patrawalla MD MPH Rutgers - NJ Medical School Global TB Institute Rutgers, The State University of New Jersey Learning Objectives Understand the current epidemiologic
Tuberculosis: Where Are We Now? Amee Patrawalla MD MPH Rutgers - NJ Medical School Global TB Institute Rutgers, The State University of New Jersey Learning Objectives Understand the current epidemiologic
Tuberculosis and Biologic Therapies: Risk and Prevention
 Tuberculosis and Biologic Therapies: Risk and Prevention Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health and Preventive Medicine Oregon Health & Science
Tuberculosis and Biologic Therapies: Risk and Prevention Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health and Preventive Medicine Oregon Health & Science
Treatment of Active Tuberculosis
 Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest