How do we diagnose hypertension today? Presentation Subtitle
|
|
|
- Cassandra Crawford
- 5 years ago
- Views:
Transcription

1 How do we diagnose hypertension today? Presentation Subtitle Renata Cífková
2 Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal history: unremarkable, healthy, menopause at the age of glaucoma diagnosed Hypertension diagnosed in October 2014 while having a preventive checkup (aged 62), antihypertensive medication was initiated immediately: irbesartan 150 mg/hydrochlorothiazide 12.5 mg o.d. bisoprolol 5 mg o.d. She felt dizzy while on medication, particularly when changing the position, therefore, she decided to reduce doses of her prescribed medication. Renata Cífková
3 Case 1 Is it correct to initiate antihypertensive medication with a combination of drugs? A. Yes B. No Renata Cífková
 Single agent Two-drug combination Switch to")
4 2013 ESH/ESC Hypertension Guidelines Monotherapy vs. drug combination strategies to achieve target BP Mild BP elevation Low/moderate CV risk Choose between Marked BP elevation High/very high CV risk (IIbC) Single agent Two-drug combination Switch to different agent Previous agent at full dose Previous combination at full dose Add a third drug Full dose monotherapy Two drug combination at full doses Switch to different two-drug combination Three drug combination at full doses Moving from a less intensive to a more intensive therapeutic strategy should be done whenever BP target is not achieved.
5 Case 1 Body weight 56.4 kg, height 156 cm, BMI 23.2 kg/m 2 ; Office BP (mercury sphygmomanometer; Baumanometer; W.A. Baum Co. Inc., New York, NY, USA): 184/102 mmhg 164/94 mmhg 156/96 mmhg 174/94 mmhg Mean of 4 readings: 170/97 mmhg Renata Cífková
6 Case 1 What is the BP goal for this patient? A. < 130/80 mmhg B. < 140/90 mmhg C. < 150/90 mmhg Renata Cífková
7 What the guidelines tell us J Hypertens 2013;31: Renata Cífková
8 Case 1 What is the BP goal for this patient? A. < 130/80 mmhg B. < 140/90 mmhg C. < 150/90 mmhg Renata Cífková
9 2013 ESH/ESC guidelines for management of arterial hypertension Key points Prompt initiation of drug treatment is recommended in individuals with grade 2-3 hypertension at any level of CV risk Initiation of antihypertensive drug treatment should also be considered in grade 1 hypertensive patients at low-to-moderate risk Main benefit of antihypertensive medication is from BP lowering per se Diuretic, beta-blockers, calcium antagonists, ACE inhibitors, and ARBs are all suitable for the initiation and maintenance of antihypertensive treatment A goal BP of < 140/90 mmhg is recommended for most hypertensive patients.

10 What the guidelines tell us J Hypertens 2013;31: Renata Cífková
11 Case 1 Body weight 56.4 kg, height 156 cm, BMI 23.2 kg/m 2 ; Office BP (mercury sphygmomanometer; Baumanometer; W.A. Baum Co. Inc., New York, NY, USA): 184/102 mmhg 184/102 mmhg 164/94 mmhg 164/94 mmhg 156/96 mmhg 156/96 mmhg 174/94 mmhg 174/94 mmhg Mean of 4 readings: 170/97 mmhg Mean of the last 3 readings: 165/95 mmhg Renata Cífková
12 Case 1 What would you do as the next step? A. Increase her antihypertensive medication B. Ambulatory blood pressure monitoring C. Home blood pressure measurement Renata Cífková


13 What the guidelines tell us J Hypertens 2013;31: Renata Cífková
14 Case 1 24h ABPM Renata Cífková
15 Case 1 24h ambulatory BP monitoring (SpaceLab 90207; Spacelabs Healthcare Company, Issaquah, WA, USA) 24-hour mean: 124/76 mmhg Daytime mean (06:00-22:00): 135/84 mmhg Nighttime mean (22:00-06:00): 107/65 mmhg Renata Cífková
16 Case 1 ABPM 24-hour mean: 124/76 mmhg Daytime mean (06:00-22:00): 135/84 mmhg Nighttime mean (22:00-06:00): 107/65 mmhg Office BP Mean of 4 readings: 170/97 mmhg Renata Cífková
17 Case 1 ABPM 24-hour mean: 124/76 mmhg Daytime mean (06:00-22:00): 135/84 mmhg Nighttime mean (22:00-06:00): 107/65 mmhg Office BP Mean of 4 readings: 170/97 mmhg Renata Cífková
18 Case 1 How would you conclude this case? Renata Cífková
19 Case 1 ABPM 24-hour mean: 124/76 mmhg Daytime mean (06:00-22:00): 135/84 mmhg Nighttime mean (22:00-06:00): 107/65 mmhg Office BP Mean of 4 readings: 170/97 mmhg Conclusions Hypertension White-coat effect Renata Cífková
20 White-coat effect Clinic BP measurement elicits an alertic reaction that may elevate BP, sometimes to a marked degree Renata Cífková
21 BP measurement Office BP simplest most large clinical trials are based on office BP - very variable - very inaccurate Home BP improves patient adherence to medication has some prognostic value - not accepted by some patients; some patients are upset - patients report only BP values they like to be reported - some patients perform self-adjustment of medication 24-hour ambulatory BP monitoring provides the largest number of BP measurements circadian BP profile - bothersome and stressful examination for some patients Renata Cífková
22 Automated office BP measurement The patient is seated in a quiet room BpTRU: oscillometric device six BP readings taken automatically, without the presence of health care personnel reading 1 is automatically deleted; readings 2-6 are shown on display, and the mean of the last 5 readings is calculated Renata Cífková



23 Renata Cífková
24 Automated office BP measurement in 284 patients during their first visit BP measurement BP (mmhg) Mean of readings 2-6 vs all subsequent measurements BMJ 2011; 342:d Renata Cífková
25 Automated office vs. office BP BP auto (mmhg) BP office (mmhg) Andreadis EA 140/88 163/96 Myers MG 136/78 150/81 Correlation of automated office BP in 3 consecutive visits: SBP 0.896, DBP Myers MG et al., BP Monitoring 2009;14:
, mean")

26 Office BP and automated office BP vs daytime ABPM Untreated hypertensives (n = 94), mean age 55 years Office BP Automated office BP Andreadis EA et al., Am J Hypertens 2011;24:661-6

27 Comparison of automated office BP and awake ABPM Can Fam Physician 2014;60:127-32
28 Hypertension 2015;66:489-95
29 Advantages of automated office BP measurement Simple Standardized Operator-independent More BP readings obtained than with office BP measurement White-coat effect amelioration/elimination Less discomfort than with 24h ABPM Renata Cífková
30 Case 1 Body weight 56.4 kg, height 156 cm, BMI 23.2 kg/m 2 ; Office BP (mercury sphygmomanometer; Baumanometer; W.A. Baum Co. Inc., New York, NY, USA): 184/102 mmhg 184/102 mmhg 164/94 mmhg 164/94 mmhg 156/96 mmhg 156/96 mmhg 174/94 mmhg 174/94 mmhg Mean of 4 readings: 170/97 mmhg Mean of the last 3 readings: 165/95 mmhg Automated office BP measurement (BpTRU Medical Devices Inc., Coquitlam, BC, Canada): 162/82 mmhg; HR 91 bpm 165/80 mmhg; HR 96 bpm 165/88 mmhg; HR 96 bpm 160/83 mmhg; HR 95 bpm 148/82 mmhg; HR 95 bpm Mean BP: 160/83 mmhg; mean HR 94 bpm Renata Cífková
31 Questions to be answered Standardization of BP measurement technique - To initiate automated BP measurement right away/immediately or after 5 minutes rest - With health care personnel present or unattended Correlation with other BP measurements (office, ABPM, home BP) in various patient subpopulations (patients with diabetes, CKD, elderly) Association with organ damage - Arterial stiffness (pulse wave velocity) - Urinary albumin excretion Renata Cífková
32 Manual Office vs Automated Office BP N = 354 Automated Office BP Office automated Correlation P Office BP office BP coefficient SBP 131.2± ± ± <0,.001 DBP 77.8± ± ± < Filipovský J et al., Blood Press 2016;25:228-34

33
34 Home vs Automated Office BP Measurement N = 114 Automated Home BP Home automated Correlation P office BP office BP coefficient SBP 127.± ± ± < DBP 75.2± ± ± < Filipovský J et al., Blood Press 2016;25:228-34
35 Case 2 LB, a 57-year-old lady referred to our center because of hypertension. Personal history: 2006 Hodgkin disease was diagnosed; treated with chemotherapy and subsequent radiation therapy resulting in disease remission. No antihypertensive medication Body weight 65.4 kg, height 172 cm, BMI 22.1 kg/m 2 ; Renata Cífková
36 Case 2 Office BP (mercury sphygmomanometer; Baumanometer; W.A. Baum Co. Inc., New York, NY, USA): 134/90 mmhg 134/86 mmhg 134/90 mmhg Mean of 3 readings: 134/88.7 mmhg Automated office BP measurement (BpTRU Medical Devices Inc., Coquitlam, BC, Canada): 125/78 mmhg; HR 92 bpm 120/81 mmhg; HR 93 bpm 121/79 mmhg; HR 91 bpm 113/79 mmhg; HR 93 bpm 118/71 mmhg; HR 96 bpm Mean BP: 119/78 mmhg; mean HR 93 bpm Difference between office and automated office BP: 15/10 mmhg Renata Cífková
37 Case 2 Office BP (mercury sphygmomanometer; Baumanometer; W.A. Baum Co. Inc., New York, NY, USA): 134/90 mmhg 134/86 mmhg 134/90 mmhg Mean of 3 readings: 134/88.7 mmhg Automated office BP measurement (BpTRU Medical Devices Inc., Coquitlam, BC, Canada): 125/78 mmhg; HR 92 bpm 120/81 mmhg; HR 93 bpm 121/79 mmhg; HR 91 bpm 113/79 mmhg; HR 93 bpm 118/71 mmhg; HR 96 bpm Mean BP: 119/78 mmhg; mean HR 93 bpm Difference between office and automated office BP: 15/10 mmhg Conclusions: High-normal BP White-coat effect Renata Cífková
38 Summary There is a huge difference between office BP and automated office BP Automated office BP correlates with mean daytime BP values obtained during 24h ABPM Automated office BP correlates with LV mass and intima-media thickness Renata Cífková
39 Current therapy of hypertension Has SPRINT changed our approach? Em prof R Fagard
40 Presenter disclosure information R. Fagard No conflict of interest Speaker
41 Case - Medical history 58-year-old man, referred by general practitioner to hypertension clinic for uncontrolled hypertension Medical history. father hypertension, myocardial infarction at age 52 hypertension, known for about 9 years (BP at diagnosis about 180/? mmhg) dyslipidaemia no cardiovascular events no particular complaints/symptoms Speaker
42 Case - Lifestyle and Drug treatment Lifestyle diet: salt restriction, low fat ex-smoker (about 9 years) physical activity: sedentary alcohol consumption: 1 glass of beer/day Drug treatment chlorthalidone 25 mg/day amlodipine 10 mg/day ramipril 10 mg/day simvastatin 40 mg/day Speaker
43 Case - Physical examination Physical examination heart: nl auscultation; no signs of heart failure carotid and peripheral arteries: nl no abdominal bruit conventional blood pressure by physician (mmhg) - sitting: 146/92; 148/94; 144/90 - standing: 138/94 height: 1.73 m; weight: 74 kg; BMI: 24.7 kg/m 2 waist circumference: 98 cm Speaker
44 Case - Laboratory & Technical examinations Blood Na: 142 mmol/l; K: 3.8 mmol/l fasting glucose: 86 mg/dl (4.78 mmol/l) creatinine: 1.13 mg/dl (100 umol/l) - egfr: 65 ml/min/1.73m 2 cholesterol: - total: 246 mg/dl (6.36 mmol/l) - HDL: 34 mg/dl (0.88 mmol/l) - LDL: 187 mg/dl (4.84 mmol/l) triglycerides: 125 mg/dl (1.41 mmol/l) Urine: nl ECG: Sokolow-Lyon index: 3.9 mv; no strain Echocardiogram: LV mass index: 146 g/m 2 ; nl LVEF Abdominal ultrasound: nl renal arteries Speaker
45 Question (1) Would this man have been a candidate for the SPRINT trial*? A. Don t know B. Yes C. No * NEJM 2015; 373: Speaker
46 The SPRINT trial A randomized trial of intensive versus standard blood pressure control. The SPRINT Research Group. NEJM 2015; 373: *Systolic Blood Pressure Intervention Trial Speaker
47 The SPRINT trial Study population: Inclusion & Exclusion criteria Inclusion criteria: age 50 yrs (mean age: 67.9 yrs) SBP: mmhg (mean SBP at baseline: mmhg)* increased risk of CV events, defined by one or more of the following: - clinical or subclinical CV disease other than stroke - chronic kidney disease - 10-yr risk of CV disease 15% (Framingham risk score) - age 75 yrs Exclusion criteria: diabetes, prior stroke, heart failure within past 6 months or LVEF < 35%, dementia, expected survival of < 3 yrs, unintentional weight loss of > 10% within past 6 months, SBP < 110 mmhg after 1 min standing, residing in nursing home 9,361 hypertension patients randomized *90.6 % of patients on antihypertensive treatment; true untreated baseline BP unknown Speaker
48 10-yr cardiovascular risk according to the Framingham risk score Variables in the equation man age: 58 yrs cholesterol - total: 246 mg/dl - HDL: 34 mg/dl systolic BP: 146 mmhg on treatment for high BP: yes Result: 21% Speaker
49
50 Question (2) Further management of hypertension: A. I am satisfied with the current BP control B. I would intensify treatment to a target conventional systolic BP of < 140 mmhg C. I would intensify treatment to a target conventional systolic BP of < 130 mmhg D. I would intensify treatment to a target conventional systolic BP of < 120 mmhg E. I would intensify treatment to a target conventional systolic BP of < 110 mmhg Speaker
51 Target systolic blood pressure 2013 ESH/ESC Hypertension Guidelines One of the important features of the 2013 ESH/ESC Guidelines for the management of arterial hypertension was the recommendation to lower conventional systolic blood pressure to < 140 mmhg in nearly all hypertensive patients with few exceptions. Should this recommendation be revisited after SPRINT? Speaker
52 The SPRINT trial Protocol Randomized controlled trial, open-label design Systolic blood pressure target: standard treatment group < 140 mmhg ( mmhg) intensive treatment group < 120 mmhg Baseline antihypertensive regimens adjusted according to study-group assignment, similar to those used in the ACCORD trial Lifestyle modification encouraged in all participants: reduction of sodium intake alcohol consumption below maximum recommended levels a heart-healthy diet (e.g. the DASH diet) weight loss for overweight participants regular aerobic exercise smoking cessation (Clin Trials 2014; 11: ) Speaker
53
54 The SPRINT trial Results Blood pressure throughout the 3.26 yrs of follow-up: - standard treatment group: mmhg - intensive treatment group: mmhg Primary outcome (composite of MI, ACS, stroke, HF, CV death): HR 0.75 (95% CI: ) P<0.001 Secondary outcomes: - death from any cause HR 0.73 ( ) P= cardiovascular death HR 0.57 ( ) P= heart failure HR 0.62 ( ) P= not significant for MI, ACS or stroke
55 The SPRINT trial Serious adverse events (SAEs) SAEs that were classified as possibly or definitely related to the intervention occurred in 4.7% in the intensive treatment group and in 2.5% in the standard treatment group (P<0.001). SAEs of hypotension, syncope, electrolyte abnormalities and acute kidney injury or acute renal failure occurred more frequently in the intensive treatment group (P<0.05 for each of them), but not injurious falls. Speaker
56 The SPRINT trial Blood pressure measurement Description in main publication: BP measured at office visits 3 measurements at each visit, mean of 3 used in analyses seated position after 5 minutes of quiet rest use of validated automatic measurement system (Model 907, Omron Healthcare)
57 The SPRINT trial Blood pressure measurement Additional information: the Manual of Operations and central training called for the study personnel to leave the room and the device was set to 5 minutes before starting the measurement. Implications thereof are that BPs taken in SPRINT cannot be directly compared with BPs in other trials and that the treatment arm goal of < 120 mmhg in SPRINT compares with a higher SBP value in the other trials.
58 Implications for guidelines Based on: the implications of the unobserved automated BP measurement in SPRINT, an achieved SBP of mmhg (not consistently < 120 mmhg in the majority of participants) in the intensive treatment group, and the conclusions from ACCORD that in patients with type 2 diabetes at high risk for CV events, targeting a (conventional) SBP of < 120 mmhg, as compared with < 140 mmhg, did not reduce the rate of a composite outcome of fatal and nonfatal major CV events (NEJM 2010; 362: ), there appears to be no compelling reason for guidelines to lower conventional target SBP to < 120 mmhg in usual clinical practice, at least not in patients at high CV risk or with diabetes. Should target SBP be lowered to < 130 mmhg?
59 How far to lower blood pressure? A meta-analysis Effects of blood pressure lowering on outcome incidence in hypertension: 7.Effects of more vs less intensive blood pressure lowering and different achieved blood pressure levels updated overview and meta-analyses of randomized trials. Thomopoulos C, Parati G, Zanchetti A. J Hypertension 2016; 34:
60 Selection of studies RCTs comparing more with less intense BP lowering, or active antihypertensive treatment vs placebo, enrolling hypertensive patients or cohorts with 40% hypertensive patients aged 18 yrs. Exclusion of trials investigating patients with acute MI, HF, acute stroke, renal dialysis or secondary hypertension. Between group difference of 2 mmhg in SBP or DBP. Follow-up of 6 months. Reporting one type of CV event or all-cause death, with minimum of 5 events during follow-up.
61 Results Effects of BP lowering in trials of active treatment vs placebo and more vs less intense treatment considered together, stratified in 3 strata with mean SBP achieved by active or more intense treatment vs mean SBP achieved in the placebo or less intense treatment: vs 150 mmhg vs 140 mmhg (143.3 vs mmhg) (137.2 vs mmhg) < 130 mmhg vs 130 mmhg (125.8 vs mmhg) Standardized risk ratios to a SBP difference of -10 mmhg.
62 Results
63 Discussion (1) The updated meta-analysis of RCTs shows that all major outcomes can be reduced by lowering SBP a few mmhg below vs above 130 mmhg. For the same BP reduction, however, the absolute risk reduction is smaller at lower BP targets. This smaller benefit should be considered when deciding the BP target to achieve in the individual patient, especially in front of a possible increase of adverse effects and a consequent decrease in the patient s adherence to the treatment.
64 Discussion (2) Meta-analyses are not a real substitute of large and good RCTs. Meta-analyses comprise trials with heterogeneous cohorts and thus identifying those individuals who would benefit most from intensive treatment to lower BP targets is difficult. The only three large RCTs (SPRINT, ACCORD, SPS3) that specifically aimed at investigating the possible benefits of lowering SBP quite below 130 mmhg have given some contrasting results and had important limitations.
65 Hope-3 study Blood pressure lowering in intermediate-risk persons without cardiovascular disease. Lonn et al, for the HOPE-3 Investigators. NEJM 2016; 374: *Heart Outcomes Prevention Evaluation
66 Hope-3 study To evaluate the role of BP lowering therapy in persons at intermediate risk defined as an annual risk of major CV events of about 1%, without CV disease or renal dysfunction, and with SBP < 160 mmhg without symptomatic hypotension. Double-blind, randomized placebo-controlled trial of a fixed-dose combination of candesartan (16 mg) and HCT (12.5 mg) vs placebo. Inclusion of men aged 55 yrs and women aged 65 yrs with 1 CV risk factor, and women aged 60 yrs with 2 CV risk factors. Participants were not selected on the basis of history of hypertension. 12,705 participants; mean age 65.7 yrs; 38% with history of hypertension.
67 Hope 3 study Results SBP (mmhg) at baseline and change during 5.6 yrs of follow-up: placebo group : 137.9, - 4.0, (133.9) active treatment group: 138.2, , (128.2) First primary outcome (composite of CV death, MI, stroke): HR 0.93 (95% CI: ) P= 0.40 Second primary outcome (first primary outcome + resuscitated cardiac arrest, HF, revascularization): HR 0.95 (95% CI: ) P= 0.51 No significant difference in stroke, heart failure, mortality from CV causes of from any cause.
68 Conclusions Should target systolic BP pressure be revisited? Based on: the issue of unattended automated BP measurements, the heterogeneity of trials included in meta-analyses, meta-analyses not being substitute for large RCTs, the contrasting results and limitations of RCTs with regard to the possible benefits of lowering SBP to < 130 mmhg, the possible increase of adverse events at lower target SBP, there appears to be no compelling indication for a change in the current recommendation to reduce the conventional target SBP of < 140 mmhg to a lower level in usual clinical practice in the large majority of hypertensive patients. It is up to Guidelines Committees to carefully consider levels of evidence and classes of recommendation based on current and future evidence.
69 Question (3) How to intensify antihypertensive treatment?* A. Increase the dose of amlodipine? B. Increase the dose of ramipril? C. Add spironolactone? D. Add a beta-blocker? E. Apply renal denervation? (*apart from improving lipid control and starting aspirin) Speaker
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
The earlier BP control the better cardiovascular outcome. Jin Oh Na Cardiovascular center Korea University Medical College
 The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
Summary of recommendations
 Summary of recommendations Measuring blood pressure (BP) Use the recommended technique at every BP reading to ensure accurate measurements and avoid common errs. Pay particular attention to the following:
Summary of recommendations Measuring blood pressure (BP) Use the recommended technique at every BP reading to ensure accurate measurements and avoid common errs. Pay particular attention to the following:
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3)
") Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3) Χάρης Γράσσος MD,FESC,PhD,EHS Διευθυντής Καρδιολόγος Γ.Ν.Α ΚΑΤ Visiting Professor University of Bolton U.K New England
Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3) Χάρης Γράσσος MD,FESC,PhD,EHS Διευθυντής Καρδιολόγος Γ.Ν.Α ΚΑΤ Visiting Professor University of Bolton U.K New England
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
New Antihypertensive Strategies to Improve Blood Pressure Control
 New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Talking about blood pressure
 Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Blood Pressure Measurement in SPRINT
 Blood Pressure Measurement in SPRINT Karen C. Johnson, MD, MPH, FAHA Vice Chair, SPRINT Steering Committee University of Tennessee Health Science Center, Department of Preventive Medicine For the SPRINT
Blood Pressure Measurement in SPRINT Karen C. Johnson, MD, MPH, FAHA Vice Chair, SPRINT Steering Committee University of Tennessee Health Science Center, Department of Preventive Medicine For the SPRINT
Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China
 What Can We Learn from the Observational Studies and Clinical Trials of Prehypertension? Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China At ARIC visit 4
What Can We Learn from the Observational Studies and Clinical Trials of Prehypertension? Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China At ARIC visit 4
Clinical cases with Coversyl 10 mg
 Clinical cases Coversyl 10 mg For upgraded benefits in hypertension A Editorial This brochure, Clinical cases Coversyl 10 mg for upgraded benefits in hypertension, illustrates a variety of hypertensive
Clinical cases Coversyl 10 mg For upgraded benefits in hypertension A Editorial This brochure, Clinical cases Coversyl 10 mg for upgraded benefits in hypertension, illustrates a variety of hypertensive
Hypertension Clinical case scenarios for primary care
 Hypertension Clinical case scenarios for primary care Implementing NICE guidance August 2011 NICE clinical guideline 127 What this presentation covers Five clinical case scenarios, including: presentation
Hypertension Clinical case scenarios for primary care Implementing NICE guidance August 2011 NICE clinical guideline 127 What this presentation covers Five clinical case scenarios, including: presentation
Slide notes: References:
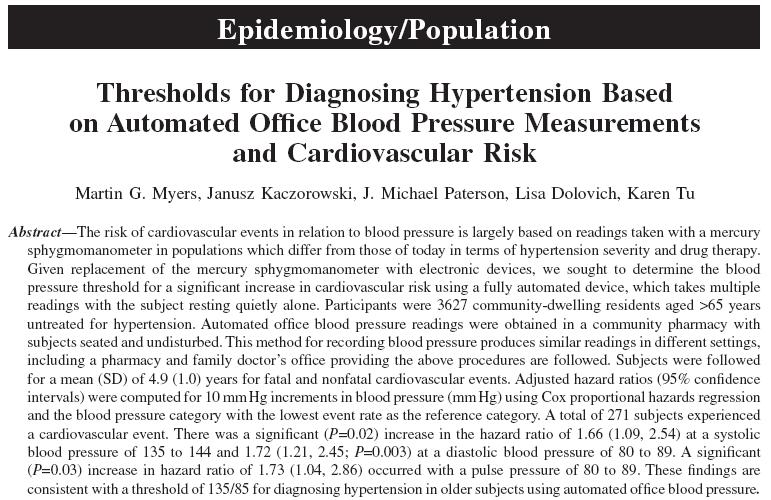
 1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Importance of Ambulatory Blood Pressure Monitoring in Adolescents
 Importance of Ambulatory Blood Pressure Monitoring in Adolescents Josep Redon, MD, PhD, FAHA Internal Medicine Hospital Clinico Universitario de Valencia University of Valencia CIBERObn Instituto de Salud
Importance of Ambulatory Blood Pressure Monitoring in Adolescents Josep Redon, MD, PhD, FAHA Internal Medicine Hospital Clinico Universitario de Valencia University of Valencia CIBERObn Instituto de Salud
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension.
 / International Society of Hypertension (ISH) Statement on Management of Hypertension.") 2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu Indicator area: Pulse rhythm assessment for AF Indicator: NM146 Date: June 2017 Introduction There is evidence
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu Indicator area: Pulse rhythm assessment for AF Indicator: NM146 Date: June 2017 Introduction There is evidence
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA
 Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Hypertension Update. Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016
 Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Evaluation and Management of Hypertension in Women. Vesna D. Garovic, M.D. Moscow, Russia, December 2016
 Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
How Low Do We Go? Update on Hypertension
 How Low Do We Go? Update on Beth L. Abramson, MD, FRCPC, FACC As presented at the University of Toronto s Saturday at the University Session (September 2003) Arecent World Health Organization report states
How Low Do We Go? Update on Beth L. Abramson, MD, FRCPC, FACC As presented at the University of Toronto s Saturday at the University Session (September 2003) Arecent World Health Organization report states
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
High-dose monotherapy vs low-dose combination therapy of calcium channel blockers and angiotensin receptor blockers in mild to moderate hypertension
 (2005) 19, 491 496 & 2005 Nature Publishing Group All rights reserved 0950-9240/05 $30.00 www.nature.com/jhh ORIGINAL ARTICLE High-dose monotherapy vs low-dose combination therapy of calcium channel blockers
(2005) 19, 491 496 & 2005 Nature Publishing Group All rights reserved 0950-9240/05 $30.00 www.nature.com/jhh ORIGINAL ARTICLE High-dose monotherapy vs low-dose combination therapy of calcium channel blockers
SUPPLEMENTARY DATA. Supplementary Table 1. Baseline Patient Characteristics
 Supplementary Table 1. Baseline Patient Characteristics Normally distributed data are presented as mean (±SD), data that were not of a normal distribution are presented as median (ICR). The baseline characteristics
Supplementary Table 1. Baseline Patient Characteristics Normally distributed data are presented as mean (±SD), data that were not of a normal distribution are presented as median (ICR). The baseline characteristics
Metabolic Syndrome. Shon Meek MD, PhD Mayo Clinic Florida Endocrinology
 Metabolic Syndrome Shon Meek MD, PhD Mayo Clinic Florida Endocrinology Disclosure No conflict of interest No financial disclosure Does This Patient Have Metabolic Syndrome? 1. Yes 2. No Does This Patient
Metabolic Syndrome Shon Meek MD, PhD Mayo Clinic Florida Endocrinology Disclosure No conflict of interest No financial disclosure Does This Patient Have Metabolic Syndrome? 1. Yes 2. No Does This Patient
CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES
 CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES C. Liakos, 1 G. Vyssoulis, 1 E. Karpanou, 2 S-M. Kyvelou, 1 V. Tzamou, 1 A. Michaelides, 1 A. Triantafyllou, 1 P. Spanos, 1 C. Stefanadis
CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES C. Liakos, 1 G. Vyssoulis, 1 E. Karpanou, 2 S-M. Kyvelou, 1 V. Tzamou, 1 A. Michaelides, 1 A. Triantafyllou, 1 P. Spanos, 1 C. Stefanadis
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
New Hypertension Guidelines. Kofi Osei, MD
 New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
What s New? Hypertension Canada Guidelines for the Management of Hypertension
 What s New? 2017 Hypertension Canada Guidelines for the Management of Hypertension What s New? About This Booklet This booklet highlights key advancements and important, enduring aspects of the Hypertension
What s New? 2017 Hypertension Canada Guidelines for the Management of Hypertension What s New? About This Booklet This booklet highlights key advancements and important, enduring aspects of the Hypertension
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Module 3.2. Management of hypertension at primary health care
 Module 3.2 Management of hypertension at primary health care What s inside Introduction Learning outcomes Topics covered Competency Teaching and learning activities Background information Introduction
Module 3.2 Management of hypertension at primary health care What s inside Introduction Learning outcomes Topics covered Competency Teaching and learning activities Background information Introduction
Blood Pressure LIMBO How Low To Go?
 Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Primary and Secondary Prevention of Cardiovascular Disease. Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group
 Primary and Secondary Prevention of Cardiovascular Disease Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group AHA Diet and Lifestyle Recommendations Balance calorie intake and physical activity to
Primary and Secondary Prevention of Cardiovascular Disease Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group AHA Diet and Lifestyle Recommendations Balance calorie intake and physical activity to
Hypertension and the SPRINT Trial: Is Lower Better
 Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Hypertension: 2016 Clinical Update
 PHASE Safety Net Community Benefit Hypertension: 2016 Clinical Update Presented by: Joseph Young, MD Hypertension Clinical Lead Kaiser Permanente Northern California October 6, 2016 Dr. Joseph Young Hypertension
PHASE Safety Net Community Benefit Hypertension: 2016 Clinical Update Presented by: Joseph Young, MD Hypertension Clinical Lead Kaiser Permanente Northern California October 6, 2016 Dr. Joseph Young Hypertension
MPharmProgramme. Hypertension (HTN)
") MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial
 1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
Management of Hypertension in Women
 Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Management in Diabetic Patients
 Hypertension Management in Diabetic Patients Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School Contents (Treatment of 2 Cases) Type 2 Diabetes Mellitus Hypertension
Hypertension Management in Diabetic Patients Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School Contents (Treatment of 2 Cases) Type 2 Diabetes Mellitus Hypertension
The State of Hypertension in NZ in 2010 personal view
 The State of Hypertension in NZ in 2010 personal view Patient referred to medical clinic Dear Dr, Please see this man with resistant hypertension 50 year old European male Blood Pressure on current meds
The State of Hypertension in NZ in 2010 personal view Patient referred to medical clinic Dear Dr, Please see this man with resistant hypertension 50 year old European male Blood Pressure on current meds
Hypertension Update. Faculty/Presenter Disclosure
 Hypertension Update Who Gives a CHEP About Targets? Faculty/Presenter Disclosure Presenter: Raj Padwal Relationships that may introduce potential bias and/or conflict of interest: Grants/Research Support:
Hypertension Update Who Gives a CHEP About Targets? Faculty/Presenter Disclosure Presenter: Raj Padwal Relationships that may introduce potential bias and/or conflict of interest: Grants/Research Support:
Managing Hypertension in 2018
 MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
What s the evidence, why do guidelines differ, and what should the GP do?
 What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
 Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical
Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical
Challenges in Hypertension: Incorporating Evolving Clinical Data Into Practice
 Challenges in Hypertension: Incorporating Evolving Clinical Data Into Practice Faculty Jan Basile, MD Professor of Medicine Seinsheimer Cardiovascular Health Program Division of General Internal Medicine
Challenges in Hypertension: Incorporating Evolving Clinical Data Into Practice Faculty Jan Basile, MD Professor of Medicine Seinsheimer Cardiovascular Health Program Division of General Internal Medicine
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
PREVER STUDY. What we learned with the PREVER-PREVENTION Trial? Dr. Sandra C. Fuchs. Professor at Universidade Federal of Rio Grande do Sul, Brazil
 11 PREVER STUDY What we learned with the PREVER-PREVENTION Trial? Dr. Sandra C. Fuchs Professor at Universidade Federal of Rio Grande do Sul, Brazil Financial Support: PREVER investigators: Sandra C. FUCHS,
11 PREVER STUDY What we learned with the PREVER-PREVENTION Trial? Dr. Sandra C. Fuchs Professor at Universidade Federal of Rio Grande do Sul, Brazil Financial Support: PREVER investigators: Sandra C. FUCHS,
Effects of Bariatric Surgery in Obese Patients with Hypertension The GATEWAY Randomized Trial
 Effects of Bariatric Surgery in Obese Patients with Hypertension The GATEWAY Randomized Trial Carlos Aurelio Schiavon, MD, FACS On behalf of the GATEWAY Executive Committee and Investigators DISCLOSURE
Effects of Bariatric Surgery in Obese Patients with Hypertension The GATEWAY Randomized Trial Carlos Aurelio Schiavon, MD, FACS On behalf of the GATEWAY Executive Committee and Investigators DISCLOSURE
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Adult Blood Pressure Clinician Guide June 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Colin Edwards. Cardiologist Auckland Heart Group Waitemata Health
 Colin Edwards Cardiologist Auckland Heart Group Waitemata Health August 2011 BP MEASUREMENTS measured seated mean of 2 or BP recordings at least 2 visits 2 x risk of developing true hypertension Size of
Colin Edwards Cardiologist Auckland Heart Group Waitemata Health August 2011 BP MEASUREMENTS measured seated mean of 2 or BP recordings at least 2 visits 2 x risk of developing true hypertension Size of
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127
 Hypertension in adults: diagnosis and management Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Hypertension in adults: diagnosis and management Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Hypertension in the Elderly. John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care
 Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE
 2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE Massimo F Piepoli, MD, PhD, FESC, Piacenza, Italy on behalf of the 6 th Joint Task Force 2 3 Guidelines still based upon the principles of
2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE Massimo F Piepoli, MD, PhD, FESC, Piacenza, Italy on behalf of the 6 th Joint Task Force 2 3 Guidelines still based upon the principles of
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Effects of Bariatric Surgery in Obese Patients with Hypertension The GATEWAY Randomized Trial
 Effects of Bariatric Surgery in Obese Patients with Hypertension The GATEWAY Randomized Trial Carlos Aurelio Schiavon, MD, FACS On behalf of the GATEWAY Executive Committee and Investigators DISCLOSURE
Effects of Bariatric Surgery in Obese Patients with Hypertension The GATEWAY Randomized Trial Carlos Aurelio Schiavon, MD, FACS On behalf of the GATEWAY Executive Committee and Investigators DISCLOSURE