Lisa T. Hannegan, MS, CNS, ACNP. Department of Neurological Surgery University of California, San Francisco
|
|
|
- Cecil Booth
- 6 years ago
- Views:
Transcription



1 Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco
2 Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature Respiratory Rate Oxygen saturation Central venous Pressure Occasional use of intracranial pressure (ICP) monitoring
3 Era of Physiologic Monitoring Intracranial Pressure Monitoring Occasional use of jugular bulb venous oxygen saturation (SjvO 2 ) monitoring
4 Era of Multimodality Monitoring and Neurophysiologic Decision Support Goal-directed therapy Wartenburg et al., Critical Care Clinics, 23 (2007)
5 Primary Brain Injury Due to an illness or condition Secondary Brain Injury Follows the initial neurologic insult

6 Primary Brain Injury Due to an illness or condition Secondary Brain Injury Follows the initial neurologic insult The primary focus of Neurocritical Care for CNS problems is the prevention, identification, and treatment of secondary brain injury. Claude Hemphill

7
8

9 WHY MONITOR? Detect neurological worsening before irreversible damage occurs Individualize patient care Guide management Monitor response to interventions Understand pathophysiology Design protocols Improve outcome
10 WHAT PROCESSES TO MONITOR? Substrate delivery Blood flow Perfusion Energy failure and cellular stress Intracranial pressure Metabolic byproducts of ischemia
11 WHICH MONITORS? Cardiac and respiratory physiology Heart rate and rhythm, EF etc. FiO 2, TV, PEEP, etc. Intracranial pressure Cerebral perfusion pressure Cerebral Blood Flow Transcranial Doppler, thermal diffusion, laser Doppler flowmetry
12 WHICH MONITORS? Brain oximetry Jugular bulb venous oxygen saturation (SjO2) Brain tissue oxygen tension (PbtO2, NIRS) Oxidative metabolism Cerebral microdialysis (lactate, LPR) Cellular stress Cerebral microdialysis (glutamate, glycerol) Continuous EEG (ceeg)
13
14 Monro-Kellie 80% brain 10% circulating blood 10% CSF

15
16 P1 Percussive peak P2 Tidal peak P3 Dichrotic notch
17 P1 Percussive peak P2 Tidal peak P3 Dichrotic notch C waves B waves A (plateau) waves
18 Normal pressure 0-10 Threshold to treat >20-25
19 CPP = MAP - ICP
20 CPP = MAP - ICP CPP = MAP JVP (if JVP > ICP)
21 CPP = MAP - ICP CPP = MAP JVP (if JVP > ICP) Must be maintained within normal limits Optimal pressure is mm HG Too low ischemia Too high increased ICP
22 Flow remains constant over a range of CPP Flow is constant from MAP of about This relationship does not hold true with very low CPP, very high CPP and in injured brain. Therefore, DIRECT MEASUREMENT is valuable in injured brain.
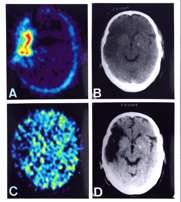
23 Kety-Schmidt technique Xenon or krypton nuclear medicine studies SPECT, Xenon CT O 15 PET Perfusion CT or MRI Transcranial Doppler (TCD) These are all static techniques

24

25
26 Commonly used as a non-invasive test of cerebral blood flow in vasospasm related to subarachnoid hemorrhage Uses flow velocity to infer vessel diameter Use of Lindegaard Index to predict vasospasm eliminates elevated velocities related to hyperemia and loss of autoregulation Results are operator-dependent
27 Continuous measurement techniques Laser Doppler Flowmetry Assesses the volume or concentration and flow velocity of red blood cells in a small volume (mm 3 ) and generates a flow signal Thermal Diffusion Quantitative estimation of flow in ml/100g per minute based on the tissue s ability to dissipate heat


28 Real-time measurement of microvascular RBC perfusion in tissue Measured in BPUs
29 Advantages Directly measures flow velocity in a region of interest Many of the probes are MRI compatible Does not need regular calibration
30 Advantages Directly measures flow velocity in a region of interest Many of the probes are MRI compatible Does not need regular calibration Disadvantages Probes are susceptible to artifact Area of flow studied is tiny at 1mm 3 BPUs not directly translatable to physiological data Results vary depending on various blood parameters such as hematocrit
31 Two thermistors at the tip of a flexible catheter embedded in the white matter. The proximal thermistor measures the brain temperature in degrees Celsius
32 Two thermistors at the tip of a flexible catheter embedded in the white matter. The proximal thermistor measures the brain temperature in degrees Celsius The distal thermistor is programmed to a temperature two degrees above the temperature at the proximal thermistor

33 The energy used by the distal thermistor to maintain the temperature 2 degrees higher reflects the tissue blood flow.


34
35 Advantages Reflects cerebral blood flow to a region of interest Direct correlation between flow intra-operatively during and after temporary arterial occlusion for aneurysm clipping. (Thome et al., J Neurosurg, 2001) Correlation between thermal diffusion CBF results with PbrO2 in patients with SAH and TBI Jaeger et al, Achta Neurochir, 2005 Larger sampling area than laser Doppler flowmetry
36 Disadvantages Small sample area reflects regional flow Temperature cutoff reduces sampling time in febrile patients Must use another invasive procedure to replace non-functioning catheter
37 Range of values for CBF Normal CBF 50mL/100g/min Loss of normal neuronal function and threshold for tissue ischemia <20mL/100g/min
38 Indications Detection of non-convulsive seizures Characterization of spells such as posturing, eye movements, and unexplained changes in heart rate and blood pressure
39 Indications Detection of non-convulsive seizures Characterization of spells such as posturing, eye movements, and unexplained changes in heart rate and blood pressure Assessment of LOC during sedation and paralysis Detection of ischemia after SAH and during procedures Prognostication
40 Up to 35% of Neuro Intensive Care patients have subclinical seizures Claassen J, et al (2004) Detection of electrographic seizures with continuous EEG Monitoring in critically ill patients. Neurology 62:

41 EEG showing focal right frontal ictal discharges in a patient with localization-related nonconvulsive status epilepticus
42

43 Elevated ICP Disturbed cerebral metabolism Glutamate elevations Increased lesional mass effect and midline shift Misdirected treatment and diagnostic evaluations Increased mortality
44 Near Infrared spectroscopy Jugular bulb venous oxygenation Direct brain tissue oxygen tension
45 Tissue oxygen pressure versus oxygen saturation SO 2 is a measure of the oxygen carried bound to hemoglobin with 4 oxygen molecules per hemoglobin molecule. PO 2 is related to the amount of oxygen dissolved in the plasma or tissue
46 Near infrared spectroscopy (NIRS) Measures regional oxygen saturation (rso 2 ) noninvasively
47 Near infrared spectroscopy (NIRS) Measures regional oxygen saturation (rso 2 ) noninvasively Works by by analyzing the differences between absorption spectra of oxygenated and deoxygenated hemoglobin
48 Near infrared spectroscopy (NIRS) Measures regional oxygen saturation (rso 2 ) noninvasively Works by by analyzing the differences between absorption spectra of oxygenated and deoxygenated hemoglobin Normal value for rso 2 is 60-80%


49
50 Advantages Non-invasive Simple to apply and change May be useful in operative monitoring for procedures such as carotid endarterectomy
51 Advantages Non-invasive Simple to apply and change May be useful in operative monitoring for procedures such as carotid endarterectomy Disadvantages Limited and variable penetration of infrared light through the skull Inconsistent reliability
52 SjvO 2 is a result of the difference between the cerebral oxygen delivery (supply) and the cerebral metabolic rate of O 2 (CMRO 2 )(demand). SjvO 2 reflects global oxygenation (hemispheric)

53 Dominant internal jugular Position verified by X-Ray Calibration on insertion and every 8 hours
54 Advantages Best use in TBI with global injury associated with hypoperfusion, hypercapnia and elevated ICP Beneficial in SAH and intraoperative use
55 Advantages Best use in TBI with global injury associated with hypoperfusion, hypercapnia and elevated ICP Beneficial in SAH and intraoperative monitoring Disadvantages Limited by changes in PaO 2 and hemodilution Frequent calibration No information about smaller regions of interest Complications Infection jugular thrombosis Pneumothorax increased ICP
56 Range of SjvO 2 Values 50-75% Normal SjvO 2 <50% indicates increased oxygen extraction fraction (OEF) SjvO 2 >75% indicates reduced OEF and hyperemia In comatose patients, even a single desaturation to SjvO 2 less than 50% was correlated with increased mortality Feldman and Robertson, Critical Care Clinics, 1997, 13:51-77
57 Measures regional tissue oxygen pressure in a small area of the brain (P b O 2, P br O 2, P ti O 2, P bt O 2 ) Uses a microcatheter inserted into the brain parenchyma in a region of interest in the white matter Depending on the device, one can also monitor temperature, PCO 2 and ph. Can be tunneled after craniotomy or placed through a multi-lumen bolt Measured tissue volume is ~17mm 3
58 Range of P bt O 2 values Normal P bt O 2 is 20 in white matter and in gray matter Levels consistently >35mmHg correlate with good recovery Levels <20 indicate cerebral hypoxia Levels < 8 mmhg predict poor outcome
59 Normal values for additional modalities P bt CO 2 is 43-55mm Hg Brain tissue ph is 7.2 Brain temperature correlates with core body temperature with a normal of 37 C

60
61 Advantages Real-time information about autoregulation Proven impact on patient management and outcome
62 Advantages Real-time information regarding autoregulation Proven impact on patient management and outcome Disadvantages Creates artifact on MRI Invasive therapy Difficult to replace non-functioning probes Regional, not global information

63 A technique used to monitor the chemistry of the extracellular space A thin dialysis probe, infused with saline or artificial CSF mimics a cerebral capillary
64 Measures Glucose (substrate) Lactate (reflects anaerobic metabolism) Pyruvate (reflects carbohydrate metabolism) Lactate to pyruvate ratio (LPR) Glutamate (reflects cell injury) Glycerol (reflects cell membrane breakdown)
65 Reduced glucose and increased lactate correlate with cerebral hypoxia and with death Temporary arterial occlusion results in lowered glucose and pyruvate and also in elevated lactate and glutamate
66 Advantages Probes are MRI safe Microdialysis can be done at the bedside at a regular interval Changes in values are early indications of ischemia
67 Advantages Probes are MRI safe Microdialysis can be done at the bedside at a regular interval Changes in values are early indications of ischemia Disadvantages Focal information Current technology is limited to observation of trends
68 DIALYSIS CONCENTRATION REINSTRUP et al SCHULZ et al CLINICAL USE Glucose (mmol/l 1.7 (+/- 0.9) 2.1 (+/- 0.2) < 2.0 LPR 23 (+/- 4) 19 (+/- 2) > 25 Glycerol (µmol/l) 82 (+/- 44) 82 (+/- 12) > 100 Glutamate (µmol/l) 16 (+/- 16) 14 (+/- 3.3) >15 Reinstrup et al,, Neurosurgery 2000; 47: Schulz et al, J Neurosurg 2000; 93: Table adapted from a presentation by Peter LeRoux, MD, FACS
69 Provide an optimal cellular environment in order to preserve neurologic function and allow the best chance for recovery to occur DeGeorgia and Deogaonkar, The Neurologist, 2005

70 Multimodality monitoring for neurophysiologic decision support Goal-directed therapy Proactive patient care management
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
Cosa chiedo alla PtO 2
 Cosa chiedo alla PtO 2 Pr Mauro Oddo Department of Medical-Surgical Intensive Care Medicine CHUV-Lausanne University Hospital Faculty of Biology and Medicine, University of Lausanne, Switzerland NEURO
Cosa chiedo alla PtO 2 Pr Mauro Oddo Department of Medical-Surgical Intensive Care Medicine CHUV-Lausanne University Hospital Faculty of Biology and Medicine, University of Lausanne, Switzerland NEURO
Stroke & Neurovascular Center of New Jersey. Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center
 Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Current bedside monitors of brain blood flow and oxygen delivery
 24. Brain Chemistry Current bedside monitors of brain blood flow and oxygen delivery Global monitors Cannot detect regional abnormalities Local monitors Sample only a small region of the brain and highly
24. Brain Chemistry Current bedside monitors of brain blood flow and oxygen delivery Global monitors Cannot detect regional abnormalities Local monitors Sample only a small region of the brain and highly
ICP (Intracranial Pressure) Monitoring Brain Tissue Oxygen Monitoring Jugular Venous Bulb Oximetry
 Monitoring Brain Tissue Oxygen Monitoring Jugular Venous Bulb Oximetry") ICP (Intracranial Pressure) Monitoring Secondary brain injury may be a direct consequence of intracranial hypertension. Therefore monitoring of ICP and cerebral perfusion pressure (CPP) are immediate priority
ICP (Intracranial Pressure) Monitoring Secondary brain injury may be a direct consequence of intracranial hypertension. Therefore monitoring of ICP and cerebral perfusion pressure (CPP) are immediate priority
Neurocritical Care Monitoring. Academic Half Day Critical Care Fellows
 Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Continuous cerebral autoregulation monitoring
 Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
Positron Emission Tomography Imaging in Brain Injured Patients
 Positron Emission Tomography Imaging in Brain Injured Patients Paul Vespa, MD Professor Director of Neurocritical Care UCLA Brain Injury Research Center Outline Clinical Context of imaging Practical issues
Positron Emission Tomography Imaging in Brain Injured Patients Paul Vespa, MD Professor Director of Neurocritical Care UCLA Brain Injury Research Center Outline Clinical Context of imaging Practical issues
Monitoring of Regional Cerebral Blood Flow Using an Implanted Cerebral Thermal Perfusion Probe Archived Medical Policy
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
R Adams Cowley Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland.
 R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
Functional cerebral monitoring in patients with critically illness
 Functional cerebral monitoring in patients with critically illness Anne-Marie Guerguerian MD PhD Assistant Professor of Critical Care Medicine & Pediatrics Scientist in Neurosciences & Mental Health, Research
Functional cerebral monitoring in patients with critically illness Anne-Marie Guerguerian MD PhD Assistant Professor of Critical Care Medicine & Pediatrics Scientist in Neurosciences & Mental Health, Research
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neuro Quiz 29 Transcranial Doppler Monitoring
 Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Near Infrared Spectroscopy in Neonatal Intensive Care
 Near Infrared Spectroscopy in Neonatal Intensive Care Adré J. du Plessis, MBChB Fetal-Neonatal Neurology, Children s Hospital, Boston, MA Children s Hospital and Harvard Medical School Disclosure Statement
Near Infrared Spectroscopy in Neonatal Intensive Care Adré J. du Plessis, MBChB Fetal-Neonatal Neurology, Children s Hospital, Boston, MA Children s Hospital and Harvard Medical School Disclosure Statement
Precision Medicine in Neurocritical Care: Should we individualize care?
 Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
Multimodal Neurocritical Care Monitoring: Conceptual Approach and Indications
 REVIEW online ML Comm J Neurocrit Care 28;1:117-127 ISSN 1226-657 Multimodal Neurocritical Care Monitoring: Conceptual Approach and Indications Scott G. Glickman, DO, PhD, MPH and Axel J. Rosengart, MD,
REVIEW online ML Comm J Neurocrit Care 28;1:117-127 ISSN 1226-657 Multimodal Neurocritical Care Monitoring: Conceptual Approach and Indications Scott G. Glickman, DO, PhD, MPH and Axel J. Rosengart, MD,
perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP?
 7. Cerebral perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP? Douglas J. Miller Miller JD, Stanek A, Langfitt
7. Cerebral perfusion pressure: Definitions. Implication on management protocols. What happens when CPP is too low, and when it is too high? Non-invasive CPP? Douglas J. Miller Miller JD, Stanek A, Langfitt
NO CONFLICTS NO CONFLICTS
 Anesthesia and Critical Care Medicine Department of Surgical Specialties, Radiological Sciences and Public Health, University of Brescia; Department of Anesthesia, Critical Care and Emergency, Spedali
Anesthesia and Critical Care Medicine Department of Surgical Specialties, Radiological Sciences and Public Health, University of Brescia; Department of Anesthesia, Critical Care and Emergency, Spedali
Bedside microdialysis for early detection of cerebral hypoxia in traumatic brain injury
 Neurosurg Focus 9 (5):E2, 2000 Bedside microdialysis for early detection of cerebral hypoxia in traumatic brain injury ASITA S. SARRAFZADEH, M.D., OLIVER W. SAKOWITZ, M.D., TIM A. CALLSEN, M.D., WOLFGANG
Neurosurg Focus 9 (5):E2, 2000 Bedside microdialysis for early detection of cerebral hypoxia in traumatic brain injury ASITA S. SARRAFZADEH, M.D., OLIVER W. SAKOWITZ, M.D., TIM A. CALLSEN, M.D., WOLFGANG
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
CEA and cerebral protection Volodymyr labinskyy, MD
 CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
Raw and Quantitative EEG for Identification of Ischemia
 Raw and Quantitative EEG for Identification of Ischemia Susan T. Herman, MD Assistant Professor of Neurology Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Disclosures None relevant
Raw and Quantitative EEG for Identification of Ischemia Susan T. Herman, MD Assistant Professor of Neurology Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Disclosures None relevant
What is elevated ICP?
 What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
9/16/2018. Recognizing & Managing Seizures in Pediatric TBI. Objectives. Definitions and Epidemiology
 Recognizing & Managing Seizures in Pediatric TBI UW Medicine EMS & Trauma 2018 Conference September 17 and 18, 2018 Mark Wainwright MD PhD Herman and Faye Sarkowsky Professor of Neurology Division Head,
Recognizing & Managing Seizures in Pediatric TBI UW Medicine EMS & Trauma 2018 Conference September 17 and 18, 2018 Mark Wainwright MD PhD Herman and Faye Sarkowsky Professor of Neurology Division Head,
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
On behalf of the education Committee of the SNACC
 Neuro Quiz 36 Cerebral Oximetry Shobana Rajan M.D, Assistant Professor Anesthesiology Cleveland Clinic Quiz Team; Suneeta Gollapudy M.D, Angele Marie Theard M.D, Verghese Cherian M.D On behalf of the education
Neuro Quiz 36 Cerebral Oximetry Shobana Rajan M.D, Assistant Professor Anesthesiology Cleveland Clinic Quiz Team; Suneeta Gollapudy M.D, Angele Marie Theard M.D, Verghese Cherian M.D On behalf of the education
JAONS. OFFICIAL JOURNAL OF THE AMERICAN ORGANIZATION OF NEUROLOGICAL SURGEONS And ACOS NEUROSURGICAL SECTION
 JAONS OFFICIAL JOURNAL OF THE AMERICAN ORGANIZATION OF NEUROLOGICAL SURGEONS And ACOS NEUROSURGICAL SECTION VOLUME 9, 2009 INSTRUCTIONS FOR AUTHORS Papers submitted should be original documentation, including
JAONS OFFICIAL JOURNAL OF THE AMERICAN ORGANIZATION OF NEUROLOGICAL SURGEONS And ACOS NEUROSURGICAL SECTION VOLUME 9, 2009 INSTRUCTIONS FOR AUTHORS Papers submitted should be original documentation, including
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
occlusions. Cerebral perfusion is driven fundamentally by regional cerebral
 Appendix Figures Figure A1. Hemodynamic changes that may occur in major anterior circulation occlusions. Cerebral perfusion is driven fundamentally by regional cerebral perfusion pressure (CPP). In response
Appendix Figures Figure A1. Hemodynamic changes that may occur in major anterior circulation occlusions. Cerebral perfusion is driven fundamentally by regional cerebral perfusion pressure (CPP). In response
Severe Traumatic Brain Injury Protocol
 Severe Traumatic Brain Injury Protocol PROTOCOL I. Objective II. Definition of Severe TBI III. Patient Care: Parameters IV. Patient Care: Management Timeline (First 7 days of TBI) V. Nursing Care: Communication
Severe Traumatic Brain Injury Protocol PROTOCOL I. Objective II. Definition of Severe TBI III. Patient Care: Parameters IV. Patient Care: Management Timeline (First 7 days of TBI) V. Nursing Care: Communication
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2): Oxford University Press
: Oxford University Press") Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2):209-217. 2011 Oxford University Press Effect of Phenylephrine and Ephedrine Bolus Treatment on Cerebral Oxygenation in Anaesthetized
Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2):209-217. 2011 Oxford University Press Effect of Phenylephrine and Ephedrine Bolus Treatment on Cerebral Oxygenation in Anaesthetized
Goals and Objectives of the Educational Program
 Goals and Objectives of the Educational Program Neurosurgical Fellowship Definition: This fellowship is designed to give concise and formal training in neurosurgical anesthesia at LAC+USC Medical Center
Goals and Objectives of the Educational Program Neurosurgical Fellowship Definition: This fellowship is designed to give concise and formal training in neurosurgical anesthesia at LAC+USC Medical Center
TCD AND VASOSPASM SAH
 CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
Stanford Neuroanesthesia Syllabus: Journal Article Directory (click on section heading)
") 1 Stanford Neuroanesthesia Syllabus: Journal Article Directory (click on section heading) The least I should read Anesthetic agents Neuroprotection Carotids Aneurysms Avms TUMors Awake craniotomy Trauma/emergencies
1 Stanford Neuroanesthesia Syllabus: Journal Article Directory (click on section heading) The least I should read Anesthetic agents Neuroprotection Carotids Aneurysms Avms TUMors Awake craniotomy Trauma/emergencies
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Alessandro Della Puppa
 Intraoperative measurement of arterial blood flow in complex cerebral aneurysms surgery Studio flussimetrico intra-operatorio nel clipping degli aneurismi complessi Alessandro Della Puppa NEUROSURGERY
Intraoperative measurement of arterial blood flow in complex cerebral aneurysms surgery Studio flussimetrico intra-operatorio nel clipping degli aneurismi complessi Alessandro Della Puppa NEUROSURGERY
Evaluation & Management of Elevated Intracranial Pressure in Adults. Dr. Tawfiq Almezeiny
 Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management of Traumatic Brain Injury. C. Werner
 Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION
 TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION ---Rune Aaslid First TCD Publication 1982 WHAT IS TCD? Uses 2 MHz pulsed Doppler ultrasound Passes through cranial windows Provides information
TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION ---Rune Aaslid First TCD Publication 1982 WHAT IS TCD? Uses 2 MHz pulsed Doppler ultrasound Passes through cranial windows Provides information
Christian T Devlin; Naimeh Tashakkorinia MD; Thomas Glenn Devlin MD PhD
 Validation of the Ornim UTLight Flowmetry Device in the Measurement of Cerebral Blood FLow in Acute Stroke Patients Undergoing Emergent Endovascular Therapy Christian T Devlin; Naimeh Tashakkorinia MD;
Validation of the Ornim UTLight Flowmetry Device in the Measurement of Cerebral Blood FLow in Acute Stroke Patients Undergoing Emergent Endovascular Therapy Christian T Devlin; Naimeh Tashakkorinia MD;
CEREBRAL OXIMETRY IN INFANTS WITH HIE DAPHNA YASOVA BARBEAU, MD FN3 MEETING 2018
 CEREBRAL OXIMETRY IN INFANTS WITH HIE DAPHNA YASOVA BARBEAU, MD FN3 MEETING 2018 OBJECTIVES 1. Understand how cerebral oximetry works 2. Understand how cerebral oximetry may guide intervention 3. Learn
CEREBRAL OXIMETRY IN INFANTS WITH HIE DAPHNA YASOVA BARBEAU, MD FN3 MEETING 2018 OBJECTIVES 1. Understand how cerebral oximetry works 2. Understand how cerebral oximetry may guide intervention 3. Learn
Plenary Address: Medico-Legal Issues in Neuro-intensive Care
 Plenary Address: Medico-Legal Issues in Neuro-intensive Care Dr Basil Matta Divisional Director, Emergency and Perioperative Care Cambridge University Hospitals NHS Foundation Trust Medico-Legal Issues
Plenary Address: Medico-Legal Issues in Neuro-intensive Care Dr Basil Matta Divisional Director, Emergency and Perioperative Care Cambridge University Hospitals NHS Foundation Trust Medico-Legal Issues
give lorazepam Page 1 UC SF First known description of status epilepticus (Sakikku cuneiform, ca. 700 B.C) NEUROCRITICAL CARE PROGRAM
 NEUROCRITICAL CARE PROGRAM") Update on Neurocritical Care J. Claude Hemphill III, MD, MAS Special Thanks to: Jan Claassen, MD, PhD Division of Critical Care Neurology Columbia University Disclosures Research Support: NIH/NINDS Stock
Update on Neurocritical Care J. Claude Hemphill III, MD, MAS Special Thanks to: Jan Claassen, MD, PhD Division of Critical Care Neurology Columbia University Disclosures Research Support: NIH/NINDS Stock
Respiratory Physiology Part II. Bio 219 Napa Valley College Dr. Adam Ross
 Respiratory Physiology Part II Bio 219 Napa Valley College Dr. Adam Ross Gas exchange Gas exchange in the lungs (to capillaries) occurs by diffusion across respiratory membrane due to differences in partial
Respiratory Physiology Part II Bio 219 Napa Valley College Dr. Adam Ross Gas exchange Gas exchange in the lungs (to capillaries) occurs by diffusion across respiratory membrane due to differences in partial
Pediatric Head Trauma August 2016
 PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
Management of Traumatic Brain Injury (and other neurosurgical emergencies)
") Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Dynamic autoregulatory response after severe head injury
 J Neurosurg 97:1054 1061, 2002 Dynamic autoregulatory response after severe head injury ROMAN HLATKY, M.D., YU FURUYA, M.D., PH.D., ALEX B. VALADKA, M.D., JORGE GONZALEZ, M.D., ARI CHACKO, M.D., YASU MIZUTANI,
J Neurosurg 97:1054 1061, 2002 Dynamic autoregulatory response after severe head injury ROMAN HLATKY, M.D., YU FURUYA, M.D., PH.D., ALEX B. VALADKA, M.D., JORGE GONZALEZ, M.D., ARI CHACKO, M.D., YASU MIZUTANI,
Continuous monitoring of jugular venous oxygen saturation in head-injured patients
 J Neurosurg 76:212-217, 1992 Continuous monitoring of jugular venous oxygen saturation in head-injured patients MICHAEL SHEINBERG, B.S., MALCOLM,J. KANTER~ M.D., CLAUDIA S. ROBERTSON, M.D., CHARLES F.
J Neurosurg 76:212-217, 1992 Continuous monitoring of jugular venous oxygen saturation in head-injured patients MICHAEL SHEINBERG, B.S., MALCOLM,J. KANTER~ M.D., CLAUDIA S. ROBERTSON, M.D., CHARLES F.
TCD IN THE NICU, PICU AND OTHER APPLICATIONS. Dorothy Bulas M.D. Professor of Pediatrics & Radiology Children s National Washington D.C.
 TCD IN THE NICU, PICU AND OTHER APPLICATIONS Dorothy Bulas M.D. Professor of Pediatrics & Radiology Children s National Washington D.C. Objectives Recognize normal and abnormal cranial blood flow patterns
TCD IN THE NICU, PICU AND OTHER APPLICATIONS Dorothy Bulas M.D. Professor of Pediatrics & Radiology Children s National Washington D.C. Objectives Recognize normal and abnormal cranial blood flow patterns
TCD in Anaesthesiology
 TCD in Anaesthesiology Background: TCD has often been used to evaluate the impact of narcotics on cerebral autoregulation. This was related to general research reasons and is not relevant for daily monitoring
TCD in Anaesthesiology Background: TCD has often been used to evaluate the impact of narcotics on cerebral autoregulation. This was related to general research reasons and is not relevant for daily monitoring
CEREBRAL DECONGESTANTS. Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS
 CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
Absolute Cerebral Oximeters for Cardiovascular Surgical Cases
 Absolute Cerebral Oximeters for Cardiovascular Surgical Cases Mary E. Arthur, MD, Associate Professor, Anesthesiology and Perioperative Medicine Medical College of Georgia at Georgia Regents University
Absolute Cerebral Oximeters for Cardiovascular Surgical Cases Mary E. Arthur, MD, Associate Professor, Anesthesiology and Perioperative Medicine Medical College of Georgia at Georgia Regents University
NEUROMONITORING AND ANESTHESIA CONSIDERATIONS. Martha Richter, MSN, CRNA
 NEUROMONITORING AND ANESTHESIA CONSIDERATIONS Martha Richter, MSN, CRNA OBJECTIVES The student will 1. Review the types of neuromonitoring currently in use 2. Identify possible procedural applications
NEUROMONITORING AND ANESTHESIA CONSIDERATIONS Martha Richter, MSN, CRNA OBJECTIVES The student will 1. Review the types of neuromonitoring currently in use 2. Identify possible procedural applications
Multimodality Monitoring in the Neurointensive Care Unit: A Special Perspective for Patients with Stroke
 Journal of Stroke 213;15(2):99-18 Review Multimodality Monitoring in the Neurointensive Care Unit: A Special Perspective for Patients with Stroke Sang-Bae Ko Department of Neurology, Seoul National University
Journal of Stroke 213;15(2):99-18 Review Multimodality Monitoring in the Neurointensive Care Unit: A Special Perspective for Patients with Stroke Sang-Bae Ko Department of Neurology, Seoul National University
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
Quiz 43. This quiz is being published on behalf of the Education Committee of the SNACC. Start. Traumatic Brain Injury 101
 Quiz 43 Traumatic Brain Injury 101 SUNEETA GOLLAPUDY, M.D ASSOCIATE PROFESSOR, DIVISION DIRECTOR - NEUROANESTHESIA, MEDICAL COLLEGE OF WISCONSIN, MILWAUKEE, WI QUIZ TEAM: SHOBANA RAJAN, M.D; SUNEETA GOLLAPUDY,
Quiz 43 Traumatic Brain Injury 101 SUNEETA GOLLAPUDY, M.D ASSOCIATE PROFESSOR, DIVISION DIRECTOR - NEUROANESTHESIA, MEDICAL COLLEGE OF WISCONSIN, MILWAUKEE, WI QUIZ TEAM: SHOBANA RAJAN, M.D; SUNEETA GOLLAPUDY,
Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency
 Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency Traumatic Brain Injury Causes Pathophysiology Neurologic assessment Therapeutic Approach Status
Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency Traumatic Brain Injury Causes Pathophysiology Neurologic assessment Therapeutic Approach Status
Concussion: Research Overview
 Concussion: Research Overview September 30, 2013 Hugh J.L. Garton, M.D.,M.HSc. Dept. of Neurosurgery University of Michigan No Disclosures Overview Anatomy / Definitions Biomechanics Cerebral Blood Flow
Concussion: Research Overview September 30, 2013 Hugh J.L. Garton, M.D.,M.HSc. Dept. of Neurosurgery University of Michigan No Disclosures Overview Anatomy / Definitions Biomechanics Cerebral Blood Flow
Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage
 Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Cerebral Oxygen Desaturation with Normal ICP and CPP in Severe TBI
 The Open Critical Care Medicine Journal,, 1, -3 Open Access Cerebral Oxygen Desaturation with Normal ICP and CPP in Severe TBI Sylvain Palmer *,1 and Mary Kay Bader 1 Orange County Neurological Associates,
The Open Critical Care Medicine Journal,, 1, -3 Open Access Cerebral Oxygen Desaturation with Normal ICP and CPP in Severe TBI Sylvain Palmer *,1 and Mary Kay Bader 1 Orange County Neurological Associates,
EEG in the ICU: Part I
 EEG in the ICU: Part I Teneille E. Gofton July 2012 Objectives To outline the importance of EEG monitoring in the ICU To briefly review the neurophysiological basis of EEG To introduce formal EEG and subhairline
EEG in the ICU: Part I Teneille E. Gofton July 2012 Objectives To outline the importance of EEG monitoring in the ICU To briefly review the neurophysiological basis of EEG To introduce formal EEG and subhairline
Trauma is the leading cause of death in the first four decades of life, with head injury being
 Correspondence to: Mr PJ Hutchinson, Academic Department of Neurosurgery, University of Cambridge, Box 167, Addenbrooke s Hospital, Cambridge CB2 2QQ, UK: p.hutch@which.net ACUTE HEAD INJURY FOR THE NEUROLOGIST
Correspondence to: Mr PJ Hutchinson, Academic Department of Neurosurgery, University of Cambridge, Box 167, Addenbrooke s Hospital, Cambridge CB2 2QQ, UK: p.hutch@which.net ACUTE HEAD INJURY FOR THE NEUROLOGIST
Conflict of Interest Disclosure J. Claude Hemphill III, MD,MAS. Difficult Diagnosis and Treatment: New Onset Obtundation
 Difficult Diagnosis and Treatment: New Onset Obtundation J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Neurology and Neurological Surgery University of California,
Difficult Diagnosis and Treatment: New Onset Obtundation J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Neurology and Neurological Surgery University of California,
Pressure reactivity: Relationship between ICP and arterial blood pressure (ABP). Pressure-reactivity index, computational methods. Clinical examples.
. Pressure-reactivity index, computational methods. Clinical examples.") Pressure reactivity: Relationship between ICP and arterial blood pressure (ABP). Pressure-reactivity index, computational methods. Clinical examples. Optimization of cerebral perfusion pressure: Relationship
Pressure reactivity: Relationship between ICP and arterial blood pressure (ABP). Pressure-reactivity index, computational methods. Clinical examples. Optimization of cerebral perfusion pressure: Relationship
Postanesthesia Care of the Patient Suffering From Traumatic Brain Injury
 Postanesthesia Care of the Patient Suffering From Traumatic Brain Injury By: Susan Letvak, PhD, RN Rick Hand, CRNA, DNSc Letvak, S. & Hand, R. (2003). Postanesthesia care of the traumatic brain injured
Postanesthesia Care of the Patient Suffering From Traumatic Brain Injury By: Susan Letvak, PhD, RN Rick Hand, CRNA, DNSc Letvak, S. & Hand, R. (2003). Postanesthesia care of the traumatic brain injured
Neurophysiology Lecture One : Neurophysiology and Evoked Potentials Lecture Two: Clinical Neuroanesthesia
 Neurophysiology Lecture One : Neurophysiology and Evoked Potentials Lecture Two: Clinical Neuroanesthesia Reza Gorji, MD University Hospital September 2007 Topics Covered Today Intracranial Pressure Intracranial
Neurophysiology Lecture One : Neurophysiology and Evoked Potentials Lecture Two: Clinical Neuroanesthesia Reza Gorji, MD University Hospital September 2007 Topics Covered Today Intracranial Pressure Intracranial
Regulation of Cerebral Blood Flow. Myogenic- pressure autoregulation Chemical: PaCO2, PaO2 Metabolic Neuronal
 Regulation of Cerebral Blood Flow Myogenic- pressure autoregulation Chemical: PaCO2, PaO2 Metabolic Neuronal The Autoregulation, Stupid! Drawing of her daughter (age 7) Flow through rigid tube Mogens Fog
Regulation of Cerebral Blood Flow Myogenic- pressure autoregulation Chemical: PaCO2, PaO2 Metabolic Neuronal The Autoregulation, Stupid! Drawing of her daughter (age 7) Flow through rigid tube Mogens Fog
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Multimodal monitoring to individualize care in TBI
 Multimodal monitoring to individualize care in TBI Critical Care Canada Forum 2017 October 4 th, 2017 Donald Griesdale MD MPH Associate Professor Department of Anesthesiology, Pharmacology & Therapeutics
Multimodal monitoring to individualize care in TBI Critical Care Canada Forum 2017 October 4 th, 2017 Donald Griesdale MD MPH Associate Professor Department of Anesthesiology, Pharmacology & Therapeutics
Cerebrovascular Pathophysiology and Monitoring in the Neurosurgical Intensive Care Unit
 CHAPTER 4 Cerebrovascular Pathophysiology and Monitoring in the Neurosurgical Intensive Care Unit Jamie S. Ullman The brain uses approximately 20% of the total body oxygen consumption, receiving 15% of
CHAPTER 4 Cerebrovascular Pathophysiology and Monitoring in the Neurosurgical Intensive Care Unit Jamie S. Ullman The brain uses approximately 20% of the total body oxygen consumption, receiving 15% of
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Quality Metrics. Stroke Related Procedure Outcomes
 Quality Metrics Stroke Related Procedure Outcomes Below is a description of some of the stroke-related procedures performed at St. Dominic Hospital in Jackson, with quality information on the complication
Quality Metrics Stroke Related Procedure Outcomes Below is a description of some of the stroke-related procedures performed at St. Dominic Hospital in Jackson, with quality information on the complication
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
T he initial cerebral damage after acute brain injury is often
 PAPER Impact of pyrexia on neurochemistry and cerebral oxygenation after acute brain injury N Stocchetti, A Protti, M Lattuada, S Magnoni, L Longhi, L Ghisoni, M Egidi, E R Zanier... See end of article
PAPER Impact of pyrexia on neurochemistry and cerebral oxygenation after acute brain injury N Stocchetti, A Protti, M Lattuada, S Magnoni, L Longhi, L Ghisoni, M Egidi, E R Zanier... See end of article
Periodic and Rhythmic Patterns. Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina
 Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio
 Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
PACT module. Traumatic Brain Injury. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography
 Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography Poster No.: C-2563 Congress: ECR 2012 Type: Educational
Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography Poster No.: C-2563 Congress: ECR 2012 Type: Educational
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Capnography 101. James A Temple BA, NRP, CCP
 Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Ischemia monitoring after aneurysmal subarachnoid haemorrhage; contribution of brain tissue oxygen and cerebral microdialysis monitoring
 Mémoire de Maitrise de médecine; code 1652 Ischemia monitoring after aneurysmal subarachnoid haemorrhage; contribution of brain tissue oxygen and cerebral microdialysis monitoring (Monitorage de l ischémie
Mémoire de Maitrise de médecine; code 1652 Ischemia monitoring after aneurysmal subarachnoid haemorrhage; contribution of brain tissue oxygen and cerebral microdialysis monitoring (Monitorage de l ischémie
Chandra Ramamoorthy MBBS; FRCA (UK) Professor of Anesthesiology, Stanford University. Director of Pediatric Cardiac Anesthesiology
 Professor of Anesthesiology, Stanford University. Director of Pediatric Cardiac Anesthesiology") Should NIRS be Standard Care for Pediatric CPB Chandra Ramamoorthy MBBS; FRCA (UK) Professor of Anesthesiology, Stanford University Director of Pediatric Cardiac Anesthesiology Stanford Children s Hospital
Should NIRS be Standard Care for Pediatric CPB Chandra Ramamoorthy MBBS; FRCA (UK) Professor of Anesthesiology, Stanford University Director of Pediatric Cardiac Anesthesiology Stanford Children s Hospital
Enhancing patient care in the ICU with NeuroMonitoring
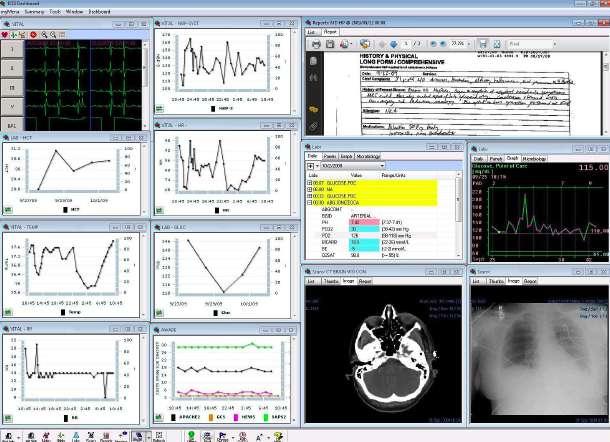
 Enhancing patient care in the ICU with NeuroMonitoring In the ICU, several patient vital signs are monitored continuously. But what about the brain? Hemodynamics Heart rate Non invasive blood pressure
Enhancing patient care in the ICU with NeuroMonitoring In the ICU, several patient vital signs are monitored continuously. But what about the brain? Hemodynamics Heart rate Non invasive blood pressure
Near-Infrared Monitoring of Brain and Tissue Oxygenation: Is the Monitor on the Right Person?
 Near-Infrared Monitoring of Brain and Tissue Oxygenation: Is the Monitor on the Right Person? Frank McGowan, MD, FAAP Professor of Anesthesiology and Critical Care Medicine University of Pennsylvania Perelman
Near-Infrared Monitoring of Brain and Tissue Oxygenation: Is the Monitor on the Right Person? Frank McGowan, MD, FAAP Professor of Anesthesiology and Critical Care Medicine University of Pennsylvania Perelman
ISPUB.COM. Transcranial Doppler: An Overview of its Clinical Applications. A Alexandrov, M Joseph INTRODUCTION SICKLE CELL DISEASE
 ISPUB.COM The Internet Journal of Neuromonitoring Volume 1 Number 1 Transcranial Doppler: An Overview of its Clinical Applications A Alexandrov, M Joseph Citation A Alexandrov, M Joseph. Transcranial Doppler:
ISPUB.COM The Internet Journal of Neuromonitoring Volume 1 Number 1 Transcranial Doppler: An Overview of its Clinical Applications A Alexandrov, M Joseph Citation A Alexandrov, M Joseph. Transcranial Doppler:
Recent trends in the management of head injury
 Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Chapter 62 Monitoring of Hemodynamic Change in Patients with Carotid Artery Stenosis During the Tilt Test Using Wearable Near-Infrared Spectroscopy
 Chapter 62 Monitoring of Hemodynamic Change in Patients with Carotid Artery Stenosis During the Tilt Test Using Wearable Near-Infrared Spectroscopy Takahiro Igarashi, Kaoru Sakatani, Norio Fujiwara, Yoshihiro
Chapter 62 Monitoring of Hemodynamic Change in Patients with Carotid Artery Stenosis During the Tilt Test Using Wearable Near-Infrared Spectroscopy Takahiro Igarashi, Kaoru Sakatani, Norio Fujiwara, Yoshihiro