What s the evidence, why do guidelines differ, and what should the GP do?
|
|
|
- Marianna Allison
- 5 years ago
- Views:
Transcription



1 What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018
2 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be aiming for in treatment? How do the guidelines deal with this and how do they differ? Conclusions
3 What is hypertension?
4
5 140/90 mmhg measured in office Or 135/85mmHg measured ABPM or Home

6 (Office measurements) ESC/ESH Hypertension Guidelines 2013
7 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults
8 Hypertension reclassified! BP Category SBP DBP Normal <120 mm Hg and <80 mm Hg Elevated mm Hg and <80 mm Hg Hypertension Stage mm Hg or mm Hg Stage mm Hg or 90 mm Hg
9 Stroke Risk increases with age & usual BP High Risk Similarly for Heart Disease Low Low High

10 Bottom line BP vs Risk 10 mmhg 38% stroke risk 18% CHD risk
11 What is in a definition? Until the new US guidelines, there was remarkable unanimity Threshold and targets 140/90mmHg (office) Threshold arbitrary (previously 160/100mmHg) Is there new evidence to change current practice?
12 How should BP be measured / Hypertension diagnosed?

13 ESH/ESC Diagnosis

14 ESH/ESC Out of office measurement
15 US: Out-of-Office and Self-Monitoring of BP recommended COR I LOE A SR Recommendation for Out-of-Office and Self-Monitoring of BP Out-of-office BP measurements are recommended to confirm the diagnosis of hypertension and for titration of BP-lowering medication, in conjunction with telehealth counseling or clinical interventions.
16 Routine measurement is often flawed Dotplot of Last_practice_systolic Dotplot of systolic Last_practice_systolic Each symbol represents up to 4 observations. Same population with routine and research measurement systolic Each symbol represents up to 12 observations
17 Blood Pressure varies through the day and between seasons Hypertension. 2006;47:
18 Multiple measurements better estimate mean blood pressure
19 Many factors affect BP measurement BMJ 2001;322;

20 Nurse measured BP is 7mmHg systolic lower than GPs Clark et al BJGP 2014
21 What really happens when GPs measure blood pressure? A prospective mystery shopper study. Sarah Stevens
22 Methods An online survey was advertised to UK charities and patient groups July 2015-January Respondents reported basic demographic and health data, if/ how BP was measured at their last surgery appointment (1 BP reading), willingness to take part in the prospective study after their next appointment. Prospectively, patients reported if and how their BP was measured at their appointment (3 BP readings) using an online questionnaire.
23 Results: Participant characteristics Total respondents = 334 Characteristic Mean (SD) / N (%) Male 172 (52%) Age 59 (12) Current smoker 25 (7.5%) Hypertensive 200 (60%) Antihypertensive medication 173 (87%) Diabetes 279 (85%) BP measured during last appointment 217 (65%) By a GP 59 (27%) By a nurse 150 (69%) By the respondent in the waiting 8 (3.7%) room
24 Results: BP measurement In those reporting all readings (n=111): Initial BP was significantly lower in those who had their BP measured once, compared to those who had it measured 2 or 3 times.
25 Results: BP measurement In those reporting all readings (n=111): Initial BP was significantly lower in those who had their BP measured once, compared to those who had it measured 2 or 3 times. A majority (n=70, 63% [53 to 72%]) had their BP measured in line with current NICE guidelines.
26 How should hypertension be diagnosed?
27 Diagnosing hypertension Traditionally based on clinic measurement Most outcome trials use clinic measures But Flawed measure (one off from continuum) Takes weeks / months to make diagnosis
28 What about ABPM? Half hourly measurements during the day Better measure usual BP Hourly at night Main outcome is mean day time ABPM Other info available (dipping etc) Better correlated with end organ damage
29 Detection of white coat and masked HT Fagard R J Hyp 2007

30 Many people currently potentially misdiagnosed... Gill 2017 Worse if only studies around diagnostic threshold used: sensitivity of 86% and specificity of 46% BMJ 2011;342:d3621 doi: /bmj.d3621

31 Cost effectiveness ABPM most cost effective for every age group Lovibond et al Lancet 2011
32 BUT ABPM may be poorly tolerated 750 people in West Midlands underwent clinic (3 occasions), home (1 week) and ABPM (24hrs) ABPM rated significantly worse esp for disturbing sleep and disturbing usual activities (esp ethnic minorities) Focus Groups confirmed this Wood BJGP 2016
33 ...what I did mind was walking along the road and then I would get the warning and have to stop...and people were watching me...and it was so embarrassing (FAC6) my children...kept asking what s wrong with you?, especially with the 24 hour one (FSA1)
34 Does everyone need ABPM for diagnosis?
.")
35 Are multiple clinic blood pressure readings associated with the home-clinic blood pressure difference? 9 Sheppard JP, et al. (2014). Journal of hypertension; 32(11):2171-8
36 Results

37 Can clinic BP be combined with other factors to reduce need for ABPM? Extension of hypothesis Derivation and validation data sets Combines BP and clinical/demographics factors
38 Results Significant predictors of the homeclinic BP difference: Clinic blood pressure change Plus age, sex, mean clinic blood pressure, pulse pressure, BMI, and history of hypertension

39 PROOF-BP online calculator

40 Proposed Algorithm
41 How does it compare to existing strategies for diagnosis? Guideline (year) Sustained hypertensive Normotensive White coat hypertensive Masked hypertensive Correctly classified Referral for ABPM AHA 625 (57%) 173 (16%) 178 (16%) 124 (11%) 798 (73%) 0 (0%) (2005) CHEP 642 (58%) 172 (16%) 179 (16%) 107 (10%) 814 (74%) 0 (0%) (2014) ESH (2013) 596 (54%) 203 (18%) 148 (13%) 151 (14%) 799 (73%) 0 (0%) NICE (2011) PROOF-BP (2015) 513 (47%) 349 (32%) 2 (0.2%) 236 (21%) 862 (78%) 590 (54%) 720 (65%) 306 (28%) 45 (4%) 29 (3%) 1,026 (93%) 640 (58%)

42 What about guiding treatment?

43 TASMINH4 Results No differences in adverse events

44 Self-monitoring & co-interventions IPD from 25 trials Increasing intensity of co-intervention leads to increased efficacy BP-SMART collaboration PLOS medicine 2017
45 Conclusions measurement and diagnosis Major guidelines now recommend out-of-office measurement for both diagnosis and ongoing management Ambulatory monitoring gold standard for diagnosis but not available for/tolerated by all Routine clinic BP is not the same as in the trials PROOF BP suggests one way of reducing need for ABPM Home monitoring now has firm evidence base for ongoing management
46 What should we be aiming for in treatment?

47 Targets SBP <140mmHg

48 BP Goal for Patients With Hypertension 130/80mmHg COR I IIb LOE SBP: B-R SR DBP: C- EO SBP: B-NR DBP: C- EO Recommendations for BP Goal for Patients With Hypertension For adults with confirmed hypertension and known CVD or 10-year ASCVD event risk of 10% or higher a BP target of less than 130/80 mm Hg is recommended. For adults with confirmed hypertension, without additional markers of increased CVD risk, a BP target of less than 130/80 mm Hg may be reasonable.
49 SPRINT NEJM 2015
50 Inclusion & Exclusion INCLUDED Age of at least 50 years, SBP 130 to 180 mm Hg (medications <4) AND increased risk CVD Clinical or subclinical CVD CKD (egfr 20 60) 10-year CVD risk 15% Age 75 years EXCLUDED: Diabetes mellitus or prior stroke
51 Targets SBP <120mmHg vs <140mmHg Forced UP and DOWN titration to target (If SBP <130 once or <135 twice then up titrated in 140mmHg group)
52 Outcomes PRIMARY Composite outcome of myocardial infarction, acute coronary syndrome, stroke, acute heart failure, or death from cardiovascular causes. SECONDARYS included Individual components of primary outcome, Death from any cause, and the composite of the primary outcome or Death from any cause Harms
53 systolic Blood Pressure Measurement Automated Clinic BP measurement Three readings mostly unattended Mean of all three Participant rested for 5 minutes Interval Plot of systolic vs occasion 95% CI for the Mean 9mmHg drop over three readings occasion 4 5 6
54 Follow-up Planned 2 years recruitment, 6 years max FU What happened? Trial terminated early Median FU 3.6/5 years

55 How do they compare to your patients? 10% not on anti HT Rx at baseline
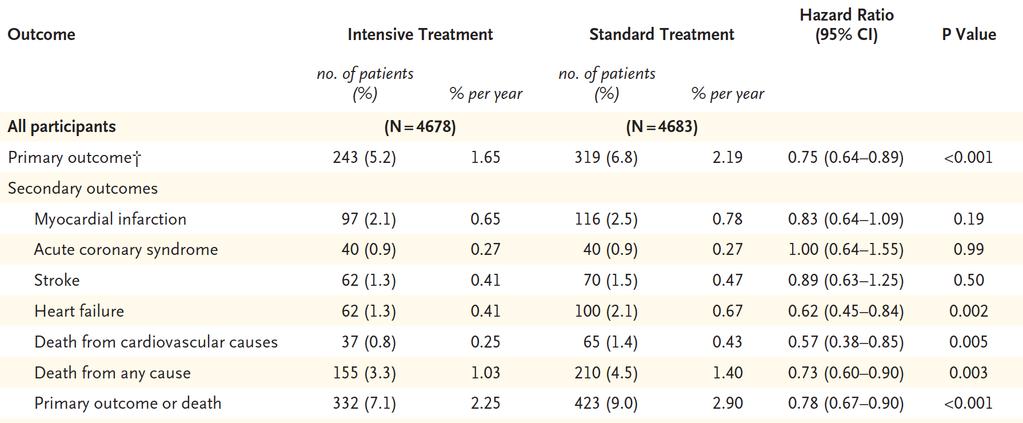
56 Results
57 NNT Primary 61 Death any cause 90

58 Outcomes over 75 Renal outcomes similar to all participants

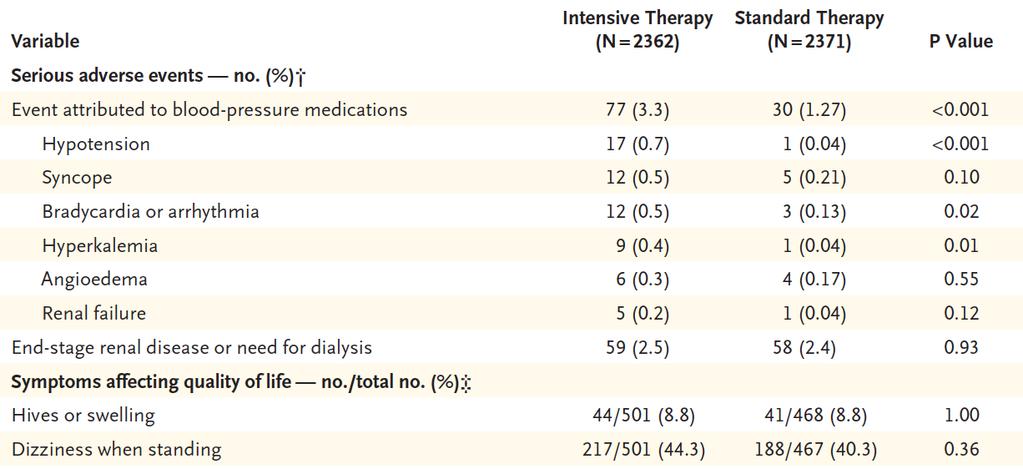
59 Adverse Events

60 Adverse Events (2)
61 accord Essentially SPRINT in type 2 Diabetes NEJM 2010

62 Outcomes Primary = nonfatal myocardial infarction, nonfatal stroke, or death from cardiovascular causes. The mean follow-up was 4.7 years.
63 Harms
64 SPS3 Lancet 2013
65 Inclusion / exclusion 30 years Normotensive or hypertensive, Recent symptomatic, MRI-confirmed lacunar stroke, Without: Carotid Artery stenosis, disabling stroke, haemorrhage or cortical stroke Targets SBP mm Hg vs <130 mm Hg. Forced UP and DOWN titration to target Third as many participants (3020)
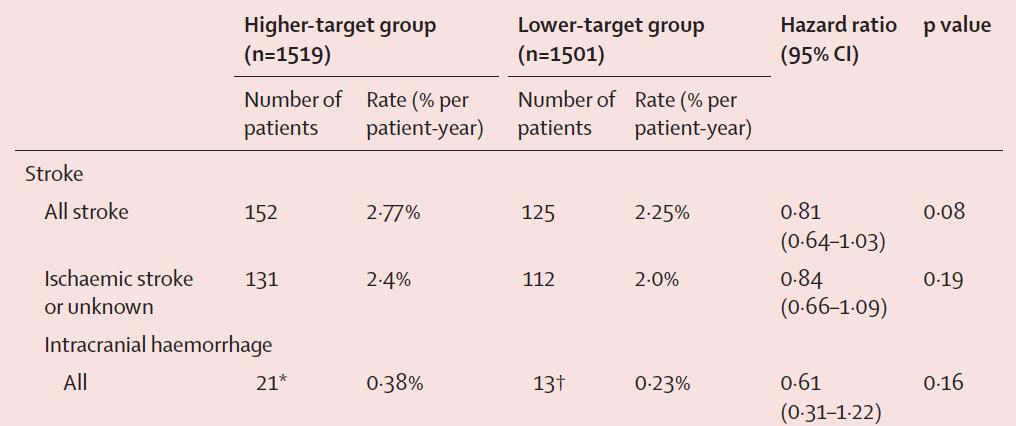
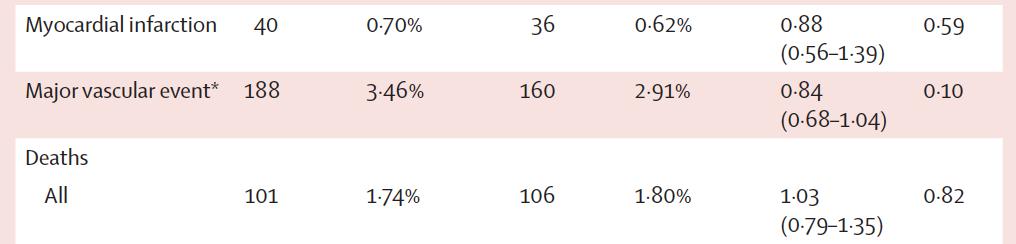
66 Outcomes
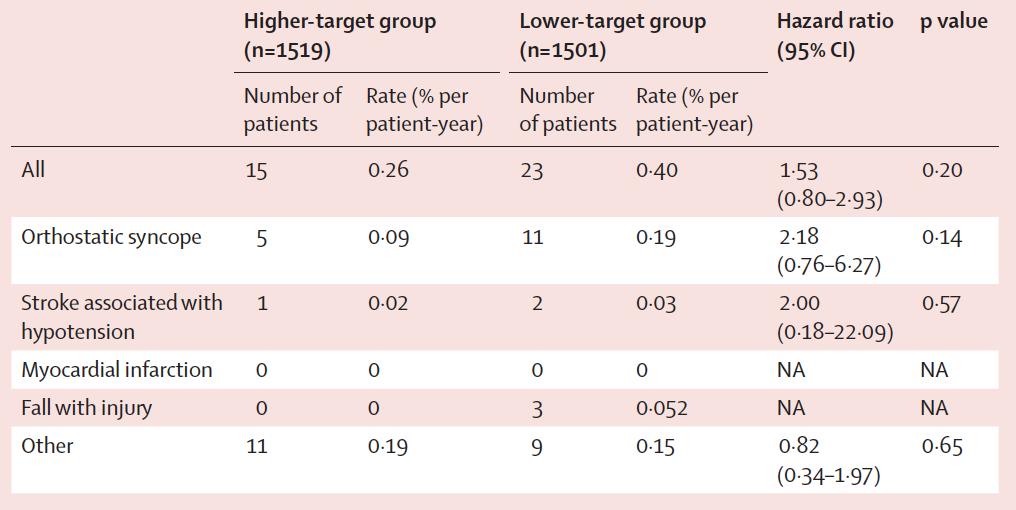
67 Harms
68 HOPE3
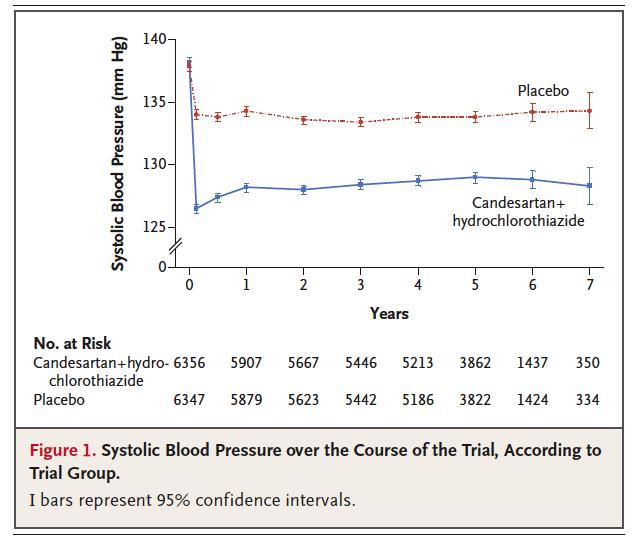
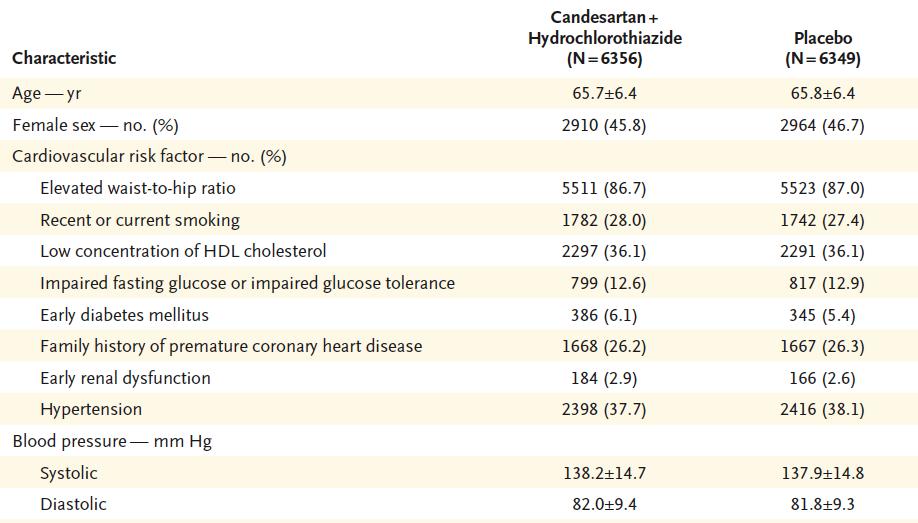
69 Methods N= 12,703; intermediate risk without CVD Men aged 55, women 65 Plus at least one of: raised hip/waist ratio, low HDL, smoker, dysglycaemia, FH premature CVD, CKD3 No clear indication for antiht Rx or statins Intervention ARB/Thiazide (candesartan/hcz) Co-primary MACE; Median follow-up 5.6 yrs
70 Results

71 Primary Outcomes First coprimary: composite of cardiovascular death, nonfatal myocardial infarction or nonfatal stroke; Second coprimary: composite of cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, resuscitated cardiac arrest, heart failure, or revascularization; First secondary: composite of cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, resuscitated cardiac arrest, heart failure, revascularization, or angina with objective evidence of ischemia.

72 HOPE3 Subgroups
73 How can we make sense of this?
74 Brunstrom SR JAMA 2017 PRIMARY PREVENTION
75 Conundrums & Conclusions SPRINT results clear: 130/80mmHg threshold but 90% already Rxd Consistent benefit across subgroups If anything older & frailer groups did better AOBP measurement Consistent point estimates with ACCORD & SPS3 which may have been underpowered HOPE 3 suggests treatment below 140/90mmHg in intermediate risk not helpful Brunstrom s Systematic Review does not support treatment below 140/90mmHg for primary prevention

76 Bottom line
77 Summary Hypertension thresholds largely arbitrary based on risk and evidence of benefit Out of office measurement now recommended for diagnosis and management of hypertension You don t need to do an ABPM on everyone and Home monitoring now has evidence base for long term FU SPRINT shows intensive treatment can work but leaves many unanswered questions HOPE3 suggests current thresholds for treatment appropriate in primary prevention New US guidelines redefine hypertension and treatment targets but European response to them awaited (2018 ESH/ESC conferences)
78 What do you think?
79 What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018
The earlier BP control the better cardiovascular outcome. Jin Oh Na Cardiovascular center Korea University Medical College
 The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
HYPERTENSION: ARE WE GOING TOO LOW?
 HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Update. Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016
 Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
HYPERTENSION: UPDATE 2018
 HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
2/11/2019 CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES DUALITY OF INTEREST
 CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES George L. Bakris, M.D.,F.A.S.N., F.A.H.A. Professor of Medicine Director, Am Heart Assoc. Comprehensive Hypertension Center University of Chicago Medicine
CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES George L. Bakris, M.D.,F.A.S.N., F.A.H.A. Professor of Medicine Director, Am Heart Assoc. Comprehensive Hypertension Center University of Chicago Medicine
Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China
 What Can We Learn from the Observational Studies and Clinical Trials of Prehypertension? Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China At ARIC visit 4
What Can We Learn from the Observational Studies and Clinical Trials of Prehypertension? Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China At ARIC visit 4
Overview. NOT A REPETION OF LOCAL GUIDELINE Dr Diviash Thakrar
 Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines. John Potter Professor Ageing & Stroke Medicine University of East Anglia
 Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure LIMBO How Low To Go?
 Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Evaluation and Management of Hypertension in Women. Vesna D. Garovic, M.D. Moscow, Russia, December 2016
 Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Blood Pressure Targets in Diabetes
 Stockholm, 29 th August 2010 ESC Meeting Blood Pressure Targets in Diabetes Peter M Nilsson, MD, PhD Department of Clinical Sciences University Hospital, Malmö Sweden Studies on BP in DM2 ADVANCE RCT (Lancet
Stockholm, 29 th August 2010 ESC Meeting Blood Pressure Targets in Diabetes Peter M Nilsson, MD, PhD Department of Clinical Sciences University Hospital, Malmö Sweden Studies on BP in DM2 ADVANCE RCT (Lancet
DECLARATION OF CONFLICT OF INTEREST. None
 DECLARATION OF CONFLICT OF INTEREST None How low should we go to avoid harm in hypertensives with comorbidities? CORONARY ARTERY DISEASE Prof. Dr. Maria DOROBANTU, FESC,FACC CARDIOLOGY EMERGENCY HOSPITAL
DECLARATION OF CONFLICT OF INTEREST None How low should we go to avoid harm in hypertensives with comorbidities? CORONARY ARTERY DISEASE Prof. Dr. Maria DOROBANTU, FESC,FACC CARDIOLOGY EMERGENCY HOSPITAL
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Managing Hypertension in 2018
 MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Hypertension: What s new since JNC 7. Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF
 Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3)
") Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3) Χάρης Γράσσος MD,FESC,PhD,EHS Διευθυντής Καρδιολόγος Γ.Ν.Α ΚΑΤ Visiting Professor University of Bolton U.K New England
Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3) Χάρης Γράσσος MD,FESC,PhD,EHS Διευθυντής Καρδιολόγος Γ.Ν.Α ΚΑΤ Visiting Professor University of Bolton U.K New England
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Masked Hypertension. Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre
 Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Slide notes: References:
 1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
Ambulatory BP Monitoring: Getting the Diagnosis of Hypertension Right. Anthony J. Viera, MD, MPH, FAHA Professor and Chair
 Ambulatory BP Monitoring: Getting the Diagnosis of Hypertension Right Anthony J. Viera, MD, MPH, FAHA Professor and Chair Objectives Review limitations of office BP in making a correct diagnosis of hypertension
Ambulatory BP Monitoring: Getting the Diagnosis of Hypertension Right Anthony J. Viera, MD, MPH, FAHA Professor and Chair Objectives Review limitations of office BP in making a correct diagnosis of hypertension
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Blood Pressure Monitoring in Chronic Kidney Disease
 Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
Hypertension and the SPRINT Trial: Is Lower Better
 Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension Guidelines 2017
 Hypertension Guidelines 2017 (American College of Cardiology and the American Heart Association) In 1977, the 1st comprehensive guideline for detection, evaluation, and management of high BP was published,
Hypertension Guidelines 2017 (American College of Cardiology and the American Heart Association) In 1977, the 1st comprehensive guideline for detection, evaluation, and management of high BP was published,
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
RESISTANT HYPERTENSION
 RESISTANT HYPERTENSION John D. Bisognano, MD PhD Professor of Medicine / Cardiology President-Elect, American Society of Hypertension Director, Outpatient Cardiology University of Rochester RESISTANT HYPERTENSION
RESISTANT HYPERTENSION John D. Bisognano, MD PhD Professor of Medicine / Cardiology President-Elect, American Society of Hypertension Director, Outpatient Cardiology University of Rochester RESISTANT HYPERTENSION
AGING, BLOOD PRESSURE & CARDIOVASCULAR DISEASE EVENT RISK. Michael Smolensky, Ph.D. The University of Texas Austin & Houston
 AGING, BLOOD PRESSURE & CARDIOVASCULAR DISEASE EVENT RISK Michael Smolensky, Ph.D. The University of Texas Austin & Houston Disclosures Partner: Circadian Ambulatory Diagnostics Consultant: Spot On Sciences
AGING, BLOOD PRESSURE & CARDIOVASCULAR DISEASE EVENT RISK Michael Smolensky, Ph.D. The University of Texas Austin & Houston Disclosures Partner: Circadian Ambulatory Diagnostics Consultant: Spot On Sciences
University of Padova, Padua, Italy, and HARVEST Study Group, Italy
 University of Padova, Padua, Italy, and HARVEST Study Group, Italy ISOLATED SYSTOLIC HYPERTENSION IN THE YOUNG DOES NOT IMPLY AN INCREASED RISK OF FUTURE HYPERTENSION NEEDING TREATMENT Mos L, Saladini
University of Padova, Padua, Italy, and HARVEST Study Group, Italy ISOLATED SYSTOLIC HYPERTENSION IN THE YOUNG DOES NOT IMPLY AN INCREASED RISK OF FUTURE HYPERTENSION NEEDING TREATMENT Mos L, Saladini
How do we diagnose hypertension today? Presentation Subtitle
 How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
KDIGO Controversies Conference on Blood Pressure in CKD
 KDIGO Controversies Conference on Blood Pressure in CKD September 7-10, 2017 Edinburgh, Scotland Kidney Disease: Improving Global Outcomes (KDIGO) is an international organization whose mission is to improve
KDIGO Controversies Conference on Blood Pressure in CKD September 7-10, 2017 Edinburgh, Scotland Kidney Disease: Improving Global Outcomes (KDIGO) is an international organization whose mission is to improve
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Supplement materials:
 Supplement materials: Table S1: ICD-9 codes used to define prevalent comorbid conditions and incident conditions Comorbid condition ICD-9 code Hypertension 401-405 Diabetes mellitus 250.x Myocardial infarction
Supplement materials: Table S1: ICD-9 codes used to define prevalent comorbid conditions and incident conditions Comorbid condition ICD-9 code Hypertension 401-405 Diabetes mellitus 250.x Myocardial infarction
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
surtout qui n est PAS à risque?
 3*25 min et surtout qui n est PAS à risque? 2018 ESC/ESH Hypertension Guidelines 2018 ESC-ESH Guidelines for the Management of Arterial Hypertension 28 th ESH Meeting on Hypertension and Cardiovascular
3*25 min et surtout qui n est PAS à risque? 2018 ESC/ESH Hypertension Guidelines 2018 ESC-ESH Guidelines for the Management of Arterial Hypertension 28 th ESH Meeting on Hypertension and Cardiovascular
Retour sur le congrès de l AHA 2017
 Retour sur le congrès de l AHA 2017 Paul Poirier MD, PhD, FRCPC, FACC, FAHA, FCCS Professeur Faculté de pharmacie Université Laval Responsable du programme de prévention/réadaptation cardiaque Canagliflozin
Retour sur le congrès de l AHA 2017 Paul Poirier MD, PhD, FRCPC, FACC, FAHA, FCCS Professeur Faculté de pharmacie Université Laval Responsable du programme de prévention/réadaptation cardiaque Canagliflozin
Blood Pressure Treatment in 2018
 Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Implications of Drug-related Increases in Blood Pressure
 Implications of Drug-related Increases in Blood Pressure Preston M. Dunnmon, MD, FACP, FACC Division of Cardiovascular and Renal Products US Food and Drug Administration July 18, 2012 Disclaimer The findings
Implications of Drug-related Increases in Blood Pressure Preston M. Dunnmon, MD, FACP, FACC Division of Cardiovascular and Renal Products US Food and Drug Administration July 18, 2012 Disclaimer The findings
Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly
 Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly Paul Muntner, PhD MHS Professor and Vice Chair Department of Epidemiology University of Alabama
Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly Paul Muntner, PhD MHS Professor and Vice Chair Department of Epidemiology University of Alabama
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
9/29/2015. Primary Prevention of Heart Disease: Objectives. Objectives. What works? What doesn t?
 Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA
 Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD
 New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
When should blood pressure be lowered? Should treatment be guided by blood pressure values or total cardiovascular risk?
 OF JOURNAL HYPERTENSION JH R RESEARCH Journal of HYPERTENSION RESEARCH www.hypertens.org/jhr Editorial J Hypertens Res (2016) 2(2):47 51 When should blood pressure be lowered? Should treatment be guided
OF JOURNAL HYPERTENSION JH R RESEARCH Journal of HYPERTENSION RESEARCH www.hypertens.org/jhr Editorial J Hypertens Res (2016) 2(2):47 51 When should blood pressure be lowered? Should treatment be guided
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD?
 Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
SESSION 3 11 AM 12:30 PM
 SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
MPharmProgramme. Hypertension (HTN)
") MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
RISE, FALL AND RESURRECTION OF RENAL DENERVATION. Michael A. Weber, MD State University of New York Downstate College of Medicine
 RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
Blood Pressure Measurement in SPRINT
 Blood Pressure Measurement in SPRINT Karen C. Johnson, MD, MPH, FAHA Vice Chair, SPRINT Steering Committee University of Tennessee Health Science Center, Department of Preventive Medicine For the SPRINT
Blood Pressure Measurement in SPRINT Karen C. Johnson, MD, MPH, FAHA Vice Chair, SPRINT Steering Committee University of Tennessee Health Science Center, Department of Preventive Medicine For the SPRINT
Is Traditional Clinic Blood Pressure Dead?
 Royal College of Physicans May 16 th 2017 Is Traditional Clinic Blood Pressure Dead? Professor Bryan Williams MD FRCP FAHA FESC Chair of Medicine UCL Director National Institute for Health Research Biomedical
Royal College of Physicans May 16 th 2017 Is Traditional Clinic Blood Pressure Dead? Professor Bryan Williams MD FRCP FAHA FESC Chair of Medicine UCL Director National Institute for Health Research Biomedical
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Dr Chris Ellis. Consultant Cardiologist Auckland
 Dr Chris Ellis Consultant Cardiologist Auckland CVD Risk Prevention in NZ 2013 & Beyond: The Clinicians View Dr Chris Ellis Cardiologist Green Lane CVS Service, Cardiology Department, Auckland City Hospital
Dr Chris Ellis Consultant Cardiologist Auckland CVD Risk Prevention in NZ 2013 & Beyond: The Clinicians View Dr Chris Ellis Cardiologist Green Lane CVS Service, Cardiology Department, Auckland City Hospital
Protecting the heart and kidney: implications from the SHARP trial
 Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Do Women Benefit From Statins for Primary Prevention?: Controversy, Challenges and Consensus
 Do Women Benefit From Statins for Primary Prevention?: Controversy, Challenges and Consensus C. Noel Bairey Merz MD, FACC, FAHA Professor and Women s Guild Endowed Chair Director, Barbra Streisand Women
Do Women Benefit From Statins for Primary Prevention?: Controversy, Challenges and Consensus C. Noel Bairey Merz MD, FACC, FAHA Professor and Women s Guild Endowed Chair Director, Barbra Streisand Women
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center
 Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
J-curve Revisited. An Analysis of Blood Pressure and Cardiovascular Events in the Treating to New Targets (TNT) Trial
 Trial") J-curve Revisited An Analysis of Blood Pressure and Cardiovascular Events in the Treating to New Targets (TNT) Trial Sripal Bangalore, MD, MHA, Franz H Messerli, MD, Chuan-Chuan Wun, PhD, Andrea L. Zuckerman,
J-curve Revisited An Analysis of Blood Pressure and Cardiovascular Events in the Treating to New Targets (TNT) Trial Sripal Bangalore, MD, MHA, Franz H Messerli, MD, Chuan-Chuan Wun, PhD, Andrea L. Zuckerman,
Blood pressure treatment target in diabetes. Should it be <130 mmhg?
 Blood pressure treatment target in diabetes Should it be
Blood pressure treatment target in diabetes Should it be
Stroke secondary prevention. Gill Cluckie Stroke Nurse Consultant St. George s Hospital
 Stroke secondary prevention Gill Cluckie Stroke Nurse Consultant St. George s Hospital Stroke recurrence The risk of recurrent stroke is greatest after first stroke 2 3% of survivors of a first stroke
Stroke secondary prevention Gill Cluckie Stroke Nurse Consultant St. George s Hospital Stroke recurrence The risk of recurrent stroke is greatest after first stroke 2 3% of survivors of a first stroke
Central pressures and prediction of cardiovascular events in erectile dysfunction patients
 Central pressures and prediction of cardiovascular events in erectile dysfunction patients N. Ioakeimidis, K. Rokkas, A. Angelis, Z. Kratiras, M. Abdelrasoul, C. Georgakopoulos, D. Terentes-Printzios,
Central pressures and prediction of cardiovascular events in erectile dysfunction patients N. Ioakeimidis, K. Rokkas, A. Angelis, Z. Kratiras, M. Abdelrasoul, C. Georgakopoulos, D. Terentes-Printzios,
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Controlling Hypertension in Primary Care: Hitting a moving target?
 Controlling Hypertension in Primary Care: Hitting a moving target? David J. Hyman, MD,MPH Professor of Medicine and Family & Community Medicine Chief, Section General Medicine Baylor College of Medicine
Controlling Hypertension in Primary Care: Hitting a moving target? David J. Hyman, MD,MPH Professor of Medicine and Family & Community Medicine Chief, Section General Medicine Baylor College of Medicine
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu Indicator area: Pulse rhythm assessment for AF Indicator: NM146 Date: June 2017 Introduction There is evidence
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu Indicator area: Pulse rhythm assessment for AF Indicator: NM146 Date: June 2017 Introduction There is evidence
Landmesser U et al. Eur Heart J 2017; https://doi.org/ /eurheartj/ehx549
 2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
SPRINT trial: quoi de neuf en hypertension? Approche pratique du patient cardiaque en médecine. générale
 SPRINT trial: quoi de neuf en hypertension? Approche pratique du patient cardiaque en médecine 17 ème édition du Congrès de la Ligue Cardiologique Belge 21 mai 2016 générale Philippe van de Borne Service
SPRINT trial: quoi de neuf en hypertension? Approche pratique du patient cardiaque en médecine 17 ème édition du Congrès de la Ligue Cardiologique Belge 21 mai 2016 générale Philippe van de Borne Service
Acute Medical Management. Bogachan Sahin, M.D., Ph.D. Department of Neurology
 Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
LDL Cholesterol Lowering with Evolocumab and Outcomes in Patients with Peripheral Artery Disease: Insights from the FOURIER Trial
 LDL Cholesterol Lowering with Evolocumab and Outcomes in Patients with Peripheral Artery Disease: Insights from the FOURIER Trial Marc P. Bonaca, Patrice Nault, Robert P. Giugliano, Anthony C. Keech, Armando
LDL Cholesterol Lowering with Evolocumab and Outcomes in Patients with Peripheral Artery Disease: Insights from the FOURIER Trial Marc P. Bonaca, Patrice Nault, Robert P. Giugliano, Anthony C. Keech, Armando
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future
 ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies