GLP-1 receptor agonists for type 2 diabetes A rationale drug. development. Bo Ahrén
|
|
|
- Arron Robbins
- 5 years ago
- Views:
Transcription
1 PROF. BO AHREN (Orcid ID : ) Article type : Mini Review GLP-1 receptor agonists for type 2 diabetes A rationale drug development Bo Ahrén Department of Clinical Sciences Lund, Lund University, Lund, Sweden Short title: GLP-1RA in type 2 diabetes Proof and correspondence Dr Bo Ahrén B11 BMC Sölvegatan LUND Sweden Bo.Ahren@med.lu.se This article has been accepted for publication and undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process, which may lead to differences between this version and the Version of Record. Please cite this article as doi: /jdi.12911
2 Abstract GLP-1 receptor agonists are today established glucose-lowering drugs in the management of type 2 diabetes. Their development emerged from the understanding that a combined islet dysfunction comprising of impaired insulin secretion and exaggerated glucagon secretion is the key defect for the hyperglycemia. GLP-1 was early shown to target these defects and following the realization that DPP-4 inactivates native GLP-1, several different DPP-4 resistant GLP-1 receptor agonists have been developed. They are administered subcutaneously but show differences in molecular structure, molecular size and pharmacokinetics, the latter allowing twice daily, once daily or once weekly administration. They have been shown to be efficient in reducing both HbA1c and body weight and to be safe and highly tolerable. Cardiovascular outcomes trials have shown them to be neutral or beneficial. GLP-1 receptor agonists are positioned as add-on to metformin alone or in combination with oral agents in the clinical paradigm. They are also efficient when combined with insulin, and fixed dose combinations with long-acting insulins have been developed. Recent development include very long administration schedule and oral availability. The research from the first demonstration of the antidiabetic action of GLP-1 in the early 1990s to the enormously accumulated data today represents a successful and rational development which has been characterized by focused perseverance to establish this therapy in the management of type 2 diabetes. Key words: GLP-1, type 2 diabetes, treatment
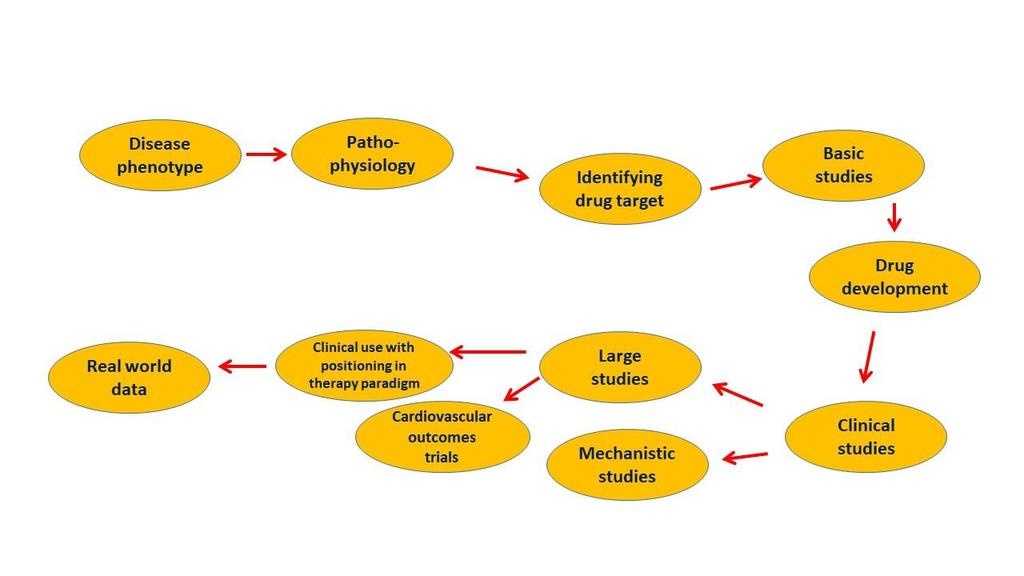
3 Development of GLP-1 receptor agonists as a treatment in the management of type 2 diabetes is an example of a rational drug design, which follows characteristic steps required for a proper pharma development (Fig. 1). The process has also engaged many players, in particular scientists, the research-oriented industry, health authorities and regulators and the patients. This contribution will focus on the phases of development of GLP-1 receptor agonists from the idea of a pathophysiology-directed target based on an endogenous hormone through drug design, clinical studies and positioning in the market. The first step leading to development of GLP-1 receptor agonists was studies establishing that impaired insulin secretion and exaggerated glucagon secretion are the key drivers of hyperglycemia in type 2 diabetes. This is today well known but in the 1980s, i.e., in the beginning of the GLP-1 area, the key role of the islets for diabetes development was not widely accepted although clearly demonstrated by islet-oriented researchers (1-6). In fact, it is today established that this combined islet defect is an early phenomenon during the development of type 2 diabetes and it has been shown to be present even before the onset of the disease in subjects at risk (7). Therefore, a pathophysiology-directed target for management if hyperglycemia in type 2 diabetes would need to correct these islet defects. Coinciding with the understanding that impaired insulin secretion and exaggerated glucagon secretion are drivers of hyperglycemia in the 1980s, it was at the same time shown that GLP-1 targets these two defects. GLP-1, which was discovered in 1983 (8), is a gut hormone which is released during meal ingestion (9,10). It is the main gut incretin hormone, i.e., the hormone responsible for the augmented insulin release after oral versus intravenous
4 glucose administration at similar glucose levels (11). This assures an appropriate insulin response to ingested meals. Stimulation of insulin secretion by GLP-1 in humans was first demonstrated by Kreymann et al in 1987 when they infused GLP-1 together with glucose and found a potentiation of glucose-stimulated insulin secretion (12). The inhibition of glucagon was first demonstrated in animal studies by Ørskov et al in 1988 (13) and Fridolf et al in 1991 (14). Indeed, when islet effects of GLP-1 were characterized in detail in humans, a marked reduction in glucagon after meal ingestion was observed (15). On top of this, GLP-1 was found to delay gastric emptying and induce satiety and weight reduction, which add to the glucose-lowering characteristic of the hormone (16). Therefore, GLP-1 fulfils criteria of being a physiological endogenous factor that has the ability to be antidiabetic through several actions in type 2 diabetes, and these characteristics were evident from the end of the 1980s. This realization was followed by the first test of GLP-1 in type 2 diabetes. We thereby infused GLP-1 or placebo during a meal ingestion in subjects with type 2 diabetes and at the same time we infused insulin in a variable rate to maintain normoglycemia. We could then calculate the meal insulin requirement during the two tests and we found that the meal insulin requirement to achieve normoglycemia after meal ingestion was markedly reduced by GLP-1 in type 2 diabetes when compared to placebo. This was associated with increased levels of C-peptide and reduced glucagon levels, as evidence for stimulation of insulin secretion and inhibition of glucagon secretion in the patients (17,18).
5 We presented this first demonstration of an antidiabetic action of GLP-1 at the EASD in 1990 (17) and published the results in 1992 (18). In an editorial accompanying the published article it was stated that If these interesting findings can be replicated, GLP-1 analogues may become useful in the treatment of patients with NIDDM, i.e., type 2 diabetes (19). This first study was later followed by several studies reporting that GLP-1 stimulates insulin secretion and reduces glucose in type 2 diabetes. For example by Nathan et al showed in 1992 that GLP-1 stimulates insulin secretion (20), Rachman et al showed in 1996 that overnight GLP-1 infusion nearly normalizes circulating glucose (21), Gutniak et al showed in 2001 that GLP-1 suppresses postprandial glucose (22) and Zander et al showed in 2002 that six weeks GLP-1 administration improves glycemic and reduces body weight (23). A problem for drug development with these early studies was that GLP-1 had to be given through a continuous subcutaneous or intravenous route to allow for a long-term effect due to the rapid inactivation of the hormone. Therefore, to really harness the antidiabetic action of GLP-1 required to overcome the fast inactivation of native GLP-1. Thus, the native hormone has a half life of only a few minutes. It was demonstrated by Mentlein et al that the enzyme dipeptidylpeptidase-4 (DPP-4) was responsible for this inactivation (24). This enzyme rapidly cleaves the two N-terminal amino acids from the rest of the hormone, which makes GLP-1 largely inactive. This was further enforced by the finding that inhibition of DPP- 4 raised the endogenous levels of GLP-1 (25), which is turn paved the way for DPP-4 inhibition as a therapy, the first clinical evidence of which was published in 2002 (26).
6 Based on the understanding that DPP-4 resistant GLP-1 receptor agonists needed to be developed, several different GLP-1 receptor agonists have emerged (27,28). They have different background and molecular and kinetics characteristics. Two of them, liraglutide and semaglutide, are true GLP-1 analogues, meaning that they are modified from the structure of native GLP-1. Thus, in both of them, the molecular structure in GLP-1 has been slightly changed and a fatty acid chain has been added, which results in a delayed absorption from the injection site, a high albumin binding and therefore a longer duration. Furthermore, two other GLP-1 receptor agonists, exenatide and lixisenatide, are based on the peptide exendin derived from the Ghila monster, which has a similar structure as GLP-1 and retains GLP-1 receptor activity. Exenatide is the synthetic recombinant form of exendin and lixisenatide is an exendin molecule which has been prolonged with six lysine residues. Moreover, two of the GLP-1 receptor agonists are larger structures based on complex drug engineering using two GLP-1 molecules. Albiglutide consists of two GLP-1 molecules which have been coupled and fused to recombinant albumin, and dulaglutide consists of two GLP- 1 molecules which through two linker peptides have been fused to Fc fragments of immunoglobulin (27). All these GLP-1 receptor agonists are administered subcutaneously but they differ in other properties. One difference is the structure: exenatide and lixisenatide are based on exendin, whereas the others are based on GLP-1. Furthermore, they differ in molecular size, since albiglutide and dulaglutide are larger whereas the others are smaller, with a similar size as native GLP-1. Moreover, the GLP-1 receptor agonists differ in pharmacokinetics and can be given twice daily (exenatide), once daily (lixisenatide, liraglutide) or once weekly (semaglutide, albiglutide, dulaglutide and an extended form of exenatide) (27).
7 The next step in development of a pharmacotherapy is to examine clinical efficacy, tolerability and safety. Here, all GLP-1 receptor agonists have gone through extended trials. These extensive programs are called AMIGO (exenatide), LEAD (liraglutide), GetGoal (lixisenatide), DURATION (extended form of exenatuide), HARMONY (albiglutide), AWARD (dulaglutide) and SUSTAIN (semaglutide) (28). These programs include several week studies with the GLP-1 receptor agonists tested in monotherapy, in combination with oral agents and in combination with insulin. The studies have shown that the GLP-1 receptor agonists efficiently improve glycemia with a reduction in HbA1c of approximately 0.8-1,5% from baseline levels of % and reduce body weight by 1-5 kg (27-29). The GLP-1 receptor agonists have also been shown to be safe and highly tolerable with transient gastrointestinal symptoms (nausea and vomiting) as the only consistent adverse event (28). The GLP-1 receptor agonists have also undergone large cardiovascular outcomes trials and some of those are already published (LEADER for liraglutide, ELIXA for lixisenatide, EXCSEL for exenatide and SUSTAIN 6 for semaglutide). In total this represents a huge development with thousands of patients. These large trials have shown non-inferiority compared with other treatments in risk for major acute cardiovascular endpoints and two GLP-1 receptor agonists (liraglutide and semaglutide) have in addition shown cardiovascular benefits in these trials (28). It should be emphasized that there are several ongoing trials with GLP-1 receptor agonists, and, therefore, in the near future, even more data will accumulate. An area of special importance is the risk of hypoglycemia during glucose-lowering therapy. In fact, avoiding hypoglycemia is the key of success for treatment of diabetes (30) and strategies need to be defined to prevent hypoglycemia (31). Here GLP-1 receptor agonists
8 are powerful and, as demonstrated in a meta-analysis, GLP-1 receptor agonists have largely the same low risk for hypoglycemia as placebo, even though HbA1c is reduced by aproximately 1% (32). One reason for the low risk of hypoglycemia is that the effect is glucose-dependent such that the effect to stimulate insulin secretion and inhibit glucagon secretion disappear when glucose levels are reduced. Sustainment of glucagon counterregulation to hypoglycemia is also very important to avoid hypoglycemia, and this was clearly shown in a study where the glucagon response to hypoglycemia in insulintreated patients with type 2 diabetes in whom the GLP-1 receptor agonist lixisenatide was added (33). In a two-step clamp technique it was shown that at 3.5 mmol/l glucose there was a slightly lower glucagon with lixisenatide than with placebo, but when glucose was reduced to 2.5 mmol/l the glucagon response was completely normal, i.e., the glucagon counterregulation to hypoglycemia is sustained which is a safeguard against hypoglycemia. Another important issue in the clinical development of GLP-1 receptor agonists is their efficacy in relation to other glucose-lowering therapy. This has been performed within the various trial programs which in general have included studies comparing a GLP-1 receptor agonist with another drug, such as sulfonylurea, usually as add-on to metformin. A recent three-year trial compared a GLP-1 receptor agonist with two other drugs and also a placebo arm, thereby representing a comprehensive approach. In this study, the efficacy and safety of the GLP-1 receptor agonist albiglutide (30-50 mg weekly) were compared with those DPP- 4 inhibitor sitagliptin (100 mg daily), the sulphonylurea glimepiride (2-4 mg daily) and placebo when added to metformin in a total of 1000 inadequately controlled patients with type 2 diabetes (34). It was found that all active treatments reduced HbA1c compared to placebo and the reduction was significantly larger after albiglutide (-0.9%) compared to
9 sitagliptin (-0.4%) and glimepiride (-0.3%) from a baseline of 8.1%. It was also found that hyperglycemic rescue, which was introduced at certain prespecified glucose levels, was lower for albiglutide (26.8%) than for sitagliptin (36.4%), glimepiride (32.7%) or placebo (59.2%). Gastrointestinal adverse events (nausea and vomiting) were the most common adverse events with albiglutide. Therefore, this, and other studies (27-29), show efficient glucose reducing effects with GLP-1 receptor agonists associated with body weight reduction and gastrointestinal adverse events as most common adverse events. Next step in development is to position GLP-1 receptor agonists in relation to other therapies in the glucose-lowering paradigm. In the position statement by EASD and ADA it is suggested that GLP-1 receptor agonists are one of six options to add to metformin in subjects in whom metformin alone is insufficient for adequate glycemic control; the others being sulphonylureas, thiazolidinediones, DPP-4 inhibitors, SGLT2- inhibitors and insulin (35). Also, GLP-1 receptor agonists may be used as third line in combination with metformin and one of sulfonylurea, thiazolidinedione or insulin. Of particular importance is the use of GLP-1 receptor agonists in combination with insulin (36). This is an important combination due to synergistic physiological effects of the two treatments. Thus, insulin stimulates glucose utilization through actions on muscle and fat tissue in combination with inhibiting hepatic glucose production through liver actions, whereas GLP-1 stimulates insulin secretion, inhibits glucose secretion and delays gastric emptying (37). This results in reduction of both fasting and postprandial glucose which is achieved together with a low risk of hypoglycemia, and the satiety effect of GLP-1 results in a lower risk of weight gain compared to treatment with insulin alone. This treatment
10 combination is now available also in fixed dose combinations with the insulin degludec with the GLP-1 receptor agonist liraglutide (38) and the insulin glargine with the GLP-1 receptor agonist lixisenatide (39), respectively. Both these combinations have shown good effect to reduce glucose and to neutralize the increase in body weight seen by insulin, and the risk for hypoglycemia is low (38,39). For the near future two new avenues have opened. One is the potential of very long-term duration, which has been introduced in the ITCA650, which uses exenatide in a mini-osmotic pump that can be introduced for up to one year (40). Another potential is the oral availability of GLP-1 receptor agonists, which has been introduced in clinical trials with oral semaglutide allowing administration once daily as a tablet (41,42). Therefore, we have had a unique experience with the development of GLP-1 based therapy throughout the recent more than 30 years. This development has been assured through a unique cooperation between several players. Scientists have targeted a drug based on pathophysiology, and industrial developers have developed unique molecular structures which have been tested in clinical trials. Cooperation has been undertaken with health care providers and regulators. Through this, patients have received a treatment that not only reduces glucose but also reduces weight and protect from hypoglycemia, a treatment with easy handling and administration and a drug with proven effect on not only glycemia and body weight but also on safety and cardiovascular outcomes.
11 The successful development has required focused efforts and indeed long-term perseverance from the first study on GLP-1 in type 2 diabetes in 1990 to the present day existence of several different GLP-1 receptor agonists. Acknowledgement This mini review is based on a lecture given at the 61st Annual Meeting of the Japan Diabetes Society, Tokyo, May 24-26, Disclosure The author has received speaking or consultancy fees from GSK, MSD, Novartis, Novo Nordisk, Sanofi and Takeda, which all are companies involved in development of incretin based therapy. References 1. Porte D Jr. Banting Lecture Beta-cells in type II diabetes mellitus. Diabetes 1991; 40: Polonsky KS. Evolution of beta-cell dysfunction in impaired glucose tolerance and diabetes. Exp Clin Endocrinol Diabetes 1999; 107: suppl 4: S Efendic S, Luft R, Wajngot A. Aspects of the pathogenesis of type 2 diabetes. Endocr Rev 1984; 5: Unger RH. The Banting Memorial Lecture Diabetes and the alpha cell. Diabetes 1975; 25:
12 5. Dunning BE, Gerich JE. The role of alpha-cell dysregulation in fasting and postprandial hyperglycemia in type 2 diabetes and therapeutic implications. Endocr Rev 2007; 28: Ahrén B. Glucagon early breakthroughs and recent discoveries. Peptides 2015; 67: Ahrén B. ß- and α-cell dysfunction in subjects developing impaired glucose tolerance. Diabetes 2009; 58: Bell GI, Sanchew-Pescador R, Mullenback GT. Hamster proglucagon contains the sequence of glucagon and two related peptides. Nature 1983; 302: Ahrén B. Islet G protein-coupled receptors as potential targets for treatment of type 2 diabetes. Nat Rev Drug Discov 2009; 8: Ahrén B, Carr RD, Deacon CF. Incretin hormone secretion over the day. Vitam Horm 2010; 84: Drucker DJ, Nauck MA. The incretin system: glucagon-like peptide-1 receptor agonists and dipeptidyl peptidasde-4 inhibitors in type 2 diabetes. Lancet 2006; 368: Kreymann B, Williams G, Ghatei MA, et al. Glucagon-like peptide : a physiological incretin in man. Lancet 1987; 2: Ørskov C, Holst JJ, Nielsen OVC. Effect of truncated glucagon-like peptide-1 [proglucagon-(78-107) amide] on endocrine secretion from pig pancreas, antrum, and nonantral stomach. Endocrinology 1988; 123: Fridolf T, Böttcher G, Sundler F, et al. GLP-1 and GLP-1 (7-36) amide: Influences on basal and stimulated insulin and glucagon secretion in the mouse. Pancreas 1991; 6:
13 15. Ahrén B, Holst JJ, Mari A. Characteristics of GLP-1 on beta cell function after meal ingestion in humans. Diabetes Care 2003; 26: Baggio LL, Drucker DJ. Biology of incretins: GLP-1 and GIP. Gastroenterology 2007; 132: Gutniak M, Ahrén B, Efendic S. Glucagon-like insulinotropic peptide 1 (7-36) - new approach to treating diabetes? 26th Assoc for the Study of Diabetes (EASD), Copenhagen 1990, Diabetologia 1990; 33:A Gutniak M, Ørskov C, Holst J, et al. Antidiabetogenic effect of glucagon-like peptide-1 (7-36)amide in normal subjects and patients with diabetes mellitus. N Engl J Med 1992; 326: Ensinck JW, D Alessio DA. The enteroinsular axis revisited. A novel role for an incretin. N Engl J Med 1992; 326: Nathan DM, Schreiber E, Fogel H, et al. Insulinotropic action of glucagonlike peptide- 1-(7-37) in diabetic and nondiabetic subjects. Diabetes Care 1992; 15: Rachman J, Barrow BAS, Levy JC, et al. Near-normalization of diurnal glucose concentrations by continuous administration of glucagon-like peptide-1 (GLP-1) in subjects with NIDDM. Diabetologia 1997; 40: Gutniak MK, Svartberg J, Hellström PM, et al. Antidiabetogenic action of glucagonlike peptide-1 related to administration relative to meal intake in subjects with type 2 diabetes. J Int Med 2001; 250: Zander M, Madsbad S, Madsen JL, et al. Effect of 6-week course of glucagon-like peptide 1 on glycaemic control, insulin sensitivity, and beta-cell function in type 2 diabetes: a parallel-group study. Lancet 2002; 359:
14 24. Mentlein R, Gallwitz B, Schmidt WE, Dipeptidyl-peptidase IV hydrolyses gastric inhibitory polypeptide, glucagon-like peptide-1(7-36) amide, peptide histidine methionine and is responsible for their degradation in human serum. Eur J Biochem 1993; 214: Deacon CF, Johnsen AH, Holst JJ. Degradation of glucagon-like peptide-1 by human plasma in vitro yields an N-terminally truncated peptide that is a major endogenous metabolite in vivo. J Clin Endocrinol Metab 1995; 80: Ahrén B, Simonsson E, Larsson H, et al. Inhibition of dipeptidyl peptidase IV improves metabolic control over a 4-week study period in type 2 diabetes. Diabetes Care 2002; 25: Ahrén B. GLP-1 receptor agonists in the treatment of type 2 diabetes. Diabetes Manage 2013; 3: Aroda VR. A review of GLP-1 receptor agonists: Evolution and advancement, through the lens of randomised clinical trials. Diabetes Obes Metab 2018; 20: suppl 1: Htike ZZ, Zaccardi F, Papamargaritis D, ET AL. Efficacy and safety of glucagon-like peptide-1 receptor agonists in type 2 diabetes: a systematic review and mixedtreatment comparison analysis. Diabetes Obes Metab 2017; 19: Ahrén B. Avoiding hypoglycemia: a key to success for glucose-lowering therapy in type 2 diabetes. Vasc Health Risk Manag 2013; 9: Ahrén B. Strategies to mitigate the risk of hypoglycaemia associated with treatment of type 2 diabetes. Treatment Strategies Diabetes 2013; 5: Liu SC, Tu YK, Chien MN, et al. Effect of antidiabetic agents added to metformin on glycaemic control, hypoglycaemia and weight change in patients with type 2 diabetes: a network meta-analysis Diabetes Obes Metab 2012; 14:
15 33. Farngren J, Persson M, Ahrén B. Effect of the GLP-1 receptor agonist lixisenatide on counter-regulatory responses to hypoglycemia in subjects with insulin-treated type 2 diabetes Diabetes Care 2016; 39: Ahrén B, Johnson SL, Stewart M, et al. HARMONY 3: 104-week randomized, doubleblind, placebo and active controlled trial assessing the efficacy and safety of albiglutide compared with placebo, sitagliptin, and glimepiride in patients with type 2 diabetes taking metformin. Diabetes Care 2014; 37: Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycaemia in type 2 diabetes, 2015: a patient-centred approach. Update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia 2015; 58: , 2015 & Diabetes Care 2015; 38: Ahrén B. Insulin plus incretin. A glucose-lowering strategy for type 2-diabetes. World J Diabetes 2014; 15: Ahrén B. Physiological aspects of the combination of insulin and GLP-1 in the regulation of blood glucose control. Diabetes Metab 2015; 41:6S3-6S Billings LK, Doshi A, Gouet D, et al. Efficacy and safety of IDegLira versus basal-bolus insulin therapy in patients with type 2 diabetes uncontrolled on metformin and basal insulin: the DUAL VII randomized clinical trial. Diabetes Care 2018; 41: Rosenstock J, Aronson R, Grunberger G, et al. Benefits of LixiLan, a titratable fixedratio combination of insulin glargine plus lixisenatide, versus insulin glargine and lixisenatide monocomponents in type 2 diabetes inadequately controlled on oral agents: The LixiLan-O Randomized Trial. Diabetes Care 2016; 39:
16 40. Rosenstock J, Buse JB, Azeem R, et al. Efficacy and safety of ITCA650, a novel drugdevice GLP-1 receptor agonist, in type 2 diabetes uncontrolled with oral antidiabetic drugs: the FREEDOM-1 trial. Diabetes Care 2018; 41: Davies M, Pieber TR, Hartoff-Nielsen ML, et al. Effect of oral semaglutide compared with placebo and subcutaneous semaglutide on glycemic control in patients with type 2 diabetes: a randomized clinical trial. JAMA 2017; 318: Lingvay I, Desouza CV, Lalic KS, et al. A 26-week randomized controlled trial of semaglutide once daily versus liraglutide and placebo in patients with type 21 diabetes suboptimally controlled on diet and exercise with or without metformin. Diabetes Care 2018; in press. Legend to Fig. 1 Schematic view of the process of development of novel pharmacotherapies; incretin based therapy is a good example of a rational drug design which followed these characteristic steps.
17 Fig. 1
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Role of incretins in the treatment of type 2 diabetes
 Role of incretins in the treatment of type 2 diabetes Jens Juul Holst Department of Medical Physiology Panum Institute University of Copenhagen Denmark Diabetes & Obesity Spanish Society of Internal Medicine
Role of incretins in the treatment of type 2 diabetes Jens Juul Holst Department of Medical Physiology Panum Institute University of Copenhagen Denmark Diabetes & Obesity Spanish Society of Internal Medicine
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP
 Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP KEY POINTS sitagliptin (Januvia) is a DPP-4 inhibitor that blocks the breakdown of the
Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP KEY POINTS sitagliptin (Januvia) is a DPP-4 inhibitor that blocks the breakdown of the
Effect of macronutrients and mixed meals on incretin hormone secretion and islet cell function
 Effect of macronutrients and mixed meals on incretin hormone secretion and islet cell function Background. Following meal ingestion, several hormones are released from the gastrointestinal tract. Some
Effect of macronutrients and mixed meals on incretin hormone secretion and islet cell function Background. Following meal ingestion, several hormones are released from the gastrointestinal tract. Some
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
The first stop for professional medicines advice
 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1 receptor analogues The first stop for professional medicines advice 1 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1
London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1 receptor analogues The first stop for professional medicines advice 1 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION.
 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION.") GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION. Patricia Garnica MS, ANP-BC, CDE, CDTC Inpatient Diabetes Nurse Practitioner North
GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION. Patricia Garnica MS, ANP-BC, CDE, CDTC Inpatient Diabetes Nurse Practitioner North
New and Emerging Therapies for Type 2 DM
 Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
GLP-1-based therapies in the management of type 2 diabetes
 GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
Diabetes: Three Core Deficits
 Diabetes: Three Core Deficits Fat Cell Dysfunction Impaired Incretin Function Impaired Appetite Suppression Obesity and Insulin Resistance in Muscle and Liver Hyperglycemia Impaired Insulin Secretion Islet
Diabetes: Three Core Deficits Fat Cell Dysfunction Impaired Incretin Function Impaired Appetite Suppression Obesity and Insulin Resistance in Muscle and Liver Hyperglycemia Impaired Insulin Secretion Islet
Current Status of Incretin Based Therapies in Type 2 Diabetes
 Current Status of Incretin Based Therapies in Type 2 Diabetes DR.M.Mukhyaprana Prabhu Professor of Internal Medicine Kasturba Medical College, Manipal, Manipal University, India 2 nd International Endocrine
Current Status of Incretin Based Therapies in Type 2 Diabetes DR.M.Mukhyaprana Prabhu Professor of Internal Medicine Kasturba Medical College, Manipal, Manipal University, India 2 nd International Endocrine
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Data from an epidemiologic analysis of
 CLINICAL TRIAL RESULTS OF GLP-1 RELATED AGENTS: THE EARLY EVIDENCE Lawrence Blonde, MD, FACP, FACE ABSTRACT Although it is well known that lowering A 1c (also known as glycated hemoglobin) is associated
CLINICAL TRIAL RESULTS OF GLP-1 RELATED AGENTS: THE EARLY EVIDENCE Lawrence Blonde, MD, FACP, FACE ABSTRACT Although it is well known that lowering A 1c (also known as glycated hemoglobin) is associated
Francesca Porcellati
 XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
Characterization of GLP-1 Effects on -Cell Function After Meal Ingestion in Humans
 Emerging Treatments and Technologies O R I G I N A L A R T I C L E Characterization of GLP-1 Effects on -Cell Function After Meal Ingestion in Humans BO AHRÉN, MD, PHD 1 JENS J. HOLST, MD, PHD 2 ANDREA
Emerging Treatments and Technologies O R I G I N A L A R T I C L E Characterization of GLP-1 Effects on -Cell Function After Meal Ingestion in Humans BO AHRÉN, MD, PHD 1 JENS J. HOLST, MD, PHD 2 ANDREA
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
GLP-1. GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4.
 GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
22 Emerging Therapies for
 22 Emerging Therapies for Treatment of Type 2 Diabetes Siddharth N Shah Abstract: The prevalence of Diabetes is progressively increasing world-wide and the growth of the disease in our country is phenomenal.
22 Emerging Therapies for Treatment of Type 2 Diabetes Siddharth N Shah Abstract: The prevalence of Diabetes is progressively increasing world-wide and the growth of the disease in our country is phenomenal.
Semaglutide the new kid on the block in the field of glucagonlike peptide-1 receptor agonists?
 Editorial Page 1 of 5 Semaglutide the new kid on the block in the field of glucagonlike peptide-1 receptor agonists? Cristian Guja 1,2, Rucsandra Dănciulescu Miulescu 1,2 1 National Institute of Diabetes,
Editorial Page 1 of 5 Semaglutide the new kid on the block in the field of glucagonlike peptide-1 receptor agonists? Cristian Guja 1,2, Rucsandra Dănciulescu Miulescu 1,2 1 National Institute of Diabetes,
Therapeutic strategy to reduce Glucagon secretion
 Clinical focus on glucagon: α-cell as a companion of β-cell Therapeutic strategy to reduce Glucagon secretion Sunghwan Suh Dong-A University Conflict of interest disclosure None Committee of Scientific
Clinical focus on glucagon: α-cell as a companion of β-cell Therapeutic strategy to reduce Glucagon secretion Sunghwan Suh Dong-A University Conflict of interest disclosure None Committee of Scientific
Abstract. Effect of sitagliptin on glycemic control in patients with type 2 diabetes. Introduction. Abbas Mahdi Rahmah
 Effect of sitagliptin on glycemic control in patients with type 2 diabetes Abbas Mahdi Rahmah Correspondence: Dr. Abbas Mahdi Rahmah Consultant Endocrinologist, FRCP (Edin) Director of Iraqi National Diabetes
Effect of sitagliptin on glycemic control in patients with type 2 diabetes Abbas Mahdi Rahmah Correspondence: Dr. Abbas Mahdi Rahmah Consultant Endocrinologist, FRCP (Edin) Director of Iraqi National Diabetes
Diabetes 2013: Achieving Goals Through Comprehensive Treatment. Session 2: Individualizing Therapy
 Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
T2DM is a global epidemic with
 : a new option for the management of type 2 diabetes Marc Evans MRCP, MD, Consultant Diabetologist, Llandough Hospital, Cardiff Incretin-based therapies for the treatment of diabetes mellitus (T2DM) present
: a new option for the management of type 2 diabetes Marc Evans MRCP, MD, Consultant Diabetologist, Llandough Hospital, Cardiff Incretin-based therapies for the treatment of diabetes mellitus (T2DM) present
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Convenience of Fixed-Ratio Basal Insulin GLP-1 RA Combination Therapy
 Convenience of Fixed-Ratio Basal Insulin GLP-1 RA Combination Therapy Xavier Cos Catalonian Health Institute Barcelona, Spain Stewart B. Harris Western University London, ON, Canada Basal Insulin GLP-1
Convenience of Fixed-Ratio Basal Insulin GLP-1 RA Combination Therapy Xavier Cos Catalonian Health Institute Barcelona, Spain Stewart B. Harris Western University London, ON, Canada Basal Insulin GLP-1
Scottish Medicines Consortium
 Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My!
 DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
Albiglutide, a Once-Weekly GLP-1RA, for the Treatment of Type 2 Diabetes
 St. Onge et al. Medical Research Archives, vol. 5, issue 11, November 2017 issue Page 1 of 10 REVIEW ARTICLE Albiglutide, a Once-Weekly GLP-1RA, for the Treatment of Type 2 Diabetes Erin St. Onge 1*, Shannon
St. Onge et al. Medical Research Archives, vol. 5, issue 11, November 2017 issue Page 1 of 10 REVIEW ARTICLE Albiglutide, a Once-Weekly GLP-1RA, for the Treatment of Type 2 Diabetes Erin St. Onge 1*, Shannon
Soliqua (insulin glargine and lixisenatide), Xultophy (insulin degludec and liraglutide)
, Xultophy (insulin degludec and liraglutide)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.48 Subject: Insulin GLP-1 Combinations Page: 1 of 5 Last Review Date: September 15, 2017 Insulin GLP-1
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.48 Subject: Insulin GLP-1 Combinations Page: 1 of 5 Last Review Date: September 15, 2017 Insulin GLP-1
Clinical Overview of Combination Therapy with Sitagliptin and Metformin
 Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Combination treatment for T2DM
 Combination treatment for T2DM Date of approval: December 2016 SAGLB.DIA.16.08.0657 Abbreviations ADA: American Diabetes Association CVD: Cardiovascular disease DPP-4: Dipeptidyl Peptidase-4 EASD: European
Combination treatment for T2DM Date of approval: December 2016 SAGLB.DIA.16.08.0657 Abbreviations ADA: American Diabetes Association CVD: Cardiovascular disease DPP-4: Dipeptidyl Peptidase-4 EASD: European
PROCEEDINGS CLINICAL RESEARCH AND EXPERIENCE WITH INCRETIN-BASED THERAPIES * Vivian A. Fonseca, MD, FRCP ABSTRACT
 CLINICAL RESEARCH AND EXPERIENCE WITH INCRETIN-BASED THERAPIES Vivian A. Fonseca, MD, FRCP ABSTRACT Despite proven lifestyle recommendations and the availability of a range of oral antidiabetic agents,
CLINICAL RESEARCH AND EXPERIENCE WITH INCRETIN-BASED THERAPIES Vivian A. Fonseca, MD, FRCP ABSTRACT Despite proven lifestyle recommendations and the availability of a range of oral antidiabetic agents,
Injectable GLP 1 therapy: weight loss effects seen in obesity with and without diabetes
 Injectable GLP 1 therapy: weight loss effects seen in obesity with and without diabetes Dr Masud Haq Consultant Lead in Diabetes & Endocrinology Maidstone & Tunbridge Wells NHS Trust & The London Preventative
Injectable GLP 1 therapy: weight loss effects seen in obesity with and without diabetes Dr Masud Haq Consultant Lead in Diabetes & Endocrinology Maidstone & Tunbridge Wells NHS Trust & The London Preventative
Disclosure. Learning Objectives. Case. Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare
 Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Dulaglutide (LY ) for the treatment of type 2 diabetes
 for the treatment of type 2 diabetes") Expert Review of Clinical Pharmacology ISSN: 1751-2433 (Print) 1751-2441 (Online) Journal homepage: http://www.tandfonline.com/loi/ierj20 (LY-2189265) for the treatment of type 2 diabetes André J. Scheen
Expert Review of Clinical Pharmacology ISSN: 1751-2433 (Print) 1751-2441 (Online) Journal homepage: http://www.tandfonline.com/loi/ierj20 (LY-2189265) for the treatment of type 2 diabetes André J. Scheen
Type 2 DM in Adolescents: Use of GLP-1 RA. Objectives. Scope of Problem: Obesity. Background. Pathophysiology of T2DM
 Type 2 DM in Adolescents: Use of GLP-1 RA Objectives Identify patients in the pediatric population with T2DM that would potentially benefit from the use of GLP-1 RA Discuss changes in glycemic outcomes
Type 2 DM in Adolescents: Use of GLP-1 RA Objectives Identify patients in the pediatric population with T2DM that would potentially benefit from the use of GLP-1 RA Discuss changes in glycemic outcomes
MOA: Long acting glucagon-like peptide 1 receptor agonist
 Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
la prise en charge du diabète de
 N21 XIII Congrès National de Diabétologie, 29 mai 2011, Alger Intérêt et place des Anti DPP4 dans la prise en charge du diabète de type 2 Nicolas PAQUOT, MD, PhD CHU Sart-Tilman, Université de Liège Belgique
N21 XIII Congrès National de Diabétologie, 29 mai 2011, Alger Intérêt et place des Anti DPP4 dans la prise en charge du diabète de type 2 Nicolas PAQUOT, MD, PhD CHU Sart-Tilman, Université de Liège Belgique
Liraglutide: First Once-Daily Human GLP-1 Analogue
 DRUG PROFILE KERALA MEDICAL JOURNAL Liraglutide: First Once-Daily Human GLP-1 Analogue Sreejith N Kumar Research Cell, IMA Kerala State, K-5, Kochar Road, Sasthamangalam Thiruvananthapuram* ABSTRACT Published
DRUG PROFILE KERALA MEDICAL JOURNAL Liraglutide: First Once-Daily Human GLP-1 Analogue Sreejith N Kumar Research Cell, IMA Kerala State, K-5, Kochar Road, Sasthamangalam Thiruvananthapuram* ABSTRACT Published
GLP-1 receptor agonists for type 2 diabetes currently available in the U.S.
 GLP-1 receptor agonists for type 2 diabetes currently available in the U.S. GLP-1 agonists are a class of antidiabetic agents that mimic the actions of the glucagon-like peptide. GLP-1 is one of several
GLP-1 receptor agonists for type 2 diabetes currently available in the U.S. GLP-1 agonists are a class of antidiabetic agents that mimic the actions of the glucagon-like peptide. GLP-1 is one of several
Expanding Treatment Options for Diabetes: GLP-1 Receptor Agonists. Copyright
 CLINICAL Viewpoint Expanding Treatment Options for Diabetes: GLP-1 Receptor Agonists Advancements in Diabetes Management: A Canadian Diabetes Steering Committee Report Copyright Not for Sale or Commercial
CLINICAL Viewpoint Expanding Treatment Options for Diabetes: GLP-1 Receptor Agonists Advancements in Diabetes Management: A Canadian Diabetes Steering Committee Report Copyright Not for Sale or Commercial
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors
 Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
(Incretin) ( glucagon-like peptide-1 GLP-1 ) GLP-1. GLP-1 ( dipeptidyl peptidase IV DPP IV ) GLP-1 DPP IV GLP-1 exenatide liraglutide FDA 2 2 2
 ( glucagon-like peptide-1 GLP-1 ) GLP-1. GLP-1 ( dipeptidyl peptidase IV DPP IV ) GLP-1 DPP IV GLP-1 exenatide liraglutide FDA 2 2 2") 007 18 189-194 (Incretin) Incretin ( ) -1 ( glucagon-like peptide-1 ) ( dipeptidyl peptidase IV ) liraglutide FDA ( Type diabetes mellitus ) -1 ( Glucagon-like peptide-1, ) ( Incretin ) ( Dipeptidyl peptidase
007 18 189-194 (Incretin) Incretin ( ) -1 ( glucagon-like peptide-1 ) ( dipeptidyl peptidase IV ) liraglutide FDA ( Type diabetes mellitus ) -1 ( Glucagon-like peptide-1, ) ( Incretin ) ( Dipeptidyl peptidase
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
DR. SUBHASH K. WANGNOO
 Photograph DR. SUBHASH K. WANGNOO M.D, D.M, FRCP (London) Senior Consultant, Endocrinologist & Diabetologist Apollo Centre for Obesity, Diabetes and Endocrinology Indraprastha Apollo Hospital, Sarita Vihar,
Photograph DR. SUBHASH K. WANGNOO M.D, D.M, FRCP (London) Senior Consultant, Endocrinologist & Diabetologist Apollo Centre for Obesity, Diabetes and Endocrinology Indraprastha Apollo Hospital, Sarita Vihar,
Scope. History. History. Incretins. Incretin-based Therapy and DPP-4 Inhibitors
 Plasma Glucose (mg/dl) Plasma Insulin (pmol/l) Incretin-based Therapy and Inhibitors Scope Mechanism of action ผศ.ดร.นพ.ว ระเดช พ ศประเสร ฐ สาขาว ชาโภชนว ทยาคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล
Plasma Glucose (mg/dl) Plasma Insulin (pmol/l) Incretin-based Therapy and Inhibitors Scope Mechanism of action ผศ.ดร.นพ.ว ระเดช พ ศประเสร ฐ สาขาว ชาโภชนว ทยาคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
Achieving and maintaining good glycemic control is an
 Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Single Technology Appraisal. Canagliflozin in combination therapy for treating type 2 diabetes
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
Pathogenesis of Type 2 Diabetes
 9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
Beyond A1C. Non-glycemic Effects of GLP-1 Receptor Agonists. Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows
 Beyond A1C Non-glycemic Effects of GLP-1 Receptor Agonists Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows Disclosures No conflicts of interest. Learning Objectives 1. Understand the physiological
Beyond A1C Non-glycemic Effects of GLP-1 Receptor Agonists Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows Disclosures No conflicts of interest. Learning Objectives 1. Understand the physiological
Novel anti-diabetic therapies
 Prof. Manfredi Rizzo, MD, PhD ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of Palermo, Italy & ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of South
Prof. Manfredi Rizzo, MD, PhD ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of Palermo, Italy & ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of South
Treatment Options for Diabetes: An Update
 Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Current evidence on the effect of DPP-4 inhibitor drugs on mortality in type 2 diabetic (T2D) patients: A meta-analysis
 patients: A meta-analysis") Current evidence on the effect of DPP-4 inhibitor drugs on mortality in type 2 diabetic (T2D) patients: A meta-analysis Raja Chakraverty Assistant Professor in Pharmacology Bengal College of Pharmaceutical
Current evidence on the effect of DPP-4 inhibitor drugs on mortality in type 2 diabetic (T2D) patients: A meta-analysis Raja Chakraverty Assistant Professor in Pharmacology Bengal College of Pharmaceutical
Mechanisms and Clinical Efficacy of Lixisenatide for the Management of Type 2 Diabetes
 Adv Ther (2013) 30(2):81 101. DOI 10.1007/s12325-013-0009-4 REVIEW Mechanisms and Clinical Efficacy of Lixisenatide for the Management of Type 2 Diabetes Michael Horowitz Christopher K. Rayner Karen L.
Adv Ther (2013) 30(2):81 101. DOI 10.1007/s12325-013-0009-4 REVIEW Mechanisms and Clinical Efficacy of Lixisenatide for the Management of Type 2 Diabetes Michael Horowitz Christopher K. Rayner Karen L.
Targeting Incretins in Type 2 Diabetes: Role of GLP-1 Receptor Agonists and DPP-4 Inhibitors. Richard E. Pratley and Matthew Gilbert
 REVIEW Targeting Incretins in Type 2 Diabetes: Role of GLP-1 Receptor Agonists and DPP-4 Inhibitors Richard E. Pratley and Matthew Gilbert Diabetes and Metabolism Translational Medicine Unit, University
REVIEW Targeting Incretins in Type 2 Diabetes: Role of GLP-1 Receptor Agonists and DPP-4 Inhibitors Richard E. Pratley and Matthew Gilbert Diabetes and Metabolism Translational Medicine Unit, University
Basal & GLP-1 Fixed Combination Use
 Basal & GLP-1 Fixed Combination Use Michelle M. Mangual, MD Diplomate of the American board of Internal Medicine and Endocrinology, Diabetes and Metabolism San Juan City hospital Learning Objectives o
Basal & GLP-1 Fixed Combination Use Michelle M. Mangual, MD Diplomate of the American board of Internal Medicine and Endocrinology, Diabetes and Metabolism San Juan City hospital Learning Objectives o
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
My Journey in Endocrinology. Samuel Cataland M.D
 My Journey in Endocrinology Samuel Cataland M.D. 1968-2015 Drs Berson M.D. Yalow phd Insulin Radioimmunoassay Nobel Prize Physiology or Medicine 1977 Rosalyn Yalow: Radioimmunoassay Technology Andrew Schally
My Journey in Endocrinology Samuel Cataland M.D. 1968-2015 Drs Berson M.D. Yalow phd Insulin Radioimmunoassay Nobel Prize Physiology or Medicine 1977 Rosalyn Yalow: Radioimmunoassay Technology Andrew Schally
Update on GLP-1 Agonists in Type 2 Diabetes is supported by an educational grant from Novo Nordisk Inc. It has been accredited by the American
 Update on GLP-1 Agonists in Type 2 Diabetes is supported by an educational grant from Novo Nordisk Inc. It has been accredited by the American Association of Diabetes Educators (AADE) for nurses, dietitians,
Update on GLP-1 Agonists in Type 2 Diabetes is supported by an educational grant from Novo Nordisk Inc. It has been accredited by the American Association of Diabetes Educators (AADE) for nurses, dietitians,
New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy
 New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy is supported by an educational grant from Novo Nordisk Inc. This program
New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy is supported by an educational grant from Novo Nordisk Inc. This program
exenatide 2mg powder and solvent for prolonged-release suspension for injection (Bydureon ) SMC No. (748/11) Eli Lilly and Company Limited
 SMC No. (748/11) Eli Lilly and Company Limited") exenatide 2mg powder and solvent for prolonged-release suspension for injection (Bydureon ) SMC No. (748/11) Eli Lilly and Company Limited 09 December 2011 The Scottish Medicines Consortium (SMC) has completed
exenatide 2mg powder and solvent for prolonged-release suspension for injection (Bydureon ) SMC No. (748/11) Eli Lilly and Company Limited 09 December 2011 The Scottish Medicines Consortium (SMC) has completed
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Treating Type 2 Diabetes with Bariatric Surgery. Goal of Treating T2DM. Remission of T2DM with Bariatric
 Treating Type 2 Diabetes with Bariatric Surgery Number (in Millions) of Persons with Diagnosed Diabetes, United States, 198 25 The number of Americans with diabetes increased from 5.6 to 15.8 million Guilherme
Treating Type 2 Diabetes with Bariatric Surgery Number (in Millions) of Persons with Diagnosed Diabetes, United States, 198 25 The number of Americans with diabetes increased from 5.6 to 15.8 million Guilherme
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Sitagliptin: A component of incretin based therapy. Rezvan Salehidoost, M.D., Endocrinologist
 Sitagliptin: A component of incretin based therapy Rezvan Salehidoost, M.D., Endocrinologist Agenda Mode of Action Evidences for sitagliptine cardiovascular safety of sitagliptin Ramadan study Impact of
Sitagliptin: A component of incretin based therapy Rezvan Salehidoost, M.D., Endocrinologist Agenda Mode of Action Evidences for sitagliptine cardiovascular safety of sitagliptin Ramadan study Impact of
DPP-4 inhibitor. The new class drug for Diabetes
 DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Intensifying Treatment Beyond Monotherapy in T2DM: Where Do Newer Therapies Fit?
 Intensifying Treatment Beyond Monotherapy in T2DM: Where Do Newer Therapies Fit? Vanita R. Aroda, MD Scientific Director & Physician Investigator MedStar Community Clinical Research Center MedStar Health
Intensifying Treatment Beyond Monotherapy in T2DM: Where Do Newer Therapies Fit? Vanita R. Aroda, MD Scientific Director & Physician Investigator MedStar Community Clinical Research Center MedStar Health
This program applies to Commercial, GenPlus and Health Insurance Marketplace formularies.
 OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
Targeting simultaneously GLP-1, GIP and glucagon receptors : a new paradigm for treating obesity and diabetes
 SHORT COMMENT FOR NATURE REVIEWS ENDOCRINOLOGY Targeting simultaneously GLP-1, GIP and glucagon receptors : a new paradigm for treating obesity and diabetes André J. SCHEEN (1), Nicolas PAQUOT (2) (1)
SHORT COMMENT FOR NATURE REVIEWS ENDOCRINOLOGY Targeting simultaneously GLP-1, GIP and glucagon receptors : a new paradigm for treating obesity and diabetes André J. SCHEEN (1), Nicolas PAQUOT (2) (1)
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Summary. Introduction REVIEW ARTICLE. Johan Jendle 1 * George Grunberger 2 Thomas Blevins 3 Francesco Giorgino 4 Ryan T. Hietpas 5 Fady T.
 REVIEW ARTICLE DIABETES/METABOLISM RESEARCH AND REVIEWS Diabetes Metab Res Rev 2016; 32: 776 790. Published online 15 May 2016 in Wiley Online Library (wileyonlinelibrary.com).2810 Efficacy and safety
REVIEW ARTICLE DIABETES/METABOLISM RESEARCH AND REVIEWS Diabetes Metab Res Rev 2016; 32: 776 790. Published online 15 May 2016 in Wiley Online Library (wileyonlinelibrary.com).2810 Efficacy and safety
DPP-4/SGLT2 inhibitor combined therapy for type 2 diabetes
 THERAPY REVIEW DPP-4/SGLT2 inhibitor combined therapy for type 2 diabetes STEVE CHAPLIN SPL DPP-4 inhibitors and SGLT2 inhibitors lower blood glucose by complementary mechanisms of action, and two fixeddose
THERAPY REVIEW DPP-4/SGLT2 inhibitor combined therapy for type 2 diabetes STEVE CHAPLIN SPL DPP-4 inhibitors and SGLT2 inhibitors lower blood glucose by complementary mechanisms of action, and two fixeddose
Il razionale delle associazioni terapeutiche sulla protezione cardiovascolare
 Il razionale delle associazioni terapeutiche sulla protezione cardiovascolare Alessandra Dei Cas UOC di Endocrinologia e Malattie del Metabolismo Dipartimento di Medicina e Chirurgia Università di Parma
Il razionale delle associazioni terapeutiche sulla protezione cardiovascolare Alessandra Dei Cas UOC di Endocrinologia e Malattie del Metabolismo Dipartimento di Medicina e Chirurgia Università di Parma
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Discussion & Conclusion
 Discussion & Conclusion 7. Discussion DPP-4 inhibitors augment the effects of incretin hormones by prolonging their half-life and represent a new therapeutic approach for the treatment of type 2 diabetes
Discussion & Conclusion 7. Discussion DPP-4 inhibitors augment the effects of incretin hormones by prolonging their half-life and represent a new therapeutic approach for the treatment of type 2 diabetes
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Incredible Incretins Abby Frye, PharmD, BCACP
 Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
Diabetes: What is the scope of the problem?
 Diabetes: What is the scope of the problem? Elizabeth R. Seaquist MD Division of Endocrinology and Diabetes Department of Medicine Director, General Clinical Research Center Pennock Family Chair in Diabetes
Diabetes: What is the scope of the problem? Elizabeth R. Seaquist MD Division of Endocrinology and Diabetes Department of Medicine Director, General Clinical Research Center Pennock Family Chair in Diabetes
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Selecting GLP-1 RA Treatment
 Selecting GLP-1 RA Treatment Dr Felicity Kaplan March 2017 Objectives Review the progressive nature of type 2 diabetes Understand the need for timely treatment intensification Examine the place of GLP-1
Selecting GLP-1 RA Treatment Dr Felicity Kaplan March 2017 Objectives Review the progressive nature of type 2 diabetes Understand the need for timely treatment intensification Examine the place of GLP-1
New Drug Evaluation: Dulaglutide
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Scottish Medicines Consortium
 Scottish Medicines Consortium saxagliptin, 5mg film-coated tablet (Onglyza ) No. (603/10) Bristol-Myers Squibb Pharmaceuticals Ltd 05 February 2010 The Scottish Medicines Consortium (SMC) has completed
Scottish Medicines Consortium saxagliptin, 5mg film-coated tablet (Onglyza ) No. (603/10) Bristol-Myers Squibb Pharmaceuticals Ltd 05 February 2010 The Scottish Medicines Consortium (SMC) has completed
The Highlights of the AWARD Clinical Program FRANCESCO GIORGINO
 The Highlights of the AWARD Clinical Program FRANCESCO GIORGINO DEPARTMENT OF EMERGENCY AND ORGAN TRANSPLANTATION SECTION OF INTERNAL MEDICINE, ENDOCRINOLOGY, ANDROLOGY AND METABOLIC DISEASES Disclaimer
The Highlights of the AWARD Clinical Program FRANCESCO GIORGINO DEPARTMENT OF EMERGENCY AND ORGAN TRANSPLANTATION SECTION OF INTERNAL MEDICINE, ENDOCRINOLOGY, ANDROLOGY AND METABOLIC DISEASES Disclaimer
Add-on saxagliptin improves glycemic status among uncontrolled type 2 diabetes mellitus
 International Journal of Research in Medical Sciences Pradhan B et al. Int J Res Med Sci. 2018 May;6(5):1682-1686 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Original Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20181758
International Journal of Research in Medical Sciences Pradhan B et al. Int J Res Med Sci. 2018 May;6(5):1682-1686 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Original Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20181758
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Ertugliflozin (Steglatro ) 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy
 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy") Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies. Module D
 Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
VICTOSA and Renal impairment DR.R.S.SAJAD
 VICTOSA and Renal impairment DR.R.S.SAJAD February 2019 Main effect of GLP-1 is : Stimulating glucose dependent insulin release from the pancreatic islets. Slow gastric emptying Inhibit inappropriate
VICTOSA and Renal impairment DR.R.S.SAJAD February 2019 Main effect of GLP-1 is : Stimulating glucose dependent insulin release from the pancreatic islets. Slow gastric emptying Inhibit inappropriate