Esophageal injuries. 新光急診張志華醫師 Facebook.com/jack119
|
|
|
- Mariah Newton
- 5 years ago
- Views:
Transcription
1 Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119
2 Pre-test 1 What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic
3 Pre-test 2 Which contrast agent is more likely to cause severe pneumonitis if aspirated? A. Barium B. Gastrografin
4 Pre-test 3 Which of the following drugs is indicated in treating impacted food in esophagus? A. Glucagon B. Primperan C. Buscopan
5 Pre-test 4 When treating esophageal foreign body, which of the followings is considered an emergency? A. Coin in esophagus causing severe stridor B. Sharp ended toothpick in esophagus C. Disk battery in esophagus D. All of the above
6 Pre-test 5 Which of the followings is contraindicated in treating acid ingestions? A. NG aspiration B. Cold water lavage C. Antacids
7 Agenda 1. Esophageal perforations 2. Esophageal foreign bodies 3. Chemical injuries of the esophagus
8 Pathophysiology Lack of serosal covering anastomotic leak more likely Most injuries to the esophagus are iatrogenic and tend to occur at natural or acquired areas of narrowing
9 Pathophysiology Toxicity of esophageal rupture 1. Chemical mediastinitis - from regurgitated gastric secretions 2. Suppurative mediastinitis - from infection
10 Mortality Depends on time of definitive treatment: Within 12h: 5~25% mortality 12~24h: 10~44% mortality Beyond 24h: 25~66% mortality Cause of death = severe suppurative mediastinitis; developed within 6~12h
11 Esophageal perforations
 2. Penetrating trauma 3.")
12 Esophageal perforations Etiology 1. Iatrogenic trauma (~66%) 2. Penetrating trauma 3. Blunt trauma
13 Iatrogenic trauma During efforts to dilate strictures During diagnostic endoscopy - biopsy, removal of sharp FB Sites prone to perforate: 1. Esophageal introitus at the cricopharygeus - narrowest, most commonly perforated 2. Diaphragmatic hiatus 3. Left mainstem bronchus

14
15 Penetrating trauma Caused by stabs or gunshot wounds Types: 1. Cervical: - more common - mainly caused by stab wounds 2. Intrathoracic / intraabdominal - less common - mainly caused by gunshot wounds
16 Blunt trauma Rare 70% cervical portion Mechanism 1. Intraluminal pressure rupture 2. Compression tear 3. Contusion necrosis
17 Esophageal injury When to suspect? 1. Presence of pleural effusion or pneumothorax in patients with penetrating wound in thoracic inlet or mediastinum 2. Cervical, thoracic, or abdominal symptoms after esophageal instrumentation
18 Esophageal perforation Symptoms 1. Chest/back/shoulder pain 2. Abdominal pain and tenderness lower esophageal perforation 3. Difficult swallowing (dysphagia) 4. Painful swallowing (odynophagia) 5. Hematemesis
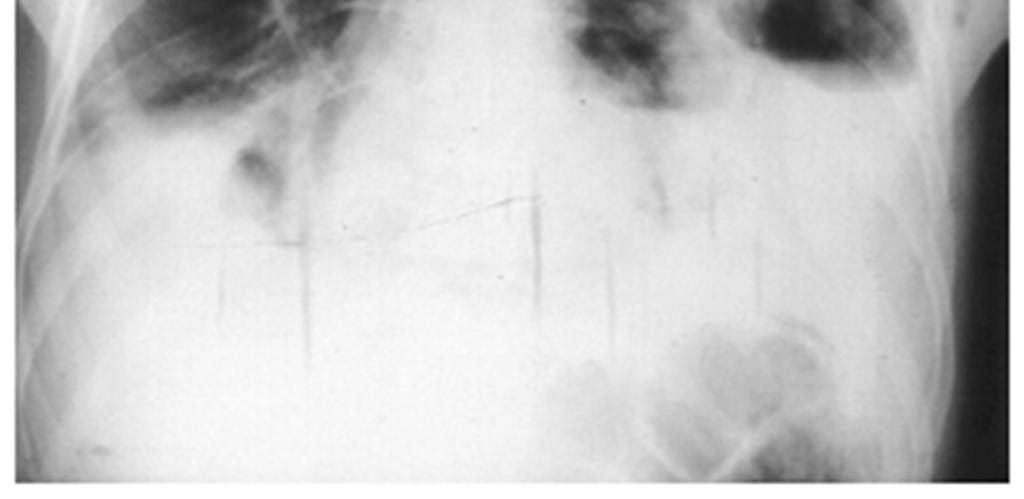
19 Esophageal perforation Signs 1. Emphysema / pneumomediastinum mediastinal / cervical 2. Pleural effusions with increased amylase after chest trauma 3. Pneumothorax 4. Fever / sepsis
20 Esophageal perforation Diagnostic tests 1. CXR 2. Contrast swallows / esophagography Gastrografin: # 40~50% false negative # cause severe pneumonitis if aspirated Barium: # < 25% false negative # aggravate mediastinitis if leaked 3. CT scan 4. Esophagoscopy

21


22



23


24


25


26


27
28 Blunt truncal trauma Abdominal s/s Explorative laparotomy (negative) Suspect thoracic injury
29 Esophageal perforation Management Surgery - esp. if sepsis present Small iatrogenic injuries of cervical esophagus or pharynx with contained leak can often be managed nonoperatively 1. NPO + NG drainage 2. Antibiotics - cover mouth organisms
30 Esophageal perforation Complications 1. Sepsis most deadly Negative contrast swallow / esophagoscopy does not rule out mediastinitis / abscess 2. Fistulas In neck heal in 2~3 wk In chest sepsis and death 3. Strictures DO dilation / colon bypass
31 Esophageal foreign bodies
32 Esophageal FB Risks: 1. Children 2. Psychiatric disease 3. Alcohol abuse 4. Mental retardation 5. Elderly dentures 6. Preexisting strictures food impaction

33 Esophageal FB Emergencies: 1. Acute obstruction 2. Sharp or irregular FB - e.g. toothpicks, pins, dentures 3. Disk battery Caution: 1. Keep patient in upright position 2. Suction for oral secretions



34
35 Esophageal FB Coins on CXR: PA on face ; lat on edge FB removal 1. Delayed edema difficult to removed increased risk of perforation 2. After removal: check with CXR / endoscope



36
37 Esophageal FB removal Catheter removal - E.g. Foley catheters Insert catheter past the object Lower head and neck Balloon inflated Catheter gently pulled back
38 Esophageal FB removal Glucagon +/- gas-forming compound FB not sharp and patient not compromised Glucagon relaxes smooth muscles and LES May stimulate nausea Dose: 1-2 mg of glucagon intravenously ( mg/kg in children, not to exceed 0.5 mg) May be followed by ingestion of [E-Z Gas ml water]. Hint: use carbonated beverages if E-Z Gas not available
39 Chemical injuries of the esophagus
40 Chemical injuries S/S: sudden difficult or painful swallowing Chemicals 1. Strong acid coagulation necrosis 2. Strong alkali (ph > 12) liquefaction necrosis muscle layers Disk batteries 1. Severe corrosive injury 2. Leaking NaOH, KOH, mercury oxide
41 Chemical injuries Endoscopy Do not pass beyond the 1 st deep circumferential burn easy perforation Need antistricture management
42 Mild alkali E.g. small amount of bleaches May cautiously give milk, dilute vinegar, or citrus juice

43 Strong alkali Lye ingestion 鹼液 Contraindications for emetics, charcoal, NG lavage


44
45 Acid ingestion Early NG aspiration Cold water lavage Antacids are contraindicated (neutralization produces heat)


46
47 Corticosteroids The use of corticosteroids for caustic ingestions is controversial Current tendency avoid steroids Literature reviews steroids may be helpful in preventing strictures in severe cases
48 Take home message 1. Low incidence, high morbidity/mortality 2. Commonly iatrogenic 3. Abdominal presentations probable 4. Check pleural fluid amylase 5. Beware of lye and disk battery 6. Repair within 6~12 h
49 Thank you
Esophageal injuries. Pre-test /11/10. 新光急診張志華醫師 Facebook.com/jack119. O What is the most common cause of esophageal injuries?
 Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 O What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic 1 Pre-test 2 O Which contrast
Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 O What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic 1 Pre-test 2 O Which contrast
Esophageal Perforation
 Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Foreign Body Management
 Foreign Body Management NYSGE Fellows Summer Course Susana Gonzalez, MD Assistant Professor of Medicine 1 Objectives Timing of endoscopy When? Anatomic location Where? High risk objects What? Choosing
Foreign Body Management NYSGE Fellows Summer Course Susana Gonzalez, MD Assistant Professor of Medicine 1 Objectives Timing of endoscopy When? Anatomic location Where? High risk objects What? Choosing
pthaigastro.org Caustic injury The 5 th Pediatric GI Days Pediatric GI & Liver Emergency : Current Practical Management
 The 5 th Pediatric GI Days Pediatric GI & Liver Emergency : Current Practical Management Caustic injury Phisek Yimyaem Pediatric Department, Khon Kaen Regional Hospital 18 July 2013 Outlines Introduction
The 5 th Pediatric GI Days Pediatric GI & Liver Emergency : Current Practical Management Caustic injury Phisek Yimyaem Pediatric Department, Khon Kaen Regional Hospital 18 July 2013 Outlines Introduction
Acquired pediatric esophageal diseases Imaging approaches and findings. M. Mearadji International Foundation for Pediatric Imaging Aid
 Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Caustic Esophageal Injury. Aliu Sanni, MD SUNY Downstate Medical Center March 21, 2013
 Caustic Esophageal Injury Aliu Sanni, MD SUNY Downstate Medical Center March 21, 2013 Case presentation 3F with no PMH presented to outside facility after drinking unmarked bottle containing oven cleaner
Caustic Esophageal Injury Aliu Sanni, MD SUNY Downstate Medical Center March 21, 2013 Case presentation 3F with no PMH presented to outside facility after drinking unmarked bottle containing oven cleaner
The Foreign Body. Neil H. Stollman, MD, FACG
 The Foreign Body Neil H. Stollman, MD, FACG Associate Clinical Professor of Medicine University of California San Francisco Chief, Division of Gastroenterology Alta Bates Summit Medical Center, Oakland,
The Foreign Body Neil H. Stollman, MD, FACG Associate Clinical Professor of Medicine University of California San Francisco Chief, Division of Gastroenterology Alta Bates Summit Medical Center, Oakland,
DR. SAAD AL-MUHAYAWI, M.D., FRCSC. ORL Head & Neck Surgery
 TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
Suspected Foreign Body Ingestion
 Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
ESOPHAGEAL PERFORATION. Anju Sidhu MD University of Louisville Gastroenterology, Hepatology, and Nutrition January 24, 2013
 ESOPHAGEAL PERFORATION Anju Sidhu MD University of Louisville Gastroenterology, Hepatology, and Nutrition January 24, 2013 OUTLINE Risk factors Diagnosis Management GOALS Make sure you don t miss it If
ESOPHAGEAL PERFORATION Anju Sidhu MD University of Louisville Gastroenterology, Hepatology, and Nutrition January 24, 2013 OUTLINE Risk factors Diagnosis Management GOALS Make sure you don t miss it If
Case Presentation Surgery Grand Round. Amid Keshavarzi, MD UCHSC 4/9/2006
 Case Presentation Surgery Grand Round Amid Keshavarzi, MD UCHSC 4/9/2006 Case Presentation 12 y/o female Presented to OSH after accidental swallowing of plastic fork in the bus, CXR/AXR form OSH did not
Case Presentation Surgery Grand Round Amid Keshavarzi, MD UCHSC 4/9/2006 Case Presentation 12 y/o female Presented to OSH after accidental swallowing of plastic fork in the bus, CXR/AXR form OSH did not
Departement of Surgery Faculty of Medicine University Sumatera Utara
 SSS EESOPHAGEAL HPOSAGEAL DISORDERS IN SURGICAL PERSPECTIVE Departement of Surgery Faculty of Medicine University Sumatera Utara CONTENT 1. Esophageal Atresia 2. Achalasia 3. Esophageal Rupture 4. Tumor
SSS EESOPHAGEAL HPOSAGEAL DISORDERS IN SURGICAL PERSPECTIVE Departement of Surgery Faculty of Medicine University Sumatera Utara CONTENT 1. Esophageal Atresia 2. Achalasia 3. Esophageal Rupture 4. Tumor
Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread
 Esophagus Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread Upper 2/3 Cephalad Lower 1/3 Caudad Physiology:
Esophagus Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread Upper 2/3 Cephalad Lower 1/3 Caudad Physiology:
A unique case of esophageal perforation caused by prickly pears
 A unique case of esophageal perforation caused by prickly pears Abstract This is a report of a previously healthy 20-yearold male presenting with the sensation of a foreign object being stuck in the throat
A unique case of esophageal perforation caused by prickly pears Abstract This is a report of a previously healthy 20-yearold male presenting with the sensation of a foreign object being stuck in the throat
Managing Foreign Objects in the GI Tract Tips & Tricks
 Managing Foreign Objects in the GI Tract Tips & Tricks STEPHEN LANDRENEAU, MD Take home o Perform emergent endoscopy in cases of: Esophageal obstruction due to food bolus impaction or foreign object. Disk
Managing Foreign Objects in the GI Tract Tips & Tricks STEPHEN LANDRENEAU, MD Take home o Perform emergent endoscopy in cases of: Esophageal obstruction due to food bolus impaction or foreign object. Disk
Chapter 153 Caustics. Episode Overview: Wisecracks. Key Points: Rosen s in Perspective
 Chapter 153 Caustics Episode Overview: 1) Compare acid and alkali caustic burns 2) Describe clinical features of significant airway and esophageal injury by caustics 3) What are indications for endoscopy
Chapter 153 Caustics Episode Overview: 1) Compare acid and alkali caustic burns 2) Describe clinical features of significant airway and esophageal injury by caustics 3) What are indications for endoscopy
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
Foreign Body Ingested
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Foreign Body Ingested Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Foreign Body Ingested Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Down the Tube: Caustic Ingestions. Significance & Management in the ED. Laura Chng PGY-3
 Down the Tube: Caustic Ingestions Significance & Management in the ED Laura Chng PGY-3 Caustic Ingestions Not common but you ll see them Controversial You drank WHAT? ED management can change outcome Who
Down the Tube: Caustic Ingestions Significance & Management in the ED Laura Chng PGY-3 Caustic Ingestions Not common but you ll see them Controversial You drank WHAT? ED management can change outcome Who
Use of Magill Forceps to Remove Foreign Bodies in Children
 THIEME Original Article e91 Use of Magill Forceps to Remove Foreign Bodies in Children Murat Oncel, MD 1 Guven Sadi Sunam, MD 1 Cagdas Elsurer, MD 2 Huseyin Yildiran, MD 1 1 Department of Thoracic Surgery,
THIEME Original Article e91 Use of Magill Forceps to Remove Foreign Bodies in Children Murat Oncel, MD 1 Guven Sadi Sunam, MD 1 Cagdas Elsurer, MD 2 Huseyin Yildiran, MD 1 1 Department of Thoracic Surgery,
Penetrating Wounds of the Esophagus
 Panagiotis N. Symbas, M.D., Denis H. Tyras, M.D., Charles R. Hatcher, Jr., M.D., and Byron Perry, M.D. ABSTRACT The histories of 22 patients with perforation of the esophagus from bullet or stab wounds
Panagiotis N. Symbas, M.D., Denis H. Tyras, M.D., Charles R. Hatcher, Jr., M.D., and Byron Perry, M.D. ABSTRACT The histories of 22 patients with perforation of the esophagus from bullet or stab wounds
Discussing feline tracheal disease
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Discussing feline tracheal disease Author : ANDREW SPARKES Categories : Vets Date : March 24, 2008 ANDREW SPARKES aims to
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Discussing feline tracheal disease Author : ANDREW SPARKES Categories : Vets Date : March 24, 2008 ANDREW SPARKES aims to
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Recurrent Retropharyngeal Abscess with Esophageal Perforation due to Chopstick Injury
 Recurrent Retropharyngeal Abscess with Esophageal Perforation due to Chopstick Injury Hye Kyung Chang, Jung-Tak Oh, Seung Hoon Choi, Seok Joo Han Division of Pediatric Surgery, Department of Surgery, Yonsei
Recurrent Retropharyngeal Abscess with Esophageal Perforation due to Chopstick Injury Hye Kyung Chang, Jung-Tak Oh, Seung Hoon Choi, Seok Joo Han Division of Pediatric Surgery, Department of Surgery, Yonsei
Endoscopic Treatment of Luminal Perforations and Leaks
 Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Imaging of Thoracic Trauma: Tips and Traps. Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania
 Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Peptic ulcer disease Disorders of the esophagus
 Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Traumatic Tracheo-Oesophageal Fistula: A Case Study
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 12 Ver. II (Dec. 2017), PP 93-98 www.iosrjournals.org Traumatic Tracheo-Oesophageal Fistula:
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 12 Ver. II (Dec. 2017), PP 93-98 www.iosrjournals.org Traumatic Tracheo-Oesophageal Fistula:
01/26/2010 GENERAL SURGERY ABSITE ANATOMY ANATOMY. Yvonne M. Carter, MD Georgetown University Medical Center. Layers. mucosa. squamous epithelium
 GENERAL SURGERY ABSITE REVIEW: ESOPHAGUS Yvonne M. Carter, MD Georgetown University Medical Center ANATOMY Layers mucosa muscle squamous epithelium columnar epithelium (distal 2cm) inner = circular outer
GENERAL SURGERY ABSITE REVIEW: ESOPHAGUS Yvonne M. Carter, MD Georgetown University Medical Center ANATOMY Layers mucosa muscle squamous epithelium columnar epithelium (distal 2cm) inner = circular outer
Oesophageal Disorders
 Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Module 2 Heartburn Glossary
 Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
REMOVAL OF IMPACTED DENTURES WITH POLYPECTOMY SNARE
 JMBR: A Peer-review Journal of Biomedical Sciences June 2012, Vol. 11 No.1 pp 14-19 REMOVAL OF IMPACTED DENTURES WITH POLYPECTOMY SNARE *OKUGBO SU, **OKORO E, ***KESIEME E ABSTRACT Impacted dentures have
JMBR: A Peer-review Journal of Biomedical Sciences June 2012, Vol. 11 No.1 pp 14-19 REMOVAL OF IMPACTED DENTURES WITH POLYPECTOMY SNARE *OKUGBO SU, **OKORO E, ***KESIEME E ABSTRACT Impacted dentures have
Clinical Case Presentation. Jared B. Smith, M.D. Surgical Grand Rounds, August 21, 2006
 Clinical Case Presentation Jared B. Smith, M.D. Surgical Grand Rounds, August 21, 2006 Clinical History CC: Can t swallow anything HPI: 50 y.o. male from western Colorado, greater than 2 years of emesis
Clinical Case Presentation Jared B. Smith, M.D. Surgical Grand Rounds, August 21, 2006 Clinical History CC: Can t swallow anything HPI: 50 y.o. male from western Colorado, greater than 2 years of emesis
老人醫療之陷阱. Objective. Falls. Recurrent injuries. Shock or not? Elder abuse is not uncommon!
 Objective 老人醫療之陷阱 Understand some of the pitfalls in the emergency and critical care of the elderly 新光醫院急診科張志華 102.01.05 Falls Very common in the elderly Most falls in the elderly are the result of their
Objective 老人醫療之陷阱 Understand some of the pitfalls in the emergency and critical care of the elderly 新光醫院急診科張志華 102.01.05 Falls Very common in the elderly Most falls in the elderly are the result of their
Swallowed Foreign Body
 Swallowed Foreign Body Page 1 of 5 INTRODUCTION Swallowed foreign bodies can be divided into five distinct groups: 1 Small blunt objects 2 Large blunt objects 3 Potentially poisonous objects 4 Sharp objects
Swallowed Foreign Body Page 1 of 5 INTRODUCTION Swallowed foreign bodies can be divided into five distinct groups: 1 Small blunt objects 2 Large blunt objects 3 Potentially poisonous objects 4 Sharp objects
Selective Nonoperative Management of Contained Intrathoracic Esophageal Disruptions
 Selective Nonoperative Management of Contained Intrathoracic Esophageal Disruptions John L. Cameron, M.D., Richard F. Kieffer, M.D., Thomas R. Hendrix, M.D., Denis G. Mehigan, M.., and R. Robinson aker,
Selective Nonoperative Management of Contained Intrathoracic Esophageal Disruptions John L. Cameron, M.D., Richard F. Kieffer, M.D., Thomas R. Hendrix, M.D., Denis G. Mehigan, M.., and R. Robinson aker,
Foreign body ingestions occur
 Navid Dehghani, MD, FRCRC, Jeffrey P. Ludemann, MDCM, FRCSC Ingested foreign bodies in children: BC Children s Hospital emergency room protocol Clinicians should be aware of the dangers presented by disc
Navid Dehghani, MD, FRCRC, Jeffrey P. Ludemann, MDCM, FRCSC Ingested foreign bodies in children: BC Children s Hospital emergency room protocol Clinicians should be aware of the dangers presented by disc
GIT RADIOLOGY. Water-soluble contrast media (e.g. gastrograffin) are the other available agents.which doesn t cause inflammatory peritonitis..
 are the other available agents.which doesn t cause inflammatory peritonitis..") GIT RADIOLOGY Imaging techniques-general principles: Contrast examinations: Barium sulphate is the best contrast for GIT (with good mucosal coating & excellent opacification & being inert); but is contraindicated
GIT RADIOLOGY Imaging techniques-general principles: Contrast examinations: Barium sulphate is the best contrast for GIT (with good mucosal coating & excellent opacification & being inert); but is contraindicated
The Alimentary System
 The Alimentary System Contrast Medium: 1. Barium Examinations of different parts of the GI tract require different densities of Barium suspension. The escape of Barium into the peritoneal cavity is extremely
The Alimentary System Contrast Medium: 1. Barium Examinations of different parts of the GI tract require different densities of Barium suspension. The escape of Barium into the peritoneal cavity is extremely
IATROGENIC OESOPHAGEAL PERFORATION
 IATROGENIC OESOPHAGEAL PERFORATION TAOLE MOKOENA DPhil FRCS PROFESSOR OF SURGERY UNIVERSITY OF PRETORIA 17 TH Controversies and Problems in Surgery Symposium 4-5 October 2013 Introduction Perforation of
IATROGENIC OESOPHAGEAL PERFORATION TAOLE MOKOENA DPhil FRCS PROFESSOR OF SURGERY UNIVERSITY OF PRETORIA 17 TH Controversies and Problems in Surgery Symposium 4-5 October 2013 Introduction Perforation of
THORACIC SURGERY: Dysphagia. Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone. Thoracic Surgery Toronto East General Hospital
 THORACIC SURGERY: Dysphagia Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone Thoracic Surgery Toronto East General Hospital Objectives Definitions Common causes Investigations Treatment options Anatomy
THORACIC SURGERY: Dysphagia Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone Thoracic Surgery Toronto East General Hospital Objectives Definitions Common causes Investigations Treatment options Anatomy
34th Annual Toronto Thoracic Surgery Refresher Course
 34th Annual Toronto Thoracic Surgery Refresher Course TREATMENT OPTIONS FOR ACHALASIA Dr. Carmine Simone Director, Intensive Care Unit Head, Division of Critical Care Departments of Medicine and Surgery
34th Annual Toronto Thoracic Surgery Refresher Course TREATMENT OPTIONS FOR ACHALASIA Dr. Carmine Simone Director, Intensive Care Unit Head, Division of Critical Care Departments of Medicine and Surgery
Case Report Thoracic Imaging. Eun Kyung Khil, MD 1, Heon Lee, MD, PhD 1, Keun Her, MD 2 INTRODUCTION CASE REPORT
 Case Report Thoracic Imaging http://dx.doi.org/10.3348/kjr.2014.15.1.173 pissn 1229-6929 eissn 2005-8330 Korean J Radiol 2014;15(1):173-177 Spontaneous Intramural Full-Length Dissection of Esophagus Treated
Case Report Thoracic Imaging http://dx.doi.org/10.3348/kjr.2014.15.1.173 pissn 1229-6929 eissn 2005-8330 Korean J Radiol 2014;15(1):173-177 Spontaneous Intramural Full-Length Dissection of Esophagus Treated
Spotlight on Esophageal Perforation A multinational study using the Pittsburgh Esophageal Perforation Severity Scoring System
 Spotlight on Esophageal Perforation A multinational study using the Pittsburgh Esophageal Perforation Severity Scoring System Michael Schweigert Department of Thoracic Surgery Objective Esophageal perforation
Spotlight on Esophageal Perforation A multinational study using the Pittsburgh Esophageal Perforation Severity Scoring System Michael Schweigert Department of Thoracic Surgery Objective Esophageal perforation
Mediastinitis. Jonathan Parks, MD Kings County Medical Center December 3, 2015
 Mediastinitis Jonathan Parks, MD Kings County Medical Center December 3, 2015 Case Presentation 69 year-old male from nursing home PMHx: COPD, asthma, HTN, Afib on pradaxa, PTSD, BPH c/o pulled pork stuck
Mediastinitis Jonathan Parks, MD Kings County Medical Center December 3, 2015 Case Presentation 69 year-old male from nursing home PMHx: COPD, asthma, HTN, Afib on pradaxa, PTSD, BPH c/o pulled pork stuck
Tracheal Trauma: Management and Treatment. Kosmas Iliadis, MD, PhD, FECTS
 Tracheal Trauma: Management and Treatment Kosmas Iliadis, MD, PhD, FECTS Thoracic Surgeon Director of Thoracic Surgery Department Hygeia Hospital, Athens INTRODUCTION Heterogeneous group of injuries mechanism
Tracheal Trauma: Management and Treatment Kosmas Iliadis, MD, PhD, FECTS Thoracic Surgeon Director of Thoracic Surgery Department Hygeia Hospital, Athens INTRODUCTION Heterogeneous group of injuries mechanism
Geoffrey Axiak M.Sc. Nursing (Manch.), B.Sc. Nursing, P.G. Dip. Nutrition & Dietetics Clinical Nutrition Practice Nurse
, B.Sc. Nursing, P.G. Dip. Nutrition & Dietetics Clinical Nutrition Practice Nurse") The Percutaneous Endoscopic Gastrostomy Geoffrey Axiak M.Sc. Nursing (Manch.), B.Sc. Nursing, P.G. Dip. Nutrition & Dietetics Clinical Nutrition Practice Nurse What is a P.E.G.? Percutaneous Endoscopic
The Percutaneous Endoscopic Gastrostomy Geoffrey Axiak M.Sc. Nursing (Manch.), B.Sc. Nursing, P.G. Dip. Nutrition & Dietetics Clinical Nutrition Practice Nurse What is a P.E.G.? Percutaneous Endoscopic
Endoscopic Management of Perforations
 Endoscopic Management of Perforations Gregory G. Ginsberg, MD Professor of Medicine University of Pennsylvania Perelman School of Medicine Gastroenterology Division Executive Director of Endoscopic Services
Endoscopic Management of Perforations Gregory G. Ginsberg, MD Professor of Medicine University of Pennsylvania Perelman School of Medicine Gastroenterology Division Executive Director of Endoscopic Services
Penetrating Neck Injuries. Jason Levine MD Lutheran Medical Center July 22, 2010
 Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Dysphagia. A Problem Swallowing Foods or Liquids
 Dysphagia A Problem Swallowing Foods or Liquids What Is Dysphagia? If you have a problem swallowing foods or liquids, you may have dysphagia. It has a number of causes. Your doctor can find out what is
Dysphagia A Problem Swallowing Foods or Liquids What Is Dysphagia? If you have a problem swallowing foods or liquids, you may have dysphagia. It has a number of causes. Your doctor can find out what is
Colon Patch Esophagoplasty: A Clinical Study For Chemical Burn Esophageal Stricture
 ISPUB.COM The Internet Journal of Surgery Volume 5 Number 1 Colon Patch Esophagoplasty: A Clinical Study For Chemical Burn Esophageal Stricture M Hourang, V Mehrabi Citation M Hourang, V Mehrabi. Colon
ISPUB.COM The Internet Journal of Surgery Volume 5 Number 1 Colon Patch Esophagoplasty: A Clinical Study For Chemical Burn Esophageal Stricture M Hourang, V Mehrabi Citation M Hourang, V Mehrabi. Colon
Acute Penetrating Tracheal Trauma
 Acute Penetrating Tracheal Trauma Panagiotis N. Symbas, M.D., Charles R. Hatcher, Jr., M.D., and Gerhard A. W. Boehm, M.D. ABSTRACT During the past ten years, 20 patients with acute penetrating tracheal
Acute Penetrating Tracheal Trauma Panagiotis N. Symbas, M.D., Charles R. Hatcher, Jr., M.D., and Gerhard A. W. Boehm, M.D. ABSTRACT During the past ten years, 20 patients with acute penetrating tracheal
KIDS PUT THINGS IN THE CRAZIEST PLACES...
 KIDS PUT THINGS IN THE CRAZIEST PLACES... YOU CAN T MAKE ME EAT MY DINNER! 2 year old observed to stuff corn up right nostril Judith Klein, MD FACEP Assistant Professor of Emergency Medicine UCSF-SFGH
KIDS PUT THINGS IN THE CRAZIEST PLACES... YOU CAN T MAKE ME EAT MY DINNER! 2 year old observed to stuff corn up right nostril Judith Klein, MD FACEP Assistant Professor of Emergency Medicine UCSF-SFGH
I thoracic surgeon as mortality rates of more than 20%
 CURRENT REVIEW Management of Esophageal Injuries Herbert E. Cohn, MD, Alan Hubbard, MD, and Gerald Patton, MD Department of Surgery, Thomas Jefferson University Hospital, Philadelphia, Pennsylvania A multiinstitutional
CURRENT REVIEW Management of Esophageal Injuries Herbert E. Cohn, MD, Alan Hubbard, MD, and Gerald Patton, MD Department of Surgery, Thomas Jefferson University Hospital, Philadelphia, Pennsylvania A multiinstitutional
Chapter 132: Foreign Bodies in the Upper Aerodigestive Tract. Trevor J. I. McGill, Laurie Ohlms
 Chapter 132: Foreign Bodies in the Upper Aerodigestive Tract Trevor J. I. McGill, Laurie Ohlms Foreign bodies in the upper aerodigestive tract are an important cause of morbidity and mortality in the two
Chapter 132: Foreign Bodies in the Upper Aerodigestive Tract Trevor J. I. McGill, Laurie Ohlms Foreign bodies in the upper aerodigestive tract are an important cause of morbidity and mortality in the two
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina
 Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Management of Delayed Diagnosed Esophageal Perforation
 ORIGINAL RESEARCH ARTICLE Tanaffos (2006) 5(1), 51-57 2006 NRITLD, National Research Institute of Tuberculosis and Lung Disease, Iran Management of Delayed Diagnosed Esophageal Perforation Mojtaba Javaherzadeh
ORIGINAL RESEARCH ARTICLE Tanaffos (2006) 5(1), 51-57 2006 NRITLD, National Research Institute of Tuberculosis and Lung Disease, Iran Management of Delayed Diagnosed Esophageal Perforation Mojtaba Javaherzadeh
CHEST INJURY PULMONARY CONTUSION
 CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
Materials. I. Iatrogenic A. Endoscopy B. Esophageal dilations C. Passage of tubes D. Major thoracotomy 11. Noniatrogenic A. B. C. D. E.
 Ruptures and Perforations of the Esophagus: The Case for Conservative Supportive Management William S. Lyons, M.D., Michael G. Seremetis, M.D., Vicente C. deguzman, M.D., and Joseph W. Peabody, Jr., M.D.
Ruptures and Perforations of the Esophagus: The Case for Conservative Supportive Management William S. Lyons, M.D., Michael G. Seremetis, M.D., Vicente C. deguzman, M.D., and Joseph W. Peabody, Jr., M.D.
Case Discussion Splenic Abscess
 Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Morbidity and mortality of oesophageal perforation
 Thorax (1972), 27, 353. Morbidity and mortality of oesophageal perforation M. R. B. KEIGHLEY, R. W. GIRDWOOD, G. H. WOOLER, and M. I. IONESCU Department of Cardiothoracic Surgery, The General Infirmary
Thorax (1972), 27, 353. Morbidity and mortality of oesophageal perforation M. R. B. KEIGHLEY, R. W. GIRDWOOD, G. H. WOOLER, and M. I. IONESCU Department of Cardiothoracic Surgery, The General Infirmary
In ESH we usually see blunt chest trauma but penetrating injuries also treated here (usually as single injuries, like stab wound)
") Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
Surgical Management of Graft Redundancy after Colon Interposition for Esophageal Reconstruction. Case 1
 Case Report imedpub Journals www.imedpub.com Medical & Clinical Reviews DOI: 10.21767/2471-299X.1000059 Surgical Management of Graft Redundancy after Colon Interposition for Esophageal Reconstruction Abdelkader
Case Report imedpub Journals www.imedpub.com Medical & Clinical Reviews DOI: 10.21767/2471-299X.1000059 Surgical Management of Graft Redundancy after Colon Interposition for Esophageal Reconstruction Abdelkader
Study of aerodigestive tract foreign bodies
 Original article Study of aerodigestive tract foreign bodies 1Dr Durga Prasad. G, 2 Dr Ravi Kumar Raju M, 3 Dr M A N Murty, 4 Dr Rahul Singh 1P.G Resident, KIMS & RF, Amalapuram 2 Prof. of ENT, KIMS &
Original article Study of aerodigestive tract foreign bodies 1Dr Durga Prasad. G, 2 Dr Ravi Kumar Raju M, 3 Dr M A N Murty, 4 Dr Rahul Singh 1P.G Resident, KIMS & RF, Amalapuram 2 Prof. of ENT, KIMS &
Surgical aspects of dysphagia
 Dysphagia Why is dysphagia important? Surgery Surgical aspects of dysphagia Adrian P. Ireland aireland@eircom.net Academic RCSI Department of Surgery, Beaumont Hospital Why important Definitons Swallowing
Dysphagia Why is dysphagia important? Surgery Surgical aspects of dysphagia Adrian P. Ireland aireland@eircom.net Academic RCSI Department of Surgery, Beaumont Hospital Why important Definitons Swallowing
Esophageal conditions such as obstruction,
 Imaging of esophageal emergencies Stephen Currie, MD; Christine O. Menias, MD; and Vincent Mellnick, MD Esophageal conditions such as obstruction, perforation, inflammation and infection are common and
Imaging of esophageal emergencies Stephen Currie, MD; Christine O. Menias, MD; and Vincent Mellnick, MD Esophageal conditions such as obstruction, perforation, inflammation and infection are common and
Pneumothorax. Defined as air in the pleural space which can occur through a number of mechanisms
 Pneumothorax Defined as air in the pleural space which can occur through a number of mechanisms Traumatic pneumothorax Penetrating chest trauma Common secondary to bullet or knife penetration Chest tube
Pneumothorax Defined as air in the pleural space which can occur through a number of mechanisms Traumatic pneumothorax Penetrating chest trauma Common secondary to bullet or knife penetration Chest tube
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic
 Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Long Term Follow-up. 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown. Is the patient alive? Yes No
 Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
CHEST INJURIES. Jacek Piątkowski M.D., Ph. D.
 CHEST INJURIES Jacek Piątkowski M.D., Ph. D. CHEST INJURIES 3-4% of all injuries 8% of patients hospitalized due to injuries 65% of patients who died at the accident place CLASSIFICATION OF THE CHEST INJURIES
CHEST INJURIES Jacek Piątkowski M.D., Ph. D. CHEST INJURIES 3-4% of all injuries 8% of patients hospitalized due to injuries 65% of patients who died at the accident place CLASSIFICATION OF THE CHEST INJURIES
Oesophageal trauma: incidence, diagnosis,
 Oesophageal trauma: incidence, diagnosis, and management EDOARDO TRIGGIANI AND RONALD BELSEY Thorax, 1977, 32, 241-249 From the Department of Surgery, Second Medical School in the University of Naples,
Oesophageal trauma: incidence, diagnosis, and management EDOARDO TRIGGIANI AND RONALD BELSEY Thorax, 1977, 32, 241-249 From the Department of Surgery, Second Medical School in the University of Naples,
Noniatrogenic Esophageal Trauma
 Noniatrogenic Esophageal Trauma Darryl S. Weiman, MD, William A. Walker, MD, Kathleen M. Brosnan, MSN, James W. Pate, MD, and Timothy C. Fabian, MD Department of Surgery, University of Tennessee College
Noniatrogenic Esophageal Trauma Darryl S. Weiman, MD, William A. Walker, MD, Kathleen M. Brosnan, MSN, James W. Pate, MD, and Timothy C. Fabian, MD Department of Surgery, University of Tennessee College
The Management of Esophageal Strictures in Children
 Akram J. Jawad, FRCS(Ed); Asal Izzidien Al-Samarrai, FRCS,FACS; Abdullah Al-Rabeeah, MS,FRCS(C); Rashed Al-Rashed, FRCP(C) From the Divisions of Pediatric Surgery (Drs. Jawad, Al-Samarrai, Al-Rabeeah)
Akram J. Jawad, FRCS(Ed); Asal Izzidien Al-Samarrai, FRCS,FACS; Abdullah Al-Rabeeah, MS,FRCS(C); Rashed Al-Rashed, FRCP(C) From the Divisions of Pediatric Surgery (Drs. Jawad, Al-Samarrai, Al-Rabeeah)
Difficult Abdominal Closure. Mark A. Carlson, MD
 Difficult Abdominal Closure Mark A. Carlson, MD Illustrative case 14 yo boy with delayed diagnosis of appendicitis POD9 Appendectomy 2 wk after onset of symptoms POD4: return to OR for midline laparotomy
Difficult Abdominal Closure Mark A. Carlson, MD Illustrative case 14 yo boy with delayed diagnosis of appendicitis POD9 Appendectomy 2 wk after onset of symptoms POD4: return to OR for midline laparotomy
RCH Trauma Guideline. Management of Traumatic Pneumothorax & Haemothorax. Trauma Service, Division of Surgery
 RCH Trauma Guideline Management of Traumatic Pneumothorax & Haemothorax Trauma Service, Division of Surgery Aim To describe safe and competent management of traumatic pneumothorax and haemothorax at RCH.
RCH Trauma Guideline Management of Traumatic Pneumothorax & Haemothorax Trauma Service, Division of Surgery Aim To describe safe and competent management of traumatic pneumothorax and haemothorax at RCH.
Shedding Light on Neonatal X-rays. Objectives. Indications for X-Rays 5/14/2018
 Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Inflammation of the Esophagus (Esophagitis) Basics
 Basics") Inflammation of the Esophagus (Esophagitis) Basics OVERVIEW Inflammation of the esophagus typically involves the tubular area of the esophagus itself (known as the esophageal body ) and the muscular area
Inflammation of the Esophagus (Esophagitis) Basics OVERVIEW Inflammation of the esophagus typically involves the tubular area of the esophagus itself (known as the esophageal body ) and the muscular area
Sept 13: Aerodigestive Foreign Bodies (updated 08/06) Preceptor: Gereau; Vacation; David & Josh
 Preceptor: Gereau; Vacation; David & Josh") Sept 13: Aerodigestive Foreign Bodies (updated 08/06) Preceptor: Gereau; Vacation; David & Josh 1. (dara) Tell us about different Acids vs. Bases and types of injuries they cause in caustic ingestion.
Sept 13: Aerodigestive Foreign Bodies (updated 08/06) Preceptor: Gereau; Vacation; David & Josh 1. (dara) Tell us about different Acids vs. Bases and types of injuries they cause in caustic ingestion.
Pneumomediastinum and pneumoretroperitoneum PNEUMOMEDIASTINUM AND PNEUMORETROPERITONEUM ASSOCAITED WITH PERFORATED ESOPHAGEAL CANCER
 167 PNEUMOMEDIASTINUM AND PNEUMORETROPERITONEUM ASSOCAITED WITH PERFORATED ESOPHAGEAL CANCER Devadoss CW 1 *, Singla S 2, Mysorekar V 1, Dang M 1, Kenkare M 1, Harish K 3 1. Department of Pathology, M.S.
167 PNEUMOMEDIASTINUM AND PNEUMORETROPERITONEUM ASSOCAITED WITH PERFORATED ESOPHAGEAL CANCER Devadoss CW 1 *, Singla S 2, Mysorekar V 1, Dang M 1, Kenkare M 1, Harish K 3 1. Department of Pathology, M.S.
Update on the Diagnosis and Treatment of Caustic Ingestion
 The Ochsner Journal 9:54 59, 2009 f Academic Division of Ochsner Clinic Foundation Update on the Diagnosis and Treatment of Caustic Ingestion Michael Lupa, MD,* Jacqueline Magne,{ J. Lindhe Guarisco, MD,
The Ochsner Journal 9:54 59, 2009 f Academic Division of Ochsner Clinic Foundation Update on the Diagnosis and Treatment of Caustic Ingestion Michael Lupa, MD,* Jacqueline Magne,{ J. Lindhe Guarisco, MD,
PANCREATIC PSEUDOCYSTS. Madhuri Rao MD PGY-5 Kings County Hospital Center
 PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
Case Report Embedded Pork Bone Causing Esophageal Perforation and an Esophagus-Innominate Artery Fistula
 Case Reports in Gastrointestinal Medicine, Article ID 969862, 4 pages http://dx.doi.org/10.1155/2014/969862 Case Report Embedded Pork Bone Causing Esophageal Perforation and an Esophagus-Innominate Artery
Case Reports in Gastrointestinal Medicine, Article ID 969862, 4 pages http://dx.doi.org/10.1155/2014/969862 Case Report Embedded Pork Bone Causing Esophageal Perforation and an Esophagus-Innominate Artery
Pediatric Ingestion Injuries: Assessment & Treatment
 Pediatric Ingestion Injuries: Assessment & Treatment Benjamin L. Eithun, MSN, CRNP, RN, CPNP-AC, CCRN, TCRN Andrea L. Williams, PhD, RN UW Health & AFCH Case #1 Presentation Dispatched to Sandstone Ridge
Pediatric Ingestion Injuries: Assessment & Treatment Benjamin L. Eithun, MSN, CRNP, RN, CPNP-AC, CCRN, TCRN Andrea L. Williams, PhD, RN UW Health & AFCH Case #1 Presentation Dispatched to Sandstone Ridge
Pneumothorax and Chest Tube Problems
 Pneumothorax and Chest Tube Problems Pneumothorax Definition Air accumulation in the pleural space with secondary lung collapse Sources Visceral pleura Ruptured esophagus Chest wall defect Gas-forming
Pneumothorax and Chest Tube Problems Pneumothorax Definition Air accumulation in the pleural space with secondary lung collapse Sources Visceral pleura Ruptured esophagus Chest wall defect Gas-forming
Oesophagus Esophagus. Symptoms of esophageal disease: Surgical Anatomy.
 Esophagus Surgical Anatomy. The esophagus is a muscular tube 25 cm long occupying the posterior mediastinum and extending from the cricopharyngeal sphincter to the cardia of the stomach 2 cm of this tube
Esophagus Surgical Anatomy. The esophagus is a muscular tube 25 cm long occupying the posterior mediastinum and extending from the cricopharyngeal sphincter to the cardia of the stomach 2 cm of this tube
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology
 Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
Myogenic Control. Esophageal Motility. Enteric Nervous System. Alimentary Tract Motility. Determinants of GI Tract Motility.
 Myogenic Control Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Basic Electrical Rythym: intrinsic rhythmic fluctuation of smooth muscle membrane potential
Myogenic Control Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Basic Electrical Rythym: intrinsic rhythmic fluctuation of smooth muscle membrane potential
Esophageal Motility. Alimentary Tract Motility
 Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions Mixing Allows for greater
Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions Mixing Allows for greater
T HE use ofsegments ofcolon to replace
 \oi. 101, No. COLONIC PERICARDIAL FISTULA* By W. B. MILLER, NI.!)., and \V. 11. NIcALISTER, M.D. ST. LOUIS, MISSOURI T HE use ofsegments ofcolon to replace 01#{149} bypass obstru cti ng esophageal lesions
\oi. 101, No. COLONIC PERICARDIAL FISTULA* By W. B. MILLER, NI.!)., and \V. 11. NIcALISTER, M.D. ST. LOUIS, MISSOURI T HE use ofsegments ofcolon to replace 01#{149} bypass obstru cti ng esophageal lesions
Barrett s Esophagus. lining of the lower esophagus that bears his name (i.e., Barrett's esophagus). We now
. We now") Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
9/18/2015. Disclosures. Objectives. Dysphagia Sherri Ekobena PA-C. I have no relevant financial interests to disclose I have no conflicts of interest
 Dysphagia Sherri Ekobena PA-C Disclosures I have no relevant financial interests to disclose I have no conflicts of interest Objectives Define what dysphagia is Define types of dysphagia Define studies
Dysphagia Sherri Ekobena PA-C Disclosures I have no relevant financial interests to disclose I have no conflicts of interest Objectives Define what dysphagia is Define types of dysphagia Define studies
Diaphragmatic Hernia Presenting With Intrathoracic Perforation
 ISPUB.COM The Internet Journal of Surgery Volume 2 Number 1 Diaphragmatic Hernia Presenting With Intrathoracic Perforation A ERDOGAN Citation A ERDOGAN.. The Internet Journal of Surgery. 2000 Volume 2
ISPUB.COM The Internet Journal of Surgery Volume 2 Number 1 Diaphragmatic Hernia Presenting With Intrathoracic Perforation A ERDOGAN Citation A ERDOGAN.. The Internet Journal of Surgery. 2000 Volume 2
INTRODUCTION TO UPPER ENDOSCOPY
 INTRODUCTION TO UPPER ENDOSCOPY Satish Nagula, MD Associate Professor of Medicine Icahn School of Medicine at Mount Sinai NYSGE First Year Fellows Course July 14, 2018 Early endoscopes 1805: Bozzini Lichtleiter
INTRODUCTION TO UPPER ENDOSCOPY Satish Nagula, MD Associate Professor of Medicine Icahn School of Medicine at Mount Sinai NYSGE First Year Fellows Course July 14, 2018 Early endoscopes 1805: Bozzini Lichtleiter
=Abstract= Ke y words : 1.Esophageal perforation. Department of Thoracic and Cardiovascular Surgery, Hanyang University Hospital
 * * * * ** ** * * * * =Abstract= A ClinicalEvaluation of EsophagealPerforation **** ** **, * *** Background: Esophageal perforation is an extremely lethal injury that requires careful management for survival.
* * * * ** ** * * * * =Abstract= A ClinicalEvaluation of EsophagealPerforation **** ** **, * *** Background: Esophageal perforation is an extremely lethal injury that requires careful management for survival.
Historical perspective
 Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
David Markowitz, MD. Physicians and Surgeons
 Esophageal Motility David Markowitz, MD Columbia University, College of Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions
Esophageal Motility David Markowitz, MD Columbia University, College of Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions
Airway Foreign Body in Children
 Joseph E. Dohar, M.D., M.S. Dr. Dohar Financial Disclosures Alcon consultant Incusmed consultant Otonomy consultant OrbiMed consultant Learning Objectives Identify clinical situations that may require
Joseph E. Dohar, M.D., M.S. Dr. Dohar Financial Disclosures Alcon consultant Incusmed consultant Otonomy consultant OrbiMed consultant Learning Objectives Identify clinical situations that may require