Managing MDR TB Treatment Side Effects
|
|
|
- Preston Oliver
- 6 years ago
- Views:
Transcription

1 Managing MDR TB Treatment Side Effects Barbara J. Seaworth, M.D. Medical Director Heartland National TB Center Pacific Islands TB Controllers Association Conference, September 14, 2017 Honolulu, Hawaii
2 Disclosure Dr. Seaworth has no financial disclosures This presentation will include the off label use of fluoroquinolones and linezolid
3 Objectives Identify common toxicities of second line TB drugs Implement monitoring for toxicity due to second line TB drugs Recognize how to modify treatment to ensure a good outcome
4 Anti-tuberculosis Drugs (ATS/CDC/IDSA) First-Line drugs Isoniazid Rifampin Rifapentene Rifabutin* Ethambutol Pyrazinamide Second-Line Drugs Cycloserine Ethionamide Levofloxacin* Moxifloxacin* PAS Streptomycin Amikacin/Kanamycin Capreomycin Linezolid* Clofazimine* Bedaquiline Delamanid* Meropenem/Clavulanic acid* *Not FDA approved for TB
 Ethionamide/ Prothionamide Cycloserine/ Terizidone Clofazimine Linezolid D1: Pyrazinamide Ethambutol High-dose INH D2: Bedaquiline Delamanid D3: P-aminosalicylic acid")
5 New Grouping of MDR-TB Drugs Group A Group B Group C Group D Fluoroquinolone Second-line injectable Other Core Second-line Add-on agents Levofloxacin Moxifloxacin Gatifloxacin Amikacin Capreomycin Kanamycin (Streptomycin) Ethionamide/ Prothionamide Cycloserine/ Terizidone Clofazimine Linezolid D1: Pyrazinamide Ethambutol High-dose INH D2: Bedaquiline Delamanid D3: P-aminosalicylic acid Imipenem/Meropenem Amoxicillin/Clavulanate (Thioacetazone)
6 Adverse Drug Events GI upset: PZA, rifabutin, fluoroquinolones, ethionamide, PAS, bedaquiline, (any drug) Central Nervous System: INH, fluoroquinolones, amikacin, ethionamide, cycloserine Musculoskeletal: PZA, fluoroquinolones, rifabutin
7 Dermatological Any drug Allergic reactions Flushing, photosensitivity, hyperpigmentation, lichenoid drug reactions Systemic DRESS Syndrome rifampin, PZA, INH-(any) Hematological most but especially linezolid Miscellaneous Adverse Drug Events Hypothyroidism ethionamide, PAS QT interval prolongation - FQNs, bedaquiline, clofazimine, delamanid

8 Sometimes our interventions can be dangerous
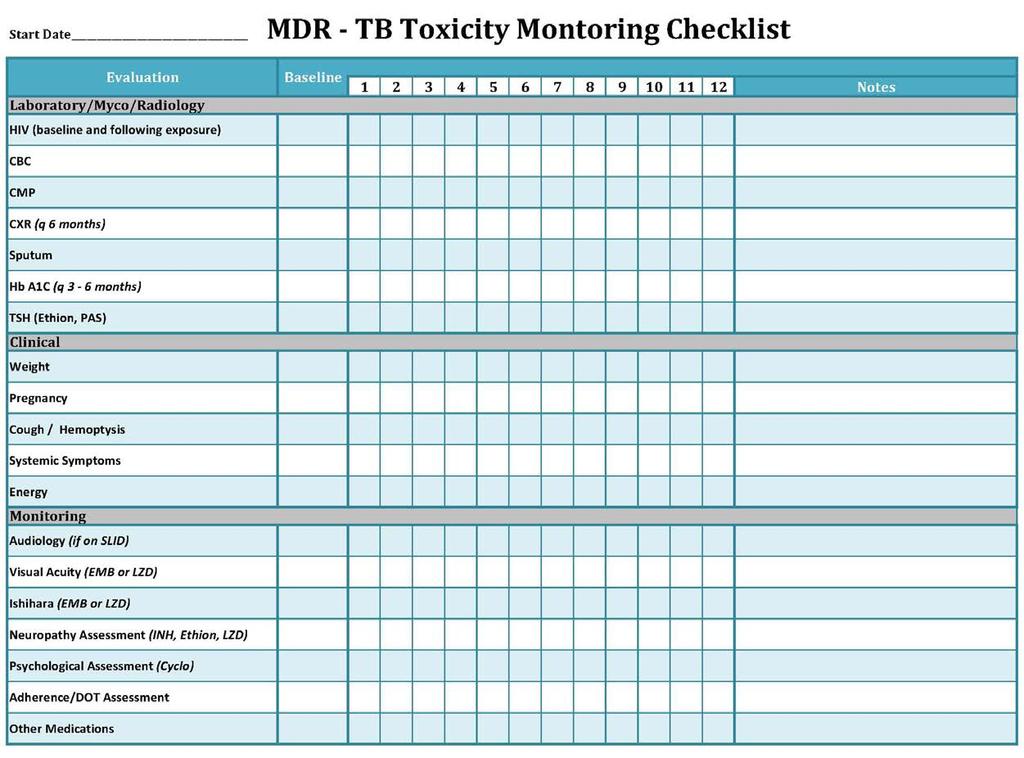
9 Toxicity Monitoring Face-to-face clinical assessments are the cornerstone of clinical monitoring for treatment adherence and adverse events. Patients should be categorically told to immediately stop medications (INH) for nausea, vomiting, abdominal discomfort, or unexplained fatigue and to contact the clinic for further evaluation Document, document, document!
10 Adverse Drug Events Side Effects or Toxicity? Patient likely cannot differentiate they both feel bad! Evaluate risk to patient and if medication needs to be stopped. Risk of long term harm to patient Risk of treatment failure/poor outcome if no replacement Work with patient to tolerate side effects
11 Strategies for Managing Adverse Reactions Prior to initiating a treatment regimen discuss the benefits and risks of therapy. Assure patients that every possible attempt to make their treatment as easy as possible will be made, but emphasize that having enough effective drugs in the regimen is essential to achieving a cure. Discuss the importance of having enough strong medications in the treatment to ensure lasting cure
12 Strategies for Managing Adverse Reactions Quickly recognize and respond to the symptoms a patient expresses Evaluate cause of symptoms; exclude other causes Develop a plan to address along with patient if possible Continue with planned regimen to manage side effects: Encourage patient to continue medication with knowledge that side effects often become more tolerable with time Stop and substitute another drug if needed and this is possible Encourage adequate hydration Correct electrolyte deficiencies Do not continue an inadequate regimen
13

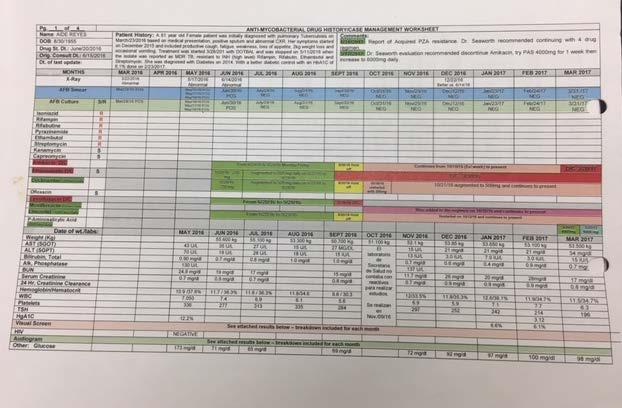
14 RX: Amikacin, Levo, LZD, Ethionamide, Cycloserine Culture neg in 1 st mo. RX Nl LFTs; Held all 9/27/16, restart Amik, moxi first then LZD, then, cyclo OK, but with ethionamide new N/V so left with 4 drug but good regimen? Possible cycloserine, but long term history of this Watch closely 4 drugs needed Likely LZD but with only 4 drugs need this S/P 9 months of amikacin, so stopped PAS added Cavity gone, but must stop LZD and ethionamide Moxifloxacin, Cycloserine, PAS Terrible Regimen but little disease, yr 2 RX
15

16
17 Responding to GI Upset Exclude hepatitis If symptoms resolve and no evidence of liver toxicity, when possible re-institute at a lower dose and/or different time give with anti-emetic 30 minutes prior to dose take with small snack, tea, soda If ethionamide or PAS can divide dose Antacids may be helpful in some patients
18 Common causes of GI symptoms Gastritis Hepatitis/ hepatotoxicity Biliary disease/pancreatitis Other infections - UTI Peptic ulcer disease Clostridium difficile colitis Inflammatory bowel disease Lactose intolerance Acute renal failure or nephrotoxicity GI TB especially if early in treatment or unrecognized TB meningitis Diabetic gastroparesis Pregnancy Other medications/etoh
19 Responding to GI Upset Minimize use of non-steroidal antiinflammatory drugs Evaluate for other medication related causes Consider hospitalization if above not helpful; do so early to prevent psychological intolerance which is very difficult to overcome In hospital space medications, hydrate, antiemetics, IV medications
20 Responding to GI Upset When problem is diarrhea (especially with PAS) this usually improves with time Exclude C. difficile colitis Exclude gastro-intestinal TB May try pro-biotics Loperamide (Imodium) 2 to 4 mg initially then 1 to 2 mg after each loose stool Exclude lactose deficiency especially if patient hospitalized and has change in diet
21 Neurotoxicity Sensory peripheral neuropathy Optic (Retrobulbar) neuritis Central Nervous System
22 Adverse Drug Events Neurotoxicity Peripheral neuropathy Drugs: INH, Linezolid ( usually > 12 weeks use), Ethionamide, Cycloserine Fluoroquinolones and EMB have rarely been associated although neuropathy has recently been added as a black box warning for the fluoroquinolones. More common in patients with Diabetes Alcoholism HIV infection Hypothyroidism Pregnancy Inadequate dietary intake of pyridoxine (Vitamin B6) Usually symmetrical Initial symptoms: tingling, prickling, burning in balls of feet/tips of toes May progress to sensory loss, loss of reflexes, unsteady gait May also involve hands and fingers Pyridoxine prophylaxis mg daily. Efficacy unclear

23 Peripheral Neuropathy Evaluation Lower Extremities Upper Extremities Patient s name: DOB: Date of evaluation: PATIENT S INTERVIEW Ask your patient the following questions: Question 1: Yes Do you have any pain in your feet? Question 2: Does your pain have any of these characteristics? Yes 1 Burning? 2 Freezing pain? 3 Electric shock-type sensation? No No Question 3: Do you have any of these symptoms in the area? Yes No 4 Tingling 5 Prickling 6 Numbness 7 Stinging/itchin g Question 4: Is the pain made worse with the touch of clothing or bed sheets? Yes No PATIENT S INTERVIEW Ask your patient the following questions: Question 1: Yes Do you have any pain in your hands? Question 2: Does your pain have any of these characteristics? Yes 1 Burning 2 Freezing pain? 3 Electric shocktype sensation? Question 3: Do you have any of these symptoms in the area? Yes 4 Tingling 5 Prickling 6 Numbness 7 Stinging/Itchin g Question 5 Is the pain made worse with the touch of clothing or bed sheets? Yes No No No No PATIENT S ASSESSMENT Question 5: 8 Hypoesthesia to touch 9 Hypoesthesia to prick 10 Extreme sensitivity to touch 11 Extreme sensitivity to prick Yes No PATIENT S ASSESMENT Question 4: 8 Hypoesthesia to touch 9 Hypoesthesia to prick 10 Extreme sensitivity to touch 11 Extreme sensitivity to prick Yes No
24 Management of Peripheral Neurotoxicity Correct vitamin and nutritional deficiencies. Address additional medical problems. Evaluate and correct electrolytes. Identify and stop (if possible) other medications that may cause peripheral neuropathy. Consider whether the dose of ETA or CS can be reduced without compromising the regimen. Consider decreasing dose of linezolid if symptoms progressive and distressing to patient, usually tolerate some peripheral numbness if needed but not painful neuropathy Monitor serum drug concentrations if doses lowered.
25 Management of Peripheral Neurotoxicity NSAIDs or acetaminophen may be helpful. Gabapentin (Neurontin) helpful for some. Adults initially 300 mg PO on Day 1, increase to 300 mg 2 x/day on Day 2, and 300 mg 3 x/day on Day 3. Titrate up to 1800 mg in 3 divided doses, as needed A low dose of tricyclic antidepressant (amitriptyline [Elavil] 25 mg PO at bedtime) can be tried if there are no contraindications. Carbamazepine (Tegretol), an anticonvulsant, at 100 to 400 mg PO BID, can be tried. Monitor CBC and liver enzymes.
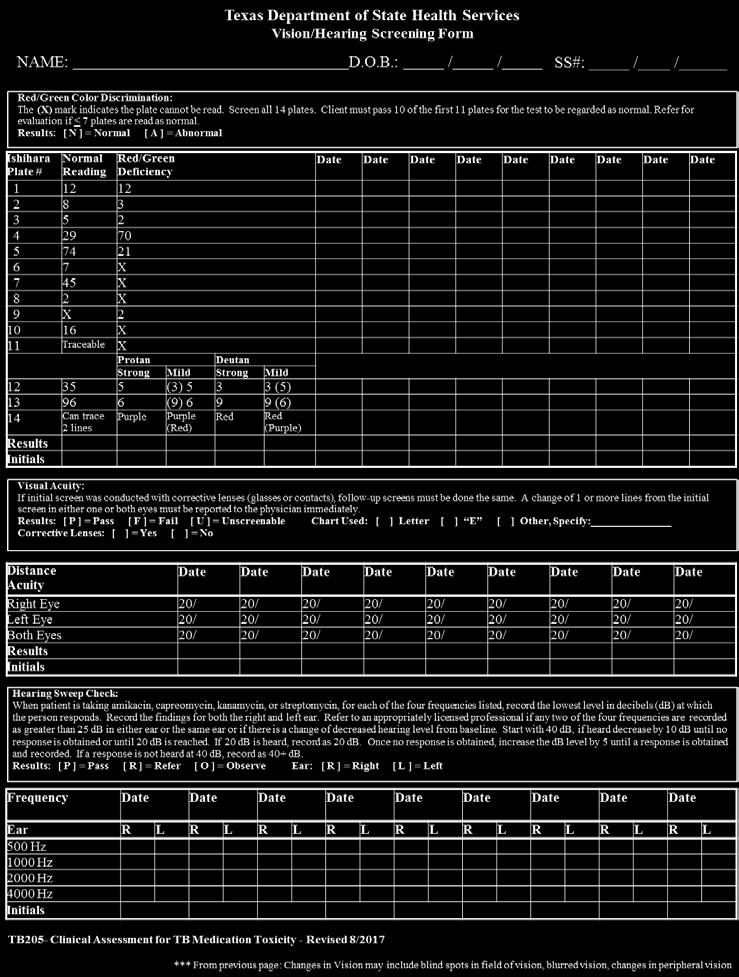
26 Retrobulbar Neuritis Toxicity: Monitoring All patients should have baseline visual acuity (Snellen) and color vision discrimination (Ishihara). PATIENT EDUCATION Symptom check (blurred vision, scotoma) with DOT Monthly testing, increased risk with EMB in pts with renal insufficiency If patient reported symptom or abnormality detected in toxicity screening, Ophthalmology evaluation Hold medication potentially responsible (EMB, Linezolid)
27 Retrobulbar Neuritis Toxicity Decreased visual acuity or red-green color discrimination Dose related, Unusual at EMB dose 15 mg/kg. Increased risk with renal insufficiency. Usually occurs after weeks of Linezolid
28
29 Central Nervous System Toxicity A variety of mild effects may occur early Drowsiness, headaches, poor concentration, irritability, mild mood changes, insomnia, & agitation. Caution patients to expect these effects and understand that they typically become less problematic after the initial weeks of therapy. Tolerance develops towards most of these effects and the patient learns to cope with them.
30 Central Nervous System Toxicity Psychiatric effects Depression may lead to suicidal ideation if medication continues Cycloserine, ethionamide, INH and due to reaction to hyperpigmentation in some taking clofazimine Medication must be stopped and patient watched closely until no longer a threat to self if suicidal May be able to restart at lower dose Psychosis Most likely drug is cycloserine, occasionally FQNs & INH Consult a psychiatrist Patient may need to be hospitalized
31 Central Nervous System Toxicity Seizures Hospitalize patient Drugs most likely responsible cycloserine, FQNs, linezolid, INH, imipenem Serotonin Syndrome At least one of following: clonus, seizure, myoclonus, ataxia, incoordination, jawtrimus, rigidity, shivering, rigors, nystagmus, tremor/twitching, hyperreflexia Also - tachycardia, fever, mydriasis, diaphoresis, hyperactive bowel, diarrhea, agitation, delirium.
32 Serotonin Syndrome Clinical symptoms and signs that occur in the presence of excess serotonin activity. 3 different mechanisms - elevated serotonin levels: inhibition of serotonin metabolism (MAO inhibitor use) blockade of serotonin reuptake at the presynaptic neuron (SSRI and/or tricyclic antidepressant use) or increase in the release of stored serotonin (amphetamine use). LZD - weak, reversible, nonselective MAO inhibitor
33 Serotonin Syndrome (SS) LZD alone is not potent enough to cause SS may occur when LZD given with medications that increase the serotonin level or when diet is high in tyramine (cheese, cured meats, fermented soy products or sauce, red wine). Although rare, it can be severe and even fatal. Syndrome does not resolve unless the offending medications are withdrawn, recognition is imperative. Clinical picture varies from mild to severe
34 Serotonin Syndrome (SS) The syndrome develops soon after the introduction of the offending medication or an increase in a dose of a previously used drug. Physical exam should focus on assessment for clonus, deep-tendon reflexes, pupil size, mucosal dryness, bowel sounds, and diaphoresis. A good drug history including use of over-the-counter medications, herbal and dietary supplements, and illicit drugs (in addition to any recently prescribed drugs) is an essential part of the evaluation. The differential diagnosis includes anticholinergic poisoning, malignant hyperthermia, and neuroleptic malignant syndrome. The drug history will help to identify the cause. The SSRIs or tricyclics cannot be abruptly stopped and even if discontinued will continue to exert effects due to their long drug half-life. Supportive care, stop linezolid
35 Severe Systemic Drug Reactions Drugs should not be continued if systemic symptoms, fever, urticaria, mucous membrane involvement, blistering of the skin, edema of the lips or eyes, or wheezing or compromise of the airway. Consult with a TB expert, a dermatologist, and possibly an allergist for desensitization prior to rechallenge with any of the anti-tuberculosis medications.

36 Quinn d, Stern T, Linezolid and Serotonin Syndrome Prim Care Companion J Clin Psychiatry 2009
37 CID 2006

38 Hematological Toxicity of TB Drugs Drug Resistant Tuberculosis: A Survival Guide for Clinicians, 3 rd edition Curry International Tuberculosis Center
39 Hematological Abnormalities May be due to medications (TB or other) May represent underlying disease Chronic renal failure anemia Chronic liver disease anemia, low platelet count GI disease with blood loss anemia Disseminated TB involving bone marrow anemia, low white blood count, low platelet count
40
41 Adverse Drug Events Nephrotoxicity Drugs: aminoglycosides, capreomycin rarely rifamycins including rifabutin Monitoring - baseline serum creatinine, repeat at least monthly Lower initial dose in patients > age 59 yrs. (10 mg/kg) If baseline creatinine clearance < 70ml/min, avoid injectable drugs if possible or consider use of intermittent dosing initially Monitor peak and trough serum drug levels and adjust dose accordingly Encourage good hydration If creatinine increases, hold medication 1 2 weeks and watch If need to continue, restart at 2 3 x/week dosing Follow creatinine weekly
42 Ototoxicity All of the aminoglycosides and CM are toxic to the eighth cranial nerve. Can cause vestibular and auditory toxicity Usually do not occur together but may in 3 5% of patients Vestibular toxicity May manifest as tinnitus, dizziness, or unsteadiness. Fullness in the ears may be an early symptom of vestibular toxicity. Auditory toxicity Some degree of hearing loss occurs in > 50% of patients
43 Ototoxicity Vestibular Toxicity Perform baseline assessment of balance and ask about tinnitus and dizziness Educate patient about toxicity and request that they identify any change at time of DOT Monitor vestibular toxicity monthly and identify changes See toxicity checklist Toxicity may be limited if found early and injectable stopped May be permanent and patient can have severe problems if drug is continued once toxicity identified
44 Assessment Tool for Ototoxicity DATE: QUESTIONS Hearing Vestibular Testing Report Ears full or stuffy Weak Nausea TYPE OF TEST Balance Walking Past Pointing Lateral Nystagmus Romberg Heel to toe walk RESPONSE OK: Left / Right IMPAIRED: Left / Right Left: Yes / No Right: Yes / No Yes / No None / Sometimes / Always RESULTS Ok / Teeters Falls? Left / Right Ok / Weaves / Stagger Yes / No Left / Right Yes / No Normal / Falls Does Well / Jerky Hesitates / Sways Past pointing A. Patient sits facing you, with his/her eyes closed B. Have him/her point their fingers, then place your fingers below theirs C. Hold your position, ask patient to raise both hands and return fingers to yours D. Deviation R & L from target fingers-past pointing Lateral Nystagmus A. Patient sits on exam table for 30 seconds B. Lies down, look for nystagmus (jerking of eyeballs side to side) C. Log roll patient to one side, wait 30 seconds, look for nystagmus, then try the other side Romberg A. Patient stands with feet together B. Encircle the patient with your arms, but do not touch C. Tell the patient I will not let you fall and have the patient close their eyes E. Falling is a positive Romberg sign Heel to toe walking A. Stand beside standing patient B. Demonstrate walking heel to toe Hertz (HZ) Frequency C. Do it together (be prepared to catch pt.) Right: X Left: O D. Observe for jerkiness, falling swaying D E C I B E L S Audiogram
45 Ototoxicity Auditory Toxicity Injectable drugs have direct toxicity to 8 th cranial nerve Streptomycin usually identified as having less auditory toxicity but not all studies agree Hearing loss is usually permanent Hearing loss may progress for months after injectable is stopped Monitor at 3 and 6 months after stopping drugs If possible stop injectable or decrease dose/ increase interval when early loss is detected Baseline audiogram should always be done Ask about prior injectable drugs, family history of hearing loss

46 USAID, KNCV Tuberculosis Foundation, Challenge TB
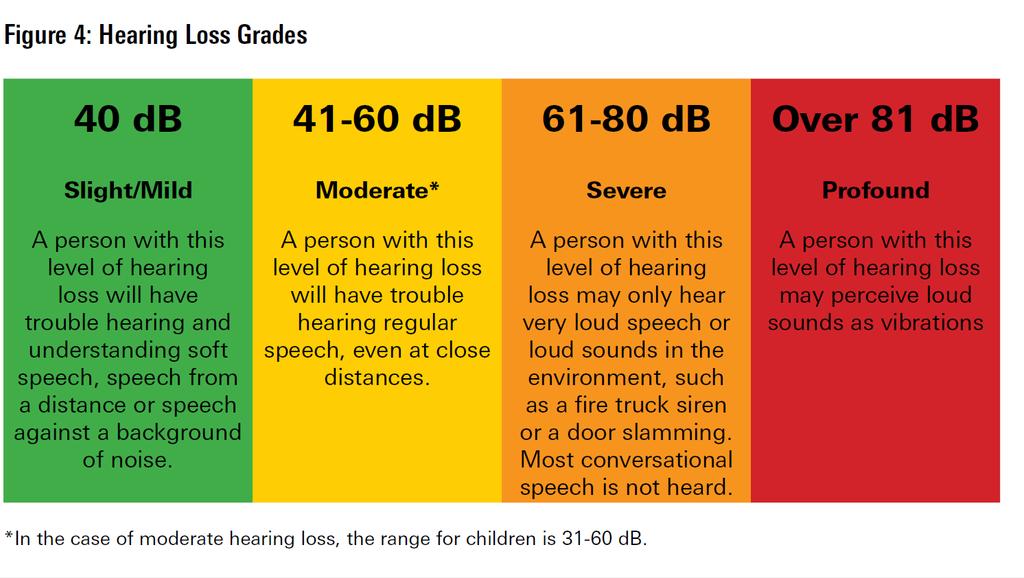
47 Ototoxicity Auditory Toxicity Normal hearing thresholds are at 25 decibels (db), or lower, in both ears. If hearing is not at this level the individual has hearing loss Damage to inner ear (cochlea) leads to sensorineural hearing loss (SNHL) nerve related Usually cannot be corrected surgically or medically Cochlear implants can be helpful Hearing aids often not very helpful Conductive hearing loss due to problem with ear canal, ear drum, or middle ear and little bones
48 Ototoxicity Auditory Toxicity Audiometry is the procedure that tests ability to hear various sound frequencies Can test air conduction and bone conduction Audiogram is the graph showing the result of a pure tone audiometry which determines faintest tones a person can hear at selected pitches or frequencies from low to high. Pitch or frequency is referred to in Hertz (Hz) Loudness is measured in decibels (db)
49 Ototoxicity Auditory Toxicity Hearing loss due to ototoxic drugs starts at high frequencies So does age related hearing loss Risk increased with HIV, genetic predisposition Baseline audiogram needed to identify hearing loss already present Repeat monthly and 6 months after drug stopped At speech frequencies Hz and higher 8000Hz Serial audiograms best indication of hearing loss

50 USAID, KNCV Tuberculosis Foundation, Challenge TB
51 Ototoxicity Auditory Toxicity Screening audiometry suggestive of ototoxicity Decrease in hearing threshold by 20 db or more at any one test frequency Decrease in hearing threshold by 10 db or more at any two adjacent frequencies Loss of response at three frequencies where responses were previously obtained Monitor more frequently if tinnitus, dizziness or vertigo noted Exclude other causes ear wax, otitis media, perforation of tympanic membrane
52 Auditory Toxicity When Should Injectable Be Stopped? Tinnitus or unsteadiness attributable to vestibular toxicity Persistent vertigo and ataxia is intolerable, not reversible Moderate or severe hearing loss; earlier if possible Ensure adequate regimen if injectable stopped
53 WHO Classification

54 Baseline -normal Initial loss Progressive loss due speech
55 What Else Might Be Done to Prevent Hearing Loss? Damage to 8 th nerve due to reactive oxygen species Theoretically possible to mitigate these effects Iron chelation but many other toxicities Aspirin Research needed to guide these efforts
56 Fluoroquinolones Moxifloxacin>levofloxacin>ofloxacin>ciprofloxacin Bedaquiline QT interval prolongation Degree of risk not determined with recent studies Risk of torsades de pointes unknown (?small) Optimal screening and monitoring unknown Classic example of risk/benefit assessment
57 Rifabutin Toxicity Hematologic toxicity: neutropenia and thrombocytopenia Drug interactions: less severe than rifampin Uveitis: Rare, < 0.01% GI Symptoms Polyarthralgias: 1-2% at standard doses Pseudojaundice (HIV, with clarithromycin and EMB) Hepatotoxicity, flu-like syndrome
58 Pyrazinamide (PZA) Toxicity Hepatotoxicity: Less at 25 mg/kg than 50 mg/kg Gastrointestinal symptoms: nausea and vomiting mild at standard doses. Nongouty polyarthralgia: Up to 40% of patients: not an indication to stop therapy. Asymptomatic hyperuricemia: Expected Acute gouty arthritis: Unusual except in patients with pre-existing gout. Rash/dermatitis: usually self limited
59 Fluoroquinolone Toxicity Musculoskeletal Tendonitis/Tendon Rupture (Black box warning) If tendon inflammation is mild: Rest the joint/nsaid s Reduce dose of FQ if possible If symptoms progress, stop the FQ If tendon inflammation is moderate/severe Stop the FQ Rest the joint/nsaid s Risk/benefit evaluation of FQ continuation Tendon rupture (usually Achilles) is rare
60 Fluoroquinolone Toxicity Gastrointestinal disturbance: nausea/bloating 0.5-2% Neurologic effects: dizziness, insomnia, tremulousness, headache 0.5% Cutaneous reactions: rash, pruritis, photosensitivity % Arrhythmias: QT prolongation (congenital, medications, MI)
61 Second-Line TB Drugs Cycloserine Central Nervous System Effects: headaches, restlessness, suicidal ideation psychosis, seizures (3% at 500 mg/day). May exacerbate underlying seizure disorders or mental illness. Pyridoxine at mg/day may help prevent neurotoxicity Administer with caution to alcoholics, patients with history of mental illness or seizures Peripheral neuropathy Rash Drug levels are necessary reduce dose if peak levels >35 even if no symptoms mcg/ml)
62 Second-Line TB Drugs Ethionamide Gastrointestinal Effects: commonly causes profound GI side-effects. Symptoms may improve if taken with food or at bedtime Hepatotoxicity: 2% of patients Neurotoxicity: Peripheral neuritis, optic neuritis, depression, psychosis Endocrine Effects: blood glucose abnormalities hypothyroidism, gynecomastia, hair loss, Acne, metallic taste in mouth
63 Injectable TB Drugs Streptomycin, Kanamycin, Amikacin, Capreomycin Ototoxicity Nephrotoxicity Electrolyte disturbances: hypokalemia, hypomagnesemia, cardiac dysrhythmias Rash
64 Second-Line TB Drugs P-Aminosalicylic acid (PAS) Gastrointestinal Distress: less with lower doses, diarrhea may be debilitating Hepatotoxicity: 0.3% of patients (including jaundice) Malabsorption syndrome Hypothyroidism: common with prolonged administration or concomitant ethionamide Rash, lymphadenopathy, leukocytosis, arthralgia Fluid overload
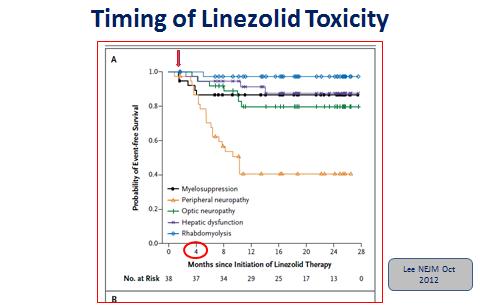
65 Second-Line TB Drugs Linezolid Myelosuppression Peripheral Neuropathy Optic Neuritis Gastrointestinal Disturbance Rash Hepatitis (rare) Serotonin Syndrome Lactic acidosis Rhabdomyolysis
66 Linezolid for treatment of chronic extensively drug-resistant tuberculosis (Myungsun et al NEJM 2012, 367; 1508) 82% clinically significant adverse events (AE s) possibly or probably linezolid related 7 episodes of myelosuppression (anemia and leukopenia) 7 episodes optic neuropathy 21 episodes of peripheral neuropathy 1 episode rhabdomyolysis Only 3 patients permanently discontinued linezolid owing to drug toxicity 1 anemia, 2 optic neuropathy
67 References Agents,Tuberculosis 2008; 66: Treatment of Tuberculosis: Am J Respir Crit Care Med, 2003; 167: Hepatotoxicity of Antituberculosis Therapy: Am J Respir Crit Care Med, 2006; 174: Official ATS/CDC/IDSA Clinical Practice Guidelines: Treatment of Drug Susceptible Tuberculosis: Clin Infect Dis, 2016;63: Drug Resistant Tuberculosis: A Survival Guide for Clinicians, 3 rd edition Curry International Tuberculosis Center Seaworth BJ, Griffith DE Therapy of multidrug-resistant and extensively drug-resistant tuberculosis. Microbiolspec April; 5(2) Hearing loss in patients on treatment for drug-resistant tuberculosis Seddon J, et al ERJ Express June 14, 2012
Drug Interactions Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Anti Tuberculosis Medications: Side Effects & adverse Events
 Anti Tuberculosis Medications: Side Effects & adverse Events Diana Fortune, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Diana Fortune, RN,
Anti Tuberculosis Medications: Side Effects & adverse Events Diana Fortune, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Diana Fortune, RN,
Tuberculosis medications: adverse drug reactions
 Tuberculosis medications: adverse drug reactions Rajesh M. Prabhu, M.D. Infectious Diseases Essentia Health, Duluth, MN July 25, 2017 2014 MFMER slide-1 No Finanial Disclosures Learning Objectives 1. Describe
Tuberculosis medications: adverse drug reactions Rajesh M. Prabhu, M.D. Infectious Diseases Essentia Health, Duluth, MN July 25, 2017 2014 MFMER slide-1 No Finanial Disclosures Learning Objectives 1. Describe
TB Nurse Case Management San Antonio, TX. TB Medications and Adverse Effects
 TB Nurse Case Management San Antonio, TX April 1 3, 2014 TB Medications and Adverse Effects Debbie Onofre RN, BSN Nurse Consultant/ Nurse Educator Heartland National TB Center April 1, 2014 Debbie Onofre,
TB Nurse Case Management San Antonio, TX April 1 3, 2014 TB Medications and Adverse Effects Debbie Onofre RN, BSN Nurse Consultant/ Nurse Educator Heartland National TB Center April 1, 2014 Debbie Onofre,
Debbie Onofre, RN, BSN March 18, TB Nurse Case Management March 17 19, 2015 San Antonio, Texas
 Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Debbie Onofre, RN, BSN March 18, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION
Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Debbie Onofre, RN, BSN March 18, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Managing Anti-TB Therapy Side Effects and Complications Lisa Armitige, MD, PhD May 9, 2012 Lisa Armitige, MD, PhD has the following
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Managing Anti-TB Therapy Side Effects and Complications Lisa Armitige, MD, PhD May 9, 2012 Lisa Armitige, MD, PhD has the following
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014
 Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Monitoring Patients for TB Adverse Reactions and Managing Side Effects Catalina Navarro, RN, BSN April 11, 2014 Catalina Navarro, RN,
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Monitoring Patients for TB Adverse Reactions and Managing Side Effects Catalina Navarro, RN, BSN April 11, 2014 Catalina Navarro, RN,
Medication Administration and Adverse Reactions Alisha Blair, LVN September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Medication Administration and Adverse Reactions Alisha Blair, LVN September 28, 2011 Alisha Blair, LVN, has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Medication Administration and Adverse Reactions Alisha Blair, LVN September 28, 2011 Alisha Blair, LVN, has the following disclosures to make:
TB Nurse Case Management San Antonio, Texas
 TB Nurse Case Management San Antonio, Texas April 1 3, 2014 Practicum: Monitoring Side Effects & Identifying Toxicities Dawn Farrell, BSN., RN. Texas Center for Infectious Disease Nurse Educator / Training
TB Nurse Case Management San Antonio, Texas April 1 3, 2014 Practicum: Monitoring Side Effects & Identifying Toxicities Dawn Farrell, BSN., RN. Texas Center for Infectious Disease Nurse Educator / Training
TB Nurse Case Management
 TB Nurse Case Management San Antonio, Texas March 2-4, 2011 TB Medications and Adverse Effects Debbie Onofre, RN, BSN March 3, 2011 Debbie Onofre, RN, BSN has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas March 2-4, 2011 TB Medications and Adverse Effects Debbie Onofre, RN, BSN March 3, 2011 Debbie Onofre, RN, BSN has the following disclosures to make: No conflict
Drug Side Effects and Toxicity
 Drug Side Effects and Toxicity Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Toxicity Nausea and vomiting Any Drug Can Cause
Drug Side Effects and Toxicity Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Toxicity Nausea and vomiting Any Drug Can Cause
DRUG SIDE EFFECTS AND TOXICITY
 DRUG SIDE EFFECTS AND TOXICITY Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Objectives After participating in this lecture,
DRUG SIDE EFFECTS AND TOXICITY Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Objectives After participating in this lecture,
Standard TB Treatment
 Standard TB Treatment Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
Standard TB Treatment Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
Dana G. Kissner, MD Detroit Department of Health & Wellness Promotion Wayne State University
 Dana G. Kissner, MD Detroit Department of Health & Wellness Promotion Wayne State University I reply to those who urge me to take medicine that they should wait at least until I am restored to my strength
Dana G. Kissner, MD Detroit Department of Health & Wellness Promotion Wayne State University I reply to those who urge me to take medicine that they should wait at least until I am restored to my strength
Shu-Hua Wang, MD, MPH &TM Assistant Professor of Medicine The Ohio State University
 Shu-Hua Wang, MD, MPH &TM Assistant Professor of Medicine The Ohio State University For anti-tuberculosis medications: Describe clinical monitoring for adverse drug reactions Review specific drug side
Shu-Hua Wang, MD, MPH &TM Assistant Professor of Medicine The Ohio State University For anti-tuberculosis medications: Describe clinical monitoring for adverse drug reactions Review specific drug side
Peter Mere Latham English physician & educator
 Poisons and medicine are oftentimes the same substance given with different intents Dana G. Kissner, MD Detroit Department of Health & Wellness Promotion Wayne State University Peter Mere Latham 1789-1875
Poisons and medicine are oftentimes the same substance given with different intents Dana G. Kissner, MD Detroit Department of Health & Wellness Promotion Wayne State University Peter Mere Latham 1789-1875
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015
 Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 TB Medications and Adverse Drug Events Presented by Evelyn Drzymala, RN, BSN February 11, 2015 Evelyn Drzymala, RN, BSN has
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 TB Medications and Adverse Drug Events Presented by Evelyn Drzymala, RN, BSN February 11, 2015 Evelyn Drzymala, RN, BSN has
Treatment: First Line Drugs TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS TREATMENT: GENERAL PRINCIPLES MECHANISM OF ACTION MID 27
 TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS Treatment: First Line Drugs 1. ISONIAZID = INH Bacteriocidal against dividing organisms Dose = 300mg = one pill = well absorbed Good CNS penetration Can be
TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS Treatment: First Line Drugs 1. ISONIAZID = INH Bacteriocidal against dividing organisms Dose = 300mg = one pill = well absorbed Good CNS penetration Can be
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Antimycobacterial drugs. Dr.Naza M.Ali lec Dec 2018
 Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
Anti Tuberculosis Medications
 Anti Tuberculosis Medications Mary Ann Rodriguez, MD March 8, 2017 TB Nurse Case Management March 7 9, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Mary Ann Rodriguez, MD has the following disclosures
Anti Tuberculosis Medications Mary Ann Rodriguez, MD March 8, 2017 TB Nurse Case Management March 7 9, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Mary Ann Rodriguez, MD has the following disclosures
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Drugs David Griffith, MD August 13, 2014 David Griffith, MD has the following disclosures to make: No conflict
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Drugs David Griffith, MD August 13, 2014 David Griffith, MD has the following disclosures to make: No conflict
Official ATS/CDC/IDSA Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis (Nahid et al, CID 2016)
") Official ATS/CDC/IDSA Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis (Nahid et al, CID 2016) APPENDIX C: DRUGS IN CURRENT USE The U.S. Food and Drug Administration (FDA) has approved
Official ATS/CDC/IDSA Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis (Nahid et al, CID 2016) APPENDIX C: DRUGS IN CURRENT USE The U.S. Food and Drug Administration (FDA) has approved
Multiple Drug-resistant Tuberculosis: a Threat to Global - and Local - Public Health
 Multiple Drug-resistant Tuberculosis: a Threat to Global - and Local - Public Health C. Robert Horsburgh, Jr. Boston University School of Public Health Background Outline Why does drug resistance threaten
Multiple Drug-resistant Tuberculosis: a Threat to Global - and Local - Public Health C. Robert Horsburgh, Jr. Boston University School of Public Health Background Outline Why does drug resistance threaten
Treatment of Tuberculosis
 TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
6/8/2018 TB TREATMENT. Bijan Ghassemieh, MD Seattle TB Clinical Intensive Disclosures. None
 TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
Treatment of Active Tuberculosis
 Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Pediatric TB Intensive San Antonio, Texas October 14, 2013
 Pediatric TB Intensive San Antonio, Texas October 14, 2013 Treatment of Tuberculosis in Children Jeffrey R. Starke, M.D. Professor of Pediatrics October 14, 2013 Jeffrey R. Starke, M.D. has the following
Pediatric TB Intensive San Antonio, Texas October 14, 2013 Treatment of Tuberculosis in Children Jeffrey R. Starke, M.D. Professor of Pediatrics October 14, 2013 Jeffrey R. Starke, M.D. has the following
Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Iris Barrera, RN April 11, 2018
 Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Iris Barrera, RN April 11, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Iris Barrera,
Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Iris Barrera, RN April 11, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Iris Barrera,
TB Intensive San Antonio, Texas December 5-7, 2012
 TB Intensive San Antonio, Texas December 5-7, 2012 TB Drug Review David Griffith, MD Thursday December 6, 2012 David Griffith, MD has the following disclosures to make: No conflict of interest. No relevant
TB Intensive San Antonio, Texas December 5-7, 2012 TB Drug Review David Griffith, MD Thursday December 6, 2012 David Griffith, MD has the following disclosures to make: No conflict of interest. No relevant
Treatment and Monitoring
 Treatment and Monitoring Disclosures We have no actual or potential conflicts of interest in relation to this presentations. We have no financial relationships to disclose. Learning Objectives After this
Treatment and Monitoring Disclosures We have no actual or potential conflicts of interest in relation to this presentations. We have no financial relationships to disclose. Learning Objectives After this
Pharmacology and Pharmacokinetics of TB Drugs Part I
 Pharmacology and Pharmacokinetics of TB Drugs Part I Charles A. Peloquin, Pharm. D. Professor, and Director Infectious Disease Pharmacokinetics Laboratory College of Pharmacy and The Emerging Pathogens
Pharmacology and Pharmacokinetics of TB Drugs Part I Charles A. Peloquin, Pharm. D. Professor, and Director Infectious Disease Pharmacokinetics Laboratory College of Pharmacy and The Emerging Pathogens
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Managing Complex TB Cases Diana M. Nilsen, MD, RN
 Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric TB: Treatment of Tuberculosis Disease Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [with help from Andrea Cruz, M.D.] Objectives At the end
Advanced Concepts in Pediatric TB: Treatment of Tuberculosis Disease Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [with help from Andrea Cruz, M.D.] Objectives At the end
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Mitnick CD, Shin SS, Seung KJ, et al. Comprehensive treatment
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Mitnick CD, Shin SS, Seung KJ, et al. Comprehensive treatment
What is the recommended shorter treatment regimen for MDR-TB?
 DRTB STAT + TAG BRIEF Is shorter better? Is shorter better? Understanding the shorter regimen for treating drugresistant tuberculosis by Safiqa Khimani Edited by Vivian Cox, Mike Frick, Jennifer Furin,
DRTB STAT + TAG BRIEF Is shorter better? Is shorter better? Understanding the shorter regimen for treating drugresistant tuberculosis by Safiqa Khimani Edited by Vivian Cox, Mike Frick, Jennifer Furin,
Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist, NH GEISELMED.DARTMOUTH.EDU GEISELMED.DARTMOUTH.
 The image part with relationship ID rid2 was not found in the file. MDR TB Management Review of the Evolution (or Revolution?) Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist,
The image part with relationship ID rid2 was not found in the file. MDR TB Management Review of the Evolution (or Revolution?) Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist,
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 TB Drugs Part 1 & 2 Vanessa Meyer, PharmD November 12, 2014 Vanessa Meyer, PharmD has the following disclosures to make: No conflict of interests No
TB Intensive San Antonio, Texas November 11 14, 2014 TB Drugs Part 1 & 2 Vanessa Meyer, PharmD November 12, 2014 Vanessa Meyer, PharmD has the following disclosures to make: No conflict of interests No
Treatment of Tuberculosis
 Treatment of Tuberculosis, 1940 s Treatment of Tuberculosis ATS/CDC/IDSA Joint Statement 2003 Saskatchewan Lung Association Outline, 2012 Treatment of Tuberculosis Principles of treatment of tuberculosis
Treatment of Tuberculosis, 1940 s Treatment of Tuberculosis ATS/CDC/IDSA Joint Statement 2003 Saskatchewan Lung Association Outline, 2012 Treatment of Tuberculosis Principles of treatment of tuberculosis
HA Convention 2016 : Special Topic Session 3 May 2016
 HA Convention 2016 : Special Topic Session 3 May 2016 Diagnosis and Management of TB in Adults Dr. Thomas Mok COS(RMD), KH Tuberculosis An airborne infectious disease caused by Mycobacterium tuberculosis
HA Convention 2016 : Special Topic Session 3 May 2016 Diagnosis and Management of TB in Adults Dr. Thomas Mok COS(RMD), KH Tuberculosis An airborne infectious disease caused by Mycobacterium tuberculosis
5. HIV-positive individuals treated with INH should receive Pyridoxine (B6) 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH
 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH") V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
Venlafaxine hydrochloride extended-release and other antidepressant medicines may cause serious side effects, including:
 Medication Guide VENLAFAXINE XR (venlafaxine hydrochloride) (Extended-Release Capsules) Read the Medication Guide that comes with venlafaxine hydrochloride extended-release before you start taking it and
Medication Guide VENLAFAXINE XR (venlafaxine hydrochloride) (Extended-Release Capsules) Read the Medication Guide that comes with venlafaxine hydrochloride extended-release before you start taking it and
DR-TB Patient Treatment Log Book
 REPUBLIC OF KENYA MINISTRY OF HEALTH DR-TB Patient Treatment Log Book Patient Name: Patient Reg. No.: VERSION 2016 DR-TB treatment outcome summary Outcome Mark one Date Cured Died Failed Defaulted Transferred
REPUBLIC OF KENYA MINISTRY OF HEALTH DR-TB Patient Treatment Log Book Patient Name: Patient Reg. No.: VERSION 2016 DR-TB treatment outcome summary Outcome Mark one Date Cured Died Failed Defaulted Transferred
Antituberculous Agents
 Antituberculous Agents Primary or First Line Drugs: Isoniazid (INH) Rifampin Rifadin or Rimactane Ethambutal Streptomycin Pyrazinamide Isoniazid(INH) Most active. Small molecule, water soluble, Structurally
Antituberculous Agents Primary or First Line Drugs: Isoniazid (INH) Rifampin Rifadin or Rimactane Ethambutal Streptomycin Pyrazinamide Isoniazid(INH) Most active. Small molecule, water soluble, Structurally
Drug Resistant Tuberculosis Self-reporting of Drugrelated. During Treatment
 Drug Resistant Tuberculosis Self-reporting of Drugrelated Adverse Events During Treatment Introduction This information has been prepared for people with tuberculosis (TB) that is resistant to the commonly
Drug Resistant Tuberculosis Self-reporting of Drugrelated Adverse Events During Treatment Introduction This information has been prepared for people with tuberculosis (TB) that is resistant to the commonly
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015
 Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 Initiation Phase Part 1 Ginny Dowell, RN, BSN February 4, 2015 Ginny Dowell RN, BSN has the following disclosures to make:
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 Initiation Phase Part 1 Ginny Dowell, RN, BSN February 4, 2015 Ginny Dowell RN, BSN has the following disclosures to make:
CONCORD INTERNAL MEDICINE. Peripheral Neuropathy. April 22, 2012
 CONCORD INTERNAL MEDICINE Peripheral Neuropathy Douglas G. Kelling, Jr., MD C. Gismondi-Eagan, MD, FACP George C. Monroe, III, MD April 22, 2012 The information contained in this protocol should never
CONCORD INTERNAL MEDICINE Peripheral Neuropathy Douglas G. Kelling, Jr., MD C. Gismondi-Eagan, MD, FACP George C. Monroe, III, MD April 22, 2012 The information contained in this protocol should never
Update on Management of
 Update on Management of DR TB Definitions Presumptive MDR-TB A patient suspected of drug-resistant TB, based on RNTCP criteria for submission of specimens for drug-susceptibility testing MDR-TB Case A
Update on Management of DR TB Definitions Presumptive MDR-TB A patient suspected of drug-resistant TB, based on RNTCP criteria for submission of specimens for drug-susceptibility testing MDR-TB Case A
Elavil (amitriptyline)
") Generic name: Amitriptyline Available strengths: 10 mg, 25 mg, 50 mg, 75 mg, 100 mg, 150 mg tablets; 10 mg/ml injection Available in generic: Yes Drug class: Tricyclic antidepressant General Information
Generic name: Amitriptyline Available strengths: 10 mg, 25 mg, 50 mg, 75 mg, 100 mg, 150 mg tablets; 10 mg/ml injection Available in generic: Yes Drug class: Tricyclic antidepressant General Information
NURSING PROCESS FOCUS: Patients Receiving Amphotericin B (Fungizone, Abelcet)
") NURSING PROCESS FOCUS: Patients Receiving Amphotericin B (Fungizone, Abelcet) ASSESSMENT Prior to administration: Obtain complete health history including allergies, drug history, and possible drug interactions.
NURSING PROCESS FOCUS: Patients Receiving Amphotericin B (Fungizone, Abelcet) ASSESSMENT Prior to administration: Obtain complete health history including allergies, drug history, and possible drug interactions.
Marcos Burgos, MD has the following disclosures to make:
 Guidelines for the Treatment of Tuberculosis Marcos Burgos, MD May 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures
Guidelines for the Treatment of Tuberculosis Marcos Burgos, MD May 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures
Short Course Treatment for MDR TB
 Objectives Short Course Treatment for MDR TB Barbara J Seaworth M.D. Medical Director Heartland National TB Center Professor of Medicine, University of Texas Health Northeast Participants will utilize
Objectives Short Course Treatment for MDR TB Barbara J Seaworth M.D. Medical Director Heartland National TB Center Professor of Medicine, University of Texas Health Northeast Participants will utilize
Managing the Patients Response to TB Treatment
 Managing the Patients Response to TB Treatment Barbarah Martinez, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Barbarah Martinez, RN, BSN has
Managing the Patients Response to TB Treatment Barbarah Martinez, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Barbarah Martinez, RN, BSN has
New Drugs, New Treatments, Shorter Regimens
 New Drugs, New Treatments, Shorter Regimens Sarah K. Brode, MD MPH FRCP(C) West Park Healthcare Centre, University Health Network, University of Toronto TB Elimination: Back to Basics November 16, 2016
New Drugs, New Treatments, Shorter Regimens Sarah K. Brode, MD MPH FRCP(C) West Park Healthcare Centre, University Health Network, University of Toronto TB Elimination: Back to Basics November 16, 2016
Medication Fact Sheets
 5 Medication Fact Sheets 3rd edition contributors: GISELA F. SCHECTER, MD, MPH & CHARLES A. PELOQUIN, PharmD, FCCP Amikacin............... 100 Meropenem............ 130 Amoxicillin/clavulanate... 102 Moxifloxacin............
5 Medication Fact Sheets 3rd edition contributors: GISELA F. SCHECTER, MD, MPH & CHARLES A. PELOQUIN, PharmD, FCCP Amikacin............... 100 Meropenem............ 130 Amoxicillin/clavulanate... 102 Moxifloxacin............
Efavirenz, stavudine and lamivudine
 efavirenz, stavudine, lamivudine: 1 efavirenz, stavudine and lamivudine First line ART treatment for HIV infection Efavirenz, stavudine and lamivudine efavirenz, stavudine, lamivudine: 2 Slide 1 Information
efavirenz, stavudine, lamivudine: 1 efavirenz, stavudine and lamivudine First line ART treatment for HIV infection Efavirenz, stavudine and lamivudine efavirenz, stavudine, lamivudine: 2 Slide 1 Information
Nursing Process Focus: Patients Receiving Penicillin G (Pentids)
") Prior to administration Assess for presence or history of local or systemic infection. Patients Receiving Penicillin G (Pentids) Risk for Infection, related to weakened immune state or contact with pathogen
Prior to administration Assess for presence or history of local or systemic infection. Patients Receiving Penicillin G (Pentids) Risk for Infection, related to weakened immune state or contact with pathogen
Dosage and Administration
 SIRTURO product information for healthcare providers 2 WARNINGS: An increased risk of death was seen in the SIRTURO (bedaquiline) treatment group (9/79, 11.4%) compared to the placebo treatment group (2/81,
SIRTURO product information for healthcare providers 2 WARNINGS: An increased risk of death was seen in the SIRTURO (bedaquiline) treatment group (9/79, 11.4%) compared to the placebo treatment group (2/81,
TB: A Supplement to GP CLINICS
 TB: A Supplement to GP CLINICS Adverse Drug events With Anti Tuberculosis Therapy What Every GP Should Know Authors: Kavitha Saravu, MD, DNB, DTM&H; Madhukar Pai, MD, PhD Standards of TB Care in India
TB: A Supplement to GP CLINICS Adverse Drug events With Anti Tuberculosis Therapy What Every GP Should Know Authors: Kavitha Saravu, MD, DNB, DTM&H; Madhukar Pai, MD, PhD Standards of TB Care in India
Norpramin (desipramine)
") Generic name: Desipramine Available strengths: 10 mg, 25 mg, 50 mg, 75 mg, 100 mg, 150 mg tablets Available in generic: Yes Drug class: Tricyclic antidepressant General Information Norpramin (desipramine)
Generic name: Desipramine Available strengths: 10 mg, 25 mg, 50 mg, 75 mg, 100 mg, 150 mg tablets Available in generic: Yes Drug class: Tricyclic antidepressant General Information Norpramin (desipramine)
Patient Name: Date: Address: Primary Care Physician: Online Website On TV In print On the radio
 927 W. Myrtle St. Boise, ID 83702 (208) 947-0100 NEW PATIENT INTAKE Patient Name: Date: Email Address: Primary Care Physician: How did you hear about AVT? (Please mark all that apply) Online Website On
927 W. Myrtle St. Boise, ID 83702 (208) 947-0100 NEW PATIENT INTAKE Patient Name: Date: Email Address: Primary Care Physician: How did you hear about AVT? (Please mark all that apply) Online Website On
PACKAGING LEAFLET: INFORMATION FOR THE USER. Isoniazid Atb 300 mg tablets Isoniazid
 MARKETING AUTHORISATION NO: 1136/2008/01-02 Annex 1 Leaflet PACKAGING LEAFLET: INFORMATION FOR THE USER Isoniazid Atb 300 mg tablets Isoniazid Read all of this leaflet carefully before you start taking
MARKETING AUTHORISATION NO: 1136/2008/01-02 Annex 1 Leaflet PACKAGING LEAFLET: INFORMATION FOR THE USER Isoniazid Atb 300 mg tablets Isoniazid Read all of this leaflet carefully before you start taking
Fluoroquinolone-Associated Disability (FQAD) Cases in Patients Being Treated for Uncomplicated Sinusitis, Bronchitis, and/or Urinary Tract Infection
 Cases in Patients Being Treated for Uncomplicated Sinusitis, Bronchitis, and/or Urinary Tract Infection") Joint Meeting of the Antimicrobial Drugs Advisory Committee and the Drug Safety and Risk Management Advisory Committee November 5, 2015 FDA s Adverse Event Reporting System (FAERS) Review: Fluoroquinolone-Associated
Joint Meeting of the Antimicrobial Drugs Advisory Committee and the Drug Safety and Risk Management Advisory Committee November 5, 2015 FDA s Adverse Event Reporting System (FAERS) Review: Fluoroquinolone-Associated
PATIENT INFORMATION LEAFLET: INFORMATION FOR THE USER. Ethionamide 125 mg Dispersible Tablets 1
 PATIENT INFORMATION LEAFLET: INFORMATION FOR THE USER Ethionamide 125 mg Dispersible Tablets 1 Read all of this leaflet carefully before you start taking this medicine because it contains important information
PATIENT INFORMATION LEAFLET: INFORMATION FOR THE USER Ethionamide 125 mg Dispersible Tablets 1 Read all of this leaflet carefully before you start taking this medicine because it contains important information
Dexamethasone is used to treat cancer. This drug can be given in the vein (IV), by mouth, or as an eye drop.
, by mouth, or as an eye drop.") Dexamethasone Other Names: Decadron About This Drug Dexamethasone is used to treat cancer. This drug can be given in the vein (IV), by mouth, or as an eye drop. Possible Side Effects (More Common) Increased
Dexamethasone Other Names: Decadron About This Drug Dexamethasone is used to treat cancer. This drug can be given in the vein (IV), by mouth, or as an eye drop. Possible Side Effects (More Common) Increased
TB Drugs. Discuss the common route for transmission of the disease. Discusses the out line for treatment of tuberculosis.
 TB Drugs Red : important Black : in male / female slides Pink : in female s slides only Blue : in male s slides only Females doctor notes Grey: Males doctor notes OBJECTIVES: By the end of this lecture,
TB Drugs Red : important Black : in male / female slides Pink : in female s slides only Blue : in male s slides only Females doctor notes Grey: Males doctor notes OBJECTIVES: By the end of this lecture,
Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over)
") Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over) Introduction / Background Treatment comes after diagnosis Diagnosis is based on
Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over) Introduction / Background Treatment comes after diagnosis Diagnosis is based on
Neuropathic Pain Treatment Guidelines
 Neuropathic Pain Treatment Guidelines Background Pain is an unpleasant sensory and emotional experience that can have a significant impact on a person s quality of life, general health, psychological health,
Neuropathic Pain Treatment Guidelines Background Pain is an unpleasant sensory and emotional experience that can have a significant impact on a person s quality of life, general health, psychological health,
CENTRAL CARE POLICY SYMPTOMS OF ILLNESS. Policy: Consumers will be observed for symptoms of physical problems, distress, pain, or unusual behaviors.
 Page 1 of 5 CENTRAL CARE POLICY SYMPTOMS OF ILLNESS SUBJECT: SYMPTOMS OF ILLNESS ANNUAL REVIEW MONTH: June RESPONSIBLE FOR REVIEW: Director of Central Care LAST REVISION DATE: June 2009 Policy: Consumers
Page 1 of 5 CENTRAL CARE POLICY SYMPTOMS OF ILLNESS SUBJECT: SYMPTOMS OF ILLNESS ANNUAL REVIEW MONTH: June RESPONSIBLE FOR REVIEW: Director of Central Care LAST REVISION DATE: June 2009 Policy: Consumers
Azathioprine toxicity criteria and severity descriptors for the listing of biological agents for rheumatoid arthritis on the PBS
 Azathioprine toxicity criteria and severity descriptors for the listing of biological agents for rheumatoid arthritis on the PBS Only valid for adult patients Azathioprine must be at a dose of at least
Azathioprine toxicity criteria and severity descriptors for the listing of biological agents for rheumatoid arthritis on the PBS Only valid for adult patients Azathioprine must be at a dose of at least
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
LTBI in Special Populations John Nava, MD October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
MULTIDRUG- RESISTANT TUBERCULOSIS. Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic
 MULTIDRUG- RESISTANT TUBERCULOSIS Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic I have no relevant financial relationships. Discussion includes off label use of: amikacin
MULTIDRUG- RESISTANT TUBERCULOSIS Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic I have no relevant financial relationships. Discussion includes off label use of: amikacin
Pamelor (nortriptyline)
") Generic name: Nortriptyline Available strengths: 10 mg, 25 mg, 50 mg, 75 mg capsules; 10 mg/5 ml oral solution Available in generic: Yes Drug class: Tricyclic antidepressant General Information Pamelor
Generic name: Nortriptyline Available strengths: 10 mg, 25 mg, 50 mg, 75 mg capsules; 10 mg/5 ml oral solution Available in generic: Yes Drug class: Tricyclic antidepressant General Information Pamelor
(levomilnacipran) extended-release capsules
 extended-release capsules") MEDICATION GUIDE FETZIMA (fet-zee-muh) (levomilnacipran) extended-release capsules Read this Medication Guide before you start taking FETZIMA and each time you get a refill. There may be new information.
MEDICATION GUIDE FETZIMA (fet-zee-muh) (levomilnacipran) extended-release capsules Read this Medication Guide before you start taking FETZIMA and each time you get a refill. There may be new information.
Discussing TECENTRIQ (atezolizumab) with your healthcare team Talking to Your Doctor
 with your healthcare team Talking to Your Doctor") Discussing TECENTRIQ (atezolizumab) with your healthcare team Talking to Your Doctor TECENTRIQ DISCUSSION SUPPORT What is TECENTRIQ? TECENTRIQ is a prescription medicine used to treat: A type of bladder
Discussing TECENTRIQ (atezolizumab) with your healthcare team Talking to Your Doctor TECENTRIQ DISCUSSION SUPPORT What is TECENTRIQ? TECENTRIQ is a prescription medicine used to treat: A type of bladder
*Monitor for significant side effects, especially symptoms of neurological or cardiovascular events.
 Assessment Prior to administration: Obtain complete health history including allergies, drug history, and possible drug reactions Assess reason for drug administration such as presence/history of anemia
Assessment Prior to administration: Obtain complete health history including allergies, drug history, and possible drug reactions Assess reason for drug administration such as presence/history of anemia
Treatment of Tuberculosis
 Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
Methotrexate. About This Drug. Possible Side Effects. Warnings and Precautions
 Methotrexate About This Drug Methotrexate is used to treat cancer. This drug is given in the vein (IV). Possible Side Effects Soreness of the mouth and throat. You may have red areas, white patches, or
Methotrexate About This Drug Methotrexate is used to treat cancer. This drug is given in the vein (IV). Possible Side Effects Soreness of the mouth and throat. You may have red areas, white patches, or
Medication Guide SARAFEM (SAIR-a-fem) (fluoxetine hydrochloride) Tablets
 (fluoxetine hydrochloride) Tablets") Medication Guide SARAFEM (SAIR-a-fem) (fluoxetine hydrochloride) Tablets Read the Medication Guide that comes with SARAFEM before you start taking it and each time you get a refill. There may be new information.
Medication Guide SARAFEM (SAIR-a-fem) (fluoxetine hydrochloride) Tablets Read the Medication Guide that comes with SARAFEM before you start taking it and each time you get a refill. There may be new information.
New TB Medications. National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention
 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention New TB Medications Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers
National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention New TB Medications Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers
Disclosures. Outline. No disclosures or conflicts of interest to report. Special LTBI situations. H t it d id ff t
 Selected Topics in LTBI June 2, 2015 Bijan Ghassemieh, MD Senior Fellow UW Division of Pulmonary/Critical Care Disclosures No disclosures or conflicts of interest to report Outline Special LTBI situations
Selected Topics in LTBI June 2, 2015 Bijan Ghassemieh, MD Senior Fellow UW Division of Pulmonary/Critical Care Disclosures No disclosures or conflicts of interest to report Outline Special LTBI situations
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Zumla A, Raviglione M, Hafner R, von Reyn CF. Tuberculosis.
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Zumla A, Raviglione M, Hafner R, von Reyn CF. Tuberculosis.
VI.2 Elements for a Public Summary DULOXETINE Pharmalex 30 mg hard gastro-resistant capsules DULOXETINE Pharmalex 60 mg hard gastro-resistant capsules
 VI.2 Elements for a Public Summary DULOXETINE Pharmalex 30 mg hard gastro-resistant capsules DULOXETINE Pharmalex 60 mg hard gastro-resistant capsules VI.2.1 Overview of disease epidemiology Depression
VI.2 Elements for a Public Summary DULOXETINE Pharmalex 30 mg hard gastro-resistant capsules DULOXETINE Pharmalex 60 mg hard gastro-resistant capsules VI.2.1 Overview of disease epidemiology Depression
LTBI Videos-Treatment
 LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
Medication Guide Fluoxetine Oral Solution USP What is the most important information I should know about fluoxetine oral solution?
 Medication Guide Fluoxetine Oral Solution USP Read the Medication Guide that comes with fluoxetine before you start taking it and each time you get a refill. There may be new information. This Medication
Medication Guide Fluoxetine Oral Solution USP Read the Medication Guide that comes with fluoxetine before you start taking it and each time you get a refill. There may be new information. This Medication
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
Cisplatin / Paclitaxel Gynaecological Cancer
 Systemic Anti Cancer Treatment Protocol Cisplatin / Paclitaxel Gynaecological Cancer PROCTOCOL REF: MPHAGYNCIP (Version No: 1.0) Approved for use in: First line treatment for stage Ib-IV with minimal residual
Systemic Anti Cancer Treatment Protocol Cisplatin / Paclitaxel Gynaecological Cancer PROCTOCOL REF: MPHAGYNCIP (Version No: 1.0) Approved for use in: First line treatment for stage Ib-IV with minimal residual
Overcoming the Challenges in Access to TB Drugs for Children
 Overcoming the Challenges in Access to TB Drugs for Children Gregory L. Kearns, PharmD, PhD Professor of Pediatrics and Pharmacology, University of Missouri Marion Merrell Dow / Missouri Chair in Pediatric
Overcoming the Challenges in Access to TB Drugs for Children Gregory L. Kearns, PharmD, PhD Professor of Pediatrics and Pharmacology, University of Missouri Marion Merrell Dow / Missouri Chair in Pediatric
PREMEDICATIONS: Antiemetic protocol for highly emetogenic chemotherapy. May not need any antiemetic with
 BCCA Protocol Summary for Palliative Therapy of Metastatic or Locally Advanced Gastric, Gastroesophageal Junction Adenocarcinoma, Esophageal Squamous Cell Carcinoma, or Anal Squamous Cell Carcinoma using
BCCA Protocol Summary for Palliative Therapy of Metastatic or Locally Advanced Gastric, Gastroesophageal Junction Adenocarcinoma, Esophageal Squamous Cell Carcinoma, or Anal Squamous Cell Carcinoma using
Elements for a public summary. VI.2.1 Overview of disease epidemiology
 VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Nosocomial pneumonia (NP): NP (hospital acquired pneumonia) is most common in elderly patients; however, patients of any age may
VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Nosocomial pneumonia (NP): NP (hospital acquired pneumonia) is most common in elderly patients; however, patients of any age may
Headache Follow-up Visit Form
 !1 Headache Follow-up Visit Form We will be unable to see you unless this form is completely filled out. We appreciate your thoroughness. Name DOB Age Today s Date Referring doctor: Primary doctor: Neurologist:
!1 Headache Follow-up Visit Form We will be unable to see you unless this form is completely filled out. We appreciate your thoroughness. Name DOB Age Today s Date Referring doctor: Primary doctor: Neurologist:
WARNING: TENDON EFFECTS and EXACERBATION OF MYASTHENIA GRAVIS
 DECLESAU (dergrafloxacin) tablets, for oral use DECLESAU (dergrafloxacin) injection, solution for intravenous use WARNING: TENDON EFFECTS and EXACERBATION OF MYASTHENIA GRAVIS Fluoroquinolones, including
DECLESAU (dergrafloxacin) tablets, for oral use DECLESAU (dergrafloxacin) injection, solution for intravenous use WARNING: TENDON EFFECTS and EXACERBATION OF MYASTHENIA GRAVIS Fluoroquinolones, including
New Patient Pain Evaluation
 New Patient Pain Evaluation Name: Date: Using the following symbols, mark the areas of the body diagrams which are affected by your pain: \\ = Stabbing * = Electrical X = Aching N = Numbness 0 = Dull S
New Patient Pain Evaluation Name: Date: Using the following symbols, mark the areas of the body diagrams which are affected by your pain: \\ = Stabbing * = Electrical X = Aching N = Numbness 0 = Dull S
Management of Multidrug- Resistant TB in Children. Jennifer Furin, MD., PhD. Sentinel Project, Director of Capacity Building
 Management of Multidrug- Resistant TB in Children Jennifer Furin, MD., PhD. Sentinel Project, Director of Capacity Building Objectives To review data on best practices for diagnosis, treatment and prevention
Management of Multidrug- Resistant TB in Children Jennifer Furin, MD., PhD. Sentinel Project, Director of Capacity Building Objectives To review data on best practices for diagnosis, treatment and prevention