CRT Vs RV Pacing Benefits
|
|
|
- Spencer Cole
- 5 years ago
- Views:
Transcription

1 CRT-P & CRT-D Indications According to Guidelines are Guidelines Fully Adopted? Salama H. Omar M.D. Prof. Critical Care Medicine, Cairo University CRT Vs RV Pacing Benefits 1


2 Benefit of Upgrade CTR-P & CRT-D Benefits 2
3 Eligible Patients Treated 10/27/2013 Relative Cost of CRT Cost per patient Total Annual Expenditures Dialysis CABG PTCA Hip/knee replace CRT CRT+ICD $60 $40 $20 $ thousands $0 $0 $5 $10 $15 $20 $ Billions Doug Smith: Results: Improvement in Quality Measures at 24 Months (Patient Level Analysis) 100% 80% 60% 40% Significant Improvement in 6 of 7 Quality Measures at 12 and 24 Months Pre-specified Primary Objective Met: Relative Improvement 20% in 3 Quality Measures * * 87% 84% 80% 86% * * 93% 94% 34% * 51% * 62% 69% 69% 69% 69% 38% * 58% * 49% * 71% * 79% 62% * * 71% 69% 20% 0% ACEI/ARB ß-blocker Aldosterone Antagonist Anticoagulant for AF Baseline 12 months 24 months CRT ICD HF Education * P<0.001 vs. baseline P-values are for relative change Fonarow GC, et al. Circulation. 2010;122:
4 Guidelines 4


5 Indications for cardiac resynchronization therapy in patients in sinus rhythm 5

6 6

7 Upgrade..?? PM Indication..?? 7

8 Atrial Fibrillation..?? 8

9 A. Fib. 9

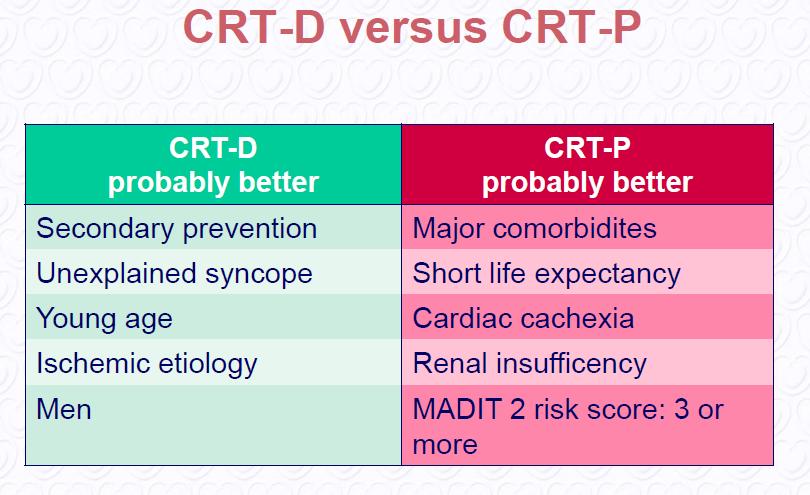
10 CRT-P Vs CRT-D 10
 already is being provided.")
 accompanied by sinus")
11 Recommendations for CRT in Patients with Systolic Heart Failure (AHA) Changes in the recommendations: All recommendations for the 2008 Guidelines and 2012 Update are predicated on the expectation that appropriate medical therapy guideline-directed medical therapy (GDMT) already is being provided. the discussion below assumes that GDMT is being provided Update provides both expansion and limitation of the indications for CRT. Previously, the only Class I recommendation for CRT was in patients with relatively severe symptoms (NYHA Functional Class III or IV heart failure) accompanied by sinus rhythm, left ventricular ejection fraction (LVEF) 35%, a QRS duration 0.12 second. 11
12 Changes in the recommendations: Since publication of the 2008 Guideline, REVERSE, MADIT-CRT, and RAFT have allowed for the refinements, (based on their inclusion criteria) that provide data for CRT use in patients with less severe symptoms. Class I 1. CRT is indicated for patients who have LVEF less than or equal to 35%, sinus rhythm, LBBB with a QRS duration greater than or equal to 150 ms, and NYHA class II, III, or ambulatory IV symptoms on GDMT. (Level of Evidence: A for NYHA class III/IV; Level of Evidence: B for NYHA class II) Modified recommendation (specifying CRT in patients with LBBB of 150 ms; expanded to include those with NYHA class II symptoms). 12
13 Rationale for the changes These large randomized studies, along with meta-analyses, have also tempered enthusiasm for CRT in patients with QRS less than 150 msec based on failure to respond to CRT for all functional NYHA classes. Furthermore, studies published in 2009 and 2010, and a meta-analysis from 2011, demonstrated that non-lbbb conduction abnormalities are associated with failure to benefit from CRT. The jury may still be out on this issue, since there are some data to suggest that patients with non-lbbb can benefit from CRT when the QRS is markedly prolonged; as such, these patients still are included in recommendation Class II Class IIa 1. CRT can be useful for patients who have LVEF less than or equal to 35%, sinus rhythm, LBBB with a QRS duration 120 to 149 ms, and NYHA class II, III, or ambulatory IV symptoms on GDMT. (Level of Evidence: B) New recommendation 2. CRT can be useful for patients who have LVEF less than or equal to 35%, sinus rhythm, a non-lbbb pattern with a QRS duration greater than or equal to 150 ms, and NYHA class III/ambulatory class IV symptoms on GDMT. (Level of Evidence: A) New recommendation 13
14 Class IIa 3. CRT can be useful in patients with atrial fibrillation and LVEF less than or equal to 35% on GDMT if a) the patient requires ventricular pacing or otherwise meets CRT criteria and b) AV nodal ablation or pharmacologic rate control will allow near 100% ventricular pacing with CRT. (Level of Evidence: B) Modified recommendation (wording changed to indicate benefit based on ejection fraction rather than NYHA class; level of evidence changed from C to B). 4. CRT can be useful for patients on GDMT who have LVEF less than or equal to 35% and are undergoing new or replacement device placement with anticipated requirement for significant (40%) ventricular pacing. (Level of Evidence: C) Modified recommendation (wording changed to indicate benefit based on ejection fraction and need for pacing rather than NYHA class); class changed from IIb to IIa. Class IIb 1. CRT may be considered for patients who have LVEF less than or equal to 30%, ischemic etiology of heart failure, sinus rhythm, LBBB with a QRS duration of greater than or equal to 150 ms, and NYHA class I symptoms on GDMT. (Level of Evidence: C) New recommendation 2. CRT may be considered for patients who have LVEF less than or equal to 35%, sinus rhythm, a non-lbbb pattern with QRS duration 120 to 149 ms, and NYHA class III/ambulatory class IV on GDMT. (Level of Evidence: B) New recommendation 3. CRT may be considered for patients who have LVEF less than or equal to 35%, sinus rhythm, a non-lbbb pattern with a QRS duration greater than or equal to 150 ms, and NYHA class II symptoms on GDMT. (Level of Evidence: B) New recommendation 14
15 Class III: No Benefit 1. CRT is not recommended for patients with NYHA class I or II symptoms and non-lbbb pattern with QRS duration less than 150 ms. (Level of Evidence: B) New recommendation 2. CRT is not indicated for patients whose comorbidities and/or frailty limit survival with good functional capacity to less than 1 year. (Level of Evidence: C) Modified recommendation (wording changed to include cardiac as well as noncardiac comorbidities). The new 2013 ACCF/AHA Guideline AICD (ICD) guidelines have not changed in the 2013 guidelines and include Class I recommendations for primary prevention of sudden cardiac death in selected patients with LVEF 35% and NYHA Class II or III symptoms, who have reasonable expectation of meaningful survival for more than 1 year. 15

16 Real World 16




17 17

18 18
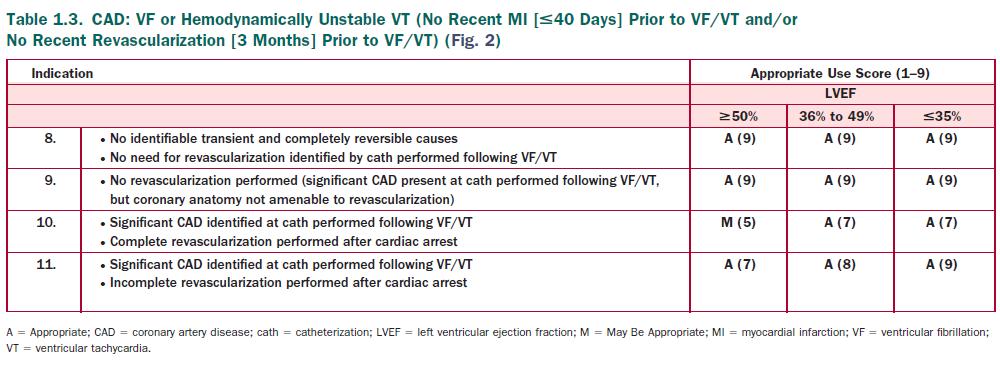
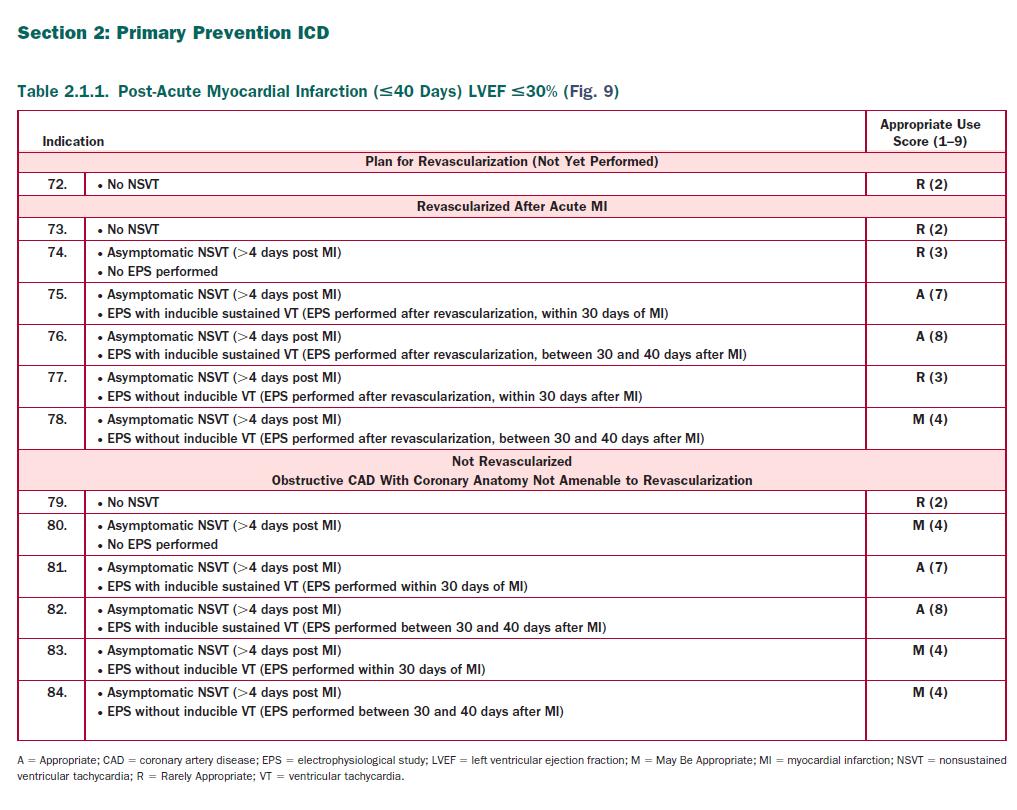
19 How to standardize? Clinical Experience.? Guidelines? There will always be groups of patients for whom guidelines are not strictly applicable AUC..? Give a range of decisions Appropriate Use Criteria for ICD/CRT 19
, May Be Appropriate (median 4 to 6), and Rarely Appropriate (median 1")
20 AUC The 369 Clinical Scenario (Indications) in this document were developed by a multidisciplinary writing group and scored by a separate independent technical panel A Score of1 to 9 is used to designate care: Appropriate (median 7 to 9), May Be Appropriate (median 4 to 6), and Rarely Appropriate (median 1 to 3). 20

21 21
22 22


23 Appropriate Use Criteria for ICD/CRT 23
24 Appropriate Use Criteria for ICD/CRT Algorithms 24
25 25
26 26
27 27
28 28
29 29
30 Conclusion 30

31 31

32 CRT.Who Responds Better..? Conclusion The Appropriate Use Criteria for ICD/CRT have the potential to enhance physician decision making, healthcare delivery, and reimbursement policy. Furthermore, recognition of clinical scenarios rated as May Be Appropriate facilitates the identification of areas that would benefit from future research. 32

33 Parachutes Appear to Reduce the Risk of Injury & mortality, Is This Supported by Randomized Controlled Trials (RCT) Conclusion Exactly as they are named guidelines. These documents synthesize the data that are available and provide recommendations to the clinician for consideration in each individual patient. There will always be groups of patients for whom guidelines are not strictly applicable. Unfortunately, at times placement of CIEDs in situations not covered by the document or contrary to the guidelines, but appropriate for the individual patient, may risk failure of reimbursement or even litigation. 33
34 Conclusion In situations where the guidelines do not apply to real world patients, it is hoped that appropriate use criteria (AUC) methodology will further guide therapy. This methodology, currently being applied to ICD and CRT therapy will examine a large number of indications or scenarios where the guidelines might not strictly apply, and provide the practitioner with levels of appropriateness based on the scale of 1 through 9. The AUC document, in combination with this current focused update, will provide the best guidance to date for application of CIED therapy. MADIT-CRT LIFR Early intervention with CRT-D in patients with mild HF symptoms is associated with sustained clinical abnsd Echocardiographic benefits during an extended perind of follow up of at least 6 years The long term benefit of CRT in this population appears to be restricted to patients with LBBB 34
35 Changes in the recommendations: Since publication of the 2008 Guideline, REVERSE, MADIT-CRT, and RAFT have allowed for the refinements, (based on their inclusion criteria) that provide data for CRT use in patients with less severe symptoms. So, 2012 update, this Class I indication is expanded to patients with NYHA Class II, extending the clear message that CRT is indicated for a population with milder symptoms. It limits, or refines, this single Class I recommendation by confining it only to patients with left bundle branch block (LBBB) and QRS 150 msec. Class IIa: The patients with LBBB, but QRS duration only msec and those with non-lbbb pattern and QRS 150 msec now receive a Class IIa recommendation. 35
36 Class IIa: In Patients with atrial fibrillation with a pacing indication and LVEF 35% if rate control allows near 100% ventricular pacing; this recommendation no longer specifies functional symptom class. In addition, there is now a IIa recommendation (as opposed to IIb) for patients with LVEF 35% who are anticipated to require ventricular pacing greater than 40% of the time. Class IIb: There are also Three other new IIb recommendations: A) for patients with LVEF 35%, a non-lbbb pattern with QRS duration msec and NYHA Class III/ functional Class IV; and, B) for patients with LVEF 35%, in sinus rhythm with non- LBBB pattern but QRS 150 msec and NYHA Class II symptoms (again expanding the option of guideline-based CRT in patients with relatively modest symptoms). A further major expansion of the indication for CRT, for the first time ever in patients with NYHA Class I symptoms, This is limited to patients with relatively severe cardiomyopathy (LVEF 30%) due to ischemia, LBBB, and QRS duration 150 msec, but expands the option of CRT to patients who previously would not have been considered candidates. 36
37 Class III The Class III recommendations, where CRT is not recommended, are reserved for patients with: 1) NYHA Class I or II symptoms, non-lbbb pattern and QRS <150 msec; in addition, 2) patients in whom cardiac or non-cardiac comorbidity and/or frailty limit survival with good functional capacity to less than 1 year. Where Do We Go From Here? With the publication of the 2012 focused update, CRT has truly come of age. Even though CRT is generally appreciated to increase the risk of complications, prolong procedural time and increase cost, in comparison to single or dual chamber ICD therapy, wellconducted randomized trials irrefutably demonstrate benefit in well-defined patient groups. The cardiovascular and clinical cardiac electrophysiology community should be congratulated for the generation of important data that provide for evidence-based recommendations for CRT. Of course, as soon as this Focused Update is published, new data will be available, and future Updates or full Guidelines will follow along with further refinement. 37
38 The new 2013 ACCF/AHA Guideline for the Management of Heart Failure Of note, for patients with non-lbbb and QRS msec, the indication is not expanded beyond patients with NYHA Class III/ ambulatory Class IV; and, to the contrary, CRT for patients in this group with NYHA Class II symptoms is not recommended. Changes in the recommendations: The patients with LBBB but QRS duration only 120 to 149 msec and those with non-lbbb pattern and QRS 150 msec, included in Class I in 2008, now receive a Class IIa recommendation. Of note, the former group (LBBB with QRS 120 to 149 msec) is now extended to patients with NHYA Class II (in addition to Class III/ambulatory Class IV). 38
ESC Guidelines. ESC Guidelines Update For internal training purpose. European Heart Journal, doi: /eurheart/ehn309
 ESC Guidelines Update 2008 ESC Guidelines Heart failure update 2008 For internal training purpose. 0 Agenda Introduction Classes of recommendations Level of evidence Treatment algorithm Changes to ESC
ESC Guidelines Update 2008 ESC Guidelines Heart failure update 2008 For internal training purpose. 0 Agenda Introduction Classes of recommendations Level of evidence Treatment algorithm Changes to ESC
Name of Policy: Bi-Ventricular Pacemakers (Cardiac Resynchronization Therapy) for the Treatment of Heart Failure
 for the Treatment of Heart Failure") Name of Policy: Bi-Ventricular Pacemakers (Cardiac Resynchronization Therapy) for the Treatment of Heart Failure Policy #: 055 Latest Review Date: April 2014 Category: Surgery Policy Grade: A Background/Definitions:
Name of Policy: Bi-Ventricular Pacemakers (Cardiac Resynchronization Therapy) for the Treatment of Heart Failure Policy #: 055 Latest Review Date: April 2014 Category: Surgery Policy Grade: A Background/Definitions:
Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides
 Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides Colette Seifer MB(Hons) FRCP(UK) Associate Professor, University of Manitoba, Cardiologist, Cardiac Sciences Program, St Boniface Hospital
Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides Colette Seifer MB(Hons) FRCP(UK) Associate Professor, University of Manitoba, Cardiologist, Cardiac Sciences Program, St Boniface Hospital
Biventricular Pacemakers (Cardiac Resynchronization Therapy) for the Treatment of Heart Failure
 for the Treatment of Heart Failure") Last Review Status/Date: June 2015 Page: 1 of 29 Resynchronization Therapy) for the Treatment Description Cardiac resynchronization therapy (CRT), which consists of synchronized pacing of the left and
Last Review Status/Date: June 2015 Page: 1 of 29 Resynchronization Therapy) for the Treatment Description Cardiac resynchronization therapy (CRT), which consists of synchronized pacing of the left and
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
Dialysis-Dependent Cardiomyopathy Patients Demonstrate Poor Survival Despite Reverse Remodeling With Cardiac Resynchronization Therapy
 Dialysis-Dependent Cardiomyopathy Patients Demonstrate Poor Survival Despite Reverse Remodeling With Cardiac Resynchronization Therapy Evan Adelstein, MD, FHRS John Gorcsan III, MD Samir Saba, MD, FHRS
Dialysis-Dependent Cardiomyopathy Patients Demonstrate Poor Survival Despite Reverse Remodeling With Cardiac Resynchronization Therapy Evan Adelstein, MD, FHRS John Gorcsan III, MD Samir Saba, MD, FHRS
Large RCT s of CRT 2002 to present
 Have We Expanded Our Use of CRT for Heart Failure Patients? Sana M. Al-Khatib, MD, MHS Associate Professor of Medicine Electrophysiology Section- Division of Cardiology Duke University Potential Conflicts
Have We Expanded Our Use of CRT for Heart Failure Patients? Sana M. Al-Khatib, MD, MHS Associate Professor of Medicine Electrophysiology Section- Division of Cardiology Duke University Potential Conflicts
Comparison of clinical trials evaluating cardiac resynchronization therapy in mild to moderate heart failure
 HOT TOPIC Cardiology Journal 2010, Vol. 17, No. 6, pp. 543 548 Copyright 2010 Via Medica ISSN 1897 5593 Comparison of clinical trials evaluating cardiac resynchronization therapy in mild to moderate heart
HOT TOPIC Cardiology Journal 2010, Vol. 17, No. 6, pp. 543 548 Copyright 2010 Via Medica ISSN 1897 5593 Comparison of clinical trials evaluating cardiac resynchronization therapy in mild to moderate heart
Biventricular Pacemakers (Cardiac Resynchronization Therapy) for the Treatment of Heart Failure
 for the Treatment of Heart Failure") Last Review Status/Date: September 2016 Page: 1 of 29 Resynchronization Therapy) for the Treatment Description Cardiac resynchronization therapy (CRT), which consists of synchronized pacing of the left
Last Review Status/Date: September 2016 Page: 1 of 29 Resynchronization Therapy) for the Treatment Description Cardiac resynchronization therapy (CRT), which consists of synchronized pacing of the left
All in the Past? Win K. Shen, MD Mayo Clinic Arizona Controversies and Advances in CV Diseases Cedars-Sinai Heart Institute, MFMER
 ICD for NICM All in the Past? Win K. Shen, MD Mayo Clinic Arizona Controversies and Advances in CV Diseases Cedars-Sinai Heart Institute, 2017 2017 MFMER 3686275-1 DISCLOSURE Relevant Financial Relationship(s)
ICD for NICM All in the Past? Win K. Shen, MD Mayo Clinic Arizona Controversies and Advances in CV Diseases Cedars-Sinai Heart Institute, 2017 2017 MFMER 3686275-1 DISCLOSURE Relevant Financial Relationship(s)
Gender and cardiac resynchronization therapy. Chairs: David Heaven & Belinda Green. Gender and Cardiac Resynchronisation Therapy
 Electrophysiology Gender and cardiac resynchronization therapy Dean Boddington Chairs: David Heaven & Belinda Green Gender and Cardiac Resynchronisation Therapy Dean Boddington Tauranga Hospital 1 Disclosure/Warning
Electrophysiology Gender and cardiac resynchronization therapy Dean Boddington Chairs: David Heaven & Belinda Green Gender and Cardiac Resynchronisation Therapy Dean Boddington Tauranga Hospital 1 Disclosure/Warning
Nonischemic cardiomyopathy, LVEF 31-35%, no prior implant, SR for ANY of the following:
 Cigna Medical Coverage Policy Subject Biventricular Pacing/Cardiac Resynchronization Therapy (CRT) Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 17 References...
Cigna Medical Coverage Policy Subject Biventricular Pacing/Cardiac Resynchronization Therapy (CRT) Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 17 References...
BSH Annual Autumn Meeting 2017
 BSH Annual Autumn Meeting 2017 Presentation title: The Development of CRT Speaker: John GF Cleland Conflicts of interest: I have received research support and honoraria from Biotronik, Boston Scientific,
BSH Annual Autumn Meeting 2017 Presentation title: The Development of CRT Speaker: John GF Cleland Conflicts of interest: I have received research support and honoraria from Biotronik, Boston Scientific,
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Cardiac Resynchronization ICD Therapy: What is New?
 Cardiac Resynchronization ICD Therapy: What is New? Emile Daoud, MD Section Chief, Cardiac Electrophysiology Professor of Medicine The Ohio State University Normal Activation, Narrow QRS Synchrony Abnormal
Cardiac Resynchronization ICD Therapy: What is New? Emile Daoud, MD Section Chief, Cardiac Electrophysiology Professor of Medicine The Ohio State University Normal Activation, Narrow QRS Synchrony Abnormal
Thoranis Chantrarat MD
 Device Therapy in Heart Failure Thoranis Chantrarat MD 1 Scope of presentation Natural history of heart failure Primary and secondary prevention ICD and its indication CRT and its indication 2 Severity
Device Therapy in Heart Failure Thoranis Chantrarat MD 1 Scope of presentation Natural history of heart failure Primary and secondary prevention ICD and its indication CRT and its indication 2 Severity
Online Appendix (JACC )
") Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
Heart Failure Management. Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist
 Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure
 New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure Deborah Budge, MD Intermountain Healthcare Heart Failure Cardiologist Objectives: State the updates from the ACC 2013 HF
New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure Deborah Budge, MD Intermountain Healthcare Heart Failure Cardiologist Objectives: State the updates from the ACC 2013 HF
BIVENTRICULAR PACEMAKER (CARDIAC RESYNCHRONIZATION THERAPY) FOR THE TREATMENT OF HEART FAILURE
 FOR THE TREATMENT OF HEART FAILURE") FOR THE TREATMENT OF HEART FAILURE Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices
FOR THE TREATMENT OF HEART FAILURE Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices
Provocative Cases: Issues in the Expanding Use of CRT in Treating CHF Patients
 Provocative Cases: Issues in the Expanding Use of CRT in Treating CHF Patients David E. Krummen, MD Associate Professor of Medicine University of California San Diego and VA San Diego Healthcare System
Provocative Cases: Issues in the Expanding Use of CRT in Treating CHF Patients David E. Krummen, MD Associate Professor of Medicine University of California San Diego and VA San Diego Healthcare System
Pattarapong Makarawate MD, FHRS Assistant Professor. Division Of Cardiology Faculty of Medicine, Khon Kaen University
 Pattarapong Makarawate MD, FHRS Assistant Professor. Division Of Cardiology Faculty of Medicine, Khon Kaen University 1. Important and impact of ICD in primary prevention 2. Risk stratification for ICD
Pattarapong Makarawate MD, FHRS Assistant Professor. Division Of Cardiology Faculty of Medicine, Khon Kaen University 1. Important and impact of ICD in primary prevention 2. Risk stratification for ICD
CRT-P or CRT-D From North Alberta to Nairobi
 CRT-P or CRT-D From North Alberta to Nairobi Dr Mzee Ngunga Aga Khan University Hospital Nairobi KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web:
CRT-P or CRT-D From North Alberta to Nairobi Dr Mzee Ngunga Aga Khan University Hospital Nairobi KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web:
Risk Stratification of Sudden Cardiac Death
 Risk Stratification of Sudden Cardiac Death Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC USA Disclosures: None Sudden Cardiac Death A Major Public Health Problem > 1/2 of
Risk Stratification of Sudden Cardiac Death Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC USA Disclosures: None Sudden Cardiac Death A Major Public Health Problem > 1/2 of
Arthur J. Moss, MD Professor of Medicine/Cardiology University of Rochester Medical Center Rochester, NY. DISCLOSURE INFORMATION Arthur J.
 Saving Lives and Preventing Heart Failure: The MADIT Family of Trials Arthur J. Moss, MD Professor of Medicine/Cardiology University of Rochester Medical Center Rochester, NY Update in Electrocardiography
Saving Lives and Preventing Heart Failure: The MADIT Family of Trials Arthur J. Moss, MD Professor of Medicine/Cardiology University of Rochester Medical Center Rochester, NY Update in Electrocardiography
Do All Patients With An ICD Indication Need A BiV Pacing Device?
 Do All Patients With An ICD Indication Need A BiV Pacing Device? Muhammad A. Hammouda, MD Electrophysiology Laboratory Department of Critical Care Medicine Cairo University Etiology and Pathophysiology
Do All Patients With An ICD Indication Need A BiV Pacing Device? Muhammad A. Hammouda, MD Electrophysiology Laboratory Department of Critical Care Medicine Cairo University Etiology and Pathophysiology
Cardiac Resynchronization Therapy Guidelines and Missing Groups
 Cardiac Resynchronization Therapy Guidelines and Missing Groups Frank Pelosi, Jr., MD, FACC, FHRS Director, Cardiac Electrophysiology Fellowship Associate Professor of Medicine University of Michigan Health
Cardiac Resynchronization Therapy Guidelines and Missing Groups Frank Pelosi, Jr., MD, FACC, FHRS Director, Cardiac Electrophysiology Fellowship Associate Professor of Medicine University of Michigan Health
Resynchronization/Defibrillation
 Resynchronization/Defibrillation for Ambulatory Heart Failure Trial Cardiac Resynchronization Therapy for Mild to Moderate Heart Failure George Wells University of Ottawa Heart Institute Department of
Resynchronization/Defibrillation for Ambulatory Heart Failure Trial Cardiac Resynchronization Therapy for Mild to Moderate Heart Failure George Wells University of Ottawa Heart Institute Department of
Workingman s Guide to CRT Indications: Making Sense of the Various Guidelines
 Workingman s Guide to CRT Indications: Making Sense of the Various Guidelines Andrew E. Epstein, MD Professor of Medicine, Cardiovascular Division University of Pennsylvania Chief, Cardiology Section Philadelphia
Workingman s Guide to CRT Indications: Making Sense of the Various Guidelines Andrew E. Epstein, MD Professor of Medicine, Cardiovascular Division University of Pennsylvania Chief, Cardiology Section Philadelphia
How do I convert my CRT Non Responder into Responder?
 How do I convert my CRT Non Responder into Responder? Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Clinical Trials and Consulting Boston Scientific, Medtronic
How do I convert my CRT Non Responder into Responder? Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Clinical Trials and Consulting Boston Scientific, Medtronic
CRT-D or CRT-P: HOW TO CHOOSE THE RIGHT PATIENT?
 CRT-D or CRT-P: HOW TO CHOOSE THE RIGHT PATIENT? Alessandro Lipari, MD Chair and Department of Cardiology University of Study and Spedali Civili Brescia -Italy The birth of CRT in Europe, 20 years ago
CRT-D or CRT-P: HOW TO CHOOSE THE RIGHT PATIENT? Alessandro Lipari, MD Chair and Department of Cardiology University of Study and Spedali Civili Brescia -Italy The birth of CRT in Europe, 20 years ago
Cardiac resynchronization therapy for heart failure: state of the art
 Cardiac resynchronization therapy for heart failure: state of the art Béla Merkely MD, PhD, DSc, FESC, FACC Vice president of the European Society of Cardiology Honorary president of the Hungarian Society
Cardiac resynchronization therapy for heart failure: state of the art Béla Merkely MD, PhD, DSc, FESC, FACC Vice president of the European Society of Cardiology Honorary president of the Hungarian Society
Effect of Ventricular Pacing on Myocardial Function. Inha University Hospital Sung-Hee Shin
 Effect of Ventricular Pacing on Myocardial Function Inha University Hospital Sung-Hee Shin Contents 1. The effect of right ventricular apical pacing 2. Strategies for physiologically optimal ventricular
Effect of Ventricular Pacing on Myocardial Function Inha University Hospital Sung-Hee Shin Contents 1. The effect of right ventricular apical pacing 2. Strategies for physiologically optimal ventricular
A Square Peg in a Round Hole: CRT IN PAEDIATRICS AND CONGENITAL HEART DISEASE
 A Square Peg in a Round Hole: CRT IN PAEDIATRICS AND CONGENITAL HEART DISEASE Adele Greyling Dora Nginza Hospital, Port Elizabeth SA Heart November 2017 What are the guidelines based on? MADIT-II Size:
A Square Peg in a Round Hole: CRT IN PAEDIATRICS AND CONGENITAL HEART DISEASE Adele Greyling Dora Nginza Hospital, Port Elizabeth SA Heart November 2017 What are the guidelines based on? MADIT-II Size:
2017 AHA/ACC/HRS Ventricular Arrhythmias and Sudden Cardiac Death Guideline. Top Ten Messages. Eleftherios M Kallergis, MD, PhD, FESC
 2017 AHA/ACC/HRS Ventricular Arrhythmias and Sudden Cardiac Death Guideline Top Ten Messages Eleftherios M Kallergis, MD, PhD, FESC Cadiology Department - Heraklion University Hospital No actual or potential
2017 AHA/ACC/HRS Ventricular Arrhythmias and Sudden Cardiac Death Guideline Top Ten Messages Eleftherios M Kallergis, MD, PhD, FESC Cadiology Department - Heraklion University Hospital No actual or potential
Citation. What is New in the 2013 ACC/AHA HF Guideline. Dimensions in Heart and Vascular Care Penn State Heart and Vascular Institute
 What is New in the 2013 ACC/AHA HF Guideline Dimensions in Heart and Vascular Care Penn State Heart and Vascular nstitute Friday October 18, 2013 Barry S. Clemson, MD Associate Professor of Medicine Penn
What is New in the 2013 ACC/AHA HF Guideline Dimensions in Heart and Vascular Care Penn State Heart and Vascular nstitute Friday October 18, 2013 Barry S. Clemson, MD Associate Professor of Medicine Penn
Primary prevention of SCD with the ICD in Nonischemic Cardiomyopathy
 Primary prevention of SCD with the ICD in Nonischemic Cardiomyopathy Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC USA Disclosures: Consulting and Clinical Trials Medtronic
Primary prevention of SCD with the ICD in Nonischemic Cardiomyopathy Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC USA Disclosures: Consulting and Clinical Trials Medtronic
Bi-Ventricular pacing after the most recent studies
 Seminars of the Hellenic Working Groups February 18th-20 20,, 2010, Thessaloniki, Greece Bi-Ventricular pacing after the most recent studies Maurizio Lunati MD Director EP Lab & Unit Cardiology Dpt. Niguarda
Seminars of the Hellenic Working Groups February 18th-20 20,, 2010, Thessaloniki, Greece Bi-Ventricular pacing after the most recent studies Maurizio Lunati MD Director EP Lab & Unit Cardiology Dpt. Niguarda
Upgrade to Resynchronization Therapy. Saeed Oraii MD, Cardiologist Interventional Electrophysiologist Tehran Arrhythmia Clinic May 2016
 Upgrade to Resynchronization Therapy Saeed Oraii MD, Cardiologist Interventional Electrophysiologist Tehran Arrhythmia Clinic May 2016 Event Free Survival (%) CRT Cardiac resynchronization therapy (CRT)
Upgrade to Resynchronization Therapy Saeed Oraii MD, Cardiologist Interventional Electrophysiologist Tehran Arrhythmia Clinic May 2016 Event Free Survival (%) CRT Cardiac resynchronization therapy (CRT)
Heart Failure Overview. Dr Chris K Y Wong
 Heart Failure Overview Dr Chris K Y Wong Heart Failure: A Growing, Global Health Issue Heart Failure 23 Million Afflicted Global Impact Worldwide ~23 million peopleworldwide afflicted with CHF 1 Exceeds
Heart Failure Overview Dr Chris K Y Wong Heart Failure: A Growing, Global Health Issue Heart Failure 23 Million Afflicted Global Impact Worldwide ~23 million peopleworldwide afflicted with CHF 1 Exceeds
The Role of Ventricular Electrical Delay to Predict Left Ventricular Remodeling With Cardiac Resynchronization Therapy
 The Role of Ventricular Electrical Delay to Predict Left Ventricular Remodeling With Cardiac Resynchronization Therapy Results from the SMART-AV Trial Michael R. Gold, MD, PhD, Ulrika Birgersdotter-Green,
The Role of Ventricular Electrical Delay to Predict Left Ventricular Remodeling With Cardiac Resynchronization Therapy Results from the SMART-AV Trial Michael R. Gold, MD, PhD, Ulrika Birgersdotter-Green,
Management Strategies for Advanced Heart Failure
 Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Biventricular Pacemakers (Cardiac Resynchronization Therapy) for the Treatment of Heart Failure
 for the Treatment of Heart Failure") Biventricular Pacemakers (Cardiac Resynchronization Therapy for the Treatment of Heart Failure 2.02.10 Biventricular Pacemakers (Cardiac Resynchronization Therapy for the Treatment of Heart Failure Policy
Biventricular Pacemakers (Cardiac Resynchronization Therapy for the Treatment of Heart Failure 2.02.10 Biventricular Pacemakers (Cardiac Resynchronization Therapy for the Treatment of Heart Failure Policy
Cardiac resynchronisation therapy (biventricular pacing) for the treatment of heart failure
 for the treatment of heart failure") NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal for the treatment of heart failure Final scope Appraisal objective To appraise the clinical and cost effectiveness of cardiac
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal for the treatment of heart failure Final scope Appraisal objective To appraise the clinical and cost effectiveness of cardiac
Heart Failure Overview. Dr Chris K Y Wong
 Heart Failure Overview Dr Chris K Y Wong Heart Failure: A Growing, Global Health Issue Heart Failure 23 Million Afflicted Global Impact Worldwide ~23 million peopleworldwide afflicted with CHF 1 Exceeds
Heart Failure Overview Dr Chris K Y Wong Heart Failure: A Growing, Global Health Issue Heart Failure 23 Million Afflicted Global Impact Worldwide ~23 million peopleworldwide afflicted with CHF 1 Exceeds
Guideline Number: NIA_CG_320 Last Revised Date: July, 2018 Responsible Department: Implementation Date: January 2019 Clinical Operations
 National Imaging Associates, Inc. Clinical guidelines CARDIAC RESYNCHRONIZATION THERAPY (CRT) CPT Codes: 33221, 33224, 33225, 33231 Original Date: February, 2013 Page 1 of 10 Last Review Date: March 2017
National Imaging Associates, Inc. Clinical guidelines CARDIAC RESYNCHRONIZATION THERAPY (CRT) CPT Codes: 33221, 33224, 33225, 33231 Original Date: February, 2013 Page 1 of 10 Last Review Date: March 2017
Response of Right Ventricular Size to Treatment with Cardiac Resynchronization Therapy and the Risk of Ventricular Tachyarrhythmias in MADIT-CRT
 Response of Right Ventricular Size to Treatment with Cardiac Resynchronization Therapy and the Risk of Ventricular Tachyarrhythmias in MADIT-CRT Heart Rhythm Society (May 11, 2012) Colin L. Doyle, BA,*
Response of Right Ventricular Size to Treatment with Cardiac Resynchronization Therapy and the Risk of Ventricular Tachyarrhythmias in MADIT-CRT Heart Rhythm Society (May 11, 2012) Colin L. Doyle, BA,*
Implantable cardioverter-defibrillators and cardiac resynchronization therapy
 Implantable cardioverter-defibrillators and cardiac resynchronization therapy Johannes Holzmeister, MD University Hospital Zurich, Zurich, Switzerland Frontiers of heart failure controversies, ESC - Paris
Implantable cardioverter-defibrillators and cardiac resynchronization therapy Johannes Holzmeister, MD University Hospital Zurich, Zurich, Switzerland Frontiers of heart failure controversies, ESC - Paris
This is What I do to Improve CRT Response for CRT Non-Responders
 This is What I do to Improve CRT Response for CRT Non-Responders Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Steering Committees (unpaid) and Clinical Trials,
This is What I do to Improve CRT Response for CRT Non-Responders Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Steering Committees (unpaid) and Clinical Trials,
SCOMPENSO CARDIACO: IL PUNTO DELLA RICERCA
 Journal Club 19 Marzo 2010 SCOMPENSO CARDIACO: IL PUNTO DELLA RICERCA Alessandro Giordano Prevalence of heart failure by sex and age (NHANES:1999-2004) Circulation 2007 Incidence of heart failure by age
Journal Club 19 Marzo 2010 SCOMPENSO CARDIACO: IL PUNTO DELLA RICERCA Alessandro Giordano Prevalence of heart failure by sex and age (NHANES:1999-2004) Circulation 2007 Incidence of heart failure by age
FINANCIAL DISCLOSURE: No relevant financial relationship exists
 The Value of Guideline Directed Medical Therapy in Heart Failure Steve Dentel RN BSN CPHQ National Director, Field Programs and Integration American Heart Association/American Stroke Association FINANCIAL
The Value of Guideline Directed Medical Therapy in Heart Failure Steve Dentel RN BSN CPHQ National Director, Field Programs and Integration American Heart Association/American Stroke Association FINANCIAL
Rate of Heart failure guideline adherence in a tertiary care center in India after accounting for the therapeutic contraindications.
 Article ID: WMC004618 ISSN 2046-1690 Rate of Heart failure guideline adherence in a tertiary care center in India after accounting for the therapeutic contraindications. Peer review status: No Corresponding
Article ID: WMC004618 ISSN 2046-1690 Rate of Heart failure guideline adherence in a tertiary care center in India after accounting for the therapeutic contraindications. Peer review status: No Corresponding
Heart Failure Therapies State of the Art 2017
 Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
Ενδείξεις αμφικοιλιακής βηματοδότησης. Ποιοι ασθενείς με καρδιακή ανεπάρκεια πρέπει να λάβουν αμφικοιλιακό απινιδωτή;
 Ενδείξεις αμφικοιλιακής βηματοδότησης. Ποιοι ασθενείς με καρδιακή ανεπάρκεια πρέπει να λάβουν αμφικοιλιακό απινιδωτή; Άννα Κωστοπούλου Επιμελήτρια Α Ωνάσειο Καρδιοχειρουργικό Κέντρο Τμήμα Ηλεκτροφυσιολογίας
Ενδείξεις αμφικοιλιακής βηματοδότησης. Ποιοι ασθενείς με καρδιακή ανεπάρκεια πρέπει να λάβουν αμφικοιλιακό απινιδωτή; Άννα Κωστοπούλου Επιμελήτρια Α Ωνάσειο Καρδιοχειρουργικό Κέντρο Τμήμα Ηλεκτροφυσιολογίας
3/17/2014. NCDR-14 ICD Registry WS # 24 Case Scenarios Including Syndromes w/ Risk of Sudden Death. Objectives
 NCDR-14 ICD Registry WS # 24 Case Scenarios Including Syndromes w/ Risk of Sudden Death Denise Pond BSN, RN The following relationships exist related to this presentation: No Disclosures Objectives Discuss
NCDR-14 ICD Registry WS # 24 Case Scenarios Including Syndromes w/ Risk of Sudden Death Denise Pond BSN, RN The following relationships exist related to this presentation: No Disclosures Objectives Discuss
WHAT DO ELECTROPHYSIOLOGISTS WANT TO KNOW FROM ECHOCARDIOGRAPHERS BEFORE, DURING&AFTER CARDIAC RESYNCHRONIZATION THERAPY?
 WHAT DO ELECTROPHYSIOLOGISTS WANT TO KNOW FROM ECHOCARDIOGRAPHERS BEFORE, DURING&AFTER CARDIAC RESYNCHRONIZATION THERAPY? Mary Ong Go, MD, FPCP, FPCC, FACC OUTLINE What is CRT Who needs CRT What does the
WHAT DO ELECTROPHYSIOLOGISTS WANT TO KNOW FROM ECHOCARDIOGRAPHERS BEFORE, DURING&AFTER CARDIAC RESYNCHRONIZATION THERAPY? Mary Ong Go, MD, FPCP, FPCC, FACC OUTLINE What is CRT Who needs CRT What does the
Heart Failure Challenges and Unmet needs
 Heart Failure Challenges and Unmet needs. Angelo Auricchio, MD FESC Director, Cardiac Electrophysiology Programme, Fondazione Cardiocentro Ticino, Lugano, Switzerland Professor of Cardiology, University
Heart Failure Challenges and Unmet needs. Angelo Auricchio, MD FESC Director, Cardiac Electrophysiology Programme, Fondazione Cardiocentro Ticino, Lugano, Switzerland Professor of Cardiology, University
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure
 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
ESC Stockholm Arrhythmias & pacing
 ESC Stockholm 2010 Take Home Messages for Practitioners Arrhythmias & pacing Prof. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Disclosures Small teaching fees from
ESC Stockholm 2010 Take Home Messages for Practitioners Arrhythmias & pacing Prof. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Disclosures Small teaching fees from
Devices and Other Non- Pharmacologic Therapy in CHF. Angel R. Leon, MD FACC Division of Cardiology Emory University School of Medicine
 Devices and Other Non- Pharmacologic Therapy in CHF Angel R. Leon, MD FACC Division of Cardiology Emory University School of Medicine Disclosure None University of Miami vs. OSU Renegade Miami football
Devices and Other Non- Pharmacologic Therapy in CHF Angel R. Leon, MD FACC Division of Cardiology Emory University School of Medicine Disclosure None University of Miami vs. OSU Renegade Miami football
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
Heart Failure Treatments
 Heart Failure Treatments Past & Present www.philippelefevre.com Background Background Chronic heart failure Drugs Mechanical Electrical Background Chronic heart failure Drugs Mechanical Electrical Sudden
Heart Failure Treatments Past & Present www.philippelefevre.com Background Background Chronic heart failure Drugs Mechanical Electrical Background Chronic heart failure Drugs Mechanical Electrical Sudden
It has been shown from meta-analysis of randomized clinical trials that patients with a pre-crt QRS duration (QRSD) >150 ms benefit
 >150 ms benefit") Cardiac Resynchronization Therapy may be detrimental in patients with a Very Wide QRSD > 180 ms (VWQRSD) and Right Bundle Branch Block Morphology: Analysis From the Medicare ICD Registry Varun Sundaram
Cardiac Resynchronization Therapy may be detrimental in patients with a Very Wide QRSD > 180 ms (VWQRSD) and Right Bundle Branch Block Morphology: Analysis From the Medicare ICD Registry Varun Sundaram
Heart Failure Guidelines For your Daily Practice
 Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Cardiac resynchronization therapy: An approach to reducing heart-failure readmissions
 Cardiac resynchronization therapy: An approach to reducing heart-failure readmissions This technique helps the ventricles contract uniformly, easing symptoms and improving quality of life. By Nancy M.
Cardiac resynchronization therapy: An approach to reducing heart-failure readmissions This technique helps the ventricles contract uniformly, easing symptoms and improving quality of life. By Nancy M.
InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions
 InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions The Clinical Revisions provide details of changes to InterQual Clinical Criteria. They do not provide information on changes made to CareEnhance
InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions The Clinical Revisions provide details of changes to InterQual Clinical Criteria. They do not provide information on changes made to CareEnhance
BENEFIT OF CRT IN MILDLY SYMPTOMATIC HEART FAILURE RECENT DATA FROM MADIT-CRT AND RAFT
 BENEFIT OF CRT IN MILDLY SYMPTOMATIC HEART FAILURE RECENT DATA FROM MADIT-CRT AND RAFT Ilan Goldenberg MD Professor of Cardiology Sheba Medical Center and Tel Aviv University, Israel University of Rochester
BENEFIT OF CRT IN MILDLY SYMPTOMATIC HEART FAILURE RECENT DATA FROM MADIT-CRT AND RAFT Ilan Goldenberg MD Professor of Cardiology Sheba Medical Center and Tel Aviv University, Israel University of Rochester
Importance of CRT team for optimization of the results: a European point of view
 Importance of CRT team for optimization of the results: a European point of view Matteo Bertini, MD, PhD Arcispedale S. Anna Azienda Ospedaliero-Universitaria Cona-Ferrara No conflict of interest to declare
Importance of CRT team for optimization of the results: a European point of view Matteo Bertini, MD, PhD Arcispedale S. Anna Azienda Ospedaliero-Universitaria Cona-Ferrara No conflict of interest to declare
Cardiac Resynchronization Therapy for Heart Failure
 Cardiac Resynchronization Therapy for Heart Failure Ventricular Dyssynchrony vs Resynchronization Ventricular Dysynchrony Ventricular Dysynchrony 1 Electrical: Inter- or Intraventricular conduction delays
Cardiac Resynchronization Therapy for Heart Failure Ventricular Dyssynchrony vs Resynchronization Ventricular Dysynchrony Ventricular Dysynchrony 1 Electrical: Inter- or Intraventricular conduction delays
Prior Authorization Review Panel MCO Policy Submission
 Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
Biventricular Pacemakers (Cardiac Resynchronization Therapy) for the Treatment of Heart Failure
 for the Treatment of Heart Failure") Biventricular Pacemakers (Cardiac Resynchronization Therapy) for the Treatment of Heart Failure Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary,
Biventricular Pacemakers (Cardiac Resynchronization Therapy) for the Treatment of Heart Failure Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary,
Managing Atrial Fibrillation in the Heart Failure Patient
 Managing Atrial Fibrillation in the Heart Failure Patient Jonathan S. Steinberg, MD Professor of Medicine (adj) University of Rochester School of Medicine & Dentistry Director, Arrhythmia Institute Valley
Managing Atrial Fibrillation in the Heart Failure Patient Jonathan S. Steinberg, MD Professor of Medicine (adj) University of Rochester School of Medicine & Dentistry Director, Arrhythmia Institute Valley
Guideline-Directed Medical Therapy
 Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
His Bundle Pacing in Bundle Branch Block May 11, 2017
 His Bundle Pacing in Bundle Branch Block May 11, 2017 Gopi Dandamudi, MD FHRS System Medical Director, IUH Cardiac EP Program Director, IUH Atrial Fibrillation Center Assistant Professor of Clinical Medicine
His Bundle Pacing in Bundle Branch Block May 11, 2017 Gopi Dandamudi, MD FHRS System Medical Director, IUH Cardiac EP Program Director, IUH Atrial Fibrillation Center Assistant Professor of Clinical Medicine
علم االنسان ما لم يعلم
 In the name of Allah, the Beneficiate, the Merciful ق ال هللا تعالي: 5 الدى علم بالق لم 4 علم االنسان ما لم يعلم سورة العلق It is He (Allah), Who has taught by the pen He has taught man which he did not
In the name of Allah, the Beneficiate, the Merciful ق ال هللا تعالي: 5 الدى علم بالق لم 4 علم االنسان ما لم يعلم سورة العلق It is He (Allah), Who has taught by the pen He has taught man which he did not
Cardiac Resynchronization Therapy. Michelle Khoo, MD
 Cardiac Resynchronization Therapy Michelle Khoo, MD 10.7.08 HuiKuri HV NEJM 2001 Sudden Death (SD) in Subset Populations HuiKuri HV NEJM 2001 Sudden Death (SD) in Subset Populations SD in Competitive Athletes
Cardiac Resynchronization Therapy Michelle Khoo, MD 10.7.08 HuiKuri HV NEJM 2001 Sudden Death (SD) in Subset Populations HuiKuri HV NEJM 2001 Sudden Death (SD) in Subset Populations SD in Competitive Athletes
USE OF ACCELEROMETER DATA TO EVALUATE PHYSICAL ACTIVITY AS A SURROGATE ENDPOINT IN HEART FAILURE CLINICAL TRIALS. Tracy Bergemann PhD
 USE OF ACCELEROMETER DATA TO EVALUATE PHYSICAL ACTIVITY AS A SURROGATE ENDPOINT IN HEART FAILURE CLINICAL TRIALS Tracy Bergemann PhD Senior Principal Statistician ASA Biopharmaceutical Section Regulatory-Industry
USE OF ACCELEROMETER DATA TO EVALUATE PHYSICAL ACTIVITY AS A SURROGATE ENDPOINT IN HEART FAILURE CLINICAL TRIALS Tracy Bergemann PhD Senior Principal Statistician ASA Biopharmaceutical Section Regulatory-Industry
Heart Failure Update. Bibiana Cujec MD May 2015
 Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Efficacy of beta-blockers in heart failure patients with atrial fibrillation: An individual patient data meta-analysis
 Efficacy of beta-blockers in heart failure patients with atrial fibrillation: An individual patient data meta-analysis Dipak Kotecha, MD PhD on behalf of the Selection of slides presented at the European
Efficacy of beta-blockers in heart failure patients with atrial fibrillation: An individual patient data meta-analysis Dipak Kotecha, MD PhD on behalf of the Selection of slides presented at the European
Live Better Electrically
 1 Live Better Electrically Steven L. Higgins, MD, FHRS Chairman, Dept. of Cardiology Director, Cardiac Electrophysiology Scripps Memorial Hospital, La Jolla San Diego, California 2 Live Better Electrically
1 Live Better Electrically Steven L. Higgins, MD, FHRS Chairman, Dept. of Cardiology Director, Cardiac Electrophysiology Scripps Memorial Hospital, La Jolla San Diego, California 2 Live Better Electrically
Nonpharmacologic Treatment of Ventricular Heart Failure
 Nonpharmacologic Treatment of Ventricular Heart Failure Hong Ryang Kil, MD, PhD Department of Pediatrics, College of Medicine, Chungnam National University 2001 AHA Guideline for CHF - Symptomatic LV dysfunction
Nonpharmacologic Treatment of Ventricular Heart Failure Hong Ryang Kil, MD, PhD Department of Pediatrics, College of Medicine, Chungnam National University 2001 AHA Guideline for CHF - Symptomatic LV dysfunction
CONTAK RENEWAL CLINICAL SUMMARY
 CAUTION: Federal law restricts this device to sale by or on the order of a physician trained or experienced in device implant and follow-up procedures. CLINICAL SUMMARY CONTAK RENEWAL Boston Scientific
CAUTION: Federal law restricts this device to sale by or on the order of a physician trained or experienced in device implant and follow-up procedures. CLINICAL SUMMARY CONTAK RENEWAL Boston Scientific
What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE. Marc Ferrini (Lyon Fr)
") What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE Marc Ferrini (Lyon Fr) Palermo (I) 1 04 2017 Consulting Fees, Honoraria: BAYER PHARMA BOEHRINGER INGELHEIM BRISTOL MEYERS
What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE Marc Ferrini (Lyon Fr) Palermo (I) 1 04 2017 Consulting Fees, Honoraria: BAYER PHARMA BOEHRINGER INGELHEIM BRISTOL MEYERS
What s new in the 2017 heart failure guidelines. Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA
 What s new in the 2017 heart failure guidelines Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA Key points to remember 2017 guidelines recommend using natriuretic peptides as biomarkers to screen for heart
What s new in the 2017 heart failure guidelines Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA Key points to remember 2017 guidelines recommend using natriuretic peptides as biomarkers to screen for heart
Implantation of a CRT-Pacemaker Rather than CRT-Defibrillator is Usually Preferred
 Implantation of a CRT-Pacemaker Rather than CRT-Defibrillator is Usually Preferred Professor John GF Cleland University of Hull Kingston-upon-Hull United Kingdom Conflict of Interest: Funding or Speakers
Implantation of a CRT-Pacemaker Rather than CRT-Defibrillator is Usually Preferred Professor John GF Cleland University of Hull Kingston-upon-Hull United Kingdom Conflict of Interest: Funding or Speakers
Left Ventricular Ejection Fraction >35%
 Controversies in Cardiac Resynchronisation Therapy Left Ventricular Ejection Fraction >35% Professor John GF Cleland University of Hull Kingston-upon-Hull United Kingdom Conflict of Interest: I have received
Controversies in Cardiac Resynchronisation Therapy Left Ventricular Ejection Fraction >35% Professor John GF Cleland University of Hull Kingston-upon-Hull United Kingdom Conflict of Interest: I have received
HF QUALITY MEASURES. Hydralazine/nitrate at discharge: Percent of black heart
 Get With The Guidelines - Heart Failure is the American Heart Association s collaborative quality improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized
Get With The Guidelines - Heart Failure is the American Heart Association s collaborative quality improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
ESC/EHRA. Guidelines on Cardiac Pacing. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece
 ESC/EHRA Guidelines on Cardiac Pacing Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Reasons for European Guidelines? Scientific reasons Cultural and political reasons
ESC/EHRA Guidelines on Cardiac Pacing Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Reasons for European Guidelines? Scientific reasons Cultural and political reasons
Author s response to reviews
 Author s response to reviews Title: Multipoint Pacing versus conventional ICD in Patients with a Narrow QRS complex (MPP Narrow QRS trial): study protocol for a pilot randomized controlled trial Authors:
Author s response to reviews Title: Multipoint Pacing versus conventional ICD in Patients with a Narrow QRS complex (MPP Narrow QRS trial): study protocol for a pilot randomized controlled trial Authors:
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Cardiac resynchronization therapy for mild-to-moderate heart failure
 For reprint orders, please contact reprints@expert-reviews.com Cardiac resynchronization therapy for mild-to-moderate heart failure Expert Rev. Med. Devices 8(3), 313 317 (2011) Haran Burri Electrophysiology
For reprint orders, please contact reprints@expert-reviews.com Cardiac resynchronization therapy for mild-to-moderate heart failure Expert Rev. Med. Devices 8(3), 313 317 (2011) Haran Burri Electrophysiology
Who does not need a primary preventive ICD?
 Who does not need a primary preventive ICD? Hildegard Tanner, Bern Universitätsklinik für Kardiologie Disclosure of potential conflicts of interest Travel grants for educational purposes from: Biosense
Who does not need a primary preventive ICD? Hildegard Tanner, Bern Universitätsklinik für Kardiologie Disclosure of potential conflicts of interest Travel grants for educational purposes from: Biosense
Treatment of Atrial Fibrillation in Heart Failure
 Stockholm, September 1st 2010 Treatment of Atrial Fibrillation in Heart Failure Rhythm control: Which drugs? Stefan H. Hohnloser J.W. Goethe University Frankfurt, Germany Presenter disclosure information:
Stockholm, September 1st 2010 Treatment of Atrial Fibrillation in Heart Failure Rhythm control: Which drugs? Stefan H. Hohnloser J.W. Goethe University Frankfurt, Germany Presenter disclosure information:
Indications for and Prediction of Successful Responses of CRT for Patients with Heart Failure
 Indications for and Prediction of Successful Responses of CRT for Patients with Heart Failure Edmund Keung, MD Clinical Chief, Cardiology Section San Francisco VAMC October 25, 2008 Presentation Outline
Indications for and Prediction of Successful Responses of CRT for Patients with Heart Failure Edmund Keung, MD Clinical Chief, Cardiology Section San Francisco VAMC October 25, 2008 Presentation Outline
First question: Does CRT Work in AF?
 CRT in AF Does it work and when to ablate AF versus AV node Maurizio Gasparini Chief EP and Pacing Unit Humanitas Research Hospital, Rozzano - Milano, Italy First question: Does CRT Work in AF? As any
CRT in AF Does it work and when to ablate AF versus AV node Maurizio Gasparini Chief EP and Pacing Unit Humanitas Research Hospital, Rozzano - Milano, Italy First question: Does CRT Work in AF? As any
Device Therapy for Heart Failure
 Device Therapy for Heart Failure Dr. Shelley Zieroth FRCPC Assistant Professor, Cardiology, University of Manitoba Director of Cardiac Transplant and Heart Failure Clinics St Boniface General Hospital,
Device Therapy for Heart Failure Dr. Shelley Zieroth FRCPC Assistant Professor, Cardiology, University of Manitoba Director of Cardiac Transplant and Heart Failure Clinics St Boniface General Hospital,
A number of large, randomized, clinical trials have demonstrated that patients left ventricular dysfunction (ejection fraction 35%) due to either
 due to either") A number of large, randomized, clinical trials have demonstrated that patients left ventricular dysfunction (ejection fraction 35%) due to either ischemic or non-ischemic cardiomyopathy benefit from ICD
A number of large, randomized, clinical trials have demonstrated that patients left ventricular dysfunction (ejection fraction 35%) due to either ischemic or non-ischemic cardiomyopathy benefit from ICD
*NOTE: When submitting CPT code and 99239, it is recommended the measure be submitted each time the code is submitted for hospital discharge.
 Quality ID #5 (NQF 0081): Heart Failure (HF): Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for Left Ventricular Systolic Dysfunction (LVSD) National Quality
Quality ID #5 (NQF 0081): Heart Failure (HF): Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for Left Ventricular Systolic Dysfunction (LVSD) National Quality