Anti Tuberculosis Medications: Side Effects & adverse Events
|
|
|
- Dwight Brown
- 5 years ago
- Views:
Transcription

1 Anti Tuberculosis Medications: Side Effects & adverse Events Diana Fortune, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Diana Fortune, RN, BSN has the following disclosures to make: No conflict of interests No relevant financial relationships with any commercial companies pertaining to this educational activity 1




2 Diana Fortune RN BSN TB Program Manager New Mexico Department of Health No relevant financial relationship with any commercial companies pertaining to this educational activity 2
3 Describe the monitoring process for adverse drug events Discuss side effects and drug toxicities Recognize the most common adverse drug events Discuss the nursing interventions and medical management of the most common adverse drug events Case Studies Cure the individual patient Minimize the risk of death & disability Reduce the transmission of TB to others NOTE: Responsibility of successful treatment is assigned to the health care provider NOT THE PATIENT 3
: the first new class of drugs to obtain FDA approval for TB")

4 Source: CDC Core Curriculum 2013; Chapter 6 pg 152 Bedaquiline (Sirturo): the first new class of drugs to obtain FDA approval for TB in 40 years (for use in MDR only cases) INH, Rifampin, PZA and EMB + Vitamin B6 The first-line anti-tb drugs Core of standard treatment regimens 4



5 Gastrointestinal (GI) Dermatologic reactions Systemic hypersensitive reactions Hematologic abnormalities Neurotoxicity Ototoxicity Ophthalmic toxicity Nephrotoxicity Musculoskeletal Endocrine Drug/Drug Interactions 5
6 Source: CDC Core Curriculum on Tuberculosis: What the Clinician should Know 2013 Chapter 6 pg. 180 Patient education & charting of education If it wasn t charted it wasn t! Really explain to patient that there will be side effects to the medications - but you will work with them to manage those side effects Nurse Case Manager every patient should be assigned a nurse case manager!! NCM is accountable all aspects of patient s care DOT: standard of care for treatment of TBD Incentives & Enablers don t forget to use! Fixed-Dose Combinations 6






7 Medical History MD/RN evaluation Chest x-ray Sputum Specimen HIV Testing Toxicity assessment Vision screenings Hearing screenings Weight CMP AST, ALT, Alk. Phos. T. Bili. Creat. CBC Platelet Initial Assessment requires that we collect thorough baseline Medical history Co-morbidities Medication list Social history TB history Signs & Symptoms Have symptoms improved/worsened? Daily Monitoring DOT log Assess tolerance to meds daily by nurse or outreach worker Side effects Adverse drug reactions Monthly Toxicity checks Assess patient, get updates, and modify regimen if needed 7
8 Which anti-tb medication has the potential of causing hepatotoxicity? A. INH B. Rifampin C. PZA D. All of the above Which anti-tb medication has the potential of causing hepatotoxicity? A. INH B. Rifampin C. PZA D. All of the above 8
9 Which anti-tb medication has the potential of causing hepatotoxicity? A. INH B. Rifampin C. PZA D. All of the above INH G.I. upset Hepatotoxicity Peripheral neuropathy Mild CNS Toxicity PZA G.I. upset Hepatotoxicity Arthralgias Gout (rare Rifampin G.I. upset Hepatotoxicity Thrombocytopenia, hemolytic anemia Renal toxicity Flu-like syndrome Orange staining of body fluids Ethambutol Optic Neuritis Rifabutin /Skin discoloration Hepatotoxicity Leukopenia Thrombocytopenia Uveitis Arthralgias 9
10 Amikacin Rash Renal toxicity Ototoxicity Vestibular toxicity Electrolyte abnormalities (hypokalemia, hypomagnesemia) Local Pain at the injection site Levofloxacin, Gatifloxacin, Moxifloxacin GI upset Hepatotoxicity (rare) Mild CNS toxicity Arthralgias, rare tendon rupture Photosensitivity EKG abnormalities Capreomycin Renal Toxicity Ototoxicity Vestibular Toxicity Electrolyte abnormalities (hypokalemia, hypocalcemia, hypomagnesemia) Local pain at the injection site Ethionamide GI upset, may be significant Hepatotoxicity Endocrine effects (gynecomastia, hair loss, acne, impotence, menstrual irregularity, reversible hypothyroidism) Peripheral neuropathy Cycloserine CNS toxicity, may include seizure, depression, suicidal ideation,psychosis Peripheral neuropathy Skin changes (lichenoid eruptions, Stevens-Johnson Syndrome) Para-Aminosalicylate (PAS) G.I. upset, may be significant Hepatoxicity Reversible hypothyroidism Clofazamine G.I. upset Discoloration and dryness of skin Photosensitivity Retinopathy Linezolid Myelosuppression Nausea and Diarrhea Optic neuropathy Peripheral neuropathy 10
11 Case Study: Hepatotoxicity 38 year old male diagnosed with pulmonary TB. Baseline labs indicated ALT 38, AST 25, Alk. Phosphatase 37, T. bili 0.5. On Mar. 13, 2012 he started standard RIPE regimen. He received medication by daily DOT that was provided by the local health department On May 15, 2012 (approx. 2 mos. later) susceptibility results indicated the isolate was pan susceptible, so EMB was discontinued. PZA was also discontinued because he had already taken 2 mos. of PZA He was continued on INH & Rifampin BIW (no longer recommended) On June 4, 2012 (approx. 3 months after starting anti TB therapy) follow-up lab results were ALT 97, AST 304, Alk phosphatase 72, T. bili 0.8. He was asymptomatic for signs of hepatitis 11
12 Baseline LFT s : ALT 38, AST 25, Alk Phos 37, T. bili 0.5. Follow up LFT s : ALT 97, AST 304, Alk phos 72, T. bili 0.8 What do we do? Normal Values: AST: u/l ALT: u/l Alk. Phos: u/l T. Bili. : ng/dl AST <5 x uln = mild toxicity AST 5-10 x uln = moderate toxicity AST >10 x uln = severe toxicity Continue therapy AST <5 x upper limit of normal and no signs /symptoms of hepatitis 20% of patients on standard therapy have asymptomatic elevation in LFT s Stop therapy AST > 5 times upper limit of normal with/ without symptoms AST > 3 times upper limit of normal with symptoms 12
13 As the nurse managing this patients anti-tb therapy, what are you going to do? Hold all TB meds!!! Probable drug induced liver injury Cannot restart anti-tb therapy until LFT s < 2 times upper limit of normal Re-challenge medications Introduce one drug at a time Monitor enzymes carefully Stop therapy if symptomatic or increased enzymes and eliminate last drug added from regimen 13
14 Underlying liver disease Clarify preexisting conditions that may increase risk of hepatotoxicity Hepatitis B and C Alcoholics Take a good social history Ask specific questions about daily ETOH use Immediate (4 months) post-partum period Those on other hepatotoxic medications Prescribed Over the counter Most importantly: Instruct patient to stop taking TB medications immediately and seek medical attention if symptoms of hepatitis occur again. 14

15 What anti-tb medications place the patient at risk for vision related toxicities? A. Rifampin B. Ethambutol C. Linezolid D. B & C only E. All of the above 15
16 What anti-tb medications place the patient at risk for vision related toxicities? A. Rifampin B. Ethambutol C. Linezolid D. B & C E. All of the above INH G.I. upset Hepatotoxicity Peripheral neuropathy Mild CNS Toxicity PZA G.I. upset Hepatotoxicity Arthralgias Gout (rare Rifampin G.I. upset Hepatotoxicity Thrombocytopenia, hemolytic anemia Renal toxicity Flu-like syndrome Orange staining of body fluids Ethambutol Optic Neuritis Rifabutin /Skin discoloration Hepatotoxicity Leukopenia Thrombocytopenia Uveitis Arthralgias Streptomycin (no longer considered a first line drug) 16
17 Cycloserine CNS toxicity, may include seizure, depression, suicidal ideation,psychosis Peripheral neuropathy Skin changes (lichenoid eruptions, Stevens-Johnson Syndrome) Para-Aminosalicylate (PAS) G.I. upset, may be significant Hepatoxicity Reversible hypothyroidism Clofazamine G.I. upset Discoloration and dryness of skin Photosensitivity Retinopathy Linezolid Myelosuppression Nausea and Diarrhea Optic neuropathy Peripheral neuropathy 17
18 21 year old male arrested and incarcerated in county jail in February After being incarcerated for 3 months he began to complain of fever, chills, productive cough, chest pain, night sweats, and weight loss. He was evaluated and given a cough suppressant. 8 mos later, on October 7, 2010, he continued to have complaints of same symptoms. He was evaluated again. This time a chest x-ray & a sputum collection was done. His chest x-ray showed left upper lobe cavitary infiltrate, and the sputum specimen was AFB smear (+) 1-10 per high power field. He was diagnosed with active pulmonary TB and started on a standard 4 drug regimen on October 12, 2010 He was responding to anti-therapy. He was afebrile, had 6 lb wt. gain, night sweats had resolved, and cough was improving InNovember 2010, an isolate was reported as isoniazid and streptomycin resistant. INH was discontinued once susceptibilities were known, and he continued on a modified regimen with RIF, PZA, EMB with a plan to treat for 9 months In January 2011, he was released from jail and he started c/o difficulty driving and reading road signs (he has now been on anti-tb therapy for 3 months). As a nurse managing this patient s anti-tb therapy, what would you do? Review his anti-tb therapy RIPE started Oct. 10, 2010 In Nov he was switched to RIF, PZA, EMB Which anti-tb medication is contributing to his vision problems? Ethambutol What do we do now? Evaluate further (snellen & Ishihara) Hold EMB Refer to the Opthalmologist 18
19 The nurse managing his case did not re-assess him. She sent him to his eye doctor. A few weeks later he was seen by optometrist, and given RX for corrective lenses. EMB continued On May 3 he complains of worsening vision (he s been c/o vision problems for 4 months) Nurse assessed his vision. Baseline visual acuity in October was 20/20 both eyes, follow up visual acuity was now 20/200 in both eyes On May 5 the EMB discontinued; continued on RIF, PZA and Levo added to regimen to complete 9 mos of treatment and he was referred to a retinal specialist. 19
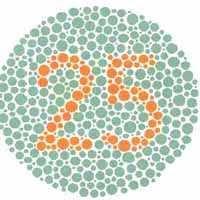
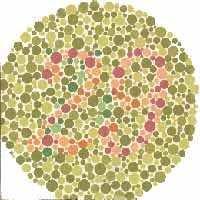
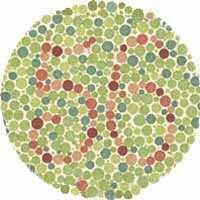
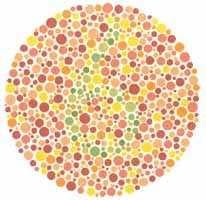
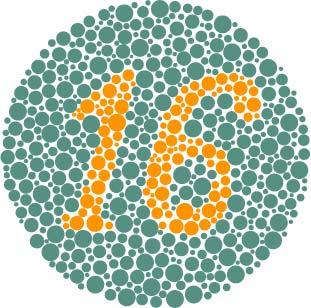
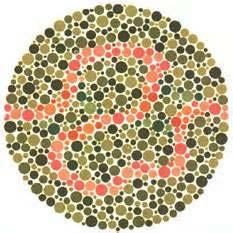
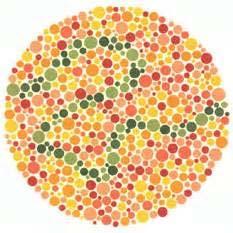
20 Ishihara Testing Snellen Eye Exam Designed to give quick & accurate assessment of color vision Most effectively done in room with adequate daylight Held 75 cm from the patient (approx. arm length) Sit & tilt plate at right angle to patients line of vision Screen all plates Must pass 10 of 11 plates to be regarded as Normal If unable to read numerals use winding lines and have patient trace between the 2 X s with a finger 20
21 21



22 Document Baseline Document monthly Screen all plates Mark (X) if plate cannot be read Must pass 10 of first 11 plates for test to be regarded as normal Refer for evaluation if 7 or less plates are read as normal Place Snellen Chart on wall Measure 20 feet from wall to where chart is placed & mark line on floor Have patient stand on marked line Have patient cover one eye with an eye cover Have the patient read letters aloud If patient misses only one letter have them continue reading the next line Record the last line the patient reads accurately Note the visual acuity measures marked at the end of each row of letters Ask patient to repeat the process with the other eye Then repeat with both eyes Each time, recording the last line patient reads You are recording the visual acuity for each eye and with both eyes uncovered 22

23 If initial screen was conducted with corrective lenses (glasses/contacts), follow-up screens must be done the same. Change of 1 or more lines from initial screen in either one or both eyes must be reported to physician immediately Which of the following aniti-tb medications requires that you monitor the patients hearing? A. Amikacin B. Rifampin C. Capreomycin D. Both A & C E. All of the above 23
24 Which of the following aniti-tb medications requires that you monitor the patients hearing? A. Amikacin B. Rifampin C. Capreomycin D. Both A & C E. All of the above Amikacin Rash Renal toxicity Ototoxicity Vestibular toxicity Electrolyte abnormalities (hypokalemia, hypomagnesemia) Local Pain at the injection site Levofloxacin, Gatifloxacin, Moxifloxacin GI upset Hepatotoxicity (rare) Mild CNS toxicity Arthralgias, rare tendon rupture Photosensitivity EKG abnormalities Capreomycin Renal Toxicity Ototoxicity Vestibular Toxicity Electrolyte abnormalities (hypokalemia, hypocalcemia, hypomagnesemia) Local pain at the injection site Ethionamide GI upset, may be significant Hepatotoxicity Endocrine effects (gynecomastia, hair loss, acne, impotence, menstrual irregularity, reversible hypothyroidism) Peripheral neuropathy 24





25 Baseline Identify pre-existing hearing loss Repeat monthly Refer for evaluation if any decrease from baseline Nurses may need to complete an audiometer training course and have certification 25

26 CDC Core Curriculum on TB: What the Clinician Should Know; 5 th edition TB Nursing: A Comprehensive Guide to Patient Care; 2 nd Edition Drug- Resistant TB: A Survival Guide for Clinicians; 2 nd Edition; Curry International TB Center TB Drug Information Guide 2 nd Edition; Curry International TB Center etails.cfm?productid=wpt-17a 26
Debbie Onofre, RN, BSN March 18, TB Nurse Case Management March 17 19, 2015 San Antonio, Texas
 Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Debbie Onofre, RN, BSN March 18, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION
Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Debbie Onofre, RN, BSN March 18, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION
TB Nurse Case Management San Antonio, TX. TB Medications and Adverse Effects
 TB Nurse Case Management San Antonio, TX April 1 3, 2014 TB Medications and Adverse Effects Debbie Onofre RN, BSN Nurse Consultant/ Nurse Educator Heartland National TB Center April 1, 2014 Debbie Onofre,
TB Nurse Case Management San Antonio, TX April 1 3, 2014 TB Medications and Adverse Effects Debbie Onofre RN, BSN Nurse Consultant/ Nurse Educator Heartland National TB Center April 1, 2014 Debbie Onofre,
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Managing Anti-TB Therapy Side Effects and Complications Lisa Armitige, MD, PhD May 9, 2012 Lisa Armitige, MD, PhD has the following
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Managing Anti-TB Therapy Side Effects and Complications Lisa Armitige, MD, PhD May 9, 2012 Lisa Armitige, MD, PhD has the following
TB Nurse Case Management
 TB Nurse Case Management San Antonio, Texas March 2-4, 2011 TB Medications and Adverse Effects Debbie Onofre, RN, BSN March 3, 2011 Debbie Onofre, RN, BSN has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas March 2-4, 2011 TB Medications and Adverse Effects Debbie Onofre, RN, BSN March 3, 2011 Debbie Onofre, RN, BSN has the following disclosures to make: No conflict
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014
 Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Monitoring Patients for TB Adverse Reactions and Managing Side Effects Catalina Navarro, RN, BSN April 11, 2014 Catalina Navarro, RN,
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Monitoring Patients for TB Adverse Reactions and Managing Side Effects Catalina Navarro, RN, BSN April 11, 2014 Catalina Navarro, RN,
Tuberculosis medications: adverse drug reactions
 Tuberculosis medications: adverse drug reactions Rajesh M. Prabhu, M.D. Infectious Diseases Essentia Health, Duluth, MN July 25, 2017 2014 MFMER slide-1 No Finanial Disclosures Learning Objectives 1. Describe
Tuberculosis medications: adverse drug reactions Rajesh M. Prabhu, M.D. Infectious Diseases Essentia Health, Duluth, MN July 25, 2017 2014 MFMER slide-1 No Finanial Disclosures Learning Objectives 1. Describe
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Standard TB Treatment
 Standard TB Treatment Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
Standard TB Treatment Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015
 Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 Initiation Phase Part 1 Ginny Dowell, RN, BSN February 4, 2015 Ginny Dowell RN, BSN has the following disclosures to make:
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 Initiation Phase Part 1 Ginny Dowell, RN, BSN February 4, 2015 Ginny Dowell RN, BSN has the following disclosures to make:
Managing the Patients Response to TB Treatment
 Managing the Patients Response to TB Treatment Barbarah Martinez, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Barbarah Martinez, RN, BSN has
Managing the Patients Response to TB Treatment Barbarah Martinez, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Barbarah Martinez, RN, BSN has
Treatment of Tuberculosis
 TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
Drug Side Effects and Toxicity
 Drug Side Effects and Toxicity Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Toxicity Nausea and vomiting Any Drug Can Cause
Drug Side Effects and Toxicity Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Toxicity Nausea and vomiting Any Drug Can Cause
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015
 Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 TB Medications and Adverse Drug Events Presented by Evelyn Drzymala, RN, BSN February 11, 2015 Evelyn Drzymala, RN, BSN has
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 TB Medications and Adverse Drug Events Presented by Evelyn Drzymala, RN, BSN February 11, 2015 Evelyn Drzymala, RN, BSN has
TB Grand Rounds. Reynard McDonald, MD & Henry Fraimow, MD January 30, Outline
 TB Grand Rounds Reynard McDonald, MD & Henry Fraimow, MD January 30, 2007 Outline Overview of 2006 ATS statement regarding hepatotoxicity of anti-tb therapy Case examples highlighting management of patients
TB Grand Rounds Reynard McDonald, MD & Henry Fraimow, MD January 30, 2007 Outline Overview of 2006 ATS statement regarding hepatotoxicity of anti-tb therapy Case examples highlighting management of patients
Medication Administration and Adverse Reactions Alisha Blair, LVN September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Medication Administration and Adverse Reactions Alisha Blair, LVN September 28, 2011 Alisha Blair, LVN, has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Medication Administration and Adverse Reactions Alisha Blair, LVN September 28, 2011 Alisha Blair, LVN, has the following disclosures to make:
6/8/2018 TB TREATMENT. Bijan Ghassemieh, MD Seattle TB Clinical Intensive Disclosures. None
 TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
Drug Interactions Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
DRUG SIDE EFFECTS AND TOXICITY
 DRUG SIDE EFFECTS AND TOXICITY Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Objectives After participating in this lecture,
DRUG SIDE EFFECTS AND TOXICITY Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Objectives After participating in this lecture,
Shu-Hua Wang, MD, MPH &TM Assistant Professor of Medicine The Ohio State University
 Shu-Hua Wang, MD, MPH &TM Assistant Professor of Medicine The Ohio State University For anti-tuberculosis medications: Describe clinical monitoring for adverse drug reactions Review specific drug side
Shu-Hua Wang, MD, MPH &TM Assistant Professor of Medicine The Ohio State University For anti-tuberculosis medications: Describe clinical monitoring for adverse drug reactions Review specific drug side
Treatment: First Line Drugs TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS TREATMENT: GENERAL PRINCIPLES MECHANISM OF ACTION MID 27
 TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS Treatment: First Line Drugs 1. ISONIAZID = INH Bacteriocidal against dividing organisms Dose = 300mg = one pill = well absorbed Good CNS penetration Can be
TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS Treatment: First Line Drugs 1. ISONIAZID = INH Bacteriocidal against dividing organisms Dose = 300mg = one pill = well absorbed Good CNS penetration Can be
Dose Counting Exercise Elizabeth Foy, RN, BSN September 8, 2016
 Dose Counting Exercise Elizabeth Foy, RN, BSN September 8, 2016 TB Nurse Case Management September 7-9, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Jessica Quintero, M.Ed., has the following disclosures
Dose Counting Exercise Elizabeth Foy, RN, BSN September 8, 2016 TB Nurse Case Management September 7-9, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Jessica Quintero, M.Ed., has the following disclosures
Treatment of Active Tuberculosis
 Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Iris Barrera, RN April 11, 2018
 Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Iris Barrera, RN April 11, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Iris Barrera,
Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Iris Barrera, RN April 11, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Iris Barrera,
Dana G. Kissner, MD Detroit Department of Health & Wellness Promotion Wayne State University
 Dana G. Kissner, MD Detroit Department of Health & Wellness Promotion Wayne State University I reply to those who urge me to take medicine that they should wait at least until I am restored to my strength
Dana G. Kissner, MD Detroit Department of Health & Wellness Promotion Wayne State University I reply to those who urge me to take medicine that they should wait at least until I am restored to my strength
Peter Mere Latham English physician & educator
 Poisons and medicine are oftentimes the same substance given with different intents Dana G. Kissner, MD Detroit Department of Health & Wellness Promotion Wayne State University Peter Mere Latham 1789-1875
Poisons and medicine are oftentimes the same substance given with different intents Dana G. Kissner, MD Detroit Department of Health & Wellness Promotion Wayne State University Peter Mere Latham 1789-1875
TB Nurse Case Management San Antonio, Texas
 TB Nurse Case Management San Antonio, Texas April 1 3, 2014 Practicum: Monitoring Side Effects & Identifying Toxicities Dawn Farrell, BSN., RN. Texas Center for Infectious Disease Nurse Educator / Training
TB Nurse Case Management San Antonio, Texas April 1 3, 2014 Practicum: Monitoring Side Effects & Identifying Toxicities Dawn Farrell, BSN., RN. Texas Center for Infectious Disease Nurse Educator / Training
Anti Tuberculosis Medications
 Anti Tuberculosis Medications Mary Ann Rodriguez, MD March 8, 2017 TB Nurse Case Management March 7 9, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Mary Ann Rodriguez, MD has the following disclosures
Anti Tuberculosis Medications Mary Ann Rodriguez, MD March 8, 2017 TB Nurse Case Management March 7 9, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Mary Ann Rodriguez, MD has the following disclosures
Case Management of the TB/HIV Infected Patient
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric TB: Treatment of Tuberculosis Disease Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [with help from Andrea Cruz, M.D.] Objectives At the end
Advanced Concepts in Pediatric TB: Treatment of Tuberculosis Disease Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [with help from Andrea Cruz, M.D.] Objectives At the end
TB Nurse Assessment. Ginny Dowell, RN, BSN October 21, 2015
 TB Nurse Assessment Ginny Dowell, RN, BSN October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19-22, 2015 Wichita, KS EXCELLENCE EXPERTISE INNOVATION Ginny Dowell,
TB Nurse Assessment Ginny Dowell, RN, BSN October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19-22, 2015 Wichita, KS EXCELLENCE EXPERTISE INNOVATION Ginny Dowell,
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012
 TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012 Challenges of TB Treatment in Special Populations in Corrections Marcos Burgos, MD November 28, 2012 Marcos Burgos, MD has the following
TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012 Challenges of TB Treatment in Special Populations in Corrections Marcos Burgos, MD November 28, 2012 Marcos Burgos, MD has the following
Antimycobacterial drugs. Dr.Naza M.Ali lec Dec 2018
 Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
TB Nurse Case Management San Antonio, Texas April 9-11, 2013
 TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
Managing Complex TB Cases Diana M. Nilsen, MD, RN
 Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Pre-Treatment Evaluation. Treatment of Latent TB Infection (LTBI) Initiating Treatment: Patient Education. Before initiating treatment for LTBI:
 Initiating Treatment: Patient Education. Before initiating treatment for LTBI:") Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer
 Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Pediatric TB Intensive San Antonio, Texas October 14, 2013
 Pediatric TB Intensive San Antonio, Texas October 14, 2013 Treatment of Tuberculosis in Children Jeffrey R. Starke, M.D. Professor of Pediatrics October 14, 2013 Jeffrey R. Starke, M.D. has the following
Pediatric TB Intensive San Antonio, Texas October 14, 2013 Treatment of Tuberculosis in Children Jeffrey R. Starke, M.D. Professor of Pediatrics October 14, 2013 Jeffrey R. Starke, M.D. has the following
LTBI Videos-Treatment
 LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
Treatment of MDR-TB in high HIV- prevalence settings. Hind Satti, M.D. PIH-Lesotho October 20, 2008
 Treatment of MDR-TB in high HIV- prevalence settings Hind Satti, M.D. PIH-Lesotho October 20, 2008 Early outcomes of MDR-TB treatment Retrospective cohort analysis Registered between July 21, 2007 and
Treatment of MDR-TB in high HIV- prevalence settings Hind Satti, M.D. PIH-Lesotho October 20, 2008 Early outcomes of MDR-TB treatment Retrospective cohort analysis Registered between July 21, 2007 and
Treatment and Monitoring
 Treatment and Monitoring Disclosures We have no actual or potential conflicts of interest in relation to this presentations. We have no financial relationships to disclose. Learning Objectives After this
Treatment and Monitoring Disclosures We have no actual or potential conflicts of interest in relation to this presentations. We have no financial relationships to disclose. Learning Objectives After this
Managing MDR TB Treatment Side Effects
 Managing MDR TB Treatment Side Effects Barbara J. Seaworth, M.D. Medical Director Heartland National TB Center Pacific Islands TB Controllers Association Conference, September 14, 2017 Honolulu, Hawaii
Managing MDR TB Treatment Side Effects Barbara J. Seaworth, M.D. Medical Director Heartland National TB Center Pacific Islands TB Controllers Association Conference, September 14, 2017 Honolulu, Hawaii
Multiple Drug-resistant Tuberculosis: a Threat to Global - and Local - Public Health
 Multiple Drug-resistant Tuberculosis: a Threat to Global - and Local - Public Health C. Robert Horsburgh, Jr. Boston University School of Public Health Background Outline Why does drug resistance threaten
Multiple Drug-resistant Tuberculosis: a Threat to Global - and Local - Public Health C. Robert Horsburgh, Jr. Boston University School of Public Health Background Outline Why does drug resistance threaten
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Patient History 1. Patient History 2. Social History. The Role of Surgery in the Management of TB. Reynard McDonald, MD & Paul Bolanowski, MD
 Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
Treatment of Tuberculosis
 Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
Tuberculosis and Diabetes Dec. 10, 2009 Dean Schillinger, M.D. and Gisela Schecter, M.D., M.P.H. 1 of 18
 Screening, Diagnosis, and Treatment of TB in Persons with Diabetes Dean Schillinger, M.D. University of California San Francisco CA Diabetes Program Gisela Schecter, M.D., M.P.H. TB Control Branch CA Department
Screening, Diagnosis, and Treatment of TB in Persons with Diabetes Dean Schillinger, M.D. University of California San Francisco CA Diabetes Program Gisela Schecter, M.D., M.P.H. TB Control Branch CA Department
Case presentation. Dr Connie Haley, MD, MPH Dr Gautam Kalyatanda, MD
 Case presentation Dr Connie Haley, MD, MPH Dr Gautam Kalyatanda, MD History of presenting illness 20 Year old woman from Nigeria who came to study at Montgomery in August 2013 About 2 weeks after arriving,
Case presentation Dr Connie Haley, MD, MPH Dr Gautam Kalyatanda, MD History of presenting illness 20 Year old woman from Nigeria who came to study at Montgomery in August 2013 About 2 weeks after arriving,
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
TB: A Supplement to GP CLINICS
 TB: A Supplement to GP CLINICS Adverse Drug events With Anti Tuberculosis Therapy What Every GP Should Know Authors: Kavitha Saravu, MD, DNB, DTM&H; Madhukar Pai, MD, PhD Standards of TB Care in India
TB: A Supplement to GP CLINICS Adverse Drug events With Anti Tuberculosis Therapy What Every GP Should Know Authors: Kavitha Saravu, MD, DNB, DTM&H; Madhukar Pai, MD, PhD Standards of TB Care in India
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
SA TB Guidelines The interface with Advanced Clinical Care
 SA TB Guidelines The interface with Advanced Clinical Care Dr Kogie Naidoo (MBCHB, PHD) Head: CAPRISA Treatment Research Programme Honorary Lecturer - UKZN Department of Public Heath Medicine Annual Workshop
SA TB Guidelines The interface with Advanced Clinical Care Dr Kogie Naidoo (MBCHB, PHD) Head: CAPRISA Treatment Research Programme Honorary Lecturer - UKZN Department of Public Heath Medicine Annual Workshop
TB Drugs. Discuss the common route for transmission of the disease. Discusses the out line for treatment of tuberculosis.
 TB Drugs Red : important Black : in male / female slides Pink : in female s slides only Blue : in male s slides only Females doctor notes Grey: Males doctor notes OBJECTIVES: By the end of this lecture,
TB Drugs Red : important Black : in male / female slides Pink : in female s slides only Blue : in male s slides only Females doctor notes Grey: Males doctor notes OBJECTIVES: By the end of this lecture,
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
LTBI in Special Populations John Nava, MD October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
DR-TB Patient Treatment Log Book
 REPUBLIC OF KENYA MINISTRY OF HEALTH DR-TB Patient Treatment Log Book Patient Name: Patient Reg. No.: VERSION 2016 DR-TB treatment outcome summary Outcome Mark one Date Cured Died Failed Defaulted Transferred
REPUBLIC OF KENYA MINISTRY OF HEALTH DR-TB Patient Treatment Log Book Patient Name: Patient Reg. No.: VERSION 2016 DR-TB treatment outcome summary Outcome Mark one Date Cured Died Failed Defaulted Transferred
5. HIV-positive individuals treated with INH should receive Pyridoxine (B6) 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH
 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH") V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
TB BASICS: PRIORITIES AND CLASSIFICATIONS
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.
TB Case Management Hepatitis
 TB Case Management Hepatitis Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
TB Case Management Hepatitis Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
Official ATS/CDC/IDSA Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis (Nahid et al, CID 2016)
") Official ATS/CDC/IDSA Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis (Nahid et al, CID 2016) APPENDIX C: DRUGS IN CURRENT USE The U.S. Food and Drug Administration (FDA) has approved
Official ATS/CDC/IDSA Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis (Nahid et al, CID 2016) APPENDIX C: DRUGS IN CURRENT USE The U.S. Food and Drug Administration (FDA) has approved
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)
") Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)-750-5496 Local health care providers, including physicians offices, labs and hospitals, are required by law to
Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)-750-5496 Local health care providers, including physicians offices, labs and hospitals, are required by law to
Antituberculous Agents
 Antituberculous Agents Primary or First Line Drugs: Isoniazid (INH) Rifampin Rifadin or Rimactane Ethambutal Streptomycin Pyrazinamide Isoniazid(INH) Most active. Small molecule, water soluble, Structurally
Antituberculous Agents Primary or First Line Drugs: Isoniazid (INH) Rifampin Rifadin or Rimactane Ethambutal Streptomycin Pyrazinamide Isoniazid(INH) Most active. Small molecule, water soluble, Structurally
PROBLEMS IN TX CASE STUDY. JB is a 42 yo BM who was admitted to
 Why TB Drugs Fail Part 2 Why TB Drugs Fail OR How We Fail TB Drugs (and Tb Patients) 1 PROBLEMS IN TX FAILURE TO RESPOND TB MENINGITIS RENAL FAILURE HEPATITIS CAN T SWALLOW PILLS GI INTOLERANCE ADVERSE
Why TB Drugs Fail Part 2 Why TB Drugs Fail OR How We Fail TB Drugs (and Tb Patients) 1 PROBLEMS IN TX FAILURE TO RESPOND TB MENINGITIS RENAL FAILURE HEPATITIS CAN T SWALLOW PILLS GI INTOLERANCE ADVERSE
Pharmacology and Pharmacokinetics of TB Drugs Part I
 Pharmacology and Pharmacokinetics of TB Drugs Part I Charles A. Peloquin, Pharm. D. Professor, and Director Infectious Disease Pharmacokinetics Laboratory College of Pharmacy and The Emerging Pathogens
Pharmacology and Pharmacokinetics of TB Drugs Part I Charles A. Peloquin, Pharm. D. Professor, and Director Infectious Disease Pharmacokinetics Laboratory College of Pharmacy and The Emerging Pathogens
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2013
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Mitnick CD, Shin SS, Seung KJ, et al. Comprehensive treatment
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Mitnick CD, Shin SS, Seung KJ, et al. Comprehensive treatment
Analysis. Answers. Action. Saturday Night Fever. Shaka Brown Capital Congress
 Saturday Night Fever Shaka Brown Capital Congress Shaka Zulu October 31, 2012 SICK SUCKS How my illness started October 2013 August to October 2013 Symptoms: Severe fatigue Night sweats Low grade fever
Saturday Night Fever Shaka Brown Capital Congress Shaka Zulu October 31, 2012 SICK SUCKS How my illness started October 2013 August to October 2013 Symptoms: Severe fatigue Night sweats Low grade fever
Treatment of Tuberculosis Disease. Treatment of Tuberculosis. Decision to Treat Initiation of Therapy 1
 Treatment of Tuberculosis Some Highlights of Most Recent Update Treatment of Tuberculosis Disease Germaine Jacquette, MD Physician Specialist NJMS Global Tuberculosis Institute September 15, 2010 The provider
Treatment of Tuberculosis Some Highlights of Most Recent Update Treatment of Tuberculosis Disease Germaine Jacquette, MD Physician Specialist NJMS Global Tuberculosis Institute September 15, 2010 The provider
Tuberculosis in Chicago 2007
 City of Chicago Communicable Disease Information Department of Public Health Richard M. Daley, Mayor May 2008 Terry Mason, MD, FACS, Commissioner www.cityofchicago.org/health/ West Side Center For Disease
City of Chicago Communicable Disease Information Department of Public Health Richard M. Daley, Mayor May 2008 Terry Mason, MD, FACS, Commissioner www.cityofchicago.org/health/ West Side Center For Disease
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, TB Nurse Case Management September 12 14, 2017
 Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Dosage and Administration
 SIRTURO product information for healthcare providers 2 WARNINGS: An increased risk of death was seen in the SIRTURO (bedaquiline) treatment group (9/79, 11.4%) compared to the placebo treatment group (2/81,
SIRTURO product information for healthcare providers 2 WARNINGS: An increased risk of death was seen in the SIRTURO (bedaquiline) treatment group (9/79, 11.4%) compared to the placebo treatment group (2/81,
Treatment of Latent TB Infection (LTBI)
") Treatment of Latent TB Infection (LTBI) Mahesh C. Patel, MD June 14, 2017 2014 MFMER slide-1 Mahesh C. Patel, MD Associate Professor Treatment of LTBI Department of Internal Medicine, Division of Infectious
Treatment of Latent TB Infection (LTBI) Mahesh C. Patel, MD June 14, 2017 2014 MFMER slide-1 Mahesh C. Patel, MD Associate Professor Treatment of LTBI Department of Internal Medicine, Division of Infectious
Treatment of Tuberculosis
 Treatment of Tuberculosis American Thoracic Society, CDC, and Infectious Diseases Society of America Please note: An erratum has been published for this article. To view the erratum, please click here.
Treatment of Tuberculosis American Thoracic Society, CDC, and Infectious Diseases Society of America Please note: An erratum has been published for this article. To view the erratum, please click here.
Treatment of Tuberculosis
 Treatment of Tuberculosis, 1940 s Treatment of Tuberculosis ATS/CDC/IDSA Joint Statement 2003 Saskatchewan Lung Association Outline, 2012 Treatment of Tuberculosis Principles of treatment of tuberculosis
Treatment of Tuberculosis, 1940 s Treatment of Tuberculosis ATS/CDC/IDSA Joint Statement 2003 Saskatchewan Lung Association Outline, 2012 Treatment of Tuberculosis Principles of treatment of tuberculosis
Etiological Agent: Pulmonary Tuberculosis. Debra Mercer BSN, RN, RRT. Definition
 Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Treatment of Tuberculosis
 Recommendations and Reports June 20, 2003 / 52(RR11);1-77 Recommendations and Reports June 20, 2003 / 52(RR11);1-77 Treatment of Tuberculosis American Thoracic Society, CDC, and Infectious Diseases Society
Recommendations and Reports June 20, 2003 / 52(RR11);1-77 Recommendations and Reports June 20, 2003 / 52(RR11);1-77 Treatment of Tuberculosis American Thoracic Society, CDC, and Infectious Diseases Society
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011
 ART Treatment Guideline Training 31 st January to 4 th February, 2011") TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Anti-Tuberculosis Drugs
 Tuberculosis in Nursing: Prevention, Treatment, and nfection Control Curry nternational Tuberculosis Center Anti-Tuberculosis Drugs What Nurses Need to Know Objectives Describe the anti-tb medications
Tuberculosis in Nursing: Prevention, Treatment, and nfection Control Curry nternational Tuberculosis Center Anti-Tuberculosis Drugs What Nurses Need to Know Objectives Describe the anti-tb medications
Management of Patients with TB Infection Catalina Navarro, RN, BSN April 7, 2015
 Management of Patients with TB Infection Catalina Navarro, RN, BSN April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Catalina Navarro,
Management of Patients with TB Infection Catalina Navarro, RN, BSN April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Catalina Navarro,
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
MANAGEMENT OF DILI in TB/HIV coinfected patients. Chimoio 31 August 2017 by Dr Ndiviwe Mphothulo
 MANAGEMENT OF DILI in TB/HIV coinfected patients Chimoio 31 August 2017 by Dr Ndiviwe Mphothulo ANTI-TB drugs Groups Drugs Group 1: First-line oral drugs Ethambutol (Emb) Pyrazinamide(PZA) Isoniazid (INH)
MANAGEMENT OF DILI in TB/HIV coinfected patients Chimoio 31 August 2017 by Dr Ndiviwe Mphothulo ANTI-TB drugs Groups Drugs Group 1: First-line oral drugs Ethambutol (Emb) Pyrazinamide(PZA) Isoniazid (INH)
Latent TB Infection Treatment
 Latent TB Infection Treatment Douglas B. Hornick, MD Pulmonologist w/ Infectious Attitude Division of Pulmonary/Critical Care/Occ Med UI Carver College of Medicine 2014 MFMER slide-1 Disclosures: None
Latent TB Infection Treatment Douglas B. Hornick, MD Pulmonologist w/ Infectious Attitude Division of Pulmonary/Critical Care/Occ Med UI Carver College of Medicine 2014 MFMER slide-1 Disclosures: None
Marcos Burgos, MD has the following disclosures to make:
 Guidelines for the Treatment of Tuberculosis Marcos Burgos, MD May 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures
Guidelines for the Treatment of Tuberculosis Marcos Burgos, MD May 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures
Disclosures. Outline. No disclosures or conflicts of interest to report. Special LTBI situations. H t it d id ff t
 Selected Topics in LTBI June 2, 2015 Bijan Ghassemieh, MD Senior Fellow UW Division of Pulmonary/Critical Care Disclosures No disclosures or conflicts of interest to report Outline Special LTBI situations
Selected Topics in LTBI June 2, 2015 Bijan Ghassemieh, MD Senior Fellow UW Division of Pulmonary/Critical Care Disclosures No disclosures or conflicts of interest to report Outline Special LTBI situations
Update on Management of
 Update on Management of DR TB Definitions Presumptive MDR-TB A patient suspected of drug-resistant TB, based on RNTCP criteria for submission of specimens for drug-susceptibility testing MDR-TB Case A
Update on Management of DR TB Definitions Presumptive MDR-TB A patient suspected of drug-resistant TB, based on RNTCP criteria for submission of specimens for drug-susceptibility testing MDR-TB Case A
Experience with Pyrazinamide and Rifampin Regimens for Latent TB Infection
 Experience with Pyrazinamide and Rifampin Regimens for Latent TB Infection Krista Powell, MD, MPH Co-Project Officer, National Surveillance for Severe Adverse Events Associated with LTBI Treatment Lead,
Experience with Pyrazinamide and Rifampin Regimens for Latent TB Infection Krista Powell, MD, MPH Co-Project Officer, National Surveillance for Severe Adverse Events Associated with LTBI Treatment Lead,
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
Utilizing All the Tools in the TB Toolbox
 Utilizing All the Tools in the TB Toolbox Sandra Morano, B.A., R.N. Public Health Nurse, City of Stamford, CT TB Talk The New England TB Consortium March 18, 2010 Background TB Program, City of Stamford,
Utilizing All the Tools in the TB Toolbox Sandra Morano, B.A., R.N. Public Health Nurse, City of Stamford, CT TB Talk The New England TB Consortium March 18, 2010 Background TB Program, City of Stamford,
The Epidemiology of Tuberculosis in Minnesota,
 The Epidemiology of Tuberculosis in Minnesota, 2011 2015 Minnesota Department of Health Tuberculosis Prevention and Control Program (651) 201-5414 Tuberculosis surveillance data for Minnesota are available
The Epidemiology of Tuberculosis in Minnesota, 2011 2015 Minnesota Department of Health Tuberculosis Prevention and Control Program (651) 201-5414 Tuberculosis surveillance data for Minnesota are available
Treatment of Tuberculosis, 2017
 Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION
 TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION Michelle Haas, M.D. Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
TB PREVENTION: TREATMENT OF LATENT TB INFECTION AND BCG VACCINATION Michelle Haas, M.D. Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES