AEDs 2. Bassel Abou-Khalil, M.D.
|
|
|
- Buddy Newton
- 5 years ago
- Views:
Transcription

1 AEDs 2 Bassel Abou-Khalil, M.D.
2 None Disclosures
3 SAE Question ARS Which is not true of phenytoin? A- half-life increases with increasing serum level B- protein-free portion is elevated in hepatic and renal failure C- level may increase with high dose oxcarbazepine D- it reduces valproate level E- valproate concomitant use results in decreased protein-free portion
4 SAE Question ARS Which is least likely to cause carbamazepine accumulation? A- erythromycin B- azithromycin C- propoxyphene D- grapefruit juice E- fluoxetine
5 SAE Question ARS The cooperative VA comparative AED trials showed A- carbamazepine and phenytoin were better tolerated than phenobarbital and primidone B- carbamazepine was more efficacious than primidone C- carbamazepine and valproate were equally effective for complex partial seizures D- phenytoin had the greatest seizure-free rate E- valproate was more effective than carbamazepine for secondarily generalized seizures
6 SAE Question ARS What is least likely to happen when oxcarbazepine is substituted for carbamazepine? A- Increased valproate level B- Decreased sodium level C- Increased prothrombin time in a patient treated with warfarin D- Increased bone density E- Decreased sex hormone binding globulin
7 SAE Question ARS Which AEDs have the greatest proportion of protein binding? A- carbamazepine and oxcarbazepine B- phenobarbital and primidone C- phenytoin and valproate D- ethosuximide and methsuximide
8 Objectives Review pharmacokinetics of PB, PRM, PHT, CBZ, OXC, VPA, ESM, CZP, DZP, LZP, CLB, ACTH, AZM Review key interactions of above Review main adverse effects of above
9 Phenobarbital (PB) In use since 1912 MOA: enhances postsynaptic GABA A receptor-mediated chloride currents by prolonging the opening of the Cl - channel. May also have other actions (HVA channels and glutamate receptors). Available as oral preparations and parenteral solution
10 PB- absorption, distribution Oral absolute bioavailability is > 90% Tmax = 2-4 hours Protein binding: ~45% V d = ~0.6 L/Kg
11 PB- elimination Elimination: 20-25% eliminated renally, unchanged; rest metabolized in the liver T 1/2 = hours in adults; ~ hours in newborns; hours before age 5 after that
12 PB- interactions PB is a potent inducer of p450 enzymes. Accelerates metabolism and reduces levels of AEDs processed by this enzyme system Reduces valproate, ethosuximide, lamotrigine, etc.. Reduces levels of CBZ (but may increase CBZ-epoxide to CBZ ratio) Reduces efficacy of warfarin, steroids, oral contraceptive Variable effect on phenytoin (due to competing for metabolism) Phenobarbital level is increased by inhibitors valproate and felbamate
13 PB adverse effects Sedation Mood changes (depression) Hyperactivity/irritability in children Decreased memory and concentration Long term use associated with decreased bone density and connective tissue disorders Dupuytren s contractures Plantar fibromatosis Frozen shoulder
14 PB- efficacy/clinical indication Effective against partial-onset (focal) seizures, generalized tonic-clonic seizures, other generalized-onset seizures except absence. Not drug of choice in developed countries May be the only affordable AED in much of the developing world
15 Phenobarbital titration & dosing Initiation Titration Optimization 30 to 60 mg at bedtime. Increase dose by mg every two weeks as needed, depending on seizure control and tolerability - Dose can be increased up to mg at bedtime if needed. While seizure control and tolerability are the main determinants, phenobarbital serum level may also be helpful in deciding on continuing titration (levels above 25 mcg/ml are associated with increased toxicity).
16 PB dosing for children 2-5 mg/kg/day over age 3 years 3-7 mg/kg/day for age 1-3 years 4-11 mg/kg/day for age 2 m- 1 year 3-4 mg/kg/day in neonates PB dosing for status epilepticus mg/kg Rate of administration <100 mg per minute (<2mg/Kg per minute for small children)
17 Primidone (PRM) Is converted to phenobarbital (PB) and phenylethylmalonamide (PEMA), which is also an active metabolite MOA: Does not have a direct effect on GABA receptors. May act synergistically with PB to reduce sustained, high-frequency, repetitive firing at clinically relevant concentrations. PB acts on the GABA A receptor to prolong opening of the chloride channel PEMA action unknown and modest
18 Primidone Phenylethylmalonamide (PEMA) Phenobarbital
19 PRM absorption, distribution Oral bioavailability is fairly complete (~92%) Tmax = ~3 h V d = 0.54 (single dose)-0.86 L/Kg Poorly soluble, precluding IV preparation Protein binding: <10% for PMD and PEMA
20 PRM- metabolism and elimination PEMA is first detected metabolite ~25% of oral PRM is converted to PB (dose of PRM required for certain PB level ~4-5 x dose of PB required for same level) In monotherapy T 1/2 = hours- with enzyme inducers T 1/2 = hours. After one dose 64% excreted unchanged in absence of induction, ~40% excreted unchanged with induction.
21 PRM- interactions Co-administration of inducers (particularly PHT) reduces ratio of PRM to PB due acceleration of PRM to PB conversion. PRM and PB are potent enzyme inducers All PB interactions are present by necessity
22 PRM adverse effects Acute toxic reactions different from PB Transient drowsiness, dizziness, ataxia, nausea, and vomiting that can be debilitating. Tolerance to acute AEs develops rapidly within hours to days. Long-term PB therapy protects from acute PRM toxicity Chronic AEs same as PB
23 PRM efficacy and indications Effective against same seizure types as phenobarbital Equal efficacy, but lower tolerability in comparison to PB, PHT, CBZ
24 Primidone titration & dosing Initiation Titration Optimization mg at bedtime. Increase dose by mg every 3 days as needed, depending on seizure control and tolerability Dose can be increased up to 500 mg tid-qid if needed. PMD level reference range: 5-12 mcg/ml
25 Primidone- Pediatric dosing Children younger than 8 years: Days 1-3: 50 mg at bedtime Days 4-6: 50 mg bid. Days 7-9: 100 mg bid. Day 10-maintenance: 125 mg tid to 250 mg tid (10-20 mg/ day)
26 Phenytoin (PHT) In use since 1938 when Houston and Merritt discovered its efficacy in the MES model MOA: binds to the active state of the sodium channel and reduces high frequency firing (as might occur during a seizure) while allowing normal action potentials to occur. Available as oral preparations and parenteral solution
27 PHT absorption, distribution Rate and extent of absorption may differ among different formulations and affected by many factors, including age and food (decreased in neonates, with NG feedings, calcium, antacids). Limited absorption in the stomach. Absorption primarily in the duodenum, where the higher ph increases PHT solubility. Tmax 4-8 hours (up to 12 hours), sooner with immediate release V d = 0.78 L/Kg Protein binding: ~90%
28 PHT- metabolism Major pathway of elimination is hydroxylation mediated mainly by the cytochrome P450 enzyme CYP2C9> CYP2C19. Nonlinear kinetics- small changes in CYP2C9 activity may have clinically significant effects. Some alleles are associated with reduced clearance. Importance of CYP2C19 increases with higher levels. Some alleles and inhibitors (e.g. ticlopidine or isoniazid) may lead to accumulation
29 PHT elimination PHT follows nonlinear elimination kinetics, unlike other AEDs T 1/2 is dependent on serum concentration. Initial T 1/2 = ~ 22 h (range 8 60). The half-life will increase as the serum concentration increases within and above the recommended therapeutic range (10-20 mg/l). ~95% is excreted in urine and feces as metabolites, < 5% unchanged PHT
30 PHT nonlinear elimination kinetics Enzymes responsible for most of PHT elimination are partially saturated at concentrations within the recommended therapeutic range (with individual variation as to concentration at which this phenomenon starts). These enzymes are not able to increase their activity in proportion to PHT concentration as the concentration increases to the recommended therapeutic range. Steady-state PHT level increases disproportionately as the maintenance dose is increased within and above the recommended therapeutic range.
31 Phenytoin nonlinear kinetics- Example of consequences Example 1: a daily dose of 300 mg per day results in a serum concentration of 9 mg/l. Increasing the dose to 400 mg per day (30% increase) would have increased the steady state concentration by 30% to 12 mg/ml if phenytoin were to follow linear elimination kinetics. With its nonlinear kinetics, the concentration may increase disproportionately by >300% to 31 mg/l with associated toxicity Example 2: a patient presents with phenytoin toxicity and a serum concentration of 40 mg/l. The T 1/2 was previously estimated at 24 hours. However, after phenytoin was stopped it took 3 days for the serum concentration to go below 20 mg/l
32 30 Non-linear kinetics (ex: phenytoin) Linear kinetics (other AEDs) Individual therapeutic range
33 PHT- forms Extended release capsules contain phenytoin sodium Immediate release tablets contain phenytoin, so they are not exactly equivalent.
34 PHT- interactions PHT affected by drugs that Decrease absorption (e.g. NG tube feedings) Compete for protein binding (VPA) Enzyme inducers or inhibiters PHT is a potent enzyme inducer that reduces the efficacy of other AEDs metabolized by p450 enzyme system
35 PHT and protein binding Free level is responsible for therapeutic effect and for toxicity Free fraction increases in presence of low protein state, renal failure, hepatic failure, old age, or with co-administration of VPA. Total level can be corrected in presence of low protein state using following formula: Cn = Co/[(0.02 x Albumin) + 0.1]
36 PHT- Adverse effects Concentration-dependent AEs: nystagmus, ataxia, incoordination, diplopia, dysarthria, drowsiness. Exacerbation of seizures may occur with levels above 30 mcg/ml. Some may experience prominent AEs within the recommended therapeutic range, including cognitive AEs.
37 PHT- Idiosyncratic AEs Idiosyncratic reactions may be related to formation of an arene oxide, a reactive metabolite that forms due to inadequate epoxide hydrolase activity. Allergic rash occurs in up to 8.5% of patients Stevens Johnson syndrome, toxic epidermal necrolysis less common Hypersensitivity syndrome with rash, fever, lymphadenopathy, eosinophilia, elevated liver enzymes, renal failure is very uncommon.
38 PHT- long-term AEs Gingival hyperplasia, hirsutism, acne Cerebellar atrophy (may also occur after acute high dose) Reduced bone density Reduced folate levels, anemia, macrocytosis Teratogenicity
39 Local reactions AEs- IV solution Pain and burning at infusion site Phlebitis Cellulitis or necrosis from extravasation Purple glove syndrome with discoloration then petechial rash Cardiovascular AEs related in part to vehicle (propylene glycol), can be avoided with slowing of infusion rate (max 50 mg/min) hypotension, conduction abnormality, arrhythmia
40 PHT- Efficacy and Clinical Indications Effective against partial onset seizures and generalized tonic-clonic seizures. Efficacy against tonic and atonic seizures less well established. Not effective against generalized myoclonic or absence seizures (and may exacerbate them).
41 Phenytoin titration & dosing Initiation Titration Optimization mg per day, initially given as one dose at bedtime -300 mg per day is usually most appropriate; 200 mg per day is preferable for the elderly and for individuals with impaired liver function; 400 mg per day can be given for young adult men with large muscle mass Titration should be primarily based on clinical response, secondarily on serum levels. In view of 0 order kinetics, smaller increments should be used when in the therapeutic range. Rough guide to titration : -increase by 100 mg if the level is <8 mcg/ml -increase by 60 mg if the level is 8-12 mcg/ml -increase by 30 mg if the level is mcg/ml -When possible, use extended release phenytoin sodium capsules (30 and 100 mg) rather than immediate release phenytoin tablets. - Use bid or even tid dosing if needed when seizures are drug-resistant -For fine tuning, combinations of 30 and 100 mg can be used for 10 mg increments or decrements Recommended therapeutic range: mg/l
42 Acute loading Oral loading dose can be given (18 mg/kg divided into three doses given 2 to 3 hours apart. IV loading dose for status epilepticus is mg/kg. Should be diluted in normal saline, not dextrose 5% in water; max rate 50 mg per minute into a large vein. Intramuscular injection not recommended due to slow and erratic absorption, and crystallization at injection site causing pain.
43 Fosphenytoin Phenytoin pro-drug Can be given IV or IM Rapidly and completely converted to phenytoin (by cleavage of the phosphate group by nonspecific phosphatases). Conversion T 1/2 is ~8-18 minutes. Conversion is complete in a little more than 1 hr. Highly bound to serum albumin (95% to 99%)- displaces phenytoin from protein binding sites after IV administration, increasing unbound phenytoin concentrations as a function of fosphenytoin concentration.
44 Fosphenytoin indications/dosing Indicated for replacement of oral PHT or for IV or IM loading Marketed in phenytoin equivalents (PE), so loading dose is equivalent to phenytoin loading dose. Loading dose mg PE/Kg, max rate 150 mg PE/min Therapeutic PHT level usually reached within 10 min after IV loading, within 30 min after IM administration.
45 Fosphenytoin AEs Lower incidence of local reactions. IV administration commonly associated with paresthesias/ itching, most often in the groin/ perianal region, on the trunk, or the back of the head; this is related to infusion rate and subsides rapidly after the end of infusion. It is not seen with IM administration.
46 Carbamazepine (CBZ) Similar in structure to tricyclic antidepressants. MOA: reduces high frequency neuronal firing through action on the sodium channel, in both a voltage- and use-dependent fashion
47 CBZ absorption, distribution Bioavailability ~ 80-90% T max = 3-4 hours. Lipophilic- crosses the blood-brain barrier readily Poorly water soluble V d = L/Kg Protein binding: 75%
48 CBZ- metabolism, elimination Cleared almost entirely via hepatic metabolism. Major pathways are epoxide-diol pathway, aromatic hydroxylation, and conjugation. Most important product is CBZ-10,11-epoxide (via oxidation through CYP3A4 and CYP2C8). It is active and also responsible for some adverse effects. Induces its own metabolism (autoinduction), with increasing clearance, shortening of T 1/2 and lowering of serum concentration over time (process takes 2-4 weeks). Cannot be started on target maintenance dose.
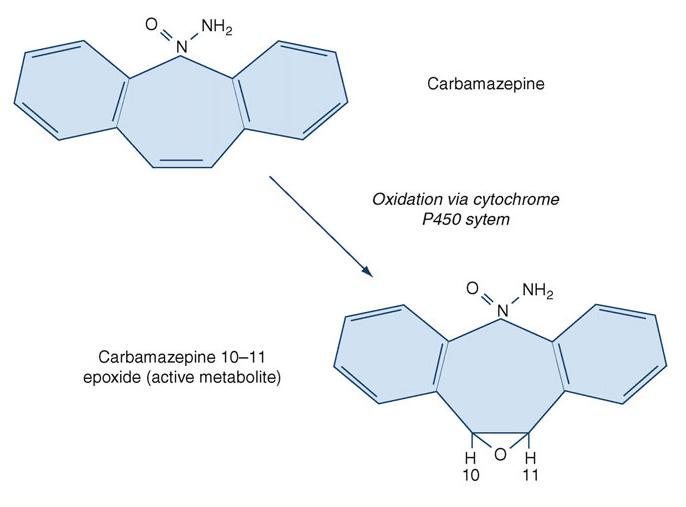
49
50 CBZ- Interactions Potent inducer of p450 enzyme system (CYP3A4, CYP2C9, CYP2C19, and CYP1A2), increasing clearance of agents metabolized by these enzymes Hormonal contraceptives Warfarin Valproate, lamotrigine, etc..
51 CBZ- Interactions Affected by agents that induce or inhibit CYP3A4 isoenzymes Inhibitors include erythromycin and related antibiotics (not azithromycin), fluoxetine, propoxyphene, grapefruit juice, etc... CBZ-epoxide increased by concomitant use of valproate, felbamate, oxcarbazepine, zonisamide
52 CBZ- adverse effects Most common AEs are nausea, GI discomfort, headache, dizziness, incoordination, unsteadiness, vertigo, sedation, tiredness, blurred vision, diplopia, nystagmus, tremor. Leukopenia is common (10-20%)- most often transient, but may be persistent. Hyponatremia Cognitive impairment on neuropsychological testing Weight gain Decreased bone density Increased sex hormone binding globulin and decreased testosterone
53 CBZ- idiosyncratic AEs Rash Stevens-Johnson syndrome, and toxic epidermal necrolysis are rare. Rare hypersensitivity syndrome, with fever, rash, and organ involvement. SLE rare Hepatotoxicity rare Aplastic anemia rare (1 per 200,000)
54 CBZ- idiosyncratic AEs Strong association between the HLA-B*1502 allele and CBZ-induced Stevens- Johnson syndrome in Asian populations and individuals of Asian descent FDA issued an alert and updated product labeling recommending genetic testing of HLA- B polymorphisms to predict carbamazepineinduced serious skin reactions in individuals of Asian descent.
55 CBZ- efficacy and indications Effective against partial onset seizures and against generalized tonic-clonic seizures May exacerbate absence and myoclonic seizures as well as atonic seizures. Recommended therapeutic range 4-12 mg/l
56 Carbamazepine titration & dosing Initiation Titration Optimization 100 mg bid for immediate release or 200 mg Qhs for extended release preparation x 3 days Increase to 200 mg bid x 3 days then 300 mg bid as initial target dose. The dose can be increased by mg every 3 days as needed -Extended release preparations provide steadier levels -Use bid dosing -Consider tid dosing for immediate release preparations - Little therapeutic benefit, toxicity expected after a level of 12 mcg/ml
57 Comparison of CBZ, PHB, PHT, or PMD in partial and secondarily generalized tonic-clonic seizures Mattson et al, N Engl J Med center, double-blind trial to compare the efficacy and toxicity of four AEDs [carbamazepine (CBZ), phenobarbital (PHB), phenytoin (PHT), or primidone (PMD)] in partial and secondarily generalized tonic-clonic seizures (SGTCS) in 622 adults Patients were randomly assigned to CBZ, PHB, PHT, or PMD and were followed for two years or until the drug failed due to uncontrolled seizures or unacceptable side effects Overall treatment success was highest with CBZ or PHT, intermediate with PhB, and lowest with PMD (p<0.002). PMD caused more intolerable acute toxic effects (nausea, vomiting, dizziness, sedation, decreased libido, impotence) Control of SGTCS did not differ significantly with the four drugs. CBZ provided complete control of partial seizures more often than PMD or PhB (p<0.03). Overall, CBZ and PHT are recommended drugs of first choice for single-drug therapy of adults with partial +/- SGTCS.
58 Seizure Freedom Treatment Group 12 months 12 months SGTCS only 12 months Partial only CBZ 47% 48% 43%* PhB 36% 43% 16% PHT 38% 43% 26% PMD 35% 45% 26% * Significantly better at every 6-month point for all 36 months
59 Oxcarbazepine (OXC) Structurally related to CBZ, but different from CBZ in metabolism and induction of metabolic pathways- rapidly and extensively metabolized to an active monohydroxy derivative (MHD)- no epoxide formation
60
61 OXC- absorption, distribution Oral absorption is virtually complete (bioavailability ~99%) MHD Tmax 4-6 hours after OXC dose (OXC Tmax 1-3 hours) MHD V d = L/Kg MHD Protein binding: 40% (OXC 60%)
62 OXC- metabolism, elimination OXC rapidly converted to the active metabolite monohydroxyderivative (MHD), which is then further metabolized MHD T½= 8-10 hrs (OXC T½= 1 to 3.7 hrs) Does not induce its own metabolism
63 OXC- interactions MHD level decreases with enzyme inducing AEDs (EIAEDs) Does not induce metabolism of other AEDs or warfarin Weakly induces CYP3A4 responsible for estrogen metabolism Weakly inhibits CYP2C19, raising PHT level at high doses Is not affected by erythromycin, fluoxetine, propoxyphene, grapefruit juice, etc..
64 OXC- Adverse effects Most common are somnolence, headache, dizziness, blurred vision, diplopia, fatigue, nausea, vomiting, ataxia Hyponatremia; more likely in older age or in association with diuretic intake Rash- ~2-4% Does not have CBZ effect on SHBG and testosterone
65 OXC- efficacy and clinical indications Effective against partial-onset seizures Multiple comparative monotherapy trials for new onset partial epilepsy OXC equal in efficacy to PHT and CBZ, but with less adverse effects/ superior tolerability OXC equal in efficacy and tolerability to VPA May exacerbate absence and myoclonic seizures
66 Oxcarbazepine titration & dosing Initial Titration Optimization 150 mg bid x 1 week then 300 mg bid May start at 300 mg bid in a young individual if rapid onset of action is important Would start at 150 mg Qhs x 1 week in an old individual at risk of hyponatremia or with other tolerabilty concern Increase by 300 mg every week as needed until seizures are controlled, adverse effects appear, or a serum level of mcg/ml has been reached Suggested titration steps (am-pm or am-noon-pm): or or or or The maximum dose used in trials was 1200 mg PO bid TID dosing may improve tolerability at doses higher than 1200 mg per day If used concomitantly with another sodium channel blocker, tolerability may be improved by a 2-hour interval between the doses of the two AEDs
67 OXC- conversion from CBZ Conversion from CBZ can be made overnight using a 1.5 to 1 ratio at a CBZ dose of < 800 mg. Lower conversion ratio advisable at higher CBZ doses. Conversion from CBZ to OXC will be accompanied by enzyme de-induction and possible elevation of other medication levels. Sodium level may decrease after conversion from CBZ
68 Valproate- divalproex (VPA) Serendipitous discovery (was used as solvent for AEDs in testing). Short-chain, branched fatty acid MOA: multiple mechanisms including blocking of Na channels, GABA potentiation, blocking T- calcium channels Main form used clinically is divalproex sodium, a complex composed of equal parts of VPA and sodium valproate
69 VPA- formulations Preparations include immediate-release VPA capsules, tablets, and syrup; delayed release enteric coated tablets of divalproex sodium (rapid release after coating dissolved) ; divalproex sodium enteric-coated sprinkles; extended release (ER) divalproex sodium; parenteral sodium valproate.
70 VPA- Absorption, distribution Bioavailability almost complete; 90% for ER Tmax depends on preparation ~2 hrs after syrup; 3-8 hrs after enteric coated divalproex DR; 4-17 hours after divalproex ER V d = L/kg in adults and L/kg in children. Protein binding ~90%; free fraction increases with increasing total concentration. 30% at 150 mg/l
71 VPA- Metabolism, elimination Metabolized by p450 enzyme system T 1/2 depends on inducing co-medication Adults: hours without induction; 9 hours with EIAEDs. Children: 11.7 and 7 hours Most abundant metabolites glucuronide and 3-oxo- VPA. Two metabolites have anticonvulsant activity similar to VPA- they accumulate slowly and are cleared slowly from the brain, accounting for some delayed effect.
72 VPA- Interactions Its metabolism is induced by PHT, CBZ, PB Levels increase after withdrawal of EIAEDs It can inhibit metabolism of PB, LTG, RFM, CBZ-epoxide It may compete for protein binding with PHT Its levels increase with co-administration of felbamate and clobazam
73 VPA- Adverse effects Gastric irritation with nausea, vomiting, GI distress, anorexia (less with enteric coated and ER formulation). Tremor Weight gain Hair loss Peripheral edema Thrombocytopenia Drowsiness, lethargy, confusion Reversible dementia and brain atrophy- more in seniors Encephalopathy with polytherapy Hyperammonemia, carnitine deficiency
74 Idiosyncratic AEs Fatal hepatotoxicity (risk factors are polytherapy and young age) 1:600 at < 3 y; 1:8,000 at 3-10 y, 1:10,000 at y; 1:31,000 at y; 1:107,000 at >40 y Pancreatitis
75 VPA- Efficacy and clinical indications Wide spectrum of efficacy against partialonset and all generalized-onset seizures, including absence and myoclonic seizures. Also indicated for migraine prophylaxis and bipolar disorder
76 Divalproex titration & dosing Initiation Titration Optimization 500 mg Qhs using the extended release preparation or 250 mg bid for the delayed release preparation -Increase by 250 mg as needed. -Avoid a dose higher than 1000 mg per day in a woman of childbearing potential. -Extended release preparations provide steadier levels -Use bid dosing to optimize seizure control in drug-resistant patients -Consider tid dosing for delayed release preparation -Little benefit and increased risk of toxicity is expected beyond a serum level of 100 mcg/ml Recommended therapeutic range: mg/l
77 A comparison of VPA with CBZ for the treatment of complex partial seizures and secondarily generalized tonic-clonic seizures in adults. Mattson et al, NEJM 1992 Multicenter, DB trial of VPA vs CBZ in 480 adults with CPS or SGTCS Patients randomly assigned to CBZ or VPA at doses adjusted to achieve blood levels in the mid-therapeutic range. Patients were followed for 1-5 years, until seizures became uncontrollable, treatment had unacceptable adverse effects, or both. For control of SGTC, CBZ and VPA were comparably effective. For CPS, 4/5 outcome measures favored CBZ (100 patients) over VPA (106 patients): total # of seizures (2.7 vs. 7.6, p=0.05), number of seizures per month (0.9 vs. 2.2, p=0.01), the time to the first seizure (p<0.02), and the seizure-rating score (p=0.04). CBZ was also superior according to a composite score of seizure control and adverse effects (P<0.001). VPA was associated more frequently than CBZ with weight gain >12 lb (20 % vs. 8 %, p< 0.001), with hair loss or change in texture (12 % vs. 6 %, p=0.02), and with tremor (45 % vs. 22 %, p<0.001). Rash was more common with CBZ (11 % vs. 1 %, p<0.001). VPA is as effective as CBZ for treatment of SGTC, but CBZ provides better control of CPS and has fewer long-term adverse effects.
78 Pediatric dosing Initial dose of 15 mg/kg Increase weekly as necessary and tolerated by 5-10 mg/kg per day, up to mg/kg per day if added to EIAED IV load Initial dose of mg/kg (at 20 mg per minute) followed by 1 mg/kg per hour.
79 Ethosuximide (ESM) MOA: blockade of T-type calcium currents in thalamus
80 ESM- absorption, distribution Oral bioavailability 90% to 95% Tmax= 1-4 hours Vd= 0.65 L/Kg Protein binding: <10%
81 ESM- metabolism, elimination Extensive hepatic oxidative biotransformation to inactive metabolite by CYP3A>> CYP2El. T 1/2 = hours (shorter in children)
82 ESM- interactions No effect on hepatic p450 enzymes and low protein binding predict low potential for causing interactions. reduced VPA level in one study Susceptible to interactions from inducers and inhibitors of p450 enzyme system. Clearance increased with enzyme inducers Clearance may decrease with VPA, isoniazid
83 ESM- adverse effects Most AEs are dose related- helped by dividing dose and administration with meals Nausea, abdominal discomfort, anorexia, vomiting. and diarrhea Drowsiness, insomnia, nervousness, dizziness, hiccups, fatigue, ataxia, and behavior changes (aggression, irritability, hyperactivity) Granulocytopenia Headaches, psychosis, depression, hallucinations (visual or auditory) not clearly dose related
84 ESM- idiosyncratic AEs Rash, Stevens-Johnson syndrome, SLE Aplastic anemia, thrombocytopenia, agranulocytosis (rare) Autoimmune thyroiditis (rare)
85 ESM- efficacy and clinical indications First-line monotherapy against typical absence seizures. Comparative trial favored its tolerability over valproate and efficacy over lamotrigine. Not effective against any other seizure type.
86 Ethosuximide titration & dosing Initiation Titration Optimization 3 to 6 years of age: 250 mg per day >6 years: 250 mg bid increase by 250 mg every week as needed for persistent seizure The optimal dose for most pediatric patients is 20 mg/kg/day Avoid increasing dose beyond 500 mg tid May use serum level for guidance (level mcg/ml)
87 Ethosuximide, valproic acid, and lamotrigine in childhood absence epilepsy Double-blind, randomized, controlled clinical trial to compare the efficacy, tolerability, and neuropsychological effects of ethosuximide, valproic acid, and lamotrigine in 453 children with newly diagnosed childhood absence epilepsy AED doses were increased until the child was free of seizures, the maximal allowable or highest tolerable dose was reached, or a criterion indicating treatment failure was met The primary outcome measure was freedom from treatment failure after 16 weeks of therapy Secondary outcome measure was attentional dysfunction Glauser et al, NEJM 2010
88 Ethosuximide, valproic acid, and lamotrigine in childhood absence epilepsy- Results 453 children were randomly assigned to treatment with ethosuximide (156), lamotrigine (149), or valproic acid (148) After 16 weeks of therapy, the freedom-from-failure rates for ethosuximide and valproic acid were similar (53% and 58%, respectively) and were higher than the rate for lamotrigine (29%; odds ratio with ethosuximide vs. lamotrigine, 2.66; 95% CI, 1.65 to 4.28; odds ratio with valproic acid vs. lamotrigine, 3.34; 95% CI, 2.06 to 5.42; P<0.001 for both comparisons) There were no significant differences among the three drugs with regard to discontinuation because of adverse events Attentional dysfunction was more common with valproic acid than with ethosuximide (in 49% of the children vs. 33%; odds ratio, 1.95; 95% CI, 1.12 to 3.41; P=0.03) Ethosuximide and valproic acid are more effective than lamotrigine in the treatment of childhood absence epilepsy. Ethosuximide is associated with fewer adverse attentional effects Glauser et al, NEJM 2010
89 Glauser et al, NEJM 2010
90 Benzodiazepines Mechanism of action: Increased frequency of GABA-mediated chloride channel openings
91 Clonazepam (CZP) Bioavailability>90% Tmax= 1-4 hours V d = 3.0 L/Kg Protein binding: 85% Metabolism: hepatic T 1/2 = hours Minimal interactions- clearance increased by inducers
92 CZP- adverse effects Drowsiness (tolerance to AEs develops) Nystagmus, incoordination, ataxia, dysarthria with higher doses Behavior disturbances more common in children- aggression, hyperactivity, paranoia Withdrawal seizures with abrupt discontinuation
93 CZP- clinical use Used for long-term treatment as well as acute management- only oral form available in USA Myoclonic seizures Wide spectrum of efficacy against partial and generalized seizure types Dose: children is 0.01 to.0.02 mg/kg per day; adults up to 8 mg per day in two or three divided doses. Tolerance develops to therapeutic effect
94 Diazepam (DZP) Bioavailability >90% Tmax: 1 hour V d = 1-2 L/Kg (high lipid solubility associated with redistribution) Protein binding: 95% T 1/2 = 36 hrs; initial T 1/2 = 1 hr Liver metabolism- active metabolites with long T 1/2 Induces CYP2B VPA increases free level through displacement from protein binding
95 DZP- adverse effects Sedation Fatigue, amnesia, ataxia, falls in the elderly Blurred vision, diplopia Respiratory depression with IV use Withdrawal seizures after chronic use
96 DZP- clinical use Available in oral tablet and liquid form, rectal gel, and parenteral solution Acute use for status epilepticus (but short duration of action requires additional agent), acute repetitive seizures (oral or rectal) Usually not adequate for chronic use, except that courses can be used in some syndromes such as Landau-Kleffner syndrome and electrical status epilepticus during sleep (ESES)
97 Lorazepam (LZP) Bioavailability >90% Tmax: hours V d = 1 L/Kg Protein binding: 90% T 1/2 = 15 hrs Metabolized in the liver through glucuronidation and excreted by the kidneys Clearance reduced by VPA and other inhibitors
98 LZP- adverse effects Sedation, dizziness, vertigo, weakness, unsteadiness, dysarthria Disorientation, depression, headache, agitation or restlessness, emotional disturbances, hallucinations, delirium Impaired psychomotor performance, anterograde amnesia Mild respiratory depression with IV use Withdrawal seizures from sudden discontinuation
99 LZP- clinical use Available in oral and parenteral forms Can be given sublingually Usually not appropriate for chronic use Status epilepticus (longer duration of action than DZP despite shorter half-life, and less respiratory depression makes it preferable) Acute repetitive seizures
100 Clobazam (CLB) The only 1,5-benzodiazepine used as an AED. Bioavailability >90% Tmax= 1-4 hours Protein binding: 85% T 1/2 = hours Metabolized in the liver to the active N- desmethyldobazam (T1/2= 42 hrs).
101 CLB- adverse effects Less sedation than with 1,4-benzodiazepines Drowsiness, fatigue, ataxia, dizziness, memory disturbance, aggressiveness Tolerance may develop, but less than with 1,4- benzodiazepines Seizures may occur with acute withdrawal
102 CLB- clinical use Available in tablets and syrup Widely used for long-term treatment of epilepsy FDA indicated for Lennox-Gastaut syndrome Wide spectrum of efficacy, as with other benzodiazepines
103 Clobazam titration & dosing Initiation Titration Optimization -10 mg Qhs or 5 mg bid Below 30 Kg: 5 mg Qhs -Increase by 5-10 mg per week, initially up to 10 mg bid or 20 mg Qhs - Increase dose by 5-10 mg per week as needed depending on seizure control and adverse effects, up to 20 mg bid or 40 mg Qhs
104 ACTH Used for short-term treatment of infantile spasms/ West syndrome Helps seizure control and improves behavior and EEG Most effective with idiopathic syndrome High dose may be more effective Alternatively, begin with 40 IU per day for 1 to 2 weeks, and increase to 60 or 80 IU per day thereafter if the response is incomplete. If effective, taper over 1 to 4 months. Less commonly used to treat Lennox Gastaut syndrome, Landau Kleffner syndrome
105 Acetazolamide (AZM) Carbonic anhydrase inhibitor Bioavailability complete with low dose, decreases with increasing dose Tmax= 2 4 hrs. Protein binding: 90 95% V d : 1.8 L/kg Terminal T 1/2 = h. Partially metabolized; 80% excreted by tubular secretion
106 AZM- adverse effects Altered taste perception (flat), loss of appetite, drowsiness, paresthesias Renal stones particularly in combination with topiramate, zonisamide, or ketogenic diet Metabolic acidosis Rare idiosyncratic: rash, hypersensitivity reactions, Steven Johnson syndrome, toxic epidermal necrolysis Rare muscle weakness, hepatic dysfunction
107 AZM- clinical use Adjunctive therapy for refractory focal and generalized epilepsies, particularly absence Adjunctive therapy for catamenial epilepsy, starting 2 days before predicted exacerbation Start at 250 mg/day and increase weekly based on response, up to 500 1,000 mg/day in 2-3 divided doses. Evidence for efficacy class 4 or anecdotal.

108 AED comparison- rash Arif et al, Neurology, 2007

109 AED comparison- rash in a patient with previous rash Arif et al, Neurology, 2007
110 How supplied Generic name Brand name How supplied Phenobarbital - 15 mg, 16.2 mg, 30 mg, 32.4 mg, 60 mg, 64.8 mg, 97.2 mg, 100 mg tablets 20 mg/5 ml elixir. Primidone Mysoline 50 mg and 250 mg tablets Generic same as above Ethosuximide Zarontin 250 mg capsules 250 mg/5 ml oral solution Generic same as above Clonazepam Klonopin 0.5 mg, 1 mg or 2 mg tablets mg, 0.25 mg, 0.5 mg, 1 mg or 2 mg orally disintegrating tablets Generic same as above Acetazolamide Diamox 125 mg, 250 mg tablets; 500 mg extended release capsule (Sequels); powder for injection
111 How supplied Generic name Brand name How supplied Phenytoin Dilantin 100 mg and 30 mg capsules of phenytoin sodium 50 mg tablets of phenytoin (infatab) 125 mg/5ml suspension Phenytek 200 mg, 300 mg capsules Generic 100 mg, 200 mg, 300 mg capsules, 125 mg/5ml suspension Carbamazepine Tegretol 100 mg chewable 200 mg tablets 100 mg/5 ml suspension Tegretol-XR Carbatrol Generic 100 mg, 200 mg, 400 mg tablets 100 mg, 200 mg, 300 mg capsules All of the above
112 How supplied Generic name Brand name How supplied Valproic acid Depakene 250 mg capsules 250 mg/ 5ml syrup Divalproex Depakote 125 mg, 250 mg, 500 mg tablets 125 mg sprinkle capsules Depakote ER Generic Oxcarbazepine Trileptal Oxtellar XR 250 mg, 500 mg tablets All the above 150 mg, 300 mg, 600 mg tablets 300 mg/5 ml oral suspension Generic same as above 150 mg, 300 mg, 600 mg tablets Clobazam Onfi 5 mg, 10 mg, 20 mg tablets
Epilepsy Medications: The Basics
 Epilepsy Medications: The Basics B R I A N A P P A V U, M D C L I N I C A L A S S I S T A N T P R O F E S S O R, D E P A R T M E N T O F C H I L D H E A L T H A N D N E U R O L O G Y, U N I V E R S I T
Epilepsy Medications: The Basics B R I A N A P P A V U, M D C L I N I C A L A S S I S T A N T P R O F E S S O R, D E P A R T M E N T O F C H I L D H E A L T H A N D N E U R O L O G Y, U N I V E R S I T
EPILEPSY: SPECTRUM OF CHANGE WITH AGE. Gail D. Anderson, Ph.D.
 EPILEPSY: SPECTRUM OF CHANGE WITH AGE Gail D. Anderson, Ph.D. Incidence: 0.5% - 1.0% of U.S. population Peak incidence of onset: first 2 years of life, ages 5-7 years, early puberty and elderly. 125,000
EPILEPSY: SPECTRUM OF CHANGE WITH AGE Gail D. Anderson, Ph.D. Incidence: 0.5% - 1.0% of U.S. population Peak incidence of onset: first 2 years of life, ages 5-7 years, early puberty and elderly. 125,000
Disclosure. Learning Objectives
 Linda D. Leary, M.D. Associate Clinical Professor of Pediatrics & Neurology South Texas Comprehensive Epilepsy Center UT Health Science Center San Antonio Disclosure Linda D. Leary, M.D. discloses the
Linda D. Leary, M.D. Associate Clinical Professor of Pediatrics & Neurology South Texas Comprehensive Epilepsy Center UT Health Science Center San Antonio Disclosure Linda D. Leary, M.D. discloses the
SEIZURES PHARMACOLOGY. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 SEIZURES PHARMACOLOGY University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Understand the pharmacodynamics involved in the medications used to treat seizures
SEIZURES PHARMACOLOGY University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Understand the pharmacodynamics involved in the medications used to treat seizures
Disclosures. AED Options. Epilepsy Pharmacotherapy: Treatment Considerations with Older AEDs
 Epilepsy Pharmacotherapy: Treatment Considerations with Older AEDs BARRY E. GIDAL, PHARMD PROFESSOR SCHOOL OF PHARMACY & DEPT. OF NEUROLOGY Disclosures Speaking honoraria: UCB, Eisai, Sunovion Consultant:
Epilepsy Pharmacotherapy: Treatment Considerations with Older AEDs BARRY E. GIDAL, PHARMD PROFESSOR SCHOOL OF PHARMACY & DEPT. OF NEUROLOGY Disclosures Speaking honoraria: UCB, Eisai, Sunovion Consultant:
ZONISAMIDE THERAPEUTICS. Brands * Zonegran. Generic? Not in US. If It Doesn t Work * Class Antiepileptic drug (AED), structurally a sulfonamide
, structurally a sulfonamide") Z:/3-PAGINATION/SBT/2-PROOFS/NWMS/9780521136723C111//9780521136723C111.3D 376 [376 380] ZONISAMIDE Brands Zonegran Generic? Not in US THERAPEUTICS Class Antiepileptic drug (AED), structurally a sulfonamide
Z:/3-PAGINATION/SBT/2-PROOFS/NWMS/9780521136723C111//9780521136723C111.3D 376 [376 380] ZONISAMIDE Brands Zonegran Generic? Not in US THERAPEUTICS Class Antiepileptic drug (AED), structurally a sulfonamide
New antiepileptic drugs
 Chapter 29 New antiepileptic drugs J.W. SANDER UCL Institute of Neurology, University College London, National Hospital for Neurology and Neurosurgery, Queen Square, London, and Epilepsy Society, Chalfont
Chapter 29 New antiepileptic drugs J.W. SANDER UCL Institute of Neurology, University College London, National Hospital for Neurology and Neurosurgery, Queen Square, London, and Epilepsy Society, Chalfont
Anticonvulsants Antiseizure
 Anticonvulsants Antiseizure Seizure disorders Head trauma Stroke Drugs (overdose, withdrawal) Brain tumor Encephalitis/ Meningitis High fever Hypoglycemia Hypocalcemia Hypoxia genetic factors Epileptic
Anticonvulsants Antiseizure Seizure disorders Head trauma Stroke Drugs (overdose, withdrawal) Brain tumor Encephalitis/ Meningitis High fever Hypoglycemia Hypocalcemia Hypoxia genetic factors Epileptic
AED Treatment Approaches. David Spencer, MD Director, OHSU Epilepsy Center Professor, Department of Neurology
 AED Treatment Approaches David Spencer, MD Director, OHSU Epilepsy Center Professor, Department of Neurology Audience Response Keypads Please utilize the keypad at your table to answer questions throughout
AED Treatment Approaches David Spencer, MD Director, OHSU Epilepsy Center Professor, Department of Neurology Audience Response Keypads Please utilize the keypad at your table to answer questions throughout
Buspirone Carbamazepine Diazepam Disulfiram Ethosuximide Flumazeil Gabapentin Lamotrigine
 CNS Depressants Buspirone Carbamazepine Diazepam Disulfiram Ethosuximide Flumazeil Gabapentin Lamotrigine Lorazepam Phenobarbital Phenytoin Topiramate Valproate Zolpidem Busprione Antianxiety 5-HT1A partial
CNS Depressants Buspirone Carbamazepine Diazepam Disulfiram Ethosuximide Flumazeil Gabapentin Lamotrigine Lorazepam Phenobarbital Phenytoin Topiramate Valproate Zolpidem Busprione Antianxiety 5-HT1A partial
Seizure medications An overview
 Seizure medications An overview Andrew Zillgitt, DO Staff Neurologist Comprehensive Epilepsy Center Department of Neurology Henry Ford Hospital None Disclosures Objectives A lot to review!!!!! Look at
Seizure medications An overview Andrew Zillgitt, DO Staff Neurologist Comprehensive Epilepsy Center Department of Neurology Henry Ford Hospital None Disclosures Objectives A lot to review!!!!! Look at
Epilepsy 101. Overview of Treatment Kathryn A. O Hara RN. American Epilepsy Society
 Epilepsy 101 Overview of Treatment Kathryn A. O Hara RN American Epilepsy Society Objectives Describe the main treatment options for epilepsy Identify factors essential in the selection of appropriate
Epilepsy 101 Overview of Treatment Kathryn A. O Hara RN American Epilepsy Society Objectives Describe the main treatment options for epilepsy Identify factors essential in the selection of appropriate
Types of epilepsy. 1)Generalized type: seizure activity involve the whole brain, it is divided into:
Generalized type: seizure activity involve the whole brain, it is divided into:") Types of epilepsy We have different types of epilepsy, so it is not one type of seizures that the patient can suffer from; we can find some patients with generalized or partial seizure. So, there are two
Types of epilepsy We have different types of epilepsy, so it is not one type of seizures that the patient can suffer from; we can find some patients with generalized or partial seizure. So, there are two
Introduction. 1 person in 20 will have an epileptic seizure at some time in their life
 Introduction 1 person in 20 will have an epileptic seizure at some time in their life Epilepsy is diagnosed on the basis of two or more epileptic seizures. Around 450,000 people in the UK have epilepsy
Introduction 1 person in 20 will have an epileptic seizure at some time in their life Epilepsy is diagnosed on the basis of two or more epileptic seizures. Around 450,000 people in the UK have epilepsy
I. Introduction Epilepsy is the tendency to have recurrent seizures unprovoked by systemic or acute neurologic insults. Antiepileptic drugs (AEDs)
") 1 2 I. Introduction Epilepsy is the tendency to have recurrent seizures unprovoked by systemic or acute neurologic insults. Antiepileptic drugs (AEDs) are those which decrease the frequency and/or severity
1 2 I. Introduction Epilepsy is the tendency to have recurrent seizures unprovoked by systemic or acute neurologic insults. Antiepileptic drugs (AEDs) are those which decrease the frequency and/or severity
Drug Monograph-Oxcarbazepine
 Drug Monograph Generic name: Oxcarbazepine Brand name: Trileptal Manufacturer: Norvatis (www.norvatis.com) Classification: Anti-epileptic drug Similar agents: Carbamazepine Summary Oxcarbazepine is a new
Drug Monograph Generic name: Oxcarbazepine Brand name: Trileptal Manufacturer: Norvatis (www.norvatis.com) Classification: Anti-epileptic drug Similar agents: Carbamazepine Summary Oxcarbazepine is a new
Antiepileptics. Medications Comment Quantity Limit Carbamazepine. May be subject Preferred to quantity limit Epitol
 Market DC Antiepileptics Override(s) Approval Duration Prior Authorization 1 year Step Therapy Quantity Limit *Indiana Medicaid See State Specific Mandate below *Maryland Medicaid See State Specific Mandate
Market DC Antiepileptics Override(s) Approval Duration Prior Authorization 1 year Step Therapy Quantity Limit *Indiana Medicaid See State Specific Mandate below *Maryland Medicaid See State Specific Mandate
improving the patient s quality of life.
 Epilepsy is the tendency to have recurrent seizures unprovoked by systemic or acute neurologic insults. Antiepileptic drugs (AEDs) are those which decrease the frequency and/or severity of seizures in
Epilepsy is the tendency to have recurrent seizures unprovoked by systemic or acute neurologic insults. Antiepileptic drugs (AEDs) are those which decrease the frequency and/or severity of seizures in
7/31/09. New AEDs. AEDs. Dr. Yotin Chinvarun M.D. Ph.D. Comprehensive Epilepsy and Sleep disorder Program PMK hospital. 1 st genera*on AEDs
 Dr. Yotin Chinvarun M.D. Ph.D. Comprehensive Epilepsy and Sleep disorder Program PMK hospital New AEDs AEDs NEW OLD Pregabalin Pregabalin 1 st genera*on AEDs Phenytoin Carbamazepine Valproate Phenobarbital
Dr. Yotin Chinvarun M.D. Ph.D. Comprehensive Epilepsy and Sleep disorder Program PMK hospital New AEDs AEDs NEW OLD Pregabalin Pregabalin 1 st genera*on AEDs Phenytoin Carbamazepine Valproate Phenobarbital
Epilepsy is one of the more common
 PART ONE An Overview of Medications Used in Epilepsy Parents, families and caregivers, as well as persons with epilepsy, frequently have questions about medications and often turn to the Internet for information
PART ONE An Overview of Medications Used in Epilepsy Parents, families and caregivers, as well as persons with epilepsy, frequently have questions about medications and often turn to the Internet for information
Modified release drug delivery system for antiepileptic drug (Formulation development and evaluation).
.") TITLE OF THE THESIS / RESEARCH: Modified release drug delivery system for antiepileptic drug (Formulation development and evaluation). INTRODUCTION: Epilepsy is a common chronic neurological disorder characterized
TITLE OF THE THESIS / RESEARCH: Modified release drug delivery system for antiepileptic drug (Formulation development and evaluation). INTRODUCTION: Epilepsy is a common chronic neurological disorder characterized
New AEDs in Uncontrolled seizures
 New AEDs in Uncontrolled seizures Uncontrolled seizures/epilepsy Intractable epilepsy, Refractory epilepsy, Pharmacoresistant epilepsy Dr. Suthida Yenjun Traditionally, referred to therapeutic failure
New AEDs in Uncontrolled seizures Uncontrolled seizures/epilepsy Intractable epilepsy, Refractory epilepsy, Pharmacoresistant epilepsy Dr. Suthida Yenjun Traditionally, referred to therapeutic failure
Neuromuscular Disease(2) Epilepsy. Department of Pediatrics Soochow University Affiliated Children s Hospital
 Epilepsy. Department of Pediatrics Soochow University Affiliated Children s Hospital") Neuromuscular Disease(2) Epilepsy Department of Pediatrics Soochow University Affiliated Children s Hospital Seizures (p130) Main contents: 1) Emphasize the clinical features of epileptic seizure and epilepsy.
Neuromuscular Disease(2) Epilepsy Department of Pediatrics Soochow University Affiliated Children s Hospital Seizures (p130) Main contents: 1) Emphasize the clinical features of epileptic seizure and epilepsy.
The Diagnostic Detective: Epilepsy
 The Diagnostic Detective: Epilepsy Some Facts About Epilepsy and Its Causes Seizures are the most common neurologic disorders affecting children 5% of children have a seizure during childhood There are
The Diagnostic Detective: Epilepsy Some Facts About Epilepsy and Its Causes Seizures are the most common neurologic disorders affecting children 5% of children have a seizure during childhood There are
TOP APS DRUGS - DIVALPROEX SODIUM BRAND NAME: DEPAKOTE (ER)
") divalproex sodium TOP APS DRUGS - DIVALPROEX SODIUM BRAND NAME: DEPAKOTE (ER) Pharmacodynamics study of what a drug does to the body Divalproex sodium is chemically compounded from sodium valproate and
divalproex sodium TOP APS DRUGS - DIVALPROEX SODIUM BRAND NAME: DEPAKOTE (ER) Pharmacodynamics study of what a drug does to the body Divalproex sodium is chemically compounded from sodium valproate and
Valproic acid. Brand Name: Depakene Drug Class: Opportunistic Infection and Other Drugs
 Brand Name: Depakene Drug Class: Opportunistic Infection and Other Drugs Drug Description Valproic acid is a carboxylic acid that increases gamma-amino butyric acid (GABA) levels in the central nervous
Brand Name: Depakene Drug Class: Opportunistic Infection and Other Drugs Drug Description Valproic acid is a carboxylic acid that increases gamma-amino butyric acid (GABA) levels in the central nervous
2. Antiepileptic Drugs INTRODUCTION
 2. Antiepileptic Drugs 89 2 Chapter 2 Antiepileptic Drugs Nathan L. Kanous II, PharmD and Barry E. Gidal, PharmD 1. INTRODUCTION 1.1. Epidemiology of Epilepsy Epilepsy is a chronic neurologic disorder
2. Antiepileptic Drugs 89 2 Chapter 2 Antiepileptic Drugs Nathan L. Kanous II, PharmD and Barry E. Gidal, PharmD 1. INTRODUCTION 1.1. Epidemiology of Epilepsy Epilepsy is a chronic neurologic disorder
Onfi (clobazam) Labeled Uses: Clobazam is used as adjuvant treatment of seizures from Lennox-Gastaut Syndrome. 1,2
 Labeled Uses: Clobazam is used as adjuvant treatment of seizures from Lennox-Gastaut Syndrome. 1,2") Onfi (clobazam) Brand Name: Onfi Generic Name: clobazam Manufacturer: Lundbeck Inc. Drug Class: Benzodiazepine Labeled Uses: Clobazam is used as adjuvant treatment of seizures from Lennox-Gastaut Syndrome.
Onfi (clobazam) Brand Name: Onfi Generic Name: clobazam Manufacturer: Lundbeck Inc. Drug Class: Benzodiazepine Labeled Uses: Clobazam is used as adjuvant treatment of seizures from Lennox-Gastaut Syndrome.
Antiepilepsy Drugs: Pharmacodynamics and Principles of Drug Selection
 Epilepsy Board Review Manual Statement of Editorial Purpose The Epilepsy Board Review Manual is a study guide for trainees and practicing physicians preparing for board examinations in epilepsy. Each manual
Epilepsy Board Review Manual Statement of Editorial Purpose The Epilepsy Board Review Manual is a study guide for trainees and practicing physicians preparing for board examinations in epilepsy. Each manual
SODIUM CHANNEL BLOCKERS IN THE 21 ST CENTURY. Professor Martin J Brodie University of Glasgow Glasgow, Scotland
 IN THE 21 ST CENTURY Professor Martin J Brodie University of Glasgow Glasgow, Scotland Eisai SODIUM CHANNEL BLOCKERS Declaration of interests UCB Pharma GlaxoSmithKline Lundbeck Takeda Advisory board,
IN THE 21 ST CENTURY Professor Martin J Brodie University of Glasgow Glasgow, Scotland Eisai SODIUM CHANNEL BLOCKERS Declaration of interests UCB Pharma GlaxoSmithKline Lundbeck Takeda Advisory board,
Prescribing and Monitoring Anti-Epileptic Drugs
 Prescribing and Monitoring Anti-Epileptic Drugs Mark Granner, MD Clinical Professor and Vice Chair for Clinical Programs Director, Iowa Comprehensive Epilepsy Program Department of Neurology University
Prescribing and Monitoring Anti-Epileptic Drugs Mark Granner, MD Clinical Professor and Vice Chair for Clinical Programs Director, Iowa Comprehensive Epilepsy Program Department of Neurology University
Valproate Case 3: Formulations Jose de Leon, MD
 Valproate Case 3: Formulations 2-12-16 Jose de Leon, MD 3.Valproate Case 3 Described in J Clin Psychiatry 2004;65:724-5 http://www.ncbi.nlm.nih.gov/pubmed/15163266 Pharmacological explanation provided
Valproate Case 3: Formulations 2-12-16 Jose de Leon, MD 3.Valproate Case 3 Described in J Clin Psychiatry 2004;65:724-5 http://www.ncbi.nlm.nih.gov/pubmed/15163266 Pharmacological explanation provided
Review of Anticonvulsant Medications: Traditional and Alternative Uses. Andrea Michel, PharmD, CACP
 Review of Anticonvulsant Medications: Traditional and Alternative Uses Andrea Michel, PharmD, CACP Objectives Review epidemiology of epilepsy Classify types of seizures Discuss non-pharmacologic and pharmacologic
Review of Anticonvulsant Medications: Traditional and Alternative Uses Andrea Michel, PharmD, CACP Objectives Review epidemiology of epilepsy Classify types of seizures Discuss non-pharmacologic and pharmacologic
Data from the World Health Organization suggest
 CONTINUING PHARMACY EDUCATION Review of the Newer Antiepileptic Drugs Angel Tidwell, PharmD; and Melanie Swims, PharmD, BCPS AUDIENCE This activity is designed for pharmacists, pharmacy directors, managed
CONTINUING PHARMACY EDUCATION Review of the Newer Antiepileptic Drugs Angel Tidwell, PharmD; and Melanie Swims, PharmD, BCPS AUDIENCE This activity is designed for pharmacists, pharmacy directors, managed
Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005
 Close this window to return to IVIS Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005 Hosted by: Reprinted in the IVIS website with the permission of the WSAVA anticonvulsant
Close this window to return to IVIS Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005 Hosted by: Reprinted in the IVIS website with the permission of the WSAVA anticonvulsant
OXCARBAZEPINE. THERAPEUTICS Brands Trileptal see index for additional brand names. Generic? Yes
 OXCARBAZEPINE THERAPEUTICS Brands Trileptal see index for additional brand names Generic? Yes Class Anticonvulsant, voltage-sensitive sodium channel antagonist Commonly Prescribed for (bold for FDA approved)
OXCARBAZEPINE THERAPEUTICS Brands Trileptal see index for additional brand names Generic? Yes Class Anticonvulsant, voltage-sensitive sodium channel antagonist Commonly Prescribed for (bold for FDA approved)
Introduction to. Pharmacokinetics. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Introduction to 1 Pharmacokinetics University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 2 Learning objectives Understand compartment models and how they effects
Introduction to 1 Pharmacokinetics University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 2 Learning objectives Understand compartment models and how they effects
Adjusting phenytoin dosage in complex patients: how to win friends and influence patient outcomes
 Adjusting phenytoin dosage in complex patients: how to win friends and influence patient outcomes Brian Hardy, PharmD, FCSHP, FCCP Coordinator Education and Clinical Programs Department of Pharmacy Sunnybrook
Adjusting phenytoin dosage in complex patients: how to win friends and influence patient outcomes Brian Hardy, PharmD, FCSHP, FCCP Coordinator Education and Clinical Programs Department of Pharmacy Sunnybrook
Anti-epileptic Drugs
 Anti-epileptic Drugs We will continue talking about epilepsy which is a chronic disease that has to be managed, so the treatment will be a management treatment, not a single day or week treatment we will
Anti-epileptic Drugs We will continue talking about epilepsy which is a chronic disease that has to be managed, so the treatment will be a management treatment, not a single day or week treatment we will
Chapter 15. Media Directory. Convulsion. Seizures. Epilepsy. Known Causes of Seizures. Drugs for Seizures
 Chapter 15 Drugs for Seizures Slide 43 Slide 45 Media Directory Diazepam Animation Valproic Acid Animation Upper Saddle River, New Jersey 07458 All rights reserved. Seizures Convulsion Abnormal or uncontrolled
Chapter 15 Drugs for Seizures Slide 43 Slide 45 Media Directory Diazepam Animation Valproic Acid Animation Upper Saddle River, New Jersey 07458 All rights reserved. Seizures Convulsion Abnormal or uncontrolled
2016 Treatment Algorithm for Generalized Convulsive Status Epilepticus (SE) in adults and children > 40 kg
 in adults and children > 40 kg") Yale New Haven Health Department of Pharmacy, Department of Neurology 2016 Treatment Algorithm for Generalized Convulsive Status Epilepticus (SE) in adults and children > 40 kg Guideline, YNHHS Original
Yale New Haven Health Department of Pharmacy, Department of Neurology 2016 Treatment Algorithm for Generalized Convulsive Status Epilepticus (SE) in adults and children > 40 kg Guideline, YNHHS Original
8/30/10. How to use Antiepileptic drugs properly. 3nd generation AEDs. Introduction. Introduction. Introduction. AEDs. Dr.Yotin Chinvarun M.D., Ph.D.
 Introduction How to use Antiepileptic drugs properly Modern treatment of seizures started in 1850 with the introduction of bromides, based on the theory that epilepsy was caused by an excessive sex drive
Introduction How to use Antiepileptic drugs properly Modern treatment of seizures started in 1850 with the introduction of bromides, based on the theory that epilepsy was caused by an excessive sex drive
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide. Revised: May 2009 LMT:2PI
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use LAMICTAL safely and effectively. See full prescribing information for LAMICTAL. LAMICTAL (lamotrigine)
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use LAMICTAL safely and effectively. See full prescribing information for LAMICTAL. LAMICTAL (lamotrigine)
Unit VIII Problem 7 Pharmacology: Principles of Management of Seizure Disorders
 Unit VIII Problem 7 Pharmacology: Principles of Management of Seizure Disorders - Terminologies: Anti-convulsants: they are used to control convulsions seen in certain types of epilepsy. Convulsions may
Unit VIII Problem 7 Pharmacology: Principles of Management of Seizure Disorders - Terminologies: Anti-convulsants: they are used to control convulsions seen in certain types of epilepsy. Convulsions may
RECENT MAJOR CHANGES Warnings and Precautions, Hemophagocytic
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use LAMICTAL safely and effectively. See full prescribing information for LAMICTAL. LAMICTAL (lamotrigine)
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use LAMICTAL safely and effectively. See full prescribing information for LAMICTAL. LAMICTAL (lamotrigine)
DOSAGE FORMS AND STRENGTHS Tablets: 25 mg, 100 mg, 150 mg, and 200 mg; scored. (3.1, 16)
") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use LAMOTRIGINE TABLETS safely and effectively. See full prescribing information for LAMOTRIGINE TABLETS.
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use LAMOTRIGINE TABLETS safely and effectively. See full prescribing information for LAMOTRIGINE TABLETS.
Done by: Rola Awad Presented to : Dr. Diana Malaeb Date: 28/2/2013
 Done by: Rola Awad Presented to : Dr. Diana Malaeb Date: 28/2/2013 1 Abbreviations AED: antiepileptic drug EEG: electroencephalography SJS: Stevens Johnson syndrome VA: Valproic acid GABA : Gamma amino
Done by: Rola Awad Presented to : Dr. Diana Malaeb Date: 28/2/2013 1 Abbreviations AED: antiepileptic drug EEG: electroencephalography SJS: Stevens Johnson syndrome VA: Valproic acid GABA : Gamma amino
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide. Revised: 11/2011
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use LAMICTAL safely and effectively. See full prescribing information for LAMICTAL. LAMICTAL (lamotrigine)
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use LAMICTAL safely and effectively. See full prescribing information for LAMICTAL. LAMICTAL (lamotrigine)
Generic Name (Brand Name) Available Strengths Formulary Limits. Primidone (Mysoline) 50mg, 250mg -- $
 Available Strengths Formulary Limits. Primidone (Mysoline) 50mg, 250mg -- $") MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Epilepsy P&T DATE: 2/15/2017 THERAPEUTIC CLASS: Neurologic Disorders REVIEW HISTORY: 2/16 LOB AFFECTED: Medi-Cal (MONTH/YEAR)
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Epilepsy P&T DATE: 2/15/2017 THERAPEUTIC CLASS: Neurologic Disorders REVIEW HISTORY: 2/16 LOB AFFECTED: Medi-Cal (MONTH/YEAR)
Anticonvulsant or Antiepileptic Drugs. Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan March, 2018
 Anticonvulsant or Antiepileptic Drugs Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan March, 2018 Anticonvulsant or Antiepileptic Drugs Seizure: an abnormal electrical activity,
Anticonvulsant or Antiepileptic Drugs Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan March, 2018 Anticonvulsant or Antiepileptic Drugs Seizure: an abnormal electrical activity,
Valproate Case 1: Pharmacokinetics Jose de Leon, MD
 Valproate Case 1: Pharmacokinetics 2-12-16 Jose de Leon, MD 1. Valproate Case 1 J Clin Psychopharmacology 2009;29:509-11 http://www.ncbi.nlm.nih.gov/pubmed/19745660 Educational Objectives At the conclusion
Valproate Case 1: Pharmacokinetics 2-12-16 Jose de Leon, MD 1. Valproate Case 1 J Clin Psychopharmacology 2009;29:509-11 http://www.ncbi.nlm.nih.gov/pubmed/19745660 Educational Objectives At the conclusion
Children Are Not Just Small Adults Choosing AEDs in Children
 Children Are Not Just Small Adults Choosing AEDs in Children Natrujee Wiwattanadittakun, MD Neurology division, Department of Pediatrics, Chiang Mai University Hospital, Chiang Mai University 20 th July,
Children Are Not Just Small Adults Choosing AEDs in Children Natrujee Wiwattanadittakun, MD Neurology division, Department of Pediatrics, Chiang Mai University Hospital, Chiang Mai University 20 th July,
APPENDIX K Pharmacological Management
 1 2 3 4 APPENDIX K Pharmacological Management Table 1 AED options by seizure type Table 1 AED options by seizure type Seizure type First-line AEDs Adjunctive AEDs Generalised tonic clonic Lamotrigine Oxcarbazepine
1 2 3 4 APPENDIX K Pharmacological Management Table 1 AED options by seizure type Table 1 AED options by seizure type Seizure type First-line AEDs Adjunctive AEDs Generalised tonic clonic Lamotrigine Oxcarbazepine
Epilepsy management What, when and how?
 Epilepsy management What, when and how? J Helen Cross UCL-Institute of Child Health, Great Ormond Street Hospital for Children, London, & National Centre for Young People with Epilepsy, Lingfield, UK What
Epilepsy management What, when and how? J Helen Cross UCL-Institute of Child Health, Great Ormond Street Hospital for Children, London, & National Centre for Young People with Epilepsy, Lingfield, UK What
Chapter 24 Antiseizures
 Chapter 24 1. Introduction Epilepsy is a heterogeneous symptom complex a chronic disorder characterized by recurrent seizures. Seizures are finite episodes of brain dysfunction resulting from abnormal
Chapter 24 1. Introduction Epilepsy is a heterogeneous symptom complex a chronic disorder characterized by recurrent seizures. Seizures are finite episodes of brain dysfunction resulting from abnormal
Epilepsy and EEG in Clinical Practice
 Mayo School of Professional Development Epilepsy and EEG in Clinical Practice November 10-12, 2016 Hard Rock Hotel at Universal Orlando Orlando, FL Course Directors Jeffrey Britton, MD and William Tatum,
Mayo School of Professional Development Epilepsy and EEG in Clinical Practice November 10-12, 2016 Hard Rock Hotel at Universal Orlando Orlando, FL Course Directors Jeffrey Britton, MD and William Tatum,
PEDIATRIC PHARMACOTHERAPY
 PEDIATRIC PHARMACOTHERAPY A Monthly Newsletter for Health Care Professionals from the Children s Medical Center at the University of Virginia Volume 7 Number 11 November 2001 A Oxcarbazepine Use in Children
PEDIATRIC PHARMACOTHERAPY A Monthly Newsletter for Health Care Professionals from the Children s Medical Center at the University of Virginia Volume 7 Number 11 November 2001 A Oxcarbazepine Use in Children
DRUGS THAT ACT IN THE CNS
 DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
LAMICTAL XR (lamotrigine) extended-release tablets, for oral use Initial U.S. Approval: 1994
 extended-release tablets, for oral use Initial U.S. Approval: 1994") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use LAMICTAL XR safely and effectively. See full prescribing information for LAMICTAL XR. LAMICTAL XR
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use LAMICTAL XR safely and effectively. See full prescribing information for LAMICTAL XR. LAMICTAL XR
Newer Anticonvulsants: Targets and Toxicity. Laura Tormoehlen, MD Neurology and EM-Toxicology
 Newer Anticonvulsants: Targets and Toxicity Laura Tormoehlen, MD Neurology and EM-Toxicology Disclosures No financial disclosures DEFINITIONS Objectives/Outline Mechanism of Action Specific Indications
Newer Anticonvulsants: Targets and Toxicity Laura Tormoehlen, MD Neurology and EM-Toxicology Disclosures No financial disclosures DEFINITIONS Objectives/Outline Mechanism of Action Specific Indications
Newer AEDs compared to LVT as adjunctive treatments for uncontrolled focal epilepsy. Dr. Yotin Chinvarun. M.D. Ph.D.
 Newer AEDs compared to LVT as adjunctive treatments for uncontrolled focal epilepsy Dr. Yotin Chinvarun. M.D. Ph.D. Chronology of antiepileptic drug introduction over the past 150 years 20 15 10 Perampanel
Newer AEDs compared to LVT as adjunctive treatments for uncontrolled focal epilepsy Dr. Yotin Chinvarun. M.D. Ph.D. Chronology of antiepileptic drug introduction over the past 150 years 20 15 10 Perampanel
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist
 and Glutamate (NMDA) Receptor Antagonist") Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Epilepsy 7/28/09! Definitions. Classification of epilepsy. Epidemiology of Seizures and Epilepsy. International classification of epilepsies
 Definitions Epilepsy Dr.Yotin Chinvarun M.D., Ph.D. Seizure: the clinical manifestation of an abnormal and excessive excitation of a population of cortical neurons Epilepsy: a tendency toward recurrent
Definitions Epilepsy Dr.Yotin Chinvarun M.D., Ph.D. Seizure: the clinical manifestation of an abnormal and excessive excitation of a population of cortical neurons Epilepsy: a tendency toward recurrent
Goals for sedation during mechanical ventilation
 New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
SEIZURE CONTROL * DAY & NIGHT
 SEIZURE CONTROL * DAY & NIGHT Equetro (carbamazepine) Extended-Release Capsules Approved for Use in Treating Epilepsy * *PLEASE SEE FOLLOWING PAGES FOR SPECIFIC INDICATIONS. PLEASE SEE IMPORTANT SAFETY
SEIZURE CONTROL * DAY & NIGHT Equetro (carbamazepine) Extended-Release Capsules Approved for Use in Treating Epilepsy * *PLEASE SEE FOLLOWING PAGES FOR SPECIFIC INDICATIONS. PLEASE SEE IMPORTANT SAFETY
PACKAGE LEAFLET: Information for the patient. DIAZEPAM Tablets 5 mg Solution for injection 10 mg / 2 ml (Diazepam)
") PACKAGE LEAFLET: Information for the patient DIAZEPAM Tablets 5 mg Solution for injection 10 mg / 2 ml (Diazepam) Read this leaflet carefully before you start taking this medicine. - Keep this leaflet.
PACKAGE LEAFLET: Information for the patient DIAZEPAM Tablets 5 mg Solution for injection 10 mg / 2 ml (Diazepam) Read this leaflet carefully before you start taking this medicine. - Keep this leaflet.
PACKAGE LEAFLET: INFORMATION FOR THE USER
 PACKAGE LEAFLET: INFORMATION FOR THE USER 250 mg film-coated tablets. 500 mg film-coated tablets. 750 mg film-coated tablets. 1000 mg film-coated tablets. Levetiracetam
PACKAGE LEAFLET: INFORMATION FOR THE USER 250 mg film-coated tablets. 500 mg film-coated tablets. 750 mg film-coated tablets. 1000 mg film-coated tablets. Levetiracetam
APPENDIX S. Removed sections from original guideline. 1.1 Pharmacological treatment Introduction
 00 0 APPENDIX S Removed sections from original guideline. Pharmacological treatment.. Introduction The evidence base for the newer AEDs (gabapentin, lamotrigine, levetiracetam, oxcarbazepine, tiagabine,
00 0 APPENDIX S Removed sections from original guideline. Pharmacological treatment.. Introduction The evidence base for the newer AEDs (gabapentin, lamotrigine, levetiracetam, oxcarbazepine, tiagabine,
Ernie Somerville Prince of Wales Hospital EPILEPSY
 Ernie Somerville Prince of Wales Hospital EPILEPSY Overview Classification New and old anti-epileptic drugs (AEDs) Neuropsychiatric side-effects Limbic encephalitis Non-drug therapies Therapeutic wishlist
Ernie Somerville Prince of Wales Hospital EPILEPSY Overview Classification New and old anti-epileptic drugs (AEDs) Neuropsychiatric side-effects Limbic encephalitis Non-drug therapies Therapeutic wishlist
4WS Neurology. Table of Contents
 4WS Neurology Table of Contents 1. Phenytoin Preparations... Page 2 Monitoring... Page 2 Therapeutic Range... Page 2 Loading Doses... Page 2 Maintenance Doses... Page 3 Sampling Times... Page 3 Dose Adjustment...
4WS Neurology Table of Contents 1. Phenytoin Preparations... Page 2 Monitoring... Page 2 Therapeutic Range... Page 2 Loading Doses... Page 2 Maintenance Doses... Page 3 Sampling Times... Page 3 Dose Adjustment...
When choosing an antiepileptic ... PRESENTATION... Pharmacokinetics of the New Antiepileptic Drugs. Based on a presentation by Barry E.
 ... PRESENTATION... Pharmacokinetics of the New Antiepileptic Drugs Based on a presentation by Barry E. Gidal, PharmD Presentation Summary A physician s choice of an antiepileptic drug (AED) usually depends
... PRESENTATION... Pharmacokinetics of the New Antiepileptic Drugs Based on a presentation by Barry E. Gidal, PharmD Presentation Summary A physician s choice of an antiepileptic drug (AED) usually depends
Psychotropic Medication
 Psychotropic Medication Part 3: Mood Stabilizers with Terry Broda MOOD STABILIZERS Carbolith, Duralith Depakene*, Epival*, Depakote* Lithium Valproic Acid, Divalproex Sodium Valproate Tegretol* Trileptal*
Psychotropic Medication Part 3: Mood Stabilizers with Terry Broda MOOD STABILIZERS Carbolith, Duralith Depakene*, Epival*, Depakote* Lithium Valproic Acid, Divalproex Sodium Valproate Tegretol* Trileptal*
LMMG New Medicine Recommendation
 LMMG New Medicine Recommendation Oxcarbazepine (Trileptal ) for the treatment of epilepsy LMMG Recommendation: Amber 0: Oxcarbazepine (Trileptal ) is recommended for use as monotherapy or adjunctive therapy
LMMG New Medicine Recommendation Oxcarbazepine (Trileptal ) for the treatment of epilepsy LMMG Recommendation: Amber 0: Oxcarbazepine (Trileptal ) is recommended for use as monotherapy or adjunctive therapy
SUMMARY OF PRODUCT CHARACTERISTICS FOR BENZODIAZEPINES AS ANXIOLYTICS OR HYPNOTICS
 SUMMARY OF PRODUCT CHARACTERISTICS FOR BENZODIAZEPINES AS ANXIOLYTICS OR HYPNOTICS Guideline Title Summary of Product Characteristics for Benzodiazepines as Anxiolytics or Hypnotics Legislative basis Directive
SUMMARY OF PRODUCT CHARACTERISTICS FOR BENZODIAZEPINES AS ANXIOLYTICS OR HYPNOTICS Guideline Title Summary of Product Characteristics for Benzodiazepines as Anxiolytics or Hypnotics Legislative basis Directive
Composition: Each tablet contain. Levocetirizine. Each 5ml contains. Montelukast. Pharmacokinetic properties:
 Composition: Each tablet contain Montelukast Levocetirizine 10mg 5mg Each 5ml contains Montelukast Levocetirizine 4mg 2.5mg Pharmacokinetic properties: Peak plasma concentrations of montelukast are achieved
Composition: Each tablet contain Montelukast Levocetirizine 10mg 5mg Each 5ml contains Montelukast Levocetirizine 4mg 2.5mg Pharmacokinetic properties: Peak plasma concentrations of montelukast are achieved
Optimizing Management of Seizure Disorders
 708 Medicine Update 121 Optimizing Management of Seizure Disorders V NAGARAJAN INTRODUCTION Seizure disorders are met with by every consultant in practice almost everyday. In the management of seizure
708 Medicine Update 121 Optimizing Management of Seizure Disorders V NAGARAJAN INTRODUCTION Seizure disorders are met with by every consultant in practice almost everyday. In the management of seizure
Lorazepam Tablets, USP
 Lorazepam Tablets, USP DESCRIPTION: Lorazepam, an antianxiety agent, has the chemical formula, 7-chloro-5-(o-chlorophenyl)-1,3-dihydro-3-hydroxy-2H -1,4-benzodiazepin-2-one: Cl H N N O Cl OH It is a white
Lorazepam Tablets, USP DESCRIPTION: Lorazepam, an antianxiety agent, has the chemical formula, 7-chloro-5-(o-chlorophenyl)-1,3-dihydro-3-hydroxy-2H -1,4-benzodiazepin-2-one: Cl H N N O Cl OH It is a white
Updated advice for nurses who care for patients with epilepsy
 NICE BULLETIN Updated advice for nurses who care for patients with epilepsy NICE provided the content for this booklet which is independent of any company or product advertised NICE BULLETIN Updated advice
NICE BULLETIN Updated advice for nurses who care for patients with epilepsy NICE provided the content for this booklet which is independent of any company or product advertised NICE BULLETIN Updated advice
TOPIRAMATE. THERAPEUTICS Brands Topamax Epitomax Topamac Topimax Trokendi XR Qsymia see index for additional brand names
 TOPIRAMATE THERAPEUTICS Brands Topamax Epitomax Topamac Topimax Trokendi XR Qsymia see index for additional brand names Generic? Yes (not for Qsymia) Class Anticonvulsant, voltage-sensitive sodium channel
TOPIRAMATE THERAPEUTICS Brands Topamax Epitomax Topamac Topimax Trokendi XR Qsymia see index for additional brand names Generic? Yes (not for Qsymia) Class Anticonvulsant, voltage-sensitive sodium channel
Epilepsy / Seizures EPI
 Epilepsy / Seizures EPI Epilepsy is a chronic condition, characterized by recurrent unprovoked seizures. It has several causes; it may be genetic or may occur in people who have a past history of birth
Epilepsy / Seizures EPI Epilepsy is a chronic condition, characterized by recurrent unprovoked seizures. It has several causes; it may be genetic or may occur in people who have a past history of birth
ANTIEPILEPTIC DRUGS. Hiwa K. Saaed, PhD. Department of Pharmacology & Toxicology College of Pharmacy University of Sulaimani
 ANTIEPILEPTIC DRUGS Hiwa K. Saaed, PhD Department of Pharmacology & Toxicology College of Pharmacy University of Sulaimani 2017-18 Antiepileptic drugs (AEDs) Definitions and Terminology Historical overview
ANTIEPILEPTIC DRUGS Hiwa K. Saaed, PhD Department of Pharmacology & Toxicology College of Pharmacy University of Sulaimani 2017-18 Antiepileptic drugs (AEDs) Definitions and Terminology Historical overview
LAMICTAL GlaxoSmithKline
 LAMICTAL GlaxoSmithKline Lamotrigine QUALITATIVE AND QUANTITATIVE COMPOSITION Tablets: LAMICTAL, 25, 50, 100 and 200 mg. Dispersible/Chewable Tablets: LAMICTAL, 2, 5, 25, 50, 100 and 200 mg. PHARMACEUTICAL
LAMICTAL GlaxoSmithKline Lamotrigine QUALITATIVE AND QUANTITATIVE COMPOSITION Tablets: LAMICTAL, 25, 50, 100 and 200 mg. Dispersible/Chewable Tablets: LAMICTAL, 2, 5, 25, 50, 100 and 200 mg. PHARMACEUTICAL
Pediatric patients 2 years and older with partial onset seizures, primary generalized tonic-clonic LGS (2.1) Migraine (2.2) 400 mg once daily
 Migraine (2.2) 400 mg once daily") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use TOPIRAMATE EXTENDED-RELEASE CAPSULES safely and effectively. See full prescribing information for
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use TOPIRAMATE EXTENDED-RELEASE CAPSULES safely and effectively. See full prescribing information for
AN UPDATE ON ANTIEPILEPTIC AGENTS: FOCUS ON AN UPDATE ON ANTIEPILEPTIC AGENTS: FOCUS ON SECOND GENERATION TREATMENT OPTIONS
 Volume 24, Issue 1 October 2008 AN UPDATE ON ANTIEPILEPTIC AGENTS: FOCUS ON SECOND GENERATION TREATMENT OPTIONS Jason Richey, Pharm.D. Candidate Epilepsy is a neurological disorder characterized by sudden
Volume 24, Issue 1 October 2008 AN UPDATE ON ANTIEPILEPTIC AGENTS: FOCUS ON SECOND GENERATION TREATMENT OPTIONS Jason Richey, Pharm.D. Candidate Epilepsy is a neurological disorder characterized by sudden
Epilepsy characterized by recurrent and unprovoked
 Literature Review New Antiepileptic Agents Linda P. Nelson, DMD, MScD Ilse Savelli-Castillo, DDS Dr. Nelson is associate in dentistry, Department of Pediatric Dentistry, Children s Hospital, and is assistant
Literature Review New Antiepileptic Agents Linda P. Nelson, DMD, MScD Ilse Savelli-Castillo, DDS Dr. Nelson is associate in dentistry, Department of Pediatric Dentistry, Children s Hospital, and is assistant
Opinion 24 July 2013
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 24 July 2013 FYCOMPA 2 mg, film-coated tablet B/7 (CIP: 34009 267 760 0 8) B/28 (CIP: 34009 268 447 4 5) FYCOMPA 4
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 24 July 2013 FYCOMPA 2 mg, film-coated tablet B/7 (CIP: 34009 267 760 0 8) B/28 (CIP: 34009 268 447 4 5) FYCOMPA 4
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Absence seizures, 6 in childhood, 95 Adults, seizures and status epilepticus in, management of, 34 35 with first-time seizures. See Seizure(s),
Index Note: Page numbers of article titles are in boldface type. A Absence seizures, 6 in childhood, 95 Adults, seizures and status epilepticus in, management of, 34 35 with first-time seizures. See Seizure(s),
DEPAKOTE ER DIVALPROEX SODIUM EXTENDED-RELEASE TABLETS R x Only
 Page 1 (No. 3826 and, 7126) 03-5235-R4-Rev. December, 2002 NEW DEPAKOTE ER DIVALPROEX SODIUM EXTENDED-RELEASE TABLETS R x Only BOX WARNING: HEPATOTOXICITY: HEPATIC FAILURE RESULTING IN FATALITIES HAS OCCURRED
Page 1 (No. 3826 and, 7126) 03-5235-R4-Rev. December, 2002 NEW DEPAKOTE ER DIVALPROEX SODIUM EXTENDED-RELEASE TABLETS R x Only BOX WARNING: HEPATOTOXICITY: HEPATIC FAILURE RESULTING IN FATALITIES HAS OCCURRED
Contact: Daina Basile FOR IMMEDIATE RELEASE Kovak-Likly Communications ,
 Contact: Daina Basile FOR IMMEDIATE RELEASE Kovak-Likly Communications 203-762-8833, dbasile@klcpr.com FDA APPROVES EXPANDED INDICATION FOR QUDEXY XR (TOPIRAMATE) EXTENDED-RELEASE CAPSULES WITHIN THE PEDIATRIC
Contact: Daina Basile FOR IMMEDIATE RELEASE Kovak-Likly Communications 203-762-8833, dbasile@klcpr.com FDA APPROVES EXPANDED INDICATION FOR QUDEXY XR (TOPIRAMATE) EXTENDED-RELEASE CAPSULES WITHIN THE PEDIATRIC
Epidiolex (cannabidiol) NEW PRODUCT SLIDESHOW
 NEW PRODUCT SLIDESHOW") Epidiolex (cannabidiol) NEW PRODUCT SLIDESHOW Introduction Brand name: Epidiolex Generic name: Cannabidiol Pharmacological class: Cannabinoid Strength and Formulation: 100mg/mL; oral soln; strawberry-flavored;
Epidiolex (cannabidiol) NEW PRODUCT SLIDESHOW Introduction Brand name: Epidiolex Generic name: Cannabidiol Pharmacological class: Cannabinoid Strength and Formulation: 100mg/mL; oral soln; strawberry-flavored;
Increase dose weekly by increments of 50 mg for first 4 weeks then 100 mg for weeks 5 to 6. Adults and pediatric. 100 mg once. 50 mg orally once daily
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use TROKENDI XR safely and effectively. See full prescribing information for TROKENDI XR. TROKENDI XR
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use TROKENDI XR safely and effectively. See full prescribing information for TROKENDI XR. TROKENDI XR
Levocetirizine dihydrochloride
 INSERT TEXT UAP Levocetirizine dihydrochloride Allerzet 5 mg Tablet Antihistamine FORMULATION Each film-coated tablet contains: Levocetirizine dihydrochloride.. 5 mg PRODUCT DESCRIPTION Levocetirine 5
INSERT TEXT UAP Levocetirizine dihydrochloride Allerzet 5 mg Tablet Antihistamine FORMULATION Each film-coated tablet contains: Levocetirizine dihydrochloride.. 5 mg PRODUCT DESCRIPTION Levocetirine 5
400 mg once daily. Once daily doses based on weight (Table 2) 200 mg to 400 mg once daily. 400 mg once daily. 5 mg/kg to 9 mg/kg once daily
 200 mg to 400 mg once daily. 400 mg once daily. 5 mg/kg to 9 mg/kg once daily") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use QUDEXY XR safely and effectively. See full prescribing information for QUDEXY XR. QUDEXY XR (topiramate)
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use QUDEXY XR safely and effectively. See full prescribing information for QUDEXY XR. QUDEXY XR (topiramate)
PRODUCT MONOGRAPH. Lamotrigine Tablets. 25 mg, 100 mg and 150 mg. Antiepileptic. 1 President's Choice Circle March 22, 2017 Brampton, Ontario L6Y 5S5
 PRODUCT MONOGRAPH Pr LAMOTRIGINE Lamotrigine Tablets 25 mg, mg and 5 mg Antiepileptic SANIS HEALTH INC. Date of Revision: President's Choice Circle March 22, 27 Brampton, Ontario L6Y 5S5 Control Number:
PRODUCT MONOGRAPH Pr LAMOTRIGINE Lamotrigine Tablets 25 mg, mg and 5 mg Antiepileptic SANIS HEALTH INC. Date of Revision: President's Choice Circle March 22, 27 Brampton, Ontario L6Y 5S5 Control Number:
EPILEPSY DIAGNOSIS. Investigations- EEG, MRI, CT, blood tests. Appendix 1 contains a guide to questions to help with diagnosis
 EPILEPSY DIAGNOSIS All adults with a recent-onset suspected seizure should be seen urgently by a specialist. The seizure type(s) and epilepsy syndrome, aetiology and co-morbidity should be determined.
EPILEPSY DIAGNOSIS All adults with a recent-onset suspected seizure should be seen urgently by a specialist. The seizure type(s) and epilepsy syndrome, aetiology and co-morbidity should be determined.
25 mg, 100 mg and 150 mg Tablets. Antiepileptic. 150 Signet Drive November 01, 2018 Toronto Ontario M9L 1T9 Control #:
 PRODUCT MONOGRAPH Pr APO-LAMOTRIGINE Lamotrigine Tablets 25 mg, 100 mg and 150 mg Tablets Antiepileptic APOTEX INC. DATE OF REVISION: 150 Signet Drive November 01, 2018 Toronto Ontario M9L 1T9 Control
PRODUCT MONOGRAPH Pr APO-LAMOTRIGINE Lamotrigine Tablets 25 mg, 100 mg and 150 mg Tablets Antiepileptic APOTEX INC. DATE OF REVISION: 150 Signet Drive November 01, 2018 Toronto Ontario M9L 1T9 Control
On completion of this chapter you should be able to: list the most common types of childhood epilepsies and their symptoms
 9 Epilepsy The incidence of epilepsy is highest in the first two decades of life. It falls after that only to rise again in late life. Epilepsy is one of the most common chronic neurological condition
9 Epilepsy The incidence of epilepsy is highest in the first two decades of life. It falls after that only to rise again in late life. Epilepsy is one of the most common chronic neurological condition
Epilepsy adjunctive therapy: pediatric patients with partial onset seizures, primary generalized tonic-clonic seizures or.
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use TOPIRAMATE tablets safely and effectively. See full prescribing information for TOPIRAMATE tablets.
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use TOPIRAMATE tablets safely and effectively. See full prescribing information for TOPIRAMATE tablets.
KEVEYIS (dichlorphenamide) tablets, for oral use Initial U.S. Approval: 1958
 tablets, for oral use Initial U.S. Approval: 1958") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use KEVEYIS safely and effectively. See full prescribing information for KEVEYIS. KEVEYIS (dichlorphenamide)
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use KEVEYIS safely and effectively. See full prescribing information for KEVEYIS. KEVEYIS (dichlorphenamide)