Diabetic Nephropathy. Objectives:
|
|
|
- Isabella Jackson
- 5 years ago
- Views:
Transcription


1 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894.
2 Objectives: Diabetic Nephropathy Recognise the importance of detection of Diabetic nephropathy. Screening for Diabetic nephropathy. Know how to manage patients with diabetic nephropathy as an integral part of their diabetic management.

3 29 years of age Abnormal vision, tired Nocturia, weight loss, thrush Past history Polycystic ovarian syndrome BMI 29 Investigations Random glucose 16.9 mmol/l C-Peptide 1040pmol/L GAD Abs negative HBA1c 12% Creatinine 79umol/L UACR 220 mg/mmol Mrs X
4 Mrs M clinical questions Does she have Type 1 or Type 2 diabetes? What is her expected tracjectory to end stage kidney disease? Can we modify this?
5 Exclude Non-Diabetic Kidney Disease Rapid deterioration in renal function Sudden development of nephrotic syndrome Persistent haematuria Absence of diabetic retinopathy Short duration of Type 1 diabetes Known other systemic disorder
6 Time-course for Diabetic Nephropathy Morgensen CE et al Diabetes 1983; 32 (suppl 2): 64-78


7 Time-course for Diabetic Nephropathy > 50% Type 2 DM will have proteinuria at time of diagnosis.

8 Parving et al. BMJ 1988; 296:
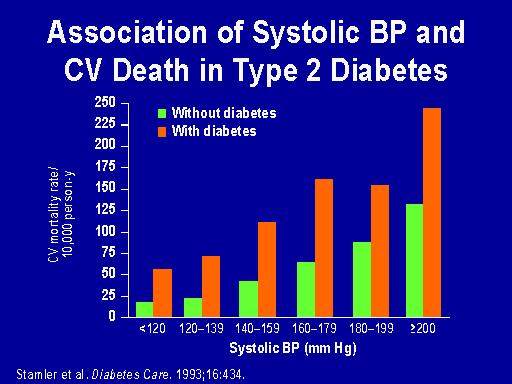
9 Risk of ESRD in type 2 diabetes Urine alb:creatinine HR 6.2 ( ) Serum creatinine. HR 2.1 ( ) Serum albumin. HR 0.7 ( ) Hemoglobin. HR 0.89 ( ) Proteinuria most important risk for progressive kidney damage in type 2 diabetic nephropathy Proteinuria also marker of cardiovascular outcome. RENNAL Study
10 Microalbuminuria Type 1 Diabetes Prevalence 12% 40-50% by 30 years Can be seen in first 5 years Incidence 2% per year Risk for progression: High normal UACR Poor glycaemic control Increased BP Presence of retinopathy Type 2 Diabetes Prevalence 10-50% depending on population studied Higher in Maori and PI Indigenous populations Incidence 2-4% per year 1/3 progress to clinical nephropathy over 5 years Cholesterol also a risk factor for progression
11 Screening Microalbuminuria False positive results: infection, exercise, DKA, poor glycaemic control, uncontrolled hypertension, obesity 2 positive results several months apart Urine albumin : creatinine ratio most convenient Early morning least variability.
12 Definitions Category Albumin:creatinine ratio (mg/mmol) 24-h collection (mg/24 h) Timed collection (µg/min) Normal M:<2.5 F:<3 <30 <20 Microalbuminuria Clinical albuminuria M: F: 3-30 M: >20 F: > >300 >200
13 Diabetic Nephropathy. Management issues. Target Blood Pressure? Drugs of choice? Does glycaemic control influence outcome? How long until renal replacement management required?
14 Management Diet, exercise Medication - blood pressure control, lipids Other risk factors? What will influence progression? What are your markers for progression?
15 Management of Microalbuminuria Does glycaemic control reduce progression? Does blood pressure control reduce progression? Do ACEI s have additional renoprotective effects? Are any other interventions effective?
16 Cumulative Incidence of Urinary Albumin Excretion [>=] 300 mg per 24 Hours (Dashed Line) and [>=] 40 mg per 24 Hours (Solid Line) in Patients with IDDM Receiving Intensive or Conventional Therapy The Diabetes Control and Complications Trial Research Group, N Engl J Med 1993;329:
17 UKPDS 1 HbA 1c 9 cross-sectional, median values HbA 1c (%) 8 7 Conventional Intensive % upper limit of normal range Years from randomisation ukpds Lancet 1998; 352:
18 UKPDS 2 Microvascular Endpoints (cumulative) % of patients with an event 30% 20% 10% 0% renal failure or death, vitreous haemorrhage or photocoagulation 346 of 3867 patients (9%) Conventional Intensive p= Risk reduction 25% (95% CI: 7% to 40%) Years from randomisation ukpds BMJ 1998;317;
19 UKPDS 3 Baseline Three years Six years Nine years Twelve years Fifteen years Microalbuminuria Urine albumin >50 mg/l Relative Risk & 99% CI RR p < Favours intensive Favours conventional ukpds BMJ 1998;317;
20 Mrs X Commenced on Metformin Date HBA1c UACR July August Oct May Dec
21 Management of Microalbuminuria Does glycaemic control reduce progression? Does blood pressure control reduce progression? Do ACEI s have additional renoprotective effects? Are any other interventions effective?

22 UKPDS No threshold for blood pressure The lower the better! BMJ 1998;317;
23 Proteinuria during 5-year follow-up in diabetics treated with enalapril or placebo Ravid, M. et. al. Ann Intern Med 1993;118:
24 Incidence of Progression to Diabetic Nephropathy during Treatment with 150 mg of Irbesartan Daily, 300 mg of Irbesartan Daily, or Placebo in Hypertensive Patients with Type 2 Diabetes and Persistent Microalbuminuria Parving, H.-H. et al. N Engl J Med 2001;345:
25 Studies of treatment effect (angiotensin-converting enzyme [ACE] inhibitor and angiotensin II receptor blocker [ARB] trials) on regression to normoalbuminuria, compared with fixedeffects and random-effects models Hollenberg, N. K. Arch Intern Med 2004;164: Copyright restrictions may apply.
26 Studies of treatment effect (angiotensin-converting enzyme [ACE] inhibitor and angiotensin II receptor blocker [ARB] trials) on risk of progression to macroalbuminuria, compared with fixed-effects and random-effects models Hollenberg, N. K. Arch Intern Med 2004;164: Copyright restrictions may apply.
27 Interventions to slow progression of A2RB Irbesartan Losartan Clinical Nephropathy -1 Increase time to doubling of creatinine Increase time to ESRF Effect over and above effect on blood pressure
28 Prediction of Response to Therapy? Prospective studies have demonstrated the initial reduction in albuminuria (surrogate end point) predicted a beneficial long term effect on GFR decline (principal end point) (Rossing P. Diabetologia 1994, Breyer J. KI 1996)
29 Mrs X Date Blood Pressure Creatinine µmol/l Medication July /98 95 Cilazapril 2.5mg/day October / Cilazapril 5mg/day December / K+ = 5.6mmol/l Cilazapril 5mg/day Candesartan 4mg Do you stop the ACEI / ARB as renal function has declined?

30 felodipine ACEI Weir M Kidney Int 2011; 80,

31 Δ GFR AII vasodilation SNGFR = Kf.NFP AII vasodilation Kf in glomerulus P 1/ r 4 Action of ACEI in CKD
32 Mrs MH 2014 Blood pressure 130/80 Wgt stable 88kg Creatinine 178umol/l, HB1Ac 6.8%, Cholesterol 4.5mmol/l, ACR 35 Meds- Candersarten, cilazapril-hydrochlorthiazide, rosiglitazone, metformin. Simvastatin aspirin.
33 Slowing the Progression of Diabetic Nephropathy High-risk patients with diabetic nephropathy Seen in a specialist Diabetologist /Nephrologist combined clinic High patients defined as significant proteinuria, hypertension, a progressive rise in plasma creatinine or diabetic complications.
34 Slowing the Progression of Diabetic Nephropathy Follow up was defined as at least two data sets (over 12 months) prior to referral, and at least 18 months of follow up thereafter. 10 year audit.
35 Interventions Aggressive glycaemic control. HbA1c < 7 Aggressive BP control < 130/80 anti-proteinuric therapy Lipid lowering therapy Endothelial protection Fear factor nephrologist HbA1c 7.3 (1.0) BP 132/70 (14/10) Alb/creat 112 (16) Chol (1.16)
36 Slowing the Progression of Diabetic Nephropathy At referral GFR decline ml/min/year (95% CI ) intervention ml/min/year (95% CI ) Estimated time to ESRF 6 yrs to 15 yrs Slade H et al. Diabetes Research and Clinical Practice 2011
37 Atherosclerosis Is Common in Newly Diagnosed Diabetes Mellitus Cardiovascular diseases are common causes of morbidity and mortality in people with diabetes >50% of patients with newly diagnosed type 2 diabetes show evidence of cardiovascular disease Atherosclerosis is a major cause of death among patients with diabetes mellitus 75% from coronary atherosclerosis 25% from cerebral or peripheral vascular disease >75% of hospitalizations for individuals with diabetes are for atherosclerotic disease Adapted from Amos AF et al Diabet Med 1997;14:S7-S85; Hill Golden S Adv Stud Med 2002;2: ; Haffner SM et al N Engl J Med 1998;339: ; Sprafka JM et al Diabetes Care 1991;14:
38 Two-Thirds of People with Diabetes Die of Cardiovascular Disease Among people with diabetes, macrovascular complications, including CHD, stroke, and peripheral vascular disease, are the leading causes of morbidity and mortality. Causes of mortality in people with diabetes 67% CHD, stroke, and peripheral vascular disease Other Adapted from Alexander CM, Antonello S Pract Diabet 2002;21:21-28.
39
40 Treatment Strategies for Patients with Diabetes Treatment goals for diabetes should include Optimum glycemic control and elimination of hyperglycemia-related symptoms Dietary and lifestyle changes Exercise Medication Prevention of microvascular complications Control of glycemia Control of blood pressure Monitoring and screening Prevention of CHD, MI, and other macrovascular complications Control dyslipidemia: LDL-C, HDL-C, TG Dietary and lifestyle changes and exercise Drug therapy with statins Adapted from Powers AC. In Harrison s Principles of Internal Medicine. 15th ed. New York: McGraw-Hill, 2001: ; American Diabetes Association Diabetes Care 2002;25(suppl 1):S74-S77.
41 Interventions to slow progression of Clinical Nephropathy-2 Lipid lowering therapy Low protein diet Glucose control Stopping smoking New approaches Aldosterone inhibition Anti-fibrotic agents Multi-Drug approaches Renal SGLT inhibitors
42

43 Lancet May 2015.


44 Figure 1. Identified potential and novel pathways associated with CV effects of SGLT-2 inhibitors based on clinical and mechanistic studies. Copyright by SAGE Publications Silvio E Inzucchi et al. Diabetes and Vascular Disease Research 2015;12:90-100
45 Summary of Canagliflozin Phase 3 Data Efficacy HbA 1c Consistent improvement across Phase 3 studies More subjects achieving HbA 1c goal (data not shown) Sustained response over 52 weeks (data not shown) Meaningful, albeit lesser, reductions in HbA 1c in subjects with renal impairment Other efficacy parameters Consistent reductions in body weight Slightly less in subjects with renal impairment Consistent reductions in systolic blood pressure
46 Summary Diabetic nephropathy epidemic Early aggressive intervention required Glycaemic control important BP ACEI and /or ARB first line targeting a normal blood pressure CV protection statins and aspirin.
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Renal Protection Staying on Target
 Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
New Treatment Options for Diabetic Nephropathy patients. Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland
 New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
Diabetes and kidney disease.
 Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes and Kidney Disease. Kris Bentley Renal Nurse practitioner 2018
 Diabetes and Kidney Disease Kris Bentley Renal Nurse practitioner 2018 Aims Develop an understanding of Chronic Kidney Disease Understand how diabetes impacts on your kidneys Be able to recognise the risk
Diabetes and Kidney Disease Kris Bentley Renal Nurse practitioner 2018 Aims Develop an understanding of Chronic Kidney Disease Understand how diabetes impacts on your kidneys Be able to recognise the risk
American Academy of Insurance Medicine
 American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
RENAAL, IRMA-2 and IDNT. Three featured trials linking a disease spectrum IDNT RENAAL. Death IRMA 2
 Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
Hot Topics in Diabetic Kidney Disease a primary care perspective
 Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Metformin should be considered in all patients with type 2 diabetes unless contra-indicated
 November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions
 Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions Andrew S Narva, MD Na/onal Kidney Disease Educa/on Program U.S. Department of Health and Human Services National Institute of
Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions Andrew S Narva, MD Na/onal Kidney Disease Educa/on Program U.S. Department of Health and Human Services National Institute of
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Diabetic Kidney Disease: Update. GKA Master Class. Istanbul 2011
 Diabetic Kidney Disease: Update GKA Master Class Istanbul 2011 DKD: Challenging dogmas Old Dogmas Type 1 and Type 2 DN have the same natural history Microalbuminuria is an early stage of DN Tight Glycemia
Diabetic Kidney Disease: Update GKA Master Class Istanbul 2011 DKD: Challenging dogmas Old Dogmas Type 1 and Type 2 DN have the same natural history Microalbuminuria is an early stage of DN Tight Glycemia
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression
 Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease
 / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease") Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meetings 1 st and 2 nd September 2016 - London and Leeds Prof Sunil
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meetings 1 st and 2 nd September 2016 - London and Leeds Prof Sunil
Diabetic Nephropathy 2009
 Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Elevation of Serum Creatinine: When to Screen, When to Refer. Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC
 Elevation of Serum Creatinine: When to Screen, When to Refer Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC Presented at the University of Calgary s CME and Professional Development 2006-2007
Elevation of Serum Creatinine: When to Screen, When to Refer Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC Presented at the University of Calgary s CME and Professional Development 2006-2007
The CARI Guidelines Caring for Australians with Renal Impairment. Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy
 Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. All hypercholesterolaemic diabetics
Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. All hypercholesterolaemic diabetics
Diabetes Mellitus. Eiman Ali Basheir. Mob: /1/2019
 Diabetes Mellitus Eiman Ali Basheir Mob: 091520385 27/1/2019 Learning Outcomes Discuss the WHO criteria for Diabetes Mellitus diagnosis Describe the steps taken to confirm diagnosis Interpret GTT. Discuss
Diabetes Mellitus Eiman Ali Basheir Mob: 091520385 27/1/2019 Learning Outcomes Discuss the WHO criteria for Diabetes Mellitus diagnosis Describe the steps taken to confirm diagnosis Interpret GTT. Discuss
The hypertensive kidney and its Management
 The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Kidney and heart: dangerous liaisons. Luis M. RUILOPE (Madrid, Spain)
") Kidney and heart: dangerous liaisons Luis M. RUILOPE (Madrid, Spain) Type 2 diabetes and renal disease: impact on cardiovascular outcomes The "heavyweights" of modifiable CVD risk factors Hypertension
Kidney and heart: dangerous liaisons Luis M. RUILOPE (Madrid, Spain) Type 2 diabetes and renal disease: impact on cardiovascular outcomes The "heavyweights" of modifiable CVD risk factors Hypertension
Morbidity & Mortality from Chronic Kidney Disease
 Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus
 Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus 1 Contents Executive Summary... 3 How to Screen for Diabetic Nephropathy... 4 What to Measure... 4 Frequency
Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus 1 Contents Executive Summary... 3 How to Screen for Diabetic Nephropathy... 4 What to Measure... 4 Frequency
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Complications of Diabetes: Screening and Prevention. Dr Martin McIntyre Consultant Physician Royal Alexandra Hospital Paisley
 Complications of Diabetes: Screening and Prevention Dr Martin McIntyre Consultant Physician Royal Alexandra Hospital Paisley Diabetic Complications Microvascular: Retinopathy Nephropathy Neuropathy Macrovascular:
Complications of Diabetes: Screening and Prevention Dr Martin McIntyre Consultant Physician Royal Alexandra Hospital Paisley Diabetic Complications Microvascular: Retinopathy Nephropathy Neuropathy Macrovascular:
CV Risk Management in Diabetes Mellitus
 CV Risk Management in Diabetes Mellitus J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine University of California, San Francisco Mr. B 40 y/o Latino male c/o fatigue,
CV Risk Management in Diabetes Mellitus J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine University of California, San Francisco Mr. B 40 y/o Latino male c/o fatigue,
The Burden of the Diabetic Heart
 The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
Launch Meeting 3 rd April 2014, Lucas House, Birmingham
 Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Prevention and management of chronic kidney disease in type 2 diabetes
 162..194 NEPHROLOGY 2010; 15, S162 S194 doi:10.1111/j.1440-1797.2010.01240.x Prevention and management of chronic kidney disease in type 2 diabetes Date written: April 2009nep_1240 Final submission: April
162..194 NEPHROLOGY 2010; 15, S162 S194 doi:10.1111/j.1440-1797.2010.01240.x Prevention and management of chronic kidney disease in type 2 diabetes Date written: April 2009nep_1240 Final submission: April
Diabetic Kidney Disease in the Primary Care Clinic
 Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor and Angiotensin II Antagonist Combination Treatment GUIDELINES
 ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
CKD & HT. Anne-Marie Angus
 CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
Diabetic Nephropathy
 Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA
 ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
DIABETES MEASURES GROUP OVERVIEW
 2014 PQRS OPTIONS F MEASURES GROUPS: DIABETES MEASURES GROUP OVERVIEW 2014 PQRS MEASURES IN DIABETES MEASURES GROUP: #1. Diabetes: Hemoglobin A1c Poor Control #2. Diabetes: Low Density Lipoprotein (LDL-C)
2014 PQRS OPTIONS F MEASURES GROUPS: DIABETES MEASURES GROUP OVERVIEW 2014 PQRS MEASURES IN DIABETES MEASURES GROUP: #1. Diabetes: Hemoglobin A1c Poor Control #2. Diabetes: Low Density Lipoprotein (LDL-C)
Ischemic Heart and Cerebrovascular Disease. Harold E. Lebovitz, MD, FACE Kathmandu November 2010
 Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Diabetic Nephropathy
 Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Glucose and CV disease
 Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Update on CVD and Microvascular Complications in T2D
 Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Chronic Kidney Disease Management for Primary Care Physicians. Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015
 Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
 http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
Complications of Diabetes: Screening and Prevention
 Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009
 The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
Hypertension and diabetic nephropathy
 Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Management of early chronic kidney disease
 Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease
 Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease July 2017 Indranil Dasgupta DM FRCP, Debasish Banerjee MD
Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease July 2017 Indranil Dasgupta DM FRCP, Debasish Banerjee MD
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Ο ρόλος των τριγλυκεριδίων στην παθογένεια των μικροαγγειοπαθητικών επιπλοκών του σακχαρώδη διαβήτη
 Ο ρόλος των τριγλυκεριδίων στην παθογένεια των μικροαγγειοπαθητικών επιπλοκών του σακχαρώδη διαβήτη Κωνσταντίνος Τζιόμαλος Επίκουρος Καθηγητής Παθολογίας Α Προπαιδευτική Παθολογική Κλινική, Νοσοκομείο
Ο ρόλος των τριγλυκεριδίων στην παθογένεια των μικροαγγειοπαθητικών επιπλοκών του σακχαρώδη διαβήτη Κωνσταντίνος Τζιόμαλος Επίκουρος Καθηγητής Παθολογίας Α Προπαιδευτική Παθολογική Κλινική, Νοσοκομείο
Diabetes Complications Guideline Based Screening, Management, and Referral
 Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
The promise of the thiazolidinediones in the management of type 2 diabetes-associated cardiovascular disease
 The promise of the thiazolidinediones in the management of type 2 diabetes-associated cardiovascular disease Steve Smith, Group Director Scientific Affairs, Diabetes & Metabolism GlaxoSmithKline R & D
The promise of the thiazolidinediones in the management of type 2 diabetes-associated cardiovascular disease Steve Smith, Group Director Scientific Affairs, Diabetes & Metabolism GlaxoSmithKline R & D
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection
 SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center
Slide 1. Slide 2. Slide 3. A Fork in the Road: Navigating Through New Terrain. Diabetes Standards of Care Then and Now
 Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Case study: Lean adult with no complications, newly diagnosed with type 2 diabetes
 Case study: Lean adult with no complications, newly diagnosed with type 2 diabetes Authored by Clifford Bailey and James LaSalle on behalf of the Global Partnership for Effective Diabetes Management. The
Case study: Lean adult with no complications, newly diagnosed with type 2 diabetes Authored by Clifford Bailey and James LaSalle on behalf of the Global Partnership for Effective Diabetes Management. The
Gli endpoint micro-vascolari nei trial di outcome cardiovascolare
 Gli endpoint micro-vascolari nei trial di outcome cardiovascolare Giorgio Sesti University Magna Graecia of Catanzaro ITALY Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di aver ricevuto
Gli endpoint micro-vascolari nei trial di outcome cardiovascolare Giorgio Sesti University Magna Graecia of Catanzaro ITALY Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di aver ricevuto
The CARI Guidelines Caring for Australians with Renal Impairment. Specific effects of calcium channel blockers in diabetic nephropathy GUIDELINES
 Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
For more information about how to cite these materials visit
 Author(s): Frank Brosius, M.D, 2011 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Frank Brosius, M.D, 2011 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
CHRONIC KIDNEY DISEASE DIAGNOSIS
 CHRONIC KIDNEY DISEASE DIAGSIS GFR categories, description and range WHO SHOULD BE TESTED FOR CKD CLASSIFICATION OF CKD USING egfr AND ACR CATEGORIES Offer testing for CKD using egfr, creatinine and ACR
CHRONIC KIDNEY DISEASE DIAGSIS GFR categories, description and range WHO SHOULD BE TESTED FOR CKD CLASSIFICATION OF CKD USING egfr AND ACR CATEGORIES Offer testing for CKD using egfr, creatinine and ACR
SLOWING PROGRESSION OF KIDNEY DISEASE. Mark Rosenberg MD University of Minnesota
 SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
CLINICIAN INTERVIEW A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY. Interview with Ralph Rabkin, MD
 A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY Interview with Ralph Rabkin, MD Dr Rabkin is Professor of Medicine, Emeritus, Active, at Stanford University School of Medicine, Stanford,
A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY Interview with Ralph Rabkin, MD Dr Rabkin is Professor of Medicine, Emeritus, Active, at Stanford University School of Medicine, Stanford,
Hypertension Management in Diabetic Patients
 Hypertension Management in Diabetic Patients Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School Contents (Treatment of 2 Cases) Type 2 Diabetes Mellitus Hypertension
Hypertension Management in Diabetic Patients Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School Contents (Treatment of 2 Cases) Type 2 Diabetes Mellitus Hypertension
Practical Diabetes. Nic Crook. (and don t use so many charts) Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua
 Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua") Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Diabetes Renal Disease Management. Dr Paul Laboi Dr Vijay Jayagopal York Hospital
 Diabetes Renal Disease Management Dr Paul Laboi Dr Vijay Jayagopal York Hospital 0 Diabetic Nephropathy Diabetic nephropathy is a clinical syndrome characterised by the following: Persistent albuminuria
Diabetes Renal Disease Management Dr Paul Laboi Dr Vijay Jayagopal York Hospital 0 Diabetic Nephropathy Diabetic nephropathy is a clinical syndrome characterised by the following: Persistent albuminuria
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
According to the US Renal Data System,
 DIABETIC NEPHROPATHY * Mohamed G. Atta, MD ABSTRACT *Based on a presentation given by Dr Atta at a CME dinner symposium for family physicians. Assistant Professor of Medicine, Division of Nephrology, Johns
DIABETIC NEPHROPATHY * Mohamed G. Atta, MD ABSTRACT *Based on a presentation given by Dr Atta at a CME dinner symposium for family physicians. Assistant Professor of Medicine, Division of Nephrology, Johns
The Metabolic Syndrome: Is It A Valid Concept? YES
 The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Supplementary Online Content
 Supplementary Online Content Afkarian M, Zelnick L, Hall YN, et al. Clinical manifestations of kidney disease among US adults with diabetes, 1988-2014. JAMA. doi:10.1001/jama.2016.10924 emethods efigure
Supplementary Online Content Afkarian M, Zelnick L, Hall YN, et al. Clinical manifestations of kidney disease among US adults with diabetes, 1988-2014. JAMA. doi:10.1001/jama.2016.10924 emethods efigure
Management of Hypertension in the Diabetic Patient:
 Management of Hypertension in the Diabetic Patient: Nicolas W. Shammas, MS, MD Research Director, Cardiovascular Medicine, PC Presentation Objectives To review: The relationship between HTN, insulin resistance
Management of Hypertension in the Diabetic Patient: Nicolas W. Shammas, MS, MD Research Director, Cardiovascular Medicine, PC Presentation Objectives To review: The relationship between HTN, insulin resistance
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
CANVAS Program Independent commentary
 CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
6/10/2014. Chronic Kidney Disease - General management and standard of care. Management of CKD according to stage (KDOQI 2002)
") Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Key Elements in Managing Diabetes
 Key Elements in Managing Diabetes Presentor Disclosure No conflicts of interest to disclose Presented by Susan Cotey, RN, CDE Lennon Diabetes Center Stephanie Tubbs Jones Health Center Cleveland Clinic
Key Elements in Managing Diabetes Presentor Disclosure No conflicts of interest to disclose Presented by Susan Cotey, RN, CDE Lennon Diabetes Center Stephanie Tubbs Jones Health Center Cleveland Clinic
The CARI Guidelines Caring for Australasians with Renal Impairment. Protein Restriction to prevent the progression of diabetic nephropathy GUIDELINES
 Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
Chronic Kidney Disease. Paul Cockwell Queen Elizabeth Hospital Birmingham
 Chronic Kidney Disease Paul Cockwell Queen Elizabeth Hospital Birmingham Paradigms for chronic disease 1. Acute and chronic disease is closely linked 2. Stratify risk and tailor interventions around failure
Chronic Kidney Disease Paul Cockwell Queen Elizabeth Hospital Birmingham Paradigms for chronic disease 1. Acute and chronic disease is closely linked 2. Stratify risk and tailor interventions around failure
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Educational and behavioral interventions hitherto published
 Treatment of High-Risk Patients with Diabetes: Motivation and Teaching Intervention: A Randomized, Prospective 8-Year Follow-Up Study Rita Rachmani, Inna Slavacheski, Maya Berla, Ronni Frommer-Shapira,
Treatment of High-Risk Patients with Diabetes: Motivation and Teaching Intervention: A Randomized, Prospective 8-Year Follow-Up Study Rita Rachmani, Inna Slavacheski, Maya Berla, Ronni Frommer-Shapira,
Complications of Diabetes mellitus. Dr Bill Young 16 March 2015
 Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have
Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have