NonConvulsive Seizure
|
|
|
- Elmer Sims
- 6 years ago
- Views:
Transcription
1 Sample Protocol #5: Management of status epilepticus and seizures in hospitalized patients nconvulsive Seizure Patient presents with alteration of consciousness unexplained by other etiologies AND suspicious for non convulsive seizure OR subclinical seizures noted on EEG ABCs Finger stick glucose Labs: CBC w/ Diff, CMP, Urine Drug Screen, Urine Pregnancy Test If KNOWN epilepsy, order antiseizure medication levels IF UNKNOWN, order Magnesium and Phosphate Seizures Terminate Patient back to baseline in minutes? Administer meds. Is there IV access? Order neurology consult Ativan (Lorazepam): 1-2 mg IV per dose, may repeat in 5 mins, up to 0.1 mg/kg, if not controlled after 2 doses, move on 0.2 mg/kg IM or IV up to max of 10mg Order Continuous EEG Order n-contrast Head CT If imaging reveals lesion, order neurosurgery consult Seizures Persist? PRE Status Epilepticus Page 1
2 nconvulsive Seizure First round of medication does not cease seizures: PRE Status Epilepticus PREFERRED unless patient meets any criteria below PREGNANCY OR SEVERE LIVER DISEASE EEG or clinical exam suggestive of MYOCLONIC SEIZURES Pt in ICU, PACU, or INTUBATED Administer Meds: CHOOSE ONE Fosphenytoin: 20mg PE/kg IV initial bolus. Complete initial bolus. If clinical or electrographic seizures persist, may give add l 5mg/kg. Rate of up to 150mg PE/min. Levetiracetam (Keppra): 1,000-3,000 mg IV, at rate of 2.5 mg/kg/min IV Valproate Sodium (Depakote): mg/kg IV, may give add l 20mg/kg, up to 3-6 mg/ kg/min Initial dose of 0.2 mg/kg; administer at infusion rate of 2mg/min; followed by continuous infusion of 0.05mg/ kg/hr. Titrate to max tolerated dose. Consider ICU transfer Close monitoring of airway - Readiness to intubate Consider LP if clinically indicated If not already ordered: Order neurology consult Order Continuous EEG Seizures Persist? Consider trying another second line agent. (ONLY REPEAT ONCE) Status Epilepticus Seizures Terminate Page 2
3 nconvulsive Seizure PREFERRED unless patient meets any criteria below Administer Meds: CHOOSE ONE Fosphenytoin: 20mg PE/kg IV initial bolus. Complete initial bolus. If clinical or electrographic seizures persist, may give add l 5mg/kg. Rate of up to 150mg PE/min. PREGNANCY OR SEVERE LIVER DISEASE EEG or clinical exam suggestive of MYOCLONIC SEIZURES Pt in ICU, PACU, or INTUBATED Levetiracetam (Keppra): 1,000-3,000 mg IV, at rate of 2.5 mg/kg/min IV Valproate Sodium (Depakote): mg/kg IV, may give add l 20mg/kg, up to 3-6 mg/kg/min Initial dose of 0.2 mg/kg; administer at infusion rate of 2mg/min; followed by continuous infusion of 0.05mg/ kg/hr. Titrate to max tolerated dose. Return to Pathway Page 3
4 nconvulsive Seizure Status Epilepticus Transfer to ICU with ceeg monitoring. Contraindication to intubation? Consider intermittent bolus therapies of valproic acid, leviteracitam, or fosphenytoin. Intubate and consider need for pressors. Administer Meds: CHOOSE ONE Treatment involves continuous infusions. Goal is to titrate to seizure suppression for 48 hrs. If seizures persist, goal is to titrate to burst suppression for 48 hrs. PREFERRED Initial dose of 0.2 mg/kg; administer at infusion rate of 2mg/min; followed by infusion of mg/kg/hr Cl. If all other therapies fail, consider lacosamide (Vimpat). Lacosamide: 200 mg IV with maintenance of 100 mg q12. Second Choice Third Choice Propofol: Start at 20 mcg/kg/min with 1-2 mg/kg loading dose mcg/kg/min Cl. Propofol infusion rate = mcg/kg/min CI. Use caution when administering high doses (>80 mcg/kg/ min) for extended periods of time (i.e., >48 h) Pentobartbital: 5-15 mg/kg, may give add l 5-10 mg/kg: administer at infusion rate of <50 mg/min mg/kg/h Cl. Consult epileptologist. Seizures Persist? Refractory Status Consider Seizure Protocol MRI to be ordered by neuro or epileptlogist. Treatment management with assistance from neuro consult and epileptologist. Consider neurosurgery consult. Maintenance anti-seizure medications: Phenytoin, Levetiracetam, Valproate, Lacosamide, Clonazepam, Phenobarbital, Topiramate, Zonisamide, Carbamazepine, Oxcarbazepine Initiation of maintenance anti-seizure medication. Selection guided by epileptologist. Consider weaning infusion anti-seizure medications/anesthetic agents if seizure free hours. Continue ceeg for hours once IV antiseizure medication/anesthetic agents infusions weaned and patient remains seizure free Transfer out of ICU per ICU transfer criteria Within 3-4 wks Follow up in Neurology Clinic with Epileptologist Page 4
5 nconvulsive Seizure Administer Meds: CHOOSE ONE Treatment involves continuous infusions. Goal is to titrate to seizure suppression for 48 hrs. If seizures persist, goal is to titrate to burst suppression for 48 hrs. PREFERRED Second Choice Third Choice Initial dose of 0.2 mg/kg; administer at infusion rate of 2mg/min; followed by infusion of mg/kg/hr Cl. Propofol: Start at 20 mcg/kg/min with 1-2 mg/kg loading dose mcg/kg/min Cl. Propofol infusion rate = mcg/kg/min CI. Use caution when administering high doses (>80 mcg/kg/ min) for extended periods of time (i.e., >48 h) Pentobartbital: 5-15 mg/kg, may give add l 5-10 mg/kg: administer at infusion rate of <50 mg/min mg/kg/h Cl. Return to Pathway Page 5
6 nconvulsive Seizure Initiation of maintenance anti-seizure medication. Selection guided by epileptologist. Consider weaning infusion anti-seizure medications/ anesthetic agents if seizure free hours. Continue ceeg for hours once IV anti-seizure medication/anesthetic agents infusions weaned and patient remains seizure free Return to Pathway Page 6
7 nconvulsive Seizure Seizures Terminate If patient on ceeg, continue for hours once patient remains seizure free. Return to Previous Page Known Epilepsy? Order Routine EEG if not already performed. Back to baseline? Order non-contrast head CT (within 2 hours) if not already ordered. Consider LP if concern for CNS infection. Assess for infection or stressors. Consider LP if concern for CNS infection. If imaging reveals lesion, order neurosurgery consult Consider head CT if concern for head injury, focal neurological examination, or prolonged alteration in mental status. Engage Social Work Treat underlying cause. Is risk of recurrent seizure high? Maintenance anti-seizure medications: Phenytoin, Levetiracetam, Valproate, Phenobarbital, Topiramate, Zonisamide, Carbamazepine, Oxcarbazepine Consider beginning or adjustment of maintenance antiseizure medication Patient ready for discharge once all acute medical needs are met Within 4 wks Follow up in Neurology Clinic. If second line agent given, recommend follow-up with epileptologist. Page 7
8 nconvulsive Seizure If patient on ceeg, continue for hours once patient remains seizure free. Return to Pathway Page 8
9 Where did the patient come from? Convulsive Seizure Patient Presents with Convulsive Seizure Is this a convulsive seizure? Check allergies Is finger stick glucose abnormal? Treat appropriately Consider Thiamine Do you know the time of presentation? Was the patient given any antiseizure medications? Assess and treat for injuries from the seizure Order non-contrast head CT (within 2 hours). Order Labs: CMP, CBC, Tox Screen, Mg, Phosphate, Urine Pregnancy Test Consider LP Did imaging reveal potential surgical lesion? Order neurosurgery consult Seizures cease within 5 minutes? Known Epilepsy? Order AED Levels. Assess for infection or stressors. Assess and treat for injuries from seizure Greater than 5 Minutes Back to baseline? Consider n- Convulsive Seizure AED levels w/in normal limits? Order Routine EEG Back to Baseline Order Urgent EEG Consider Labs: CMP, CBC, Tox Screen, Urine Pregnancy Test. Consider LP and Imaging Order Labs: CMP, CBC, Tox Screen, Urine Pregnancy Test. Consider LP and Imaging nconvulsive pathway Are there seizures on the EEG? Engage Social Work Treat underlying cause, if determined Is risk of recurrent seizure high? Consider beginning or adjustment of maintenance AED Maintenance AEDs: Phenytoin, Levetiracetam, Valproate, Phenobarbital, Topiramate, Zonisamide, Carbamazepine, Oxcarbazepine Patient ready for discharge once all acute medical needs are met Within 4 wks Follow up in Neurology Clinic
10 Must treat acutely with 1 st line anti-seizure meds Convulsive Seizure Seizure persists for >5 min Lorazepam: 2-4mg IV per dose, may repeat in 5 mins, up to 0.1 mg/kg, if not controlled after 2 doses, move on Is there IV access? 0.2 mg/kg IM or IV up to max of 10mg Imaging: Order non-contrast head CT, (within 2 hours) if not already ordered Labs: CMP, CBC, Tox Screen, Mg, Phosphate, Urine Pregnancy Test, AED Levels, if not already ordered. Strongly consider LP EEG Routine: Pt back to baseline Urgent: if altered mental status greater than 30 minutes post convulsions Assess for injuries Perform neurological exam Assess for provoking factors Order Imaging, labs, EEG Seizures Persist? Known Epilepsy? Order AED Levels. Assess for infection, stressors, injuries. PENDING Status Epilepticus Consider neuro consult. If imaging reveals lesion, order neurosurgery consult Consider Labs: CMP, CBC, Tox Screen, Urine Pregnancy Test. Consider LP and Imaging AED levels w/in normal limits? Order Labs: CMP, CBC, Tox Screen, Urine Pregnancy Test. Consider LP and Imaging Engage social work Maintenance AEDs: Phenytoin, Levetiracetam, Valproate, Phenobarbital, Topiramate, Zonisamide, Carbamazepine, Oxcarbazepine Begin or alter maintenance AED, further treatment at discretion of neurology consult and primary service Patient ready for discharge once all acute medical needs are met Within 4 weeks Follow up in Neurology Clinic
11 Convulsive Seizure First line of medication does not cease seizures: PENDING Status Epilepticus Does the patient have severe liver disease or are they pregnant? YES Levetiracetam: 1,000-3,000 mg IV, at rate of 2.5 mg/kg/ min IV Order Neurology Consult Order Continuous EEG Does the EEG or clinical exam suggest myoclonic seizures? YES Valproate Sodium: mg/kg IV, may give add l 20mg/kg, up to 3-6 mg/kg/min Consider ICU transfer if: - vitals unstable Is the patient already in the ICU, PACU, or intubated? YES Initial dose of 0.2 mg/kg; administer at infusion rate of 2mg/min; followed by continuous infusion of 0.05mg/ kg/hr. Titrate to max tolerated dose. Fosphenytoin: 20mg PE/kg IV initial bolus. Complete initial bolus. If clinical or electrographic seizures persist, may give add l 5mg/kg. Rate of up to 150mg PE/min. (cont ) Check with pharmacy Monitor heart rate Be aware of risk of bradycardia, heart block, and hypertension Seizures Persist? Status Epilepticus Maintenance AEDs: Phenytoin, Levetiracetam, Valproate, Phenobarbital, Topiramate, Zonisamide, Carbamazepine, Oxcarbazepine Treat Underlying Cause Begin or alter maintenance AED per neurologist recommendation If continuous EEG not yet performed, change order to Stat EEG Patient ready for discharge once all acute medical needs are met Within 4 wks Follow up in Neurology Clinic
12 Convulsive Seizure Status Epilepticus Transfer to ICU with ceeg monitoring. Is there a strong clinical reason to avoid intubation? Intubate and consider need for pressors Consider intermittent bolus therapies of valproic acid, leviteracitam, or fosphenytoin. Propofol infusion rate = mcg/ kg/min CI. Use caution when administering high doses (>80 mcg/kg/ min) for extended periods of time (i.e., >48 h) Initial dose of 0.2 mg/kg; administer at infusion rate of 2mg/min; followed by infusion of mg/kg/hr Cl. Preferred Propofol: Start at 20 mcg/kg/ min with 1-2 mg/kg loading dose mcg/kg/min Cl. Administer continuous infusion of 3 rd line meds: Choose One Pentobartbital: 5-15 mg/kg, may give add l 5-10 mg/ kg: administer at infusion rate of <50 mg/min mg/ kg/h Cl. If all other therapies fail, consider lacosamide. Lacosamide: 200 mg IV with maintenance of 100 mg q12. Consider Seizure Protocol MRI to be ordered by neuro or epileptlogist. Treatment management with assistance from neuro consult and epileptologist. Consider neurosurgery consult. Consult epileptologist. Titrate to continuous infusion of 3 rd line agent to seizure suppression based on ceeg or clinical exam for 48 hrs Refractory Status Seizures Persist? Consider weaning infusion of third line meds Have you weaned the continuous infusion of 3 rd line meds? Maintain continuous infusion while initiating maintenance AED If seizures persist, goal is to titrate to burst suppression for 48 hrs Maintenance AEDs: Phenytoin, Levetiracetam, Valproate, Lacosamide, Clonazepam, Phenobarbital, Topiramate, Zonisamide, Carbamazepine, Oxcarbazepine Has patient been seizure free for 24-48hrs? Has the patient been seizure free for 24-48hr after stopping infusion of 3 rd line meds? Transfer out of ICU per ICU transfer criteria & continue maint AED Within 3-4 wks Stop the ceeg Follow up in epilepsy clinic
13
14
Refractory Seizures. Dr James Edwards EMCORE May 30th 2014
 Refractory Seizures Dr James Edwards EMCORE May 30th 2014 Refractory Seizures Seizures are a common presentation to the ED and some patients will have multiple seizures or have a reduced level of consciousness
Refractory Seizures Dr James Edwards EMCORE May 30th 2014 Refractory Seizures Seizures are a common presentation to the ED and some patients will have multiple seizures or have a reduced level of consciousness
Status Epilepticus: Implications Outside the Neuro-ICU
 Status Epilepticus: Implications Outside the Neuro-ICU Jeffrey M Singh MD Critical Care and Neurocritical Care Toronto Western Hospital October 31 st, 2014 Disclosures I (unfortunately) have no disclosures
Status Epilepticus: Implications Outside the Neuro-ICU Jeffrey M Singh MD Critical Care and Neurocritical Care Toronto Western Hospital October 31 st, 2014 Disclosures I (unfortunately) have no disclosures
Refractory Status Epilepticus in Children: What are the Options?
 Refractory Status Epilepticus in Children: What are the Options? Weng Man Lam, PharmD, BCPS, BCPPS PICU Clinical Pharmacy Specialist Memorial Hermann Texas Medical Center November 11, 2017 Objectives 1.
Refractory Status Epilepticus in Children: What are the Options? Weng Man Lam, PharmD, BCPS, BCPPS PICU Clinical Pharmacy Specialist Memorial Hermann Texas Medical Center November 11, 2017 Objectives 1.
Prescribing and Monitoring Anti-Epileptic Drugs
 Prescribing and Monitoring Anti-Epileptic Drugs Mark Granner, MD Clinical Professor and Vice Chair for Clinical Programs Director, Iowa Comprehensive Epilepsy Program Department of Neurology University
Prescribing and Monitoring Anti-Epileptic Drugs Mark Granner, MD Clinical Professor and Vice Chair for Clinical Programs Director, Iowa Comprehensive Epilepsy Program Department of Neurology University
Epilepsy CASE 1 Localization Differential Diagnosis
 2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
2016 Treatment Algorithm for Generalized Convulsive Status Epilepticus (SE) in adults and children > 40 kg
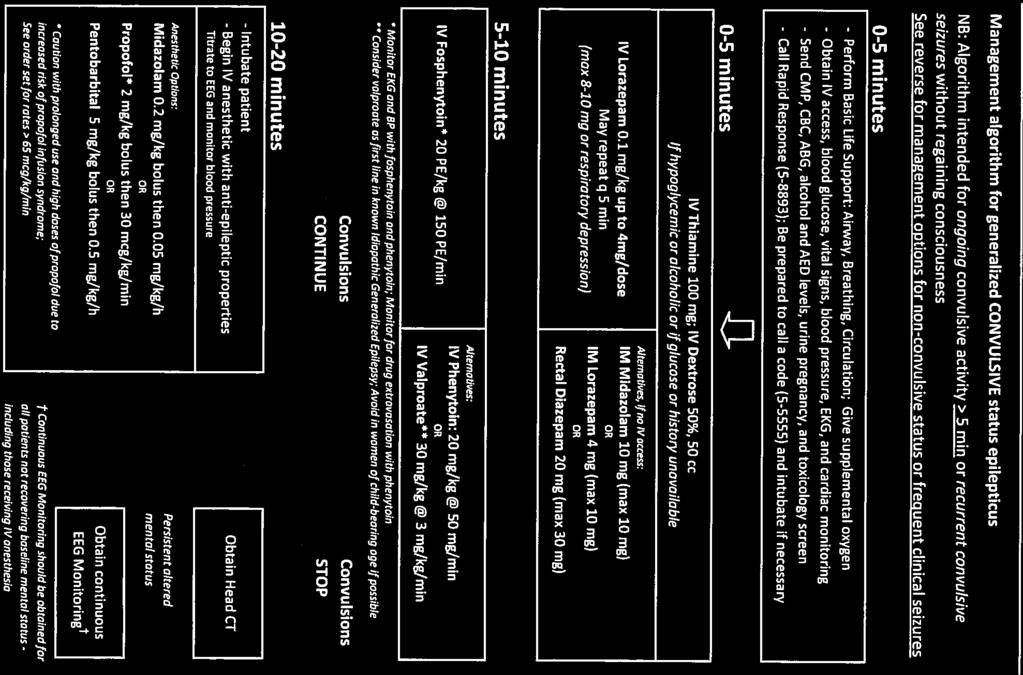
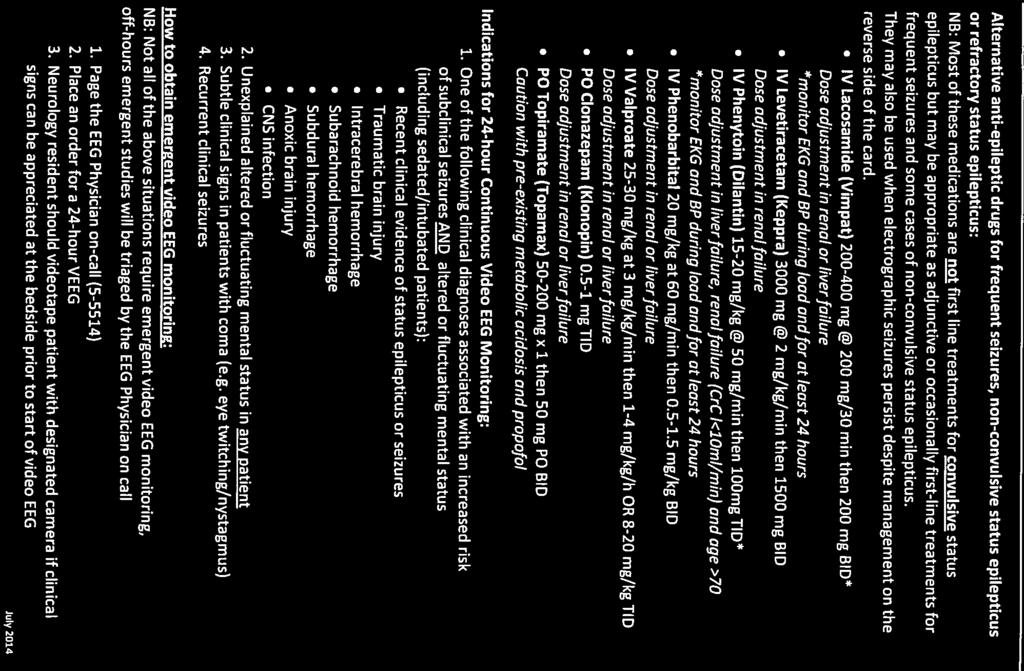
 in adults and children > 40 kg") Yale New Haven Health Department of Pharmacy, Department of Neurology 2016 Treatment Algorithm for Generalized Convulsive Status Epilepticus (SE) in adults and children > 40 kg Guideline, YNHHS Original
Yale New Haven Health Department of Pharmacy, Department of Neurology 2016 Treatment Algorithm for Generalized Convulsive Status Epilepticus (SE) in adults and children > 40 kg Guideline, YNHHS Original
APPENDIX K Pharmacological Management
 1 2 3 4 APPENDIX K Pharmacological Management Table 1 AED options by seizure type Table 1 AED options by seizure type Seizure type First-line AEDs Adjunctive AEDs Generalised tonic clonic Lamotrigine Oxcarbazepine
1 2 3 4 APPENDIX K Pharmacological Management Table 1 AED options by seizure type Table 1 AED options by seizure type Seizure type First-line AEDs Adjunctive AEDs Generalised tonic clonic Lamotrigine Oxcarbazepine
Management of Neonatal Seizures
 Management of Neonatal Seizures Manal E. Moustafa Assistant Professor of Pediatric Neurology and Epilepsy Children s Healthcare of Atlanta/Emory University Disclosures I have none! 1 Objectives Recognition
Management of Neonatal Seizures Manal E. Moustafa Assistant Professor of Pediatric Neurology and Epilepsy Children s Healthcare of Atlanta/Emory University Disclosures I have none! 1 Objectives Recognition
WHOLE LOTTA SHAKIN GOIN ON
 WHOLE LOTTA SHAKIN GOIN ON ADAM M. YATES, MD FACEP ASSOCIATE CHIEF OF EMERGENCY SERVICES UPMC MERCY SEIZURE DEFINITIONS Partial(focal) only involves part of the brain General Involves entire brain Simple
WHOLE LOTTA SHAKIN GOIN ON ADAM M. YATES, MD FACEP ASSOCIATE CHIEF OF EMERGENCY SERVICES UPMC MERCY SEIZURE DEFINITIONS Partial(focal) only involves part of the brain General Involves entire brain Simple
Outline. What is a seizure? What is epilepsy? Updates in Seizure Management Terminology, Triage & Treatment
 Outline Updates in Seizure Management Terminology, Triage & Treatment Joseph Sullivan, MD! Terminology! Videos of different types of seizures! Diagnostic evaluation! Treatment options! Acute! Maintenance
Outline Updates in Seizure Management Terminology, Triage & Treatment Joseph Sullivan, MD! Terminology! Videos of different types of seizures! Diagnostic evaluation! Treatment options! Acute! Maintenance
Status Epilepticus And Prolonged Seizures: Guideline For Management In Adults. Contents
 Status Epilepticus And Prolonged Seizures: Guideline For Management In Adults Classification: Clinical guideline Lead Author: Rajiv Mohanraj, Consultant Neurologist Additional author(s): Matt Jones, Consultant
Status Epilepticus And Prolonged Seizures: Guideline For Management In Adults Classification: Clinical guideline Lead Author: Rajiv Mohanraj, Consultant Neurologist Additional author(s): Matt Jones, Consultant
Status Epilepticus. Ednea Simon, MD Swedish Pediatric Neuroscience Center
 Status Epilepticus Ednea Simon, MD Swedish Pediatric Neuroscience Center 1 Status Epilepticus Status epilepticus (SE) is a condition resulting either from failure of the mechanisms responsible for seizure
Status Epilepticus Ednea Simon, MD Swedish Pediatric Neuroscience Center 1 Status Epilepticus Status epilepticus (SE) is a condition resulting either from failure of the mechanisms responsible for seizure
CrackCast Episode 18 Seizures
 CrackCast Episode 18 Seizures Episode overview: 1) Define status epilepticus 2) List the doses of common medications used for status epilepticus 3) List 10 differential diagnoses for seizures 4) List 10
CrackCast Episode 18 Seizures Episode overview: 1) Define status epilepticus 2) List the doses of common medications used for status epilepticus 3) List 10 differential diagnoses for seizures 4) List 10
Guideline of status epilepticus management 2017
 Guideline of status epilepticus management 2017 Kanitpong Phabphal Professor of Neurology Guideline 1966 to Jan 2005 European Foundation Neurology Society 2010 Hong Kong Epilepsy Society Society 2017 Published
Guideline of status epilepticus management 2017 Kanitpong Phabphal Professor of Neurology Guideline 1966 to Jan 2005 European Foundation Neurology Society 2010 Hong Kong Epilepsy Society Society 2017 Published
Status Epilepticus: A refresher. Objectives
 Status Epilepticus: A refresher Ruben D. Villanueva, Pharm.D., BCPS OU Medical Center Trauma ICU Pharmacist Objectives Define seizures, convulsive and non convulsive status epilepticus, and refractory
Status Epilepticus: A refresher Ruben D. Villanueva, Pharm.D., BCPS OU Medical Center Trauma ICU Pharmacist Objectives Define seizures, convulsive and non convulsive status epilepticus, and refractory
Epilepsy the Essentials
 INSTITUTE OF NEUROLOGY DCEE / NSE Epilepsy the Essentials Fergus Rugg-Gunn Consultant Neurologist Dept of Clinical and Experimental Epilepsy Institute of Neurology, University College London Epilepsy Society
INSTITUTE OF NEUROLOGY DCEE / NSE Epilepsy the Essentials Fergus Rugg-Gunn Consultant Neurologist Dept of Clinical and Experimental Epilepsy Institute of Neurology, University College London Epilepsy Society
CHAIR SUMMIT 7TH ANNUAL #CHAIR2014. Master Class for Neuroscience Professional Development. September 11 13, Westin Tampa Harbour Island
 #CHAIR2014 7TH ANNUAL CHAIR SUMMIT Master Class for Neuroscience Professional Development September 11 13, 2014 Westin Tampa Harbour Island Sponsored by #CHAIR2014 Clinical Case Challenge: Seizure Emergency
#CHAIR2014 7TH ANNUAL CHAIR SUMMIT Master Class for Neuroscience Professional Development September 11 13, 2014 Westin Tampa Harbour Island Sponsored by #CHAIR2014 Clinical Case Challenge: Seizure Emergency
Talk outline. Some definitions. Emergency epilepsy now what? Recognising seizure types. Dr Richard Perry. Management of status epilepticus
 Emergency epilepsy now what? Dr Richard Perry Imperial College NHS Trust Imperial College Talk outline Recognising seizure types Management of status epilepticus Some definitions Epileptic seizure A clinical
Emergency epilepsy now what? Dr Richard Perry Imperial College NHS Trust Imperial College Talk outline Recognising seizure types Management of status epilepticus Some definitions Epileptic seizure A clinical
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Absence seizures, 6 in childhood, 95 Adults, seizures and status epilepticus in, management of, 34 35 with first-time seizures. See Seizure(s),
Index Note: Page numbers of article titles are in boldface type. A Absence seizures, 6 in childhood, 95 Adults, seizures and status epilepticus in, management of, 34 35 with first-time seizures. See Seizure(s),
11/1/2018 STATUS EPILEPTICUS DISCLOSURE SPEAKER FOR SUNOVION AND UCB PHARMACEUTICALS. November is National Epilepsy Awareness Month
 STATUS EPILEPTICUS ALBERTO PINZON, MD, MSBE, PhD November is National Epilepsy Awareness Month DISCLOSURE SPEAKER FOR SUNOVION AND UCB PHARMACEUTICALS 1 SEIZURE A transient occurrence of signs and/or symptoms
STATUS EPILEPTICUS ALBERTO PINZON, MD, MSBE, PhD November is National Epilepsy Awareness Month DISCLOSURE SPEAKER FOR SUNOVION AND UCB PHARMACEUTICALS 1 SEIZURE A transient occurrence of signs and/or symptoms
8/27/2017. Super-Refractory Status Epilepticus 2014 Pediatric Chula Experience. Definition SE. Definition SE. Epidemiology CSE. Classification of SE
 Super-Refractory Status Epilepticus 2014 Pediatric Chula Experience Definition SE Traditional : Prolonged seizure lasting 30 mins or series of seizure without full recovery to baseline lasting 30 mins
Super-Refractory Status Epilepticus 2014 Pediatric Chula Experience Definition SE Traditional : Prolonged seizure lasting 30 mins or series of seizure without full recovery to baseline lasting 30 mins
Management of Epilepsy In Primary Care Practice. Video Examples. Talk Like a Neurologist: Seizure Types
 Management of Epilepsy In Primary Care Practice S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Vice Chairman, Department of Neurology Director,
Management of Epilepsy In Primary Care Practice S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Vice Chairman, Department of Neurology Director,
David Dredge, MD MGH Child Neurology CME Course September 9, 2017
 David Dredge, MD MGH Child Neurology CME Course September 9, 2017 } 25-40,000 children experience their first nonfebrile seizure each year } AAN/CNS guidelines developed in early 2000s and subsequently
David Dredge, MD MGH Child Neurology CME Course September 9, 2017 } 25-40,000 children experience their first nonfebrile seizure each year } AAN/CNS guidelines developed in early 2000s and subsequently
Status Epilepticus in Children. Azhar Daoud Professor of Child Neurology Jordan Univ of science and Tech
 Status Epilepticus in Children Azhar Daoud Professor of Child Neurology Jordan Univ of science and Tech Status epilepticus (SE) presents in a multitude of forms, dependent on etiology and patient age
Status Epilepticus in Children Azhar Daoud Professor of Child Neurology Jordan Univ of science and Tech Status epilepticus (SE) presents in a multitude of forms, dependent on etiology and patient age
Management of Seizures and Status Epilepticus. Emergent ICP Management
 Management of Seizures and Status Epilepticus S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department of
Management of Seizures and Status Epilepticus S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department of
Guidelines for the Evaluation and Management of Status Epilepticus
 Guidelines for the Evaluation and Management of Status Epilepticus Gretchen M. Brophy, Rodney Bell, Jan Claassen, Brian Alldredge, Thomas P. Bleck, Tracy Glauser, Suzette M. LaRoche, James J. Riviello,
Guidelines for the Evaluation and Management of Status Epilepticus Gretchen M. Brophy, Rodney Bell, Jan Claassen, Brian Alldredge, Thomas P. Bleck, Tracy Glauser, Suzette M. LaRoche, James J. Riviello,
Can t Stop the Seizing!
 Can t Stop the Seizing! Joseph Miller, MD, MS MCEP Critical Care March, 2019 Objectives Describe the importance of time to treatment Delineate treatment based on best evidence Describe novel diagnostic
Can t Stop the Seizing! Joseph Miller, MD, MS MCEP Critical Care March, 2019 Objectives Describe the importance of time to treatment Delineate treatment based on best evidence Describe novel diagnostic
Lieven Lagae Department of Paediatric Neurology Leuven University Leuven, Belgium. Management of acute seizure settings from infancy to adolescence
 Lieven Lagae Department of Paediatric Neurology Leuven University Leuven, Belgium Management of acute seizure settings from infancy to adolescence Consequences of prolonged seizures Acute morbidity and
Lieven Lagae Department of Paediatric Neurology Leuven University Leuven, Belgium Management of acute seizure settings from infancy to adolescence Consequences of prolonged seizures Acute morbidity and
Anesthesiology Practice & Seizures
 Anesthesiology Practice & Seizures Barbara Van de Wiele MD Clinical Professor, Vice Chair & Director Neurosurgical Anesthesiology UCLA Department of Anesthesiology and Perioperative Medicine 1. Incidence,
Anesthesiology Practice & Seizures Barbara Van de Wiele MD Clinical Professor, Vice Chair & Director Neurosurgical Anesthesiology UCLA Department of Anesthesiology and Perioperative Medicine 1. Incidence,
8/27/2017. Management of Status Epilepticus & Super-Refractory SE Definition SE. Definition SE. Epidemiology CSE. Classification of SE
 Management of Status Epilepticus & Super-Refractory SE 2017 TAYARD DESUDCHIT MD. HEAD, DIV. OF PED. NEUROLOGY FACULTY OF MEDICINE CHULALONGKORN U. Definition SE Traditional : Prolonged seizure lasting
Management of Status Epilepticus & Super-Refractory SE 2017 TAYARD DESUDCHIT MD. HEAD, DIV. OF PED. NEUROLOGY FACULTY OF MEDICINE CHULALONGKORN U. Definition SE Traditional : Prolonged seizure lasting
Tom Heaps Consultant Acute Physician
 Tom Heaps Consultant Acute Physician 76-year-old male no PMHx witnessed generalized seizure at home ~2min further seizure in ambulance terminated after 5min with IV diazepam 10mg GCS 8 on arrival in ED
Tom Heaps Consultant Acute Physician 76-year-old male no PMHx witnessed generalized seizure at home ~2min further seizure in ambulance terminated after 5min with IV diazepam 10mg GCS 8 on arrival in ED
5/23/14. Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments
 Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments Andi Marmor, MD, MSEd Associate Professor, Pediatrics University of California,
Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments Andi Marmor, MD, MSEd Associate Professor, Pediatrics University of California,
ALL orders are active unless: 1. Order is manually lined through to inactivate 2. Orders with check boxes ( ) are unchecked DRUG AND TREATMENT ORDERS
 are unchecked DRUG AND TREATMENT ORDERS") Available at: ALL Adult Facilities Non Categorized SUB Protocol(SUB)* SUB Protocol Lab Orders(SUB)* ED Rainbow Tubes(SUB)* ***Reminder: Order ED Rainbow Tubes (SUB) as a separate form*** Nursing Orders
Available at: ALL Adult Facilities Non Categorized SUB Protocol(SUB)* SUB Protocol Lab Orders(SUB)* ED Rainbow Tubes(SUB)* ***Reminder: Order ED Rainbow Tubes (SUB) as a separate form*** Nursing Orders
Measures have been taken, by the Utah Department of Health, Bureau of Health Promotions, to ensure no conflict of interest in this activity
 Measures have been taken, by the Utah Department of Health, Bureau of Health Promotions, to ensure no conflict of interest in this activity Seizures in the School Setting Meghan Candee, MD MS Assistant
Measures have been taken, by the Utah Department of Health, Bureau of Health Promotions, to ensure no conflict of interest in this activity Seizures in the School Setting Meghan Candee, MD MS Assistant
Self Report Seizure Survey Summary 2017
 Self Report Seizure Survey Summary 2017 Tetrasomy 18p 61 responses 33 had at least one seizure = 54% 8 had a seizure in the last year Valproate (Depakote) 7 Valproate (Depakote, Epilium) 2 Lamotrigene
Self Report Seizure Survey Summary 2017 Tetrasomy 18p 61 responses 33 had at least one seizure = 54% 8 had a seizure in the last year Valproate (Depakote) 7 Valproate (Depakote, Epilium) 2 Lamotrigene
42 y/o woman with unwitnessed episode of loss of consciousness and urinary incontinence
 Top Five Neurological Emergencies: When To Refer February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation 1 CASE 1 42 y/o woman with unwitnessed episode
Top Five Neurological Emergencies: When To Refer February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation 1 CASE 1 42 y/o woman with unwitnessed episode
Author(s): C. James Holliman, M.D. (Penn State University), 2008
: C. James Holliman, M.D. (Penn State University), 2008") Project: Ghana Emergency Medicine Collaborative Document Title: Status Epilepticus (SE) Author(s): C. James Holliman, M.D. (Penn State University), 2008 License: Unless otherwise noted, this material is
Project: Ghana Emergency Medicine Collaborative Document Title: Status Epilepticus (SE) Author(s): C. James Holliman, M.D. (Penn State University), 2008 License: Unless otherwise noted, this material is
ESETT OUTCOMES. Investigator Kick-off Meeting Robert Silbergleit, MD
 ESETT OUTCOMES Investigator Kick-off Meeting Robert Silbergleit, MD Primary objective The primary objective is to determine the most effective and/or the least effective treatment of benzodiazepinerefractory
ESETT OUTCOMES Investigator Kick-off Meeting Robert Silbergleit, MD Primary objective The primary objective is to determine the most effective and/or the least effective treatment of benzodiazepinerefractory
Status Epilepticus. Mindy M. Messinger, PharmD Clinical Pharmacy Specialist Neurology Texas Children s Hospital. Pediatrics
 Status Epilepticus Mindy M. Messinger, PharmD Clinical Pharmacy Specialist Neurology Texas Children s Hospital Objectives Define the various stages of status epilepticus and explain the proposed pathophysiology
Status Epilepticus Mindy M. Messinger, PharmD Clinical Pharmacy Specialist Neurology Texas Children s Hospital Objectives Define the various stages of status epilepticus and explain the proposed pathophysiology
1/31/2009. Paroxysmal, uncontrolled electrical discharge of neurons in brain interrupting normal function
 Paroxysmal, uncontrolled electrical discharge of neurons in brain interrupting normal function In epilepsy abnormal neurons undergo spontaneous firing Cause of abnormal firing is unclear Firing spreads
Paroxysmal, uncontrolled electrical discharge of neurons in brain interrupting normal function In epilepsy abnormal neurons undergo spontaneous firing Cause of abnormal firing is unclear Firing spreads
Initial Treatment of Seizures in Childhood
 Initial Treatment of Seizures in Childhood Roderic L. Smith, MD, Ph.D. Pediatric Neurology Clinic of Alaska,PC Incidence of Seizures Overall 5% by age 20 yrs. Lifetime risk= 5-10% CNS Infections= 5% TBI=10%
Initial Treatment of Seizures in Childhood Roderic L. Smith, MD, Ph.D. Pediatric Neurology Clinic of Alaska,PC Incidence of Seizures Overall 5% by age 20 yrs. Lifetime risk= 5-10% CNS Infections= 5% TBI=10%
Updated advice for nurses who care for patients with epilepsy
 NICE BULLETIN Updated advice for nurses who care for patients with epilepsy NICE provided the content for this booklet which is independent of any company or product advertised NICE BULLETIN Updated advice
NICE BULLETIN Updated advice for nurses who care for patients with epilepsy NICE provided the content for this booklet which is independent of any company or product advertised NICE BULLETIN Updated advice
11/7/2018 EPILEPSY UPDATE. Dr.Ram Sankaraneni. Disclosures. Speaker bureau LivaNova
 EPILEPSY UPDATE Dr.Ram Sankaraneni Disclosures Speaker bureau LivaNova 1 Outline New onset Seizure Investigations in patients with epilepsy Medical management of epilepsy Non Pharmacological options in
EPILEPSY UPDATE Dr.Ram Sankaraneni Disclosures Speaker bureau LivaNova 1 Outline New onset Seizure Investigations in patients with epilepsy Medical management of epilepsy Non Pharmacological options in
SEIZURE IN CHILDREN. IAP UG Teaching slides
 SEIZURE IN CHILDREN 1 DEFINITION Seizure Sudden paroxysmal transitory disturbance in brain function which starts suddenly, stops spontaneously and shows a tendency to recur. Manifestations can include
SEIZURE IN CHILDREN 1 DEFINITION Seizure Sudden paroxysmal transitory disturbance in brain function which starts suddenly, stops spontaneously and shows a tendency to recur. Manifestations can include
Contemporary Developments in Childhood Epilepsy Management. Olivia O Mahony, Cork University Hospital, Cork, and Mercy University Hospital
 Contemporary Developments in Childhood Epilepsy Management Olivia O Mahony, Cork University Hospital, Cork, and Mercy University Hospital Developments in Epilepsy Care Standardised epilepsy care using
Contemporary Developments in Childhood Epilepsy Management Olivia O Mahony, Cork University Hospital, Cork, and Mercy University Hospital Developments in Epilepsy Care Standardised epilepsy care using
Shake It Up: Seizure Prophylaxis and Status Epilepticus Management. Emily Yarborough, PharmD PGY2 Critical Care Pharmacy Resident January 4, 2018
 + Shake It Up: Seizure Prophylaxis and Status Epilepticus Management Emily Yarborough, PharmD PGY2 Critical Care Pharmacy Resident January 4, 2018 + Patient Case 1 + Patient Case 1 n JM is a 68 yo M involved
+ Shake It Up: Seizure Prophylaxis and Status Epilepticus Management Emily Yarborough, PharmD PGY2 Critical Care Pharmacy Resident January 4, 2018 + Patient Case 1 + Patient Case 1 n JM is a 68 yo M involved
In our patients the cause of seizures can be broadly divided into structural and systemic causes.
 Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
NASDAQ: ZGNX. Company Presentation. October 2017
 NASDAQ: ZGNX Company Presentation October 2017 2 Forward Looking Statement Zogenix cautions you that statements included in this presentation that are not a description of historical facts are forward-looking
NASDAQ: ZGNX Company Presentation October 2017 2 Forward Looking Statement Zogenix cautions you that statements included in this presentation that are not a description of historical facts are forward-looking
Physician Orders LEB PICU Status Epilepticus Plan. [ ] No known allergies
![Physician Orders LEB PICU Status Epilepticus Plan. [ ] No known allergies](/thumbs/80/82315048.jpg "Physician Orders LEB PICU Status Epilepticus Plan. [ ] No known allergies") Height: cm Weight: kg Allergies: [ ] No known allergies [ ] Initiate Powerplan Phase T;N, Phase: LEB PICU Admit Phase Admission/Transfer/Discharge [ ] Admit Patient to Dr. [ ] Admit Status: [ ] Inpatient
Height: cm Weight: kg Allergies: [ ] No known allergies [ ] Initiate Powerplan Phase T;N, Phase: LEB PICU Admit Phase Admission/Transfer/Discharge [ ] Admit Patient to Dr. [ ] Admit Status: [ ] Inpatient
Seizures Emergency Treatment
 Seizures Emergency Treatment Emergency Seizures SEIZURE CLASSIFICATION Cluster seizures - 2 or more generalized convulsive seizures in 24 hours Simon R. Platt BVM&S MRCVS Dipl. ACVIM (Neurology) Dipl.ECVN
Seizures Emergency Treatment Emergency Seizures SEIZURE CLASSIFICATION Cluster seizures - 2 or more generalized convulsive seizures in 24 hours Simon R. Platt BVM&S MRCVS Dipl. ACVIM (Neurology) Dipl.ECVN
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Seizures Seizures & Status Epilepticus Seizures are episodes of disturbed brain activity that cause changes in attention or behavior. Donna Lindsay, MN RN, CNS-BC, CCRN, CNRN Neuroscience Clinical Nurse
Seizures Seizures & Status Epilepticus Seizures are episodes of disturbed brain activity that cause changes in attention or behavior. Donna Lindsay, MN RN, CNS-BC, CCRN, CNRN Neuroscience Clinical Nurse
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Project: Ghana Emergency Medicine Collaborative. Document Title: Seizures. Author(s): Ryan LaFollette, MD (University of Cincinnati), 2013
: Ryan LaFollette, MD (University of Cincinnati), 2013") Project: Ghana Emergency Medicine Collaborative Document Title: Seizures Author(s): Ryan LaFollette, MD (University of Cincinnati), 2013 License: Unless otherwise noted, this material is made available
Project: Ghana Emergency Medicine Collaborative Document Title: Seizures Author(s): Ryan LaFollette, MD (University of Cincinnati), 2013 License: Unless otherwise noted, this material is made available
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
APPENDIX T - Unit costs of anti-epileptic drugs for 2012 guideline
 Drug name APPENDIX T - Unit costs of anti-epileptic drugs for 2012 guideline Unit costs and weighted average unit costs for drug used in the treatment of focal and generalised epilepsies Prescription Cost
Drug name APPENDIX T - Unit costs of anti-epileptic drugs for 2012 guideline Unit costs and weighted average unit costs for drug used in the treatment of focal and generalised epilepsies Prescription Cost
Periodic and Rhythmic Patterns. Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina
 Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
Unit VIII Problem 7 Pharmacology: Principles of Management of Seizure Disorders
 Unit VIII Problem 7 Pharmacology: Principles of Management of Seizure Disorders - Terminologies: Anti-convulsants: they are used to control convulsions seen in certain types of epilepsy. Convulsions may
Unit VIII Problem 7 Pharmacology: Principles of Management of Seizure Disorders - Terminologies: Anti-convulsants: they are used to control convulsions seen in certain types of epilepsy. Convulsions may
On completion of this chapter you should be able to: list the most common types of childhood epilepsies and their symptoms
 9 Epilepsy The incidence of epilepsy is highest in the first two decades of life. It falls after that only to rise again in late life. Epilepsy is one of the most common chronic neurological condition
9 Epilepsy The incidence of epilepsy is highest in the first two decades of life. It falls after that only to rise again in late life. Epilepsy is one of the most common chronic neurological condition
Management of Epilepsy in Primary Care and the Community. Carrie Burke, Epilepsy Specialist Nurse
 Management of Epilepsy in Primary Care and the Community Carrie Burke, Epilepsy Specialist Nurse Epilepsy & Seizures Epilepsy is a common neurological disorder characterised by recurring seizures (NICE,
Management of Epilepsy in Primary Care and the Community Carrie Burke, Epilepsy Specialist Nurse Epilepsy & Seizures Epilepsy is a common neurological disorder characterised by recurring seizures (NICE,
Dr. Dafalla Ahmed Babiker Jazan University
 Dr. Dafalla Ahmed Babiker Jazan University change in motor activity and/or behaviour due to abnormal electrical activity in the brain. seizures in children either - provoked by somatic disorders originating
Dr. Dafalla Ahmed Babiker Jazan University change in motor activity and/or behaviour due to abnormal electrical activity in the brain. seizures in children either - provoked by somatic disorders originating
Management of Complex Febrile Seizures
 Management of Complex Febrile Seizures An 13 month old girl presents to the ED after having a shaking episode at home. Mom describes shaking of both arms and legs, lasting 20 minutes. The child has no
Management of Complex Febrile Seizures An 13 month old girl presents to the ED after having a shaking episode at home. Mom describes shaking of both arms and legs, lasting 20 minutes. The child has no
Epilepsy and Epileptic Seizures
 Epilepsy and Epileptic Seizures Petr Marusič Dpt. of Neurology Charles University, Second Faculty of Medicine Motol University Hospital Diagnosis Steps Differentiation of nonepileptic events Seizure classification
Epilepsy and Epileptic Seizures Petr Marusič Dpt. of Neurology Charles University, Second Faculty of Medicine Motol University Hospital Diagnosis Steps Differentiation of nonepileptic events Seizure classification
PICU Therapeutic Hypothermia Post Cardiac Arrest Re Warming Phase
 Arrest Re Warming Phase Weight Allergies Patient Care ***After 24 hours initiate re warming (or after 72 hours for an infant less than one month old)*** PICU Re Warming Protocol ***See Reference Text***
Arrest Re Warming Phase Weight Allergies Patient Care ***After 24 hours initiate re warming (or after 72 hours for an infant less than one month old)*** PICU Re Warming Protocol ***See Reference Text***
Status Epilepticus in Children
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Status Epilepticus in Children. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Status Epilepticus in Children. These podcasts are designed to give medical students an overview of key topics in pediatrics.
Status epilepticus. Dr FL Chow
 Status epilepticus Dr FL Chow Terms Seizure paroxysmal event due to abnormal excessive neuronal activity in brain Epilepsy recurrent seizures due to chronic, underlying process; epilepsy syndromes Classification
Status epilepticus Dr FL Chow Terms Seizure paroxysmal event due to abnormal excessive neuronal activity in brain Epilepsy recurrent seizures due to chronic, underlying process; epilepsy syndromes Classification
Management of acute seizure and status epilepticus. Apisit Boongird, MD Division of Neurology Ramathibodi hospital
 Management of acute seizure and status epilepticus Apisit Boongird, MD Division of Neurology Ramathibodi hospital Outlines Seizure cluster/ Acute repetitive seizures Status epilepticus Seizure cluster
Management of acute seizure and status epilepticus Apisit Boongird, MD Division of Neurology Ramathibodi hospital Outlines Seizure cluster/ Acute repetitive seizures Status epilepticus Seizure cluster
Epilepsy 101. Overview of Treatment Kathryn A. O Hara RN. American Epilepsy Society
 Epilepsy 101 Overview of Treatment Kathryn A. O Hara RN American Epilepsy Society Objectives Describe the main treatment options for epilepsy Identify factors essential in the selection of appropriate
Epilepsy 101 Overview of Treatment Kathryn A. O Hara RN American Epilepsy Society Objectives Describe the main treatment options for epilepsy Identify factors essential in the selection of appropriate
Refractory Status Elipticus
 Refractory Status Elipticus In the 13 th round Laufey Yr Sigurdardottir MD Nemours Children s Hospital Department of Neurology NCH ED on Nov 29 th 2015 at 11:02 am First triage: fam here on vacation. pt
Refractory Status Elipticus In the 13 th round Laufey Yr Sigurdardottir MD Nemours Children s Hospital Department of Neurology NCH ED on Nov 29 th 2015 at 11:02 am First triage: fam here on vacation. pt
Anticonvulsants Antiseizure
 Anticonvulsants Antiseizure Seizure disorders Head trauma Stroke Drugs (overdose, withdrawal) Brain tumor Encephalitis/ Meningitis High fever Hypoglycemia Hypocalcemia Hypoxia genetic factors Epileptic
Anticonvulsants Antiseizure Seizure disorders Head trauma Stroke Drugs (overdose, withdrawal) Brain tumor Encephalitis/ Meningitis High fever Hypoglycemia Hypocalcemia Hypoxia genetic factors Epileptic
NEONATAL SEIZURES-PGPYREXIA REVIEW
 NEONATAL SEIZURES-PGPYREXIA REVIEW This is a very important Postgraduate topics will few Q asked in undergraduation also. Lets see them in detail. References: 1.Volpe s Neurology of newborn 2.Nelson s
NEONATAL SEIZURES-PGPYREXIA REVIEW This is a very important Postgraduate topics will few Q asked in undergraduation also. Lets see them in detail. References: 1.Volpe s Neurology of newborn 2.Nelson s
RESULTS: Seizures Primary Outcomes Survey AUGUST 2016
 RESULTS: Seizures Primary Outcomes Survey AUGUST 2016 1 Statistical analysis Descriptive statistics were used to describe the characteristics and responses of the respondents overall and split by specialty
RESULTS: Seizures Primary Outcomes Survey AUGUST 2016 1 Statistical analysis Descriptive statistics were used to describe the characteristics and responses of the respondents overall and split by specialty
Generalized seizures, generalized spike-waves and other things. Charles Deacon MD FRCPC Centre Hospitalier Universitaire de Sherbrooke
 Generalized seizures, generalized spike-waves and other things Charles Deacon MD FRCPC Centre Hospitalier Universitaire de Sherbrooke Objectives Give an overview of generalized EEG discharges and seizures
Generalized seizures, generalized spike-waves and other things Charles Deacon MD FRCPC Centre Hospitalier Universitaire de Sherbrooke Objectives Give an overview of generalized EEG discharges and seizures
Objectives. Amanda Diamond, MD
 Amanda Diamond, MD Objectives Recognize symptoms suggestive of seizure and what those clinical symptoms represent Understand classification of epilepsy and why this is important Identify the appropriate
Amanda Diamond, MD Objectives Recognize symptoms suggestive of seizure and what those clinical symptoms represent Understand classification of epilepsy and why this is important Identify the appropriate
Treatment of Status Epilepticus SUDA JIRASAKULDEJ, MD KING CHULALONGKORN MEMORIAL HOSPITAL AUGUST 21, 2016
 Treatment of Status Epilepticus SUDA JIRASAKULDEJ, MD KING CHULALONGKORN MEMORIAL HOSPITAL AUGUST 21, 2016 Outline Definition of status epilepticus Classification of status epilepticus Treatment of status
Treatment of Status Epilepticus SUDA JIRASAKULDEJ, MD KING CHULALONGKORN MEMORIAL HOSPITAL AUGUST 21, 2016 Outline Definition of status epilepticus Classification of status epilepticus Treatment of status
Generic Name (Brand Name) Available Strengths Formulary Limits. Primidone (Mysoline) 50mg, 250mg -- $
 Available Strengths Formulary Limits. Primidone (Mysoline) 50mg, 250mg -- $") MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Epilepsy P&T DATE: 2/15/2017 THERAPEUTIC CLASS: Neurologic Disorders REVIEW HISTORY: 2/16 LOB AFFECTED: Medi-Cal (MONTH/YEAR)
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Epilepsy P&T DATE: 2/15/2017 THERAPEUTIC CLASS: Neurologic Disorders REVIEW HISTORY: 2/16 LOB AFFECTED: Medi-Cal (MONTH/YEAR)
Epilepsy 7/28/09! Definitions. Classification of epilepsy. Epidemiology of Seizures and Epilepsy. International classification of epilepsies
 Definitions Epilepsy Dr.Yotin Chinvarun M.D., Ph.D. Seizure: the clinical manifestation of an abnormal and excessive excitation of a population of cortical neurons Epilepsy: a tendency toward recurrent
Definitions Epilepsy Dr.Yotin Chinvarun M.D., Ph.D. Seizure: the clinical manifestation of an abnormal and excessive excitation of a population of cortical neurons Epilepsy: a tendency toward recurrent
Review of Anticonvulsant Medications: Traditional and Alternative Uses. Andrea Michel, PharmD, CACP
 Review of Anticonvulsant Medications: Traditional and Alternative Uses Andrea Michel, PharmD, CACP Objectives Review epidemiology of epilepsy Classify types of seizures Discuss non-pharmacologic and pharmacologic
Review of Anticonvulsant Medications: Traditional and Alternative Uses Andrea Michel, PharmD, CACP Objectives Review epidemiology of epilepsy Classify types of seizures Discuss non-pharmacologic and pharmacologic
Objectives / Learning Targets: The learner who successfully completes this lesson will be able to demonstrate understanding of the following concepts:
 Boone County Fire District EMS Education-Paramedic Program EMS 270 Medical Cases-Seizures Resources Seizures screencast Seizures Flowchart and Seizures Flowchart Video Explanation Objectives / Learning
Boone County Fire District EMS Education-Paramedic Program EMS 270 Medical Cases-Seizures Resources Seizures screencast Seizures Flowchart and Seizures Flowchart Video Explanation Objectives / Learning
Child-Youth Epilepsy Overview, epidemiology, terminology. Glen Fenton, MD Professor, Child Neurology and Epilepsy University of New Mexico
 Child-Youth Epilepsy Overview, epidemiology, terminology Glen Fenton, MD Professor, Child Neurology and Epilepsy University of New Mexico New onset seizure case An 8-year-old girl has a witnessed seizure
Child-Youth Epilepsy Overview, epidemiology, terminology Glen Fenton, MD Professor, Child Neurology and Epilepsy University of New Mexico New onset seizure case An 8-year-old girl has a witnessed seizure
Disclosures. What is Status Epilepticus? Purpose of Today s Discussion. Nothing to Disclose. How do I recognize Status Epilepticus?
 Disclosures Nothing to Disclose Neurologic Emergencies SID W. ATKINSON MD Chief, Division of Child Neurology, and Developmental Pediatrics Purpose of Today s Discussion Understand 2 Neurologic Emergencies
Disclosures Nothing to Disclose Neurologic Emergencies SID W. ATKINSON MD Chief, Division of Child Neurology, and Developmental Pediatrics Purpose of Today s Discussion Understand 2 Neurologic Emergencies
Antiepileptics Audit
 Antiepileptics Audit Dr Kate Marley Dr Lucy Potter Dr Melanie Brooks Dr Averil Fountain CNS Sue Croft External Reviewer: Dr A Nicolson Consultant Neurologist c CURRENT GUIDANCE 4.1 GENERAL PRINCIPLES Anti-epileptic
Antiepileptics Audit Dr Kate Marley Dr Lucy Potter Dr Melanie Brooks Dr Averil Fountain CNS Sue Croft External Reviewer: Dr A Nicolson Consultant Neurologist c CURRENT GUIDANCE 4.1 GENERAL PRINCIPLES Anti-epileptic
Introduction. 1 person in 20 will have an epileptic seizure at some time in their life
 Introduction 1 person in 20 will have an epileptic seizure at some time in their life Epilepsy is diagnosed on the basis of two or more epileptic seizures. Around 450,000 people in the UK have epilepsy
Introduction 1 person in 20 will have an epileptic seizure at some time in their life Epilepsy is diagnosed on the basis of two or more epileptic seizures. Around 450,000 people in the UK have epilepsy
New Patient Questionnaire - Epilepsy
 New Patient Questionnaire - Epilepsy Person completing this form: (if other than the patient) GENERAL SEIZURE HISTORY Relationship: When do you think your child had their first seizure? When was the last
New Patient Questionnaire - Epilepsy Person completing this form: (if other than the patient) GENERAL SEIZURE HISTORY Relationship: When do you think your child had their first seizure? When was the last
Physician Orders PEDIATRIC: : LEB ED Trauma (Major) Plan
 Plan") LEB ED Standing Orders Trauma (Major) Ph Non Categorized Criteria: Patients between 0-18 years of age that present with a Major Trauma that meet LeBonheur Trauma stat or Trauma Alert Guidelines.(NOTE)*
LEB ED Standing Orders Trauma (Major) Ph Non Categorized Criteria: Patients between 0-18 years of age that present with a Major Trauma that meet LeBonheur Trauma stat or Trauma Alert Guidelines.(NOTE)*
SAGE-547 for super-refractory status epilepticus
 NIHR Innovation Observatory Evidence Briefing: April 2017 SAGE-547 for super-refractory status epilepticus NIHRIO (HSRIC) ID: 10866 NICE ID: 8456 Status epilepticus is a single epileptic seizure lasting
NIHR Innovation Observatory Evidence Briefing: April 2017 SAGE-547 for super-refractory status epilepticus NIHRIO (HSRIC) ID: 10866 NICE ID: 8456 Status epilepticus is a single epileptic seizure lasting
Dravet syndrome : Clinical presentation, genetic investigation and anti-seizure medication. Bradley Osterman MD, FRCPC, CSCN
 Dravet syndrome : Clinical presentation, genetic investigation and anti-seizure medication Bradley Osterman MD, FRCPC, CSCN Objectives Learn about the typical early clinical presentation of Dravet syndrome
Dravet syndrome : Clinical presentation, genetic investigation and anti-seizure medication Bradley Osterman MD, FRCPC, CSCN Objectives Learn about the typical early clinical presentation of Dravet syndrome
Epilepsy Currents and Pearls. Eniko Nagy-Wilde, MD Medical Director of Epilepsy and Clinical Neurophysiology Sutter Medical Center, Sacramento
 Epilepsy Currents and Pearls Eniko Nagy-Wilde, MD Medical Director of Epilepsy and Clinical Neurophysiology Sutter Medical Center, Sacramento No disclosures Presenter Disclosure Information Learning Objectives
Epilepsy Currents and Pearls Eniko Nagy-Wilde, MD Medical Director of Epilepsy and Clinical Neurophysiology Sutter Medical Center, Sacramento No disclosures Presenter Disclosure Information Learning Objectives
Hypothermia Short Set-Critical Care HYPOTHERMIA SS- CRITICAL CARE
 Hypothermia Short Set-Critical Care HYPOTHERMIA SS- CRITICAL CARE Inclusion Criteria all must be present Cardiac arrest with return of spontaneous circulation (ROSC) ROSC within 60 mins of witnessed arrest;
Hypothermia Short Set-Critical Care HYPOTHERMIA SS- CRITICAL CARE Inclusion Criteria all must be present Cardiac arrest with return of spontaneous circulation (ROSC) ROSC within 60 mins of witnessed arrest;
ONE day after he stops drinking, a 50-year-old alcoholic experiences a generalized tonic-clonic convulsion; a 30-year-old man with AIDS watches his
 EPILEPSY ONE day after he stops drinking, a 50-year-old alcoholic experiences a generalized tonic-clonic convulsion; a 30-year-old man with AIDS watches his arm jerk uncontrollably for two minutes; a 70-year-old
EPILEPSY ONE day after he stops drinking, a 50-year-old alcoholic experiences a generalized tonic-clonic convulsion; a 30-year-old man with AIDS watches his arm jerk uncontrollably for two minutes; a 70-year-old
Pharmacological Treatment of Non-Lesional Epilepsy December 8, 2013
 Pharmacological Treatment of Non-Lesional Epilepsy December 8, 2013 Michael Privitera, MD Professor of Neurology University of Cincinnati, Neuroscience Institute American Epilepsy Society Annual Meeting
Pharmacological Treatment of Non-Lesional Epilepsy December 8, 2013 Michael Privitera, MD Professor of Neurology University of Cincinnati, Neuroscience Institute American Epilepsy Society Annual Meeting
Chapter 15. Media Directory. Convulsion. Seizures. Epilepsy. Known Causes of Seizures. Drugs for Seizures
 Chapter 15 Drugs for Seizures Slide 43 Slide 45 Media Directory Diazepam Animation Valproic Acid Animation Upper Saddle River, New Jersey 07458 All rights reserved. Seizures Convulsion Abnormal or uncontrolled
Chapter 15 Drugs for Seizures Slide 43 Slide 45 Media Directory Diazepam Animation Valproic Acid Animation Upper Saddle River, New Jersey 07458 All rights reserved. Seizures Convulsion Abnormal or uncontrolled
Disclosures. Learning Objectives. Dan Lowenstein UCSF Epilepsy Center. Case 1: Duane 32 years 2/17/2012. A series of clinical cases to review:
 Disclosures NeuroVista, Inc. Neurologix, Inc. Scientific Advisory Board Scientific Advisory Board Dan Lowenstein UCSF Epilepsy Center Recent Advances in Neurology February 16th, 2012 Learning Objectives
Disclosures NeuroVista, Inc. Neurologix, Inc. Scientific Advisory Board Scientific Advisory Board Dan Lowenstein UCSF Epilepsy Center Recent Advances in Neurology February 16th, 2012 Learning Objectives
Adult Seizure and Epilepsy Management Pathway (16 years of age and above)
") Adult Seizure and Epilepsy Management Pathway (16 years of age and above) SUSPECTED SEIZURE Secure and record eyewitness account if available ECG Abnormal ECG Cardiac cause clinically possible Epilepsy
Adult Seizure and Epilepsy Management Pathway (16 years of age and above) SUSPECTED SEIZURE Secure and record eyewitness account if available ECG Abnormal ECG Cardiac cause clinically possible Epilepsy
Opinion 24 July 2013
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 24 July 2013 FYCOMPA 2 mg, film-coated tablet B/7 (CIP: 34009 267 760 0 8) B/28 (CIP: 34009 268 447 4 5) FYCOMPA 4
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 24 July 2013 FYCOMPA 2 mg, film-coated tablet B/7 (CIP: 34009 267 760 0 8) B/28 (CIP: 34009 268 447 4 5) FYCOMPA 4
Epilepsy 101. Russell P. Saneto, DO, PhD. Seattle Children s Hospital/University of Washington November 2011
 Epilepsy 101 Russell P. Saneto, DO, PhD Seattle Children s Hospital/University of Washington November 2011 Specific Aims How do we define epilepsy? Do seizures equal epilepsy? What are seizures? Seizure
Epilepsy 101 Russell P. Saneto, DO, PhD Seattle Children s Hospital/University of Washington November 2011 Specific Aims How do we define epilepsy? Do seizures equal epilepsy? What are seizures? Seizure
Is it epilepsy? Does the patient need long-term therapy?
 Is it a seizure? Definition Transient occurrence of signs and/or symptoms due to abnormal excessive or synchronous neuronal activity in the brain Is it provoked or unprovoked? Is it epilepsy? Does the
Is it a seizure? Definition Transient occurrence of signs and/or symptoms due to abnormal excessive or synchronous neuronal activity in the brain Is it provoked or unprovoked? Is it epilepsy? Does the
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Lacosamide (Vimpat) Reference Number: CP.PMN.155 Effective Date: 10.01.18 Last Review Date: 07.13.18 Line of Business: Oregon Health Plan Revision Log See Important Reminder at the end
Clinical Policy: Lacosamide (Vimpat) Reference Number: CP.PMN.155 Effective Date: 10.01.18 Last Review Date: 07.13.18 Line of Business: Oregon Health Plan Revision Log See Important Reminder at the end
SIGN 143 Diagnosis and management of epilepsy in adults. Quick Reference Guide. May 2015 Revised Evidence
 SIGN 143 iagnosis and management of epilepsy in adults Quick Reference Guide May 2015 Revised 2018 Evidence Key to evidence statements and recommendations Recommendations are graded to indicate the strength
SIGN 143 iagnosis and management of epilepsy in adults Quick Reference Guide May 2015 Revised 2018 Evidence Key to evidence statements and recommendations Recommendations are graded to indicate the strength
Jeffrey W Boyle, MD, PhD Avera Medical Group Neurology Sioux Falls, SD
 Jeffrey W Boyle, MD, PhD Avera Medical Group Neurology Sioux Falls, SD Disclosures: None Objectives Recognize the incidence of seizure and epilepsy in the US population Appreciate the differences in seizure
Jeffrey W Boyle, MD, PhD Avera Medical Group Neurology Sioux Falls, SD Disclosures: None Objectives Recognize the incidence of seizure and epilepsy in the US population Appreciate the differences in seizure