Improved IPGM: Demonstrating the Value to both Patients and Hospitals
|
|
|
- Jordan Chase
- 5 years ago
- Views:
Transcription

 Proper nutrition for")
1 Improved IPGM: Demonstrating the Value to both Patients and Hospitals Osama Hamdy, MD, PhD, FACE Medical Director, Inpatient Diabetes Program Joslin Diabetes Center Harvard Medical School, Boston, MA Cost and epidemiology inpatient diabetes management Three successful models of better resource utilizations Diabetes care by an endocrinology team versus hospitalists EVADE protocol (management of DKA in ED) Proper nutrition for patients with diabetes 1


2 Blood Glucose >180 mg/dl Cook CE et al. J Hosp Med 2009; 4:E7-E14 Total estimated cost of diabetes in 2012 was $245 billion (41% up from 2007), with $176 billion direct cost and 69 billion reduced productivity Largest component of medical expenditures attributed to diabetes was hospital inpatient care (~43%% of costs) Diabetes Care. 2013; 36(4):
3 According to the CDC, diabetes ranked second after circulatory diseases as a first-listed diagnosis upon hospital discharge Discharges with diabetes as a first-listed diagnosis accounted for ~2.8 million days of hospital stay 1 in 5 healthcare dollars is spent on diabetes $83 billion per year in hospital fees, 23% of total hospital spending Average stay: 5.3 days Average cost: $7,830 CDC. Diabetes Program. Data & Trends. United States AHRQ Report: Hospital Stays for Patients with Diabetes, 2008 Resource Utilization for Inpatient Diabetes Management and its Impact on 30-day Readmission and Overall Cost 3
4 756 Charts Reviewed (Patients admitted to non-critical care Jul 15,2012 Jan ) 392 Eligible Charts (Age >18, non-pregnant, Type 1 or 2 for >3 months) 262 Patients were matched 131 Primary Service Team (PST) 131 Diabetes Team (DT) * Matching was based on the average 4 blood glucose readings after admission Primary Service Team (PST) - House staff - General Discharge plan - Follow up Diabetes Team (DT) - Endocrinologist - Basic Diabetes Education - Diabetes Discharge plan - Transition of care 4
 A1C of 7.4% = eag of 166 mg/dl Hamdy O et al, ADA 2013 DT A1C of 8.")
5 HbA1C (%) 5/19/2016 Baseline Characteristics of the Intervention Groups: Primary Service Team (PST) versus Diabetes Team (DT) Data is presented as mean + standard deviation NS= None Significant 10.0% 9.0% 8.7% 8.0% 7.4% 7.0% 6.0% 5.0% 4.0% PST *p<0.001 n= 262 (131 in each group) A1C of 7.4% = eag of 166 mg/dl Hamdy O et al, ADA 2013 DT A1C of 8.7% = eag of 203 mg/dl 5
 7.4+1.3 8.7+2.1 <0.001 Patients with type 1 4.6 34.1 <0.001 Patients on oral hypoglycemic agents 21.4 9.9 0.011 Patients on basal insulin 45.8 58.0 0.")
6 Percentage of total readmission (%) 5/19/2016 Degree of Complexity during Hospitalization per Intervention Group: Primary Service Team (PST) versus Diabetes Team (DT) PST DT P-value % % n Most recent HbA1C (%) <0.001 Patients with type <0.001 Patients on oral hypoglycemic agents Patients on basal insulin Patients on insulin pump <0.001 Patients on insulin drip Patients with any infection NS Patients with any inpatient complication <0.001 Patients seen by JDT have higher A1C, more of type 1 and more complicated Data is presented as mean + standard deviation NS= None Significant Chi-Square Goodness of Fitness Test used for significance testing Hamdy O et al, ADA % Reduction All Readmission 2011 All Readmission 2012 BST JDT 5 0 Medical Service *p<0.05 n= 262 (131 in each group) Hamdy O et al, ADA 2013 Surgical Service Total Diabetes Admissions to non-icu Medicine Surgery
7 Percentage of Patients 5/19/ Early Intermediate Late 10 0 Total Medicine Surgery Type of Service Involvement of DT in Diabetes management in surgical patients is relatively late Early = within 24 hours of admission Intermediate = 24 hours to <1/2 LOS Late = >1/2 LOS Transition of Care per Intervention Group: Primary Service Team (PST) versus Diabetes Team (DT) PST JDT P-Value Transition of Care: ALL Patients (%) PCP/Surgery <0.001 Endocrinologist <0.001 Compliance with transition: ALL Patients (%) PCP/Surgery <0.001 Endocrinologist <0.001 Patients seen by DT have better transition of care to PCPs and Endocrinologists Data is presented as percent NS= None Significant *Fisher s Exact Test used for frequency of events<5, otherwise chi-square used for significance testing Hamdy O et al, ADA
8 Cost in US Dollars ($) 5/19/2016 $500,000 Medical Service Surgical Service $113,535 $125, $0 -$500,000 -$1,000,000 -$1,500,000 -$1,182,134 -$1,303,836 Estimated net cost saving in $1,068,599* Estimated net cost saving in $1,178,566* Hamdy O et al, ADA 2013 * Model is calculated based on the Average National cost of admission to non-critical care unit for 2010 ($7,830 per admission for diabetic patient) Postulated Model of Cost Saving if Diabetes Team (DT) Manages All Patients with Diabetes Admitted to the Studied hospital (649 Beds) (Model Calculated Based on the Actual Admissions in 2011, 2012) PST DT Savings Total Cost 2011 $60,878,250 $57,307,770 $3,570,480 Total Cost 2012 $50,480,010 $47,504,610 $2,975,400 Two Years Saving: $6.546 Million *Average National cost of admission to non-critical care unit for
9 Study Conclusions Management of patient with diabetes by specialized diabetes team reduces 30-day readmission by 30% Transition of care and adherence to post discharge appointments are significantly higher Significant cost saving and better resource utilization is achieved by shifting diabetes care to a specialized diabetes team DKA Management and Emergency Valuable Approach and Diabetes Education (EVADE) 9

10 Goals A significant percentage of admissions are avoidable in well-managed, coordinated health care systems Goals To provide optimal and costeffective management for DKA To reduce DKA admission by ~10% in order to reduce cost and improve and maintain good quality of care Admissions Avoidable Admissions ED Visit EVADE 10

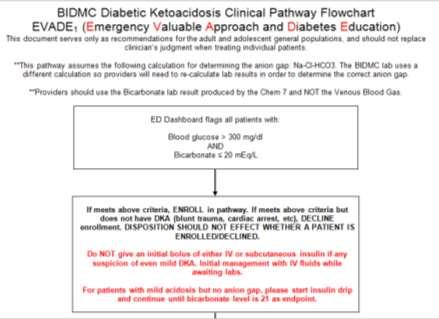
11 Blood glucose >300 mg/dl Flagged Bicarbonate 20 meq/l EVADE Protocol Implementation 11

12 EVADE Cost savings: ~$12,000/patient (difference between ER only vs. ICU admittance) Emergency Department Team 1. Identify the potential cases (electronic algorithm) 2. Confirm the diagnosis according to the protocol 3. Manage independently 4. Decide if admission is needed after observation for up to 24 hours Joslin Team 1. Help identify the cause of DKA 2. Provide the needed education to prevent its recurrence 3. Craft the insulin plan that the patient may use after discharge 4. Follow-up with patient The dashboard reviews all patients every seconds If it detects that a patient meets the enrollment criteria it will display a message Consider DKA pathway Smith, James Carroll, Stephanie Fisher, Daniel Land, Jean Saw, Jake Adams, Amy 12

13 The user can then: Enroll or Decline the patient. MD s will not be able to admit or discharge the patient without addressing the flag. Once a patient is enrolled, an auto-page is sent to the primary RN and to the Joslin EVADE Team Notification John Doe /14/90 Mary Noinsulin 26 13
14
15
16
17
18 35 Education Individualized for each patient Identification of situation leading up to DKA Review insulin action and technique of administration Review sick days rules Review ways to prevent recurrence of episode (i.e. etiology, adequate BG testing, etc) Lack of generalized knowledge of urine ketone testing Provide supplies (glucometer) 36 18
19 Education Insulin Pump Removal of entire infusion set Evaluate site of infusion set Evaluate cannulas Observe technique of infusion set placement by patient (air in pump) 37 Discharge Plan Follow-up Joslin educator will follow up with patients within 24 hours of discharge Patients who do not see Joslin for diabetes care may choose to go to their regular PCP or Joslin for a follow up appointment Patients who see Joslin for diabetes care will receive a follow up phone call within 24 hours of discharge Educational specialists will attempt to make contact with the patient via phone. If no contact is made, a voic will be left for the patient. For patients seen on a Friday or weekend, BIDMC will notify Joslin that a priority follow up call should be made on Monday morning
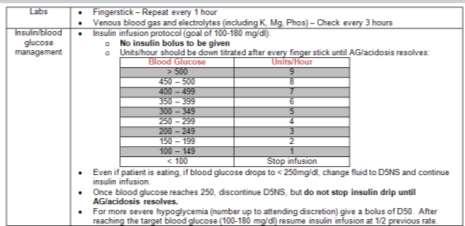
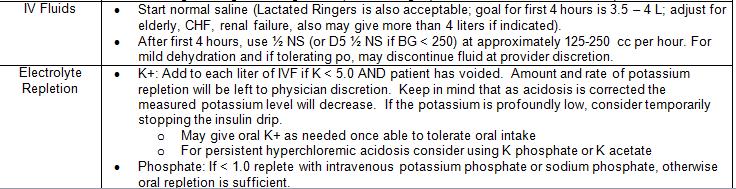
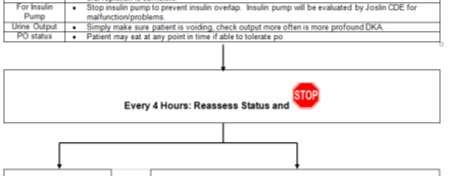
20 Yes No n/a or Unkno wn QA Result Enrollment parameter met % - Meeting enrollment parameter No insulin bolus given % - Still getting insulin bolus Fingersticks performed every hour % - Not getting fingersticks every hour VBGs and electrolytes drawn every 3 hours Insulin gtt adjusted appropriately to glucose level NS or LR given, at 3.5-4L within the first 4 hours Appropriate electrolyte repletion D5 initiated and stopped according to parameters Individual insulin pump stopped if present All 4 hour stops met with appropriate disposition (discharge/obs/admit) Once anion gap has closed 18% - Not getting VBGs and electrolytes drawn every 3 hours 12% - Insulin gtt not adjusted appropriate to glucose level 53% - Not getting NS or LR at 3.5-4L within the first 4 hours 14% - Not getting appropriate electrolyte repletion 10% - Not getting D5 and/or having D5 stopped according to parameters 59% - Not having individual insulin pump stopped (when present) 17% - 4 hour stops not met with appropriate disposition Appropriate subcutaneous insulin given % - No subcutaneous insulin given Insulin drip stopped per appropriate parameters 18 5 Discharged per appropriate parameters % - Insulin drip stopped per appropriate parameters 1% - Not discharged per appropriate parameters EVADE Results 9/1/13-3/24/ Flagged as potential candidates 54 Ineligible for pathway 97 Eligible for pathway 74 Admitted 23 Discharged 15 Not placed on pathway, but patient correctly dispositioned 31% Discharged from ED 82 Placed on pathway 31% treated and discharged from ED 74% Good adherence to EVADE pathway 61 Good pathway adherence (> 75% markers) 10 Fair pathway adherence (50-75% markers) 11 Poor pathway adherence (<50% markers) 9/1/2013 thru 3/24/
21 Length of Hospital Stay 97 Eligible for pathway 23 Discharged from ED 74 Admitted LOS in ED 20 hrs 20 to non-icu LOS 133 hrs LOS in non-icu reduced to 133 hrs LOS in ICU + Post ICU reduced to 113 hrs 54 to ICU LOS in ICU 34 hrs LOS after ICU discharge 79 hrs 9/1/2013 thru 3/24/2014 EVADE Program 43% Reduction in DKA Admissions Decrease LOS Pre-EVADE LOS Post-EVADE LOS Reduction in LOS 6 mos DKA Admissions (9/1/13-3/24/14) Decrease LOS impact* ICU $108,000 Non-ICU $24,092 National data (2010) DKA admission cost ICU $13,000 / 6.5 (LOS) = $2,000 National data (2010) DKA admission cost non-icu $7,830 / 6.5 (LOS) = $1,204 Estimated EVADE impact for 6 mos $221,000. Annualized savings $464,185 21
22 EVADE Conclusions Treatment of mild and moderate DKA by ED team is feasible and reduces hospital admission for DKA management by 43% Length of stay for admitted patients is lower by 1.8 days in ICU and 1 day in non-icu Cost saving per evaded single admission to the ICU is ~$12,000 Differences in Resource Utilization Between Diabetic Patients Receiving Diabetes-Specific Nutrition Formula Versus Standard Nutrition Formula In US Hospitals 22
23 Objective and Methods Design Retrospective review of all inpatients and hospital-based outpatients within Premier Research Database N=>500 geographically diverse hospitals Comparisons made between: Diabetic patients fed diabetes specific formula (DSF) Diabetic patients fed standard nutrition (STD) Population All inpatients discharged - Jan 1, 00 and Dec 31, 09 (acute setting) Diagnosis of diabetes (identified using ICD-9 code 249.x and 250.x). Patients receiving STD or DSF nutrition were matched across many characteristics to isolate impact of nutrition type Propensity score matching was utilized to adjust for imbalances in the patient demographic and clinical characteristics. This score was used to match DSF fed patients and similar patients that received STD before modeling of outcomes. Matching Variables Demographics/Patient Characteristics Age/Gender/Race Primary Payor Diabetes type APR-DRG Severity of Illness and Mortality Risk Insulin types Oral/parenteral non-insulin antidiabetic agents Co-morbidities (e.g., obesity, hypertension ) Hospital Characteristics Regional Mix Bed Size Urban Teaching Status Regression variables Discharge Status Admit Type and Source Nutrition Duration (days) Infection Amputation Obesity Malnutrition Renal failure 23
24 Population Flow Diabetic Population 8.8 million discharges ( ) Fed either STD or DSF 193,473 discharges Tube Fed 85,481 discharges Diabetic Nutrition 37,171 discharges Standard Nutrition 48,310 discharges Results Feeding DSF to patients with diabetes results in significant* improvement in patient efficiency and cost of care Per patient Average Length of Hospital Stay Savings from feeding DSF rather than STD formula Tube Fed PWD 0.9 days Total Hospital Costs $2,586 * Average LOS and hospital cost statistically significant at P <
25 Adjusted Cost per Patient ($) 5/19/2016 Using DSF drives reduction in room & board, pharmacy, and labor costs for tube fed PWD Tube Fed PWD - $2,586 total savings per patient $28,000 $26,769 ($1,257) $26,000 ($341) ($354) ($82) (~$552) $24,183 $24,000 $22,000 $20,000 STD Nutrition Room and Board Pharmacy Nursing Labor Supply Other DSF Nutrition Note: Analysis adjusted the Other cost consistent with total cost savings since all costs independently modeled. Other costs include Surgery, Lab, Diagnostic Imaging, and Cardiology. All cost values statistically significant at P < except TF Central Supply Costs (P < 0.003). N for each sample population > 30k Study Conclusions The use of diabetes-specific nutrition formula for tube feeding of hospitalized patients with diabetes reduces the length of stay (LOS) and the overall hospital cost in comparison to standard nutrition Considering that 43% of the $176 billion direct cost is attributed to hospital cost, this magnitude of saving is valuable and warrants better resource utilization for inpatient nutrition 25
26 Take Home Messages Better resource utilizations result in significant value to both patients and hospitals Managing diabetes by a specialized diabetes team versus primary service team and hospitalists reduces 30-day readmission, improves post-discharge adherence and reduces overall hospital cost Managing mild and moderate cases of DKA by a trained ED team supplement by diabetes education reduces admission to ICU, hospital LOS and increases patients quality of life Using diabetes-specific formula for tube feeding reduce LOS and overall hospital cost Thank You 26
DKA/HHS Pathway Phase 1 (Adult) Insulin Potassium Bicarbonate
 Insulin Potassium Bicarbonate") Approved by Diabetes Steering Committee, MMC, 2015 DKA/HHS Pathway Phase 1 (Adult) DKA Diagnostic Criteria (See page 3 for more details): Blood glucose >250 mg/dl, Arterial ph
Approved by Diabetes Steering Committee, MMC, 2015 DKA/HHS Pathway Phase 1 (Adult) DKA Diagnostic Criteria (See page 3 for more details): Blood glucose >250 mg/dl, Arterial ph
The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It
 The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It Cassie Brady, MD Assistant Professor of Pediatrics Division of Endocrinology and Diabetes Monroe Carell Junior Children s Hospital
The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It Cassie Brady, MD Assistant Professor of Pediatrics Division of Endocrinology and Diabetes Monroe Carell Junior Children s Hospital
Impact of a critical pathway on inpatient management of diabetic ketoacidosis Ilag L L, Kronick S, Ernst R D, Grondin L, Alaniz C, Liu L, Herman W H
 Impact of a critical pathway on inpatient management of diabetic ketoacidosis Ilag L L, Kronick S, Ernst R D, Grondin L, Alaniz C, Liu L, Herman W H Record Status This is a critical abstract of an economic
Impact of a critical pathway on inpatient management of diabetic ketoacidosis Ilag L L, Kronick S, Ernst R D, Grondin L, Alaniz C, Liu L, Herman W H Record Status This is a critical abstract of an economic
DKA Adult ICU Powerplan
 DKA Adult ICU Powerplan Key Points for ED to ICU DKA power plan In addition to NS fluids and maintenance the regular insulin drip will either already be infusing from ED or needs to be initiated. Regular
DKA Adult ICU Powerplan Key Points for ED to ICU DKA power plan In addition to NS fluids and maintenance the regular insulin drip will either already be infusing from ED or needs to be initiated. Regular
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT *****ALSO ORDER SUB ACUTE DKA IV FLUIDS REGIMEN & SUB ACUTE ELECTROLYTE REPLACEMENT on separate forms ***** Condition/Status For purpose of this DKA Regimen, DKA is considered clear
DRUG AND TREATMENT *****ALSO ORDER SUB ACUTE DKA IV FLUIDS REGIMEN & SUB ACUTE ELECTROLYTE REPLACEMENT on separate forms ***** Condition/Status For purpose of this DKA Regimen, DKA is considered clear
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE
 SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: DKA / HHNS PATIENTS REQUIRING INTRAVENOUS INSULIN DRIPS -ADULTS Nursing DATE: REVIEWED: PAGES: 12/14 5/18 1 of 8 RESPONSIBILITY: *RN (Renal/Diabetes/Wound
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: DKA / HHNS PATIENTS REQUIRING INTRAVENOUS INSULIN DRIPS -ADULTS Nursing DATE: REVIEWED: PAGES: 12/14 5/18 1 of 8 RESPONSIBILITY: *RN (Renal/Diabetes/Wound
DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT Acute Diabetic Ketoacidosis Condition/Status ***(NOTE)*** For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS
DRUG AND TREATMENT Acute Diabetic Ketoacidosis Condition/Status ***(NOTE)*** For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS
CHI Franciscan. Matt Levi Director Virtual Health Services. March 31, 2015
 CHI Franciscan Matt Levi Director Virtual Health Services March 31, 2015 Reflection / 2 Agenda Introduction and background Matt Levi Director of Franciscan Health System Virtual Health Katie Farrell Manager
CHI Franciscan Matt Levi Director Virtual Health Services March 31, 2015 Reflection / 2 Agenda Introduction and background Matt Levi Director of Franciscan Health System Virtual Health Katie Farrell Manager
Diabetes Quality Improvement Initiative
 Diabetes Quality Improvement Initiative Community Care of North Carolina 2300 Rexwoods Drive, Ste. 100 Raleigh, NC 27607 (919) 745-2350 www.communitycarenc.org 2007 Background The Clinical Directors of
Diabetes Quality Improvement Initiative Community Care of North Carolina 2300 Rexwoods Drive, Ste. 100 Raleigh, NC 27607 (919) 745-2350 www.communitycarenc.org 2007 Background The Clinical Directors of
LIBERTYHEALTH. Jersey City Medical Center Department of Patient Care Services. Approved by Policy Committee:
 LIBERTYHEALTH Jersey City Medical Center Department of Patient Care Services Guidelines: CRITICAL CARE INSULIN PROTOCOL (MICU/SICU, CCU, ED) Developed by: Pharmacy Dept Approved by: Rita Smith, DNP Senior
LIBERTYHEALTH Jersey City Medical Center Department of Patient Care Services Guidelines: CRITICAL CARE INSULIN PROTOCOL (MICU/SICU, CCU, ED) Developed by: Pharmacy Dept Approved by: Rita Smith, DNP Senior
A Children s Bedtime Story
 A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
Hypoglycemia Reduction STARTER PACK WEBINAR #1
 Hypoglycemia Reduction STARTER PACK WEBINAR #1 Why is it important to reduce hypoglycemia? Why Hypoglycemia Reduction? Key Statistics Overall 29% reduction in ADEs since 2010 Hypoglycemia still occurs
Hypoglycemia Reduction STARTER PACK WEBINAR #1 Why is it important to reduce hypoglycemia? Why Hypoglycemia Reduction? Key Statistics Overall 29% reduction in ADEs since 2010 Hypoglycemia still occurs
GLYCEMIC CONTROL SURVEY
 GLYCEMIC CONTROL SURVEY Objective: To gain an understanding of the current state of glycemic control (ie, intensive insulin therapy and frequent blood glucose testing) protocol use in hospital inpatients.
GLYCEMIC CONTROL SURVEY Objective: To gain an understanding of the current state of glycemic control (ie, intensive insulin therapy and frequent blood glucose testing) protocol use in hospital inpatients.
ALL orders are active unless: 1. Order is manually lined through to inactivate 2. Orders with check boxes ( ) are unchecked
 are unchecked") Available at: BMC-B BMC-D BMC-N BMC-S Condition/Status ***(NOTE)***For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS than 12
Available at: BMC-B BMC-D BMC-N BMC-S Condition/Status ***(NOTE)***For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS than 12
Hospital Transition Management. Barbara Wood, BSN, MBA
 Hospital Transition Management Barbara Wood, BSN, MBA Director, Embedded Care Management Programs OBJECTIVES Improve health care quality for our patients by streamlining care transitions Reduce avoidable
Hospital Transition Management Barbara Wood, BSN, MBA Director, Embedded Care Management Programs OBJECTIVES Improve health care quality for our patients by streamlining care transitions Reduce avoidable
NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING
 Sharp HealthCare s 2016 Diabetes Conference November 11, 2016 NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING Tamara Swigert, MSN, RN, CDE Speaker Disclosure Tammy Swigert has no conflicts
Sharp HealthCare s 2016 Diabetes Conference November 11, 2016 NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING Tamara Swigert, MSN, RN, CDE Speaker Disclosure Tammy Swigert has no conflicts
DKA : Diabetic Ketoacidosis & HHS: Hyperlgycemic Hyperosmolar Syndrome Protocol. Glycemic Task Force September 2014
 DKA : Diabetic Ketoacidosis & HHS: Hyperlgycemic Hyperosmolar Syndrome Protocol Glycemic Task Force September 2014 Hyperglycemic Crises: Pathophysiology DKA HHS Hyperglycemia DKA HHS Umpierrez, In Shoemaker,
DKA : Diabetic Ketoacidosis & HHS: Hyperlgycemic Hyperosmolar Syndrome Protocol Glycemic Task Force September 2014 Hyperglycemic Crises: Pathophysiology DKA HHS Hyperglycemia DKA HHS Umpierrez, In Shoemaker,
Diabetic Ketoacidosis (DKA) Critical Care Guideline Two Bag System
 Critical Care Guideline Two Bag System") Critical Care Guideline Two Bag System Inclusion Criteria (Definition of DKA): Blood glucose (BG) > 200 mg/dl Acidosis (bicarbonate < 15 or blood gas ph < 7.3) Associated glycosuria, ketonuria &/or ketonemia
Critical Care Guideline Two Bag System Inclusion Criteria (Definition of DKA): Blood glucose (BG) > 200 mg/dl Acidosis (bicarbonate < 15 or blood gas ph < 7.3) Associated glycosuria, ketonuria &/or ketonemia
123 Are You Providing Evidence-Based Diabetes Care? - Martin
 Donna Martin, DNP, RN, CDE, CMSRN Lewis University Learner will be able to: Identify current inpatient standards of care for patients with diabetes Describe causes of hyperglycemia / hypoglycemia in the
Donna Martin, DNP, RN, CDE, CMSRN Lewis University Learner will be able to: Identify current inpatient standards of care for patients with diabetes Describe causes of hyperglycemia / hypoglycemia in the
In - Hospital Diabetes Care. A review and personal experience
 In - Hospital Diabetes Care A review and personal experience Hyperglycemia in the Hospital The Problem Hospitalizations with Diabetes http://www.cdc.gov/diabetes/statistics/dmany/fig1.htm Prevalence of
In - Hospital Diabetes Care A review and personal experience Hyperglycemia in the Hospital The Problem Hospitalizations with Diabetes http://www.cdc.gov/diabetes/statistics/dmany/fig1.htm Prevalence of
Special Situations 1
 Special Situations 1 Outline Continuous Nutrition Tube feeds TPN Steroids Pumps Perioperative BG Control 2 Patient receiving continuous TF or TPN Continuous nutrition coverage options: Analog q4hr Regular
Special Situations 1 Outline Continuous Nutrition Tube feeds TPN Steroids Pumps Perioperative BG Control 2 Patient receiving continuous TF or TPN Continuous nutrition coverage options: Analog q4hr Regular
Meeting the Challenge of Inpatient Glycemic Management in the Non-Critical Care Setting
 Meeting the Challenge of Inpatient Glycemic Management in the Non-Critical Care Setting Jane Jeffrie Seley, DNP, MPH, GNP, BC-ADM, CDE, CDTC, FAAN, FAADE Diabetes Nurse Practitioner, Inpatient Diabetes
Meeting the Challenge of Inpatient Glycemic Management in the Non-Critical Care Setting Jane Jeffrie Seley, DNP, MPH, GNP, BC-ADM, CDE, CDTC, FAAN, FAADE Diabetes Nurse Practitioner, Inpatient Diabetes
Improving Glycemic Control in the Critical Care
 Improving Glycemic Control in the Critical Care Setting /Hospitalists Outline Review current guidelines Review current glycemic targets DKA Treatment Building a perfect glycemic control protocol Transition
Improving Glycemic Control in the Critical Care Setting /Hospitalists Outline Review current guidelines Review current glycemic targets DKA Treatment Building a perfect glycemic control protocol Transition
DIABETES MANAGEMENT DISCHARGE COMMUNICATION (DM-DC) AUDIT TOOL
 AUDIT TOOL") DIABETES MANAGEMENT DISCHARGE COMMUNICATION (DM-DC) AUDIT TOOL Facility: Date: Data Collector s name: Email/Phone: Purpose: To evaluate your facility practices regarding communication of requisite diabetes
DIABETES MANAGEMENT DISCHARGE COMMUNICATION (DM-DC) AUDIT TOOL Facility: Date: Data Collector s name: Email/Phone: Purpose: To evaluate your facility practices regarding communication of requisite diabetes
Session #206, March 8, 2018 Susan J. Kressly, MD, FAAP, Kressly Pediatrics Dr. Jacques Orces, D.O., Nicklaus Children s Hospital
 Improving Preventative Care in Pediatrics through Health and Technology: A Davies Story Session #206, March 8, 2018 Susan J. Kressly, MD, FAAP, Kressly Pediatrics Dr. Jacques Orces, D.O., Nicklaus Children
Improving Preventative Care in Pediatrics through Health and Technology: A Davies Story Session #206, March 8, 2018 Susan J. Kressly, MD, FAAP, Kressly Pediatrics Dr. Jacques Orces, D.O., Nicklaus Children
Collaborative Approach in Managing the High Risk Diabetic Patient in a Patient Centered Medical Home
 Collaborative Approach in Managing the High Risk Diabetic Patient in a Patient Centered Medical Home Background Safety net facility serving the community for more than 140 years Employ over 3500 health
Collaborative Approach in Managing the High Risk Diabetic Patient in a Patient Centered Medical Home Background Safety net facility serving the community for more than 140 years Employ over 3500 health
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Pharmacy-Driven Inpatient
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Pharmacy-Driven Inpatient
Standardizing Detection of Acute Kidney Injury in an Integrated Delivery Health System
 Standardizing Detection of Acute Kidney Injury in an Integrated Delivery Health System Tarush Kothari, MD, MPH Physician Informaticist, Northwell Health Laboratories Assistant Professor in Pathology and
Standardizing Detection of Acute Kidney Injury in an Integrated Delivery Health System Tarush Kothari, MD, MPH Physician Informaticist, Northwell Health Laboratories Assistant Professor in Pathology and
ADMIT DIABETIC KETOACIDOSIS (DKA) PLAN - Phase: Begin Immediately/Emergency Center
 PLAN - Phase: Begin Immediately/Emergency Center") - Phase: Begin Immediately/Emergency Center Weight PHYSICIAN S Allergies Admit/Discharge/Transfer Patient Status Requested Location: MICU, Pt Status: Inpatient (LOS > 2 midnights) Requested Location: 5E
- Phase: Begin Immediately/Emergency Center Weight PHYSICIAN S Allergies Admit/Discharge/Transfer Patient Status Requested Location: MICU, Pt Status: Inpatient (LOS > 2 midnights) Requested Location: 5E
Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting
 Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting Greg Maynard MD, MSc Clinical Professor of Medicine and CQO, UC Davis Medical Center Sacramento, CA Greg Maynard Disclosure SHM
Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting Greg Maynard MD, MSc Clinical Professor of Medicine and CQO, UC Davis Medical Center Sacramento, CA Greg Maynard Disclosure SHM
Session 15 Improved Outcomes and a Proven ROI Model for Quality Improvement: Transforming Diabetes Care
 Session 15 Improved Outcomes and a Proven ROI Model for Quality Improvement: Transforming Diabetes Care Charles G Macias MD, MPH Chief Clinical Systems Integration Officer Director of Evidence-Based Outcomes
Session 15 Improved Outcomes and a Proven ROI Model for Quality Improvement: Transforming Diabetes Care Charles G Macias MD, MPH Chief Clinical Systems Integration Officer Director of Evidence-Based Outcomes
Pharmacist Opportunities within Telemedicine
 Pharmacist Opportunities within Telemedicine Bryan Robinette, PharmD, BCPS-AQ Cardiology, Sonia Everhart, PharmD, BCPS, BCCCP Desiree Kosmisky, PharmD, BCCCP March 13 th, 2017 Disclosures Sonia Everhart,
Pharmacist Opportunities within Telemedicine Bryan Robinette, PharmD, BCPS-AQ Cardiology, Sonia Everhart, PharmD, BCPS, BCCCP Desiree Kosmisky, PharmD, BCCCP March 13 th, 2017 Disclosures Sonia Everhart,
Systematic Improvement of Diabetes Care in the Inpatient Setting
 Success Story Systematic Improvement of Diabetes Care in the Inpatient Setting EXECUTIVE SUMMARY Texas Children s Hospital is improving the care delivery of its patients with diabetes, one of the most
Success Story Systematic Improvement of Diabetes Care in the Inpatient Setting EXECUTIVE SUMMARY Texas Children s Hospital is improving the care delivery of its patients with diabetes, one of the most
Reducing Readmissions and Improving Outcomes at OhioHealth Mansfield Hospital:
 Reducing Readmissions and Improving Outcomes at OhioHealth Mansfield Hospital: Eugenio H. Zabaleta, Ph.D. Clinical Chemist OhioHealth Mansfield Hospital Reducing Readmissions and Improving Outcomes at
Reducing Readmissions and Improving Outcomes at OhioHealth Mansfield Hospital: Eugenio H. Zabaleta, Ph.D. Clinical Chemist OhioHealth Mansfield Hospital Reducing Readmissions and Improving Outcomes at
Quality Outcomes and Financial Benefits of Nutrition Intervention. Tracy R. Smith, PhD, RD, LD Senior Clinical Manager, Abbott Nutrition
 Quality Outcomes and Financial Benefits of Nutrition Intervention Tracy R. Smith, PhD, RD, LD Senior Clinical Manager, Abbott Nutrition January 28, 2016 SHIFTING MARKET DYNAMICS PROVIDE AN OPPORTUNITY
Quality Outcomes and Financial Benefits of Nutrition Intervention Tracy R. Smith, PhD, RD, LD Senior Clinical Manager, Abbott Nutrition January 28, 2016 SHIFTING MARKET DYNAMICS PROVIDE AN OPPORTUNITY
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes
 Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
Report Reference Guide. THERAPY MANAGEMENT SOFTWARE FOR DIABETES CareLink Report Reference Guide 1
 Report Reference Guide THERAPY MANAGEMENT SOFTWARE FOR DIABETES CareLink Report Reference Guide 1 How to use this guide Each type of CareLink report and its components are described in the following sections.
Report Reference Guide THERAPY MANAGEMENT SOFTWARE FOR DIABETES CareLink Report Reference Guide 1 How to use this guide Each type of CareLink report and its components are described in the following sections.
Deepika Reddy MD Department of Endocrinology
 Deepika Reddy MD Department of Endocrinology Management of hyperglycemic crisis Review need for inpatient glycemic control Brief overview of relevant trials Case based review of diabetes management strategies/review
Deepika Reddy MD Department of Endocrinology Management of hyperglycemic crisis Review need for inpatient glycemic control Brief overview of relevant trials Case based review of diabetes management strategies/review
Hypoglycemia Task Force: A Quality Improvement Initiative to Reduce Inpatient Hypoglycemia
 Hypoglycemia Task Force: A Quality Improvement Initiative to Reduce Inpatient Hypoglycemia Shiv Patil, MD, MPH, BC-ADM Clinical Assistant Professor of Family Medicine Brody School of Medicine at East Carolina
Hypoglycemia Task Force: A Quality Improvement Initiative to Reduce Inpatient Hypoglycemia Shiv Patil, MD, MPH, BC-ADM Clinical Assistant Professor of Family Medicine Brody School of Medicine at East Carolina
COMPLIANCE WITH THIS DOCUMENT IS MANDATORY
 COVER SHEET `NAME OF DOCUMENT TYPE OF DOCUMENT at Shoalhaven Hospital Group Critical Care Procedure DOCUMENT NUMBER DATE OF PUBLICATION February 2018 RISK RATING Medium REVIEW DATE February 2021 FORMER
COVER SHEET `NAME OF DOCUMENT TYPE OF DOCUMENT at Shoalhaven Hospital Group Critical Care Procedure DOCUMENT NUMBER DATE OF PUBLICATION February 2018 RISK RATING Medium REVIEW DATE February 2021 FORMER
Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events. September 13, 2016
 Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events September 13, 2016 St Joseph s Health Fast Facts Founded 1869 by Sisters of St. Francis Patient Volumes (2014) Inpatient
Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events September 13, 2016 St Joseph s Health Fast Facts Founded 1869 by Sisters of St. Francis Patient Volumes (2014) Inpatient
Arterial blood gas Capillary blood glucose every hour. Continue to monitor hourly capillary blood glucose as per protocol (See Appendix A and B)
") Page 1 of 6 Hyperglycemic Emergency Management (DKA/HHS 1 ) - Adult PATIENT PRESENTATION Patient with history of Type 1 or 2 Diabetes Mellitus or presenting with polyuria, polydipsia, nausea/ vomiting,
Page 1 of 6 Hyperglycemic Emergency Management (DKA/HHS 1 ) - Adult PATIENT PRESENTATION Patient with history of Type 1 or 2 Diabetes Mellitus or presenting with polyuria, polydipsia, nausea/ vomiting,
Water Works. The Value of Water
 Water Works The Value of Water The Value of Water Water Works Water is vital for the body Accounting for roughly 60% of body weight, water is the largest component of the human body and the major constituent
Water Works The Value of Water The Value of Water Water Works Water is vital for the body Accounting for roughly 60% of body weight, water is the largest component of the human body and the major constituent
5/15/2018 DISCLOSURE OBJECTIVES. FLORIDA HOSPITAL ORLANDO Not for profit organization Acute care medical center 1,368 licensed beds BACKGROUND
 DISCLOSURE PHARMACIST DIRECTED MANAGEMENT OF GLUCOCORTICOID INDUCED HYPERGLYCEMIA AT A LARGE COMMUNITY HOSPITAL Jill Zaccardelli, PharmD PGY1 Pharmacy Resident Florida Hospital Orlando Jill.Zaccardelli@flhosp.org
DISCLOSURE PHARMACIST DIRECTED MANAGEMENT OF GLUCOCORTICOID INDUCED HYPERGLYCEMIA AT A LARGE COMMUNITY HOSPITAL Jill Zaccardelli, PharmD PGY1 Pharmacy Resident Florida Hospital Orlando Jill.Zaccardelli@flhosp.org
DIABETES MELLITUS. IAP UG Teaching slides
 DIABETES MELLITUS 1 DIABETES MELLITUS IN CHILDREN Introduction, Definition Classification, pathogenesis Clinical features Investigations and diagnosis Therapy and follow up Complications Carry home message
DIABETES MELLITUS 1 DIABETES MELLITUS IN CHILDREN Introduction, Definition Classification, pathogenesis Clinical features Investigations and diagnosis Therapy and follow up Complications Carry home message
Arterial blood gas Capillary blood glucose every hour. Continue to monitor hourly capillary blood glucose as per protocol (See Appendix A and B)
") Page 1 of 6 Hyperglycemic Emergency Management (DKA/HHS 1 ) - Adult PATIENT PRESENTATION Patient with history of Type 1 or 2 Diabetes Mellitus or presenting with polyuria, polydipsia, nausea/ vomiting,
Page 1 of 6 Hyperglycemic Emergency Management (DKA/HHS 1 ) - Adult PATIENT PRESENTATION Patient with history of Type 1 or 2 Diabetes Mellitus or presenting with polyuria, polydipsia, nausea/ vomiting,
Report Reference Guide
 Report Reference Guide How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used to generate the sample reports was from sample patient
Report Reference Guide How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used to generate the sample reports was from sample patient
Learning Objectives. Perioperative SWEET Success
 Perioperative SWEET Success PERIOPERATIVE SWEET SUCCESS PRESENTED BY: KENDRA MARTIN, RN, BSN, CDE JENNIFER SIMPSON, RN, BC-ADM, MSN, CNS Disclosure to Participants Notice of Requirements For Successful
Perioperative SWEET Success PERIOPERATIVE SWEET SUCCESS PRESENTED BY: KENDRA MARTIN, RN, BSN, CDE JENNIFER SIMPSON, RN, BC-ADM, MSN, CNS Disclosure to Participants Notice of Requirements For Successful
Performance Analysis:
 Performance Analysis: Healthcare Utilization of CCNC- Population 2007-2010 Prepared by Treo Solutions JUNE 2012 Table of Contents SECTION ONE: EXECUTIVE SUMMARY 4-5 SECTION TWO: REPORT DETAILS 6 Inpatient
Performance Analysis: Healthcare Utilization of CCNC- Population 2007-2010 Prepared by Treo Solutions JUNE 2012 Table of Contents SECTION ONE: EXECUTIVE SUMMARY 4-5 SECTION TWO: REPORT DETAILS 6 Inpatient
2017 Diabetes. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Diabetes Program Evaluation Our mission is to improve the health and quality of life of our members Diabetes Program Evaluation Program Title: Diabetes Program Evaluation Period: January 1, 2017 December
2017 Diabetes Program Evaluation Our mission is to improve the health and quality of life of our members Diabetes Program Evaluation Program Title: Diabetes Program Evaluation Period: January 1, 2017 December
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!!
 Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Calgary Diabetes Centre Insulin Pump Therapy: Preparation and Expectations
 Calgary Diabetes Centre Insulin Pump Therapy: Preparation and Expectations This is a long and important document. It lists the steps for starting insulin pump therapy at the Calgary Diabetes Centre. It
Calgary Diabetes Centre Insulin Pump Therapy: Preparation and Expectations This is a long and important document. It lists the steps for starting insulin pump therapy at the Calgary Diabetes Centre. It
Provincial Clinical Knowledge Topic Insulin Pump Therapy, Pediatric and Adult Acute Care V 1.0
 Provincial Clinical Knowledge Topic Insulin Pump Therapy, Pediatric and Adult Acute Care V 1.0 Copyright: 2018, Alberta Health Services. This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives
Provincial Clinical Knowledge Topic Insulin Pump Therapy, Pediatric and Adult Acute Care V 1.0 Copyright: 2018, Alberta Health Services. This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives
2015 Diabetes. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2015 Diabetes Program Evaluation Our mission is to improve the health and quality of life of our members Diabetes Care Program Evaluation Program Title: Diabetes Care Program Evaluation Period: January
2015 Diabetes Program Evaluation Our mission is to improve the health and quality of life of our members Diabetes Care Program Evaluation Program Title: Diabetes Care Program Evaluation Period: January
Adherence to Heart Failure
 Disease Management Programs Adherence to Heart Failure Management Guidelines Raed Odeh, Nurse Specialist Co-Authers: Elias Fadel, MB Bdeir, A. Mukhtar, T. Conboy, M. Al-Mallah. King Abdul Aziz Medical
Disease Management Programs Adherence to Heart Failure Management Guidelines Raed Odeh, Nurse Specialist Co-Authers: Elias Fadel, MB Bdeir, A. Mukhtar, T. Conboy, M. Al-Mallah. King Abdul Aziz Medical
In-hospital management of diabetes
 Dr. Tom Elliott MBBS, FRCPC Medical Director 400-210 W Broadway phone: 604.683.3734 Vancouver, BC fax: 604.628.3821 V5Y 3W2 Canada email: moa@bcdiabetes.ca In-hospital management of diabetes General Management
Dr. Tom Elliott MBBS, FRCPC Medical Director 400-210 W Broadway phone: 604.683.3734 Vancouver, BC fax: 604.628.3821 V5Y 3W2 Canada email: moa@bcdiabetes.ca In-hospital management of diabetes General Management
EmergencyKT: New Onset Diabetes, Non-DKA Definition: ED patient with newly discovered hyperglycemia, >200 mg %
 EmergencyKT: New Onset, Non-DKA Definition: ED patient with newly discovered hyperglycemia, >200 mg % Obtain: CBCD EP1 VBG Serum Ketone Hemoglobin A1c (for follow up) UA β-hcg (female at risk for pregnancy)
EmergencyKT: New Onset, Non-DKA Definition: ED patient with newly discovered hyperglycemia, >200 mg % Obtain: CBCD EP1 VBG Serum Ketone Hemoglobin A1c (for follow up) UA β-hcg (female at risk for pregnancy)
16 th Annual IHA Stakeholders Meeting Session 2C
 16 th Annual IHA Stakeholders Meeting Session 2C September 19, 2017 Hilton Los Angeles Airport Thank you to our Content Partner: Medication Adherence AppleCare Pharmacy Programs Confidential and proprietary.
16 th Annual IHA Stakeholders Meeting Session 2C September 19, 2017 Hilton Los Angeles Airport Thank you to our Content Partner: Medication Adherence AppleCare Pharmacy Programs Confidential and proprietary.
Diabetes (DIA) Measures Document
 Measures Document") Diabetes (DIA) Measures Document DIA Version: 2.1 - covering patients discharged between 01/07/2016 and present. Programme Lead: Liz Kanwar Clinical Lead: Dr Aftab Ahmad Number of Measures In Clinical
Diabetes (DIA) Measures Document DIA Version: 2.1 - covering patients discharged between 01/07/2016 and present. Programme Lead: Liz Kanwar Clinical Lead: Dr Aftab Ahmad Number of Measures In Clinical
Type of intervention Secondary prevention. Economic study type Cost-effectiveness analysis.
 Improved outcomes in indigent patients with ketosis-prone diabetes: effect of a dedicated diabetes treatment unit Maldonado M R, D'Amico S, Rodriguez L, Iyer D, Balasubramanyam A Record Status This is
Improved outcomes in indigent patients with ketosis-prone diabetes: effect of a dedicated diabetes treatment unit Maldonado M R, D'Amico S, Rodriguez L, Iyer D, Balasubramanyam A Record Status This is
Pathogenesis of disease diabetic ketoacidosis
 Pathogenesis of disease diabetic ketoacidosis Dr Ketan Dhatariya MBBS MSc MD MS FRCP Consultant in Diabetes and Endocrinology Norfolk and Norwich University Hospitals None Disclosures Diagnostic Criteria
Pathogenesis of disease diabetic ketoacidosis Dr Ketan Dhatariya MBBS MSc MD MS FRCP Consultant in Diabetes and Endocrinology Norfolk and Norwich University Hospitals None Disclosures Diagnostic Criteria
Peripartum and Postpartum Management of Diabetes
 Peripartum and Postpartum Management of Diabetes General Principles Glucose goal ~ 100 mg/dl (70-110 mg/dl) Labor is EXERCISE with increased metabolic demands. Insulin requirements decrease however the
Peripartum and Postpartum Management of Diabetes General Principles Glucose goal ~ 100 mg/dl (70-110 mg/dl) Labor is EXERCISE with increased metabolic demands. Insulin requirements decrease however the
CareLink. software REPORT REFERENCE GUIDE. Management Software for Diabetes
 CareLink Management Software for Diabetes software REPORT REFERENCE GUIDE How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used
CareLink Management Software for Diabetes software REPORT REFERENCE GUIDE How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used
Implementing Glucose Control in 2009 and Beyond: Changes in Patterns and Perceptions
 Implementing Glucose Control in 2009 and Beyond: Changes in Patterns and Perceptions Charles C. Reed MSN, RN, CNRN Patient Care Coordinator Surgical Trauma ICU University Hospital San Antonio, Texas Relationships
Implementing Glucose Control in 2009 and Beyond: Changes in Patterns and Perceptions Charles C. Reed MSN, RN, CNRN Patient Care Coordinator Surgical Trauma ICU University Hospital San Antonio, Texas Relationships
NoCVA Preventing Avoidable Readmissions Collaborative. Pre-work: Assessing Risk April 21, 2014
 NoCVA Preventing Avoidable Readmissions Collaborative Pre-work: Assessing Risk April 21, 2014 Agenda Context Collaborative Overview Setting up to succeed Why assess risk of readmission Methods to assess
NoCVA Preventing Avoidable Readmissions Collaborative Pre-work: Assessing Risk April 21, 2014 Agenda Context Collaborative Overview Setting up to succeed Why assess risk of readmission Methods to assess
AJHM Volume 1 Issue 3 (Jul-Sept 2017) ORIGINAL ARTICLE
 ORIGINAL ARTICLE") Impact of Transition of Care Model On Hospital Diabetic Ketoacidosis Readmission Rates: A Pilot Study Amrita Dhillon 1, Bridget Akel 2, Ruban Dhaliwal 3, Prashant Nadkarni 3, Nidhi Bansal 3 1 Department
Impact of Transition of Care Model On Hospital Diabetic Ketoacidosis Readmission Rates: A Pilot Study Amrita Dhillon 1, Bridget Akel 2, Ruban Dhaliwal 3, Prashant Nadkarni 3, Nidhi Bansal 3 1 Department
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care
 Accelero Health Partners, 2015 WHITE PAPER Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Jason Pry, Senior Director ABSTRACT Every year more than a quarter of a million
Accelero Health Partners, 2015 WHITE PAPER Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Jason Pry, Senior Director ABSTRACT Every year more than a quarter of a million
Lung Day University of Washington. June 17, Translating Data Into Practice in the MICU. Richard K. Albert, M.D.
 Lung Day 2011 University of Washington June 17, 2011 Translating Data Into Practice in the MICU Richard K. Albert, M.D. Chief of Medicine Denver Health Professor of Medicine University of Colorado Adjunct
Lung Day 2011 University of Washington June 17, 2011 Translating Data Into Practice in the MICU Richard K. Albert, M.D. Chief of Medicine Denver Health Professor of Medicine University of Colorado Adjunct
Across The Chasm: The Transition From Volume To Value
 Across The Chasm: The Transition From Volume To Value Joseph Bisordi, MD, Executive Vice President & CMO Ochsner Health System Our Mission is to Serve, Heal, Lead, Educate, and Innovate $1.6 Revenue ($B)
Across The Chasm: The Transition From Volume To Value Joseph Bisordi, MD, Executive Vice President & CMO Ochsner Health System Our Mission is to Serve, Heal, Lead, Educate, and Innovate $1.6 Revenue ($B)
Standard Operating Procedure 11. Completion of DAFNE Data Collection: Full Post Course Form F04.010, Version 8
 Standard Operating Procedure 11 Completion of DAFNE Data Collection: Full Post Course Form F04.010, Version 8 Date Version Issue Review Contact Approved Date Date Person October 2013 9 October 2013 March
Standard Operating Procedure 11 Completion of DAFNE Data Collection: Full Post Course Form F04.010, Version 8 Date Version Issue Review Contact Approved Date Date Person October 2013 9 October 2013 March
FINANCES OF PALLIATIVE CARE
 FINANCES OF PALLIATIVE CARE Andrew Molosky, MBA Vice President of Operations Seasons Hospice & Palliative Care Learning Objectives: Distinguish and identify the unique needs of one's organization as it
FINANCES OF PALLIATIVE CARE Andrew Molosky, MBA Vice President of Operations Seasons Hospice & Palliative Care Learning Objectives: Distinguish and identify the unique needs of one's organization as it
Monthly Campaign Webinar February 21, 2019
 Monthly Campaign Webinar February 21, 2019 2 Today s Webinar Together 2 Goal Updates Webinar Reminders AMGA Annual Conference New Campaign Partnership 2019 Million Hearts Hypertension Control Challenge
Monthly Campaign Webinar February 21, 2019 2 Today s Webinar Together 2 Goal Updates Webinar Reminders AMGA Annual Conference New Campaign Partnership 2019 Million Hearts Hypertension Control Challenge
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care
 Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Every year more than a quarter of a million people over the age of 65 are admitted to a hospital with a hip fracture. Mortality
Accelero Identifies Opportunities to Provide Greater Value in Hip Fracture Care Every year more than a quarter of a million people over the age of 65 are admitted to a hospital with a hip fracture. Mortality
Montgomery General Hospital- Medstar Healthcare Improving Glycemic Control to Enhance Patient Outcomes
 Organization: Solution Title: Montgomery General Hospital- Medstar Healthcare Improving Glycemic Control to Enhance Patient Outcomes Program/Project Description:What was the problem to be solved? How was
Organization: Solution Title: Montgomery General Hospital- Medstar Healthcare Improving Glycemic Control to Enhance Patient Outcomes Program/Project Description:What was the problem to be solved? How was
Getting Off the Merry-Go-Round Reducing Readmissions for Patients with Diabetes
 Getting Off the Merry-Go-Round Reducing Readmissions for Patients with Diabetes Kristi Kulasa, MD Associate Clinical Professor of Medicine Director, Inpatient Glycemic Control University of California
Getting Off the Merry-Go-Round Reducing Readmissions for Patients with Diabetes Kristi Kulasa, MD Associate Clinical Professor of Medicine Director, Inpatient Glycemic Control University of California
Reducing COPD Exacerbation Readmissions in a Community-Based Teaching Hospital
 Reducing COPD Exacerbation Readmissions in a Community-Based Teaching Hospital Dawn Waddell, PharmD, BCPS Clinical Pharmacy Manager Lisa Kingdon, PharmD, BCPS Clinical Pharmacy Specialist Dawn Waddell
Reducing COPD Exacerbation Readmissions in a Community-Based Teaching Hospital Dawn Waddell, PharmD, BCPS Clinical Pharmacy Manager Lisa Kingdon, PharmD, BCPS Clinical Pharmacy Specialist Dawn Waddell
Physician Orders PEDIATRIC: LEB DKA Diabetes Mellitus Admit Plan
 Initiate Orders Phase Non Categorized R Powerplan Open Care Sets/Protocols/PowerPlans Initiate Powerplan Phase Phase: Admit DKA Two-Bag Calculations Phase, When to Initiate: Initiate Powerplan Phase Phase:
Initiate Orders Phase Non Categorized R Powerplan Open Care Sets/Protocols/PowerPlans Initiate Powerplan Phase Phase: Admit DKA Two-Bag Calculations Phase, When to Initiate: Initiate Powerplan Phase Phase:
How Doctors Choose Medicines when Treating Patients with Type 2 Diabetes
 HARVARD MEDICAL SCHOOL How Doctors Choose Medicines when Treating Patients with Type 2 Diabetes Richard W. Grant MD MPH Endocrine Society Beta Cell meeting January 9-10, 2009 Outline Background Observed
HARVARD MEDICAL SCHOOL How Doctors Choose Medicines when Treating Patients with Type 2 Diabetes Richard W. Grant MD MPH Endocrine Society Beta Cell meeting January 9-10, 2009 Outline Background Observed
Welcome Everyone. Monitoring, Sick Days, Inpatient Management - Objectives. Mrs. Jones has new diabetes. She asks you: Page 1
 Welcome Everyone Sign-In Enjoy Breakfast Meet someone new Enter Raffle Pick a team name Please silence phones We start at 8:00am Monitoring, Sick Days, Inpatient Management - Objectives Objectives: Strategies
Welcome Everyone Sign-In Enjoy Breakfast Meet someone new Enter Raffle Pick a team name Please silence phones We start at 8:00am Monitoring, Sick Days, Inpatient Management - Objectives Objectives: Strategies
Huangdao People's Hospital
 Table of contents 1. Background... 3 2. Integrated care pathway implementation... 6 (1) Workload indicators... 6 A. In eligible for care pathway... 6 B. Care pathway implementation... 7 (2) Outcome indicators...
Table of contents 1. Background... 3 2. Integrated care pathway implementation... 6 (1) Workload indicators... 6 A. In eligible for care pathway... 6 B. Care pathway implementation... 7 (2) Outcome indicators...
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline
 Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
TACKLING COPD READMISSIONS. Wendy Presley RN
 TACKLING COPD READMISSIONS Wendy Presley RN WHY START WITH COPD? HIGH VOLUME PROBLEM PRONE COSTLY And you just can t resist a challenge Chronic Obstructive Pulmonary Disease (COPD) is a preventable and
TACKLING COPD READMISSIONS Wendy Presley RN WHY START WITH COPD? HIGH VOLUME PROBLEM PRONE COSTLY And you just can t resist a challenge Chronic Obstructive Pulmonary Disease (COPD) is a preventable and
Health Services & High Risk Admissions Registries. David Carnahan, MD MSCE DHA CEI Branch Chief 12 June 2014
 Health Services & High Risk Admissions Registries David Carnahan, MD MSCE DHA CEI Branch Chief 12 June 2014 Introduction Background Information Variables of Interest (potential markers) ACG Use case Readmissions
Health Services & High Risk Admissions Registries David Carnahan, MD MSCE DHA CEI Branch Chief 12 June 2014 Introduction Background Information Variables of Interest (potential markers) ACG Use case Readmissions
DIAGNOSIS OF DIABETES NOW WHAT?
 DIAGNOSIS OF DIABETES NOW WHAT? DISCUSS GOALS FOR DIABETES CARE IDENTIFY COMMON COMPLIANCE- ADHERENCE ISSUES DESCRIBE TECHNOLOGY TO ASSIST AND / OR IMPROVE DIABETES CARE WHAT DO WE WANT OUR PATIENTS TO
DIAGNOSIS OF DIABETES NOW WHAT? DISCUSS GOALS FOR DIABETES CARE IDENTIFY COMMON COMPLIANCE- ADHERENCE ISSUES DESCRIBE TECHNOLOGY TO ASSIST AND / OR IMPROVE DIABETES CARE WHAT DO WE WANT OUR PATIENTS TO
Dana L. Gilbert Chief Operating Officer Sharon Rudnick Vice President Outpatient Care Management
 Ambulatory Sensitive Admissions Dana L. Gilbert Chief Operating Officer Sharon Rudnick Vice President Outpatient Care Management 1 Sites Of Care Advocate Health Care 12 Hospitals 10 acute care hospitals
Ambulatory Sensitive Admissions Dana L. Gilbert Chief Operating Officer Sharon Rudnick Vice President Outpatient Care Management 1 Sites Of Care Advocate Health Care 12 Hospitals 10 acute care hospitals
Burden of Hospitalizations Primarily Due to Uncontrolled Diabetes: Implications of Inadequate Primary Health Care in the United States
 Diabetes Care In Press, published online February 8, 007 Burden of Hospitalizations Primarily Due to Uncontrolled Diabetes: Implications of Inadequate Primary Health Care in the United States Received
Diabetes Care In Press, published online February 8, 007 Burden of Hospitalizations Primarily Due to Uncontrolled Diabetes: Implications of Inadequate Primary Health Care in the United States Received
Insulin Pump An information session to help you decide if you are ready to use an insulin pump.
 Insulin Pump An information session to help you decide if you are ready to use an insulin pump. Welcome Welcome to the insulin pump information session. We hope this session helps you to decide whether
Insulin Pump An information session to help you decide if you are ready to use an insulin pump. Welcome Welcome to the insulin pump information session. We hope this session helps you to decide whether
Adherence to pediatric diabetic ketoacidosis guidelines by community emergency departments providers
 Zee-Cheng et al. International Journal of Emergency Medicine (2017) 10:11 DOI 10.1186/s12245-017-0137-8 International Journal of Emergency Medicine ORIGINAL RESEARCH Open Access Adherence to pediatric
Zee-Cheng et al. International Journal of Emergency Medicine (2017) 10:11 DOI 10.1186/s12245-017-0137-8 International Journal of Emergency Medicine ORIGINAL RESEARCH Open Access Adherence to pediatric
Diabetic Ketoacidosis
 October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
Spending More to Save More CareMore Health Plan. Douglas Allen, MD., MMM.
 Spending More to Save More CareMore Health Plan Douglas Allen, MD., MMM. CareMore History Staff Model Medical Group Iterative, Intuitive, Care Model Development NP based programs starting with diabetes
Spending More to Save More CareMore Health Plan Douglas Allen, MD., MMM. CareMore History Staff Model Medical Group Iterative, Intuitive, Care Model Development NP based programs starting with diabetes
With Dr. Sarah Reid and Dr. Sarah Curtis
 5. Headaches 6. Known diabetes 7. Specific high risk groups (ie. Teenagers, children on insulin pumps and those from lower socio-economic status). Episode 63 Pediatric Diabetic Ketoacidosis With Dr. Sarah
5. Headaches 6. Known diabetes 7. Specific high risk groups (ie. Teenagers, children on insulin pumps and those from lower socio-economic status). Episode 63 Pediatric Diabetic Ketoacidosis With Dr. Sarah
The Diamond Study: Continuous Glucose Monitoring In Patients on Mulitple Daily Insulin Injections
 8/5/217 The Diamond Study: Continuous Glucose Monitoring In Patients on Mulitple Daily Insulin Injections Richard M. Bergenstal, MD Executive Director International Diabetes Center at Park Nicollet Minneapolis,
8/5/217 The Diamond Study: Continuous Glucose Monitoring In Patients on Mulitple Daily Insulin Injections Richard M. Bergenstal, MD Executive Director International Diabetes Center at Park Nicollet Minneapolis,
The Role of the Diabetes Educator within the Patient-Centered Medical Home & Future Roles
 The Role of the Diabetes Educator within the Patient-Centered Medical Home & Future Roles Linda M. Siminerio, RN, PhD, CDE Professor of Medicine University of Pittsburgh School of Medicine & Nursing Objectives
The Role of the Diabetes Educator within the Patient-Centered Medical Home & Future Roles Linda M. Siminerio, RN, PhD, CDE Professor of Medicine University of Pittsburgh School of Medicine & Nursing Objectives
SARASOTA MEMORIAL HOSPITAL
 SARASOTA MEMORIAL HOSPITAL TITLE: NURSING PROCEDURE MANAGEMENT OF PATIENT S OWN INSULIN PUMP/CONTINUOUS SUBCUTANEOUS INSULIN INFUSION PUMP (dia13) DATE: REVIEWED: PAGES: 08/84 11/18 1 of 7 PS1094 ISSUED
SARASOTA MEMORIAL HOSPITAL TITLE: NURSING PROCEDURE MANAGEMENT OF PATIENT S OWN INSULIN PUMP/CONTINUOUS SUBCUTANEOUS INSULIN INFUSION PUMP (dia13) DATE: REVIEWED: PAGES: 08/84 11/18 1 of 7 PS1094 ISSUED
Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State. Adam Bursua, Pharm.D., BCPS
 Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State Adam Bursua, Pharm.D., BCPS Objectives Describe the epidemiology of diabetic ketoacidosis (DKA) and the hyperglycemic hyperosmolar
Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State Adam Bursua, Pharm.D., BCPS Objectives Describe the epidemiology of diabetic ketoacidosis (DKA) and the hyperglycemic hyperosmolar
Hypoglycaemia in the community
 Hypoglycaemia in the community Using local data to monitor the quality of diabetes services Adrian R Scott 11 th April 2008 Sheffield Teaching Hospitals NHS Foundation Trust DCCT: the price of improved
Hypoglycaemia in the community Using local data to monitor the quality of diabetes services Adrian R Scott 11 th April 2008 Sheffield Teaching Hospitals NHS Foundation Trust DCCT: the price of improved
Disclosures. Learning Objectives 4/26/2017
 Implementation of a quality improvement initiative to ensure the safe transition from prior-to-admission concentrated insulins to a formulary insulin regimen ERICA J. RHEIN, PHARMD PGY1 PHARMACY PRACTICE
Implementation of a quality improvement initiative to ensure the safe transition from prior-to-admission concentrated insulins to a formulary insulin regimen ERICA J. RHEIN, PHARMD PGY1 PHARMACY PRACTICE
Mentors on Discharge
 Mentors on Discharge Repeated psychiatric hospitalizations are costly, impede recovery and are demoralizing to individuals, families, and clinicians. Between 40 to 50 percent of patients with a history
Mentors on Discharge Repeated psychiatric hospitalizations are costly, impede recovery and are demoralizing to individuals, families, and clinicians. Between 40 to 50 percent of patients with a history
Welcome to CareLink Pro
 Reference Guide Welcome to CareLink Pro This guide was developed to serve as a reference for obtaining patient data and reviewing CareLink Pro reports. Getting Started with CareLink Pro Adding New Patients
Reference Guide Welcome to CareLink Pro This guide was developed to serve as a reference for obtaining patient data and reviewing CareLink Pro reports. Getting Started with CareLink Pro Adding New Patients