Nicolas Bianchi M.D. May 15th, 2012
|
|
|
- Cody Scott
- 6 years ago
- Views:
Transcription
1 Nicolas Bianchi M.D. May 15th, 2012
2 New concepts in TIA Differential Diagnosis Stroke Syndromes


3 To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the major TIA/stroke syndromes and mimics.
4
5 200K-500K per year in US. Incidence /1000 per year. The incidence of TIA increases exponentially with age regardless of race and gender. Among patients who present with stroke, the prevalence of prior TIA has been reported to range from 7% to 40%.

6 TIA: sudden, focal neurological deficit of presumed vascular origin lasting less than 24 hours. Reversible ischemic neurological deficit : 1-7 days. Became obsolete in the 1970 s as it was found that they all lead to new infarction.
7 transient ischemic attack (TIA): a brief episode of neurological dysfunction caused by focal brain or retinal ischemia, with clinical symptoms typically lasting less than one hour, and without evidence of acute infarction DWI+ in 33% of TIA by old definition More than 6 hours = 50% chance of DWI + DWI+ in some cases of less 30 symptoms.
8

9 TIA: TRANSIENT episode of neurological dysfunction caused by FOCAL brain, spinal cord, or retinal ischemia, without acute infarction. Ischemic Stroke: an infarction of central nervous system tissue. Maybe symptomatic or silent May be DWI -
10 True TIAs Migraines Seizures Syncope Vertigo Myasthenia Medication Side Effects Drugs Use or Intoxications Paroxysmal Dyskinesia Periodic Paralysis
11 For patients with relatively brief symptom duration (i.e. symptoms that persist several hours but less than a day) who do not receive a detailed diagnostic evaluation, it may be difficult to determine whether stroke or TIA is the most appropriate diagnosis. Analogous to the term Acute Coronary Syndrome used in cardiology

12 Transient Ischemic Attack Generally lasts minutes, not seconds or hours Usually stroke risk factors are present Migraine with Aura Multiple identical events; lasts minutes to hours No permanent signs or corresponding MRI findings Often with nausea, photophobia, phonophobia Headache may or may not be present Partial Seizure Often lasts seconds, followed by postictal state Limb shaking and/or change in mentation
13 Among TIA patients who go to ED: 5% have stroke in next 2 days 10% have stroke in next 3 months 25% have recurrent TIA in next 3 months 2.6% have major CV event in next 3 months Admit patient for rapid etiological evaluation and decrease risk of stroke if proper therapy instituted.
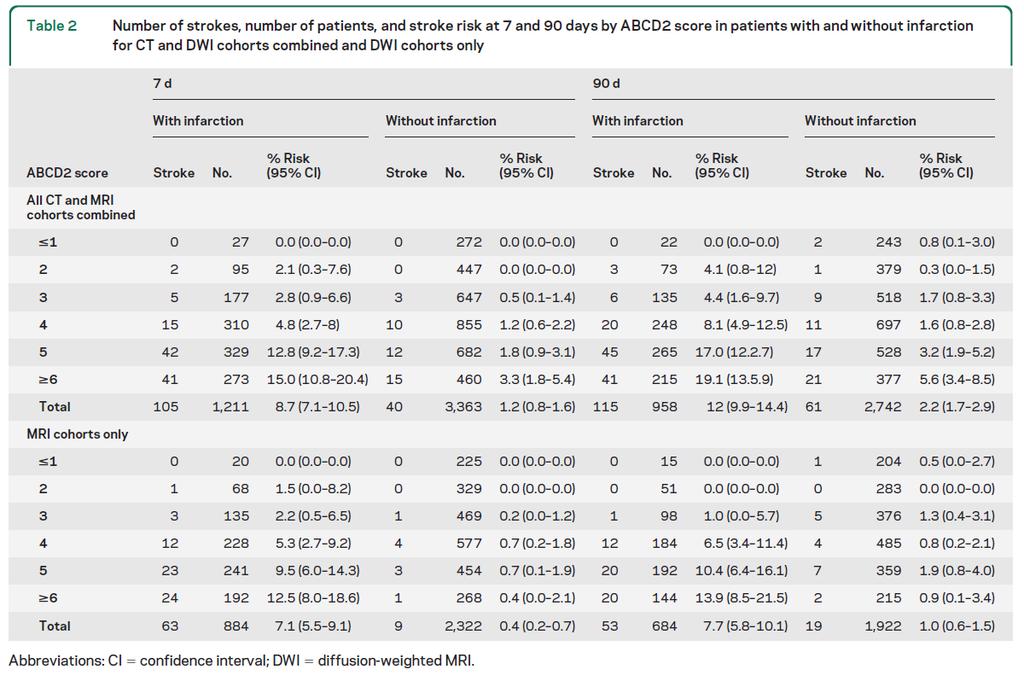
 after tissue-negative events (p diff<0.0001). CT: 12.8% (9.3 17.4) and 3.0% (2.0 4.2), respectively (p diff < 0.0001). The ABCD2 score had predictive value in tissue-positive and tissue-negative events (AUC = 0.")
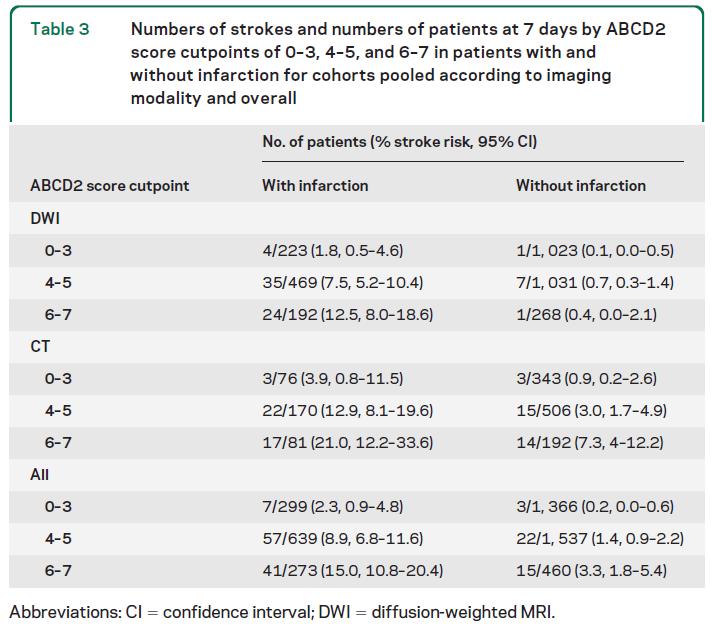
14 4,574 patients from 12 centers. DWI patients (n = 3,206), Recurrent stroke rates at 7 days: DWI: 7.1% (95% confidence interval ) after tissue-positive and 0.4% ( ) after tissue-negative events (p diff<0.0001). CT: 12.8% ( ) and 3.0% ( ), respectively (p diff < ). The ABCD2 score had predictive value in tissue-positive and tissue-negative events (AUC = 0.68 [95% confidence interval ] and 0.73 [ ], respectively; p sig < for both results, p diff = 0.17). Tissue-positive events with low ABCD2 scores and tissuenegative events with high ABCD2 scores had similar stroke risks, especially after a 90-day follow-up.
15
16
17 Predictors of new vascular events included Symptom duration of >1 hour DWI abnormality. Vascular events occurred in 40% of patients with both of these features. Presence of large-vessel occlusive disease.
18 Will allow for rapid thrombolysis in the event a stroke occurs. It permits cardiac monitoring and facilitates rapid diagnostic evaluation: to obtain evidence of a vascular origin for the symptoms either directly (evidence of hypoperfusion and/or acute infarction) or indirectly (identification of a presumptive source such as a large-vessel stenosis). to exclude an alternative non-ischemic origin to ascertain the underlying vascular mechanism of the event which allows selection of the optimal therapy to identify prognostic outcome categories. Rates of adherence to secondary prevention interventions may also be greater after hospitalization.
19 Sudden Focal Neurologic symptom Weakness, Numbness Slurred speech Difficulty speaking or understanding Vertigo, imbalance, difficulty walking, fall Incoordination Impaired vision: amaurosis fugax, Cranial nerve palsies
20 Ischemic stroke Intracerebral hemorrhage Partial seizure with Todd s Paralysis Hypoglycemia Toxic-metabolic insult with old lesion Subdural hematoma Tumor with bleed or seizure Abscess with seizure
21 Ischemic 87% Large Vessel Disease Cardio Embolism Small Vessel Disease Hemodynamic Undetermined Other: dissection Cryptogenic Hemorrhagic 10 % SAH 3%
22 Hemispheric Contralateral Hemiparesis/Heminumbness F/A/T/L Contralateral Visual Field defect Contralateral neglect (Nondominant Cortical) Aphasia (Dominant Cortical) Dysarthria Cerebellar Ipsilateral Ataxia Brainstem Quadriparesis Vertigo Diplopia Dysarthria Dysphagia
23 430 Subarachnoid hemorrhage 431 Intracerebral hemorrhage 432 Other and unspecified intracranial hemorrhage 433 Occlusion and stenosis of precerebral arteries 434 Occlusion of cerebral arteries 435 Transient cerebral ischemia 436 Acute, but ill-defined, cerebrovascular disease 437 Other and ill-defined cerebrovascular disease 438 Late effects of cerebrovascular disease
24 2012 ICD-9-CM Diagnosis Code 435 Transient cerebral ischemia 2012 ICD-9-CM Diagnosis Code Basilar artery syndrome 2012 ICD-9-CM Diagnosis Code Vertebral artery syndrome 2012 ICD-9-CM Diagnosis Code Subclavian steal syndrome 2012 ICD-9-CM Diagnosis Code Vertebrobasilar artery syndrome 2012 ICD-9-CM Diagnosis Code Other specified transient cerebral ischemias 2012 ICD-9-CM Diagnosis Code Unspecified transient cerebral ischemia recurring, transient episodes of neurologic dysfunction caused by cerebral ischemia; onset is usually sudden, often when the patient is active; the attack may last a few seconds to several hours; neurologic symptoms depend on the artery involved. A brief attack (from a few minutes to an hour) of cerebral dysfunction of vascular origin, with no persistent neurological deficit.

25
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
CMS Limitations Guide - Radiology Services
 CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Vague Neurological Conditions
 Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
It s Always a Stroke; Except For When It s Not..
 It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Emergency Department Stroke Registry Indicator Specifications 2018 Report Year (07/01/2017 to 06/30/2018 Discharge Dates)
") 2018 Report Year (07/01/2017 to 06/30/2018 Discharge Dates) Summary of Changes I62.9 added to hemorrhagic stroke ICD-10-CM diagnosis code list (table 3) Measure Description Methodology Rationale Measurement
2018 Report Year (07/01/2017 to 06/30/2018 Discharge Dates) Summary of Changes I62.9 added to hemorrhagic stroke ICD-10-CM diagnosis code list (table 3) Measure Description Methodology Rationale Measurement
Ministry of Health. BC Chronic Disease and Selected Procedure Case Definitions. Chronic Disease Information Working Group. Date Created: June 29, 2015
 Ministry of Health BC Chronic Disease and Selected Procedure Case Definitions Author: Chronic Disease Information Working Group Date Created: June 29, 2015 Last Updated: February 01, 2018 Version: Email:
Ministry of Health BC Chronic Disease and Selected Procedure Case Definitions Author: Chronic Disease Information Working Group Date Created: June 29, 2015 Last Updated: February 01, 2018 Version: Email:
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
TIAs and posterior circulation problems
 TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
Key Clinical Concepts
 Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
Vertebrobasilar Insufficiency
 Equilibrium Res Vol. (3) Vertebrobasilar Insufficiency Toshiaki Yamanaka Department of Otolaryngology-Head and Neck Surgery, Nara Medical University School of Medicine Vertebrobasilar insufficiency (VBI)
Equilibrium Res Vol. (3) Vertebrobasilar Insufficiency Toshiaki Yamanaka Department of Otolaryngology-Head and Neck Surgery, Nara Medical University School of Medicine Vertebrobasilar insufficiency (VBI)
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
TIA Transient Ischaemic Attack?
 TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
PFO closure group total no. PFO closure group no. of males
 Suppl Table. Characteristics of the five trials included in this meta-analysis. Trial name Device used for Definition of medical Primary Endpoint group total no. group no. of males group age (yrs) group
Suppl Table. Characteristics of the five trials included in this meta-analysis. Trial name Device used for Definition of medical Primary Endpoint group total no. group no. of males group age (yrs) group
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)).
).") 12.0 Outcomes 12.1 Definitions 12.1.1 Neurologic Outcome Events a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)). Criteria:
12.0 Outcomes 12.1 Definitions 12.1.1 Neurologic Outcome Events a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)). Criteria:
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Management of TIA. Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital
 Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Emergency Department Stroke Registry Process of Care Indicator Specifications (July 1, 2011 June 30, 2012 Dates of Service)
") Specifications Description Methodology NIH Stroke Scale (NIHSS) Performed in Initial Evaluation used to assess the percentage of adult stroke patients who had the NIHSS performed during their initial evaluation
Specifications Description Methodology NIH Stroke Scale (NIHSS) Performed in Initial Evaluation used to assess the percentage of adult stroke patients who had the NIHSS performed during their initial evaluation
Redgrave JN, Coutts SB, Schulz UG et al. Systematic review of associations between the presence of acute ischemic lesions on
 6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
What Do You Think of My Posterior?
 What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
Medical Review Guidelines Magnetic Resonance Angiography
 Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
CHAPTER 6 NERVOUS SYSTEM G00-G99. Presented by Jan Halloran
 CHAPTER 6 NERVOUS SYSTEM G00-G99 Presented by Jan Halloran 1 LEARNING OUTCOMES After studying this chapter you should be able to: Explain the difference between the central and peripheral nervous systems
CHAPTER 6 NERVOUS SYSTEM G00-G99 Presented by Jan Halloran 1 LEARNING OUTCOMES After studying this chapter you should be able to: Explain the difference between the central and peripheral nervous systems
Headache Assessment In Primary Eye Care
 Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
The determination of eligible population for this measure requires administrative claims data.
 Overuse of Imaging Measure 6: Ratio of Magnetic Resonance Imaging Scans to Computed Tomography Scans for the Evaluation of Children with Atraumatic Headache Description This measure assesses the ratio
Overuse of Imaging Measure 6: Ratio of Magnetic Resonance Imaging Scans to Computed Tomography Scans for the Evaluation of Children with Atraumatic Headache Description This measure assesses the ratio
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
Identifying Cerebrovascular Disorders. Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine
 Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Approach to a Neurologic Diagnosis
 Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Cerebrovascular accident icd 10
 Cerebrovascular accident icd 10 I69.21 is a billable ICD code used to specify a diagnosis of cognitive deficits following other nontraumatic intracranial hemorrhage. A 'billable code' is detailed. Conventions.
Cerebrovascular accident icd 10 I69.21 is a billable ICD code used to specify a diagnosis of cognitive deficits following other nontraumatic intracranial hemorrhage. A 'billable code' is detailed. Conventions.
Cerebrovascular Disease. RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009
 Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Stroke in the Emergency Room: What do we need to know?
 Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
PFO Management update
 PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 04/26/2014 Radiology Quiz of the Week # 108 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 04/26/2014 Radiology Quiz of the Week # 108 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke (2 of 2) Seizures Altered Mental Status (AMS)
 Stroke (2 of 2) Seizures Altered Mental Status (AMS)") 1 2 3 4 5 Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women
1 2 3 4 5 Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women
Current Clinical Trials for Stroke Survivors in NJ and Philadelphia Areas
 Current Clinical Trials for Survivors in NJ and Philadelphia Areas For more information go to https://clinicaltrials.gov/ and search for the title in search box Condition / Disease 1. Spatial Neglect and
Current Clinical Trials for Survivors in NJ and Philadelphia Areas For more information go to https://clinicaltrials.gov/ and search for the title in search box Condition / Disease 1. Spatial Neglect and
CMS Limitations Guide MRA Radiology Services
 CMS Limitations Guide MRA Radiology Services Starting July 1, 2008, CMS has placed numerous medical necessity limits on tests and procedures. This reference guide provides you with all of the latest changes.
CMS Limitations Guide MRA Radiology Services Starting July 1, 2008, CMS has placed numerous medical necessity limits on tests and procedures. This reference guide provides you with all of the latest changes.
CVA. Alison Atwater PA-C
 CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
Appendix 2C - Stroke Services in Fife
 Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
American Osteopathic College of Occupational and Preventive Medicine 2012 Mid-Year Educational Conference St Petersburg, Florida
 Neurological Neurological Liz Clark, D.O., MPH & TM FAOCOPM MY-2012 49 CFR 391.41(b)(7) "A person is physically qualified to drive a commercial motor vehicle if that person Has no established medical history
Neurological Neurological Liz Clark, D.O., MPH & TM FAOCOPM MY-2012 49 CFR 391.41(b)(7) "A person is physically qualified to drive a commercial motor vehicle if that person Has no established medical history
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Stroke Mimics. Paul Guyler
 Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke (2 of 2) Seizures Altered Mental Status (AMS) Brain Structure and Function
 Stroke (2 of 2) Seizures Altered Mental Status (AMS) Brain Structure and Function") 1 Chapter 15 Neurological Emergencies 2 Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women have
1 Chapter 15 Neurological Emergencies 2 Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women have
OHSU Health Care System
 Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Pathophysiology of stroke
 A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
An Introduc+on to Stroke
 An Introduc+on to Stroke Elizabeth Huntoon MS, MD Assistant Professor Department of Physical Medicine and Rehabilita>on Vanderbilt University School of Medicine Defini+on Sudden focal neurologic deficit
An Introduc+on to Stroke Elizabeth Huntoon MS, MD Assistant Professor Department of Physical Medicine and Rehabilita>on Vanderbilt University School of Medicine Defini+on Sudden focal neurologic deficit
Stroke Mimics. Atlantic Canada Stroke Conference. Dr Warren Fieldus FRCP
 Stroke Mimics Atlantic Canada Stroke Conference Dr Warren Fieldus FRCP No Conflicts of Interest the plan stroke or no stroke QEII Acute Stroke Protocol things to do before the CT common stroke mimics (25
Stroke Mimics Atlantic Canada Stroke Conference Dr Warren Fieldus FRCP No Conflicts of Interest the plan stroke or no stroke QEII Acute Stroke Protocol things to do before the CT common stroke mimics (25
The NIHSS score is 4 (considering 2 pts for the ataxia involving upper and lower limbs.
 Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Chapter 15. Neurologic Emergencies
 Chapter 15 Neurologic Emergencies Introduction (1 of 4) Stroke is the third leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More men than
Chapter 15 Neurologic Emergencies Introduction (1 of 4) Stroke is the third leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More men than
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Neurology Clerkship Learning Objectives
 Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance
Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
DISORDERS OF THE NERVOUS SYSTEM
 DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
Dr Jo-Anne Pon. Consultant Ophthalmologist and Oculoplastic Surgeon Southern Eye Specialists Christchurch
 Dr Jo-Anne Pon Consultant Ophthalmologist and Oculoplastic Surgeon Southern Eye Specialists Christchurch 12:15-12:30 Visual Migraines to be Worried About Visual Migraines To Be Worried About Jo-Anne Pon
Dr Jo-Anne Pon Consultant Ophthalmologist and Oculoplastic Surgeon Southern Eye Specialists Christchurch 12:15-12:30 Visual Migraines to be Worried About Visual Migraines To Be Worried About Jo-Anne Pon
Brain Attacks and Acute Stroke Management
 Brain Attacks and Acute Stroke Management WWW.RN.ORG Reviewed January, 2017, Expires January, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
Brain Attacks and Acute Stroke Management WWW.RN.ORG Reviewed January, 2017, Expires January, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
THE FRAMINGHAM STUDY Protocol for data set vr_soe_2009_m_0522 CRITERIA FOR EVENTS. 1. Cardiovascular Disease
 THE FRAMINGHAM STUDY Protocol for data set vr_soe_2009_m_0522 CRITERIA FOR EVENTS 1. Cardiovascular Disease Cardiovascular disease is considered to have developed if there was a definite manifestation
THE FRAMINGHAM STUDY Protocol for data set vr_soe_2009_m_0522 CRITERIA FOR EVENTS 1. Cardiovascular Disease Cardiovascular disease is considered to have developed if there was a definite manifestation
Cerebrovascular accident icd 10
 Cerebrovascular accident icd 10 Search 1-10-2017 Free, official coding info for 2018 ICD - 10 -CM I69.398 - includes detailed rules, notes, synonyms, ICD -9-CM conversion, index and annotation crosswalks,
Cerebrovascular accident icd 10 Search 1-10-2017 Free, official coding info for 2018 ICD - 10 -CM I69.398 - includes detailed rules, notes, synonyms, ICD -9-CM conversion, index and annotation crosswalks,
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
De-novo headache with transient vertebro-basilar symptoms: role of embryonic hypoglossal artery
 J Headache Pain (2011) 12:639 643 DOI 10.1007/s10194-011-0394-5 BRIEF REPORT De-novo headache with transient vertebro-basilar symptoms: role of embryonic hypoglossal artery Angelo Maurizio Clerici Giuseppe
J Headache Pain (2011) 12:639 643 DOI 10.1007/s10194-011-0394-5 BRIEF REPORT De-novo headache with transient vertebro-basilar symptoms: role of embryonic hypoglossal artery Angelo Maurizio Clerici Giuseppe
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Posterior Circulation Stroke
 Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
University Journal of Medicine and Medical Sciences
 ISSN 2455-2852 Volume 2 Issue 5 2016 Case report -Opalski's syndrome A rare variant of lateral medullary syndrome in TAKAYASUS ARTERITIS SHANKAR GANESH N NAINAR Department of Neurology, MADRAS MEDICAL
ISSN 2455-2852 Volume 2 Issue 5 2016 Case report -Opalski's syndrome A rare variant of lateral medullary syndrome in TAKAYASUS ARTERITIS SHANKAR GANESH N NAINAR Department of Neurology, MADRAS MEDICAL
10/13/2017. AllinaHealthSystems. Stroke Recognition Sandra K Hanson, MD Medical Director United Hospital Stroke Program
 Agenda Stroke Recognition Sandra K Hanson, MD Medical Director United Hospital Stroke Program Vascular anatomy NIH Stroke Scale Recognizing the hard to recognize Distinguishing stroke mimics 1 Symptoms
Agenda Stroke Recognition Sandra K Hanson, MD Medical Director United Hospital Stroke Program Vascular anatomy NIH Stroke Scale Recognizing the hard to recognize Distinguishing stroke mimics 1 Symptoms
TCD AND VASOSPASM SAH
 CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
GOVERNANCE BOARD. 14th January Clinical Audit of Stroke Services. At Shrewsbury and Telford Hospitals NHS Trust
 GOVERNANCE BOARD 14th January 2014 Clinical Audit of Stroke Services At Shrewsbury and Telford Hospitals NHS Trust 1.0 Introduction A clinical review of cases recorded and coded as with a 0-1 day length
GOVERNANCE BOARD 14th January 2014 Clinical Audit of Stroke Services At Shrewsbury and Telford Hospitals NHS Trust 1.0 Introduction A clinical review of cases recorded and coded as with a 0-1 day length
PTA 106 Unit 1 Lecture 3
 PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
Contractor Information. LCD Information. Local Coverage Determination (LCD): Magnetic Resonance Angiography (L34424) Document Information
: Magnetic Resonance Angiography (L34424) Document Information") Local Coverage Determination (LCD): Magnetic Resonance Angiography (L34424) Links in PDF documents are not guaranteed to work. To follow a web link, please use the MCD Website. Contractor Information Contractor
Local Coverage Determination (LCD): Magnetic Resonance Angiography (L34424) Links in PDF documents are not guaranteed to work. To follow a web link, please use the MCD Website. Contractor Information Contractor
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Faculty Disclosure. Sanjay P. Singh, MD, FAAN. Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion
 Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
JAWDA Guidelines for Pre-hospital Emergency Medical Service (EMS)
") JAWDA Guidelines for Pre-hospital Emergency Medical Service (EMS) January 2019 Page 1 of 17 Table of Contents Executive Summary... 3 About this Guidance... 4 Emergency Medical Service Performance Indicators...
JAWDA Guidelines for Pre-hospital Emergency Medical Service (EMS) January 2019 Page 1 of 17 Table of Contents Executive Summary... 3 About this Guidance... 4 Emergency Medical Service Performance Indicators...
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
Manual 3c. Stroke Cohort Surveillance Procedures Manual of Operations
 ATHEROSCLEROSIS RISK IN COMMUNITIES STUDY Manual 3c Stroke Cohort Surveillance Procedures Manual of Operations Version 1 8/31/2018 Sponsored by: http://www.nhlbi.nih.gov/ National Heart, Lung, and Blood
ATHEROSCLEROSIS RISK IN COMMUNITIES STUDY Manual 3c Stroke Cohort Surveillance Procedures Manual of Operations Version 1 8/31/2018 Sponsored by: http://www.nhlbi.nih.gov/ National Heart, Lung, and Blood
Supplementary Online Content
 Supplementary Online Content Guimarães PO, Krishnamoorthy A, Kaltenbach LA, et al. Accuracy of medical claims for identifying cardiovascular and bleeding events after myocardial infarction: a secondary
Supplementary Online Content Guimarães PO, Krishnamoorthy A, Kaltenbach LA, et al. Accuracy of medical claims for identifying cardiovascular and bleeding events after myocardial infarction: a secondary
with susceptibility-weighted imaging and computed tomography perfusion abnormalities in diagnosis of classic migraine
 Emerg Radiol (2012) 19:565 569 DOI 10.1007/s10140-012-1051-2 CASE REPORT Susceptibility-weighted imaging and computed tomography perfusion abnormalities in diagnosis of classic migraine Christopher Miller
Emerg Radiol (2012) 19:565 569 DOI 10.1007/s10140-012-1051-2 CASE REPORT Susceptibility-weighted imaging and computed tomography perfusion abnormalities in diagnosis of classic migraine Christopher Miller
SYNCOPE. Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope
 SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
Cognitive Rehabilitation
 Last Review Date: March 10, 2017 Number: MG.MM.ME.58Cv2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Last Review Date: March 10, 2017 Number: MG.MM.ME.58Cv2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Documentation for the IRF Provider
 Documentation for the IRF Provider Timothy N. Brundage, MD, CCDS Certified Clinical Documentation Specialist DrBrundage@gmail.com 1 Medicare controls the ball field If you want to play ball, you have to
Documentation for the IRF Provider Timothy N. Brundage, MD, CCDS Certified Clinical Documentation Specialist DrBrundage@gmail.com 1 Medicare controls the ball field If you want to play ball, you have to
Single Seizure of Unknown Cause
 S1: Medical Standards for Safety Critical Workers with Seizures of Unknown Cause 1. Seizure or Epilepsy of Unknown Cause are the classifications used in these medical standards for a probable seizure(s),
S1: Medical Standards for Safety Critical Workers with Seizures of Unknown Cause 1. Seizure or Epilepsy of Unknown Cause are the classifications used in these medical standards for a probable seizure(s),
NEURORADIOLOGY DIL part 4
 NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL