INTENSIVE INSULIN THERAPY: A Long History of Conflicting Data.
|
|
|
- Claud Shannon Boone
- 5 years ago
- Views:
Transcription
1 INTENSIVE INSULIN THERAPY: A Long History of Conflicting Data. Candice Preslaski, PharmD BCPS Clinical Pharmacist Specialist SICU Denver Health Medical Center December 2014
2 OBJECTIVES Review the risk factors and pathophysiology involved in stress hyperglycemia Discuss the theoretical and proven consequences of both hyper- and hypoglycemia Discuss the role and potential benefits of insulin therapy Determine the appropriate blood glucose targets for your ICU patients
3 OBJECTIVES Review the risk factors and pathophysiology involved in stress hyperglycemia Discuss the theoretical and proven consequences of both hyper- and hypoglycemia Discuss the role and potential benefits of insulin therapy Determine the appropriate blood glucose targets for your ICU patients..maybe
4 WHO NEEDS INSULIN? Diabetics Type 1 always! Type 2 if unable to control BG with oral agents DKA or HHS Patients receiving steroids sometimes Some hospitalized patients under stress Infection Trauma Surgery
5 STRESS HYPERGLYCEMIA Defined as a blood glucose > 200 mg/dl Common in critically ill medical, surgical, trauma, and burn patients Generally considered to be an appropriate and adaptive response to insult/injury However, persistent hyperglycemia and insulin resistance have been associated with increased morbidity and mortality Likely the result of a multifactorial process Xiu F, et al. International J of Endocrinology 2014 Farrokhi et al. Best Practice & Research Clinical Endocrinology & Metabolism 2011
6 CAUSES and CONSEQUENCES Farrokhi et al. Best Practice & Research Clinical Endocrinology & Metabolism 2011
7 ASSOCIATED CLINICAL OUTCOMES mortality risk of infections (surgical site, pneumonia, urinary tract) time on mechanical ventilation Polyneuropathy Skeletal muscle wasting Metabolic derangements risk of acute kidney injury need for blood transfusions lengths of stay (hospital and ICU) Ouattara et al. Anesthesia 2005 Williams et al. Neurology 2002 Pittas et al. Arch Int Med 2004 Latham et al. Infect Cont 2001 Van den Berghe et al. NEJM 2001
8 ENDOGENOUS INSULIN Peptide hormone Synthesized and secreted in the pancreas Cleaved in the b cell from pro-insulin to the active insulin peptide and C-peptide Release is stimulated by: Glucose Proteins Vagal stimulation b adrenergic stimulation

9 MECHANISM OF ACTION Primary activity of insulin is regulation of glucose metabolism Lowers blood glucose by: Stimulating peripheral glucose uptake by skeletal muscle fat Inhibiting hepatic glucose production Insulin inhibits lipolysis and proteolysis, and enhances protein synthesis
10 WHAT IS THE GOAL? Intensive Insulin Therapy historically refers to a targeting a blood glucose mg/dl
11 INTENSIVE INSULIN THERAPY Van den Berghe NEJM 2001 Van den Berghe NEJM 2006 NICE-SUGAR NEJM 2009 Population Surgical ICU Medical ICU Mixed ICU N BG Goals Intensive Conventional Intensive Conventional Intensive Conventional <180 Primary Outcome Mortality (I vs C) 4.6% vs 8%, p < 0.04 Mortality (I vs C) 37.3% vs 40%, p=0.33 Mortality (I vs C) 27.5% vs 25%, p=0.02* 10.6% vs 20.2%, p= % vs 38.1%, p=0.05 Secondary Outcomes need for dialysis, septicemia, acute kidney injury, time on ventilator, hypoglycemia, ICU length of stay, polyneuropathy, ICU length of stay time on ventilator blood transfusions
 4.6% vs 8%, p < 0.04 Mortality (I vs C) 37.3% vs 40%, p=0.33 Mortality (I vs C) 27.")
12 INTENSIVE INSULIN THERAPY Van den Berghe NEJM 2001 Van den Berghe NEJM 2006 NICE-SUGAR NEJM 2009 Population Surgical ICU Medical ICU Mixed ICU N BG Goals Intensive Conventional Intensive Conventional Intensive Conventional <180 Primary Outcome Mortality (I vs C) 4.6% vs 8%, p < 0.04 Mortality (I vs C) 37.3% vs 40%, p=0.33 Mortality (I vs C) 27.5% vs 25%, p=0.02* 10.6% vs 20.2%, p= % vs 38.1%, p=0.05 Secondary Outcomes need for dialysis, septicemia, acute kidney injury, time on ventilator, hypoglycemia, ICU length of stay, polyneuropathy, ICU length of stay time on ventilator blood transfusions
13 PRIMARY OUTCOME Mortality benefit seen primarily after 5 days of ICU care
14 SECONDARY OUTCOME VARIABLE (%) CONVENTIONAL (N=783) INTENSIVE (N=765) P VALUE ICU LOS > 14 days 15.7% 12% 0.01 Mechanical ventilation > 14 days 11.9% 7.5% Renal impairment 12.3% 9% 0.04 Dialysis or CVVH 8.2% 4.8% Hyperbilirubinemia 26% 22% 0.04 Bloodstream infection 7.8% 4.2% Antibiotics > 10 days 17.1% 11.2% < Polyneuropathy evidence 51% 28% # blood transfusions/patient 2 1 < 0.001
15 CONTROVERSIES Study population was > 60% cardiac surgery Strict protocol adherence not very practical: Arterial whole-blood samples for measurements every 1 to 4 hours Algorithm was carried out by the study physician (Van den Berghe) not involved in clinical care of the patient IV glucose ( grams/24 hr) was given continuously to all patients on Day 1 then TPN ± enteral feeds were continued thereafter Hypoglycemia (< 40 mg/dl) was observed in 39 patients (5.1%) vs. 6 patients (0.8%), no p-value reported but likely significant NO STUDY HAS BEEN ABLE TO REPRODUCE THE SAME RESULTS..
16 INTENSIVE INSULIN THERAPY Van den Berghe NEJM 2001 Van den Berghe NEJM 2006 NICE-SUGAR NEJM 2009 Population Surgical ICU Medical ICU Mixed ICU N BG Goals Intensive Conventional Intensive Conventional Intensive Conventional <180 Primary Outcome Mortality (I vs C) 4.6% vs 8%, p < 0.04 Mortality (I vs C) 37.3% vs 40%, p=0.33 Mortality (I vs C) 27.5% vs 25%, p=0.02* 10.6% vs 20.2%, p= % vs 38.1%, p=0.05 Secondary Outcomes need for dialysis, septicemia, acute kidney injury, time on ventilator, hypoglycemia, ICU length of stay, polyneuropathy, ICU length of stay time on ventilator blood transfusions
17 OUTCOMES Variable (%) Conventional (n=605) Intensive (n=595) P value Hospital mortality 40% 37.5% 0.33 ICU mortality 26% 24% day mortality 38% 36% 0.53 New kidney injury 8.9% 5.9% Bacteremia 8% 7% 0.5 Weaning from MV HR: 1.21; 95% CI,
18 SUBGROUP: ICU LOS 3 days Variable (%) Conventional (n=605) Intensive (n=595) P value Hospital mortality 52% 43% ICU mortality 38% 31% day mortality 49% 42% 0.06 New kidney injury 12.6% 8% 0.05 Bacteremia 11% 31% 0.09 Weaning from MV HR: 1.43; 95% CI,
19 CONCLUSIONS No mortality benefit in the MICU patient population Only subgroup analysis revealed mortality benefit in those who required ICU care for 3 days Earlier weaning from mechanical ventilation and less acute kidney injury were found in intensive insulin group Limitations: Many subgroup analysis, only post hoc analysis showed significance Larger patient population would be needed to show a mortality reduction with intent-to-treat analysis
20 VISEP Trial Population: 537 patients with severe sepsis Intensive goal mg/dl vs. Conventional mg/dl Primary Outcomes: 28-day mortality Morbidity (sequential organ failure dysfunction, SOFA) Safety end-point: hypoglycemia (BG< 40 mg/dl) Stopped early for safety reasons Patients getting intensive insulin therapy had: no difference in mortality (24.7 vs. 26%) or SOFA score (7.8 vs. 7.7) but increased risk of hypoglycemia (17 vs. 4%) Brunkhorst, et al. NEJM 2008
21 GLUCONTROL Population: 1078 mixed med-surgical ICU patients Intensive goal mg/dl vs. Conventional mg/dl Stopped early due to protocol violations Lack of clinical benefit and increased risk of severe hypoglycemia Severe hypoglycemia (BG<40 mg/dl) more frequent in tight group (8.6 vs. 4%) No difference in mortality (18.7 vs. 15.3%) Preiser, et al. Intensive Care Med 2009
22 INTENSIVE INSULIN THERAPY Van den Berghe NEJM 2001 Van den Berghe NEJM 2006 NICE-SUGAR NEJM 2009 Population Surgical ICU Medical ICU Mixed ICU N BG Goals Intensive Conventional Intensive Conventional Intensive Conventional <180 Primary Outcome Mortality (I vs C) 4.6% vs 8%, p < 0.04 Mortality (I vs C) 37.3% vs 40%, p=0.33 Mortality (I vs C) 27.5% vs 25%, p=0.02* 10.6% vs 20.2%, p= % vs 38.1%, p=0.05 Secondary Outcomes need for dialysis, septicemia, acute kidney injury, time on ventilator, hypoglycemia, ICU length of stay, polyneuropathy, ICU length of stay time on ventilator blood transfusions
23 BASELINE CHARACTERISTICS Characteristic Conventional (n=3050) Intensive (n=3054) Operative admission 37.2% 36.9% Emergent surgery 59.9% 61.3% Trauma 37.9% 41.6% APACHE II score (mean) APACHE II score 25 (%) 31.4% 30.8% Severe sepsis (%) 20.8% 22.4% History of diabetes (%) 19% 20% Mean Admission BG (mg/dl)

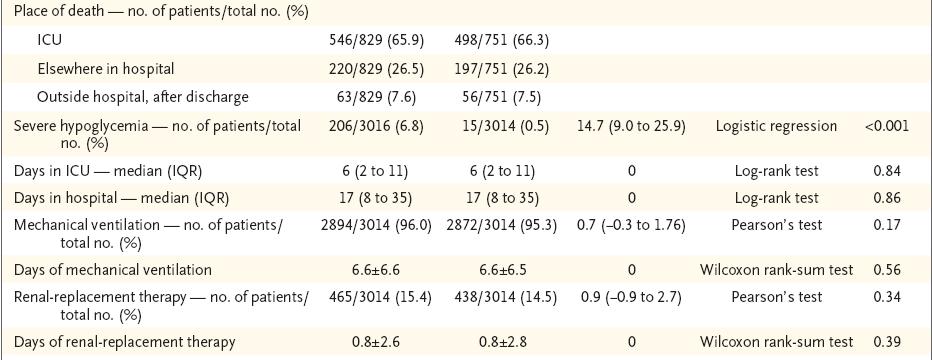
24 OUTCOMES
25 90-DAY MORTALITY
26 CONCLUSIONS Conventional glucose control had an absolute reduction in mortality at 90 days of 2.6% vs. intensive insulin control Severe hypoglycemia (<40mg/dL) was significantly reduced in the conventional control group 6.8% to 0.5% Morbidity and complications associated with ICU care were not reduced by intensive glucose control Authors recommend against the use of intensive insulin control in critically ill
27 WHAT IS THE GOAL? Tight Glycemic Control historically refers to a targeting a blood glucose mg/dl Current recommendations lean towards < 180
28 WHAT IS THE GOAL? Tight Glycemic Control historically refers to a targeting a blood glucose mg/dl Current recommendations lean towards < 180 Is there still evidence for tighter control?
29 Scalea et al. TRAUMA PATIENTS Population: 2129 trauma ICU patients Evaluated a patients before and after protocol implementation that targeted goal glucose mg/dl Tight glycemic control significantly: infection rate (29% to 21%) ventilator days (17 to 15) length of stay (24 to 21) mortality (14% to 10%) Scalea et al. Ann Surg 2007

30 TRAUMA PATIENTS Sperry et al. Multicenter implementation of intensive insulin protocol Average maximum daily glucose values from post-injury day #2-5 Stratified outcomes by glucose level: Sperry et al. J Trauma 2009
31 NICE-SUGAR SUBGROUPS
32 NICE-SUGAR SUBGROUPS
33 BURN PATIENTS Hemmila, et al. 152 burn ICU patients Goal mg/dl vs. historical control Patients with a maximum glucose > 140 mg/dl had significantly higher risk of infection (OR 11.3, 95% CI 4-32, p < 0.01) Pneumonia and urinary tract most common infections No difference in mortality Unable to determine if BG control would prevent infection or if BG > 140 was a sign of infection Hemmila, et al. Surgery 2008
34 BURN PATIENTS Murphy, et al. 46 burn ICU patients Goal 150 mg/dl for at least 2 consecutive days by postburn day #3 (n=26) Failure of early glycemic control was associated with higher mortality HR 6.8, 95% CI , p = 0.03 Adjustments for age, TBSA, and inhalational injury Murphy, et al. J Burn Care Res 2011
35 BRAIN INJURY Hyperglycemia strongly associated with increased mortality and worse functional outcome following: Ischemic stroke Intraparenchymal hemorrhage Aneurysmal subarachnoid hemorrhage Traumatic brain injury In patients with ischemic stroke, those who are responsive to insulin therapy have a better prognosis Kruyt, et al. Stroke 2009 Rovlias, et al. Neurosurgery 2000 Fogelholm, et al. J Neurol Neurosurg Psychiatr 2005 Garg, et al. Stroke2006 Capes, et al. Stroke 2001 Gentile, et al. Acad Emerg Med 2006

36 BRAIN INJURY Jacobi, et al. Crit Care Med 2012
37 WHAT IS THE GOAL? Tight Glycemic Control historically refers to a targeting a blood glucose mg/dl Current recommendations lean towards < 180 Is there still evidence for tighter control? Is absolute blood glucose the right target?
38 GLUCOSE VARIABILITY Lanspa, et al. Population: 6101 critically ill adults Electronic protocol for managing insulin Co-efficient of variation independently associated with 30-day mortality OR 1.23 for every 10% increase, p < In non-diabetics: OR 1.37 Lanspa, et al. Critical Care 2014

39 DYSGLYCEMIA and MORTALITY Badawi, et al. Criti Care Med 2012

40 DYSGLYCEMIA and MORTALITY Badawi, et al. Criti Care Med 2012
41 HYPOGLYCEMIA Signs and Symptoms Mild Cold clammy skin Palpitations Tremulous/ weak Sweaty Confused Mood/Personality Change Severe Unresponsiveness Convulsions Coma Death A single incident decreases outcomes in TBI patients Risk factor for cardiovascular events in diabetic patients Can result in agitation, altered mental status, seizures, and death if not corrected

42 NICE-SUGAR HYPOGLYCEMIA
43 WHAT IS THE GOAL? Tight Glycemic Control historically refers to a targeting a blood glucose mg/dl Current recommendations lean towards < 180 Is there still evidence for tighter control? Is absolute blood glucose the right target? DEFINITELY < 180 mg/dl for all critically ill patients
44 WHAT IS THE GOAL? Tight Glycemic Control historically refers to a targeting a blood glucose mg/dl Current recommendations lean towards < 180 Is there still evidence for tighter control? Is absolute blood glucose the right target? PROBABLY < 150 mg/dl for CERTAIN populations especially within surgery
45 WHAT IS THE GOAL? Tight Glycemic Control historically refers to a targeting a blood glucose mg/dl Current recommendations lean towards < 180 Is there still evidence for tighter control? Is absolute blood glucose the right target? NEVER < 110 mg/dl for all critically ill patients
46 WHAT IS THE GOAL? Tight Glycemic Control historically refers to a targeting a blood glucose mg/dl Current recommendations lean towards < 180 Is there still evidence for tighter control? Is absolute blood glucose the right target? AVOID large swings in blood glucose
47 QUESTIONS?
48 SOMETHING TO PONDER. Early mobilization decreased insulin requirements 0.07 units/kg/day vs. 0.2 units/kg/day, p< with similar median blood glucoses vs mg/dl
Controversies in Hospital Medicine: Critical Care. Vasopressors, Steroids, and Insulin Therapy
 Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Control of Blood Glucose in the ICU: Reconciling the Conflicting Data
 Control of Blood Glucose in the ICU: Reconciling the Conflicting Data Steven E. Nissen MD Disclosure Consulting: Many pharmaceutical companies Clinical Trials: AbbVie, Amgen, Astra Zeneca, Esperion, Eli
Control of Blood Glucose in the ICU: Reconciling the Conflicting Data Steven E. Nissen MD Disclosure Consulting: Many pharmaceutical companies Clinical Trials: AbbVie, Amgen, Astra Zeneca, Esperion, Eli
Deepika Reddy MD Department of Endocrinology
 Deepika Reddy MD Department of Endocrinology Management of hyperglycemic crisis Review need for inpatient glycemic control Brief overview of relevant trials Case based review of diabetes management strategies/review
Deepika Reddy MD Department of Endocrinology Management of hyperglycemic crisis Review need for inpatient glycemic control Brief overview of relevant trials Case based review of diabetes management strategies/review
 C CONFERENCIAS MAGISTRALES Vol. 36. Supl. 1 Abril-Junio 2013 pp S61-S68 Management of hyperglycemia in the perioperative patient. 39 th Annual Refresher Course on Anesthesiology and Perioperative Medicine,
C CONFERENCIAS MAGISTRALES Vol. 36. Supl. 1 Abril-Junio 2013 pp S61-S68 Management of hyperglycemia in the perioperative patient. 39 th Annual Refresher Course on Anesthesiology and Perioperative Medicine,
VANDERBILT UNIVERSITY MEDICAL CENTER MULTIDISCIPLINARY SURGICAL CRITICAL CARE TRAUMA INTENSIVE CARE UNIT GLYCEMIC CONTROL PROTOCOL
 VANDERBILT UNIVERSITY MEDICAL CENTER MULTIDISCIPLINARY SURGICAL CRITICAL CARE TRAUMA INTENSIVE CARE UNIT GLYCEMIC CONTROL PROTOCOL Background: For some time, the presence of diabetes and hyperglycemia
VANDERBILT UNIVERSITY MEDICAL CENTER MULTIDISCIPLINARY SURGICAL CRITICAL CARE TRAUMA INTENSIVE CARE UNIT GLYCEMIC CONTROL PROTOCOL Background: For some time, the presence of diabetes and hyperglycemia
Disclosures. Glycemic Control in the Intensive Care Unit. Objectives. Hyperglycemia. Hyperglycemia. History. No disclosures
 Disclosures Glycemic Control in the Intensive Care Unit No disclosures Jorie Frasiolas, Pharm.D., BCPS Clinical Pharmacy Manager, CTICU NewYork-Presbyterian Hospital Columbia University Medical Center
Disclosures Glycemic Control in the Intensive Care Unit No disclosures Jorie Frasiolas, Pharm.D., BCPS Clinical Pharmacy Manager, CTICU NewYork-Presbyterian Hospital Columbia University Medical Center
123 Are You Providing Evidence-Based Diabetes Care? - Martin
 Donna Martin, DNP, RN, CDE, CMSRN Lewis University Learner will be able to: Identify current inpatient standards of care for patients with diabetes Describe causes of hyperglycemia / hypoglycemia in the
Donna Martin, DNP, RN, CDE, CMSRN Lewis University Learner will be able to: Identify current inpatient standards of care for patients with diabetes Describe causes of hyperglycemia / hypoglycemia in the
Endocrine and Metabolic Complications in the ICU
 Endocrine and Metabolic Complications in the ICU Linda Liu, M.D. Associate Professor UCSF Department of Anesthesia UC SF 1 New Progress Discovery of complex neuro-endocrine adaptation to critical illness
Endocrine and Metabolic Complications in the ICU Linda Liu, M.D. Associate Professor UCSF Department of Anesthesia UC SF 1 New Progress Discovery of complex neuro-endocrine adaptation to critical illness
Glucose Management in the ICU: The Role of the Pharmacist
 Objectives Glucose Management in the ICU: The Role of the Pharmacist James Gilmore PharmD, BCPS Senior Pharmacist- Surgical Intensive Care Unit Brigham and Women s Hospital Boston, MA Evaluate primary
Objectives Glucose Management in the ICU: The Role of the Pharmacist James Gilmore PharmD, BCPS Senior Pharmacist- Surgical Intensive Care Unit Brigham and Women s Hospital Boston, MA Evaluate primary
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS
 GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS David Zygun MD MSc FRCPC Professor and Director Division of Critical Care Medicine University of Alberta Zone Clinical Department Head Critical Care Medicine,
GLYCEMIC CONTROL IN NEUROCRITICAL CARE PATIENTS David Zygun MD MSc FRCPC Professor and Director Division of Critical Care Medicine University of Alberta Zone Clinical Department Head Critical Care Medicine,
Journal Club ICU
 Journal Club 2018.9.4 ICU Crit Care Med. 2018 Aug;46(8):1224-1229 Introduction Stress hyperglycemia SH SH >124 mg/dl or >200 mg/dl Lancet 2009;373:1798. stress hyperglycemia Lancet 2009;373:1798. SH Critical
Journal Club 2018.9.4 ICU Crit Care Med. 2018 Aug;46(8):1224-1229 Introduction Stress hyperglycemia SH SH >124 mg/dl or >200 mg/dl Lancet 2009;373:1798. stress hyperglycemia Lancet 2009;373:1798. SH Critical
What Should Be the Therapeutic Glycemic Target in Intensive Care Units?
 What Should Be the Therapeutic Glycemic Target in Intensive Care Units? Irl B. Hirsch, M.D. Professor of Medicine University of Washington School of Medicine Disclosures Research/Grants: Sanofi, Halozyme
What Should Be the Therapeutic Glycemic Target in Intensive Care Units? Irl B. Hirsch, M.D. Professor of Medicine University of Washington School of Medicine Disclosures Research/Grants: Sanofi, Halozyme
ESPEN Congress Madrid 2018
 ESPEN Congress Madrid 2018 Dysglycaemia In Acute Patients With Nutritional Therapy Mechanisms And Consequences Of Dysglycaemia In Patients Receiving Nutritional Therapy M. León- Sanz (ES) Mechanisms and
ESPEN Congress Madrid 2018 Dysglycaemia In Acute Patients With Nutritional Therapy Mechanisms And Consequences Of Dysglycaemia In Patients Receiving Nutritional Therapy M. León- Sanz (ES) Mechanisms and
10.4.a. Optimal glucose control: Insulin therapy March 2013
 10.4.a. Optimal glucose control: Insulin therapy March 2013 2013 Recommendation: Based on 26 level 2 studies, we recommend that hyperglycemia (blood sugars > 10 mmol/l) be avoided in all critically ill
10.4.a. Optimal glucose control: Insulin therapy March 2013 2013 Recommendation: Based on 26 level 2 studies, we recommend that hyperglycemia (blood sugars > 10 mmol/l) be avoided in all critically ill
Insulin sensitivity, its variability and glycaemic outcome:
 MCBMS 2009 Insulin sensitivity, its variability and glycaemic outcome: A model-based analysis of the difficulty in achieving tight glycaemic control in critical care JG Chase et al Dept of Mechanical Engineering
MCBMS 2009 Insulin sensitivity, its variability and glycaemic outcome: A model-based analysis of the difficulty in achieving tight glycaemic control in critical care JG Chase et al Dept of Mechanical Engineering
Inpatient Management of Diabetes Mellitus. Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy
 Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
Brain dysfunction in the ICU
 High cortisol levels are associated with brain dysfunction but low prolactin cortisol ratio levels are associated with nosocomial infection in severe sepsis Duc Nam Nguyen Luc Huyghens Johan Schiettecatte
High cortisol levels are associated with brain dysfunction but low prolactin cortisol ratio levels are associated with nosocomial infection in severe sepsis Duc Nam Nguyen Luc Huyghens Johan Schiettecatte
Postoperative Glucose Control and SCIP Measures. Gorav Ailawadi, MD Chief, Adult Cardiac Surgery University of Virginia April 25, 2015
 Postoperative Glucose Control and SCIP Measures Gorav Ailawadi, MD Chief, Adult Cardiac Surgery University of Virginia April 25, 2015 Diabetes in CABG Incidence of Diabetes in cardiac surgery increased
Postoperative Glucose Control and SCIP Measures Gorav Ailawadi, MD Chief, Adult Cardiac Surgery University of Virginia April 25, 2015 Diabetes in CABG Incidence of Diabetes in cardiac surgery increased
ESPEN Congress Lisbon Water and electrolytes. Hyperglycemia management. G Van Den Berghe
 ESPEN Congress Lisbon 2004 Water and electrolytes Hyperglycemia management G Van Den Berghe Intensive Insulin Therapy in ICU G. Van den Berghe M.D., Ph.D. Department of Intensive Care Medicine University
ESPEN Congress Lisbon 2004 Water and electrolytes Hyperglycemia management G Van Den Berghe Intensive Insulin Therapy in ICU G. Van den Berghe M.D., Ph.D. Department of Intensive Care Medicine University
Glycemic Control Insulin In The Hospital Setting
 Glycemic Control Insulin In The Hospital Setting Glycemic Control The Evidence For Insulin s s Benefit The Mechanism of Insulin s s Benefit The Achievement of Insulin s s Benefit A Few Cases Hyperglycemia
Glycemic Control Insulin In The Hospital Setting Glycemic Control The Evidence For Insulin s s Benefit The Mechanism of Insulin s s Benefit The Achievement of Insulin s s Benefit A Few Cases Hyperglycemia
Intensive Insulin in the Intensive Care Unit
 TABLE OF CONTENTS Introduction to Intensive Insulin in Adult Critical Care Patients - UIMCC Guideline for Insulin Infusion in Adult ICU Patients - P&T Committee Formulary Action Intensive Insulin in the
TABLE OF CONTENTS Introduction to Intensive Insulin in Adult Critical Care Patients - UIMCC Guideline for Insulin Infusion in Adult ICU Patients - P&T Committee Formulary Action Intensive Insulin in the
Peri-operative Glucose Control Is it Important?
 Peri-operative Glucose Control Is it Important? Dr Ketan Dhatariya MSc MD MS FRCP Consultant in Diabetes and Endocrinology Norfolk and Norwich University Hospitals Do Peri-Operative High Glucose Levels
Peri-operative Glucose Control Is it Important? Dr Ketan Dhatariya MSc MD MS FRCP Consultant in Diabetes and Endocrinology Norfolk and Norwich University Hospitals Do Peri-Operative High Glucose Levels
BETA BLOCKADE: IT S NOT JUST FOR CARDIOLOGY PATIENTS
 BETA BLOCKADE: IT S NOT JUST FOR CARDIOLOGY PATIENTS Sympathetic Receptors Agonists Kristan Staudenmayer, M.D. M.S. Assistant Professor of Surgery Stanford University May 31, 2012 Antagonists Beta Blockade
BETA BLOCKADE: IT S NOT JUST FOR CARDIOLOGY PATIENTS Sympathetic Receptors Agonists Kristan Staudenmayer, M.D. M.S. Assistant Professor of Surgery Stanford University May 31, 2012 Antagonists Beta Blockade
When to start SPN in critically ill patients? Refereeravond IC
 When to start SPN in critically ill patients? Refereeravond IC Introduction (1) Protein/calorie malnutrition is very frequent in critically ill patients Protein/calorie malnutrition is associated with
When to start SPN in critically ill patients? Refereeravond IC Introduction (1) Protein/calorie malnutrition is very frequent in critically ill patients Protein/calorie malnutrition is associated with
What other beneficial effects might GLN exert in critical illness??
 What other beneficial effects might GLN exert in critical illness?? Prevention of Enhanced Gut Permeability Who believes bacteria translocate from the gut to blood and cause infection? Yes No Bacteria
What other beneficial effects might GLN exert in critical illness?? Prevention of Enhanced Gut Permeability Who believes bacteria translocate from the gut to blood and cause infection? Yes No Bacteria
MANAGEMENT OF HYPERGLYCEMIA IN CRITICALLY ILL SURGICAL (NON-CARDIAC) PATIENTS
 PATIENTS") DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Parenterale voeding tijdens kritieke ziekte: bijkomende analyses van de EPaNIC studie
 Parenterale voeding tijdens kritieke ziekte: bijkomende analyses van de EPaNIC studie Namens alle auteurs Michaël P. Casaer M.D. Department of Intensive Care Medicine University Hospital Gasthuisberg Catholic
Parenterale voeding tijdens kritieke ziekte: bijkomende analyses van de EPaNIC studie Namens alle auteurs Michaël P. Casaer M.D. Department of Intensive Care Medicine University Hospital Gasthuisberg Catholic
In - Hospital Diabetes Care. A review and personal experience
 In - Hospital Diabetes Care A review and personal experience Hyperglycemia in the Hospital The Problem Hospitalizations with Diabetes http://www.cdc.gov/diabetes/statistics/dmany/fig1.htm Prevalence of
In - Hospital Diabetes Care A review and personal experience Hyperglycemia in the Hospital The Problem Hospitalizations with Diabetes http://www.cdc.gov/diabetes/statistics/dmany/fig1.htm Prevalence of
Inpatient Diabetes Management: The Slippery Slope of Sliding Scale Insulin
 Inpatient Diabetes Management: The Slippery Slope of Sliding Scale Insulin David Newman, MD University of North Dakota School of Medicine Sanford Health Big Sky Conference 2017 Dr. David Newman, Personal/Professional
Inpatient Diabetes Management: The Slippery Slope of Sliding Scale Insulin David Newman, MD University of North Dakota School of Medicine Sanford Health Big Sky Conference 2017 Dr. David Newman, Personal/Professional
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE
 CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
Extubation Failure & Delay in Brain-Injured Patients
 Extubation Failure & Delay in Brain-Injured Patients Niall D. Ferguson, MD, FRCPC, MSc Director, Critical Care Medicine University Health Network & Mount Sinai Hospital Associate Professor of Medicine
Extubation Failure & Delay in Brain-Injured Patients Niall D. Ferguson, MD, FRCPC, MSc Director, Critical Care Medicine University Health Network & Mount Sinai Hospital Associate Professor of Medicine
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Augmented Renal Clearance: Let s Get the Discussion Flowing
 Augmented Renal Clearance: Let s Get the Discussion Flowing Terry Makhoul, PharmD PGY-2 Emergency Medicine Pharmacy Resident University of Rochester Medical Center Strong Memorial Hospital Disclosures
Augmented Renal Clearance: Let s Get the Discussion Flowing Terry Makhoul, PharmD PGY-2 Emergency Medicine Pharmacy Resident University of Rochester Medical Center Strong Memorial Hospital Disclosures
Is Intense Glycemic Control Really Better?
 University of Wyoming Wyoming Scholars Repository Honors Theses AY 16/17 Undergraduate Honors Theses Spring 5-12-2017 Is Intense Glycemic Control Really Better? Cierra W. Schutzman University of Wyoming,
University of Wyoming Wyoming Scholars Repository Honors Theses AY 16/17 Undergraduate Honors Theses Spring 5-12-2017 Is Intense Glycemic Control Really Better? Cierra W. Schutzman University of Wyoming,
Nutrition Support in Critically Ill Cardiothoracic Patients
 Nutrition Support in Critically Ill Cardiothoracic Patients อ.นพ.พรพจน เปรมโยธ น สาชาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล Outline Malnutrition in cardiothoracic patients Nutritional
Nutrition Support in Critically Ill Cardiothoracic Patients อ.นพ.พรพจน เปรมโยธ น สาชาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล Outline Malnutrition in cardiothoracic patients Nutritional
Fluid Treatments in Sepsis: Meta-Analyses
 Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
A Children s Bedtime Story
 A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
and ICU - an update Michal Horácek
 Glycemic control in perioperative period and ICU - an update Michal Horácek 73 The three Leuwen studies (1-3), especially the first one published in 2001 (1), caused a revolution in the approach to glucose
Glycemic control in perioperative period and ICU - an update Michal Horácek 73 The three Leuwen studies (1-3), especially the first one published in 2001 (1), caused a revolution in the approach to glucose
Hyperglycemia is common among medical and surgical. Clinical Guideline
 Clinical Guideline Annals of Internal Medicine Intensive Insulin Therapy in Hospitalized Patients: A Systematic Review Devan Kansagara, MD, MCR; Rongwei Fu, PhD; Michele Freeman, MPH; Fawn Wolf, MD; and
Clinical Guideline Annals of Internal Medicine Intensive Insulin Therapy in Hospitalized Patients: A Systematic Review Devan Kansagara, MD, MCR; Rongwei Fu, PhD; Michele Freeman, MPH; Fawn Wolf, MD; and
Supplement Table 1. Definitions for Causes of Death
 Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
Relationship between glucose meter error and glycemic control efficacy
 Relationship between glucose meter error and glycemic control efficacy Brad S. Karon, M.D., Ph.D. Professor of Laboratory Medicine and Pathology Department of Laboratory Medicine and Pathology Mayo Clinic
Relationship between glucose meter error and glycemic control efficacy Brad S. Karon, M.D., Ph.D. Professor of Laboratory Medicine and Pathology Department of Laboratory Medicine and Pathology Mayo Clinic
Endocrinology Emergencies & Glycemic Control in the ICU
 Endocrinology Emergencies & Glycemic Control in the ICU Mark Franklin, MD Dartmouth-Hitchcock Medical Center - Lebanon, NH Avera Health eicu - Sioux Falls, SD Objectives Recognize and understand the treatment
Endocrinology Emergencies & Glycemic Control in the ICU Mark Franklin, MD Dartmouth-Hitchcock Medical Center - Lebanon, NH Avera Health eicu - Sioux Falls, SD Objectives Recognize and understand the treatment
Timing of Parenteral Nutrition
 Timing of Parenteral Nutrition Arun Bansal; MD, FCCM, MRCPCH Professor Pediatric Critical Care PGIMER, Chandigarh, INDIA drarunbansal@gmail.com Malnutrition in Critically Ill Incidence: from 19 32% Associated
Timing of Parenteral Nutrition Arun Bansal; MD, FCCM, MRCPCH Professor Pediatric Critical Care PGIMER, Chandigarh, INDIA drarunbansal@gmail.com Malnutrition in Critically Ill Incidence: from 19 32% Associated
Lung Day University of Washington. June 17, Translating Data Into Practice in the MICU. Richard K. Albert, M.D.
 Lung Day 2011 University of Washington June 17, 2011 Translating Data Into Practice in the MICU Richard K. Albert, M.D. Chief of Medicine Denver Health Professor of Medicine University of Colorado Adjunct
Lung Day 2011 University of Washington June 17, 2011 Translating Data Into Practice in the MICU Richard K. Albert, M.D. Chief of Medicine Denver Health Professor of Medicine University of Colorado Adjunct
Hyperglycemia occurs frequently in critically ill patients.
 Mayo Clin Proc, December 2003, Vol 78 Hyperglycemia and Increased Hospital Mortality 1471 Original Article Association Between Hyperglycemia and Increased Hospital Mortality in a Heterogeneous Population
Mayo Clin Proc, December 2003, Vol 78 Hyperglycemia and Increased Hospital Mortality 1471 Original Article Association Between Hyperglycemia and Increased Hospital Mortality in a Heterogeneous Population
By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital
 MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital") By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital Introduction The significance of nutrition in hospital setting (especially the ICU) cannot be overstated.
By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital Introduction The significance of nutrition in hospital setting (especially the ICU) cannot be overstated.
Transfusion & Mortality. Philippe Van der Linden MD, PhD
 Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
[No conflicts of interest]
![[No conflicts of interest]](/thumbs/86/94144068.jpg "[No conflicts of interest]") [No conflicts of interest] Patients and staff at: Available evidence pre-calories Three meta-analyses: Gramlich L et al. Does enteral nutrition compared to parenteral nutrition result in better outcomes
[No conflicts of interest] Patients and staff at: Available evidence pre-calories Three meta-analyses: Gramlich L et al. Does enteral nutrition compared to parenteral nutrition result in better outcomes
Top 5 (Topics) Papers In GIM Rocky Mountain ACP Internal Medicine Meeting Raj Padwal November 13, 2008
 Papers In GIM Rocky Mountain ACP Internal Medicine Meeting Raj Padwal November 13, 2008") Top 5 (Topics) Papers In GIM 2008 Rocky Mountain ACP Internal Medicine Meeting Raj Padwal November 13, 2008 Methods Searched ACPJC/EBM, TOC of top medical journals, MEDSCAPE Best Evidence, consultation
Top 5 (Topics) Papers In GIM 2008 Rocky Mountain ACP Internal Medicine Meeting Raj Padwal November 13, 2008 Methods Searched ACPJC/EBM, TOC of top medical journals, MEDSCAPE Best Evidence, consultation
Outcomes after administration of drotrecogin alfa in patients with severe sepsis at an urban safety net hospital.
 Outcomes after administration of drotrecogin alfa in patients with severe sepsis at an urban safety net hospital. Aryan J. Rahbar, University Medical Center of Southern Nevada Marina Rabinovich, Emory
Outcomes after administration of drotrecogin alfa in patients with severe sepsis at an urban safety net hospital. Aryan J. Rahbar, University Medical Center of Southern Nevada Marina Rabinovich, Emory
The Use of Metabolic Resuscitation in Sepsis
 The Use of Metabolic Resuscitation in Sepsis Jennifer M. Roth, PharmD, BCPS, BCCCP Critical Care Clinical Specialist - Surgical Trauma ICU Baylor University Medical Center Disclosures No conflicts of interest
The Use of Metabolic Resuscitation in Sepsis Jennifer M. Roth, PharmD, BCPS, BCCCP Critical Care Clinical Specialist - Surgical Trauma ICU Baylor University Medical Center Disclosures No conflicts of interest
Parenteral Nutrition The Sweet and Sour Truth. From: Division of Endocrinology, Diabetes and Bone Disease Icahn School of Medicine at Mount Sinai
 ENDOCRINE PRACTICE Rapid Electronic Article in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited, typeset
ENDOCRINE PRACTICE Rapid Electronic Article in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited, typeset
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Insulin therapy protects the central and peripheral nervous system of intensive care patients
 protects the central and peripheral nervous system of intensive care patients G. Van den Berghe, MD, PhD; K. Schoonheydt, MD; P. Becx, MD; F. Bruyninckx, MD; and P.J. Wouters, MSc Abstract Objective: To
protects the central and peripheral nervous system of intensive care patients G. Van den Berghe, MD, PhD; K. Schoonheydt, MD; P. Becx, MD; F. Bruyninckx, MD; and P.J. Wouters, MSc Abstract Objective: To
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley
 Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley British Journal of Surgery 2013; 100: 1045 1049 The risk of 30 day mortality
Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley British Journal of Surgery 2013; 100: 1045 1049 The risk of 30 day mortality
Guidelines and Beyond: Traumatic Brain Injury
 Guidelines and Beyond: Traumatic Brain Injury Aimee Gowler, PharmD, BCCCP, BCPS Neuromedicine Critical Care Clinical Pharmacy Specialist UF Health Shands Disclosures I have no financial interests to disclose.
Guidelines and Beyond: Traumatic Brain Injury Aimee Gowler, PharmD, BCCCP, BCPS Neuromedicine Critical Care Clinical Pharmacy Specialist UF Health Shands Disclosures I have no financial interests to disclose.
The impact of metoprolol on insulin sensitivity in the ICU
 MCBMS 2009 The impact of metoprolol on insulin sensitivity in the ICU JG Chase et al Dept of Mechanical Engineering Centre for Bio-Engineering University of Canterbury New Zealand Introduction Why do we
MCBMS 2009 The impact of metoprolol on insulin sensitivity in the ICU JG Chase et al Dept of Mechanical Engineering Centre for Bio-Engineering University of Canterbury New Zealand Introduction Why do we
What is the Role of Albumin in Sepsis? An Evidenced Based Affair. Justin Belsky MD PGY3 2/6/14
 What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
VUMC Multidisciplinary Surgical Critical Care
 VUMC Multidisciplinary Surgical Critical Care Gastrointestinal Stress Ulcer Prophylaxis Guideline: Background: Work by Cooke and colleagues ascribed the risk of overt bleeding to be 4.4% and clinically
VUMC Multidisciplinary Surgical Critical Care Gastrointestinal Stress Ulcer Prophylaxis Guideline: Background: Work by Cooke and colleagues ascribed the risk of overt bleeding to be 4.4% and clinically
Usefulness of Procalcitonin in the management of Infections in ICU. P Damas CHU Sart Tilman Liège
 Usefulness of Procalcitonin in the management of Infections in ICU P Damas CHU Sart Tilman Liège Procalcitonin Peptide 116 AA Produced by parenchymal cells during «sepsis»: IL1, TNF, IL6 : stimulators
Usefulness of Procalcitonin in the management of Infections in ICU P Damas CHU Sart Tilman Liège Procalcitonin Peptide 116 AA Produced by parenchymal cells during «sepsis»: IL1, TNF, IL6 : stimulators
4.2a Composition of Enteral Nutrition: (Carbohydrate/fat): High fat/low CHO March 2013
: High fat/low CHO March 2013") 4.2a Composition of Enteral Nutrition: (Carbohydrate/fat): March 203 There were no new randomized controlled trials since the 2009 update and hence there are no changes to the following Summary of Evidence.
4.2a Composition of Enteral Nutrition: (Carbohydrate/fat): March 203 There were no new randomized controlled trials since the 2009 update and hence there are no changes to the following Summary of Evidence.
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
SEPSIS 2015 DISCLOSURES FINANCIAL DISCLOSURES 9/1/2015. William M. Johnson, MD Nebraska Pulmonary Specialties. William Johnson
 SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
5/15/2018. Reduced Platelet Activity
 ASSOCIATION OF DESMOPRESSIN ACETATE ON OUTCOMES IN ACUTE INTRACRANIAL HEMORRHAGE IN PATIENTS ON ANTIPLATELET THERAPY Jessica McManus, Pharm. D. PGY2 Critical Care Pharmacy Resident UF Health Jacksonville
ASSOCIATION OF DESMOPRESSIN ACETATE ON OUTCOMES IN ACUTE INTRACRANIAL HEMORRHAGE IN PATIENTS ON ANTIPLATELET THERAPY Jessica McManus, Pharm. D. PGY2 Critical Care Pharmacy Resident UF Health Jacksonville
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: The National Heart, Lung, and Blood Institute Acute Respiratory
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: The National Heart, Lung, and Blood Institute Acute Respiratory
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Glycemic control has become a growing trend
 72 Performance Improvement Measures in Achieving Glycemic Control in the Acute Brain Injury Population Megan T. Moyer ABSTRACT Glycemic control is becoming a standard practice in the intensive care environment
72 Performance Improvement Measures in Achieving Glycemic Control in the Acute Brain Injury Population Megan T. Moyer ABSTRACT Glycemic control is becoming a standard practice in the intensive care environment
Disclosures. Objectives. Procalcitonin: Pearls and Pitfalls in Daily Practice
 Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Do PPIs Reduce Bleeding in ICU? Revisiting Stress Ulcer Prophylaxis. Deborah Cook
 Do PPIs Reduce Bleeding in ICU? Revisiting Stress Ulcer Prophylaxis Deborah Cook ICU-Acquired Upper GI Bleeding Case series of 300 ICU patients describing stressrelated erosive syndrome Frequent Fatal
Do PPIs Reduce Bleeding in ICU? Revisiting Stress Ulcer Prophylaxis Deborah Cook ICU-Acquired Upper GI Bleeding Case series of 300 ICU patients describing stressrelated erosive syndrome Frequent Fatal
Therapeutic Effect of Insulin in Reducing Critical Illness; Polyneuropathy and Myopathy in the Pediatric Intensive Care Unit
 original ARTICLE Therapeutic Effect of Insulin in Reducing Critical Illness; Polyneuropathy and Myopathy in the Pediatric Intensive Care Unit How to Cite this Article: Bilan N, Sadegvand, Ranjbar Sh. Therapeutic
original ARTICLE Therapeutic Effect of Insulin in Reducing Critical Illness; Polyneuropathy and Myopathy in the Pediatric Intensive Care Unit How to Cite this Article: Bilan N, Sadegvand, Ranjbar Sh. Therapeutic
Diabetes: Inpatient Glucose control
 Diabetes: Inpatient Glucose control Leanne Current, PharmD, BCPS This activity is funded through the Medicaid section 1115(a) Demonstration Texas Healthcare Transformation and Quality Improvement Program
Diabetes: Inpatient Glucose control Leanne Current, PharmD, BCPS This activity is funded through the Medicaid section 1115(a) Demonstration Texas Healthcare Transformation and Quality Improvement Program
Nutritional Demands of Disease and Trauma
 al Demands of Disease and Trauma Lecture 89 Medical School al Requirements Based on needs to support optimal physiological function Are changed by disease or injury metabolism is altered to prevent further
al Demands of Disease and Trauma Lecture 89 Medical School al Requirements Based on needs to support optimal physiological function Are changed by disease or injury metabolism is altered to prevent further
Transfusion for the sickest ICU patients: Are there unanswered questions?
 Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
Steroid in Paediatric Sepsis. Dr Pon Kah Min Hospital Pulau Pinang
 Steroid in Paediatric Sepsis Dr Pon Kah Min Hospital Pulau Pinang Contents Importance of steroid in sepsis Literature Review for adult studies Literature Review for paediatric studies Conclusions. Rationale
Steroid in Paediatric Sepsis Dr Pon Kah Min Hospital Pulau Pinang Contents Importance of steroid in sepsis Literature Review for adult studies Literature Review for paediatric studies Conclusions. Rationale
Implementing Glucose Control in 2009 and Beyond: Changes in Patterns and Perceptions
 Implementing Glucose Control in 2009 and Beyond: Changes in Patterns and Perceptions Charles C. Reed MSN, RN, CNRN Patient Care Coordinator Surgical Trauma ICU University Hospital San Antonio, Texas Relationships
Implementing Glucose Control in 2009 and Beyond: Changes in Patterns and Perceptions Charles C. Reed MSN, RN, CNRN Patient Care Coordinator Surgical Trauma ICU University Hospital San Antonio, Texas Relationships
Hypoglycemia in congenital hyperinsulinism
 How a normal body works: Our body is constantly at work. Our cells need a source of energy, and this source of energy is called glucose. The process is quite simple; think of it like an assembly line.
How a normal body works: Our body is constantly at work. Our cells need a source of energy, and this source of energy is called glucose. The process is quite simple; think of it like an assembly line.
Basic pathophysiology of recovery: the role of endocrine metabolic response. Franco Carli McGill University Montreal, Canada
 Basic pathophysiology of recovery: the role of endocrine metabolic response Franco Carli McGill University Montreal, Canada ASER, Washington, 2016 postoperative recovery, 1950 Loss of body weight, less
Basic pathophysiology of recovery: the role of endocrine metabolic response Franco Carli McGill University Montreal, Canada ASER, Washington, 2016 postoperative recovery, 1950 Loss of body weight, less
Let s not sugar coat it: Promoting excellence in glucose control in hospitalized and perioperative patients WELCOME!
 Let s not sugar coat it: Promoting excellence in glucose control in hospitalized and perioperative patients WELCOME! 1. Evaluate the evidence for variable glycemic control for patients in the hospital
Let s not sugar coat it: Promoting excellence in glucose control in hospitalized and perioperative patients WELCOME! 1. Evaluate the evidence for variable glycemic control for patients in the hospital
World Journal of Research and Review
 Glycemic Control In Critical Ill Patients; Literature Review Of Glycemic Targets Thesis Report Submitted by Dr. Mohamed Milad Abu Hmaira Supervisor: Dr. Onyebuchi Okosieme World Journal of Research and
Glycemic Control In Critical Ill Patients; Literature Review Of Glycemic Targets Thesis Report Submitted by Dr. Mohamed Milad Abu Hmaira Supervisor: Dr. Onyebuchi Okosieme World Journal of Research and
Pedro A. Mendez-Tellez, MD
 Critical Illness Polyneuropathy and Myopathy: Epidemiology and Risk Factors Pedro A. Mendez-Tellez, MD Johns Hopkins University Baltimore, Maryland, USA pmendez@jhmi.edu Conflict of Interest I have no
Critical Illness Polyneuropathy and Myopathy: Epidemiology and Risk Factors Pedro A. Mendez-Tellez, MD Johns Hopkins University Baltimore, Maryland, USA pmendez@jhmi.edu Conflict of Interest I have no
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes
 Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
Oklahoma Dietetic Association. Ainsley Malone, MS, RD, LD, CNSD April, 16, 2008 Permissive Underfeeding: What, Where and Why? Mt.
 The What, Why and When of Permissive Ainsley Malone, MS, RD, CNSD Nutrition Support Team Mt. Carmel West Hospital Mt. Carmel West 500 bed academic center Non-physician based NST Dietitian, pharmacist and
The What, Why and When of Permissive Ainsley Malone, MS, RD, CNSD Nutrition Support Team Mt. Carmel West Hospital Mt. Carmel West 500 bed academic center Non-physician based NST Dietitian, pharmacist and
Supplementary Online Content
 Supplementary Online Content Gershengorn HB, Scales DC, Kramer A, Wunsch H. Association between overnight extubations and outcomes in the intensive care unit. JAMA Intern Med. Published online September
Supplementary Online Content Gershengorn HB, Scales DC, Kramer A, Wunsch H. Association between overnight extubations and outcomes in the intensive care unit. JAMA Intern Med. Published online September
The following content was supplied by the author as supporting material and has not been copy-edited or verified by JBJS.
 Page 1 The following content was supplied by the author as supporting material and has not been copy-edited or verified by JBJS. Appendix TABLE E-1 Care-Module Trigger Events That May Indicate an Adverse
Page 1 The following content was supplied by the author as supporting material and has not been copy-edited or verified by JBJS. Appendix TABLE E-1 Care-Module Trigger Events That May Indicate an Adverse
ENDPOINTS FOR AKI STUDIES
 ENDPOINTS FOR AKI STUDIES Raymond Vanholder, University Hospital, Ghent, Belgium SUMMARY! AKI as an endpoint! Endpoints for studies in AKI 2 AKI AS AN ENDPOINT BEFORE RIFLE THE LIST OF DEFINITIONS WAS
ENDPOINTS FOR AKI STUDIES Raymond Vanholder, University Hospital, Ghent, Belgium SUMMARY! AKI as an endpoint! Endpoints for studies in AKI 2 AKI AS AN ENDPOINT BEFORE RIFLE THE LIST OF DEFINITIONS WAS
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya
 DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
Diabetic Emergencies. Chapter 15
 Diabetic Emergencies Chapter 15 Diabetes- is a disorder of glucose metabolism or difficulty metabolizing carbohydrates, fats and proteins Full name is diabetes mellitus which refers to the presence of
Diabetic Emergencies Chapter 15 Diabetes- is a disorder of glucose metabolism or difficulty metabolizing carbohydrates, fats and proteins Full name is diabetes mellitus which refers to the presence of
Insulin reduces Neuromuscular Complications and Prolonged Mechanical Ventilation in a Medical ICU. Online data supplement
 Insulin reduces Neuromuscular Complications and Prolonged Mechanical Ventilation in a Medical ICU Greet Hermans 1, Alexander Wilmer 1, Wouter Meersseman 1, Ilse Milants 2, Pieter J. Wouters 2, Herman Bobbaers
Insulin reduces Neuromuscular Complications and Prolonged Mechanical Ventilation in a Medical ICU Greet Hermans 1, Alexander Wilmer 1, Wouter Meersseman 1, Ilse Milants 2, Pieter J. Wouters 2, Herman Bobbaers
Year in Review: Critical Care Medicine
 Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
REVIEW Beyond diabetes: saving lives with insulin in the ICU
 (2002) 26, Suppl 3, S3 S8 ß 2002 Nature Publishing Group All rights reserved 0307 0565/02 $25.00 www.nature.com/ijo REVIEW Beyond diabetes: saving lives with insulin in the ICU 1 * 1 Department of Intensive
(2002) 26, Suppl 3, S3 S8 ß 2002 Nature Publishing Group All rights reserved 0307 0565/02 $25.00 www.nature.com/ijo REVIEW Beyond diabetes: saving lives with insulin in the ICU 1 * 1 Department of Intensive
Surviving Sepsis. Brian Woodcock MBChB MRCP FRCA FCCM
 1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
Nutrition in Acute Kidney Injury Enrico Fiaccadori
 Nutrition in Acute Kidney Injury Enrico Fiaccadori Nephrology Dept. Parma University Medical School Parma, Italy Diagnosis, epidemiology and prognostic impact of proteinenergy wasting (PEW) in AKI Pathogenetic
Nutrition in Acute Kidney Injury Enrico Fiaccadori Nephrology Dept. Parma University Medical School Parma, Italy Diagnosis, epidemiology and prognostic impact of proteinenergy wasting (PEW) in AKI Pathogenetic
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis
 How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis") Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Perioperative Glycemic Control
 REVIEW ARTICLES David S. Warner, M.D., and Mark A. Warner, M.D., Editors Anesthesiology 2009; 110:408 21 Copyright 2009, the American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc.
REVIEW ARTICLES David S. Warner, M.D., and Mark A. Warner, M.D., Editors Anesthesiology 2009; 110:408 21 Copyright 2009, the American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc.
Metabolic response to stress. Pierre Singer, MD Institute for Nutrition Research Critical Care Medicine Rabin Medical Center Tel Aviv University
 Metabolic response to stress Pierre Singer, MD Institute for Nutrition Research Critical Care Medicine Rabin Medical Center Tel Aviv University Disclosures Speaker fees from Abbott, GE, Cosmed, B Braun,
Metabolic response to stress Pierre Singer, MD Institute for Nutrition Research Critical Care Medicine Rabin Medical Center Tel Aviv University Disclosures Speaker fees from Abbott, GE, Cosmed, B Braun,
Effect of an Intensive Glucose Management Protocol on the Mortality of Critically Ill Adult Patients
 ORIGINAL ARTICLE GLUCOSE MANAGEMENT IN CRITICALLY ILL ADULT PATIENTS Effect of an Intensive Glucose Management Protocol on the Mortality of Critically Ill Adult Patients JAMES STEPHEN KRINSLEY, MD OBJECTIVE:
ORIGINAL ARTICLE GLUCOSE MANAGEMENT IN CRITICALLY ILL ADULT PATIENTS Effect of an Intensive Glucose Management Protocol on the Mortality of Critically Ill Adult Patients JAMES STEPHEN KRINSLEY, MD OBJECTIVE: