Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
|
|
|
- Alvin Long
- 5 years ago
- Views:
Transcription
1 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017
2 Agenda Indications Different insulin preparations Insulin initiation Insulin intensification
3 Indications for insulin therapy Type 1 diabetes Women with diabetes who become pregnant or are breastfeeding Transiently in type 2 diabetes in special situations In type 2 diabetes, inadequately controlled on glucoselowering medicines (secondary failure)
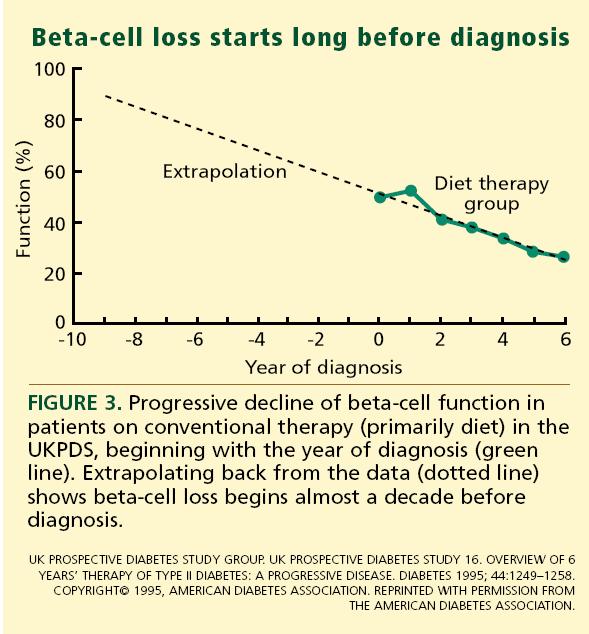
4 Progressive beta cell damage Type 2 diabetes is a progressive disease At the time of diagnosis, patients with type 2 diabetes have an estimated loss of about 50% of their insulin-producing
5
6
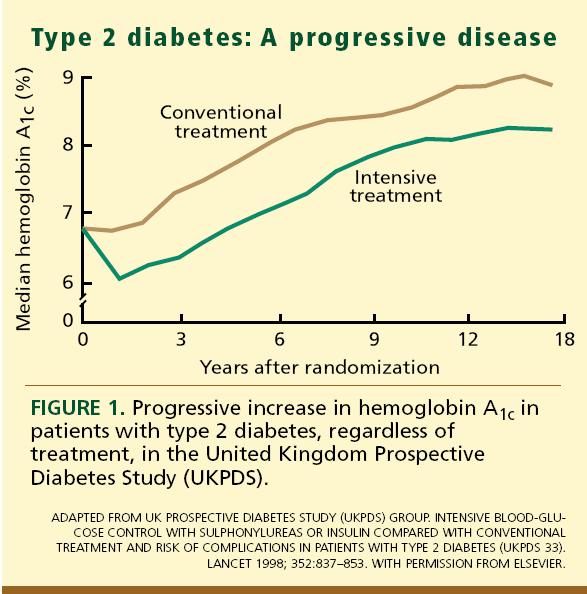
7 Need for Insulin Insulin therapy is thus frequently required during the course of the disease to maintain glycemic control and prevent diabetes complications. In the UK Prospective Diabetes Study, 9 years after diagnosis almost 80%of patients on oral agents required insulin supplementation
8 Insulin Insulin A hormone secreted by the beta cells Secreted in response to glucose or other stimuli, such as amino acids Normal response characterized by low basal levels of insulin, with surges of insulin triggered by a rise in blood glucose Breakfast Lunch Supper
9 Insulin action 1. Increases glucose uptake, particularly in muscle, liver and adipose tissue 2. Suppresses glucose output from the liver 3. Increases formation of fat 4. Inhibits breakdown of fats 5. Promotes amino-acid uptake and prevents protein breakdown
10 Insulin remains the most potent antihyperglycemic agent available for uncontrolled T2DM patients Intervention Expected in HbA 1c Insulin No upper limit Metformin 1.5% Sulfonylureas 1.5% Glinides 1 to 1.5% a TZDs 0.5 to 1.4% -Glucosidase inhibitors 0.5 to 0.8% GLP-1 agonist 0.5 to 1.0% Pramlintide 0.5 to 1.0% DPP-IV inhibitors ~0.8% a Repaglinide is more effective than nateglinide Adapted from Nathan DM et al. Diabetes Care 2006;29(8):

11
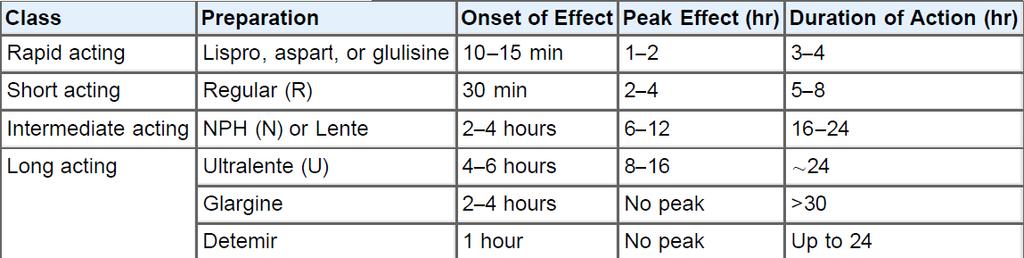
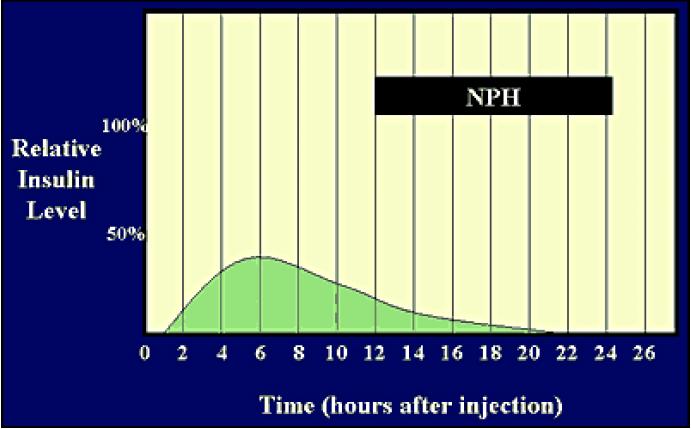
12 Summary of available insulin preparations Glucose lowering Agent Type / Administration Basal Post-meal NPH Intermediate-acting human Once or twice daily at bedtime ± breakfast Detemir Long-acting analogue Once or twice daily at bedtime ± breakfast Glargine Long-acting analogue Once daily at bedtime or before breakfast Premixed Human or analogue mix Twice daily before breakfast and dinner Regular Fast-acting human Before meals Aspart, glulisine, lispro Rapid-acting analogue Before meals
13 MIMICKING NATURE WITH INSULIN THERAPY The Basal/Bolus Insulin Concept Basal Insulin Suppresses glucose production between meals and overnight Nearly constant levels 50% of daily needs Bolus Insulin (Mealtime or Prandial) Limits hyperglycemia after meals Immediate rise and sharp peak at 1 hour 10% to 20% of total daily insulin requirement at each meal 6-20
14 The Ideal Basal Insulin 1 injection daily covers 24 hours No peaks Low incidence of hypoglycemia Good glycemic control Less weight gain Safe Predictable

15 INSULIN TACTICS: Insulin Glargine A New Long-acting Insulin Analogue Modifications to human insulin chain Substitution of glycine at position A21 Addition of two arginines at position B30 Gradual release pattern from injection site Gly Asp Substitution Asp Extension Arg Arg


16 INSULIN DETEMIR A soluble derivative of human insulin Threonine has been removed at position B30 A 14-carbon fatty acid side-chain has been attached to position B29
17 Glucose Utilization Rate (mg/kg/h) INSULIN TACTICS: Glargine Vs. NPH Insulin in Type 1 DM Action Profiles by Glucose Clamp Glargine insulin NPH insulin End of observation period Time (h) after S.C. Injection
18
19
20 Basal Insulin Long acting (e.g. glargine) Intermediate acting (e.g. NPH) - Provides optimal basal insulin coverage with a once daily dosing - Lower risk of hypoglycemia - Less optimal as a basal insulin, because it doesn t have a flat insulin release profile - More hypoglycemic episodes - Flat release profile
21 NPH vs Glargine Three large RCT have compared once- daily, bedtime NPH or Glargine added to oral agents in pts with type 2 DM Less nocturnal hypoglycemia Less weight gain HbA1c,No difference Diabetes care, 2001, 24: Diabetes care, 2000, 23: Diabetes care, 2003,26(11):
22 Activity Profile of Insulin Lispro 60 Insulin (mu/l) Normal insulin response Regular human insulin (injection 5 minutes before meals) Insulin Lispro (injection 5 minutes before meals)* * Aspart has similar profile Meal Minutes Based on a study of 6 patients with type 1 diabetes and some residual b-cell function and 6 control subjects without diabetes Adapted from Pampanelli S et al. Diabetes Care 1995;18:
23
24

25
26 ADA Standards of Medical Care in Diabetes-2017 Updates to standards of medical care in diabetes 2016 Diabetes Care 2017;40(Suppl. 1):S1 S138
27 Treatment: stepwise approach???
28 Start with monotherapy unless: A1c is greater than or equal to 9%, consider dual therapy A1c is greater than or equal to 10 %, blood glucose is greater than or equal to 300 mg/dl or patient is markedly symptomatic, consider combination injectable therapy Monotherapy Metformin Lifestyle Management EFFICACY* HYPO RISK WEIGHT SIDE EFFECTS COSTS* high low risk neutral/loss GI/lactic acidosis low If A1c is not achieved approximately after 3 months of monotherapy, proceed to 2-drug combination (order not meant to denote any specific preference- choice dependent on variety of patient- & disease-specific factors) Dual Therapy Metformin + Lifestyle Management Sulfonylurea Thiazolidinedione DPP-4 inhibitor SGLT2 inhibitor GLP-1 receptor agonist Insulin (Basal) EFFICACY* high high intermediate intermediate high highest HYPO RISK moderate risk low risk low risk low risk low risk high risk WEIGHT gain gain neutral loss loss gain SIDE EFFECTS hypoglycemia Edema, HF, fxs rare GU, dehydration, fxs GI hypoglycemia COSTS* low low high high high high If A1c is not achieved approximately after 3 months of dual therapy, proceed to 3-drug combination (order not meant to denote any specific preferencechoice dependent on variety of patient- & disease-specific factors) Diabetes Care 2017;40(Suppl. 1):S1 S138
29 Contd. Dual Therapy Triple Therapy Metformin + Lifestyle Management Sulfonylurea + Thiazolidinedione + DPP-4 inhibitor + SGLT2 inhibitor + GLP-1 receptor agonist + Insulin (Basal) + TZD SU SU SU SU TZD DPP-4-i DPP-4-i TZD TZD TZD or or or or or or DPP-4-i or SGLT2-i or SGLT2-i or SGLT2-i or DPP-4-i or SGLT2-i or SGLT2-i or GLP-1-RA or GLP-1-RA or Insulin $ or GLP-1-RA or Insulin $ or GLP-1-RA or Insulin $ or Insulin $ or Insulin $ If A1c is not achieved approximately after 3 months of triple therapy, and patient (1) on oral combination, move to basal insulin or GLP-1 RA, (2) on GLP-1 RA, add basal insulin or (3) on optimally titrated basal insulin, addaglp-1 RA or meal time insulin. Metformin therapy should be maintained, while other oral agents may be discontinued on an individual basis to avoid unnecessary complex or costly regimens. (i.e. adding fourth antihyperglycemic agent). Combination Injectable Therapy Fig.8.1: Antihyperglycemic therapy in type 2 diabetes: general recommendations. The order in the chart is determined by historical availability and the route of administration, with injectables to the right; it is not meant to denote any specific preference. Potential sequences of antihyperglycemic therapy for patients with type 2 diabetes are displayed, with the usual transition moving vertically from top to bottom (although horizontal movement within therapy stages is also possible, depending on the circumstances). DPP-4-i, DPP-4 inhibitor; fxs, fractures; GI, gastrointestinal; GLP-1 RA, GLP-1 receptor agonist; GU, genitourinary; HF, heart failure; Hypo, hypoglycemia; SGLT2-i, SGLT2 inhibitor; SU, sulfonylurea; TZD, thiazolidinedione. $ Usually a basal insulin (NPH, glargine, detemir, degludec). Adapted with permission from Inzucchi et al 2015 *Inzucchi SE, Bergenstal RM, Buse JB, et al.management of hyperglycemia in type 2 diabetes,2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Studyof Diabetes. Diabetes Care 2015;38: Diabetes Care 2017;40(Suppl. 1):S1 S138
 Symptomatic (e.g.")
30 Insulin Therapy Indications in Type2 DM 1) HbA 1c 10%or BS > 30 0mg/dl 2) Symptomatic (e.g., sudden persistent weight loss, ketosis) 3) When multiple non-insulin therapies fail to achieve targets

31 11/28/
")
32 Consider different proportions in Mixed Insulin (75/25, 50/50) 11/28/
33 Initiation of Basal Insulin Add single insulin dose in the evening (10 U or 0.1 U/kg) NPH Insulin glargine Insulin detemir
34 Adjust dose on the basis of FBG Increase insulin every 3-5 days as needed (provided no hypoglycemia occurs) Increase by 2 U if FBG > 120 mg/dl Increase by 4 U if FBG > 140 mg/dl Increase by 6 U if FBG > 160 mg/dl
35 When to add the first prandial insulin
36 stepwise pattern Patients should be instructed to monitor FBG and 2-hpp. Rapid-acting insulin analogs can be added before the meal(s) associated with the highest post prandial. This prandial insulin should be adjusted to achieve 2-hpp target glucose
37 stepwise pattern For example, a patient may be started on 3-4 U of rapidacting insulin before the biggest meal, and the dose can be adjusted by 1-2 U as needed according to 2-hpp.
38 stepwise pattern Once target levels are achieved at one meal, additional prandial boluses of rapid-acting insulin can be added at other meal times and adjusted in a similar pattern.
39 stepwise pattern Oral insulin secretagogues should be stopped at this point, but insulin sensitizers can be continued. With this stepwise pattern, the patient is gradually transitioned to a basal-bolus regimen similar to that used in type 1 diabetes.
40 Premix insulins Biphasic Human insulin (NPH +Regular ) Insulin analogues (Insulin Aspart 70/30, Lispro 75/25 and 50/50,)
41 Formulation of premixes Premixed suspension of: Soluble insulin aspart 30% 30% Soluble human insulin Protamine-crystallised insulin aspart NPH NovoMix 30 Premixed human insulin 45
42 Premixed regimen This strategy may be appropriate for certain patients who eat regularly and may be in need of a simplified approach beyond basal insulin Disadvantages: inability to titrate the shorter- from the longer-acting component
43 Premix insulin No need for self mixing Minimizing dosing error Less injections (attractive alternative to basal bolus) Fixed ratio (Less flexibility)
44 NovoMix 30: A consensus statement Simple algorithms for intensification Basal insulin OD or BID HbA1c 7-8% HbA1c > 8.0% FPG > 6mmol/L (FPG > 110 mg/dl) Titrate basal to achieve FPG <6 mmol/l (110 mg/dl) FPG: 4-6 mmol/l (FPG > mg/dl) Switch TO BIAsp 30 BID *If recurrent hypoglycaemia limits up-titration of the basal dose, or the daily dose reaches 0.5 U/kg (insulin units per kg body weight), switching to BIAsp 30 twice daily can be considered
45 FBS Change in Dose of Predinner Insulin Predinner Blood Glucose Level <60-4U <60-4U U U Change in Dose of Prebreakfast Insulin NO CHANGE NO CHANGE U U U U >180 +6U >180 +6U

46 Staying on NovoMix 30 Intensification from NovoMix 30 twice daily to three times daily: Add 2-6 units or 10% of total daily dose of NovoMix 30 before lunch
47 Criteria for successful insulin therapy Efficacy: HbA 1c <7.0% Low rates of hypoglycaemia Minimal weight gain Flexibility Treatment satisfaction
48 ow to Switch Between Insulin Products
49 Goal achievement? Attainment of glycemic targets using insulin remains difficult In a recent review of 48 randomized clinical trials using insulin in T2DM patients with a mean baseline HbA1c of 8.7%, only 40 54% achieved an HbA1c of less than7% Diabetes Res Clin Pract2011, 92:1 10

50
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Insulin and Post Prandial
 Insulin and Post Prandial Pr Luc Martinez PCDE Meeting Barcelona 2016 Conflicts of interest disclosure Advis consultant f Amgen Inc.; AstraZeneca Pharmaceuticals LP; GlaxoSmithKline; Ipsen; Lilly; Mayoly
Insulin and Post Prandial Pr Luc Martinez PCDE Meeting Barcelona 2016 Conflicts of interest disclosure Advis consultant f Amgen Inc.; AstraZeneca Pharmaceuticals LP; GlaxoSmithKline; Ipsen; Lilly; Mayoly
Objectives 2/13/2013. Figuring out the dose. Sub Optimal Glycemic Control: Moving to the Appropriate Treatment
 Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol
 Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach
 Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach Update to a Position Statement of the American Diabetes Association (ADA) and the European Association f the Study of Diabetes
Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach Update to a Position Statement of the American Diabetes Association (ADA) and the European Association f the Study of Diabetes
Position Statement of ADA / EASD 2012
 Management of Hyperglycemia in Type2 Diabetes: A Patient- Centered Approach Position Statement of ADA / EASD 2012 Cause of : Type 2 diabetes Cardiovascular disorders Blindness End-stage renal failure Amputations
Management of Hyperglycemia in Type2 Diabetes: A Patient- Centered Approach Position Statement of ADA / EASD 2012 Cause of : Type 2 diabetes Cardiovascular disorders Blindness End-stage renal failure Amputations
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Tips and Tricks for Starting and Adjusting Insulin. MC MacSween The Moncton Hospital
 Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
UKPDS: Over Time, Need for Exogenous Insulin Increases
 UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
INSULIN 101: When, How and What
 INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Individualising Insulin Regimens: Premixed or basal plus/bolus?
 Individualising Insulin Regimens: Premixed or basal plus/bolus? Dr. Ted Wu Director, Diabetes Centre, Hospital Sydney, Australia Turkey, April 2015 Centre of Health Professional Education Optimising insulin
Individualising Insulin Regimens: Premixed or basal plus/bolus? Dr. Ted Wu Director, Diabetes Centre, Hospital Sydney, Australia Turkey, April 2015 Centre of Health Professional Education Optimising insulin
APPENDIX American Diabetes Association. Published online at
 APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes
 Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
INSULIN THERAPY. Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital
 INSULIN THERAPY Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital 3 Sep. 2013 Case Somsak is a 64-year-old man was diagnosed with T2DM, HT, and dyslipidemia 9 years ago. No history of hypoglycemia
INSULIN THERAPY Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital 3 Sep. 2013 Case Somsak is a 64-year-old man was diagnosed with T2DM, HT, and dyslipidemia 9 years ago. No history of hypoglycemia
Type 2 Diabetes Mellitus Insulin Therapy 2012
 Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Update on Insulin-based Agents for T2D. Harry Jiménez MD, FACE
 Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Injecting Insulin into Out Patient Practice
 Injecting Insulin into Out Patient Practice Kathleen Colleran, MD Associate Professor UNMHSC 4/22/10 Overview Natural history of Type 2 diabetes Reasons clinicians are reluctant to start insulin therapy
Injecting Insulin into Out Patient Practice Kathleen Colleran, MD Associate Professor UNMHSC 4/22/10 Overview Natural history of Type 2 diabetes Reasons clinicians are reluctant to start insulin therapy
nocturnal hypoglycemia percentage of Hispanics in the insulin glargine than NPH during forced patients who previously This study excluded
 Clinical Trial Design/ Primary Objective Insulin glargine Treat-to-Target Trial, Riddle et al., 2003 (23) AT.LANTUS trial, Davies et al., 2005 (24) INSIGHT trial, Gerstein et al., 2006 (25) multicenter,
Clinical Trial Design/ Primary Objective Insulin glargine Treat-to-Target Trial, Riddle et al., 2003 (23) AT.LANTUS trial, Davies et al., 2005 (24) INSIGHT trial, Gerstein et al., 2006 (25) multicenter,
Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control
 Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control can prevent many of early type 1 DM(in DCCT trail ). UK
Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control can prevent many of early type 1 DM(in DCCT trail ). UK
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
New basal insulins Are they any better? Matthew C. Riddle, MD Professor of Medicine Oregon Health & Science University Keystone Colorado 15 July 2011
 New basal insulins Are they any better? Matthew C. Riddle, MD Professor of Medicine Oregon Health & Science University Keystone Colorado 15 July 2011 Presenter Disclosure I have received the following
New basal insulins Are they any better? Matthew C. Riddle, MD Professor of Medicine Oregon Health & Science University Keystone Colorado 15 July 2011 Presenter Disclosure I have received the following
Your Chart Review Data. Lara Zisblatt, MA Assistant Director Continuing Medical Education Boston University School of Medicine
 Your Chart Review Data Lara Zisblatt, MA Assistant Director Continuing Medical Education Boston University School of Medicine Participation 243 registered for the program 98 have completed the Practice
Your Chart Review Data Lara Zisblatt, MA Assistant Director Continuing Medical Education Boston University School of Medicine Participation 243 registered for the program 98 have completed the Practice
Insulin Therapy Management. Insulin Therapy
 Insulin Therapy Management Insulin Therapy Contents Insulin and its effect on glycemic control Physiology of insulin secretion Insulin pharmacokinetics and regimens Insulin dose adjustment for pregnancy
Insulin Therapy Management Insulin Therapy Contents Insulin and its effect on glycemic control Physiology of insulin secretion Insulin pharmacokinetics and regimens Insulin dose adjustment for pregnancy
Pathogenesis of Type 2 Diabetes
 9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
Self-Monitoring Blood Glucose (SMBG) Frequency & Pattern Tool
 Frequency & Pattern Tool") Self-Monitoring Blood Glucose () Pattern Recommendation: Basal Insulin Only (To Target) NPH or long-acting analogue, typically given at. at least as often as is being given. Optional, less frequent can
Self-Monitoring Blood Glucose () Pattern Recommendation: Basal Insulin Only (To Target) NPH or long-acting analogue, typically given at. at least as often as is being given. Optional, less frequent can
Diabetes: Definition Pathophysiology Treatment Goals. By Scott Magee, MD, FACE
 Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Diabetes Mellitus in Older Adults. Presenter Disclosure Information
 Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
INSULIN THERAY دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد
 INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
Newer Insulins. Boca Raton Regional Hospital 15th Annual Internal Medicine Conference
 Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Current Clinical Practice Guideline for Diabetes Management
 Current Clinical Practice Guideline for Diabetes Management Chaicharn Deerochanawong M.D. Professor of Medicine, i Rangsit Medical University it Diabetes and Endocrinology Unit Department of Medicine Rajavithi
Current Clinical Practice Guideline for Diabetes Management Chaicharn Deerochanawong M.D. Professor of Medicine, i Rangsit Medical University it Diabetes and Endocrinology Unit Department of Medicine Rajavithi
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Insulin Intensification: A Patient-Centered Approach
 MARTIN J. ABRAHAMSON, MD Harvard Medical School, Boston, MA Insulin Intensification: A Patient-Centered Approach Dr Abrahamson is associate professor of medicine at Harvard Medical School and medical director
MARTIN J. ABRAHAMSON, MD Harvard Medical School, Boston, MA Insulin Intensification: A Patient-Centered Approach Dr Abrahamson is associate professor of medicine at Harvard Medical School and medical director
GLP-1RA and insulin: friends or foes?
 Tresiba Expert Panel Meeting 28/06/2014 GLP-1RA and insulin: friends or foes? Matteo Monami Careggi Teaching Hospital. Florence. Italy Dr Monami has received consultancy and/or speaking fees from: Merck
Tresiba Expert Panel Meeting 28/06/2014 GLP-1RA and insulin: friends or foes? Matteo Monami Careggi Teaching Hospital. Florence. Italy Dr Monami has received consultancy and/or speaking fees from: Merck
DEMYSTIFYING INSULIN THERAPY
 DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
第十五章. Diabetes Mellitus
 Diabetes-1/9 第十五章 Diabetes Mellitus 陳曉蓮醫師 2/9 - Diabetes 羅東博愛醫院 Management of Diabetes mellitus A. DEFINITION OF DIABETES MELLITUS Diabetes Mellitus is characterized by chronic hyperglycemia with disturbances
Diabetes-1/9 第十五章 Diabetes Mellitus 陳曉蓮醫師 2/9 - Diabetes 羅東博愛醫院 Management of Diabetes mellitus A. DEFINITION OF DIABETES MELLITUS Diabetes Mellitus is characterized by chronic hyperglycemia with disturbances
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Silvio E. Inzucchi MD Section of Endocrinology Yale School of Medicine
 Gegia Chapter of the American Association of Clinical Endocrinologists, 2017 Annual Meeting January 28, 2017 Silvio E. Inzucchi MD Section of Endocrinology Yale School of Medicine DIABETES MANAGEMENT GUIDELINES
Gegia Chapter of the American Association of Clinical Endocrinologists, 2017 Annual Meeting January 28, 2017 Silvio E. Inzucchi MD Section of Endocrinology Yale School of Medicine DIABETES MANAGEMENT GUIDELINES
ClinicalTrials.gov Identifier: sanofi-aventis. Sponsor/company:
 These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinicalTrials.gov
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinicalTrials.gov
Role of Insulin Analogs in
 Role of Insulin Analogs in Type 2 Diabetes Supported by an educational grant from Novo Nordisk Inc. This program is supported by an educational grant from Novo Nordisk Inc. It has been accredited by the
Role of Insulin Analogs in Type 2 Diabetes Supported by an educational grant from Novo Nordisk Inc. This program is supported by an educational grant from Novo Nordisk Inc. It has been accredited by the
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Insulin Prior Authorization with optional Quantity Limit Program Summary
 Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Mixed Insulins Pick Me
 Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
The Diabetes Guidelines Trek: The Next Generation. Inpatient Diabetes Guidelines. Learning Objectives. Current Inpatient Guidelines
 The Diabetes Guidelines Trek: The Next Generation J. Christopher Lynch, PharmD, BCACP Southern Illinois University Edwardsville School of Pharmacy Susan Cornell BS, PharmD, CDE, FAPhA, FAADE Midwestern
The Diabetes Guidelines Trek: The Next Generation J. Christopher Lynch, PharmD, BCACP Southern Illinois University Edwardsville School of Pharmacy Susan Cornell BS, PharmD, CDE, FAPhA, FAADE Midwestern
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
In-Hospital Management of Diabetes. Dr Benjamin Schiff Assistant Professor McGill University
 In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary
 Number 14 Effective Health Care Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary Background and Key Questions
Number 14 Effective Health Care Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary Background and Key Questions
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE
 INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
T2DM and Need for Insulin. Insulin Pharmacokinetics. When To Start Insulin in T2DM. FDA-approved Insulins for Subcutaneous Injection
 Plasma Insulin Levels Patients Requiring Insulin (%) Effective Use of Insulin in the Primary Care Practice: Insulin Therapy Initiation, Intensification, and the Insulinizing Complex Patients with T2DM:
Plasma Insulin Levels Patients Requiring Insulin (%) Effective Use of Insulin in the Primary Care Practice: Insulin Therapy Initiation, Intensification, and the Insulinizing Complex Patients with T2DM:
Faculty. Timothy S. Reid, MD (Co-Chair, Presenter) Medical Director Mercy Diabetes Center Janesville, WI
 Medical Director Mercy Diabetes Center Janesville, WI") Activity Overview In this case-based webcast, meet Jackie, a 62-year-old woman with type 2 diabetes. Her glycated hemoglobin (HbA1C) is 9.2%, and she is taking 2 oral agents and basal insulin; however,
Activity Overview In this case-based webcast, meet Jackie, a 62-year-old woman with type 2 diabetes. Her glycated hemoglobin (HbA1C) is 9.2%, and she is taking 2 oral agents and basal insulin; however,
Drugs used in Diabetes. Dr Andrew Smith
 Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
5/16/2018. Insulin Update: New and Emerging Insulins. Disclosures to Participants. Learning Objectives
 Insulin Update: New and Emerging Insulins Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA Disclosures to
Insulin Update: New and Emerging Insulins Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA Disclosures to
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES
 PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
Sponsor / Company: Sanofi Drug substance(s): HOE901-U300 (insulin glargine) According to template: QSD VERSION N 4.0 (07-JUN-2012) Page 1
: HOE901-U300 (insulin glargine) According to template: QSD VERSION N 4.0 (07-JUN-2012) Page 1") These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
Evolving insulin therapy: Insulin replacement methods and the impact on cardiometabolic risk
 Evolving insulin therapy: Insulin replacement methods and the impact on cardiometabolic risk Harvard/Joslin Primary Care Congress for Cardiometabolic Health 2013 Richard S. Beaser, MD Medical Executive
Evolving insulin therapy: Insulin replacement methods and the impact on cardiometabolic risk Harvard/Joslin Primary Care Congress for Cardiometabolic Health 2013 Richard S. Beaser, MD Medical Executive
Inpatient Management of Diabetes Mellitus. Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy
 Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
BRIAN MOSES, MD, FRCPC (INTERNAL MEDICINE) CHIEF OF MEDICINE, SOUTH WEST HEALTH
 CHIEF OF MEDICINE, SOUTH WEST HEALTH") Insulin Initiation BRIAN MOSES, MD, FRCPC (INTERNAL MEDICINE) CHIEF OF MEDICINE, SOUTH WEST HEALTH Disclosures In the past 12 months, I have received speakers honoraria from AstraZeneca, Boehringer Ingelheim,
Insulin Initiation BRIAN MOSES, MD, FRCPC (INTERNAL MEDICINE) CHIEF OF MEDICINE, SOUTH WEST HEALTH Disclosures In the past 12 months, I have received speakers honoraria from AstraZeneca, Boehringer Ingelheim,
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Guide to Starting and Adjusting Insulin for Type 2 Diabetes*
 Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
Session 3: Insulin Strategies for Primary Care Providers: Addressing a Core Defect in Diabetes Learning Objectives
 Session 3: Insulin Strategies for Primary Care Providers: Addressing a Core Defect in Diabetes Learning Objectives 1. Design strategies to help patients overcome cultural barriers to using insulin, and
Session 3: Insulin Strategies for Primary Care Providers: Addressing a Core Defect in Diabetes Learning Objectives 1. Design strategies to help patients overcome cultural barriers to using insulin, and
Intensification of Diabetic Therapy. Case studies
 Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
Guideline for antihyperglycaemic therapy in adults with type 2 diabetes
 Guideline for antihyperglycaemic therapy in adults with type 2 diabetes Version Control Version Number Date Amendments made 1 January 2018 1.1 February 2018 Amended to reflect updated SPC advice for sitagliptin
Guideline for antihyperglycaemic therapy in adults with type 2 diabetes Version Control Version Number Date Amendments made 1 January 2018 1.1 February 2018 Amended to reflect updated SPC advice for sitagliptin
Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς
 Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς Αναστασία Θανοπούλου Επίκουρη Καθηγήτρια Β Παθολογικής Κλινικής Πανεπιστημίου Αθηνών Διαβητολογικό Κέντρο, Ιπποκράτειο Νοσοκομείο
Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς Αναστασία Θανοπούλου Επίκουρη Καθηγήτρια Β Παθολογικής Κλινικής Πανεπιστημίου Αθηνών Διαβητολογικό Κέντρο, Ιπποκράτειο Νοσοκομείο
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy
 Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
MANAGEMENT OF TYPE 1 DIABETES MELLITUS
 MANAGEMENT OF TYPE 1 DIABETES MELLITUS INVESTIGATIONS AND TREATMENT MANSI NAIK VII SEMESTER INVESTIGATIONS FASTING BLOOD SUGAR PLASMA GLUCOSE HEMOGLOBIN A 1c SYMPTOMS OF TYPE 1 DIABETES MELLITUS Polyuria
MANAGEMENT OF TYPE 1 DIABETES MELLITUS INVESTIGATIONS AND TREATMENT MANSI NAIK VII SEMESTER INVESTIGATIONS FASTING BLOOD SUGAR PLASMA GLUCOSE HEMOGLOBIN A 1c SYMPTOMS OF TYPE 1 DIABETES MELLITUS Polyuria
New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection
 New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection Date of Review: March 2016 End Date of Literature Search: November 11, 2015 Generic Name: Insulin degludec and insulin aspart Brand
New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection Date of Review: March 2016 End Date of Literature Search: November 11, 2015 Generic Name: Insulin degludec and insulin aspart Brand
5/16/2018. Insulin Workshop. Disclosures to Participants. Learning Objectives. This presentation will cover the following learning objectives:
 Insulin Workshop Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA Holly Divine, PharmD, BCACP, BCGP, CDE,
Insulin Workshop Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA Holly Divine, PharmD, BCACP, BCGP, CDE,
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Sponsor / Company: Sanofi Drug substance(s): HOE901-U300 (insulin glargine)
: HOE901-U300 (insulin glargine)") These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
7/8/2016. Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine
 Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
MOA: Long acting glucagon-like peptide 1 receptor agonist
 Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Progressive Loss of β-cell Function in T2DM
 Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current as of November 2015. The content and views presented in this educational activity are those of
Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current as of November 2015. The content and views presented in this educational activity are those of
BEST 4 Diabetes. Optimisation of insulin module
 BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS
 Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure
Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure
Sponsor / Company: Sanofi Drug substance(s): insulin glargine (HOE901) According to template: QSD VERSION N 4.0 (07-JUN-2012) Page 1
: insulin glargine (HOE901) According to template: QSD VERSION N 4.0 (07-JUN-2012) Page 1") These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
Diabetes, Type 2 Management
 CLINICAL GUIDELINE Diabetes, Type 2 Management A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised on the applicability
CLINICAL GUIDELINE Diabetes, Type 2 Management A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised on the applicability
BEST 4 Diabetes. Optimisation of insulin module
 BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
Review of biphasic insulin aspart in the treatment of type 1 and 2 diabetes
 REVIEW Review of biphasic insulin aspart in the treatment of type 1 and 2 diabetes Nazia Raja-Khan Sarah S Warehime Robert A Gabbay Division of Endocrinology, Diabetes, and Metabolism, Penn State Institute
REVIEW Review of biphasic insulin aspart in the treatment of type 1 and 2 diabetes Nazia Raja-Khan Sarah S Warehime Robert A Gabbay Division of Endocrinology, Diabetes, and Metabolism, Penn State Institute
Treatment Options for Diabetes: An Update
 Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Starting and Helping People with Type 2 Diabetes on Insulin
 Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
COPYRIGHT. Advancing to Insulin Replacement Therapy: When, Why, and How? Update in Internal Medicine December 5, Richard S.
 Advancing to Insulin Replacement Therapy: When, Why, and How? Update in Internal Medicine - 2016 December 5, 2016 Richard S. Beaser, MD Medical Director, Professional Education Joslin Diabetes Center Associate
Advancing to Insulin Replacement Therapy: When, Why, and How? Update in Internal Medicine - 2016 December 5, 2016 Richard S. Beaser, MD Medical Director, Professional Education Joslin Diabetes Center Associate
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES
 PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
Insulin Therapies for T2DM
 Insulin Therapies for T2DM Defects in T2DM Decreased insulin secretion Inefficient glucose uptake (skeletal muscles) Increased hepatic glucose production Decreased incretin effect Increased glucagon secretion
Insulin Therapies for T2DM Defects in T2DM Decreased insulin secretion Inefficient glucose uptake (skeletal muscles) Increased hepatic glucose production Decreased incretin effect Increased glucagon secretion
Diabetes: Inpatient Glucose control
 Diabetes: Inpatient Glucose control Leanne Current, PharmD, BCPS This activity is funded through the Medicaid section 1115(a) Demonstration Texas Healthcare Transformation and Quality Improvement Program
Diabetes: Inpatient Glucose control Leanne Current, PharmD, BCPS This activity is funded through the Medicaid section 1115(a) Demonstration Texas Healthcare Transformation and Quality Improvement Program
Efficacy and safety of premixed insulin analogs in Asian patients with type 2 diabetes: A systematic review
 Efficacy and safety of premixed insulin analogs in Asian patients with type 2 diabetes: A systematic review Wayne H-H Sheu 1,2,3,LinongJi 4,WooJeLee 5, Abdul Jabbar 6,JeongHeeHan 7,ThomasLew 8 * 1 Division
Efficacy and safety of premixed insulin analogs in Asian patients with type 2 diabetes: A systematic review Wayne H-H Sheu 1,2,3,LinongJi 4,WooJeLee 5, Abdul Jabbar 6,JeongHeeHan 7,ThomasLew 8 * 1 Division
Application of the Diabetes Algorithm to a Patient
 Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Achieving Glycemic Control: When Optimized Basal Insulin Isn t Adequate
 Achieving Glycemic Control: When Optimized Basal Insulin Isn t Adequate AAFP State Chapter Meeting Faculty Louis Kuritzky MD Clinical Assistant Profess Emeritus Department of Community Health and Family
Achieving Glycemic Control: When Optimized Basal Insulin Isn t Adequate AAFP State Chapter Meeting Faculty Louis Kuritzky MD Clinical Assistant Profess Emeritus Department of Community Health and Family
Julie White, MS Administrative Director Boston University School of Medicine Continuing Medical Education
 MENTOR QI Diabetes Performance Improvement Initiative, Getting Patients to Goal in Glycemic Control: Current Data Julie White, MS Administrative Director Boston University School of Medicine Continuing
MENTOR QI Diabetes Performance Improvement Initiative, Getting Patients to Goal in Glycemic Control: Current Data Julie White, MS Administrative Director Boston University School of Medicine Continuing
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017
 TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive