Diabetes in the Last Hours and Days of Life. November 2016
|
|
|
- Stella Moody
- 5 years ago
- Views:
Transcription
1 Diabetes in the Last Hours and Days of Life November 2016
2 Guideline Development Group Members Dr Julie Raj Consultant in Palliative Medicine, Aintree University Hospital NHS Foundation Trust Mrs Sue Howarth Clinical Nurse Specialist in Palliative Medicine, Aintree University Hospital NHS Foundation Trust Mrs Jenny Hill Clinical Nurse Specialist in Palliative Medicine, Aintree University Hospital NHS Foundation Trust Mrs Ann Griffiths Clinical Nurse Specialist in Palliative Medicine, Clatterbridge Cancer Centre Dr Dan Monnery ST5 Palliative Medicine, Willowbrook Hospice and St Helen s and Knowsley NHS Foundation Trust Dr Teena Cartwright-Terry Specialty doctor, Willowbrook Hospice n Dr Claire McCourt Specialty doctor, Wirral Hospice St John s
3 With Special Thanks to Patient, Carer and Public Representatives Bob Giles, John Roberts and Angela Fell External Reviewer Dr Paula Chattington Consultant in Diabetes and Endocrinology, Warrington Hospital

4 Current Standards and Guidelines Last Reviewed Jan 2009 Guidelines for the Management of Diabetes in Palliative Care Dr E McKenna, Dr L Chapman, Mrs T Hutchinson
5 Summary of Current Guidelines Outlines the general principles of symptom control in diabetic patients approaching the end of life Provides dietary advice and oral medication advice for patients with type 2 diabetes Provides guidance of insulin dose reduction in type 1 diabetic patients towards the end of life Advises monitoring regimen for patients with different types of diabetes
6 Current Standards Gliclazide is the oral hypoglycaemic of choice [Grade B] Long acting insulins such as Glargine are the insulins of choice [Grade B] Diabetic control should be monitored using capillary blood glucose and venous blood glucose. Urinalysis should not be used for routine monitoring [Grade B] Sliding scales of insulin and the use of Actrapid should be avoided in the management of episodes of hyperglycaemia [Grade D]
7 Systematic Literature Review April-May 2016
8 Our Questions using PICO 1. In patients with diabetes in the last hours to days of life (P), what method of monitoring glycaemic control (I) is the most effective to maximise symptom control (O) 2. In patients with diabetes in the last hours to days of life (P), what method of managing diabetes (I) is most effective to maximise symptom control (O)
9 Literature Search (Palliat* OR End of life ) AND diabet* AND (monitor* OR Manag*) Medline, EMBASE and CINAHL databases: 347 articles 42 abstracts 11 articles 4 Full texts included Cochrane and NICE- No Evidence Found
10 Included articles Pilkey J, et al. (2012). Corticosteroid-Induced diabetes in Palliative Care. Journal of Palliative Medicine, 15(6); Cohort Study The risk of steroid induced diabetes correlates with dose of steroid and duration of use. Once steroid induced diabetes develops, reducing the dose does not improve blood sugars, and steroid induced diabetes may persist for months following discontinuation of steroids [Level 2-].
11 Included articles Quinn K, Hudson P, & Dunning T. (2006). Diabetes management in patients receiving palliative care. Journal of pain and symptom management,32(3); Qualitative study of professional attitudes using questionnaires and focus groups There is variable practice in terms of monitoring and management of diabetes at the end of life, further evidence-based guidance is needed. Discuss with diabetes experts if unsure [Level 3]
12 Included articles Kondo S, Kondo M, & Kondo A. (2013). Glycaemia control using A1C level in terminal cancer patients with pre-existing type 2 diabetes. Journal of palliative medicine, 16(7); Cohort Study Patients with poorly controlled type 2 diabetes die faster after progressing through chemotherapy then those with well controlled type 2 diabetes [Level 2-].
13 Included articles Ford-Dunn S, Smith A, & Quinn J. (2006). Management of diabetes during the last days of life: attitudes of consultant diabetologists and consultant palliative care physicians in the UK. Palliative Medicine, 20; Qualitative study of semi-structured questionnaire of attitudes Palliative care physicians agree with diabetologists mostly around stopping monitoring and treatment of type 2 diabetes at the end of life, but there is less agreement around how to manage type 1 diabetes [Level 4] (due to lack of analysis)
14 Diabetes UK End of life diabetes care: clinical care recommendations (2013) Offers guidance on how to alter monitoring, blood glucose targets and rationalise treatments in patients in the last year of life. Also contains guidance specific to last hours to days of life, including management of hyperglycaemia and hypoglycaemia. It is a document based on expert opinion, not evidence based, and appears to contain no discussion or opinion of palliative care physicians.
15 Diabetes in the last hours to days of Life- Audit results Undertaken September- October 2016 Professional Practice survey- 37 Responses Case Note Audit- 83 Responses
16 Updated Guideline Recommendations and Standards
17 Introduction In 2006, 171 million people worldwide suffered from diabetes and this figure was predicted to increase dramatically into the future 2. The incidence of diabetes in patients with cancer is thought to be six times greater than that found in the general population 2 It is difficult to maintain optimal glycaemic control in patients approaching the end of life. This is balanced against the need to maintain the dignity and comfort of patients approaching the end of life, where evidence about the benefit of glycaemic control in improving symptoms is lacking 6. Nevertheless, strategies aimed at avoiding unpleasant osmotic symptoms or treatment related hypoglycaemia are felt to be in the interest of patients with diabetes approaching the end of life 7.
18 Introduction In the absence of interventional studies examining the optimal monitoring and treatment strategies for patients with diabetes in the last hours to days of life, guidance has been provided by Diabetes UK 1 on best practice when dealing with this clinical entity. These guidelines are based on the expert opinion of the diabetes clinical community. Whilst this guideline takes a comfort-focussed approach to the management of diabetes in patients in the last hours to days of life, its applicability in the different treatment areas (hospital, hospice or home) has not fully been considered, and it may not fully reflect the opinions of those in the palliative medicine community. In addition, some recommendations in said guideline are now out of date, requiring a fresh consensus around some practices.
19 General Principles of Monitoring Blood glucose acceptable range can be considered 6-15mmol/L 1. Hyperglycaemia is defined as blood glucose >20mmol/L, Hypoglycaemia is <4mmol/L 1 If a patient is felt to be imminently dying, and it would be inappropriate to treat any episode of hyper/hypoglycaemia identified, it would be reasonable to explain this to the patient and/or those important to them, document it, and discontinue monitoring. Repeat blood glucose measurements are uncomfortable for the patient 7. Therefore, generally diabetes should be monitored as infrequently as safety permits, and using the least invasive methods possible [Level 4]. Given the importance of prioritising comfort at the end of life, a patient with symptoms of hyper or hypoglycaemia in the last hours to days of life should have their capillary blood glucose checked 1 [Level 4].
20 Monitoring in patients with Type 2 Diabetes NOT receiving medication Due to the low risk of patients with type 2 diabetes developing either diabetic ketoacidosis or hypoglycaemia (providing they are not receiving insulin or sulfonylurea therapy), regular monitoring can be discontinued in the last hours to days of life 6,1 [Level 4]. If the patient develops symptoms of hyper or hypoglycaemia, a capillary blood glucose measurement is indicated 1 [Level 4]. If on an individual clinical basis, regular monitoring is thought to be necessary, this should be done through capillary glucose monitoring [Level 4]
21 Monitoring in patients with Type 1 Diabetes and Type 2 diabetes receiving medication In type 1 diabetes patients it is often the case that treatment will be continued in the last hours to days of life 6. It is therefore recommended that glucose monitoring on a regular basis be continued to avoid episodes of hypoglycaemia during a period of reduced oral intake [Level 4]. Glucose monitoring should take the form of blood glucose monitoring once daily at teatime if the patient is still eating 6,1 but may be undertaken at any time if the patient is no longer taking any nutrition [Level 4]. Whilst there is no data to recommend monitoring schedules for patients with type 2 diabetes still receiving treatment, extrapolating from type 1 diabetes care in whom treatment is not stopped, it is sensible to suggest regular blood glucose monitoring daily at teatime also if able to eat, or any time if not taking any nutrition [Level 4].
22 Monitoring in patients with steroid induced diabetes Prior to commencing steroids, baseline blood sugar should be checked. For those patients without known diabetes who are commenced on steroids, twice weekly monitoring is recommended as the frequency at which monitoring is not unduly burdensome but which is effective at detecting the onset of steroid induced diabetes 11 [Level 2-]. If patients have a random capillary blood glucose measurement of >8mmol/L, the diagnoses of steroid induced diabetes can be confirmed IF APPROPRIATE with a venous glucose measurement >11mmol/L 1. Patients with steroid induced diabetes who remain on steroids regardless of their treatment for the diabetes should receive regular monitoring. This should take the form of capillary blood glucose monitoring daily at teatime. [Level 4]. If steroids are discontinued in patients in the last hours to days of life, any diabetes medications should be reviewed, reduced or possibly discontinued 1. Regular monitoring should continue for any patients still receiving treatment for their diabetes 5 [Level 4].
23 Symptoms/signs of hyper/hypoglycaemia Table 1. Symptoms and signs of hyperglycaemia 1 Polydipsia Polyuria Blurred vision Fatigue Headache Nausea/ vomiting Shortness of breath Smell of ketones on breath Dry mouth Weakness Confusion/ agitation Abdominal pain Drowsiness Coma Table 2. Symptoms and signs of hypoglycaemia 1 Sudden onset of hunger Sweating Palpitations/ anxiety Dizziness Poor concentration Confusion Drowsiness Coma
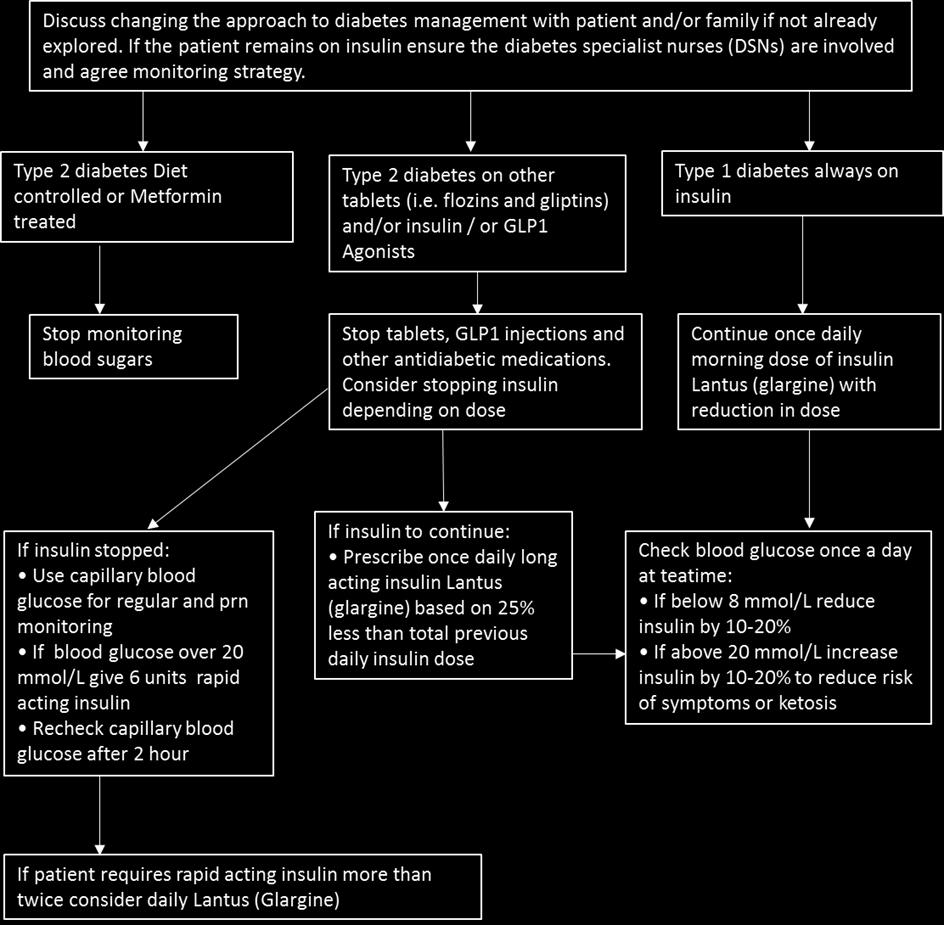
24 Management: Withdrawing treatment The primary reason for glycaemic control in the last hours to days of life is symptom control and avoidance of osmotic symptoms from hyperglycaemia, or symptoms of hypoglycaemia. Therefore, withdrawal of diabetes medications should be balanced against the patient s symptoms, and these should be assessed regularly as treatment is withdrawn 7 [Level 2-] In a patient who is taking oral hypoglycaemia medications in the last hours to days of life, it is reasonable to stop these without the need to commence insulin replacement unless symptomatic 6 [Level 4]. For patients receiving insulin therapy, published professional opinion is in favour of stopping insulin in type 2 diabetics who are only receiving low dose insulin 1 [Level 4]. For type 1 diabetics or type 2 diabetics on higher dose insulin or with a history of developing ketosis, the recommendation is to continue insulin at a low dose and a simplified regime i.e. once daily Lantus (glargine) in the morning 1 [Level 4]
25 Management: Steroid Induced diabetes The risk of developing hyperglycaemia due to steroid therapy correlates with the dose of the steroid 11 [Level 2-]. Management of symptomatic hyperglycaemia in patients on steroids should not rely on a change in the steroid dose 11 [Level 2-]. For patients with steroid induced hyperglycaemia, insulin therapy is appropriate if patients become symptomatic or are found to have a capillary blood glucose of >20mmol/L; a low dose long acting insulin i.e. Lantus (glargine) once daily in the morning is advised 1 [Level 4].
26 Management: Hyperglycaemia (>15mmol/L) If a patient is asymptomatic, consider whether there is a need to treat hyperglycaemia 10 [Level 3]. If patients are symptomatic of hyperglycaemia or are found to have a capillary blood glucose of >20mmol/L, then a one off dose of a short acting insulin 6 units should be administered 1 [Level 4]. If 2 or more doses of short acting insulin are required to keep blood glucose <20mmol/L in a 24-hour period, then consider commencing a long acting insulin in the morning 1 [Level 4]. If a patient is already taking a long acting insulin and requires 2 or more doses of short acting insulin in a 24-hour period an increase in the dose of long acting insulin of 10-20% should be made 1 [Level 4]. If uncertain, referral to your local diabetologist for advice is appropriate when planning the management of hyperglycaemia in patients in the last hours to days of life 10 [Level 4].
27
28 Management: Hypoglycaemia (<4mmol/L) The decision of whether to treat (including the potential for invasive treatment) should be made taking into account the overall condition of the patient, whether the hypoglycaemia is felt to be a result of the dying process or whether it has caused a rapid unexpected decline in the patient s condition, their comfort, any advance wishes/directives of the patient and the views of those important to them (if known) [Level 4]. A capillary blood glucose <6mmol/L should prompt a review of the patient s current anti-diabetes medications. A capillary blood glucose <4mmol/L should prompt consideration of treatment [Level 4]. It is appropriate to consider treating patients with hypoglycaemia in the last hours to days of life. Hypoglycaemia can be a reversible cause for a patient becoming acutely unwell and should be addressed as such [Level 4], even in patients approaching the end of life.
29 Management: Hypoglycaemia (<4mmol/L) If a patient receiving insulin therapy develops an episode of hypoglycaemia, there is a need to reduce the dose or stop the insulin (if already receiving low dose) 1 [Level 4]. A typical reduction in daily insulin will be of 20%, but seek expert advice if unsure. If a patient is found to be hypoglycaemic (either on the basis of becoming symptomatic or through routine glucose monitoring if receiving insulin) a medical review should be sought. If uncertain, referral to your local hypoglycaemia guidelines or diabetologist for advice is appropriate when planning the management of hypoglycaemia in patients in the last hours to days of life 10 [Level 4].

30
31 Mental Capacity Act Where a patient is shown to lack capacity to consent to treatment, the Mental Capacity Act, 2005 must be followed. Lasting Power of Attorney, Advanced Decisions, Independent Mental Capacity Advocates and Deprivation of Liberty Safeguards should be utilised where appropriate.
32 Advance Care Planning When a patient is in the last 12 months of life or in a deteriorating phase of their illness consider discussing advance care planning. Explore the wishes of the patient and their carers regarding the monitoring and management of diabetes at the end of life [Level 4]. Any advance decisions about diabetes monitoring and management in the last hours to days of life should be recorded as part of the advance care plan. [Level 4]. Patients and those important to them may regard a relaxation in blood glucose monitoring and management as a sign of giving up. It is important that these processes are explained sensitively and in the context of symptom control, recognising that the emphasis is on avoiding unnecessary burdens for the patient in the last hours to days of life [Level 4].
33 Standards 1. When it is recognised that a patient is approaching the last hours to days of life, review intensity of monitoring and medications (Grade D) 2. All patients with diabetes in the last hours to days of life should be reviewed every 24 hours by a healthcare professional (Grade D) 3. Where regular insulin is required, a long acting insulin e.g. Lantus (Glargine) should be used (Grade D) 4. All patients receiving insulin should have regular capillary blood glucose monitoring daily (Grade D)
34 Standards 5. Variable rate insulin should be avoided in the management of diabetes in the last hours to days of life (Grade D) 6. Short acting insulin should be considered in patients with symptomatic hyperglycaemia with blood glucose >15, or asymptomatic hyperglycaemia with blood glucose >20 [Grade D]. 7. Treatment of hypoglycaemia (symptomatic or not) should be undertaken unless an assessment that the patient is imminently dying or that further invasive treatment is not appropriate has been documented (Grade D)
35 Standards 8. Patients and those close to them should be involved in discussion regarding the monitoring/management of their diabetes at the end of life, and this should be clearly documented (Grade D) 9.Patients with diabetes in the last hours to days of life should have a documented care plan regarding the monitoring and management of their diabetes at the end of life (Grade D) 10. Patients and those important to them should have a documented offer of written information regarding diabetes monitoring/management at the end of life (Grade D)
36 References 1. Diabetes UK. End of life diabetes care: clinical care recommendations. Second edition. Diabetes UK; World Health Organization Global Report of Diabetes. Available at [Accessed 8/10/16] 3. Boyd K. Diabetes Mellitus in hospice patients: some guidelines. Palliative medicine, 1993; 7: Dunning T. Care of people with diabetes: a manual of nursing practice Oxford: Blackwell publishing. 5. Poulson J. The management of diabetes in patients with advanced cancer. Journal of Pain and Symptom Management, 1997;13(6): Ford-Dunn S, Smith A, & Quin J. Management of diabetes during the last days of life: attitudes of consultant diabetologists and consultant palliative care physicians in the UK. Palliative Medicine, 2006;20: Kondo S, Kondo M, & Kondo A. Glycaemia control using A1C level in terminal cancer patients with pre-existing type 2 diabetes. Journal of Palliative Medicine, 2013;16(7): Merseyside and Cheshire Palliative Care Network Audit Group. Standards and Guidelines. 4th Edition Liverpool: Merseyside and Cheshire Palliative Care Network Audit Group; Cheshire and Merseyside Palliative and End of Life Care Network Audit Group. Guideline Development Manual. 1st Edition Liverpool: Cheshire and Merseyside Palliative and End of Life Care Network Audit Group; Quinn K, Hudson P, & Dunning T. Diabetes management in patients receiving palliative care. Journal of pain and symptom management, 2006;32(3): Pilkey J, Streeter L, Beel A, Hiebert T, & Li X. Corticosteroid-induced diabetes in palliative care. Journal of palliative medicine, 2012;15(6): Department of Constitutional Affairs. Mental Capacity Act 2005 Code of Practice. London Available from: [accessed 8/1016]
37 Invited Expert Comments Dr Paula Chattington
38 Public Representative Comments Mr Bob Giles
39 Questions/ Comments from the group Suggested topics: 1. What is the potential to explore the role of continuous blood glucose monitoring using new transdermal monitors? 2. Should we include further guidance or a standard about criteria for discussion with a specialist, and if so, what should these be? 3. Should steroid induced diabetes monitoring and management form part of this guideline or The use of corticosteroids in palliative care? (You re welcome, corticosteroid group) 4. Are we content to advocate CBG monitoring instead of urinary glucose monitoring despite the diabetes UK guideline recommending the opposite?
GUIDELINES FOR THE MANAGEMENT OF DIABETES IN PALLIATIVE CARE
 GUIDELINES FOR THE MANAGEMENT OF DIABETES IN PALLIATIVE CARE 16.1 GENERAL PRINCIPLES Diabetes occurs more frequently in palliative care patients than the general population. 1 Patients with pancreatic
GUIDELINES FOR THE MANAGEMENT OF DIABETES IN PALLIATIVE CARE 16.1 GENERAL PRINCIPLES Diabetes occurs more frequently in palliative care patients than the general population. 1 Patients with pancreatic
Diabetes Management in Palliative Care. Ryan Liebscher and Carolyn Wilkinson
 Diabetes Management in Palliative Care Ryan Liebscher and Carolyn Wilkinson What are your learning needs? Objectives Review types and prevalence of diabetes Review what is unique to management in the palliative
Diabetes Management in Palliative Care Ryan Liebscher and Carolyn Wilkinson What are your learning needs? Objectives Review types and prevalence of diabetes Review what is unique to management in the palliative
Four is the Floor Symptoms can be felt at higher levels if control is poor Worth confirmation using BG meter if at all possible
 Sandra Coats Diabetes Specialist Nurse 1 Hypoglycaemia Hyperglycaemia Diabetes and Illness sick day Diabetic Ketoacidosis HONK/HHS 2 What is Hypoglycaemia BG levels below 4mmol/l. Four is the Floor Floor
Sandra Coats Diabetes Specialist Nurse 1 Hypoglycaemia Hyperglycaemia Diabetes and Illness sick day Diabetic Ketoacidosis HONK/HHS 2 What is Hypoglycaemia BG levels below 4mmol/l. Four is the Floor Floor
The most recent estimates suggest that. A study of inpatient diabetes care on medical wards. Saqib Javed, Yaser Javed, Kate Barnabas, Kalpana Kaushal
 A study of inpatient diabetes care on medical wards Saqib Javed, Yaser Javed, Kate Barnabas, Kalpana Kaushal Article points 1. It is well established that poor glycaemic control is associated with increased
A study of inpatient diabetes care on medical wards Saqib Javed, Yaser Javed, Kate Barnabas, Kalpana Kaushal Article points 1. It is well established that poor glycaemic control is associated with increased
Objectives. Why is blood glucose important? Hypoglycaemia. Hyperglycaemia. Acute Diabetes Emergencies (DKA,HONK)
") Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow September 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood
Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow September 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood
Objectives. Why is blood glucose important? Hypoglycaemia. Hyperglycaemia. Acute Diabetes Emergencies (DKA,HONK)
") Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow June 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood Glucose
Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow June 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood Glucose
End of Life Diabetes Care
 End of Life Diabetes Care Commissioned by Diabetes UK Supplementary Documents and Flowcharts Endorsed By: Diabetes Phases of End of Life and Medications A - Blue: All From Diagnosis Stable With Year Plus
End of Life Diabetes Care Commissioned by Diabetes UK Supplementary Documents and Flowcharts Endorsed By: Diabetes Phases of End of Life and Medications A - Blue: All From Diagnosis Stable With Year Plus
PROCEDURE FOR BLOOD GLUCOSE MONITORING
 PROCEDURE FOR BLOOD GLUCOSE MONITORING First Issued Issue Version Two Purpose of Issue/Description of Change Planned Review Date To promote safe and effective blood glucose monitoring using Trust equipment
PROCEDURE FOR BLOOD GLUCOSE MONITORING First Issued Issue Version Two Purpose of Issue/Description of Change Planned Review Date To promote safe and effective blood glucose monitoring using Trust equipment
Managing Hyperglycaemia in Acute (Adult) Inpatients Requiring Enteral Feeding Guidelines
 Inpatients Requiring Enteral Feeding Guidelines") Document Control Title Managing Hyperglycaemia in Acute (Adult) Inpatients Requiring Author Author s job title Specialist Nurse Consultant Physician Department Directorate Unscheduled Care Version Date
Document Control Title Managing Hyperglycaemia in Acute (Adult) Inpatients Requiring Author Author s job title Specialist Nurse Consultant Physician Department Directorate Unscheduled Care Version Date
New NICE guidance: Changes in practice for multidisciplinary teams. Part 1: Type 1 diabetes in children and young people
 Article New NICE guidance: Changes in practice for multidisciplinary teams. Part 1: Type 1 diabetes in children and young people Helen Thornton This is the first of two articles on the 2015 NICE NG18 guideline,
Article New NICE guidance: Changes in practice for multidisciplinary teams. Part 1: Type 1 diabetes in children and young people Helen Thornton This is the first of two articles on the 2015 NICE NG18 guideline,
Guidelines for the management of agitation in the last weeks of life
 Guidelines for the management of agitation in the last weeks of life 14.09.17 Overview 1. Aim 2. Literature Review 3. Current Standards 4. Audit Results 5. Patient Representative Input 6. Proposed New
Guidelines for the management of agitation in the last weeks of life 14.09.17 Overview 1. Aim 2. Literature Review 3. Current Standards 4. Audit Results 5. Patient Representative Input 6. Proposed New
Training booklet for understanding. Hypoglycaemia - LOW Blood glucose levels Hyperglycaemia - HIGH Blood glucose levels
 Integrated Community Diabetes Services The Poynt, Units 2-3 Poynters Road Luton, LU4 0LA Tel: 0333 405 3128 Training booklet for understanding Hypoglycaemia - LOW Blood glucose levels Hyperglycaemia -
Integrated Community Diabetes Services The Poynt, Units 2-3 Poynters Road Luton, LU4 0LA Tel: 0333 405 3128 Training booklet for understanding Hypoglycaemia - LOW Blood glucose levels Hyperglycaemia -
Executive Summary Management of Type 1 Diabetes Mellitus during illness in children and young people under 18 years (Sick Day Rules)
") Executive Summary Management of Type 1 Diabetes Mellitus during illness in children and young people under 18 years (Sick Day Rules) SETTING FOR STAFF PATIENTS Medical and nursing staff Children and young
Executive Summary Management of Type 1 Diabetes Mellitus during illness in children and young people under 18 years (Sick Day Rules) SETTING FOR STAFF PATIENTS Medical and nursing staff Children and young
Endoscopy or colonoscopy guidelines
 Endoscopy or colonoscopy guidelines for patients with diabetes The development and audit of local pilot guidelines for patients with diabetes undergoing an endoscopy or colonoscopy as an out-patient D
Endoscopy or colonoscopy guidelines for patients with diabetes The development and audit of local pilot guidelines for patients with diabetes undergoing an endoscopy or colonoscopy as an out-patient D
Nutritional Screening Assessment in Palliative Care Standard Operating Procedure
 Nutritional Screening Assessment in Palliative Care Standard Operating Procedure DOCUMENT CONTROL: Version: 1 Ratified by: Clinical Quality and Standards Group Date ratified: 5 January 2016 Name of originator/author:
Nutritional Screening Assessment in Palliative Care Standard Operating Procedure DOCUMENT CONTROL: Version: 1 Ratified by: Clinical Quality and Standards Group Date ratified: 5 January 2016 Name of originator/author:
The principles of insulin adjustment guidance
 The principles of insulin adjustment guidance Tips for insulin titration Blood glucose (BG) monitoring is needed to help identify the efficacy of treatment in diabetes. Monitor blood glucose according
The principles of insulin adjustment guidance Tips for insulin titration Blood glucose (BG) monitoring is needed to help identify the efficacy of treatment in diabetes. Monitor blood glucose according
Individual healthcare plan for Type 1 diabetes. for children/young people with diabetes in schools and Early Years settings
 Individual healthcare plan for Type 1 diabetes for children/young people with diabetes in schools and Early Years settings Individual healthcare plan for Type 1 diabetes for children/young people with
Individual healthcare plan for Type 1 diabetes for children/young people with diabetes in schools and Early Years settings Individual healthcare plan for Type 1 diabetes for children/young people with
9 Diabetes care. Back to contents
 Back to contents Diabetes is a major risk factor for the development of peripheral vascular disease and 349/628 (55.6%) of the patients in this study had diabetes. Hospital inpatients with diabetes are
Back to contents Diabetes is a major risk factor for the development of peripheral vascular disease and 349/628 (55.6%) of the patients in this study had diabetes. Hospital inpatients with diabetes are
Audit support for continuous subcutaneous insulin infusion for the treatment of diabetes mellitus (review of technology appraisal guidance 57)
") Audit support for continuous subcutaneous insulin (review of technology appraisal guidance 57) Issue date: 2008 Audit support Continuous subcutaneous insulin infusion for the treatment of diabetes mellitus
Audit support for continuous subcutaneous insulin (review of technology appraisal guidance 57) Issue date: 2008 Audit support Continuous subcutaneous insulin infusion for the treatment of diabetes mellitus
National Diabetes Inpatient Audit (NaDIA) 2016
 2016") National Diabetes Inpatient Audit (NaDIA) 2016 DIABETES A summary report for people with diabetes and anyone interested in the quality of care for people with diabetes when they stay in hospital. Based
National Diabetes Inpatient Audit (NaDIA) 2016 DIABETES A summary report for people with diabetes and anyone interested in the quality of care for people with diabetes when they stay in hospital. Based
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
Developing a pathway of. and care planning for people with diabetes
 Developing a pathway of preoperative assessment and care planning for people with diabetes Louise Hilton, Marie Digner Diabetes is a common endocrine condition affecting 1.4 million people in the UK, with
Developing a pathway of preoperative assessment and care planning for people with diabetes Louise Hilton, Marie Digner Diabetes is a common endocrine condition affecting 1.4 million people in the UK, with
SERVICE SPECIFICATION 6 Conservative Management & End of Life Care
 SERVICE SPECIFICATION 6 Conservative Management & End of Life Care Table of Contents Page 1 Key Messages 2 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies
SERVICE SPECIFICATION 6 Conservative Management & End of Life Care Table of Contents Page 1 Key Messages 2 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies
NHS Greater Glasgow & Clyde Managed Clinical Network for Diabetes
 Guidelines for the Diagnosis of Diabetes Mellitus NHS Greater Glasgow & Clyde Managed Clinical Network for Diabetes Lead Authors: Dr Brian Kennon, Dr David Carty June 2015 Review due: December 2016 Diagnosis
Guidelines for the Diagnosis of Diabetes Mellitus NHS Greater Glasgow & Clyde Managed Clinical Network for Diabetes Lead Authors: Dr Brian Kennon, Dr David Carty June 2015 Review due: December 2016 Diagnosis
Information for all patients taking insulin who are admitted to hospital on day of surgery
 Information for all patients taking insulin who are admitted to hospital on day of surgery Exceptional healthcare, personally delivered Introduction Many patients are now admitted to hospital on the day
Information for all patients taking insulin who are admitted to hospital on day of surgery Exceptional healthcare, personally delivered Introduction Many patients are now admitted to hospital on the day
TYPE 2 DIABETES AND STEROID TABLETS
 MEDICATION TYPE 2 DIABETES AND STEROID TABLETS WHY IS THIS LEAFLET FOR YOU? Taking steroid treatment when you have diabetes can make your blood glucose levels more difficult to control. This leaflet will
MEDICATION TYPE 2 DIABETES AND STEROID TABLETS WHY IS THIS LEAFLET FOR YOU? Taking steroid treatment when you have diabetes can make your blood glucose levels more difficult to control. This leaflet will
Diabetes and steroids: Storm conditions
 Article Diabetes and steroids: Storm conditions June James Citation: James J (2016) Diabetes and steroids: Storm conditions. Journal of Diabetes Nursing 20: 128 33 Article points 1. Steroids are often
Article Diabetes and steroids: Storm conditions June James Citation: James J (2016) Diabetes and steroids: Storm conditions. Journal of Diabetes Nursing 20: 128 33 Article points 1. Steroids are often
DIABETES AND RAMADAN FASTING
 DIABETES AND RAMADAN FASTING Dr. A. Nigam, M.B.B.S., M.D. (Medicine) Specialist Internal Medicine Al Zahrawi Hospital, Ras Al Khaimah, U.A.E. It is estimated that UAE s population currently stands at approximately
DIABETES AND RAMADAN FASTING Dr. A. Nigam, M.B.B.S., M.D. (Medicine) Specialist Internal Medicine Al Zahrawi Hospital, Ras Al Khaimah, U.A.E. It is estimated that UAE s population currently stands at approximately
Policy for the Provision of Insulin Pumps for Patients with Diabetes Mellitus
 Policy for the Provision of Insulin Pumps for Patients with Diabetes Mellitus Version No. Changes Made Version of July 2018 V0.5 Changes made to the policy following patient engagement including: - the
Policy for the Provision of Insulin Pumps for Patients with Diabetes Mellitus Version No. Changes Made Version of July 2018 V0.5 Changes made to the policy following patient engagement including: - the
Essential Shared Care Agreement: Lithium
 Ref No. E042 Essential Shared Care Agreement: Lithium Please complete the following details: Patient s name, address, date of birth Treatment (indication, dose regimen, brand name) Monitoring (proposed
Ref No. E042 Essential Shared Care Agreement: Lithium Please complete the following details: Patient s name, address, date of birth Treatment (indication, dose regimen, brand name) Monitoring (proposed
Guidelines for managing people with diabetes at the end of life
 Guidelines for managing people with diabetes at the end of life Guidelines for managing people with diabetes at the end of life FINAL REPORT June 2010 Trisha Dunning Peter Martin Sally Savage Nicole Duggan
Guidelines for managing people with diabetes at the end of life Guidelines for managing people with diabetes at the end of life FINAL REPORT June 2010 Trisha Dunning Peter Martin Sally Savage Nicole Duggan
Placename CCG. Policies for the Commissioning of Healthcare
 Placename CCG Policies for the Commissioning of Healthcare Policy for the Provision of Continuous Glucose Monitoring and Flash Glucose Monitoring to patients with Diabetes Mellitus. This document is part
Placename CCG Policies for the Commissioning of Healthcare Policy for the Provision of Continuous Glucose Monitoring and Flash Glucose Monitoring to patients with Diabetes Mellitus. This document is part
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Continuous subcutaneous insulin infusion for the treatment of diabetes (review) Final scope Appraisal objective To review
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal Continuous subcutaneous insulin infusion for the treatment of diabetes (review) Final scope Appraisal objective To review
Diabetes is a lifelong, chronic. Survey on the quality of diabetes care in prison settings across the UK. Keith Booles
 Survey on the quality of diabetes care in prison settings across the UK Article points 1. The Royal College of Nursing Diabetes Forum conducted an audit of prisons within the UK to determine the level
Survey on the quality of diabetes care in prison settings across the UK Article points 1. The Royal College of Nursing Diabetes Forum conducted an audit of prisons within the UK to determine the level
Quality of Life (F309 End of Life) Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol
 Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol") 483.25 Quality of Life (F309 End of Life) Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol 2 483.25 End of Life Each resident must receive and the facility must provide the necessary
483.25 Quality of Life (F309 End of Life) Surveyor Train the Trainer: Interpretive Guidance Investigative Protocol 2 483.25 End of Life Each resident must receive and the facility must provide the necessary
This guideline was adapted in collaboration with Dr Georgina Walker and the Palliative Care Team at Rowcroft Hospice. With thanks.
 Title: Directorate: Responsible for review: Ratified by: DIABETES, MANAGEMENT OF IN PALLIATIVE CARE PATIENTS General Medicine Diabetes Specialist Nurse Service Delivery Unit Clinical Director of Pharmacy
Title: Directorate: Responsible for review: Ratified by: DIABETES, MANAGEMENT OF IN PALLIATIVE CARE PATIENTS General Medicine Diabetes Specialist Nurse Service Delivery Unit Clinical Director of Pharmacy
undiagnosed type 1 diabetes in children is a medical emergency. A Healthcare Professionals guide to an early diagnosis
 undiagnosed type 1 diabetes in children is a medical emergency. A Healthcare Professionals guide to an early diagnosis Improving early diagnosis of diabetes in the young How can we diagnose Type 1 diabetes
undiagnosed type 1 diabetes in children is a medical emergency. A Healthcare Professionals guide to an early diagnosis Improving early diagnosis of diabetes in the young How can we diagnose Type 1 diabetes
NHS GG&C Introduction of Freestyle Libre flash glucose monitoring system
 NHS GG&C Introduction of Freestyle Libre flash glucose monitoring system The Freestyle Libre flash glucose monitoring system is a sensor based, factory-calibrated system that measures interstitial fluid
NHS GG&C Introduction of Freestyle Libre flash glucose monitoring system The Freestyle Libre flash glucose monitoring system is a sensor based, factory-calibrated system that measures interstitial fluid
Controlling nausea and vomiting: anti-emetic therapy advice
 Controlling nausea and vomiting: anti-emetic therapy advice Chemotherapy A guide for patients and carers Contents Treatments that may cause nausea and vomiting... 2 Physical reasons that may cause nausea
Controlling nausea and vomiting: anti-emetic therapy advice Chemotherapy A guide for patients and carers Contents Treatments that may cause nausea and vomiting... 2 Physical reasons that may cause nausea
Specialist Palliative Care Service Referral Criteria and Guidance
 Specialist Palliative Care Service Referral Criteria and Guidance Specialist Palliative Care Service Referrals These guidelines cover referrals for patients with progressive terminal illness, whether
Specialist Palliative Care Service Referral Criteria and Guidance Specialist Palliative Care Service Referrals These guidelines cover referrals for patients with progressive terminal illness, whether
Hyperglycemia Procedure: Management and Treatment Adult Patients
 Approved by: Chief Operating Officer; and Chief Medical Officer Hyperglycemia Procedure: Management and Treatment Corporate Policy & Procedures Manual Number: VII-B-465 Date Approved January 23, 2018 Date
Approved by: Chief Operating Officer; and Chief Medical Officer Hyperglycemia Procedure: Management and Treatment Corporate Policy & Procedures Manual Number: VII-B-465 Date Approved January 23, 2018 Date
MANAGEMENT OF PREGNANT WOMEN WITH DIABETES WHO ARE IN-PATIENTS IN THE ROYAL INFIRMARY
 MANAGEMENT OF PREGNANT WOMEN WITH DIABETES WHO ARE IN-PATIENTS IN THE ROYAL INFIRMARY Background Management is different in different groups of women with diabetes. Women with Type 1 Diabetes (previously
MANAGEMENT OF PREGNANT WOMEN WITH DIABETES WHO ARE IN-PATIENTS IN THE ROYAL INFIRMARY Background Management is different in different groups of women with diabetes. Women with Type 1 Diabetes (previously
Essential advice for people with diabetes from Accu-Chek. Get the low-down on hypos
 Essential advice for people with diabetes from Accu-Chek Get the low-down on hypos The low-down on hypos If you have diabetes, a hypo is one of those things you have to deal with from time to time. FIRST
Essential advice for people with diabetes from Accu-Chek Get the low-down on hypos The low-down on hypos If you have diabetes, a hypo is one of those things you have to deal with from time to time. FIRST
Monitoring in Type 2 Diabetes. Learning Outcomes. Type 2 Diabetes. Senga Hunter Community Diabetes Specialist Nurse
 Monitoring in Type 2 Diabetes Senga Hunter Community Diabetes Specialist Nurse Learning Outcomes Understand why blood monitoring is necessary Understand the blood tests for monitoring diabetes Understand
Monitoring in Type 2 Diabetes Senga Hunter Community Diabetes Specialist Nurse Learning Outcomes Understand why blood monitoring is necessary Understand the blood tests for monitoring diabetes Understand
Personal statement on Continuous Subcutaneous Insulin Infusion Professor John Pickup
 1 Personal statement on Continuous Subcutaneous Insulin Infusion Professor John Pickup King s College London School of Medicine, Guy s Hospital, London SE1 9RT Experience of the technology I am the lead
1 Personal statement on Continuous Subcutaneous Insulin Infusion Professor John Pickup King s College London School of Medicine, Guy s Hospital, London SE1 9RT Experience of the technology I am the lead
Unit reference number T/616/7338 Level: 3. Credit value: 6 Guided learning hours: 46. Unit summary
 Unit 28: Awareness of Diabetes Unit reference number T/616/7338 Level: 3 Unit type: Optional Credit value: 6 Guided learning hours: 46 Unit summary It is estimated that more than 3.8 million people over
Unit 28: Awareness of Diabetes Unit reference number T/616/7338 Level: 3 Unit type: Optional Credit value: 6 Guided learning hours: 46 Unit summary It is estimated that more than 3.8 million people over
GUIDELINES FOR THE MANAGEMENT OF URINARY INCONTINENCE IN THE PALLIATIVE CARE SETTING
 GUIDELINES FOR THE MANAGEMENT OF URINARY INCONTINENCE IN THE PALLIATIVE CARE SETTING 43.1 GENERAL PRINCIPLES Urinary continence can be defined as the ability to store urine in the bladder and to excrete
GUIDELINES FOR THE MANAGEMENT OF URINARY INCONTINENCE IN THE PALLIATIVE CARE SETTING 43.1 GENERAL PRINCIPLES Urinary continence can be defined as the ability to store urine in the bladder and to excrete
Blood Glucose monitoring during extra-corporeal renal therapy and plasmapheresis.
 Blood Glucose monitoring during extra-corporeal renal therapy and plasmapheresis. Lead Clinician: Dr. R. Diwakar Implementation date: July 2013 Last updated: August 2017 Last review date: Planned review
Blood Glucose monitoring during extra-corporeal renal therapy and plasmapheresis. Lead Clinician: Dr. R. Diwakar Implementation date: July 2013 Last updated: August 2017 Last review date: Planned review
2012 Edition. Part B: 3 3. DIABETES MELLITUS Effects of diabetes on driving Evidence of crash risk. 3.2.
 2012 Edition DIABETES MELLITUS 3. DIABETES MELLITUS Refer also to section 6 Neurological conditions, section 2 Cardiovascular conditions, section 8 Sleep disorders section 10 Vision eye disorders. 3.1
2012 Edition DIABETES MELLITUS 3. DIABETES MELLITUS Refer also to section 6 Neurological conditions, section 2 Cardiovascular conditions, section 8 Sleep disorders section 10 Vision eye disorders. 3.1
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Policy for Continuous Glucose Monitoring for Type 1 Diabetic Paediatric Patients (<18 years of age)
") Policy for Continuous Glucose Monitoring for Type 1 Diabetic Paediatric Patients (
Policy for Continuous Glucose Monitoring for Type 1 Diabetic Paediatric Patients (
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER
 1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
Clinical Guidelines. Management of adult patients with diabetes undergoing endoscopic procedures
 Clinical Guidelines Management of adult patients with diabetes undergoing endoscopic s Document Detail Document type Clinical Guideline Management of adult Patients with diabetes Undergoing Document name
Clinical Guidelines Management of adult patients with diabetes undergoing endoscopic s Document Detail Document type Clinical Guideline Management of adult Patients with diabetes Undergoing Document name
ANZCOR Guideline First aid Management of a Diabetic Emergency
 ANZCOR Guideline 9.2.9 First aid Management of a Diabetic Emergency Summary Who does this guideline apply to? This guideline applies to adult and child victims. Who is the audience for this guideline?
ANZCOR Guideline 9.2.9 First aid Management of a Diabetic Emergency Summary Who does this guideline apply to? This guideline applies to adult and child victims. Who is the audience for this guideline?
THE SHEFFIELD AREA PRESCRIBING GROUP. Position Statement for Prescribing of Freestyle Libre In Type 1 Diabetes. Date: March 2018.
 THE SHEFFIELD AREA PRESCRIBING GROUP Position Statement for Prescribing of Freestyle Libre In Type 1 Diabetes Date: March 2018 Overview Freestyle Libre is a flash glucose sensor device that measures *interstitial
THE SHEFFIELD AREA PRESCRIBING GROUP Position Statement for Prescribing of Freestyle Libre In Type 1 Diabetes Date: March 2018 Overview Freestyle Libre is a flash glucose sensor device that measures *interstitial
Hydration at the End of Life:
 Hydration at the End of Life: A systematic literature review and audit of current practice November 12 th 2015 Dr Alison Coackley- Consultant in Palliative Medicine, Clatterbridge Cancer Centre Dr Catherine
Hydration at the End of Life: A systematic literature review and audit of current practice November 12 th 2015 Dr Alison Coackley- Consultant in Palliative Medicine, Clatterbridge Cancer Centre Dr Catherine
Placename CCG. Policies for the Commissioning of Healthcare
 Placename CCG Policies for the Commissioning of Healthcare Policy for the funding of insulin pumps and continuous glucose monitoring devices for patients with diabetes 1 Introduction 1.1 This document
Placename CCG Policies for the Commissioning of Healthcare Policy for the funding of insulin pumps and continuous glucose monitoring devices for patients with diabetes 1 Introduction 1.1 This document
PERIOPERATIVE DIABETES GUIDELINE
 PERIOPERATIVE DIABETES GUIDELINE This Guideline does not replace the need for the application of clinical judgment in respect to each individual patient. Background Diabetes mellitus is estimated to affect
PERIOPERATIVE DIABETES GUIDELINE This Guideline does not replace the need for the application of clinical judgment in respect to each individual patient. Background Diabetes mellitus is estimated to affect
Management of adults with diabetes undergoing surgery and elective procedures: Improving standards
 Management of adults with diabetes undergoing surgery and elective procedures: Improving standards Revised September 2015 Changes in the second edition of the peri-operative document Preoperative pathway
Management of adults with diabetes undergoing surgery and elective procedures: Improving standards Revised September 2015 Changes in the second edition of the peri-operative document Preoperative pathway
Blood Glucose and Hyperglycaemia Management in Hospital for Adults with Diabetes Clinical Guideline V2.0. March 2018
 Blood Glucose and Hyperglycaemia Management in Hospital for Adults with Diabetes Clinical Guideline V2.0 March 2018 Page 1 of 8 Summary flow chart for monitoring of blood glucose if >11mmol/L For Adults
Blood Glucose and Hyperglycaemia Management in Hospital for Adults with Diabetes Clinical Guideline V2.0 March 2018 Page 1 of 8 Summary flow chart for monitoring of blood glucose if >11mmol/L For Adults
SHARED CARE GUIDELINE ON THE USE OF FIASP FOR THE MANAGEMENT OF TYPE 1 DIABETES IN ADULTS
 SHARED CARE GUIDELINE ON THE USE OF FIASP FOR THE MANAGEMENT OF TYPE 1 DIABETES IN ADULTS INDICATION Fiasp is indicated for the treatment of diabetes mellitus in adults. Special Note: DMAG has approved
SHARED CARE GUIDELINE ON THE USE OF FIASP FOR THE MANAGEMENT OF TYPE 1 DIABETES IN ADULTS INDICATION Fiasp is indicated for the treatment of diabetes mellitus in adults. Special Note: DMAG has approved
CASE 8 Unwell insulin-dependent diabetic
 50 CASE 8 Unwell insulin-dependent diabetic INFORMATION FOR THE DOCTOR This is a telephone consultation. Name Michael Ede Age 29 Past medical history Type 1 diabetes 2 years ago Patello-femoral knee joint
50 CASE 8 Unwell insulin-dependent diabetic INFORMATION FOR THE DOCTOR This is a telephone consultation. Name Michael Ede Age 29 Past medical history Type 1 diabetes 2 years ago Patello-femoral knee joint
Response to the proposed advice for health and social care practitioners involved in looking after people in the last days of life
 Response to the proposed advice for health and social care practitioners involved in looking after people in the last days of life Introduction i. Few conditions are as devastating as motor neurone disease
Response to the proposed advice for health and social care practitioners involved in looking after people in the last days of life Introduction i. Few conditions are as devastating as motor neurone disease
EFFECTIVE SHARE CARE AGREEMENT. FOR THE off license use of GLP1 mimetics in combination with insulin IN DUDLEY
 Specialist details Patient identifier Name Tel: EFFECTIVE SHARE CARE AGREEMENT FOR THE off license use of GLP1 mimetics in combination with insulin IN DUDLEY The aim of Effective Shared Care Guidelines
Specialist details Patient identifier Name Tel: EFFECTIVE SHARE CARE AGREEMENT FOR THE off license use of GLP1 mimetics in combination with insulin IN DUDLEY The aim of Effective Shared Care Guidelines
People living with type 1 diabetes face a. Barriers to improving glycaemic control in CSII. Joan Everett, Anita Bowes, David Kerr
 Barriers to improving glycaemic control in CSII Article points 1. Focus groups were conducted to determine why some people with type 1 diabetes using continuous subcutaneous insulin infusion (CSII) maintain
Barriers to improving glycaemic control in CSII Article points 1. Focus groups were conducted to determine why some people with type 1 diabetes using continuous subcutaneous insulin infusion (CSII) maintain
Annual Audit Review Meeting. Welcome
 Cheshire and Merseyside Palliative and End of Life Care Network Annual Audit Review Meeting 03/03/2016 Welcome Today s Agenda 1. Welcome and Overview Dr Alison Coackley 2. Review of 2015/2016 Highlights
Cheshire and Merseyside Palliative and End of Life Care Network Annual Audit Review Meeting 03/03/2016 Welcome Today s Agenda 1. Welcome and Overview Dr Alison Coackley 2. Review of 2015/2016 Highlights
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE GUIDANCE EXECUTIVE (GE)
") NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE GUIDANCE EXECUTIVE (GE) Review of TA151 Continuous subcutaneous insulin infusion for the treatment of diabetes mellitus This guidance was issued in
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE GUIDANCE EXECUTIVE (GE) Review of TA151 Continuous subcutaneous insulin infusion for the treatment of diabetes mellitus This guidance was issued in
Community and Mental Health Services. Palliative Care. Criteria and
 Community and Mental Health Services Specialist Palliative Care Service Referral Criteria and Guidance November 2018 Specialist Palliative Care Service Referrals These guidelines cover referrals for patients
Community and Mental Health Services Specialist Palliative Care Service Referral Criteria and Guidance November 2018 Specialist Palliative Care Service Referrals These guidelines cover referrals for patients
PHARMACOLOGY AND PHARMACOKINETICS
 DRUG GUIDELINE Insulin, human neutral (Actrapid ) Intravenous Infusion for SCOPE (Area): FOR USE IN: Critical Care Unit, Emergency Department and Operating Suite EXCLUSIONS: Paediatrics (seek Paediatrician
DRUG GUIDELINE Insulin, human neutral (Actrapid ) Intravenous Infusion for SCOPE (Area): FOR USE IN: Critical Care Unit, Emergency Department and Operating Suite EXCLUSIONS: Paediatrics (seek Paediatrician
Unmet palliative care needs in heart failure heart failure. Dr Claire Hookey
 Unmet palliative care needs in heart failure heart failure Dr Claire Hookey Discomfort was not necessarily greatest in those dying from cancer; patients dying of heart failure, or renal failure, or both,
Unmet palliative care needs in heart failure heart failure Dr Claire Hookey Discomfort was not necessarily greatest in those dying from cancer; patients dying of heart failure, or renal failure, or both,
Intrathecal chemotherapy
 Intrathecal chemotherapy Chemotherapy A guide for patients and carers Contents What is intrathecal chemotherapy?... 1 Why do I need intrathecal chemotherapy?... 1 What will happen before the procedure?...
Intrathecal chemotherapy Chemotherapy A guide for patients and carers Contents What is intrathecal chemotherapy?... 1 Why do I need intrathecal chemotherapy?... 1 What will happen before the procedure?...
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE TREATMENT OF HYPERGLYCEMIA - ADULT SCOPE Provincial: Acute Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Diabetes, Obesity & Nutrition Strategic Clinical Network PARENT
TITLE TREATMENT OF HYPERGLYCEMIA - ADULT SCOPE Provincial: Acute Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Diabetes, Obesity & Nutrition Strategic Clinical Network PARENT
NCEPOD - Measuring the Units; A review of patients who died with alcohol-related liver disease
 NCEPOD - Measuring the Units; A review of patients who died with alcohol-related liver disease Hospital Number Admission to hospital 5. Trusts should ensure that medical patients are reviewed by a consultant
NCEPOD - Measuring the Units; A review of patients who died with alcohol-related liver disease Hospital Number Admission to hospital 5. Trusts should ensure that medical patients are reviewed by a consultant
DIABETES AND ENTERAL FEEDING
 DIABETES AND ENTERAL FEEDING kk WHY IS THIS LEAFLET FOR YOU? This leaflet is for people with diabetes established on an enteral feeding regimen, and for the people who support them at home, in residential
DIABETES AND ENTERAL FEEDING kk WHY IS THIS LEAFLET FOR YOU? This leaflet is for people with diabetes established on an enteral feeding regimen, and for the people who support them at home, in residential
Peri-operative management of the surgical patient with diabetes GL059
 DT Peri-operative management of the surgical patient with diabetes GL059 Approval Approval Group Job Title, Chair of Committee Date Anaesthetics Clinical Governance Chair Anaesthetic governance Nov 2016
DT Peri-operative management of the surgical patient with diabetes GL059 Approval Approval Group Job Title, Chair of Committee Date Anaesthetics Clinical Governance Chair Anaesthetic governance Nov 2016
The Scottish Public Services Ombudsman Act 2002
 Scottish Public Services Ombudsman The Scottish Public Services Ombudsman Act 2002 Investigation Report UNDER SECTION 15(1)(a) SPSO 4 Melville Street Edinburgh EH3 7NS Tel 0800 377 7330 SPSO Information
Scottish Public Services Ombudsman The Scottish Public Services Ombudsman Act 2002 Investigation Report UNDER SECTION 15(1)(a) SPSO 4 Melville Street Edinburgh EH3 7NS Tel 0800 377 7330 SPSO Information
5. Diabetes Education
 5. iabetes Education 5.1. Structured education aimed at families and/or patients with diabetes mellitus Key question: Are structured educational programs aimed at people with diabetes mellitus type 1 and
5. iabetes Education 5.1. Structured education aimed at families and/or patients with diabetes mellitus Key question: Are structured educational programs aimed at people with diabetes mellitus type 1 and
Hypoglyceamia and Exercise
 Hypoglyceamia and Exercise Noreen Barker Diabetes Specialist Nurse May 2016 Hypoglyceamia What is a hypo? Why are we concerned? Signs and symptoms Treatments Causes Hypo unawareness Managing diabetes and
Hypoglyceamia and Exercise Noreen Barker Diabetes Specialist Nurse May 2016 Hypoglyceamia What is a hypo? Why are we concerned? Signs and symptoms Treatments Causes Hypo unawareness Managing diabetes and
THE FACTS ABOUT FASTING DURING RAMADAN INFORMATION KIT FOR PEOPLE WITH TYPE 2 DIABETES
 THE FACTS ABOUT FASTING DURING RAMADAN INFORMATION KIT FOR PEOPLE WITH TYPE 2 DIABETES INTRODUCTION This information kit is designed to provide you with facts and practical advice about fasting during
THE FACTS ABOUT FASTING DURING RAMADAN INFORMATION KIT FOR PEOPLE WITH TYPE 2 DIABETES INTRODUCTION This information kit is designed to provide you with facts and practical advice about fasting during
Certificate of Merit in Disorders of the Body Lesson 2: Epilepsy, Diabetes and Multiple Sclerosis
 Certificate of Merit in Disorders of the Body Lesson 2: Epilepsy, Diabetes and Multiple Sclerosis Epilepsy Epilepsy is a condition in which there is a sudden burst of electrical energy in the brain, which
Certificate of Merit in Disorders of the Body Lesson 2: Epilepsy, Diabetes and Multiple Sclerosis Epilepsy Epilepsy is a condition in which there is a sudden burst of electrical energy in the brain, which
Lynda Astbury Lead Diabetes Specialist Nurse
 Lynda Astbury Lead Diabetes Specialist Nurse WARNING SIGNS AND SYMPTOMS Is patient Feeling unwell? Blood glucose level above 13mmol/L Or higher than the patients day to day readings (even if not eating)
Lynda Astbury Lead Diabetes Specialist Nurse WARNING SIGNS AND SYMPTOMS Is patient Feeling unwell? Blood glucose level above 13mmol/L Or higher than the patients day to day readings (even if not eating)
Information for Patients
 Information for Patients Guidance for Diabetic Persons having an OGD or Bronchoscopy This guidance is provided to assist with your preparation for your endoscopic procedure. If you feel unclear about how
Information for Patients Guidance for Diabetic Persons having an OGD or Bronchoscopy This guidance is provided to assist with your preparation for your endoscopic procedure. If you feel unclear about how
Specialist Palliative Care Audit and Guidelines Group (SPAGG)
") Specialist Palliative Care Audit and Guidelines Group (SPAGG) Clinical Guideline for the Prescribing and Administration of Furosemide via continuous subcutaneous infusion (CSCI) for Heart Failure Patients
Specialist Palliative Care Audit and Guidelines Group (SPAGG) Clinical Guideline for the Prescribing and Administration of Furosemide via continuous subcutaneous infusion (CSCI) for Heart Failure Patients
COMPLIANCE WITH THIS DOCUMENT IS MANDATORY
 COVER SHEET `NAME OF DOCUMENT TYPE OF DOCUMENT at Shoalhaven Hospital Group Critical Care Procedure DOCUMENT NUMBER DATE OF PUBLICATION February 2018 RISK RATING Medium REVIEW DATE February 2021 FORMER
COVER SHEET `NAME OF DOCUMENT TYPE OF DOCUMENT at Shoalhaven Hospital Group Critical Care Procedure DOCUMENT NUMBER DATE OF PUBLICATION February 2018 RISK RATING Medium REVIEW DATE February 2021 FORMER
Diabetes, Ketone testing in Type 1 Diabetes
 CLINICAL GUIDELINE Diabetes, Ketone testing in Type 1 Diabetes A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised
CLINICAL GUIDELINE Diabetes, Ketone testing in Type 1 Diabetes A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised
GUIDELINES FOR CONVERSION FROM A STRONG OPIOID TO METHADONE
 GUIDELINES FOR CONVERSION FROM A STRONG OPIOID TO METHADONE GENERAL PRINCIPLES Methadone may be used as a strong opioid alternative when severe cancer-related pain responds poorly to other opioids, or
GUIDELINES FOR CONVERSION FROM A STRONG OPIOID TO METHADONE GENERAL PRINCIPLES Methadone may be used as a strong opioid alternative when severe cancer-related pain responds poorly to other opioids, or
667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY
 667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY Contents Introduction... 1 Patient Education for People with Type 2 Diabetes... 2 Dietary Advice for People with Type 2 Diabetes...
667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY Contents Introduction... 1 Patient Education for People with Type 2 Diabetes... 2 Dietary Advice for People with Type 2 Diabetes...
Diabetes. HED\ED:NS-BL 037-3rd
 Diabetes HED\ED:NS-BL 037-3rd Diabetes Diabetes mellitus is an epidemic disease and based on a recent study published on 2011, the estimated number of affected people is 366 million worldwide and the number
Diabetes HED\ED:NS-BL 037-3rd Diabetes Diabetes mellitus is an epidemic disease and based on a recent study published on 2011, the estimated number of affected people is 366 million worldwide and the number
Managing the Medically Compromised Patient in General Dental Practice Risk Assessment
 Managing the Medically Compromised Patient in General Dental Practice Risk Assessment Core subject Aim: To provide an outline of the risk factors that should be considered in order to provide the safe
Managing the Medically Compromised Patient in General Dental Practice Risk Assessment Core subject Aim: To provide an outline of the risk factors that should be considered in order to provide the safe
Northumbria Healthcare NHS Foundation Trust. Diabetes & Steroid Therapy. Issued by the Diabetes Service
 Northumbria Healthcare NHS Foundation Trust Diabetes & Steroid Therapy Issued by the Diabetes Service What are Steroids? Steroids (Corticosteroids) are a group of medicines that can be used in the treatment
Northumbria Healthcare NHS Foundation Trust Diabetes & Steroid Therapy Issued by the Diabetes Service What are Steroids? Steroids (Corticosteroids) are a group of medicines that can be used in the treatment
A Suite of Enhanced Services for. Prudent Structured Care for Adults with Type 2 Diabetes
 An Enhanced Service for Prudent Structured Care for Adults with Type 2 Diabetes Page 1 A Suite of Enhanced Services for Prudent Structured Care for Adults with Type 2 Diabetes 1. Introduction All practices
An Enhanced Service for Prudent Structured Care for Adults with Type 2 Diabetes Page 1 A Suite of Enhanced Services for Prudent Structured Care for Adults with Type 2 Diabetes 1. Introduction All practices
Transplanting donated pancreatic islet cells for patients with type 1 diabetes
 Understanding NICE guidance Information for people who use NHS services Transplanting donated pancreatic islet cells for patients with type 1 diabetes NICE interventional procedures guidance advises the
Understanding NICE guidance Information for people who use NHS services Transplanting donated pancreatic islet cells for patients with type 1 diabetes NICE interventional procedures guidance advises the
Palliative Care Asking the questions that matter to me
 Palliative Care Asking the questions that matter to me THE PALLIATIVE HUB Adult This booklet has been developed by the Palliative Care Senior Nurses Network and adapted with permission from Palliative
Palliative Care Asking the questions that matter to me THE PALLIATIVE HUB Adult This booklet has been developed by the Palliative Care Senior Nurses Network and adapted with permission from Palliative
Director of Quality & Nursing Clinical End of Life Diabetes Care. Via training and Community Trust Communications. Document Links. Amendments History
 Title Trust Ref No 2020- Local Ref (optional) Main points the document covers Who is the document aimed at? Author Approved by (Committee/Director) Document Details End Of Life Diabetes Care- commissioned
Title Trust Ref No 2020- Local Ref (optional) Main points the document covers Who is the document aimed at? Author Approved by (Committee/Director) Document Details End Of Life Diabetes Care- commissioned
Diabetes Management in New Brunswick Nursing Homes
 Diabetes Management in New Brunswick Nursing Homes Prepared by Dr. Angela McGibbon March, 2016 As the population ages and with the rising incidence of diabetes, there are increasing numbers of people with
Diabetes Management in New Brunswick Nursing Homes Prepared by Dr. Angela McGibbon March, 2016 As the population ages and with the rising incidence of diabetes, there are increasing numbers of people with
DIABETES STRUCTURED EDUCATION IN WORCESTERSHIRE Information for Healthcare Professionals May 2011
 DIABETES STRUCTURED EDUCATION IN WORCESTERSHIRE Information for Healthcare Professionals May 2011 What is Structured Education? Diabetes Structured Education is referred to in the Diabetes NSF standards
DIABETES STRUCTURED EDUCATION IN WORCESTERSHIRE Information for Healthcare Professionals May 2011 What is Structured Education? Diabetes Structured Education is referred to in the Diabetes NSF standards