Can we abolish skull x-rays for head injury?
|
|
|
- Derrick Dennis
- 5 years ago
- Views:
Transcription
1 ADC Online First, published on April 25, 2005 as /adc Can we abolish skull x-rays for head injury? Matthew J Reed, Jen G Browning, A. Graham Wilkinson & Tom Beattie Corresponding author: Matthew J Reed, Accident and Emergency Department, Royal Hospital for Sick Children, Sciennes Road, Edinburgh, UK. address: mattreed1@hotmail.com Royal Hospital for Sick Children Arch Dis Child: first published as /adc on 25 April Downloaded from on 19 August 2018 by guest. Protected by copyright. 1 Copyright Article author (or their employer) Produced by BMJ Publishing Group Ltd (& RCPCH) under licence.
2 Abstract Objectives: To assess the effect of a change in skull x-ray policy on the rate of admission, CT imaging, radiation dose per head injury and detection of intracranial injuries. To compare the characteristics of patients meeting criteria for CT scanning with a group matched for age, triage category and sex. To compare the characteristics of patients with a normal CT scan to those with an abnormal CT scan. Design: Retrospective cohort study. Setting: UK paediatric teaching hospital emergency department (ED). Patients: 1535 patients aged between 1 and 14 years of age presenting to the ED between August 1 st 1998 and July 31 st 1999, and 1867 patients aged between 1 and 14 years of age presenting between August 1 st 2002 and July 31 st 2003 with a head injury. Intervention: Hospital notes and computer systems were analysed and data were collected on all patients presenting with a head injury. Results: The abolition of skull x-rays in children over 1 year of age prevented about 400 normal skull x-rays being performed in period 2. The percentage of children undergoing CT rose from 1.0% to 2.1% with no change in the positive CT pick up rate (25.6% compared to 25.0%). There was no significant change in admission rate (10.9% compared to 10.1%), and a slight decrease in the radiation dose per head injury (0.042mSv compared to msv). Conclusions: Skull x-rays can be successfully abandoned in those aged 1 to 14 without any significant increase in admission rate, radiation dose per head injury, or missed intracranial injury rate. We suggest that routine skull x-rays have no place in the paediatric ED for those children aged 1 year and over. Mechanism of injury, history and a reduced GCS are probably the most important indicators of significant head injury in children. Key words: Head injury, skull x-ray, CT scan. Arch Dis Child: first published as /adc on 25 April Downloaded from on 19 August 2018 by guest. Protected by copyright. 2
3 Introduction One million patients are treated annually in UK emergency departments (ED) for head injury [1]. Children under the age of 16 years make up one half of these [2]. Forty-five percent of these childhood injuries occur in those under 5 years of age [3], most being minor. There are 4011 ED attendances, 400 admissions and 5.3 deaths per 100,000 children per year [4]. Head injuries contribute to 10% of childhood hospital admissions (about 50,000 per year in the UK) [5], and they are one of the leading causes of developed world trauma deaths accounting for 15% of fatalities between the ages of 1 and 15 [6]. Present paediatric guidelines differ in their emphasis on skull x-ray usage. National Institute for Clinical Effectiveness (NICE) guidelines suggest skull x-rays have a role combined with high quality in-patient observation where Computed Tomography (CT) scanning is unavailable [7]. Scottish Intercollegiate Guideline Network (SIGN) guidelines place more emphasis on skull x-rays where there are risk factors for fracture or intracranial injury, although they acknowledge that skull fractures in children are less commonly associated with intracranial injury, and therefore their detection is less helpful than in the adult population [8]. Head injury guidelines from North America omit skull x-rays, and CT is the predominant scanning modality. In the US, up to 60% of head injured patients undergo CT with a resultant low positive rate of between 5 and 10%. Less than 30% of those with intracranial abnormalities go on to require neurosurgical intervention [9]. Between 23% and 50% of skull fractures are missed by junior doctors [10], and there are many false positive diagnoses. The presence of a skull fracture has previously been suggested to hugely increase the risk of an intracranial injury [11,12]. However in children, severe intracranial injury can occur in the absence of a skull fracture [10]. Our ED head injury policy was revised in 1999 to reduce the emphasis on skull x-rays, and to restrict the ordering of them to those aged under 1 year (infants) whom we believe are a special population. They are extremely difficult to assess for symptoms and signs of head injury and they suffer a much higher incidence of non-accidental injury (NAI). This study is therefore restricted to children between the ages of 1 and 14. The revision of our head injury policy gives us a unique opportunity to assess the impact of the abolition of skull x-rays on the management of paediatric head injured patients. There are three main aims to our study: firstly, to assess the effect of a change in skull x-ray policy on the rate of admission, CT imaging, radiation dose per head injury and detection of intracranial injuries in a paediatric ED; secondly, to compare the characteristics of patients meeting criteria for CT scanning with a group matched for age, triage category and sex; and finally, to compare the characteristics of patients having a normal CT scan with those having an abnormal CT scan. Design This study is a retrospective cohort study conducted in the dedicated paediatric ED of a UK teaching hospital. The departmental head injury policy was revised in 1999 to restrict the ordering of skull x-rays to those aged under 1 year (Table 1). For the initial part of the study, the ED computers were interrogated and notes were retrieved for all patients aged over 1 year and under 14 years, presenting within two periods. Period 1 was between August 1 st 1998 and July 31 st 1999, and period 2 was between August 1 st 2002 and July 31 st The first period was chosen as it represents the last full year before the revision of the departmental head injury policy, and the latter period as it represents the most recent comparable full year since the introduction of the revised head injury policy. The radiology department computer was also interrogated, and a list of all CT scans and skull x-rays performed during these periods was compiled. Total radiation doses were calculated for each period using typical radiation doses [13]. The techniques used for skull x-rays and CT scans during both periods Arch Dis Child: first published as /adc on 25 April Downloaded from on 19 August 2018 by guest. Protected by copyright. 3
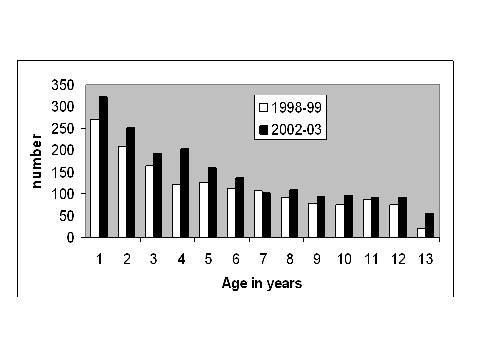
4 were identical. Details of the patient s age, triage category and subsequent destination were also available. For the second part of the study, all patients who underwent a CT scan during period 2 were compared to an equal number of patients matched for age, triage category and sex who also presented during period 2, and who did not undergo a CT scan. The purpose of this was to define characteristics of patients who were thought to be at high risk of a significant head injury and therefore required CT scanning. Hospital notes were retrieved for all patients in both groups, and details of their injury, treatment and subsequent course were all entered on a specially designed proforma. Records were scanned to identify children who returned for unexpected review, or those who deteriorated or developed complications after initial discharge. As our hospital is the only admitting paediatric hospital in the area, all children in this category would have re-attended here or would have been admitted here. Finally, patients having a normal CT scan were compared to patients having an abnormal CT scan. Positive and Negative predictive values were calculated to determine the likelihood of an abnormal CT scan in the presence of each factor, and the likelihood of a normal CT scan in the absence of each factor. These values were calculated in order to determine the usefulness of each factor at predicting significant head injury. Comparison with the second part of the study will determine which factors lead to a CT scan being performed, but which are poorly associated with an abnormal scan. All information collected was analysed using Microsoft Excel. The Fisher exact test was used to compare categorical data and the Mann-Whitney U-test was used to compare non-parametric numerical data. Results During period 1, 1535 patients over 1 year of age and less than 14 years of age presented to the ED, compared to 1867 patients in this age range during period 2 (Table 2). Figure 1 shows the distribution of head injuries by age during both time periods. The male: female ratio in period 1 was 64%: 36% and the median age was 5.02 years (interquartile range ). This compared to a male: female ratio of 67%: 33% during period 2 (p=0.42) with a median age of 4.87 years (IQR years, p=0.62). During period 1 there were 44 patients (2.9% of the total head injuries between 1 and 14 years of age) allocated to triage category 1 or 2 (very serious and urgent categories), and 1491 patients (97.1%) allocated to triage category 3 or 4 (less severe and less urgent). During period 2, equivalent figures were 50 patients (2.7%) allocated to triage category 1 or 2, and 1817 patients (97.3%) allocated to triage category 3 or 4 (p=0.75). 340 patients (22.1%) underwent a skull x-ray in period 1 compared to none in period 2. Three hundred and twenty-eight (96.5%) of these x-rays during period 1 were normal. There were 12 (3.5%) x-rays which were abnormal. Three of these were suspicious of a skull fracture and these patients went on to have a normal CT scan (receiving a dose of radiation twice). Of the 9 that showed a definite skull fracture, 2 went on to have a CT scan. One CT scan showed an 8mm right frontal depressed skull fracture with a small underlying contusion, and one an isolated left parietal bone fracture with no intracranial injury. There were 2 other significant (i.e. patients with an abnormal brain CT) head injuries during period one (Table 3). Both of these injuries occurred in patients undergoing a CT scan as initial imaging modality. In total, 16 (1.0%) patients underwent a CT scan during period 1 resulting in 4 abnormal scans (25.0% positive CT rate). 3 scans showed intracranial injury, none of which required neurosurgical intervention. This compares to 39 patients (2.1%) undergoing CT scanning during period 2 (p=0.02). Of these 39 CT scans, 10 scans (25.6% of all period 2 CT scans) were abnormal. There were 7 patients with underlying intracranial injury (p=0.53), and 2 patients who Arch Dis Child: first published as /adc on 25 April Downloaded from on 19 August 2018 by guest. Protected by copyright. 4
5 required neurosurgical intervention (p=0.30) (Table 3). No patients received an ultrasound scan or a MRI scan in the acute setting during either period, and all patients survived to hospital discharge. 154 patients (10.1%) were admitted during period 1 compared to 203 (10.9%) patients during period 2 (p=0.43). Of those admitted during period 1, 5 patients (3.2%) went to the intensive care or high dependency unit and 149 patients (96.1%) went to the ward. During the second period, 13 patients (6.0%) went to the intensive care or high dependency unit and 190 patients (93.6%) went to the ward (p=0.23). The total radiation dose for period 1 was msv compared to a total dose of 78.0 msv for period 2. Radiation dose per head injury for period 1 was 0.045mSv compared to msv for period 2. Statistical analysis of this data is not possible due to the pattern of its spread. Figures 2a and 2b summarize the flow of patients through their investigations and management. There were no adverse sequelae in either group attributable to either policy decisions. For the second part of the study, the 39 patients who underwent a CT scan during period 2 were compared to 39 patients matched for age, triage category and sex who presented during period 2, and who did not undergo a CT scan (Table 4). Patients undergoing a CT scan had a higher proportion of falls from a height greater than 1 meter and road traffic accidents, and a lower proportion of falls less than 1 meter. They also had a higher proportion of all types of neurological symptoms. Patients undergoing CT were less likely to have a scalp laceration. However there was little difference with other injury type. The small number of patients in each category precludes further useful statistical analysis of this data. Finally, patients with a normal CT scan in the period were compared with those with an abnormal CT scan in the same period (Table 5). Of the 10 patients who had an abnormal CT scan, the commonest injury mechanisms were falling more than 1 meter (3 patients) and being involved in a road traffic accident (6 patients). Of the 29 patients having a normal CT scan, the commonest injury mechanisms were a fall of less than 1 meter (9 patients) and a direct blow to the head (8 patients). Drowsiness (6 patients) and loss of consciousness (5 patients) were the commonest symptoms in the 10 patients having an abnormal scan. All 8 patients undergoing CT because of persistent vomiting had a normal scan. Injuries found on examination were not predictive of an abnormal CT scan, and all patients who had an abnormal scan received their scan within 1 hour. Again, the small number of patients precludes further statistical analysis. Discussion The publication of guidelines by NICE and SIGN has signalled that a new approach to the management of head injury is needed. The publication by Lloyd et al has indicated that too many skull x-rays are being requested, with a significant unnecessary exposure to radiation by a large number of children [10]. Any change in policy however must ensure that clinical safety is not being compromised. We introduced a change in radiographic policy for head trauma after a careful examination of the literature, and ensured that child safety would be ensured by liberalising the option to admit, with a more liberal policy on CT request. The outcome from this change in policy is unique in that this is the first paper to evaluate such a policy. In addition it anticipates the approach suggested by NICE and provides a framework within which other departments might alter policy. Our results indicate that the abolition of skull x-rays in children aged 1 year and over prevented about 400 normal skull x-rays being performed in period 2 with no detriment to any child in terms of missed injury. The percentage of children undergoing CT rose from 1.0% to 2.1% with no change in the positive CT pick up rate (25.6% in period 2 compared to 25.0% in period 1). This compares favourably with figures from the American literature of 10% [9]. There was no significant change in admission rate (10.9% compared to 10.1%). However there was a slight nonsignificant increase in the percentage of patients being admitted to HDU and ITU (6.0% compared Arch Dis Child: first published as /adc on 25 April Downloaded from on 19 August 2018 by guest. Protected by copyright. 5
6 to 3.2%). This is due to the greater number of significant head injuries that occurred during the second period. There was a slight decrease in the radiation dose per head injury presentation (0.042mSv compared to msv). Whilst there was a reduction in the radiation dose, there were a few patients in period 2 who received a much higher dose of radiation (those who underwent a CT scan), and a huge number who received no radiation. This drop in radiation dose would probably have been much more impressive if it was not for the slight increase in injury severity seen during period 2. Comparison of the patients with a normal CT with those with an abnormal CT suggests that the mechanism of injury is an important predictor of head injury severity. An abnormal CT scan was more likely in a patient who had sustained a fall greater than 1 meter or who had been involved in a road traffic accident. Falls less than 1 meter and direct blows to the head were both more likely to be associated with a normal CT scan. The exception to this may be injury caused by a blow to the head with a golf club, a relatively common childhood leisure pursuit in Scotland compared to anywhere else. In our series there were no serious injuries from this mechanism. This has been shown in the past to be a risk factor for significant head injury [14]. Patients who had an abnormal scan were more likely to have had a history of loss of consciousness or drowsiness. No patients with a history of vomiting had an abnormal scan. This has been shown previously to be a poor diagnostic sign of significant head injury [15]. Neurological observations were a more reliable predictor of intracranial injury than documented superficial injuries. This may be due to a failure to document superficial injuries accurately when the patient has neurological signs that are an immediate indicator for a CT scan, and highlights a limitation of retrospective data collection. All patients who ended up having an abnormal brain CT were scanned immediately. This suggests that although it is well documented that intracranial injury can present some time after the initial injury, clinical suspicion is an extremely good predictor of head injury. This bears out the work of Sainsbury and Sibert [16]. They determined in a Welsh population that all significant head injuries in children declared themselves as such within 6 hours of injury. 10 out of 18 (55.6%) CT scans that were arranged within one hour of the patient attending the ED were positive. None of these immediate scans were in patients presenting late after sustaining their injury. Finally, 9 out of 14 (64%) patients undergoing CT scanning due to a reduced Glasgow Coma Score (GCS) had an abnormal scan, whilst all patients with a CT indication of vomiting or persistent headache had a normal scan. Conclusion This study demonstrates that skull x-rays can be successfully abandoned in those aged 1 to 14 without any significant increase in admission rate, radiation dose per head injury, or missed intracranial injury rate. We suggest that routine skull x-rays have no place in the paediatric ED for those children aged 1 year and over. Mechanism of head injury (falls >1 meter and road traffic accidents), a history of drowsiness or loss of consciousness, and a reduced Glasgow Coma Score are probably the most important indicators of serious head injury in children. Arch Dis Child: first published as /adc on 25 April Downloaded from on 19 August 2018 by guest. Protected by copyright. 6
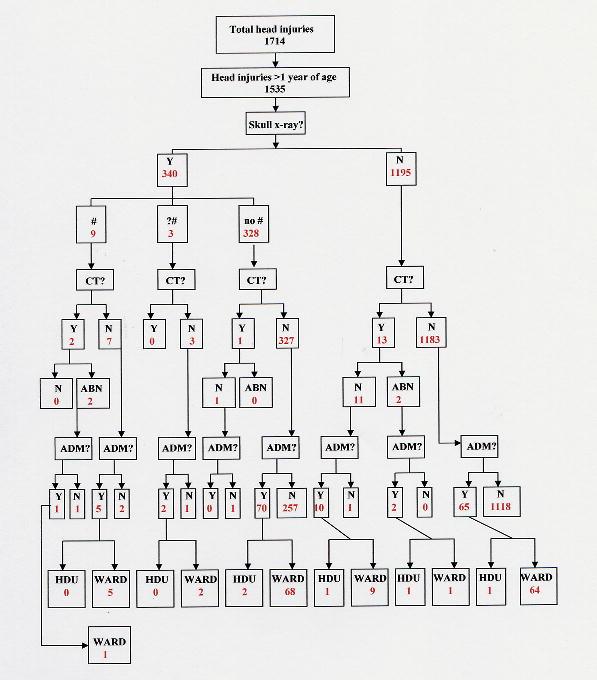
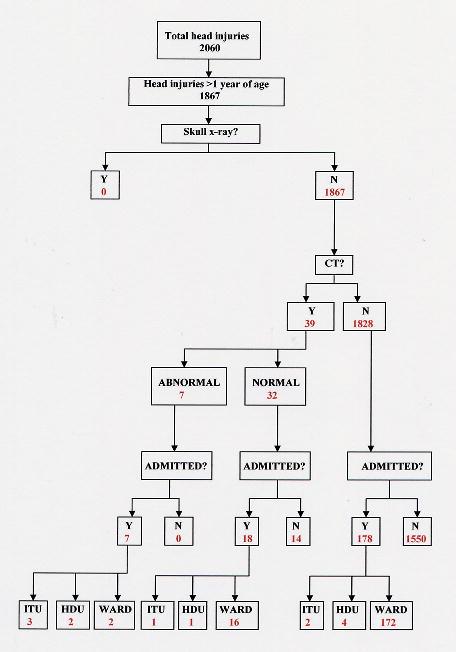
7 Table and Figure Legends Table 1 Table 2 Table 3 Table 4 Table and guidelines for radiological imaging in head injuries (RHSCE Emergency Department s head injury policy). Comparison between the two study periods, one before and one after the abolition of skull x-rays. Details of patients sustaining significant head injuries during both study periods. Comparison between 39 patients undergoing CT scanning in and 39 age, sex and triage category matched patients presenting during the same period. Comparison between patients having a normal CT scan and patients having an abnormal CT scan in Figure 1 Distribution of head injuries by age. Figure 2a Patient flow chart Figure 2b Patient flow chart Acknowledgements We thank Rik Smith at the Scottish Trauma Audit Group for statistical advice, and the radiographers in the x-ray department at RHSCE for help with retrieval of CT and x-ray data. Licence statement The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive licence (or non-exclusive for government employees) on a worldwide basis to the BMJ Publishing Group Ltd and its Licensees to permit this article to be published in ADC editions and any other BMJPGL products to exploit all subsidiary rights, as set out in our licence ( Arch Dis Child: first published as /adc on 25 April Downloaded from on 19 August 2018 by guest. Protected by copyright. 7
8 References 1 Royal College of Surgeons of England. Report of the working party on the management of patients with head injury. London: Royal College of Surgeons of England, Jennet B. Epidemiology of head injury. Archives of Disease in Childhood. May 1998; 78(5): Strang I, Macmillan R, Jennet B. Head injuries in accident and emergency departments in Scotland. Injury 1978; 10: Jennett B. Epidemiology of head injury. J Neurol Neurosurg Psychiatry 1996; 60: Jennett B, MacMillan R. Epidemiology of head injury. BMJ 1981; 282: Sharples PM, Storey A, Aynsley-Green A, et al. Avoidable factors contributing to death of children with head injury. BMJ 1990; 300: National Institute for Clinical Excellence (NICE) clinical guideline number 4. Head injury. Triage, assessment, investigation and early management of head injuries in infants, children and adults. June Scottish Intercollegiate Guidelines Network (SIGN) publication number 46. Early Management of Patients with Head Injury. August Palchak MJ, Holmes JF, Vance CW, et al. A decision rule for identifying children at low risk for brain injuries after blunt trauma. Ann Emerg Med. 2003; 42: Lloyd DA, Carty H. Predictive value of skull radiography for intracranial injury in children with blunt head injury. Lancet 1997; 349: Teasdale GM, Murray G, Anderson E, et al. Risks of acute traumatic intracranial haematoma in children and adults: implications for managing head injuries. BMJ 1990; 300: Mendelow AD, Teasdale G, Jennett B, et al. Risks of intracranial haematoma in head injured adults. BMJ 1983; 287: Wall BF, Hart D. Revised radiation doses for typical x-ray examinations. The British Journal of Radiology 1997, 70: Macgregor DM. Golf related head injuries in children. Emergency Medicine Journal Nov 2002; 19(6): 576-7, 15 Brown FD, Brown J, Beattie TF. Why do children vomit after minor head injury? Journal of Accident & Emergency Medicine Jul 2000; 17(4): Sainsbury CP, Sibert JR. How long do we need to observe head injuries in hospital? Archives of Disease in Childhood. Sep 1984; 59(9): Arch Dis Child: first published as /adc on 25 April Downloaded from on 19 August 2018 by guest. Protected by copyright. 8
9 Table Radiological guidelines Skull x-ray History of head injury in a child of any age. Admission for observation and/or CT Loss of consciousness more than 5 minutes. Amnesia. Persisting headache, vomiting or lethargy. Coagulation or bleeding diathesis (also needs discussion with haematology). Immediate CT head GCS less than 14. Focal neurological signs. Seizure (focal or prolonged). Signs of base of skull fracture.? Penetrating injury.? Depressed fracture Radiological guidelines Skull x-ray Age less than 1 year and visible evidence of head injury. Age less than 1 year and suspicious history for NAI. Admission for observation and/or CT Loss of consciousness more than 5 minutes. Amnesia. Persisting headache, vomiting or lethargy. Coagulation or bleeding diathesis (also needs discussion with haematology). Immediate CT head GCS less than 14. Focal neurological signs. Seizure (focal or prolonged). Signs of base of skull fracture.? Penetrating injury.? Depressed fracture. Arch Dis Child: first published as /adc on 25 April Downloaded from on 19 August 2018 by guest. Protected by copyright. 9
10 Table P= Head injuries >1 and <14 years Male : Female ratio 975 : : Median age (years) (IQR) 5.02 ( ) 4.87 ( ) Urgent triage (1 or 2) 44 (2.9%) 50 (2.7%) Delayed triage (3 or 4) 1491 (97.1%) 1817 (97.3%) Skull x-rays 340 (22.1%) 0 Number of 1-view x-rays 7 (2.1%) 0 Number of 2-view x-rays 233 (68.5%) 0 Number of 3-view x-rays 100 (29.4%) 0 Normal skull x-rays 328 (96.5%) 0 Abnormal skull x-rays 12 (3.5%) 0 SXR total radiation dose msv 0 msv CT scans 16 (1.0%) 39 (2.1%) Abnormal CT scans 4 (25.0%) 10 (25.6%) CT total radiation dose 32.0 msv 78.0 msv Discharged 1381 (89.9%) 1664 (89.1%) Admitted 154 (10.1%) 203 (10.9%) ITU / HDU 5 (3.2%) 13 (6.0%) Ward 149 (96.1%) 190 (93.6%) Total radiation dosage msv 78.0 msv Radiation dosage / head injury msv msv Intracranial injuries 3 (0.20%) 7 (0.37%) Neurosurgical intervention 0 (0%) 2 (0.10%) = Mann-Whitney U-test. 2= Fisher exact test. Arch Dis Child: first published as /adc on 25 April Downloaded from on 19 August 2018 by guest. Protected by copyright. 10
11 Table Patient 1: Extensive middle cranial fossa fractures with some small areas of contusion. Patient 2: Comminuted, depressed right parietal fracture with underlying contusion. Patient 3: 8mm right frontal depressed skull fracture with a small underlying contusion Patient 1: Right parietal fracture and extradural haematoma requiring craniotomy. Patient 2: Frontal fracture with associated subdural and extradural haematomas requiring craniotomy. Patient 3: Right parietal fracture with contusions. Patient 4: Right frontal fracture with contusions. Patient 5: Widespread cerebral contusions. Patient 6: Right frontal lobe subdural haematoma with contusions. Patient 7: Left parietal/occipital fracture with an underlying extradural haematoma. Arch Dis Child: first published as /adc on 25 April Downloaded from on 19 August 2018 by guest. Protected by copyright. 11
12 Table 4 CT scan group Matched non-ct scan group (n=39) (n=39) n % n % Mechanism unknown Fall > 1 meter Fall < 1 meter Fall down stairs Road traffic accident Direct blow to head Loss of consciousness Seizure Vomiting Drowsiness ?NAI Amnesia Headache No abnormality Facial haematoma Facial laceration Scalp haematoma Scalp laceration Arch Dis Child: first published as /adc on 25 April Downloaded from on 19 August 2018 by guest. Protected by copyright. 12
13 Normal CT scan (n=29) Table 5 Abnormal CT scan (n=10) Positive Predictive Value Negative Predictive Value n % n % % % Mechanism unknown Fall > 1 meter Fall < 1 meter Fall down stairs Road traffic accident Direct blow to head Loss of consciousness Seizure Vomiting Drowsiness ?NAI Amnesia Headache No abnormality Facial haematoma Facial laceration Scalp haematoma Scalp laceration Within 1 hour hours Same day Next day Same week Next week Prior to GA Vomiting Confusion Persistent headache Boggy haematoma Reduced GCS Seizure Amnesia Worrying mechanism Collapse Irritability Drowsiness Dizziness ?Base of skull # Unknown Arch Dis Child: first published as /adc on 25 April Downloaded from on 19 August 2018 by guest. Protected by copyright. 13
14
15
16
O ne million patients are treated annually in United
 859 ORIGIAL ARTICLE Can we abolish skull x rays for head injury? M J Reed, J G Browning, A G Wilkinson, T Beattie... See end of article for authors affiliations... Correspondence to: Matthew J Reed, Accident
859 ORIGIAL ARTICLE Can we abolish skull x rays for head injury? M J Reed, J G Browning, A G Wilkinson, T Beattie... See end of article for authors affiliations... Correspondence to: Matthew J Reed, Accident
recommendations of the Royal College of
 Archives of Emergency Medicine, 1993, 10, 138-144 Skull X-ray after head injury: the recommendations of the Royal College of Surgeons Working Party Report in practice R. E. MACLAREN, H. I. GHOORAHOO &
Archives of Emergency Medicine, 1993, 10, 138-144 Skull X-ray after head injury: the recommendations of the Royal College of Surgeons Working Party Report in practice R. E. MACLAREN, H. I. GHOORAHOO &
A bout million patients present to UK hospitals
 420 ORIGINAL ARTICLE Application of the Canadian CT head rules in managing minor head injuries in a UK emergency department: implications for the implementation of the NICE guidelines H Y Sultan, A Boyle,
420 ORIGINAL ARTICLE Application of the Canadian CT head rules in managing minor head injuries in a UK emergency department: implications for the implementation of the NICE guidelines H Y Sultan, A Boyle,
Use of CT in minor traumatic brain injury. Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD
 Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
The significance of traumatic haematoma in the
 Journal of Neurology, Neurosurgery, and Psychiatry 1986;49:29-34 The significance of traumatic haematoma in the region of the basal ganglia P MACPHERSON, E TEASDALE, S DHAKER, G ALLERDYCE, S GALBRAITH
Journal of Neurology, Neurosurgery, and Psychiatry 1986;49:29-34 The significance of traumatic haematoma in the region of the basal ganglia P MACPHERSON, E TEASDALE, S DHAKER, G ALLERDYCE, S GALBRAITH
Why do accident and emergency doctors
 Archives of Emergency Medicine, 1984, 3, 143-150 Why do accident and emergency doctors request X-rays? R. A. WARREN AND D. G. FERGUSON Department of Accident and Emergency Medicine, Royal Hallamshire Hospital,
Archives of Emergency Medicine, 1984, 3, 143-150 Why do accident and emergency doctors request X-rays? R. A. WARREN AND D. G. FERGUSON Department of Accident and Emergency Medicine, Royal Hallamshire Hospital,
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Predicting the need for operation in the patient with an occult traumatic intracranial hematoma
 J Neurosurg 55:75-81, 1981 Predicting the need for operation in the patient with an occult traumatic intracranial hematoma SAM GALBRAITH, M.D., F.R.C.S., AND GRAHAM TEASDALE, M.R.C.P., F.R.C.S. Department
J Neurosurg 55:75-81, 1981 Predicting the need for operation in the patient with an occult traumatic intracranial hematoma SAM GALBRAITH, M.D., F.R.C.S., AND GRAHAM TEASDALE, M.R.C.P., F.R.C.S. Department
Hit head, on blood thinner-wife wants CT. Will Davies June 2014
 Hit head, on blood thinner-wife wants CT Will Davies June 2014 Selection of Adults with Head Injury for CT Scan Early management of head injury: summary of updated NICE guidance. Hodgkinson S, Pollit V,
Hit head, on blood thinner-wife wants CT Will Davies June 2014 Selection of Adults with Head Injury for CT Scan Early management of head injury: summary of updated NICE guidance. Hodgkinson S, Pollit V,
Referral Criteria for Medical CT Radiation Exposures. Neuro Referrals
 Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY
 Measure #416: Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 2 through 17 Years - National Quality Strategy Domain: Efficiency and Cost Reduction
Measure #416: Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 2 through 17 Years - National Quality Strategy Domain: Efficiency and Cost Reduction
Analysis of pediatric head injury from falls
 Neurosurg Focus 8 (1):Article 3, 2000 Analysis of pediatric head injury from falls K. ANTHONY KIM, MICHAEL Y. WANG, M.D., PAMELA M. GRIFFITH, R.N.C., SUSAN SUMMERS, R.N., AND MICHAEL L. LEVY, M.D. Division
Neurosurg Focus 8 (1):Article 3, 2000 Analysis of pediatric head injury from falls K. ANTHONY KIM, MICHAEL Y. WANG, M.D., PAMELA M. GRIFFITH, R.N.C., SUSAN SUMMERS, R.N., AND MICHAEL L. LEVY, M.D. Division
Derivation of the children s head injury algorithm for the prediction of important clinical events decision rule for head injury in children
 885 ORIGINAL ARTICLE Derivation of the children s head injury algorithm for the prediction of important clinical events decision rule for head injury in children J Dunning, J Patrick Daly, J-P Lomas, F
885 ORIGINAL ARTICLE Derivation of the children s head injury algorithm for the prediction of important clinical events decision rule for head injury in children J Dunning, J Patrick Daly, J-P Lomas, F
Pediatric head trauma: the evidence regarding indications for emergent neuroimaging
 DOI 10.1007/s00247-008-0996-5 ALARA: BUILDING BRIDGES BETWEEN RADIOLOGY AND EMERGENCY MEDICINE Pediatric head trauma: the evidence regarding indications for emergent neuroimaging Nathan Kuppermann Received:
DOI 10.1007/s00247-008-0996-5 ALARA: BUILDING BRIDGES BETWEEN RADIOLOGY AND EMERGENCY MEDICINE Pediatric head trauma: the evidence regarding indications for emergent neuroimaging Nathan Kuppermann Received:
2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Efficiency
 Measure #416: Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 2 Through 17 Years - National Quality Strategy Domain: Efficiency and Cost Reduction
Measure #416: Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 2 Through 17 Years - National Quality Strategy Domain: Efficiency and Cost Reduction
Head injuries in children. Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead
 Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
The management of minor traumatic brain injury
 8 8 Accid Emerg Med 1998;15:8-88 REVIEW University Department of Neurosurgery, Addenbrooke's Hospital, Cambridge, UK P J A Hutchinson P J Kirkpatrick J Addison S Jackson J D Pickard Correspondence to:
8 8 Accid Emerg Med 1998;15:8-88 REVIEW University Department of Neurosurgery, Addenbrooke's Hospital, Cambridge, UK P J A Hutchinson P J Kirkpatrick J Addison S Jackson J D Pickard Correspondence to:
Correlation of Computed Tomography findings with Glassgow Coma Scale in patients with acute traumatic brain injury
 Journal of College of Medical Sciences-Nepal, 2014, Vol-10, No-2 ABSTRACT OBJECTIVE To correlate Computed Tomography (CT) findings with Glasgow Coma Scale (GCS) in patients with acute traumatic brain injury
Journal of College of Medical Sciences-Nepal, 2014, Vol-10, No-2 ABSTRACT OBJECTIVE To correlate Computed Tomography (CT) findings with Glasgow Coma Scale (GCS) in patients with acute traumatic brain injury
Audit Report. National Audit of Paediatric Radiology Services in Hospitals
 Audit Report National Audit of Paediatric Radiology Services in Hospitals www.rcr.ac.uk 2 Contents Introduction 3 Standards 4 Material and methods 5 Results 6 Discussion 8 References 10 www.rcr.ac.uk 3
Audit Report National Audit of Paediatric Radiology Services in Hospitals www.rcr.ac.uk 2 Contents Introduction 3 Standards 4 Material and methods 5 Results 6 Discussion 8 References 10 www.rcr.ac.uk 3
Head trauma is a common chief complaint among children visiting
 Discussions in Surgery Validation of the Sainte-Justine Head Trauma Pathway for children younger than two years of age Sarah Spénard Serge Gouin, MDCM Marianne Beaudin, MD Jocelyn Gravel, MD, MSc Partial
Discussions in Surgery Validation of the Sainte-Justine Head Trauma Pathway for children younger than two years of age Sarah Spénard Serge Gouin, MDCM Marianne Beaudin, MD Jocelyn Gravel, MD, MSc Partial
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
Disclosure Statement. Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk.
 Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Head injury in children
 Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
:: Closed Head Injury in Adults
 ADULT TRAUMA CLINICAL PRACTICE GUIDELINES Initial Management of :: Closed Head Injury in Adults Suggested citation: Dr Duncan Reed 2007, Adult Trauma Clinical Practice Guidelines, Initial Management of
ADULT TRAUMA CLINICAL PRACTICE GUIDELINES Initial Management of :: Closed Head Injury in Adults Suggested citation: Dr Duncan Reed 2007, Adult Trauma Clinical Practice Guidelines, Initial Management of
Epilepsy after two different neurosurgical approaches
 Journal ofneurology, Neurosurgery, and Psychiatry, 1976, 39, 1052-1056 Epilepsy after two different neurosurgical approaches to the treatment of ruptured intracranial aneurysm R. J. CABRAL, T. T. KING,
Journal ofneurology, Neurosurgery, and Psychiatry, 1976, 39, 1052-1056 Epilepsy after two different neurosurgical approaches to the treatment of ruptured intracranial aneurysm R. J. CABRAL, T. T. KING,
AGE RELATED PATTERN AND OUTCOME OF HEAD INJURY IN INDIGENOUS AFRICA
 Nigerian Journal of Clinical Practice Sept. 2008 Vol 11(3):265-269 AGE RELATED PATTERN AND OUTCOME OF HEAD INJURY IN INDIGENOUS AFRICA TO Department of Surgery, University of Ilorin Teaching Hospital,
Nigerian Journal of Clinical Practice Sept. 2008 Vol 11(3):265-269 AGE RELATED PATTERN AND OUTCOME OF HEAD INJURY IN INDIGENOUS AFRICA TO Department of Surgery, University of Ilorin Teaching Hospital,
The risk of a bleed after delayed head injury presentation to the ED: systematic review protocol. Correspondence to:
 The risk of a bleed after delayed head injury presentation to the ED: systematic review protocol. Carl Marincowitz, Christopher M. Smith, William Townend Emergency Department, Hull Royal, Hull, UK Correspondence
The risk of a bleed after delayed head injury presentation to the ED: systematic review protocol. Carl Marincowitz, Christopher M. Smith, William Townend Emergency Department, Hull Royal, Hull, UK Correspondence
Factors associated with Outcome in Patients Admitted with Traumatic Brain Injury at the University Teaching Hospital, Lusaka, Zambia
 ORIGINAL ARTICLE Factors associated with Outcome in Patients Admitted with Traumatic Brain Injury at the University Teaching Hospital, Lusaka, Zambia K. Mwala, J.C Munthali, L. Chikoya Department of Surgery,
ORIGINAL ARTICLE Factors associated with Outcome in Patients Admitted with Traumatic Brain Injury at the University Teaching Hospital, Lusaka, Zambia K. Mwala, J.C Munthali, L. Chikoya Department of Surgery,
DIAGNOSTIC PROCEDURES IN MILD TRAUMATIC BRAIN INJURY: RESULTS OF THE WHO COLLABORATING CENTRE TASK FORCE ON MILD TRAUMATIC BRAIN INJURY
 J Rehabil Med 2004; Suppl. 43: 61 75 DIAGNOSTIC PROCEDURES IN MILD TRAUMATIC BRAIN INJURY: RESULTS OF THE WHO COLLABORATING CENTRE TASK FORCE ON MILD TRAUMATIC BRAIN INJURY Jörgen Borg, 1 Lena Holm, 2
J Rehabil Med 2004; Suppl. 43: 61 75 DIAGNOSTIC PROCEDURES IN MILD TRAUMATIC BRAIN INJURY: RESULTS OF THE WHO COLLABORATING CENTRE TASK FORCE ON MILD TRAUMATIC BRAIN INJURY Jörgen Borg, 1 Lena Holm, 2
UHSM ED Pathway ELDERLY FALL / COLLAPSE
 UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
Original Article. Emergency Department Evaluation of Ventricular Shunt Malfunction. Is the Shunt Series Really Necessary? Raymond Pitetti, MD, MPH
 Original Article Emergency Department Evaluation of Ventricular Shunt Malfunction Is the Shunt Series Really Necessary? Raymond Pitetti, MD, MPH Objective: The malfunction of a ventricular shunt is one
Original Article Emergency Department Evaluation of Ventricular Shunt Malfunction Is the Shunt Series Really Necessary? Raymond Pitetti, MD, MPH Objective: The malfunction of a ventricular shunt is one
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article A Study of Paediatric Head Injuries and Its Outcome Raje Vinayak, Raje Vaishali, Pednekar Akshay,
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article A Study of Paediatric Head Injuries and Its Outcome Raje Vinayak, Raje Vaishali, Pednekar Akshay,
The AHEAD Study: Managing anticoagulatedpatients who suffer head injury
 AHEAD Study The AHEAD Study: Managing anticoagulatedpatients who suffer head injury Suzanne Mason 1,2, Maxine Kuczawski 1, Matthew Stevenson 1, Dawn Teare 1, Michael Holmes 1, ShammiRamlakhan 1, Steve
AHEAD Study The AHEAD Study: Managing anticoagulatedpatients who suffer head injury Suzanne Mason 1,2, Maxine Kuczawski 1, Matthew Stevenson 1, Dawn Teare 1, Michael Holmes 1, ShammiRamlakhan 1, Steve
SKULL RADIOGRAPH IN HEAD INJURIES. Authors: ** Njeze, Ngozi R Umerah, B.C Mgbor, S.O
 SKULL RADIOGRAPH IN HEAD INJURIES Authors: ** Njeze, Ngozi R Umerah, B.C Mgbor, S.O **Address: Department of Radiation Medicine University of Nigeria Teaching Hospital, Enugu, Nigeria. E-mail: ngozinjeze
SKULL RADIOGRAPH IN HEAD INJURIES Authors: ** Njeze, Ngozi R Umerah, B.C Mgbor, S.O **Address: Department of Radiation Medicine University of Nigeria Teaching Hospital, Enugu, Nigeria. E-mail: ngozinjeze
The New England Journal of Medicine A POPULATION-BASED STUDY OF SEIZURES AFTER TRAUMATIC BRAIN INJURIES
 A POPULATION-BASED STUDY OF SEIZURES AFTER TRAUMATIC BRAIN INJURIES JOHN F. ANNEGERS, PH.D., W. ALLEN HAUSER, M.D., SHARON P. COAN, M.S., AND WALTER A. ROCCA, M.D., M.P.H. ABSTRACT Background The risk
A POPULATION-BASED STUDY OF SEIZURES AFTER TRAUMATIC BRAIN INJURIES JOHN F. ANNEGERS, PH.D., W. ALLEN HAUSER, M.D., SHARON P. COAN, M.S., AND WALTER A. ROCCA, M.D., M.P.H. ABSTRACT Background The risk
SUDANESE JOURNAL OF PAEDIATRICS 2014; Vol 14, Issue No. 1
 Education and Practice Case Report and Literature Review Managing traumatic brain injury in children: When do we need a computed tomography of the head? Mohammed A Kambal (1), Manal E Abou (2), Iman Al
Education and Practice Case Report and Literature Review Managing traumatic brain injury in children: When do we need a computed tomography of the head? Mohammed A Kambal (1), Manal E Abou (2), Iman Al
Pediatric Surgery MODE, PRESENTATION, CT FINDINGS AND OUTCOME OF PEDIATRIC HEAD INJURY
 Pediatric Surgery MODE, PRESENTATION, CT FINDINGS AND OUTCOME OF PEDIATRIC HEAD INJURY M. Sharma A.K. Sharma ABSTRACT Twenty five to thirty per cent of all patients admitted with head injuries to any large
Pediatric Surgery MODE, PRESENTATION, CT FINDINGS AND OUTCOME OF PEDIATRIC HEAD INJURY M. Sharma A.K. Sharma ABSTRACT Twenty five to thirty per cent of all patients admitted with head injuries to any large
Extradural hematoma (EDH) accounts for 2% of all head injuries (1). In
 accounts for 2% of all head injuries (1). In") CASE REPORT Conservative management of extradural hematoma: A report of sixty-two cases A. Rahim H. Zwayed 1, Brandon Lucke-Wold 2 Zwayed ARH, Lucke-wold B. Conservative management of extradural hematoma:
CASE REPORT Conservative management of extradural hematoma: A report of sixty-two cases A. Rahim H. Zwayed 1, Brandon Lucke-Wold 2 Zwayed ARH, Lucke-wold B. Conservative management of extradural hematoma:
Correspondence should be addressed to Sorayouth Chumnanvej;
 Neurology Research International Volume 2016, Article ID 2737028, 7 pages http://dx.doi.org/10.1155/2016/2737028 Research Article Assessment and Predicting Factors of Repeated Brain Computed Tomography
Neurology Research International Volume 2016, Article ID 2737028, 7 pages http://dx.doi.org/10.1155/2016/2737028 Research Article Assessment and Predicting Factors of Repeated Brain Computed Tomography
PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES
 PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES INTRODUCTION: Traumatic Brain Injury (TBI) is an important clinical entity in acute care surgery without well-defined guidelines
PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES INTRODUCTION: Traumatic Brain Injury (TBI) is an important clinical entity in acute care surgery without well-defined guidelines
Author Manuscript. Received Date : 27-Oct Revised Date : 09-Jan-2017 Accepted Date : 31-Jan-2017
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 Received Date : 27-Oct-2016 Revised Date : 09-Jan-2017 Accepted Date : 31-Jan-2017 Article type ABSTRACT : Original Contribution
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 Received Date : 27-Oct-2016 Revised Date : 09-Jan-2017 Accepted Date : 31-Jan-2017 Article type ABSTRACT : Original Contribution
Surgical management of diastatic linear skull fractures in infants
 Surgical management of diastatic linear skull fractures in infants JOHN B. THOMPSON, M.D., THOMAS H. MASON, M.D., GERALD L. HAINES, M.D., AND ROBERT J. CASSIDY, M.D. Divisions of Neurosurgery and Neurology,
Surgical management of diastatic linear skull fractures in infants JOHN B. THOMPSON, M.D., THOMAS H. MASON, M.D., GERALD L. HAINES, M.D., AND ROBERT J. CASSIDY, M.D. Divisions of Neurosurgery and Neurology,
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
Supplementary Table 1. ICD-9/-10 codes used to identify cycling injury hospitalizations. Railway accidents injured pedal cyclist
 Supplementary Table 1. ICD-9/-10 codes used to identify cycling injury hospitalizations. ICD Code ICD-9 E800-E807(.3) E810-E816, E818-E819(.6) E820-E825(.6) E826-E829(.1) ICD-10-CA V10-V19 (including all
Supplementary Table 1. ICD-9/-10 codes used to identify cycling injury hospitalizations. ICD Code ICD-9 E800-E807(.3) E810-E816, E818-E819(.6) E820-E825(.6) E826-E829(.1) ICD-10-CA V10-V19 (including all
Overview of Abusive Head Trauma: What Everyone Needs to Know. 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012
 Overview of Abusive Head Trauma: What Everyone Needs to Know 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012 Deborah Lowen, MD Associate Professor Pediatrics Director, Child Abuse
Overview of Abusive Head Trauma: What Everyone Needs to Know 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012 Deborah Lowen, MD Associate Professor Pediatrics Director, Child Abuse
Kristin s Head Trauma Board Questions 11/07/14
 Kristin s Head Trauma Board Questions { 11/07/14 A healthy 15 y/o boy was playing football at a park near his home with a group of friends when he tripped over a friend s leg while trying to catch a pass.
Kristin s Head Trauma Board Questions { 11/07/14 A healthy 15 y/o boy was playing football at a park near his home with a group of friends when he tripped over a friend s leg while trying to catch a pass.
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Evaluation of Craniocerebral Trauma Using Computed Tomography
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 9 Ver. IV (Sep. 2014), PP 57-62 Evaluation of Craniocerebral Trauma Using Computed Tomography
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 9 Ver. IV (Sep. 2014), PP 57-62 Evaluation of Craniocerebral Trauma Using Computed Tomography
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Reviewing the recent literature to answer clinical questions: Should I change my practice?
 Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Initial Management of Closed Head Injury in Adults
 ADULT TRAUMA CLINICAL PRACTICE GUIDELINES Initial Management of Closed Head Injury in Adults Summary Document 2nd Edition NSW Ministry of Health 73 Miller St NORTH SYDNEY NSW 2060 Tel (02) 9391 9000 Fax
ADULT TRAUMA CLINICAL PRACTICE GUIDELINES Initial Management of Closed Head Injury in Adults Summary Document 2nd Edition NSW Ministry of Health 73 Miller St NORTH SYDNEY NSW 2060 Tel (02) 9391 9000 Fax
PEDIATRIC MILD TRAUMATIC HEAD INJURY
 PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Diagnostic Testing for Acute Head Injury in Children: When Are Head Computed Tomography and Skull Radiographs Indicated?
 Diagnostic Testing for Acute Head Injury in Children: When Are Head Computed Tomography and Skull Radiographs Indicated? Kimberly S. Quayle, MD*; David M. Jaffe, MD*; Nathan Kuppermann, MD, MPH ; Bruce
Diagnostic Testing for Acute Head Injury in Children: When Are Head Computed Tomography and Skull Radiographs Indicated? Kimberly S. Quayle, MD*; David M. Jaffe, MD*; Nathan Kuppermann, MD, MPH ; Bruce
USE OF CT SCAN IN A CHILD WITH MTBI
 TO SCAN OR NOT TO SCAN USE OF CT SCAN IN A CHILD WITH MTBI LISA AYOUB-RODRIGUEZ MD PEDIATRIC HOSPITALIST MIKE LEE MD PEDIATRIC RESIDENT BERT JOHANSSON MD PEDIATRIC HOSPITALIST DISCLOSURES I M NOT A SURGEON
TO SCAN OR NOT TO SCAN USE OF CT SCAN IN A CHILD WITH MTBI LISA AYOUB-RODRIGUEZ MD PEDIATRIC HOSPITALIST MIKE LEE MD PEDIATRIC RESIDENT BERT JOHANSSON MD PEDIATRIC HOSPITALIST DISCLOSURES I M NOT A SURGEON
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Instructional Course #34. Review of Neuropharmacology in Pediatric Brain Injury. John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD
 Instructional Course #34 Review of Neuropharmacology in Pediatric Brain Injury John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD Outline of Course 1. Introduction John Pelegano MD 2. Neuropharmocologic
Instructional Course #34 Review of Neuropharmacology in Pediatric Brain Injury John Pelegano MD Jilda Vargus-Adams MD, MSc Micah Baird MD Outline of Course 1. Introduction John Pelegano MD 2. Neuropharmocologic
Outcome Evaluation of Chronic Subdural Hematoma Using Glasgow Outcome Score
 Outcome Evaluation of Chronic Subdural Hematoma Using Glasgow Outcome Score Mehdi Abouzari, Marjan Asadollahi, Hamideh Aleali Amir-Alam Hospital, Medical Sciences/University of Tehran, Tehran, Iran Introduction
Outcome Evaluation of Chronic Subdural Hematoma Using Glasgow Outcome Score Mehdi Abouzari, Marjan Asadollahi, Hamideh Aleali Amir-Alam Hospital, Medical Sciences/University of Tehran, Tehran, Iran Introduction
Lothian Audit of the Treatment of Cerebral Haemorrhage (LATCH)
") 1. INTRODUCTION Stroke physicians, emergency department doctors, and neurologists are often unsure about which patients they should refer for neurosurgical intervention. Early neurosurgical evacuation
1. INTRODUCTION Stroke physicians, emergency department doctors, and neurologists are often unsure about which patients they should refer for neurosurgical intervention. Early neurosurgical evacuation
Neurological examination of the neurosurgical patient. Dániel Bereczki SU Department of Neurology
 Neurological examination of the neurosurgical patient Dániel Bereczki SU Department of Neurology E-learning Indivudual study Interactive learning Self assessment at the end of chapters E-learning Indivudual
Neurological examination of the neurosurgical patient Dániel Bereczki SU Department of Neurology E-learning Indivudual study Interactive learning Self assessment at the end of chapters E-learning Indivudual
USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG)
") USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG) Note: The intent of this CPG is to serve as general guidance for medics and medical officers. It
USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG) Note: The intent of this CPG is to serve as general guidance for medics and medical officers. It
GUIDELINES FOR THE MANAGEMENT OF HEAD INJURIES IN REMOTE AND RURAL ALASKA
 GUIDELINES FOR THE MANAGEMENT OF HEAD INJURIES IN REMOTE AND RURAL ALASKA Approximately 800 patients with head injuries die or are hospitalized in the state of Alaska each year 1. In addition, thousands
GUIDELINES FOR THE MANAGEMENT OF HEAD INJURIES IN REMOTE AND RURAL ALASKA Approximately 800 patients with head injuries die or are hospitalized in the state of Alaska each year 1. In addition, thousands
A Comprehensive Study on Post Traumatic Temporal Contusion in Adults
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/318 A Comprehensive Study on Post Traumatic Temporal Contusion in Adults R Renganathan 1, P John Paul 2, Heber Anandan
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/318 A Comprehensive Study on Post Traumatic Temporal Contusion in Adults R Renganathan 1, P John Paul 2, Heber Anandan
A protocol for the development of a prediction model in mild traumatic brain injury with CT scan abnormality: which patients are safe for discharge?
 Marincowitz et al. Diagnostic and Prognostic Research (2018) 2:6 https://doi.org/10.1186/s41512-018-0027-4 Diagnostic and Prognostic Research PROTOCOL A protocol for the development of a prediction model
Marincowitz et al. Diagnostic and Prognostic Research (2018) 2:6 https://doi.org/10.1186/s41512-018-0027-4 Diagnostic and Prognostic Research PROTOCOL A protocol for the development of a prediction model
Head Injury Management Guidelines For St Mary s Major Trauma Centre
 Head Injury Management Guidelines For St Mary s Major Trauma Centre Table of Contents Introduction... 2 Referral Process, Admission and Resuscitation... 2 The Trauma Tree Pathway:... 2 Neurosurgery Registrar
Head Injury Management Guidelines For St Mary s Major Trauma Centre Table of Contents Introduction... 2 Referral Process, Admission and Resuscitation... 2 The Trauma Tree Pathway:... 2 Neurosurgery Registrar
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
Risk Factors Predicting Mortality in Spinal Cord Injury in Nigeria
 Article ID: WMC00807 ISSN 2046690 Risk Factors Predicting Mortality in Spinal Cord Injury in Nigeria Corresponding Author: Dr. Ahidjo Kawu, Consultant Surgeon, Dept of Orthopaedics, UATH, Gwagwalada Abuja
Article ID: WMC00807 ISSN 2046690 Risk Factors Predicting Mortality in Spinal Cord Injury in Nigeria Corresponding Author: Dr. Ahidjo Kawu, Consultant Surgeon, Dept of Orthopaedics, UATH, Gwagwalada Abuja
Severe Head Injury in an Army Pilot
 Severe Head Injury in an Army Pilot Royal Aeronautical Society Aerospace Medicine Symposium Lt Col C Goldie RAMC 12 Dec 17 Joint Helicopter Command Scope Case History Literature review Aeromedical policy
Severe Head Injury in an Army Pilot Royal Aeronautical Society Aerospace Medicine Symposium Lt Col C Goldie RAMC 12 Dec 17 Joint Helicopter Command Scope Case History Literature review Aeromedical policy
School of Hard Knocks! Richard Beebe MS RN NRP MedicThink LLC
 School of Hard Knocks! Richard Beebe MS RN NRP MedicThink LLC Fall of a Teton How Bad is He Hurt? What REALLY happened inside Johnny s head? How common are these types of injuries? PONDER THIS What part
School of Hard Knocks! Richard Beebe MS RN NRP MedicThink LLC Fall of a Teton How Bad is He Hurt? What REALLY happened inside Johnny s head? How common are these types of injuries? PONDER THIS What part
Imaging Biomarkers Significance S100B NSE. Admitted within 6 hours of injury and CT scan occurred after initial examination. N = 1,064 CT+ N = 50 4.
 Concussion Guidelines Step 1: Systematic Review of Prevalent Indicators Supplemental Content 7 Evidence Table. Included Studies For Key Question 4 Imaging and Biomarker Publications Medium Potential for
Concussion Guidelines Step 1: Systematic Review of Prevalent Indicators Supplemental Content 7 Evidence Table. Included Studies For Key Question 4 Imaging and Biomarker Publications Medium Potential for
Andrzej Żyluk 1, Agnieszka Mazur 1, Bernard Piotuch 1, Krzysztof Safranow 2
 POLSKI PRZEGLĄD CHIRURGICZNY 2013, 85, 12, 699 705 10.2478/pjs-2013-0107 Analysis of the reliability of clinical examination in predicting traumatic cerebral lesions and skull fractures in patients with
POLSKI PRZEGLĄD CHIRURGICZNY 2013, 85, 12, 699 705 10.2478/pjs-2013-0107 Analysis of the reliability of clinical examination in predicting traumatic cerebral lesions and skull fractures in patients with
Sports/activities and ALD
 Sports/activities and ALD Gerald Raymond, MD Penn State Children s Hospital 15:00 Dr Gerald Raymond- Sports and ALD 1 Can Head Injury Influence the site of Demyelination in Adrenoleukodystrophy? Wilkinson
Sports/activities and ALD Gerald Raymond, MD Penn State Children s Hospital 15:00 Dr Gerald Raymond- Sports and ALD 1 Can Head Injury Influence the site of Demyelination in Adrenoleukodystrophy? Wilkinson
3/14/2014 USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION THE PROBLEM OLD THINKING
 USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION Immobilization following injury used to be a simple decision--but no one was thinking. Up to 5 million people per year receive
USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION Immobilization following injury used to be a simple decision--but no one was thinking. Up to 5 million people per year receive
Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/300 Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm Raja S Vignesh
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/300 Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm Raja S Vignesh
Chest pain in the accident and emergency department: is chest radiography worthwhile?
 Archives of Emergency Medicine, 1991, 8, 97-101 Chest pain in the accident and emergency department: is chest radiography worthwhile? worthwhile? P. A. TEMPLETON, W. A. McCALLION, L. A. McKINNEY, H. K.
Archives of Emergency Medicine, 1991, 8, 97-101 Chest pain in the accident and emergency department: is chest radiography worthwhile? worthwhile? P. A. TEMPLETON, W. A. McCALLION, L. A. McKINNEY, H. K.
Intraoperative contralateral extradural hematoma during evacuation of traumatic acute extradural hematoma: A case report with review of literature
 Intraoperative contralateral extradural hematoma during evacuation of traumatic acute extradural hematoma: A case report with review of literature Anand Sharma 1, Arti Sharma 2, Yashbir Dewan 1 1 Artemis
Intraoperative contralateral extradural hematoma during evacuation of traumatic acute extradural hematoma: A case report with review of literature Anand Sharma 1, Arti Sharma 2, Yashbir Dewan 1 1 Artemis
The Nottingham Head Injury Register: a survey of 1,276 adult cases of moderate and severe traumatic brain injury in a British neurosurgery centre
 The Intensive Care Society 2011 Audits and surveys The Nottingham Head Injury Register: a survey of 1,276 adult cases of moderate and severe traumatic brain injury in a British neurosurgery centre G Fuller,
The Intensive Care Society 2011 Audits and surveys The Nottingham Head Injury Register: a survey of 1,276 adult cases of moderate and severe traumatic brain injury in a British neurosurgery centre G Fuller,
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8:
 Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Correlation of D-Dimer level with outcome in traumatic brain injury
 2014; 17 (1) Original Article Correlation of D-Dimer level with outcome in traumatic brain injury Pradip Prasad Subedi 1, Sushil Krishna Shilpakar 2 Email: Abstract Introduction immense. The major determinant
2014; 17 (1) Original Article Correlation of D-Dimer level with outcome in traumatic brain injury Pradip Prasad Subedi 1, Sushil Krishna Shilpakar 2 Email: Abstract Introduction immense. The major determinant
Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision
 Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision Support Using the Canadian CT Head Rule to Reduce Unnecessary
Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision Support Using the Canadian CT Head Rule to Reduce Unnecessary
Research Article Analysis of Repeated CT Scan Need in Blunt Head Trauma
 Hindawi Publishing Corporation Emergency Medicine International Volume 2013, Article ID 916253, 5 pages http://dx.doi.org/10.1155/2013/916253 Research Article Analysis of Repeated CT Scan Need in Blunt
Hindawi Publishing Corporation Emergency Medicine International Volume 2013, Article ID 916253, 5 pages http://dx.doi.org/10.1155/2013/916253 Research Article Analysis of Repeated CT Scan Need in Blunt
Risk factors predicting operable intracranial hematomas in head injury
 J Neurosarg 77:9-14, 1992 Risk factors predicting operable intracranial hematomas in head injury MICHAEL B. GUTMAN, M.D., PH.D., RICHARD J. MOULTON, M.D., F.R.C.S.(C), IRENE SULLIVAN, B.A., Dw.C.S., GILLIAN
J Neurosarg 77:9-14, 1992 Risk factors predicting operable intracranial hematomas in head injury MICHAEL B. GUTMAN, M.D., PH.D., RICHARD J. MOULTON, M.D., F.R.C.S.(C), IRENE SULLIVAN, B.A., Dw.C.S., GILLIAN
Intravenous drug abusers attending an inner city accident and emergency department
 Archives of Emergency Medicine, 99, 9, -9 Intravenous drug abusers attending an inner city accident and emergency department R. M. MAKOWER, A. G. PENNYCOOK & C. MOULTON Registrars in Accident and Emergency
Archives of Emergency Medicine, 99, 9, -9 Intravenous drug abusers attending an inner city accident and emergency department R. M. MAKOWER, A. G. PENNYCOOK & C. MOULTON Registrars in Accident and Emergency
England & Wales 2 YEARS OF SEVERE INJURY IN CHILDREN
 England & Wales 2 YEARS OF SEVERE INJURY IN CHILDREN January 2013-December 2014 THE TRAUMA AUDIT AND RESEARCH NETWORK The TARNlet Committee Mr Ross Fisher Co-chairman of TARNlet Consultant in Paediatric
England & Wales 2 YEARS OF SEVERE INJURY IN CHILDREN January 2013-December 2014 THE TRAUMA AUDIT AND RESEARCH NETWORK The TARNlet Committee Mr Ross Fisher Co-chairman of TARNlet Consultant in Paediatric
Best-evidence Review of Acute Care for Moderate to Severe Traumatic Brain Injury
 Pragmatic Evidence-based Review Best-evidence Review of Acute Care for Moderate to Severe Traumatic Brain Injury Reviewer Mark Ayson MBChB DPH Date Report Completed August 2011 Important Note: It is not
Pragmatic Evidence-based Review Best-evidence Review of Acute Care for Moderate to Severe Traumatic Brain Injury Reviewer Mark Ayson MBChB DPH Date Report Completed August 2011 Important Note: It is not
Occurrence and Risk Factors for Post-traumatic Epilepsy in Civilian Poulations December 2, 2012
 Occurrence and Risk Factors for Post-traumatic Epilepsy in Civilian Poulations December 2, 2012 Dale C Hesdorffer, PhD GH Sergievsky Center Columbia University American Epilepsy Society Annual Meeting
Occurrence and Risk Factors for Post-traumatic Epilepsy in Civilian Poulations December 2, 2012 Dale C Hesdorffer, PhD GH Sergievsky Center Columbia University American Epilepsy Society Annual Meeting
Journal reading. Introduction. Introduction. Ottawa Ankle Rules. Method
 Journal reading Presenter: PGY 林聖傑 Supervisor: Dr. 林俊龍 102.12.23 The accuracy of ultrasound evaluation in foot and ankle trauma Salih Ekinci, MD American Journal of Emergency Medicine 31 (2013) 1551 1555
Journal reading Presenter: PGY 林聖傑 Supervisor: Dr. 林俊龍 102.12.23 The accuracy of ultrasound evaluation in foot and ankle trauma Salih Ekinci, MD American Journal of Emergency Medicine 31 (2013) 1551 1555
Children diagnosed with skull fractures are often. Transfer of children with isolated linear skull fractures: is it worth the cost?
 clinical article J Neurosurg Pediatr 17:602 606, 2016 Transfer of children with isolated linear skull fractures: is it worth the cost? Ian K. White, MD, 1 Ecaterina Pestereva, BS, 1 Kashif A. Shaikh, MD,
clinical article J Neurosurg Pediatr 17:602 606, 2016 Transfer of children with isolated linear skull fractures: is it worth the cost? Ian K. White, MD, 1 Ecaterina Pestereva, BS, 1 Kashif A. Shaikh, MD,
COMPUTERIZED TOMOGRAPHY FINDINGS IN PATIENTS PRESENTING WITH HEAD INJURY IN CALABAR, NIGERIA
 Asian Journal of Medical Science, Volume-5(2014) COMPUTERIZED TOMOGRAPHY FINDINGS IN PATIENTS PRESENTING WITH HEAD INJURY IN CALABAR, NIGERIA ORIGINAL ARTICLE,Vol-5 No.2 http://nepjol.info/index.php/ajms
Asian Journal of Medical Science, Volume-5(2014) COMPUTERIZED TOMOGRAPHY FINDINGS IN PATIENTS PRESENTING WITH HEAD INJURY IN CALABAR, NIGERIA ORIGINAL ARTICLE,Vol-5 No.2 http://nepjol.info/index.php/ajms
Flow-diverting stents (in the Treatment of intracranial aneurysms)
") National Hospital for Neurology and Neurosurgery Flow-diverting stents (in the Treatment of intracranial aneurysms) Lysholm Department of Neuroradiology If you would like this document in another language
National Hospital for Neurology and Neurosurgery Flow-diverting stents (in the Treatment of intracranial aneurysms) Lysholm Department of Neuroradiology If you would like this document in another language
Ischemic Stroke in Critically Ill Patients with Malignancy
 Ischemic Stroke in Critically Ill Patients with Malignancy Jeong-Am Ryu 1, Oh Young Bang 2, Daesang Lee 1, Jinkyeong Park 1, Jeong Hoon Yang 1, Gee Young Suh 1, Joongbum Cho 1, Chi Ryang Chung 1, Chi-Min
Ischemic Stroke in Critically Ill Patients with Malignancy Jeong-Am Ryu 1, Oh Young Bang 2, Daesang Lee 1, Jinkyeong Park 1, Jeong Hoon Yang 1, Gee Young Suh 1, Joongbum Cho 1, Chi Ryang Chung 1, Chi-Min
Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report
 214 Balasa et al - Acute cerebral MCA ischemia Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report D. Balasa 1, A. Tunas 1, I. Rusu
214 Balasa et al - Acute cerebral MCA ischemia Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report D. Balasa 1, A. Tunas 1, I. Rusu
National guidelines CSSL / Head injury. Guidelines on the management of a patient with a head injury
 Guidelines on the management of a patient with a head injury College of Surgeons of Sri Lanka 2007 1 Authors Dr. Prasanna Gunasena Consultant Neurosurgeon Teaching Hospital Anuradhapura (Group Coordinator)
Guidelines on the management of a patient with a head injury College of Surgeons of Sri Lanka 2007 1 Authors Dr. Prasanna Gunasena Consultant Neurosurgeon Teaching Hospital Anuradhapura (Group Coordinator)
spontaneous localises pain withdraws to pain abnormal flexion abnormal extension none > 5 years 2 5 years 0 2 years
 APPENDIX. GLASGOW COMA SCALES (GCS) For Adults Alert patients have a total score of 5 Eye Opening: to voice to pain Verbal Score: 5 oriented confused but answers questions inappropriate words: recognises
APPENDIX. GLASGOW COMA SCALES (GCS) For Adults Alert patients have a total score of 5 Eye Opening: to voice to pain Verbal Score: 5 oriented confused but answers questions inappropriate words: recognises
Determinants of hospital costs associated with traumatic brain injury in England and Wales*
 Anaesthesia, 2008, 63, pages 499 508 doi:10.1111/j.1365-2044.2007.05432.x Determinants of hospital costs associated with traumatic brain injury in England and Wales* S. Morris, 1 S. Ridley, 2 F. E. Lecky,
Anaesthesia, 2008, 63, pages 499 508 doi:10.1111/j.1365-2044.2007.05432.x Determinants of hospital costs associated with traumatic brain injury in England and Wales* S. Morris, 1 S. Ridley, 2 F. E. Lecky,
Each year more than children are seen in hospital
 CMAJ Research CATCH: a clinical decision rule for the use of computed tomography in children with minor head injury Martin H. Osmond MD CM, Terry P. Klassen MD, George A. Wells PhD, Rhonda Correll RN,
CMAJ Research CATCH: a clinical decision rule for the use of computed tomography in children with minor head injury Martin H. Osmond MD CM, Terry P. Klassen MD, George A. Wells PhD, Rhonda Correll RN,
S pinal injury in the paediatric trauma patient can have
 860 ORIGINAL ARTICLE Patterns and risks in spinal trauma B W Martin, E Dykes, F E Lecky... See end of article for authors affiliations... Correspondence to: Dr B W Martin, Hope Hospital, Stott Lane, Salford
860 ORIGINAL ARTICLE Patterns and risks in spinal trauma B W Martin, E Dykes, F E Lecky... See end of article for authors affiliations... Correspondence to: Dr B W Martin, Hope Hospital, Stott Lane, Salford
Spectrum of various patterns of injuries in cranio-cerebral trauma: CT evaluation
 Original article: Spectrum of various patterns of injuries in cranio-cerebral trauma: CT evaluation 1Dr. Kaleem Ahmad, 2 Dr. RK Rauniyar, 3 Dr. Sajid Ansari, 4 Dr. Mukesh Kumar Gupta 1Associate Professor,
Original article: Spectrum of various patterns of injuries in cranio-cerebral trauma: CT evaluation 1Dr. Kaleem Ahmad, 2 Dr. RK Rauniyar, 3 Dr. Sajid Ansari, 4 Dr. Mukesh Kumar Gupta 1Associate Professor,
Referral for CT brain in adult patients with head injury: are Emergency Centre doctors adhering to the Western Cape Head Injury guidelines?
 Referral for CT brain in adult patients with head injury: are Emergency Centre doctors adhering to the Western Cape Head Injury guidelines? AUTHORS Dr DN Moiloa MBChB Dr Dave Fredericks MBChB, FCEM (SA)
Referral for CT brain in adult patients with head injury: are Emergency Centre doctors adhering to the Western Cape Head Injury guidelines? AUTHORS Dr DN Moiloa MBChB Dr Dave Fredericks MBChB, FCEM (SA)