Nottingham Neonatal Service Guideline
|
|
|
- Phebe Bryan
- 5 years ago
- Views:
Transcription
1 Title: Screening and Management of Neonatal Hypoglycaemia Version: 10 Ratification Date: Review Date: Jan 2023 Approval: Nottingham Neonatal Service Clinical Guideline Meeting Author: Shalini Ojha 1, Lara Shipley 2, Stephen Wardle, Helen Giddins Previous versions: V7: Lisa Barker, Chris Jarvis, Helen Budge, Judith Grant; V6: Neil Marlow, Jane Porter, Alison Atkinson, Trudi Cameron Job Title: 1 Consultant Neonatologist, 2 Specialist Trainee, Paediatrics, Consultation: Nottingham Neonatal Service Staff and Clinical Guideline Meeting, Midwifery Services Guideline Dr Stephen Wardle Consultant Neonatologist co/ Stephanie Tyrrell, Contact Nottingham Neonatal Service stephanie.tyrrell@nuh.nhs.uk Distribution: Nottingham Neonatal Service, Neonatal Intensive Care Units Target audience: Staff of the Nottingham Neonatal Service, Delivery Suites and Postnatal Wards Patients to whom Patients of the Nottingham Neonatal Service and newborn infants on the this applies: Postnatal Wards and Labour Suites of the Nottingham University Hospitals NHS Trust who fit the inclusion criteria of the guideline below Key Words: Neonatal hypoglycaemia Risk Managed: Neonatal hypoglycaemia and its complications Evidence used: The contemporary evidence base has been used to develop this guideline. References to studies utilised in the preparation of this guideline are given at its end. Clinical guidelines are guidelines only. The interpretation and application of clinical guidelines remain the responsibility of the individual clinician. If in doubt, contact a senior colleague. Caution is advised when using guidelines after the review date. This guideline has been registered with the Nottingham University Hospitals NHS Trust. The Hypoglycaemia Guideline will be monitored in conjunction with the NUH Maternity Services Clinical and Operational Monitoring Plan. Key recommendations for blood glucose measurements in newborn infants: Blood glucose measurement is indicated: if the baby is at risk (see Table 3) if symptoms suggestive of hypoglycaemia are present in the investigation of coma or convulsions during neonatal intensive care Key practice points: An infant who is unrousable for a feed should be screened for hypoglycaemia. Jitteriness alone is not a reason to measure blood glucose. Jitteriness is defined as involuntary, symmetrical rhythmical movement that can be stopped by gently flexing or holding the limb.
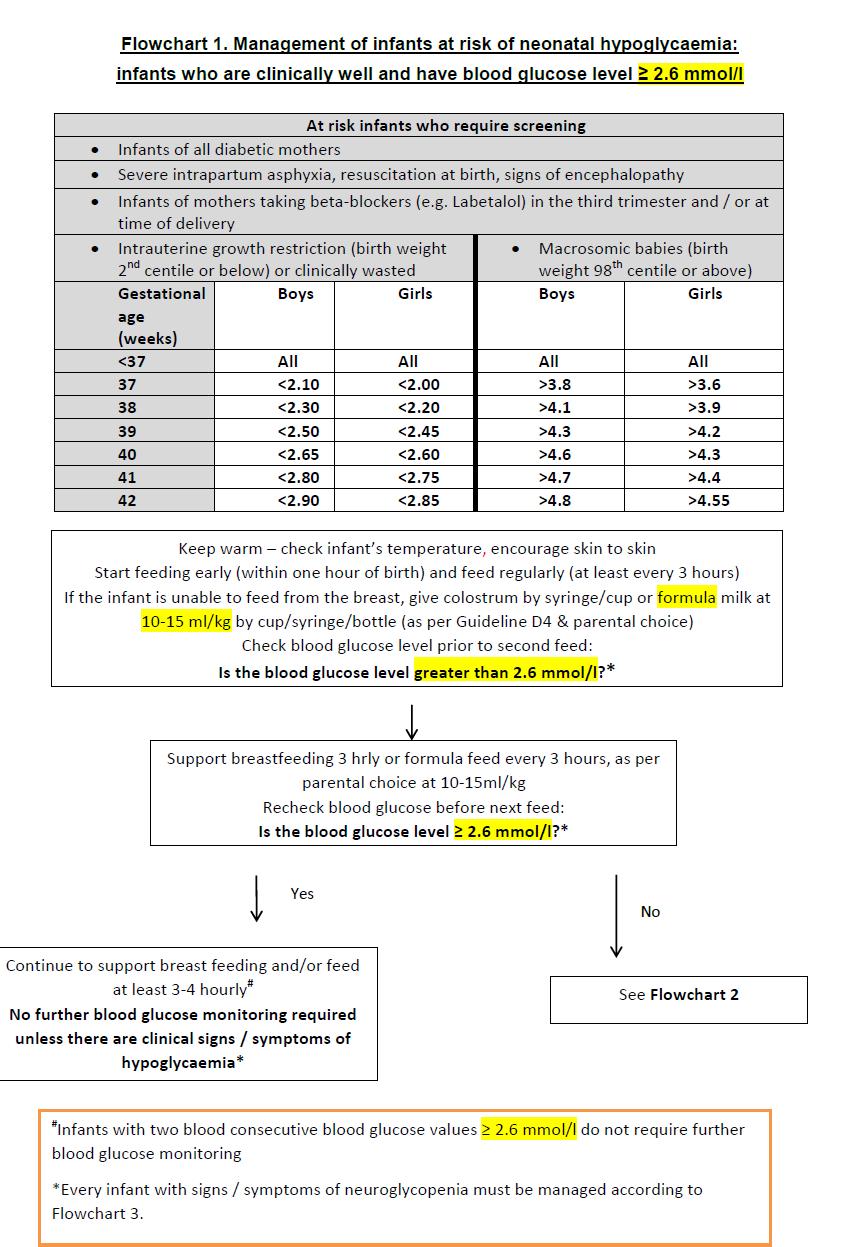
2 QUICK REFERENCE GUIDE FOR STAFF ON THE LABOUR SUITE OR POSTNATAL WARDS Please note only to be used in conjunction with the full neonatal guideline Newborn infants at risk of hypoglycaemia: Preterm (less than 37 weeks gestation) Birth weight less than 2 nd centile (see Table below) Large for gestational age (see Table below) Maternal diabetes Infants of mothers taking beta-blockers (e.g. Labetalol) in the third trimester and / or at time of delivery Severe intrapartum asphyxia, resuscitation at birth Ill babies (e.g infection, grunting) Babies with a low temperature Babies with congenital disorders (Beckwith-Weidermann) Intrauterine growth restriction (birth weight 2nd centile or below) Macrosomic babies (birth weight 98th centile or above) Gestational age (weeks) Boys Girls Boys Girls <37 All All All All 37 <2.10 <2.00 >3.8 > <2.30 <2.20 >4.1 > <2.50 <2.45 >4.3 > <2.65 <2.60 >4.6 > <2.80 <2.75 >4.7 > <2.90 <2.85 >4.8 >4.55 Healthy term babies have an innate ability to use alternative fuel stored in their bodies for energy if they don t consume calories via milk. This is called counter regulation.
3 Healthy term babies are therefore probably not at risk of coming to harm due to hypoglycaemia in the first few days of life. However, some babies, such as those listed as at risk of hypoglycaemia (see above) may not be able to use these alternative fuels and need to be fed regularly and have their blood sugar levels monitored. It is essential these babies undergo early feeding and skin to skin care is encouraged to keep baby warm. Even a small amount of colostrum can raise the blood glucose level. If parents wish to use formula feed this is also satisfactory. Currently blood glucose less than 2.6 mmol/l is considered neonatal hypoglycaemia. Infants with two pre feed blood glucose readings equal to or more than 2.6 mmol/l at least 3 hours apart can discontinue blood glucose monitoring. Blood sugar levels If the blood glucose is 2.6 mmol/l or above and showing no signs of hypoglycaemia continue with FLOWCHART 1 If the blood glucose is between 1.0 and 2.6 mmol/l and showing no signs of hypoglycaemia, go to FLOWCHART 2 If the blood glucose is between mmol/l for more than two measurements contact a neonatal doctor as the baby may need NICU admission and assessment for causes of persistent hypoglycaemia If the blood glucose is under 1 mmol/l or symptomatic, go to FLOWCHART 3 and refer immediately to a neonatologist. Symptomatic hypoglycaemia: If a newborn is unwell or shows signs of hypoglycaemia): Change in level of consciousness: stupor or lethargy or irritability Hypotonia, inactivity Seizures High-pitched cry, poor feeding Hypothermia Respiratory depression: cyanosis, apnoea The neonatal ST1-3 doctor should be informed urgently. * Crash call neonatal team on 2222 via switchboard
4 1 Background In majority of healthy neonates, the frequently observed low blood glucose concentrations are not related to any significant problem and merely reflect normal processes of metabolic adaptation to extra-uterine life [1]. However, when low blood glucose levels are prolonged or recurrent, they may result in acute systemic effects and other neurologic sequelae. In addition, in a small number of infants, who may have maladaptation of glucose homeostasis, blood glucose monitoring and proactive management is required. 1.1 Extra-uterine adaption of glucose homeostasis The fetus depends entirely on maternal supply and facilitated diffusion across the placenta to maintain glucose levels and, under normal condition, gluconeogenesis appears only after birth. Following the clamping of the umbilical cord, blood glucose concentration decreases rapidly followed by a gradual stabilisation over the next 6-12 hours. Studies have demonstrated a wide range of glucose concentrations during the first 72 hours, with values ranging from mmol/l in healthy breast fed infants [2] [3]. Low plasma glucose activates a number of counter-regulatory pathways resulting in increased systemic lipolysis with ketone utilisation by the brain [3]. Other alternative fuels such as pyruvate and lactate are also utilised by the brain and, as a result of these, the healthy newborn infant is probably not at risk of hypoglycaemia associated neuronal injury over the first few days. In contrast, preterm infants and those with altered homeostasis due to hyperinsulinemic states or intrauterine growth restriction may not produce alternative metabolites and are, therefore, at higher risk. 1.2 Definition of hypoglycaemia Significant hypoglycaemia cannot be defined by a single number that can be applied universally to every infant but may be unique to each individual and vary with their physiologic stage as well as any existent pathology. To deal with such uncertainty, an operational threshold has been suggested as the concentration of plasma or blood glucose at which clinicians should consider intervention, based on the evidence currently available in the literature [1]. Recent guidance from the AAP [4] and NICE [5] have recommended changing practice from a definitive threshold level for treatment of hypoglycaemia to an operational threshold of 2.0 mmol/l with a therapeutic goal of 2.6 mmol/l. Current guidance recommends initiating intervention for hypoglycaemia following two consecutive blood sugars of < 2.0 mmol/l. Furthermore, BAPM guidance [6] has also recommended an operational threshold approach, which advocates using 2.0mmol/l for infants who are at risk of hypoglycaemia but not exhibiting symptoms. For infants who are at risk of hypoglycaemia, we consider the value for blood glucose at which intervention is warranted to be 2.6 mmol/l but this will be reviewed in light of the above guidance and may be changed in the future. This recent change in guidance is based on several studies which do not support the original study advocating 2.6 mmol/l as a definitive cut off level for hypoglycaemia. Lucas et al. reported that infants with recurrent episodes of blood glucose levels < 2.6 mmol/l had a significantly reduced developmental score at 18 months corrected age and has a 3.5 times increased incidence of neurodevelopmental impairment (95% confidence interval (CI) )[7]. However, the infants included in this study were preterm (mean (standard deviation) gestational age 30.5 (2.7) weeks) and was subjected to both sample and recall bias. Importantly, the authors state that confounding factors, which could contribute to neurodevelopmental impairment were not accounted for in their analysis, therefore, the association between modest hypoglycaemia and poor neurodevelopmental might not be casual but merely a failure to adequately adjust for confounding factors. More recently,
5 McKinlay et al. demonstrated that neonatal hypoglycaemia, when treated to maintain a blood glucose concentration of at least 2.6 mmol/l (equivalent to 47 mg/dl), was not associated with adverse neurological outcomes [8] Furthermore, Tin et al followed up 781 preterm infants (< 32 weeks) at both 2yrs and 15 yrs of age, who had recurrent episodes of blood glucose <2.6mmol/l and found no difference in neurodevelopmental outcome compared to matched controls [9] Recommendation: Infants with a single blood sugar < 1.0 mmol/l or symptomatic infants with a blood sugar < 2.6 mmol/l require intervention for hypoglycaemia until two consecutive readings above 2.6 mmol/l are obtained.
6 2 Measurement of blood glucose On the NICU, blood glucose measurement should be made using the blood gas machine. If this facility is unavailable, a blood glucose test should be sent to the laboratory. The point of care glucose stick meters may be inaccurate in their estimation of hypoglycaemia, particularly in the presence of conditions such as high haematocrit, high blood oxygen tension and acidosis [10] [11]. These should not be used in the NICU. On the postnatal wards, where access to a blood gas machine is not immediate, initial blood glucose measurement may be made using a new generation glucose stick test. However, if the result obtained using this method is <2.0 mmol/l, it must always be re-checked immediately by undertaking a repeat measurement from the blood gas machine or a laboratory sample. Recommendation: - In NICU and on Labour Suite: all samples taken for blood glucose levels should be measured on a blood gas machine - On postnatal wards: blood glucose levels may be measured with bedside glucose sticks but values < 2.0 mmol/l should be confirmed by the gas machine or a laboratory sample 3 Symptoms of hypoglycaemia Infants may manifest neuroglycopenic signs and symptoms when blood glucose level is low. These can be subtle and are often non-specific such as those given in Table 1. However, it is vital that infants with signs/symptoms of neuroglycopenia are treated as these infants are generally considered at risk of poor neurological outcome. If truly caused by hypoglycaemia, such signs are relatively easily and quickly reversed by normalisation of glucose levels. Table 1. Features of neuroglycopenia in newborn infants Change in level of consciousness: stupor or lethargy or irritability Hypotonia, inactivity Seizures High-pitched cry, poor feeding Hypothermia Respiratory depression: cyanosis, apnoea 4 Causes of hypoglycaemia in newborn infants Neonatal hypoglycaemia may occur due to conditions that interrupt the normal extra-uterine adaptation of glucose metabolism or may be a consequence of a co-existing pathology. Some of the conditions that pre-dispose a newborn infant to low blood glucose levels are listed below. Table 2. Some conditions that predispose to hypoglycaemia Prematurity Intra-uterine growth restriction and low birth weight Sepsis Perinatal stress such as hypoxia-ischemia, respiratory distress, meconium aspiration Hypothermia Maternal drugs such as Tolbutamide and beta blockers, e.g. Labetalol, Polycythaemia
7 Congenital disorders such as Beckwith-Weidemann, presence of midline defects Hyperinsulinaemic states such as in infants of diabetic mothers, congenital hyperinsulinemia Inborn errors of metabolism such as galactosaemia, beta oxidation defects, glycogen storage diseases 5 Infants who require blood glucose monitoring Normal term infants (> 37 weeks gestation) who are bottle / breast feeding do not require blood glucose monitoring unless they have a predisposing factor (Table 2) or are unwell. As discussed in Section 1.1, term healthy infants may have low blood glucose levels which are normal and safe. Infants at risk of maladaptation of glucose homeostasis should be proactively identified and treated. Infants who require screening and proactive management of neonatal hypoglycaemia are listed in Table 3. These infants are at increased risk of hypoglycaemia and require regular blood glucose monitoring until it is established that they have made a successful transition to extra-uterine glucose homeostasis. Blood glucose must also be tested in any infant who has symptoms of neuroglycopenia (Table 1). Recommendation: Infants in the at-risk groups require regular blood glucose monitoring and proactive management to maintain blood glucose levels above a level of 2.6 mmol/l (Table 3) 5.1 Infants of diabetic mothers The following recommendations are adapted from the NICE guidelines for management of diabetes in pregnancy [5] Infants of women with diabetes should stay with their mothers unless there is a clinical complication or there are abnormal signs that warrant admission for intensive or special care Blood glucose testing should be carried out routinely 2-4 hours after birth Infants of women with diabetes should not be transferred to community care until they are at least 24 hours old and not before it is ensured that the infant is maintaining blood glucose levels and is feeding well. 5.2 Clinical macrosomia Infants with birth weight 4.5kg are considered macrosomic irrespective of gestational age. However, many infants can have features of fetal overgrowth even when they may not have reached this weight cut off for macrosomia. Such babies may appear fat i.e. excess subcutaneous fat such as chubby cheeks. Infants born to women with gestational diabetes, overweight or obese mothers or women with excess gestational weight gain may be at risk of the macrosomic phenotype. Despite being <4.5kg, these infants may be at increased risk of hypoglycaemia. Infants who are greater than 98 th centile in weight for their gestational age (Table 3 or use individualised growth chart) are more likely to have excess fetal growth and may also be considered at risk for hypoglycaemia.
8 Table 3 Infants who require screening and proactive management of neonatal hypoglycaemia The following groups are at risk of neurological sequelae of neonatal hypoglycaemia, and measures should be in place to identify them at birth for early milk / energy provision and monitoring of blood glucose concentration Infants of all diabetic mothers Infants of mothers taking beta-blockers (e.g. Labetalol) in the third trimester and / or at time of delivery Intrauterine growth restriction (birth Macrosomic babies (birth weight 2 nd centile or below) or clinically weight 98 th centile or above) wasted Gestational age (weeks) Boys Girls Boys Girls <37 All All All All 37 <2.10 <2.00 >3.8 > <2.30 <2.20 >4.1 > <2.50 <2.45 >4.3 > <2.65 <2.60 >4.6 > <2.80 <2.75 >4.7 > <2.90 <2.85 >4.8 > Prevention and management of hypoglycaemia Women should be encouraged to have skin to skin contact with their baby as soon as possible after birth, which will help maintain normothermia and encourage breastfeeding. Babies should not be separated from their mothers for management of hypoglycaemia wherever possible. 6.1 At-risk babies on postnatal ward, labour suite or the neonatal unit: Flowchart 1 describes the initial management of all infants who fall in at-risk categories listed in Table Infants of diabetic mothers The following recommendations are adapted from the NICE guidelines for management of diabetes in pregnancy [5] Infants of women with diabetes should stay with their mothers unless there is a clinical complication or there are abnormal signs that warrant admission for intensive or special care
9 Blood glucose testing should be carried out routinely 2-4 hours after birth Infants of women with diabetes should not be transferred to community care until they are at least 24 hours old and not before it is ensured that the infant is maintaining blood glucose levels and is feeding well. 6.3 Clinical macrosomia Infants with birth weight >98 th centile considered macrosomic. However, many infants can have features of fetal overgrowth even when they may not have reached this weight cut off for macrosomia. Such babies may appear fat i.e. excess subcutaneous fat such as chubby cheeks. Infants born to women with gestational diabetes, overweight or obese mothers or women with excess gestational weight gain may be at risk of the macrosomic phenotype. Despite being <4.5kg, these infants may be at increased risk of hypoglycaemia. Infants who are greater than 98 th centile in weight for their gestational age (Table 3 or use individualised growth chart) are more likely to have excess fetal growth and may also be considered at risk for hypoglycaemia. 6.4 Management of hypoglycaemia in babies on postnatal ward, labour suite or the neonatal unit: Flowchart 2 describes the management of all infants whose blood glucose is between 1.0mmol/l to 2.6mmol/l and have no abnormal clinical signs. 6.5 Management of infants with persistent low blood glucose, symptomatic infants and those with blood glucose <1mmol/l A summary of management of this group of infants is given in Flowchart 3. The information in Flowchart 3 should be used in conjunction with the following: Continue milk feeds Milk feeds (breastmilk) should be continued whenever possible and safe to do so. Galactose derived from hydrolysis of lactose in the gut increases hepatic glycogen production and allows for sustained between-feeding hepatic glucose release [12]. Feeds also induce production of intestinal peptides such as incretins that promote insulin secretion at a steadier pace than the spikes seen with intravenous bolus of glucose. Milk feeds also increase levels of alternative fuels such as ketones derived from fatty acids in milk and amino acids which are substrates for gluconeogenesis. Feed volumes may be increased to at least a day ahead of usual fluid requirement (refer to Guidelines D2 and D3) and may even be increased further, as tolerated Intravenous 10% glucose bolus and use of oral glucose gel Infants with very low blood glucose (< 1mmol/l) or signs / symptoms of neuroglycopenia should receive a bolus of 10% glucose (2.5ml/kg) as soon as intravenous access is obtained and blood samples taken for tests for hypoglycaemia. Any intravenous bolus of glucose must be followed by increasing the amount of carbohydrate delivered to avoid the risk of rebound hypoglycaemia. Only 10% glucose should be used for intravenous boluses of glucose greater concentrations of glucose must never be given as boluses. If intravenous access is not readily obtainable, 200 mg/kg of oral glucose gel (0.5ml/kg of 40% glucose gel) may be administered in to the oral mucosa while intravenous access is established. A feed should be given after this bolus. A randomised controlled trial of glucose gel (200 mg/kg) vs. placebo for management of hypoglycaemia in weeks in the first 48 hours of life demonstrated that
10 treatment with 40% glucose gel was effective in reversal of hypoglycaemia without increasing the risk of rebound hypoglycaemia and was not associated with adverse effects [13]. Infants who require IV or oral bolus of glucose should be admitted to the NICU and adequate blood glucose levels with milk feeds must be established prior to discharge Monitor fluid electrolyte balance A combination of IV glucose with the continuation of enteral feeding can result in large volumes of fluid being administered to infants with hypoglycaemia. A careful assessment of fluid and electrolyte balance with monitoring of urinary output and serum electrolytes is required. Large fluid volumes may be administered inadvertently. This may be avoided by using higher concentration of glucose to limit the volume delivered. Large volume of IV fluids without adequate electrolytes may cause dangerous electrolyte imbalances. Serum electrolytes must be monitored regularly and electrolytes should be added to IV fluids as required. 6.6 Infants with signs / symptoms of neuroglycopenia Establish IV access Obtain blood samples for hypoglycaemia screen (ensure minimal delay in treatment to obtain blood samples) Give a bolus of IV glucose (2.5ml/kg) followed by continuous glucose infusion at ml/kg/d Check blood glucose 30 min after and monitor regularly. If blood glucose remains low, increase glucose delivery as given in Section 6.8. In the absence of clearly identifiable risk factors (as in Table 3 or if the infant has hypoglycaemic encephalopathy, investigation of the underlying cause of hypoglycaemia is mandatory (consider the conditions listed in Table 2 or other possible differential diagnoses). Investigations should be undertaken as soon as possible after the low blood glucose result (Appendix 12.1). 6.7 Following intervention, if the blood glucose improves to 2.6 mmol/l Rate of glucose delivery can be reduced if the blood glucose remains stable (i.e. 2.6 mmol/l) on two consecutive measurements. Intravenous glucose should be gradually reduced and enteral feeding continued with monitoring of pre-feed blood glucose with each blood glucose level >2.6 mmol/l. When the infant is on full enteral feeds the feed interval can then be gradually increased until 3-4 hourly. Blood glucose monitoring can be discontinued following two consecutive levels >2.6mmol/l whilst on 3-4 hourly feeds. 6.8 Following intervention, if the blood glucose remains between 1.0 to 2.5 mmol/l and there are no abnormal clinical signs Consider the following: Increase feed volume if tolerated and appropriate Decrease feed intervals to hourly feeds If / when the feed interval is hourly and the feed volume cannot be increased any further (e.g. infant is unable to tolerate larger volume of milk such as due to vomiting/ large gastric aspirates):
11 increase volume of intravenous glucose infusion, if fluid electrolyte balance allows (note caution in Section 6.5.3) increase concentration of glucose infusion to deliver more glucose at same or smaller volume of infusion ( Table 4). Central venous access will be required for delivering glucose solutions over 12.5% concentration. 6.9 Choice of enteral feed Enteral feeds should be continued whenever possible. This should preferably be as breast feeds or cup or gastric tube feeds with expressed breast milk (EBM). Appropriate formula for gestational age or birth weight may be given if not breast feeding (see Guideline D4). If feed volume cannot be increased further, or is not being tolerated, then a glucose polymer, such as Maxijul, can be added to EBM or formula milk. Changing to a high energy milk or preterm formula is not recommended as these formulae have higher concentrations of nonglucose components which are not required by infants with hypoglycaemia. The use of glucose polymer and any change from of milk should be discussed with the neonatal consultant. Maxijul can be added to EBM or formula milk to increase the glucose and energy in the same volume of milk (Appendix 12.2). Table 4. Rates of glucose delivery Rate of glucose delivery (mg/kg/min) Strength of IV glucose solution 10% 12.5% 15%* 20%* Fluid infusion rate (ml/kg/d) *15% and 20% glucose solutions must be delivered via a central line Glucose delivery rates in white (in black boxes) indicate the need for investigating for hyperinsulinaemia, particularly when required at > 48 hours of age 7 Glucose utilisation rates If hypoglycaemia persists and / or there is difficulty weaning the IV glucose, glucose utilisation rates should be calculated and IV fluids weaned slowly so that the increase in enteral volume maintains or increases the glucose delivery (See table 7 for enteral feed glucose content).
12 Normal glucose utilisation rates are 4-6 mg/kg/min. Infants in the high-risk groups or those with other pathologies frequently require 6-10 mg/kg/min. The rate of glucose delivery to an infant can be calculated by the formula given below. (%glucosex10) x ml/kg/day %glucose x ml/kg/day = 24 x = glucose infusion rate (mg/kg/min) Infants who require >10 mg/kg/min, particularly beyond the first 48 hours of life usually have a pathological basis for their hypoglycaemia. These cases must be discussed with the Duty Neonatal Consultant and a referral to the Paediatric Endocrinology team considered. 8 Special investigations These are required if: glucose infusion rates to prevent hypoglycaemia are persistently >12 mg/kg/min in a well grown or large for gestational age baby (small for gestational age babies quite often need high glucose infusion rates for several days) there is evidence of hypothalamic dysfunction such as unstable temperature or, in a boy, small or abnormal genitalia profound hypoglycaemia occurs unexpectedly in a well-grown term baby hypoglycaemia is associated with other abnormalities (e.g. exomphalos, coloboma) there is a family history of sudden infant death, Reye syndrome, severe developmental delay, poorly defined neuropathy or myopathy, or other evidence suggestive of an inborn error of metabolism. In children, circulating insulin concentrations are usually undetectable (<1 microu/l) when the blood glucose concentration is <4.5 mmol/l. In the newborn infant, up to 48 hours old, it can be normal to have circulating insulin concentrations up to 10microU/l even when the blood glucose is 3mmol/l or less. However, after this, low blood sugars with detectable insulin levels must be investigated further, in discussion with the consultant and in liaison with the Paediatric Endocrinology team. A list of suggested initial investigations is given in Appendix Ensure that these results have been reviewed and noted prior to discharge. If any result is pending at the time of discharge, this must be mentioned in the discharge summary and communicated to the infant s named Neonatal Consultant. 9 Management of hyperinsulinism Infants who are suspected or confirmed to have hyperinsulinism must be managed in consultation with the Paediatric Endocrinology team and the investigations given in Appendix 12.1 should be augmented, if required, on their advice. A provocative fasting test may be required for identifying the aetiology of hypoglycaemia [11]. This may be performed under supervision of the Paediatric Endocrinologist. Adequate carbohydrate intake at appropriate intervals must be determined prior to discharge and any pharmacological treatment required to decrease insulin secretion should be considered after discussion with Duty Neonatal Consultant and the Paediatric Endocrinologist. These may include such as diazoxide (Proglycem) (starting dose 5 mg/kg/day in 3 divided doses) with chlorothiazide (5 mg/kg twice a day) or somatostatin (as octreotide, 1microgram/kg subcutaneously every 4 hours or as a continuous subcutaneous infusion 0.25micrograms/kg/hour) with glucagon by continuous IV infusion (5 10micrograms/kg/hour). Diazoxide can cause both sodium and water retention causing a
13 potential risk of both hyponatraemia or hypernatraemia and pulmonary hypertension. Chlorthiazide is given alongside diazoxide to reduce the risk of retention, as well as potentiating its glycaemic effect. Referral by the Paediatric Endocrinologist to a centre skilled in the management of these conditions may be required. 10 Going home with Blood Sugar Monitoring A small number of babies may need to go home with blood sugar monitoring. To do so, is a decision made jointly by the Duty Consultant Neonatologist and the Consultant Paediatric Endocrinologist. Infants who have unstable blood glucose and / or require blood sugar monitoring at home should not be discharge unless they are term gestation. Liaison with the Paediatric Endocrinology Nurses is required and parents must receive appropriate training and have follow-up arrangements as per the Children s Hospital guidelines for going home with blood sugar monitoring. 11 Audit points Appropriate screening of infants at risk of neonatal hypoglycaemia Appropriate management of infants with neonatal hypoglycaemia
14 12 Appendix 12.1 Laboratory investigations Table 5. Laboratory investigations required in significant hypoglycaemia Test Sample type Volume Turnaround time Glucose 0.5ml 60 minutes Lactate Blood Fluoride oxalate 0.5ml 60 minutes Free fatty acids (Grey top) 3-hydroxybutyrate 0.5ml One week Ammonia Liver Function Tests Thyroid Function Tests Serum amino acids Blood Lithium heparin (Green top) 2 ml 60 minutes One week Acylcarnitine 1 ml Serum cortisol Insulin C peptide Growth hormone Urine organic acids Urine amino acids Blood Serum (Yellow top) Urine Universal pot 1ml One day 2 ml One week 10 ml One week Urine ketones Bedside stick 1 drop immediate

15 12.2 Addition of glucose polymer If feed volume cannot be increased further or is not being tolerated, the glucose polymer, Maxijul, can be added to EBM or formula milk to increase the glucose and energy in the same volume of milk. Changing to enriched formula milk which increases all nutrition is not recommended. The use of glucose supplements to EBM or formula milk should be discussed with the Attending Neonatal Consultant. Addition of 2 x 2.5ml scoops to either EBM or term formula milk gives approximately 10% concentration of carbohydrate, so increasing milk and decreasing IV 10% dextrose will ensure an equivalent carbohydrate intake (see table 7 below). If Maxijul needs to be added to EBM or formula milk, the possible cause of the hypoglycaemia must be re-evaluated and a hypoglycaemia screen initiated and the Neonatal Dietitian consulted. No scoop other than a small 2.5ml scoop as shown below should be used Table 6. Protein, Carbohydrate and Energy Profile of Milks and Supplements Per 100ml or as stated Protein g Carbohydrate g Energy kcal Breast milk/c&g First Maxijul per100g nil x2.5ml dark blue scoop = 1.3g nil x2.5ml dark blue scoop = 2.6g nil ml EBM/term formula + 1x2.5ml dark blue scoop Maxijul *A small supply of Maxijul in 200g tins + separate 2.5ml scoops are kept on both NICUs. Further supplies are available from the Paediatric Dietitians (ext 63170) at QMC and are ordered by the purchasing team via the Dietetic Dept (ext 57639/8) at City. Out of hours there is an emergency supply on D34, Children s Hospital, QMC, ext There is no scoop in the tin so separate 2.5ml scoops are available on request from the neonatal or children s dietitians. These require washing in hot soapy water and drying with a paper towel before use and then storing in the tin for future use. Tin and scoop should be discarded 1 month after opening.
16 13 References [1] M. Cornblath, Controversies regarding definition of neonatal hypoglycaemia suggesting operational thresholds, Pediatrics, vol. 105, no. 5, pp , [2] I. Swenne, Inter-relationship between serum concentrations of glucose, glucagon and insulin during the first two days of life in healthy newborns, Acta Paediatr, vol. 83, no. 9, pp , [3] W. Hay, Knowledege gaps and research needs for understanding and treating neonatal hypoglycaemia: workshop report from Eunice Kennedy Shriver National Institute of CHild Health and HUman Development, J Pediatr, vol. 155, no. 5, pp , [4] A. Adamkin, Clinical Report- Postnatal Glucose Homeostasis in Late Preterm and Term infants, Pediatrics, vol. 127, pp , [5] NICE, Diabetes in pregnancy: management from preconception to the postnatal period., [6] BAPM, Identification and Management of, [7] A. Lucas, R. Morley and T. Cole, Adverse neurodevelopmental outcome of moderate neonatal hypoglycaemia, BMJ, vol. 297, no. 6, p. 1304, [8] C. McKinley, Neonatal Glycemia and Neurodevelopmental Outcomes at 2 Years, N Engl J Med, vol. 373, no. 16, pp , [9] W. Tin, S. Fritz and G. Brunskill, 15-year follow up of reccurrent hypoglycaemia in preterm infants. [10] K. Bearsley, Measurement of glucose levels in the newborn, Early Hum Dev, vol. 86, no. 5, pp , [11] P. Thornton, Recommendations from the Pediatric Endocrine Society for Evaluation and Management of Persistent Hypoglycemia in Neonates, Infants, and Children., J Pediatr, vol. 167, no. 2, pp , [12] P. Rozance and W. Hay, Describing hypoglycemia--definition or operational threshold?, Early Hum, vol. 86, no. 5, pp , Dev. [13] D. Harris, Dextrose gel for neonatal hypoglycaemia (the Sugar Babies Study): a randomised, double-blind, placebo-controlled trial, Lancet, vol. 382, no. 9910, pp , 2013.
17
18
19
Neonatal Hypoglycaemia Guidelines
 N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed versions of the document. The Intranet should be referred to for the current version of the
N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed versions of the document. The Intranet should be referred to for the current version of the
CARE OF THE NEWBORN HYPOGLYCAEMIA
 CARE OF THE NEWBORN HYPOGLYCAEMIA Background Definition A true blood glucose of less than 2.6 mmol/l venous sample. Neonatal hypoglycaemia is commonly defined as a true blood glucose of less than 2.6 mmol/l
CARE OF THE NEWBORN HYPOGLYCAEMIA Background Definition A true blood glucose of less than 2.6 mmol/l venous sample. Neonatal hypoglycaemia is commonly defined as a true blood glucose of less than 2.6 mmol/l
Guideline for the Prevention and Management of Neonatal Hypoglycaemia GL359
 Guideline for the Prevention and Management of Neonatal Hypoglycaemia GL359 Approval and Authorisation Approved by Job Title Date Paediatric Clinical Chair of Paediatric Clinical Governance Governance
Guideline for the Prevention and Management of Neonatal Hypoglycaemia GL359 Approval and Authorisation Approved by Job Title Date Paediatric Clinical Chair of Paediatric Clinical Governance Governance
Learning Objectives. At the conclusion of this module, participants should be better able to:
 Learning Objectives At the conclusion of this module, participants should be better able to: Treat asymptomatic neonatal hypoglycemia with buccal dextrose gel Develop patient-specific approaches to intravenous
Learning Objectives At the conclusion of this module, participants should be better able to: Treat asymptomatic neonatal hypoglycemia with buccal dextrose gel Develop patient-specific approaches to intravenous
Prevention and Management of Hypoglycaemia of the Breastfed Newborn Reference Number:
 This is an official Northern Trust policy and should not be edited in any way Prevention and Management of Hypoglycaemia of the Breastfed Newborn Reference Number: NHSCT/10/293 Target audience: Midwifery,
This is an official Northern Trust policy and should not be edited in any way Prevention and Management of Hypoglycaemia of the Breastfed Newborn Reference Number: NHSCT/10/293 Target audience: Midwifery,
Guidelines for the Prevention and Management of Hypoglycaemia
 ASHFORD & ST PETER S HOSPITALS NHS TRUST CHILDREN S SERVICES Guidelines for the Prevention and Management of Hypoglycaemia 1. The Care Plan for Prevention of Hypoglycaemia on Labour Ward and the Postnatal
ASHFORD & ST PETER S HOSPITALS NHS TRUST CHILDREN S SERVICES Guidelines for the Prevention and Management of Hypoglycaemia 1. The Care Plan for Prevention of Hypoglycaemia on Labour Ward and the Postnatal
Neonatal Hypoglycemia
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Neonatal Hypoglycemia. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Neonatal Hypoglycemia. These podcasts are designed to give medical students an overview of key topics in pediatrics.
HYPOGLYCAEMIA OF THE NEWBORN ON BIRTHING SUITE AND POSTNATAL WARD
 HYPOGLYCAEMIA OF THE NEWBORN ON BIRTHING SUITE AND POSTNATAL WARD INTRODUCTION Healthy term infants are able to mobilise energy stores through a process known as counter regulation and are unlikely to
HYPOGLYCAEMIA OF THE NEWBORN ON BIRTHING SUITE AND POSTNATAL WARD INTRODUCTION Healthy term infants are able to mobilise energy stores through a process known as counter regulation and are unlikely to
Evidence-Based Update: Using Glucose Gel to Treat Neonatal Hypoglycemia
 Neonatal Nursing Education Brief: Evidence-Based Update: Using Glucose Gel to Treat Neonatal Hypoglycemia http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/
Neonatal Nursing Education Brief: Evidence-Based Update: Using Glucose Gel to Treat Neonatal Hypoglycemia http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/
7/11/2018. Oral Dextrose Gel Treatment for Newborns with Hypoglycemia Reduces NICU Admissions DISCLOSURE. Objectives
 Gaps in Knowledge, Competence, Performance, or Patient Outcomes DISCLOSURE The content of this presentation does not relate to any product of a commercial entity; therefore, I have no relationships to
Gaps in Knowledge, Competence, Performance, or Patient Outcomes DISCLOSURE The content of this presentation does not relate to any product of a commercial entity; therefore, I have no relationships to
Deb Cobie Judy Evans Professionally Approved By Dr Saravanan Consultant Lead for Risk Management June 2009
 TREATMENT OF NEONATAL HYPOGLYCAEMIA Developed in response to: Contributes to CQC Standards No CLINICAL GUIDELINES Register No: 04219 Status: Public Intrapartum NICE Guidelines RCOG guideline C5a Consulted
TREATMENT OF NEONATAL HYPOGLYCAEMIA Developed in response to: Contributes to CQC Standards No CLINICAL GUIDELINES Register No: 04219 Status: Public Intrapartum NICE Guidelines RCOG guideline C5a Consulted
PRACTICE GUIDELINES WOMEN S HEALTH PROGRAM
 C Title: NEWBORN: HYPOGLYCEMIA IN NEONATES BORN AT 35+0 WEEKS GESTATION AND GREATER: DIAGNOSIS AND MANAGEMENT IN THE FIRST 72 HOURS Authorization Section Head, Neonatology, Program Director, Women s Health
C Title: NEWBORN: HYPOGLYCEMIA IN NEONATES BORN AT 35+0 WEEKS GESTATION AND GREATER: DIAGNOSIS AND MANAGEMENT IN THE FIRST 72 HOURS Authorization Section Head, Neonatology, Program Director, Women s Health
Hypoglycaemia of the neonate. Dr. L.G. Lloyd Dept. Paediatrics
 Hypoglycaemia of the neonate Dr. L.G. Lloyd Dept. Paediatrics Why is glucose important? It provides 60-70% of energy needs Utilization obligatory by red blood cells, brain and kidney as major source of
Hypoglycaemia of the neonate Dr. L.G. Lloyd Dept. Paediatrics Why is glucose important? It provides 60-70% of energy needs Utilization obligatory by red blood cells, brain and kidney as major source of
Prevention and Management of Hypoglycaemia
 Prevention and Management of Hypoglycaemia Use for ALL babies on the Labour Ward, Postnatal Ward & Transitional Care. This guideline is based on the BAPM Hypoglycaemia Guideline 2017. This guideline should
Prevention and Management of Hypoglycaemia Use for ALL babies on the Labour Ward, Postnatal Ward & Transitional Care. This guideline is based on the BAPM Hypoglycaemia Guideline 2017. This guideline should
Neonatal Hypoglycaemia
 Neonatal Hypoglycaemia Dr Shubha Srinivasan Paediatric Endocrinologist The Children s Hospital at Westmead Hypoglycaemia and the Brain CSF glucose is 2/3 that of plasma Intracerebral glucose 1/3 that of
Neonatal Hypoglycaemia Dr Shubha Srinivasan Paediatric Endocrinologist The Children s Hospital at Westmead Hypoglycaemia and the Brain CSF glucose is 2/3 that of plasma Intracerebral glucose 1/3 that of
Clinical Director for Women s and Children s Directorate
 TREATMENT OF NEONATAL HYPOGLYCAEMIA IN THE HIGH RISK INFANT CLINICAL GUIDELINES Register No: 12025 Status: Public Developed in response to: Intrapartum NICE Guidelines RCOG guideline Contributes to CQC
TREATMENT OF NEONATAL HYPOGLYCAEMIA IN THE HIGH RISK INFANT CLINICAL GUIDELINES Register No: 12025 Status: Public Developed in response to: Intrapartum NICE Guidelines RCOG guideline Contributes to CQC
Neonatal Hypoglycemia. Presented By : Kamlah Olaimat 25\7\2010
 Neonatal Hypoglycemia Presented By : Kamlah Olaimat 25\7\2010 Definition The S.T.A.B.L.E. Program defines hypoglycemia as: Glucose delivery or availability is inadequate to meet glucose demand (Karlsen,
Neonatal Hypoglycemia Presented By : Kamlah Olaimat 25\7\2010 Definition The S.T.A.B.L.E. Program defines hypoglycemia as: Glucose delivery or availability is inadequate to meet glucose demand (Karlsen,
HYPOGLYCAEMIA OF THE NEWBORN
 HYPOGLYCAEMIA OF THE NEWBORN INTRODUCTION Healthy term infants are able to mobilise energy stores through a process known as counter regulation and are unlikely to suffer any ill effects if fed on demand
HYPOGLYCAEMIA OF THE NEWBORN INTRODUCTION Healthy term infants are able to mobilise energy stores through a process known as counter regulation and are unlikely to suffer any ill effects if fed on demand
NEONATAL HYPOGLYCEMIA HEATHER MCKNIGHT-MENCI, MSN, CRNP CHILDREN S HOSPITAL OF PHILADELPHIA
 NEONATAL HYPOGLYCEMIA HEATHER MCKNIGHT-MENCI, MSN, CRNP CHILDREN S HOSPITAL OF PHILADELPHIA WHAT IS NEONATAL HYPOGLYCEMIA? Glucose concentration low enough to cause signs and symptoms of impaired brain
NEONATAL HYPOGLYCEMIA HEATHER MCKNIGHT-MENCI, MSN, CRNP CHILDREN S HOSPITAL OF PHILADELPHIA WHAT IS NEONATAL HYPOGLYCEMIA? Glucose concentration low enough to cause signs and symptoms of impaired brain
W1A- Cases I Learned From
 W1A- Cases I Learned From David H Adamkin, MD Professor of Pediatrics Director, Division of Neonatology Director of Nutritional Research Rounsavall Chair of Neonatal Medicine Co-Director of Neonatal Fellowship
W1A- Cases I Learned From David H Adamkin, MD Professor of Pediatrics Director, Division of Neonatology Director of Nutritional Research Rounsavall Chair of Neonatal Medicine Co-Director of Neonatal Fellowship
National Metabolic Biochemistry Network Guidelines for the investigation of hypoglycaemia in infants and children
 National Metabolic Biochemistry Network Guidelines for the investigation of hypoglycaemia in infants and children Aim To provide guidance on the biochemical investigation of hypoglycaemia in infants and
National Metabolic Biochemistry Network Guidelines for the investigation of hypoglycaemia in infants and children Aim To provide guidance on the biochemical investigation of hypoglycaemia in infants and
Controversies in Neonatal Hypoglycemia PAC / LAC CONFERENCE, JUNE 1 ST 2017
 Controversies in Neonatal Hypoglycemia PRIYA JEGATHEESAN, MD PAC / LAC CONFERENCE, JUNE 1 ST 2017 Disclosure I have no conflicts of interest to disclose Objectives Review Recommendations from different
Controversies in Neonatal Hypoglycemia PRIYA JEGATHEESAN, MD PAC / LAC CONFERENCE, JUNE 1 ST 2017 Disclosure I have no conflicts of interest to disclose Objectives Review Recommendations from different
Neurodevelopmental Risk?
 Normal Newborn During transitional hypoglycemia normal newborns have an enhanced ketogenic response to fasting. Newborn brains have enhanced capability to use ketone bodies for fuel Allows newborns to
Normal Newborn During transitional hypoglycemia normal newborns have an enhanced ketogenic response to fasting. Newborn brains have enhanced capability to use ketone bodies for fuel Allows newborns to
Title Hypoglycaemia Management and Prevention in Neonates Guideline. Author s job title Senior Neonatal Staff Nurse and Educator Directorate Medical
 Document Control Title in Neonates Guideline Author Author s job title Senior Neonatal Staff Nurse and Educator Directorate Medical Department SCU Version Date Issued Status Comment / Changes / Approval
Document Control Title in Neonates Guideline Author Author s job title Senior Neonatal Staff Nurse and Educator Directorate Medical Department SCU Version Date Issued Status Comment / Changes / Approval
Staff at the Nottingham Children s Hospital. Guidelines process; paediatric endocrinology team
 Hypoglycaemia Title of Guideline Contact Name and Job Title (author) Hypoglycaemia in infants and children: aetiology, investigation and treatment Dr. Hoong-Wei Gan ST6 Paediatric Endocrinology & Diabetes
Hypoglycaemia Title of Guideline Contact Name and Job Title (author) Hypoglycaemia in infants and children: aetiology, investigation and treatment Dr. Hoong-Wei Gan ST6 Paediatric Endocrinology & Diabetes
Hypoglycemia in congenital hyperinsulinism
 How a normal body works: Our body is constantly at work. Our cells need a source of energy, and this source of energy is called glucose. The process is quite simple; think of it like an assembly line.
How a normal body works: Our body is constantly at work. Our cells need a source of energy, and this source of energy is called glucose. The process is quite simple; think of it like an assembly line.
Guidelines for the Management and Prevention of Neonatal Hypoglycaemia in the at-risk infant Maternity Staff
 Guidelines for the Management and Prevention of Neonatal Hypoglycaemia in the at-risk infant Maternity Staff Policy Reference: N001 Date of Issue: May 2015 Prepared by: Janet Kellock Senior Staff Midwife
Guidelines for the Management and Prevention of Neonatal Hypoglycaemia in the at-risk infant Maternity Staff Policy Reference: N001 Date of Issue: May 2015 Prepared by: Janet Kellock Senior Staff Midwife
Newborn Hypoglycemia
 Newborn Hypoglycemia Self Learning Module Developed by the Interprofessional Education and Research Committee of the Champlain Maternal Newborn Regional Program (CMNRP) 2013 TABLE OF CONTENTS Definition....3
Newborn Hypoglycemia Self Learning Module Developed by the Interprofessional Education and Research Committee of the Champlain Maternal Newborn Regional Program (CMNRP) 2013 TABLE OF CONTENTS Definition....3
Hyperglycaemia. Clinical presentation. Definition of hyperglycaemia. Approach to the problem
 Hyperglycaemia 1 Clinical presentation Hyperglycaemia is usually picked up incidentally on routine blood glucose assessment or in response to finding glycosuria. It may be noted as part of the workup of
Hyperglycaemia 1 Clinical presentation Hyperglycaemia is usually picked up incidentally on routine blood glucose assessment or in response to finding glycosuria. It may be noted as part of the workup of
PES Recommendations for Evaluation and Management of Hypoglycemia in Neonates, Infants, and Children Paul S. Thornton On behalf of the Team
 Cook Children s 1 PES Recommendations for Evaluation and Management of Hypoglycemia in Neonates, Infants, and Children Paul S. Thornton On behalf of the Team Cook Children s 2 Co-Chair: Charles Stanley
Cook Children s 1 PES Recommendations for Evaluation and Management of Hypoglycemia in Neonates, Infants, and Children Paul S. Thornton On behalf of the Team Cook Children s 2 Co-Chair: Charles Stanley
Summary of Changes: References/content updated to reflect most current standards of practice.
 Alaska Native Medical Center: Mother Baby Unit Guideline: Neonatal Hypoglycemia Subject: Neonatal Hypoglycemia REVISION DATE: Jan 2015,12/2011, 02/2009, 11, 2007, 07/2007,04/2001, 04/1999 REPLACES: NSY:
Alaska Native Medical Center: Mother Baby Unit Guideline: Neonatal Hypoglycemia Subject: Neonatal Hypoglycemia REVISION DATE: Jan 2015,12/2011, 02/2009, 11, 2007, 07/2007,04/2001, 04/1999 REPLACES: NSY:
Intrapartum and Postpartum Management of the Diabetic Mother and Infant
 Intrapartum and Postpartum Management of the Diabetic Mother and Infant Intrapartum Management Women with gestational diabetes who maintain normal glucose levels during pregnancy on diet and exercise therapy
Intrapartum and Postpartum Management of the Diabetic Mother and Infant Intrapartum Management Women with gestational diabetes who maintain normal glucose levels during pregnancy on diet and exercise therapy
Hypoglycemia. Objectives. Glucose Metabolism
 Hypoglycemia Instructor: Janet Mendis, MSN, RNC-NIC, CNS Outline: Janet Mendis, MSN, RNC-NIC, CNS Summer Morgan, MSN, RNC-NIC, CPNP UC San Diego Health System Objectives State the blood glucose level at
Hypoglycemia Instructor: Janet Mendis, MSN, RNC-NIC, CNS Outline: Janet Mendis, MSN, RNC-NIC, CNS Summer Morgan, MSN, RNC-NIC, CPNP UC San Diego Health System Objectives State the blood glucose level at
DIABETES WITH PREGNANCY
 DIABETES WITH PREGNANCY Prof. Aasem Saif MD,MRCP(UK),FRCP (Edinburgh) Maternal and Fetal Risks Diabetes in pregnancy is associated with risks to the woman and to the developing fetus. Maternal and Fetal
DIABETES WITH PREGNANCY Prof. Aasem Saif MD,MRCP(UK),FRCP (Edinburgh) Maternal and Fetal Risks Diabetes in pregnancy is associated with risks to the woman and to the developing fetus. Maternal and Fetal
بنام خدا هیپوگلیسمی درنوزادان و گاالکتوزمی دکتر انتظاری
 بنام خدا هیپوگلیسمی درنوزادان و گاالکتوزمی دکتر انتظاری Serum glucose< 35 mg/dl 1-3 hr of life < 40 mg/dl 3-24 hr < 45 mg/dl after 24 hr 10% NL newborns can t maintain BS>30 if delayed feeding >3-6 hrs
بنام خدا هیپوگلیسمی درنوزادان و گاالکتوزمی دکتر انتظاری Serum glucose< 35 mg/dl 1-3 hr of life < 40 mg/dl 3-24 hr < 45 mg/dl after 24 hr 10% NL newborns can t maintain BS>30 if delayed feeding >3-6 hrs
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE 1.0 PURPOSE AND INTENT Title: Approval Date: March 2016 Approved by: Neonatal Patient Care Teams, HSC & SBH Women s Health Maternal Newborn Committee Child Health Standards
NEONATAL CLINICAL PRACTICE GUIDELINE 1.0 PURPOSE AND INTENT Title: Approval Date: March 2016 Approved by: Neonatal Patient Care Teams, HSC & SBH Women s Health Maternal Newborn Committee Child Health Standards
Diabetes and Pregnancy
 Diabetes and Pregnancy Dr Warren Gillibrand Deputy Director of Postgraduate Education Department of Nursing & Midwifery Department of AHP and Sports Science w.p.gillibrand@hud.ac.uk Aims of the session
Diabetes and Pregnancy Dr Warren Gillibrand Deputy Director of Postgraduate Education Department of Nursing & Midwifery Department of AHP and Sports Science w.p.gillibrand@hud.ac.uk Aims of the session
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Fortification of Maternal Expressed Breast Milk
 Fortification of Maternal Expressed Breast Milk Title: Version: 2 Ratification Date: April 2016 Review Date: April 2019 Approval: Nottingham Neonatal Service Clinical Guideline Group 20 th April 2016 Author:
Fortification of Maternal Expressed Breast Milk Title: Version: 2 Ratification Date: April 2016 Review Date: April 2019 Approval: Nottingham Neonatal Service Clinical Guideline Group 20 th April 2016 Author:
Identification and Management of Neonatal Hypoglycaemia in the Full Term Infant. Framework for Practice
 Identification and Management of Neonatal Hypoglycaemia in the Full Term Infant Framework for Practice April 2017 Members of the working group Co-chairs Professor James Boardman, Professor of Neonatal
Identification and Management of Neonatal Hypoglycaemia in the Full Term Infant Framework for Practice April 2017 Members of the working group Co-chairs Professor James Boardman, Professor of Neonatal
Diabetes Emergency Caesarean section or other unplanned surgery (GL822)
") Diabetes Emergency Caesarean section or other unplanned surgery (GL822) i.e. insulin dependent diabetic having unplanned surgery e.g. a diabetic woman with pre-labour SROM prior to elective Caesarean section.
Diabetes Emergency Caesarean section or other unplanned surgery (GL822) i.e. insulin dependent diabetic having unplanned surgery e.g. a diabetic woman with pre-labour SROM prior to elective Caesarean section.
ENTERAL NUTRITION Identifying risk of patients for enteral feeding problems: Low risk: Moderate risk: High risk:
 ENTERAL NUTRITION Statement of best practice Feeding with mother s own breastmilk is protective against sepsis, NEC and death All mothers should be informed about this and strongly encouraged to express
ENTERAL NUTRITION Statement of best practice Feeding with mother s own breastmilk is protective against sepsis, NEC and death All mothers should be informed about this and strongly encouraged to express
INTRAVENOUS FLUID THERAPY
 INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
Infection. Risk factor for infection ACoRN alerting sign with * Clinical deterioration. Problem List. Respiratory. Cardiovascular
 The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
What is symptomatic? Neonatal hypoglycemia: how low can you go? Hypoglycemia and MRI. Conflicts. What s the problem? Hypoglycemia and MRI
 Neonatal hypoglycemia: how low can you go? Kristi Watterberg, MD Professor of Pediatrics, UNM What is symptomatic? Jitteriness Cyanosis Poor feeding Weak, high-pitched cry Seizures Apnea Lethargy, low
Neonatal hypoglycemia: how low can you go? Kristi Watterberg, MD Professor of Pediatrics, UNM What is symptomatic? Jitteriness Cyanosis Poor feeding Weak, high-pitched cry Seizures Apnea Lethargy, low
Diabetes Labour guideline (GL820)
") Diabetes Labour guideline (GL820) Approval Approval Group Job Title, Chair of Committee Date Maternity & Childrens Services Mr Mark Selinger, Consultant 6 th June 2014 Clinical Governance Committee Obstetrician
Diabetes Labour guideline (GL820) Approval Approval Group Job Title, Chair of Committee Date Maternity & Childrens Services Mr Mark Selinger, Consultant 6 th June 2014 Clinical Governance Committee Obstetrician
Executive Summary Management of Type 1 Diabetes Mellitus during illness in children and young people under 18 years (Sick Day Rules)
") Executive Summary Management of Type 1 Diabetes Mellitus during illness in children and young people under 18 years (Sick Day Rules) SETTING FOR STAFF PATIENTS Medical and nursing staff Children and young
Executive Summary Management of Type 1 Diabetes Mellitus during illness in children and young people under 18 years (Sick Day Rules) SETTING FOR STAFF PATIENTS Medical and nursing staff Children and young
INTRAVENOUS FLUIDS PRINCIPLES
 INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
Metabolic Programming. Mary ET Boyle, Ph. D. Department of Cognitive Science UCSD
 Metabolic Programming Mary ET Boyle, Ph. D. Department of Cognitive Science UCSD nutritional stress/stimuli organogenesis of target tissues early period critical window consequence of stress/stimuli are
Metabolic Programming Mary ET Boyle, Ph. D. Department of Cognitive Science UCSD nutritional stress/stimuli organogenesis of target tissues early period critical window consequence of stress/stimuli are
Hypoglycaemia (low blood sugar) & ketotic hypoglycaemia
 & ketotic hypoglycaemia") Information for parents and carers Hypoglycaemia (low blood sugar) & ketotic hypoglycaemia What is hypoglycaemia? Hypoglycemia is having a blood glucose (also known as blood sugar) level that is too low
Information for parents and carers Hypoglycaemia (low blood sugar) & ketotic hypoglycaemia What is hypoglycaemia? Hypoglycemia is having a blood glucose (also known as blood sugar) level that is too low
Case 1. Managing Neonatal Hypoglycemia: Can formula supplementation be avoided? Faculty Financial Disclosures 3/8/2018
 Managing Neonatal Hypoglycemia: Can formula supplementation be avoided? Shawnte R. James, MD, FAAP Assistant Professor Newborn Medicine Hospitalist Emory University School of Medicine Department of Pediatrics
Managing Neonatal Hypoglycemia: Can formula supplementation be avoided? Shawnte R. James, MD, FAAP Assistant Professor Newborn Medicine Hospitalist Emory University School of Medicine Department of Pediatrics
Guideline scope Neonatal parenteral nutrition
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Neonatal parenteral nutrition The Department of Health in England has asked NICE to develop a new guideline on parenteral nutrition in
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Neonatal parenteral nutrition The Department of Health in England has asked NICE to develop a new guideline on parenteral nutrition in
Module : Clinical correlates of disorders of metabolism Block 3, Week 2
 Module : Clinical correlates of disorders of metabolism Block 3, Week 2 Department of Paediatrics and Child Health University of Pretoria Tutor : Prof DF Wittenberg : dwittenb@medic.up.ac.za Aim of this
Module : Clinical correlates of disorders of metabolism Block 3, Week 2 Department of Paediatrics and Child Health University of Pretoria Tutor : Prof DF Wittenberg : dwittenb@medic.up.ac.za Aim of this
Newborn Glucose Management Clinical Decision Support System
 Newborn Glucose Management Clinical Decision Support System Marie Kozel, MBA, BSN, RNC-BC 6 th Annual Nursing Quality Conference 2012 Thursday, January 26, 2012 2:45 PM Objectives 1. Describe a newborn
Newborn Glucose Management Clinical Decision Support System Marie Kozel, MBA, BSN, RNC-BC 6 th Annual Nursing Quality Conference 2012 Thursday, January 26, 2012 2:45 PM Objectives 1. Describe a newborn
Clinical Guideline MANAGEMENT OF INFANTS BORN TO MOTHERS WITH GRAVES DISEASE AND AT RISK OF THYROTOXICOSIS
 Clinical Guideline MANAGEMENT OF INFANTS BORN TO MOTHERS WITH GRAVES DISEASE AND AT RISK OF THYROTOXICOSIS Date of First Issue 18/07/2016 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
Clinical Guideline MANAGEMENT OF INFANTS BORN TO MOTHERS WITH GRAVES DISEASE AND AT RISK OF THYROTOXICOSIS Date of First Issue 18/07/2016 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
A S Y N T H E S I Z E D H A N D B O O K ON G E S T A T I O N A L D I A B E T E S
 A S Y N T H E S I Z E D H A N D B O O K ON G E S T A T I O N A L D I A B E T E S P R E F A C E Dear reader, This is a synthesized handbook conceived to serve as a tool to health personnel in the screening,
A S Y N T H E S I Z E D H A N D B O O K ON G E S T A T I O N A L D I A B E T E S P R E F A C E Dear reader, This is a synthesized handbook conceived to serve as a tool to health personnel in the screening,
3 HYDROXY 3 METHYLGLUTARYL CoA (3 HMG CoA) LYASE DEFICIENCY RECOMMENDATIONS ON EMERGENCY MANAGEMENT OF METABOLIC DISEASES
 LYASE DEFICIENCY RECOMMENDATIONS ON EMERGENCY MANAGEMENT OF METABOLIC DISEASES") 3 HYDROXY 3 METHYLGLUTARYL CoA (3 HMG CoA) LYASE DEFICIENCY RECOMMENDATIONS ON EMERGENCY MANAGEMENT OF METABOLIC DISEASES Patient s name: Date of birth: Please read carefully. Meticulous and prompt treatment
3 HYDROXY 3 METHYLGLUTARYL CoA (3 HMG CoA) LYASE DEFICIENCY RECOMMENDATIONS ON EMERGENCY MANAGEMENT OF METABOLIC DISEASES Patient s name: Date of birth: Please read carefully. Meticulous and prompt treatment
ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version)
") Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
Seasonal Influenza in Pregnancy and Puerperium Guideline (GL1086)
") Seasonal Influenza in Pregnancy and Puerperium Guideline (GL1086) Approval Approval Group Job Title, Chair of Committee Date Maternity & Children s Services Clinical Governance Committee Chair, Maternity
Seasonal Influenza in Pregnancy and Puerperium Guideline (GL1086) Approval Approval Group Job Title, Chair of Committee Date Maternity & Children s Services Clinical Governance Committee Chair, Maternity
Diabetes in pregnancy
 Issue date: March 2008 Diabetes in pregnancy Management of diabetes and its complications from pre-conception to the postnatal period Developed by the National Collaborating Centre for Women s and Children
Issue date: March 2008 Diabetes in pregnancy Management of diabetes and its complications from pre-conception to the postnatal period Developed by the National Collaborating Centre for Women s and Children
DRUG GUIDELINE. HYDRALAZINE (Intravenous severe hypertension in pregnancy)
") DRUG GUIDELINE HYDRALAZINE (Intravenous severe hypertension SCOPE (Area): FOR USE IN: Labour Ward, HDU, Theatre and ED EXCLUSIONS: Paediatrics (seek Paediatrician advice) and other general wards. SCOPE
DRUG GUIDELINE HYDRALAZINE (Intravenous severe hypertension SCOPE (Area): FOR USE IN: Labour Ward, HDU, Theatre and ED EXCLUSIONS: Paediatrics (seek Paediatrician advice) and other general wards. SCOPE
Vishwanath Pattan Endocrinology Wyoming Medical Center
 Vishwanath Pattan Endocrinology Wyoming Medical Center Disclosure Holdings in Tandem Non for this Training Introduction In the United States, 5 to 6 percent of pregnancies almost 250,000 women are affected
Vishwanath Pattan Endocrinology Wyoming Medical Center Disclosure Holdings in Tandem Non for this Training Introduction In the United States, 5 to 6 percent of pregnancies almost 250,000 women are affected
Guideline for the Management of Diabetes in Pregnancy
 Guideline for the Management of Diabetes in Pregnancy INITIATED BY: Directorate of Obstetrics, Gynaecology & Sexual Health APPROVED BY: Integrated Business, Obstetrics, Gynaecology, Sexual Health & Patient
Guideline for the Management of Diabetes in Pregnancy INITIATED BY: Directorate of Obstetrics, Gynaecology & Sexual Health APPROVED BY: Integrated Business, Obstetrics, Gynaecology, Sexual Health & Patient
Information for health professionals
 Introduction of a new screening test for newborn babies in Wales Newborn bloodspot screening for Medium chain acyl-coa dehydrogenase deficiency (MCADD) Newborn bloodspot screening for MCADD is being introduced
Introduction of a new screening test for newborn babies in Wales Newborn bloodspot screening for Medium chain acyl-coa dehydrogenase deficiency (MCADD) Newborn bloodspot screening for MCADD is being introduced
NICE guideline Published: 25 February 2015 nice.org.uk/guidance/ng3
 Diabetes in pregnancy: management from preconception to the postnatal period NICE guideline Published: 25 February 2015 nice.org.uk/guidance/ng3 NICE 2017. All rights reserved. Subject to Notice of rights
Diabetes in pregnancy: management from preconception to the postnatal period NICE guideline Published: 25 February 2015 nice.org.uk/guidance/ng3 NICE 2017. All rights reserved. Subject to Notice of rights
Principles of nutrition in the preterm infant. Importance of nutrition: Undernutrition is very common in VLBW infants
 Principles of nutrition in the preterm infant Dr. S. Navarro-Psihas Pädiatrie IV, Klinik für Neonatologie Medizinische Universität Innsbruck Importance of nutrition: Undernutrition is very common in VLBW
Principles of nutrition in the preterm infant Dr. S. Navarro-Psihas Pädiatrie IV, Klinik für Neonatologie Medizinische Universität Innsbruck Importance of nutrition: Undernutrition is very common in VLBW
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE 1.0 PURPOSE AND INTENT Title: Approval Date: March 2016, Last Revised July 2018 Approved by: Neonatal Patient Care Teams, HSC & SBH Women s Health Maternal Newborn
NEONATAL CLINICAL PRACTICE GUIDELINE 1.0 PURPOSE AND INTENT Title: Approval Date: March 2016, Last Revised July 2018 Approved by: Neonatal Patient Care Teams, HSC & SBH Women s Health Maternal Newborn
Early Life Nutrition: Feeding Preterm Babies for Lifelong Health
 Early Life Nutrition: Feeding Preterm Babies for Lifelong Health Jane Alsweiler Frank Bloomfield Anna Tottman Barbara Cormack Tanith Alexander Jane Harding Feeding Preterm Babies for Lifelong Health Why
Early Life Nutrition: Feeding Preterm Babies for Lifelong Health Jane Alsweiler Frank Bloomfield Anna Tottman Barbara Cormack Tanith Alexander Jane Harding Feeding Preterm Babies for Lifelong Health Why
Objectives. Birth Depression Management. Birth Depression Terms
 Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
NUTRITIONAL REQUIREMENTS
 NUTRITION AIMS To achieve growth and nutrient accretion similar to intrauterine rates To achieve best possible neurodevelopmental outcome To prevent specific nutritional deficiencies Target population
NUTRITION AIMS To achieve growth and nutrient accretion similar to intrauterine rates To achieve best possible neurodevelopmental outcome To prevent specific nutritional deficiencies Target population
Neonatal Parenteral Nutrition Guideline Dr M Hogan, Maire Cullen ANNP, Una Toland Ward Manager, Sandra Kilpatrick Neonatal Pharmacist
 CLINICAL GUIDELINES ID TAG Title: Author: Designation: Speciality / Division: Directorate: Neonatal Parenteral Nutrition Guideline Dr M Hogan, Maire Cullen ANNP, Una Toland Ward Manager, Sandra Kilpatrick
CLINICAL GUIDELINES ID TAG Title: Author: Designation: Speciality / Division: Directorate: Neonatal Parenteral Nutrition Guideline Dr M Hogan, Maire Cullen ANNP, Una Toland Ward Manager, Sandra Kilpatrick
Gestational Diabetes Mellitus Dr. Fawaz Amin Saad
 Gestational Diabetes Mellitus Dr. Fawaz Amin Saad Senior Consultant OB/GYN, Al-Hayat Medical Center, Doha, Qatar DISCLOSURE OF CONFLICT OF INTEREST I am a full-time Employee at Al-Hayat Medical Center.
Gestational Diabetes Mellitus Dr. Fawaz Amin Saad Senior Consultant OB/GYN, Al-Hayat Medical Center, Doha, Qatar DISCLOSURE OF CONFLICT OF INTEREST I am a full-time Employee at Al-Hayat Medical Center.
Minimal Enteral Nutrition
 Abstract Minimal Enteral Nutrition Although parenteral nutrition has been used widely in the management of sick very low birth weight infants, a smooth transition to the enteral route is most desirable.
Abstract Minimal Enteral Nutrition Although parenteral nutrition has been used widely in the management of sick very low birth weight infants, a smooth transition to the enteral route is most desirable.
4/15/2014. Nurses Take the Lead to Improve Overall Infant Growth. Improving early nutrition. Problem Identification
 Nurses Take the Lead to Improve Overall Infant Growth Cathy Lee Leon, RN, BSN, MBA, NE-BC California Pacific Medical Center-San Francisco Improving early nutrition Standardized feeding protocol Problem
Nurses Take the Lead to Improve Overall Infant Growth Cathy Lee Leon, RN, BSN, MBA, NE-BC California Pacific Medical Center-San Francisco Improving early nutrition Standardized feeding protocol Problem
GESTATIONAL DIABETES (DIET/INSULIN/ METFORMIN) CARE OF WOMEN IN BIRTHING SUITE
 CARE OF WOMEN IN BIRTHING SUITE") GESTATIONAL DIABETES (DIET/INSULIN/ METFORMIN) CARE OF WOMEN IN BIRTHING SUITE DEFINITION A disorder characterised by hyperglycaemia first recognised during pregnancy due to increased insulin resistance
GESTATIONAL DIABETES (DIET/INSULIN/ METFORMIN) CARE OF WOMEN IN BIRTHING SUITE DEFINITION A disorder characterised by hyperglycaemia first recognised during pregnancy due to increased insulin resistance
NEONATOLOGY Healthy newborn. Neonatal sequelaes
 NEONATOLOGY Healthy newborn. Neonatal sequelaes Ágnes Harmath M.D. Ph.D. senior lecturer 11. November 2016. Tasks of the neonatologist Prenatal diagnosed condition Inform parents, preparation of necessary
NEONATOLOGY Healthy newborn. Neonatal sequelaes Ágnes Harmath M.D. Ph.D. senior lecturer 11. November 2016. Tasks of the neonatologist Prenatal diagnosed condition Inform parents, preparation of necessary
MSUD Dietetic Management Pathway
 MSUD Dietetic Management Pathway Presumptive positive screen for MSUD (symptomatic infant) Refer to Clinical Management Guidelines and Initial Clinical Referral Guidelines and Standards (www.bimdg.org)
MSUD Dietetic Management Pathway Presumptive positive screen for MSUD (symptomatic infant) Refer to Clinical Management Guidelines and Initial Clinical Referral Guidelines and Standards (www.bimdg.org)
PARENTERAL NUTRITION
 PARENTERAL NUTRITION DEFINITION Parenteral nutrition [(PN) or total parenteral nutrition (TPN)] is the intravenous infusion of some or all nutrients for tissue maintenance, metabolic requirements and growth
PARENTERAL NUTRITION DEFINITION Parenteral nutrition [(PN) or total parenteral nutrition (TPN)] is the intravenous infusion of some or all nutrients for tissue maintenance, metabolic requirements and growth
Diabetes in obstetric patients
 Diabetes in obstetric patients Swedish Society of Obstetric Anaesthesia & Intensive Care Anita Banerjee Obstetric Physician Diabetes & Endocrinology Consultant Outline Scope of the problem Diabetes and
Diabetes in obstetric patients Swedish Society of Obstetric Anaesthesia & Intensive Care Anita Banerjee Obstetric Physician Diabetes & Endocrinology Consultant Outline Scope of the problem Diabetes and
PHARMACOLOGY AND PHARMACOKINETICS
 DRUG GUIDELINE Insulin, human neutral (Actrapid ) Intravenous Infusion for SCOPE (Area): FOR USE IN: Critical Care Unit, Emergency Department and Operating Suite EXCLUSIONS: Paediatrics (seek Paediatrician
DRUG GUIDELINE Insulin, human neutral (Actrapid ) Intravenous Infusion for SCOPE (Area): FOR USE IN: Critical Care Unit, Emergency Department and Operating Suite EXCLUSIONS: Paediatrics (seek Paediatrician
Nutrition in the preterm - current menu Dr Heena Hooker Consulting Neonatal Paediatrician Aga Khan University Hospital, Nairobi
 Nutrition in the preterm - current menu Dr Heena Hooker Consulting Neonatal Paediatrician Aga Khan University Hospital, Nairobi Outline O Background O Challenges in preterm nutrition O Parenteral Nutrition
Nutrition in the preterm - current menu Dr Heena Hooker Consulting Neonatal Paediatrician Aga Khan University Hospital, Nairobi Outline O Background O Challenges in preterm nutrition O Parenteral Nutrition
Infant Of Diabetic Mother(IDM)
") Infant Of Diabetic Mother(IDM) Sangram Satish Magar 1, Sanskriti Mirashi 2 1. M.D. Sch.(Kaumarbhrutya-Balrog) 2.Guide (Kaumarbhrutya-Balrog), L.R.P.Medical college,islampur,tal- Walwa, dist- Sangli, Maharashtra,
Infant Of Diabetic Mother(IDM) Sangram Satish Magar 1, Sanskriti Mirashi 2 1. M.D. Sch.(Kaumarbhrutya-Balrog) 2.Guide (Kaumarbhrutya-Balrog), L.R.P.Medical college,islampur,tal- Walwa, dist- Sangli, Maharashtra,
Trust Guideline on Routine Oxygen Saturation Measurement on the New-born (Pulse Oximetry)
") Trust Guideline on Routine Oxygen Saturation Measurement on the New-born For Use in: By: For: Division responsible for document: Key words: Name and job title of document author: Name and job title of
Trust Guideline on Routine Oxygen Saturation Measurement on the New-born For Use in: By: For: Division responsible for document: Key words: Name and job title of document author: Name and job title of
PARTICULARS, SCHEDULE 2- THE SERVICES, A- SERVICE SPECIFICATIONS. A17/S(HSS)/a Congenital hyperinsulinism service (Children)
/a Congenital hyperinsulinism service (Children)") A17/S(HSS)/a 2013/14 NHS STANDARD CONTRACT FOR CONGENITAL HYPERINSULINISM SERVICE (CHILDREN) PARTICULARS, SCHEDULE 2- THE SERVICES, A- SERVICE SPECIFICATIONS Service Specification No. Service Commissioner
A17/S(HSS)/a 2013/14 NHS STANDARD CONTRACT FOR CONGENITAL HYPERINSULINISM SERVICE (CHILDREN) PARTICULARS, SCHEDULE 2- THE SERVICES, A- SERVICE SPECIFICATIONS Service Specification No. Service Commissioner
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 Gestational diabetes: risk assessment, testing, diagnosis and management bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They
Gestational diabetes: risk assessment, testing, diagnosis and management bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They
4/23/2015. Linda Steinkrauss, MSN, PNP. No conflicts of interest
 Linda Steinkrauss, MSN, PNP No conflicts of interest 1 5 year old African-American female presented to our Endocrinology Clinic with hypoglycemia Abnormal chromosomes Duplication of 11q13.5-11p14.1 affecting
Linda Steinkrauss, MSN, PNP No conflicts of interest 1 5 year old African-American female presented to our Endocrinology Clinic with hypoglycemia Abnormal chromosomes Duplication of 11q13.5-11p14.1 affecting
Neonatal Seizure. Dr.Nawar Yahya. Presented by: Sarah Khalil Zeina Shamil Zainab Waleed Zainab Qahtan. Supervised by:
 Neonatal Seizure Supervised by: Dr.Nawar Yahya Presented by: Sarah Khalil Zeina Shamil Zainab Waleed Zainab Qahtan Objectives: What is neonatal seizure Etiology Clinical presentation Differential diagnosis
Neonatal Seizure Supervised by: Dr.Nawar Yahya Presented by: Sarah Khalil Zeina Shamil Zainab Waleed Zainab Qahtan Objectives: What is neonatal seizure Etiology Clinical presentation Differential diagnosis
The spectrum and outcome of the. neonates with inborn errors of. metabolism at a tertiary care hospital
 The spectrum and outcome of the neonates with inborn errors of metabolism at a tertiary care hospital Dr. Sevim Ünal Neonatology Division, Ankara Children s Hematology Oncology Research Hospital, Ankara,
The spectrum and outcome of the neonates with inborn errors of metabolism at a tertiary care hospital Dr. Sevim Ünal Neonatology Division, Ankara Children s Hematology Oncology Research Hospital, Ankara,
Insulinoma - 72 hour Fast Protocol - RNS Endocrinology
 Page 1 of 9 - RNS Endocrinology Test name 72 hour fast Alternate test names. Related Tests Mixed meal test Indication(s) Differential diagnosis of causes of hypoglycaemia. Hypoglycaemia is rare in persons
Page 1 of 9 - RNS Endocrinology Test name 72 hour fast Alternate test names. Related Tests Mixed meal test Indication(s) Differential diagnosis of causes of hypoglycaemia. Hypoglycaemia is rare in persons
Pregnancies complicated by diabetes. Marina Mickleson Nurse Practitioner Midwife CDE
 Pregnancies complicated by diabetes Marina Mickleson Nurse Practitioner Midwife CDE Two types Pre gestational Gestational diabetes Both types are on the increase Pre conception work up is imperative for
Pregnancies complicated by diabetes Marina Mickleson Nurse Practitioner Midwife CDE Two types Pre gestational Gestational diabetes Both types are on the increase Pre conception work up is imperative for
Human Milk Analysis Measure protein, fat and carbohydrate. The first step in a healthy preterm baby s life is nutrition
 Human Milk Analysis Measure protein, fat and carbohydrate The first step in a healthy preterm baby s life is nutrition Preterm babies Premature babies are incredibly fragile and what we do during the first
Human Milk Analysis Measure protein, fat and carbohydrate The first step in a healthy preterm baby s life is nutrition Preterm babies Premature babies are incredibly fragile and what we do during the first
Metformin Hydrochloride
 Metformin Hydrochloride 500 mg, 850 mg, 500 mg LA and 750 mg LA Tablet Description Informet is a preparation of metformin hydrochloride that belongs to a biguanide class of oral antidiabetic drugs. Metformin
Metformin Hydrochloride 500 mg, 850 mg, 500 mg LA and 750 mg LA Tablet Description Informet is a preparation of metformin hydrochloride that belongs to a biguanide class of oral antidiabetic drugs. Metformin
ANTENATAL BREAST EXPRESSION. Dr. Christina Raimondi MD CCFP Dr. Katherine Kearns MD CCFP
 ANTENATAL BREAST EXPRESSION Dr. Christina Raimondi MD CCFP Dr. Katherine Kearns MD CCFP OBJECTIVES: 1) What is antenatal breast expression (ABE) 2) Discuss potential benefits and harms of ABE 3) Discuss
ANTENATAL BREAST EXPRESSION Dr. Christina Raimondi MD CCFP Dr. Katherine Kearns MD CCFP OBJECTIVES: 1) What is antenatal breast expression (ABE) 2) Discuss potential benefits and harms of ABE 3) Discuss
PROTOCOL FOR PARENTERAL NUTRITION
 PROTOCOL FOR PARENTERAL NUTRITION Based on; Roberton s textbook of neonatology. 4 th edition. 2005. Sudha Chaudari and Sandeep Kumar.TPN in neonates. Indian Paediatrics. November 2006 Deepak Chawla, Anu
PROTOCOL FOR PARENTERAL NUTRITION Based on; Roberton s textbook of neonatology. 4 th edition. 2005. Sudha Chaudari and Sandeep Kumar.TPN in neonates. Indian Paediatrics. November 2006 Deepak Chawla, Anu
Staff at the Nottingham Children s Hospital. Guidelines process.
 Diabetes and Surgery Title of Guideline Contact Name and Job Title (author) Guideline for the management of children and young people with diabetes aged 18 or under requiring surgery Dr Priyha Santhanam,
Diabetes and Surgery Title of Guideline Contact Name and Job Title (author) Guideline for the management of children and young people with diabetes aged 18 or under requiring surgery Dr Priyha Santhanam,
Running head: ORAL DEXTROSE GEL IN THE TREATMENT OF NH 1. Oral Dextrose Gel in the Treatment of Neonatal Hypoglycemia:
 Running head: ORAL DEXTROSE GEL IN THE TREATMENT OF NH 1 Oral Dextrose Gel in the Treatment of Neonatal Hypoglycemia: An Evidence Based Practice Change Sylvia Cruz Arizona State University NEONATAL HYPOGLYCEMIA
Running head: ORAL DEXTROSE GEL IN THE TREATMENT OF NH 1 Oral Dextrose Gel in the Treatment of Neonatal Hypoglycemia: An Evidence Based Practice Change Sylvia Cruz Arizona State University NEONATAL HYPOGLYCEMIA
LRI Children s Hospital
 LRI Children s Hospital Hypoglycaemia in Infants & Children (not for use in the NNU or for Children diagnosed with diabetes) Staff relevant to: Clinical staff working within the UHL Children s Hospital.
LRI Children s Hospital Hypoglycaemia in Infants & Children (not for use in the NNU or for Children diagnosed with diabetes) Staff relevant to: Clinical staff working within the UHL Children s Hospital.
** SURFACTANT THERAPY**
 ** SURFACTANT THERAPY** Full Title of Guideline: Surfactant Therapy Author (include email and role): Stephen Wardle (V4) Reviewed by Dushyant Batra Consultant Neonatologist Division & Speciality: Division:
** SURFACTANT THERAPY** Full Title of Guideline: Surfactant Therapy Author (include email and role): Stephen Wardle (V4) Reviewed by Dushyant Batra Consultant Neonatologist Division & Speciality: Division:
Pediatric Toxic Hypoglycemia. Sara Kazim, MD, FRCP (EM) Clinical Pharmacology and Medical Toxicology Fellowship IEMC May Antalya
 Clinical Pharmacology and Medical Toxicology Fellowship IEMC May Antalya") Pediatric Toxic Hypoglycemia Sara Kazim, MD, FRCP (EM) Clinical Pharmacology and Medical Toxicology Fellowship IEMC May 2016 - Antalya Conflicts of Interests... None Learning Needs... By the end of this
Pediatric Toxic Hypoglycemia Sara Kazim, MD, FRCP (EM) Clinical Pharmacology and Medical Toxicology Fellowship IEMC May 2016 - Antalya Conflicts of Interests... None Learning Needs... By the end of this
Overview. o Limitations o Normal regulation of blood glucose o Definition o Symptoms o Clinical forms o Pathophysiology o Treatment.
 Pål R. Njølstad MD PhD KG Jebsen Center for Diabetes Research University of Bergen, Norway Depertment of Pediatrics Haukeland University Hospital Broad Institute of Harvard & MIT Cambridge, MA, USA Hypoglycemia
Pål R. Njølstad MD PhD KG Jebsen Center for Diabetes Research University of Bergen, Norway Depertment of Pediatrics Haukeland University Hospital Broad Institute of Harvard & MIT Cambridge, MA, USA Hypoglycemia