Alan Barber. Professor of Clinical Neurology University of Auckland
|
|
|
- Alberta Gilbert
- 5 years ago
- Views:
Transcription

1 Alan Barber Professor of Clinical Neurology University of Auckland
2 Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal neurology
3 Diagnosed as TIA Discharged from hospital outpatient appointment at stroke clinic
4 Stroke
5 Loss of focal brain (or eye) function Of presumed vascular origin temporary loss of blood flow to brain/eye Symptoms resolve <24 hours Stroke
6 Loss of focal brain (or eye) function Of presumed vascular origin temporary loss of blood flow to brain/eye Symptoms resolve <24 hours A TIA is where stroke symptoms disappear within 24 hours Stroke
7
8 But
9 But most TIA s last only minutes 60% <1 hour 71% <2 hours 14% 2-24 hours
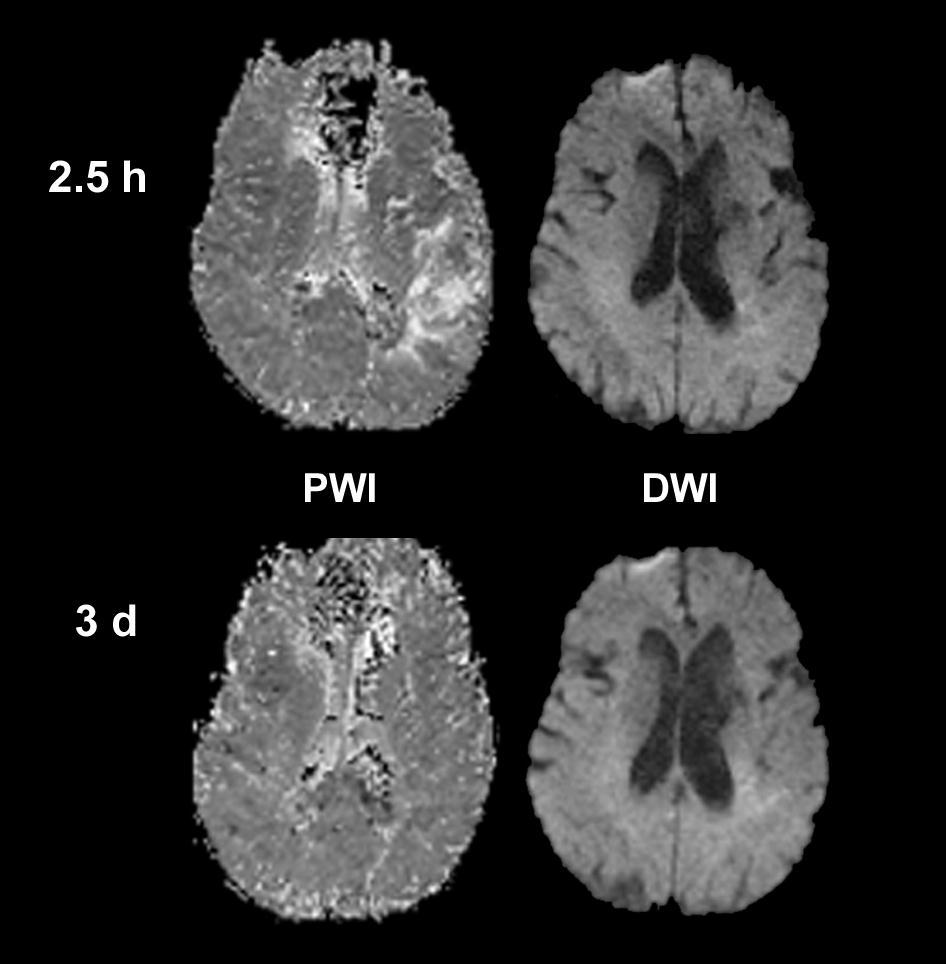
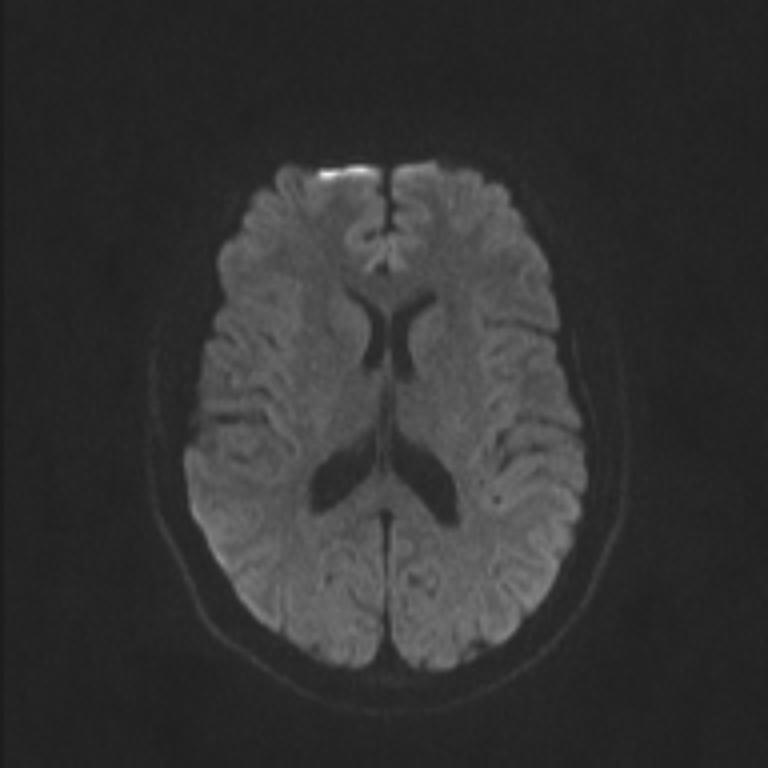
10 But 1/3 of TIA patients have acute cerebral infarction on MRI scans
11 Transient episode of neurological dysfunction caused by focal brain, spinal cord or retinal ischemia, without evidence of acute infarction
12 Transient episode of neurological dysfunction caused by focal brain, spinal cord or retinal ischemia, without evidence of acute infarction Tissue based definitions useful infarction distinguishes MI from angina focuses on pathophysiology, not temporal factors
13 An infarction of central nervous system tissue
14 TIAs don t precede cerebral hemorrhage don t cause loss of consciousness
15 TIAs don t precede cerebral hemorrhage don t cause loss of consciousness TIAs almost never cause isolated focal symptoms double vision or dysphagia non-focal symptoms faintness, dizziness, confusion
16 1 in 5 people with stroke had a TIA first
17 1 in 5 people with stroke had a TIA first The risk of stroke following a TIA is high
18 1 in 5 people with stroke had a TIA first The risk of stroke following a TIA is high Strokes after TIA are severe 1 in 5 fatal 2 in 3 survivors disabled
19 1 in 5 people with stroke had a TIA first The risk of stroke following a TIA is high Strokes after TIA are severe 1 in 5 fatal 2 in 3 survivors are disabled Not all TIAs carry the same stroke risk
20 Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal neurology
21
22 Age 60 1
23 Age 60 1 Blood pressure high 1
24 Age 60 1 Blood pressure high 1 Clinical no weakness 0 speech/no weakness 1 unilateral weakness 2
25 Age 60 1 Blood pressure high 1 Clinical no weakness 0 speech/no weakness 1 unilateral weakness 2 Duration <10 mins mins 1 1 hour 2

26 Age 60 1 Blood pressure high 1 Clinical no weakness 0 speech/no weakness 1 unilateral weakness 2 Duration <10 mins mins 1 1 hour 2 Diabetes 1
27 Presented with L numbness & slurred speech 2 episodes - 1 st 10 mins, 2 nd 2 hrs Hypertension Type II DM Examination normal but BP 160/95 ABCD2 = 6
28 25% 20% Stroke Risk 15% 10% 2-Day Risk 7-Day Risk 30-Day Risk 90-Day Risk 5% 0% ABCD 2 Score
29 ABCD2 score: Proportion of TIAs 34% 45% 21% Stroke risk at 2 days days months
30 As bad or worse than unstable angina Unstable angina 12% 30 day risk of death or MI Lancet 2002;359:189-98
31 80% of strokes after TIA can be prevented start aspirin (or clopidogrel) straight away blood pressure lowering therapy cholesterol lowering therapy stop smoking urgent carotid revascularisation
32 Discharged from hospital no change to usual aspirin outpatient appointment at stroke clinic Represented 4 days later with severe stroke left hemiparesis, sensory loss and neglect
33 Patients who need to be seen urgently ABCD 2 4 ABCD 2 <4 and In atrial fibrillation On an anti-coagulant Crescendo (recurrent TIAs) Patients who don t need to be seen urgently ABCD 2 <4 TIA more than a week ago ABCD 2 no good for posterior circulation
34 Patients who need to be seen urgently ABCD 2 4 ABCD 2 <4 and In atrial fibrillation On an anti-coagulant Crescendo (recurrent TIAs) Patients who don t need to be seen urgently ABCD 2 <4 TIA more than a week ago n
35 Patients who need to be seen urgently ABCD 2 4 ABCD 2 <4 and In atrial fibrillation On an anti-coagulant Crescendo (recurrent TIAs) Patients who don t need to be seen urgently ABCD 2 <4 TIA more than a week ago ABCD 2 no good for posterior circulation



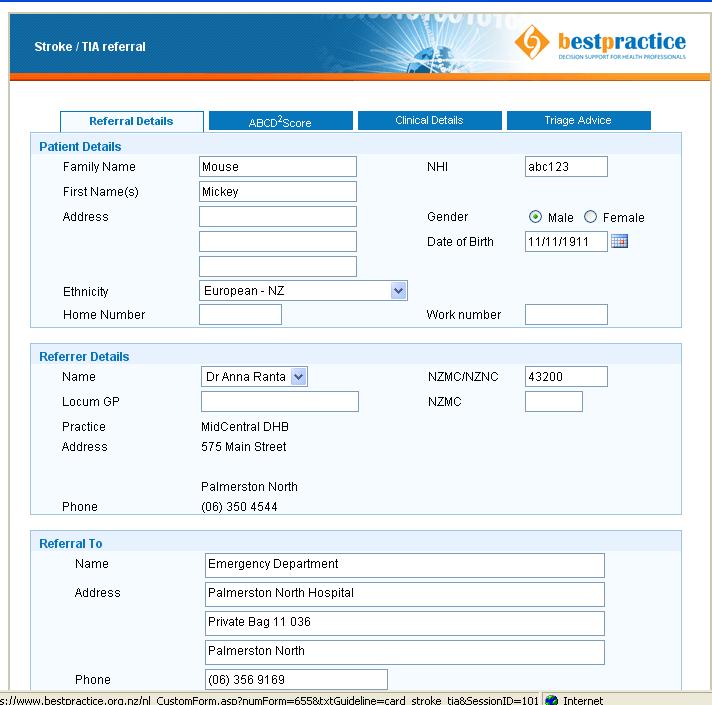
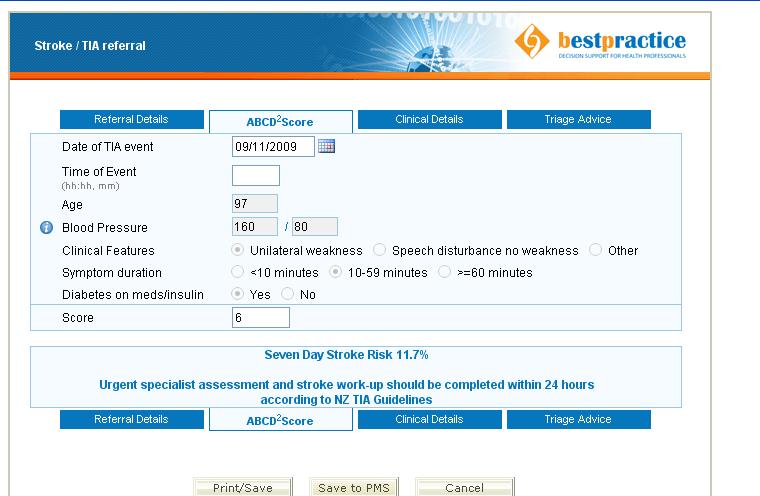
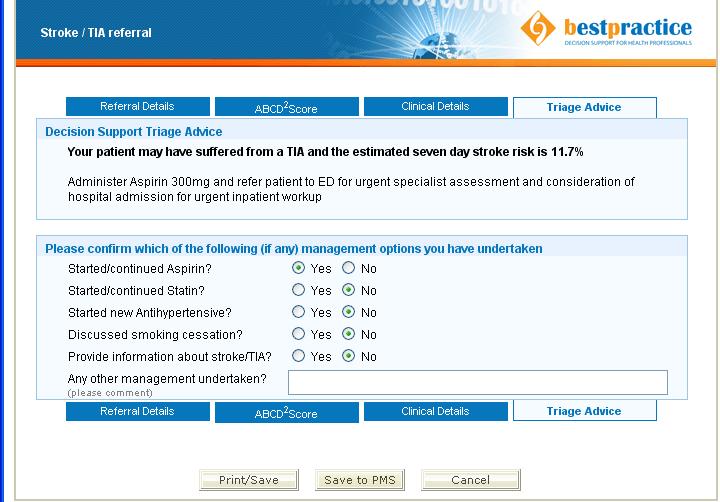
36 Dr Anna Ranta, MD, FRACP on behalf of the FASTEST Trial Team

37
38 In primary care, an electronic decision support tool Improved guideline adherence Reduced 90 day stroke risk Reduced treatment costs without affecting safety A Ranta Neurology 2015
39
40 R weakness lasting <10 mins Past history nil / no meds never smoked Diagnosed TIA
41 Age 60 1 Blood pressure high 1 Clinical no weakness 0 speech/no weakness 1 unilateral weakness 2 Duration <10 mins mins 1 1 hour 2 Diabetes 1
42 R weakness lasting <10 mins Past history nil / no meds never smoked ABCD2 = 2 3% three month stroke risk
43 R weakness lasting <10 mins Past history nil / no meds never smoked ABCD2 = 2 3% three month stroke risk No meds started & referred to outpatients
44 Admitted 3 days later slurred speech R face, arm and leg weakness BP 220/120 L subcortical infarct
45 We recommend sending patients to ED if ABCD 2 4 ABCD 2 <4 and In atrial fibrillation On an anti-coagulant Crescendo (recurrent TIAs)
46 But ABCD 2 = 2 patient still at risk for stroke (1 in 33)
47 But ABCD 2 = 2 patient still at risk for stroke (1 in 33) Before they leave start secondary prevention aspirin or clopidogrel anti-hypertensive lipid lowering therapy
48
49 Successive days had transient (10-15 mins) right amaurosis fugax left hand weakness one episode of right leg weakness Hypertensive, cholesterol, ex smoker R carotid bruit & normal neuro examination
50 Age 60 1 Blood pressure high 1 Clinical no weakness 0 speech/no weakness 1 unilateral weakness 2 Duration <10 mins mins 1 1 hour 2 Diabetes 1 10% three month stroke risk
51 Successive days had transient (10-15 mins) right amaurosis fugax left hand weakness one episode of right leg weakness Hypertensive, cholesterol, ex smoker R carotid bruit & normal neuro examination Started aspirin & sent in
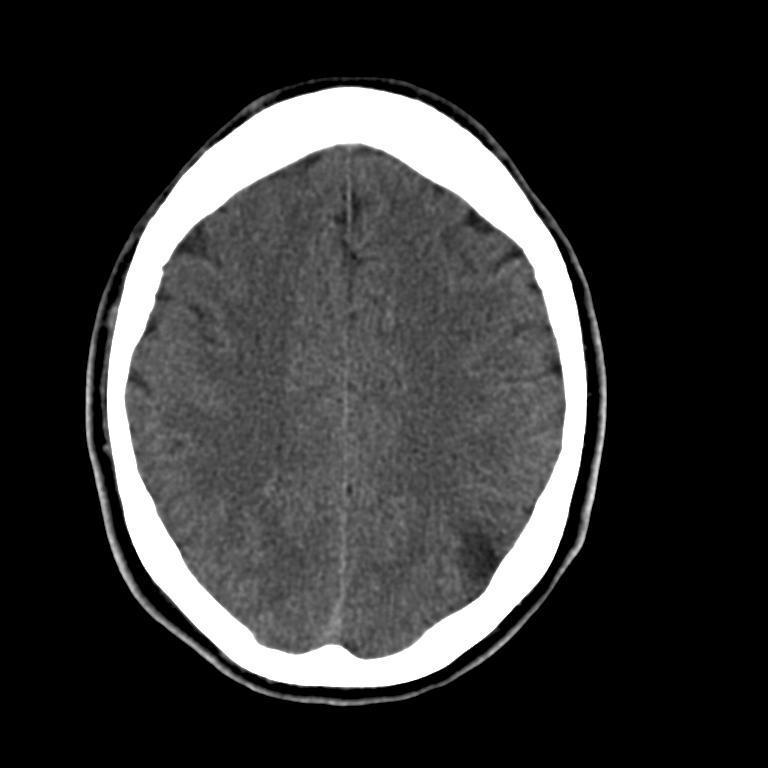
52 CT head normal Carotid US >70% right ICA stenosis L ICA occlusion Management iv heparin urgent carotid endarterectomy no further events
53 Send people to ED if recurrent TIAs regardless of ABCD 2 iv heparin often used with crescendo TIAs Urgent carotid US for people with carotid territory TIAs most benefit of carotid revascularisation in 1 st days after a TIA or minor stroke
54 Send people to ED if recurrent TIAs regardless of ABCD 2 iv heparin often used with crescendo TIAs Urgent carotid US for people with carotid territory TIAs most benefit of carotid revascularisation in 1 st days after a TIA or minor stroke What was the cause of right leg weakness?
55
56 Presented with slurred speech resolved after 1 h very mild L leg weakness (persisting when seen) Background HT dyslipidaemia TIA diagnosed & aspirin started
57 Admitted 3 weeks later headache L leg heavy and dragging Examination mild left arm & leg incoordination

58
59 It s not a TIA if neurological symptoms & signs when you see them TIA patients need brain imaging
60
61 Presented with left sided tongue numbness & tingling numbness slowly spread over 10 mins left mouth, face, upper limb & lower limb left upper & lower limbs felt heavy Background Nil Oral contraceptive
62 Examination Alert and oriented left facial, arm & leg sensory loss 4+/5 weakness left upper & lower limbs Investigations ECG normal Bloods normal

63
64 What s going on?
65 What s going on? Migraine
66 What s going on? Migraine Had low grade left-sided pressure that she hadn t commented on until asked Nothing to suggest previous migraine No family history of migraine Started Amitriptyline increasing to 75 mg at night
67 Tingling is a positive symptom should prompt consideration of migraine or sensory seizures Sensory march of symptoms over minutes typical for migraine Headache in migraine can be subtle
68
69 Presented with multiple episodes of L arm weakness L face and hand numbness/tingling lasting 20 mins Hypertensive Normal examination Multiple TIAs
70 Age 60 1 Blood pressure high 1 Clinical no weakness 0 speech/no weakness 1 unilateral weakness 2 Duration <10 mins mins 1 1 hour 2 Diabetes 1 10% three month stroke risk

71
72 What s going on?
73 What s going on? Subarachnoid blood Sensory seizures Episodes stopped on phenytoin
74 Tingling is a positive symptom should prompt consideration of migraine or sensory seizures
75
76 Recurrent thunderclap headaches Recurrent episodes of ataxia bilateral LL weakness & sensory loss visual blurring Fluoxetine for depression Daily cannabis use


77
78 Admission

79 Admission 6 weeks later
80 94% thunderclap headaches 22% cortical SAH 16% TIA 4% stroke 6% intracerebral hemorrhage 3% seizures Ducros A. Brain;2007;130:3091
81 RCVS 37% spontaneous 7% post partum 55% vasoactive substances cannabis 30% SSRI 19% decongestants 12% cocaine 5% Ducros A. Brain;2007;130:3091
82
83 Presented (while driving) with Left upper limb fat & heavy Had to steer with right hand Then involuntary jerking left arm over 45 mins No alteration of awareness or other symptoms
84 Left parietal infarct at 30 years Left MCA TIA 2008 normal carotid ultrasound scan Smoker Migraine

85
86 What s going on?
87 What s going on? Focal onset seizures
88 What s going on? Focal onset seizures What do you do?
89 What s going on? Focal onset seizures What do you do? Lamotrigine; increasing to 100 mg BD Driving restriction
90
91 6x episodes over 4 weeks L upper & lower limb shaking when standing or walking eased if lay down Background R MCA infarct at 34 years Occluded R ICA Hypertensive, elevated lipids, smoker

92 L & R ICA systems separate with no Circle of Willis flow R ICA occluded R CCA stensosed L ICA patent
93
94 Jerky, coarse, involuntary movements upper +/- lower limbs multiple episodes last < 5 minutes precipitated by rising, exercising, coughing often accompanied by paresis 10% of patients with ICA occlusion Persoon S. Brain;2010;133:915
95 Due to low cerebral blood flow Not recurrent emboli epileptic no change level of consciousness face & trunk spared no Jacksonian march normal EEG Persoon S. Brain;2010;133:915


96 L & R ICA systems separate with no Circle of Willis flow R ICA occluded R CCA stensosed L ICA patent R CCA stented
97
98 TIAs precede ¼ strokes carry a poor prognosis up to 80% of strokes can be prevented stroke risk can be determined by ABCD2 score
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
TIA Transient Ischaemic Attack?
 TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Management of TIA. Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital
 Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Vague Neurological Conditions
 Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide
 User Guide") New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers and
New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers and
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
It s Always a Stroke; Except For When It s Not..
 It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
PAPER F National Collaborating Centre for Chronic Conditions at the Royal College of Physicians
 6.3 Early carotid imaging in acute stroke or TIA Evidence Tables IMAG4: Which patients with suspected stroke/tia should be referred for urgent carotid imaging? Reference Ahmed AS, Foley E, Brannigan AE
6.3 Early carotid imaging in acute stroke or TIA Evidence Tables IMAG4: Which patients with suspected stroke/tia should be referred for urgent carotid imaging? Reference Ahmed AS, Foley E, Brannigan AE
PFO closure group total no. PFO closure group no. of males
 Suppl Table. Characteristics of the five trials included in this meta-analysis. Trial name Device used for Definition of medical Primary Endpoint group total no. group no. of males group age (yrs) group
Suppl Table. Characteristics of the five trials included in this meta-analysis. Trial name Device used for Definition of medical Primary Endpoint group total no. group no. of males group age (yrs) group
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Neurological Dilemmas in Primary Care
 Neurological Dilemmas in Primary Care David Clark, DO dclark@oregonneurology.com When to test? How to test? Pitfalls in testing? When to treat? How to treat? How long to treat? Neurological Dilemmas Seizure
Neurological Dilemmas in Primary Care David Clark, DO dclark@oregonneurology.com When to test? How to test? Pitfalls in testing? When to treat? How to treat? How long to treat? Neurological Dilemmas Seizure
Aortic arch pathology. Cerebral ischemia following carotid artery stenosis.
 Important: -Subclavian Steal Syndrome -Cerebral ischemia Aortic arch pathology. Cerebral ischemia following carotid artery stenosis. Mina Aubeed & Alba Hernández Pinilla Aortic arch pathology Common arch
Important: -Subclavian Steal Syndrome -Cerebral ischemia Aortic arch pathology. Cerebral ischemia following carotid artery stenosis. Mina Aubeed & Alba Hernández Pinilla Aortic arch pathology Common arch
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
E X P L A I N I N G STROKE
 EXPLAINING STROKE Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
EXPLAINING STROKE Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
Appendix 2C - Stroke Services in Fife
 Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Cerebrovascular Disease. RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009
 Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Referral Guideline for Patients with TIA
 DERBYSHIRE COUNTY PCT & NHS DERBY CITY Clinical Effectiveness & Guidelines Group Referral Guideline for Patients with TIA Key Messages This is a revised guideline for patients referred to the TIA service
DERBYSHIRE COUNTY PCT & NHS DERBY CITY Clinical Effectiveness & Guidelines Group Referral Guideline for Patients with TIA Key Messages This is a revised guideline for patients referred to the TIA service
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion
 Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million life insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
25/09/2018 HEADACHE. Dr Nick Pendleton
 HEADACHE Dr Nick Pendleton September 2018 1 Small Group Work Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache
HEADACHE Dr Nick Pendleton September 2018 1 Small Group Work Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million Life Insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
HEADACHE. Dr Nick Pendleton. September Headache
 HEADACHE Dr Nick Pendleton September 2017 Headache Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache Raised ICP
HEADACHE Dr Nick Pendleton September 2017 Headache Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache Raised ICP
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TIAs and posterior circulation problems
 TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to
 It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to George Eliot The Cripples (1949) All cerebrovascular events in
It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to George Eliot The Cripples (1949) All cerebrovascular events in
There are several types of epilepsy. Each of them have different causes, symptoms and treatment.
 1 EPILEPSY Epilepsy is a group of neurological diseases where the nerve cell activity in the brain is disrupted, causing seizures of unusual sensations, behavior and sometimes loss of consciousness. Epileptic
1 EPILEPSY Epilepsy is a group of neurological diseases where the nerve cell activity in the brain is disrupted, causing seizures of unusual sensations, behavior and sometimes loss of consciousness. Epileptic
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
How do we assess risk in TIA?
 How do we assess risk in TIA? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give them
How do we assess risk in TIA? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give them
Acute Complications of Sickle Cell Disease Case Study 5 year old girl with Hemoglobin SS, weakness and slurred speech
 Acute Complications of Sickle Cell Disease Case Study 5 year old girl with Hemoglobin SS, weakness and slurred speech Beatrice E. Gee, MD Medical Director, Sickle Cell and Hematology Program Children s
Acute Complications of Sickle Cell Disease Case Study 5 year old girl with Hemoglobin SS, weakness and slurred speech Beatrice E. Gee, MD Medical Director, Sickle Cell and Hematology Program Children s
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)).
).") 12.0 Outcomes 12.1 Definitions 12.1.1 Neurologic Outcome Events a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)). Criteria:
12.0 Outcomes 12.1 Definitions 12.1.1 Neurologic Outcome Events a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)). Criteria:
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
GOVERNANCE BOARD. 14th January Clinical Audit of Stroke Services. At Shrewsbury and Telford Hospitals NHS Trust
 GOVERNANCE BOARD 14th January 2014 Clinical Audit of Stroke Services At Shrewsbury and Telford Hospitals NHS Trust 1.0 Introduction A clinical review of cases recorded and coded as with a 0-1 day length
GOVERNANCE BOARD 14th January 2014 Clinical Audit of Stroke Services At Shrewsbury and Telford Hospitals NHS Trust 1.0 Introduction A clinical review of cases recorded and coded as with a 0-1 day length
How to Think like a Neurologist Review of Exam Process and Assessment Findings
 Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Mimics. Atlantic Canada Stroke Conference. Dr Warren Fieldus FRCP
 Stroke Mimics Atlantic Canada Stroke Conference Dr Warren Fieldus FRCP No Conflicts of Interest the plan stroke or no stroke QEII Acute Stroke Protocol things to do before the CT common stroke mimics (25
Stroke Mimics Atlantic Canada Stroke Conference Dr Warren Fieldus FRCP No Conflicts of Interest the plan stroke or no stroke QEII Acute Stroke Protocol things to do before the CT common stroke mimics (25
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
P1: OTA/XYZ P2: ABC c01 BLBK231-Ginsberg December 23, :43 Printer Name: Yet to Come. Part 1. The Neurological Approach COPYRIGHTED MATERIAL
 Part 1 The Neurological Approach COPYRIGHTED MATERIAL 1 2 Chapter 1 Neurological history-taking The diagnosis and management of diseases of the nervous system have been revolutionized in recent years by
Part 1 The Neurological Approach COPYRIGHTED MATERIAL 1 2 Chapter 1 Neurological history-taking The diagnosis and management of diseases of the nervous system have been revolutionized in recent years by
OVER- REACT. HOW MANY OF THE 10 STROKE SYMPTOMS DO YOU KNOW? Learn them inside > If you suspect STROKE, CALL 911 immediately
 OVER- REACT We were out with friends when my husband suddenly had trouble walking. I suspected stroke, so I CALLED 911 IMMEDIATELY. It helped save his life. If you suspect STROKE, CALL 911 immediately
OVER- REACT We were out with friends when my husband suddenly had trouble walking. I suspected stroke, so I CALLED 911 IMMEDIATELY. It helped save his life. If you suspect STROKE, CALL 911 immediately
Redgrave JN, Coutts SB, Schulz UG et al. Systematic review of associations between the presence of acute ischemic lesions on
 6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
Stroke Awareness. Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director
 Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
STROKE INTRODUCTION OBJECTIVES. When the student has finished this module, he/she will be able to:
 STROKE INTRODUCTION Stroke is the medical term for a specific type of neurological event that causes damage to the brain. There are two types of stroke, but both types of stroke cause the same type of
STROKE INTRODUCTION Stroke is the medical term for a specific type of neurological event that causes damage to the brain. There are two types of stroke, but both types of stroke cause the same type of
Understanding Stroke
 MINTO PREVENTION & REHABILITATION CENTRE CENTRE DE PREVENTION ET DE READAPTATION MINTO Understanding Stroke About This Kit Stroke is the fourth leading cause of death in Canada after heart disease and
MINTO PREVENTION & REHABILITATION CENTRE CENTRE DE PREVENTION ET DE READAPTATION MINTO Understanding Stroke About This Kit Stroke is the fourth leading cause of death in Canada after heart disease and
David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK
 Risk Stratification in TIA/Stroke? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give
Risk Stratification in TIA/Stroke? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give
ICSS Safety Results NOT for PUBLICATION. June 2009 ICSS ICSS ICSS ICSS. International Carotid Stenting Study: Main Inclusion Criteria
 Safety Results NOT for The following slides were presented to the Investigators Meeting on 22/05/09 and most of them were also presented at the European Stroke Conference on 27/05/09 They are NOT for in
Safety Results NOT for The following slides were presented to the Investigators Meeting on 22/05/09 and most of them were also presented at the European Stroke Conference on 27/05/09 They are NOT for in
Neurology Topics. Ian Rosemergy
 Neurology Topics Ian Rosemergy Plan An unusual presentation of a not so unusual problem Some seizure cases 49 year old female Patient 1 Hit on back and neck by swinging car door o Severe neck and shoulder
Neurology Topics Ian Rosemergy Plan An unusual presentation of a not so unusual problem Some seizure cases 49 year old female Patient 1 Hit on back and neck by swinging car door o Severe neck and shoulder
TIA triage in Not all that glitters is gold
 TIA triage in 2016 Not all that glitters is gold Disclosures No industry related disclosures Expert witness work Overview Definition Implications Guidelines, secondary prevention Implementation of guidelines
TIA triage in 2016 Not all that glitters is gold Disclosures No industry related disclosures Expert witness work Overview Definition Implications Guidelines, secondary prevention Implementation of guidelines
Neuropathology lecture series. III. Neuropathology of Cerebrovascular Disease. Physiology of cerebral blood flow
 Neuropathology lecture series III. Neuropathology of Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O
Neuropathology lecture series III. Neuropathology of Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O
REFERRAL GUIDELINES VASCULAR SURGERY
 REFERRAL GUIDELINES VASCULAR SURGERY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template IMPORTANT: The
REFERRAL GUIDELINES VASCULAR SURGERY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template IMPORTANT: The
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015
 Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
Stroke Quality Measures. Kathy Wonderly RN, BSPA, CPHQ Performance Improvement Coordinator Developed: May, 2012 Most recently updated: December 2012
 1 Stroke Quality Measures Kathy Wonderly RN, BSPA, CPHQ Performance Improvement Coordinator Developed: May, 2012 Most recently updated: December 2012 2 Application of the Stroke Measure Set The stroke
1 Stroke Quality Measures Kathy Wonderly RN, BSPA, CPHQ Performance Improvement Coordinator Developed: May, 2012 Most recently updated: December 2012 2 Application of the Stroke Measure Set The stroke
Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
 STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
Recent Advances in Neurology Difficult Cases
 Patient X: History Part 1 Recent Advances in Neurology Difficult Cases Heather J. Fullerton, MD, MAS Professor of Neurology & Pediatrics Director, Pediatric Brain Center Previously healthy 14-year old
Patient X: History Part 1 Recent Advances in Neurology Difficult Cases Heather J. Fullerton, MD, MAS Professor of Neurology & Pediatrics Director, Pediatric Brain Center Previously healthy 14-year old
Stroke: Every Minute Counts! Primary Stroke Center, Ingalls Memorial Hospital
 Stroke: Every Minute Counts! Primary Stroke Center, Ingalls Memorial Hospital Objectives Describe the A & P of the nervous system Outline pathophysiological changes in the nervous system that may alter
Stroke: Every Minute Counts! Primary Stroke Center, Ingalls Memorial Hospital Objectives Describe the A & P of the nervous system Outline pathophysiological changes in the nervous system that may alter
Sex Differences in Stroke Risk and Quality of Life after Stroke
 Sex Differences in Stroke Risk and Quality of Life after Stroke Cheryl Bushnell, MD, MHS Associate Professor of Neurology Director, WFB Stroke Center Disclosures Research funding from: World Federation
Sex Differences in Stroke Risk and Quality of Life after Stroke Cheryl Bushnell, MD, MHS Associate Professor of Neurology Director, WFB Stroke Center Disclosures Research funding from: World Federation
Critical Review Form Therapy
 Critical Review Form Therapy A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects, Lancet-Neurology 2007; 6: 953-960 Objectives: To evaluate the effect of
Critical Review Form Therapy A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects, Lancet-Neurology 2007; 6: 953-960 Objectives: To evaluate the effect of
TCD in Subclavian Steal Syndrome
 ISSN 2005-7881 Journal of Neurosonology 2(Suppl. 1):25-30, 2010 TCD in Subclavian Steal Syndrome Soon-Tae Lee, M.D., Ph.D. Department of Neurology, Seoul National University Hospital, Seoul, South Korea
ISSN 2005-7881 Journal of Neurosonology 2(Suppl. 1):25-30, 2010 TCD in Subclavian Steal Syndrome Soon-Tae Lee, M.D., Ph.D. Department of Neurology, Seoul National University Hospital, Seoul, South Korea
Disclosures. An Update on TIA and Minor Stroke. The Agenda PROGNOSIS PATHOPHYSIOLOGY GUIDELINES AND PROVEN MANAGEMENT STRATEGIES AGGRESSIVE TREATMENT
 Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Department Specific Guideline
 Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
ESM 1. Survey questionnaire sent to French GPs. Correct answers are in bold. Part 2: Clinical cases: (Good answer are in bold) Clinical Case 1:
 Clinical Case 1:") ESM 1. Survey questionnaire sent to French GPs. Correct answers are in bold. Part 2: Clinical cases: (Good answer are in bold) Clinical Case 1: to your office at 2 pm for a feeling of weakness and numbness
ESM 1. Survey questionnaire sent to French GPs. Correct answers are in bold. Part 2: Clinical cases: (Good answer are in bold) Clinical Case 1: to your office at 2 pm for a feeling of weakness and numbness
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
IDPH EMS Region Five. Stroke Education
 IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.
IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.
Faculty of Clinical Forensic Medicine Committee 1/2018
 Guideline Subject: Clinical Forensic Assessment and Management of Non-Fatal Strangulation Approval Date: January 2018 Review Date: January 2021 Review By: Number: Faculty of Clinical Forensic Medicine
Guideline Subject: Clinical Forensic Assessment and Management of Non-Fatal Strangulation Approval Date: January 2018 Review Date: January 2021 Review By: Number: Faculty of Clinical Forensic Medicine
Current Clinical Trials for Stroke Survivors in NJ and Philadelphia Areas
 Current Clinical Trials for Survivors in NJ and Philadelphia Areas For more information go to https://clinicaltrials.gov/ and search for the title in search box Condition / Disease 1. Spatial Neglect and
Current Clinical Trials for Survivors in NJ and Philadelphia Areas For more information go to https://clinicaltrials.gov/ and search for the title in search box Condition / Disease 1. Spatial Neglect and
Guideline scope Stroke and transient ischaemic attack in over 16s: diagnosis and initial management (update)
") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Stroke Workshop. Pre-Workshop Handout. With Walter Himmel, Meeta Patel & Anton Helman
 2018 Stroke Workshop Pre-Workshop Handout With Walter Himmel, Meeta Patel & Anton Helman Instructions for Getting the Most Out of The EMU Stroke Workshop Handout This workshop has been designed around
2018 Stroke Workshop Pre-Workshop Handout With Walter Himmel, Meeta Patel & Anton Helman Instructions for Getting the Most Out of The EMU Stroke Workshop Handout This workshop has been designed around
Variables in Riksstroke - TIA
 Variables in Riksstroke - TIA The TIA registration started 2010 for patients treated in hospital and 2015 it was 67 of 72 hospitals are registrating TIA On the www.riksstroke.org/forms/ you find the Riksstroke
Variables in Riksstroke - TIA The TIA registration started 2010 for patients treated in hospital and 2015 it was 67 of 72 hospitals are registrating TIA On the www.riksstroke.org/forms/ you find the Riksstroke
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Document Title: The Management of Acute Ischemic Stroke & TIA
 Project: Ghana Emergency Medicine Collaborative Document Title: The Management of Acute Ischemic Stroke & TIA Author(s): Rashmi U. Kothari, M.D. (KCMS/MSU), 2012 License: Unless otherwise noted, this material
Project: Ghana Emergency Medicine Collaborative Document Title: The Management of Acute Ischemic Stroke & TIA Author(s): Rashmi U. Kothari, M.D. (KCMS/MSU), 2012 License: Unless otherwise noted, this material
An Introduc+on to Stroke
 An Introduc+on to Stroke Elizabeth Huntoon MS, MD Assistant Professor Department of Physical Medicine and Rehabilita>on Vanderbilt University School of Medicine Defini+on Sudden focal neurologic deficit
An Introduc+on to Stroke Elizabeth Huntoon MS, MD Assistant Professor Department of Physical Medicine and Rehabilita>on Vanderbilt University School of Medicine Defini+on Sudden focal neurologic deficit
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent