Update on HTN and ABPM. Raj Padwal Division of General Internal Medicine University of Alberta
|
|
|
- Myron Bates
- 5 years ago
- Views:
Transcription

1 Update on HTN and ABPM Raj Padwal Division of General Internal Medicine University of Alberta
2 Disclosures Funding: CIHR, AIHS, HSF, UHF Research Collaboration: Novo Nordisk, CVRx Consulting: Vivus, Medtronic Speaking and other Honoraria: Abbott
3 Outline 1. Understand how to interpret ABPM. 2. Review the pros and cons of different methods to diagnose hypertension. 3. Discuss some current controversies in HTN management.
4 Epidemiology and Significance
5 European Society of Hypertension Classification of Blood Pressure Category Systolic Diastolic Optimal <120 and / or <80 Normal <130 and / or <85 High-Normal and / or Grade 1 (mild hypertension ) and / or Grade 2 (moderate hypertension) and / or Grade 3 (severe hypertension) 180 and / or 110 Isolated Systolic Hypertension (ISH) 140 and <90 The category pertains to the highest risk blood pressure *ISH=Isolated Systolic Hypertension. J Hypertens 2007;25:

6 Hypertension in Canada: Prevalence and Control Overall prevalence is 21% McAlister et al. CMAJ 2011
7 Life time risk of Hypertension in Normotensive Women and Men aged 65 years Risk of Hypertension % Risk of Hypertension % Women 80 Men Years to Follow-up Years to Follow-up JAMA 2002: Framingham data.
8 Diagnosing Hypertension
. 4.")
9 Blood Pressure Assessment: Patient preparation and posture Standardized Preparation: Patient 1. No acute anxiety, stress or pain. 2. No caffeine, smoking or nicotine in the preceding 30 minutes. 3. No use of substances containing adrenergic stimulants such as phenylephrine or pseudoephedrine (may be present in nasal decongestants or ophthalmic drops). 4. Bladder and bowel comfortable. 5. No tight clothing on arm or forearm. 6. Quiet room with comfortable temperature 7. Rest for at least 5 minutes before measurement 8. Patient should stay silent prior and during the procedure.






10 II. Criteria for the diagnosis of hypertension and recommendations for follow-up BP: / Clinic BP ABPM (If available) Home BPM Hypertension visit 3 >160 SBP or >100 DBP <160 / 100 or Hypertension visit 4-5 Diagnosis of HTN ABPM or HBPM Awake BP <135/85 and 24-hour <130/80 Awake BP >135 SBP or >85 DBP or 24-hour >130 SBP or >80 DBP < 135/85 Confirm with repeat Home BPM or ABPM >135/85 >140 SBP or >90 DBP < 140 / 90 Diagnosis of HTN Continue to follow-up Continue to follow-up Diagnosis of HTN Continue to follow-up Diagnosis of HTN Patients with high normal blood pressure (clinic SBP and/or DBP 85-89) should be followed annually.
11 Clinic, Home, Ambulatory (ABP) Blood Pressure Measurement Equivalence Numbers A clinic blood pressure of 140/90 mmhg has a similar risk of a: Description Blood Pressure mmhg Home pressure average 135 / 85 Daytime average ABP 135 / hour average ABP 130 / 80

12 ABPM Indications Chughtai and Peixoto. Hosp Phys 2003
13 Contraindications to ABPM 1. Not cooperative 2. Severe PVD or thrombocytopenia 3. Afib (relative): not accurate 4. Arm too big 5. Severe office HTN ( 220/120)
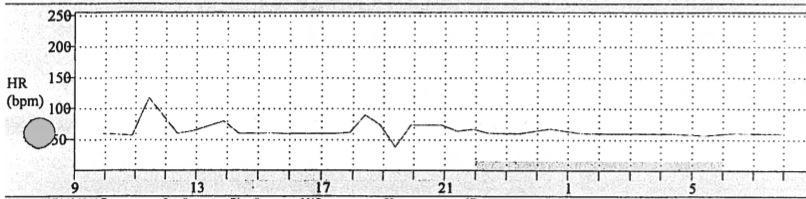
14 ABPM 1
15 ABPM 1
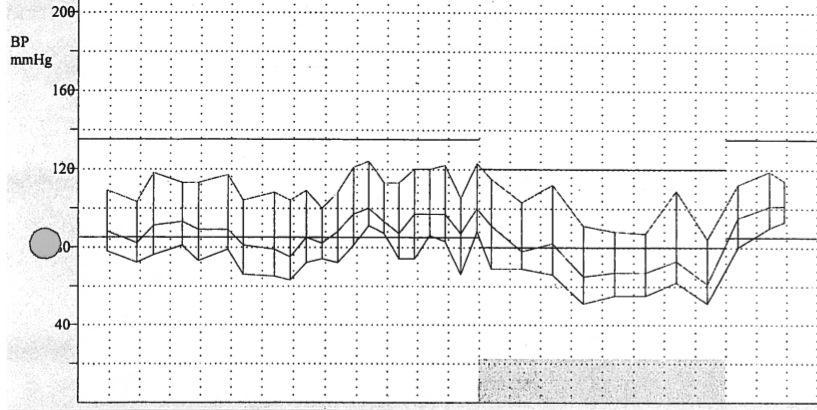
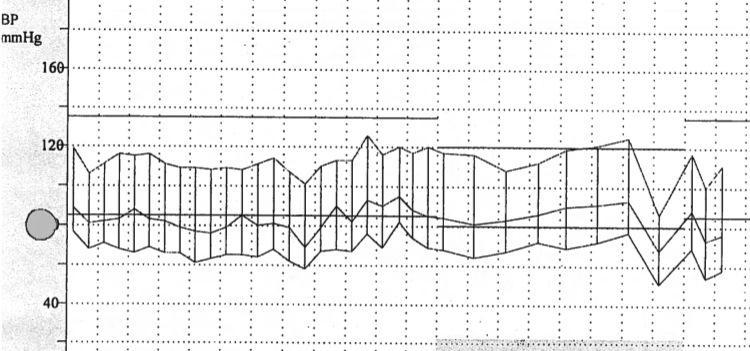
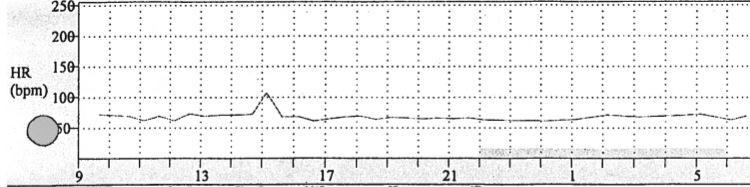
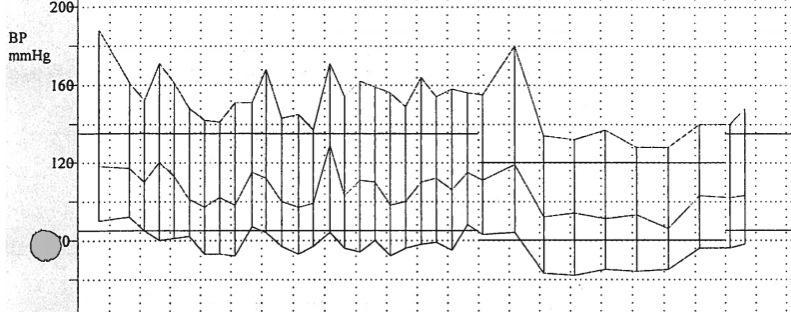
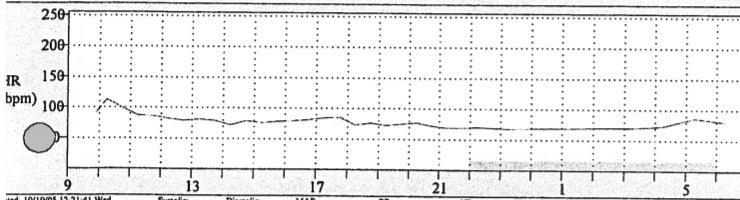
16 Information Provided by ABPM 1. Estimate of true overall 24 hour BP 2. Diurnal variation in BP 3. Variability in BP 4. Duration of action of drug

17 ABPM Normal Parameters BP should dip by 10-20% during sleep Chughtai and Peixoto. Hosp Phys 2003
18 ABPM 2
19 ABPM 2
20 ABPM 3
21 ABPM 3
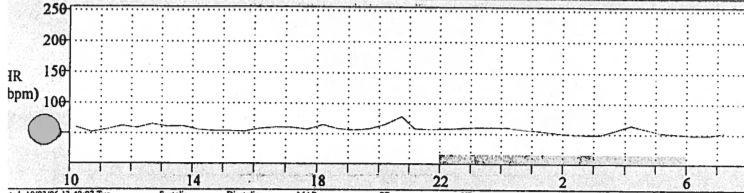
22 ABPM 4
23 ABPM: Number of Readings Recommendation is at least 14 readings in the daytime (NICE Guidance). Minimum number is 2 per hour. We usually do a reading an hour at night.
24 ABPM 5
25 ABPM 5

26 ABPM 5 Ziemmsen. J Neurol Sci 2010
27 Home/Ambulatory SBP mmhg White Coat and Masked Hypertension Masked Hypertension Hypertension Normotension White Coat Hypertension Office SBP mmhg Derived from Pickering et al. Hypertension 2002: 40:

28 Prognosis of Masked Hypertension Prevalence of masked hypertension is approximately 10% in the general population but is higher in patients with diabetes J Hypertension 2007;25:
29 Prognostic Significance of Clinic vs. ABPM Dawes. BP Monit 2006
30 Prognostic Significance of Clinic vs. ABPM Dawes. BP Monit 2006

31 Diagnostic Utility of BP Measures NICE 2011 Guidance Document

32 Diagnostic Utility of BP Measures Hodgkinson. BMJ 2011
33 Cost-Effectiveness of ABPM Lovibond. Lancet 2011
34 Diagnosis of Hypertension: Key Points Non-automated office BP measurements are not accurate. This results in inappropriate management. Out-of-office measurement particularly ABPM should be used to confirm the diagnosis of HTN.

35 Bedtime Dosing of Antihypertensive Drugs
36 Predictive Role of Nighttime BP Hansen. Hypertension 2012
37 The MAPEC Trial
38 MAPEC Hypothesis: Bedtime chronotherapy leads to better BP control and reduces CV endpoints. Design: PROBE RCT Country: Spain Sample Size: 2156; mean age 56 Endpoints: 1. All-cause mortality and CVD events (huge composite endpoint) hour ABPM

39 MAPEC: Results Baseline awake systolic ABPM was 134 mm Hg. Baseline asleep systolic ABPM was 123 mm Hg.
40 MAPEC: Results
41 MAPEC Study: Issues Inconsistent numbers presented across trial publications. Is this truly an RCT with a predefined start and end? Original sample size in the protocol was Subsequent publication mentions 734 normotensive subjects uncertain if they are included in the main paper. Most of the literature in the field comes from a single centre and one group of investigators. Huge effect size from such a small, simple change.
42 Bottom Line: Bedtime Dosing Practical point: relatively simple intervention Conversely, I don t view the data as definitive yet. I don t routinely do it; however, I will in refractory hypertension. Also, in this group, I often use drugs that need bedtime dosing (alpha blockers and some CCBs).

43 Choice of Thiazide Diuretic for HTN Chlorthalidone vs. HCTZ
44 Pharmacologic Structure Chlorthalidone is often mislabeled as thiazidelike. It is a non-thiazide with a distinct pharmacological structure..that has similar pharmacological action (DCT NaCl symporter blockade) Kurtz. Hypertension 2012.
45 Thiazides and Non-thiazides Thiazides Hydrochlorothiazide Chlorothiazide Methychlothiazide Polythiazide Bendroflumethiazide Non-thiazides Chlorthalidone Indapamide Metolazone
46 Pharmacokinetics DRUG ONSET (h) PEAK T1/2 (h) Duration (h) HCTZ (single) 8-15 (long term) 12 (single) (long term) Chlorthalidone (single) (long term) (single) (long term) Carter BL. Hypertension 2004;43:4-9

47 BP Control Meta-analysis of 108 HCTZ and 20 chlorthalidone studies (n=10443) Comparisons are indirect, not head-to-head Dose Chlorthalidone is a more potent drug Ernst, ME. Am J Hypertens. 2010
48 MRFIT Trial Results MRFIT. JAMA 1986
49 Trial Results Trial Drug Result MRFIT Both + HDFP Chlorthalidone + ALLHAT Chlorthalidone + SHEP Chlorthalidone + Oslo BP HCTZ - MAPHY HCTZ - MRC HCTZ - Wing HCTZ - Amery HCTZ + MIDAS HCTZ + ANBP HCTZ + INSIGHT HCTZ + ACCOMPLISH HCTZ -
50 Diuretic Choice: Summary Thiazides and non-thiazides are similar and dissimilar properties. Chlorthalidone (non-thiazide) is more potent and can reduce BP more than HCTZ at equal doses. Non-definitive hard outcome indirect comparisons:?chlorthalidone better
51 Diuretic Choice: Practical Considerations Chlorthalidone: smallest dose available in Canada is 50 mg. Chlorthalidone: not commonly available in combos (atenolol only). HCTZ: many combos If BP controlled on HCTZ, I don t change. If I need to choose a fixed dose combo with a diuretic, I use perindopril indapamide or a HCTZ combo ($$ and coverage considered) In uncontrolled refractory hypertension, I will usually use chlorthalidone

52 Treatment Target in Mild HTN

53 Treatment of Mild Hypertension

54 Treatment of Mild Hypertension
55 Treatment of Mild Hypertension Primary Prevention Subjects with Mild HTN Total events 77 vs 90: Nearly all from one study Diao et al. Cochrane Collaboration 2013
56 Comments on This Review 1. Essentially reflects one study (that used BB in half the active treatment group) 2. Underpowered study not designed to specifically look at this subgroup. Randomization not stratified for this subgroup. 3. The authors excluded relevant studies: a) Non-placebo controlled studies (e.g., HDFP). b) Didn t have data for some studies (VA, Oslo, others) but number of events for these would have been small
57 Major Trials Including Patients with Mild Hypertension Trial (n) MRC y ANBP y Age BP Results for Primary Endpoint (intervention vs. control) Stroke events: 60 vs vs per 100 pt*y p<0.01 ARD 0.12% over 5 y Nonfatal and fatal CV events:138 vs vs. 2.5 per 100 pt*y P<0.05 ARD 0.5% over 4 y HDFP y Total mortality: 349 vs % vs. 7.7% P<0.01; ARD 1.3% over 5 y
58 Major Trials Including Patients with Mild Hypertension Trial (n) HDFP 7825 Age BP stratum Results for Primary Endpoint (intervention vs. control) Total mortality: 231 vs % vs. 7.4% P<0.01; ARD 1.5%

59 HDFP Mortality RRR HDFP. JAMA 1971
60 Canadian Hypertension Education Program Recommendations For Initiating Drug Therapy 1. Prescribe for DBP 100 or SBP 160 (Grade A). 2. Strongly consider for DBP 90 and TOD or other CV risk factors (Grade A). 3. Strongly consider for SBP 140 and TOD (Grade C for mild HTN).
61 Major Trials Including Patients with Mild Hypertension Trial (n) MRC y ANBP y HDFP y Age BP Results for Primary Endpoint (intervention vs. control) Stroke events: 60 vs vs per 100 pt*y p<0.01 ARD 0.12% over 5 y Nonfatal and fatal CV events:138 vs vs. 2.5 per 100 pt*y P<0.05 ARD 0.5% over 4 y Total mortality: 349 vs % vs. 7.7% P<0.01; ARD 1.3% over 5 y NNT over 1 year NNT over 10 y NNT over 10y for statins for CV event in high-risk patient is 11 and in mod risk pt. is 23.
62 Major Trials Including Patients with Mild Hypertension Trial (n) Age BP Results for Primary Endpoint (intervention vs. control) NNT over 1 year NNT over 10 y HDFP subgroup stratum Total mortality: 231 vs % vs. 7.4% P<0.01; ARD 1.5%
63 HDFP Trial Alderman. Hypertension 1983
64 II. Indications for Pharmacotherapy after diagnosis of hypertension (1) Patients at low risk with stage 1 hypertension ( /90-99 mmhg) lifestyle modification can be the sole therapy. Patients with target organ damage (e.g. left ventricular hypertrophy) ( /90-99 mmhg) Treat with pharmacotherapy Patients with chronic kidney disease should be considered for pharmacotherapy if the blood pressure is equal or over 140/90 mmhg Patients with diabetes should be considered for pharmacotherapy if the blood pressure is equal or over 140/90 mmhg
65 II. Indications for Pharmacotherapy after diagnosis of hypertension (2) Patients with other risk factors (over 90% of Canadians with hypertension have other risk factors) ( /90-99 mmhg despite lifestyle modification) Treat with pharmacotherapy Treatment Gap Alert: Many younger hypertensive Canadians with multiple cardiovascular risks are currently not treated with pharmacotherapy. Health care professionals need to be aware of this important care gap and recommend pharmacotherapy.
66 Treatment of Mild Hypertension: Key Points 1. All patients should be treated with lifestyle modification. 2. Decision to institute drug treatment should take into account global risk.
67 Renal Denervation
68 Resistant Hypertension Failure to achieve BP target despite treatment with three antihypertensive drugs (including a diuretic) at optimal doses. Prevalence is not well studied. Appears to be about 10-20% of hypertensive patients. Sarafidis. J Clin Hypertens 2011
69 Sympathectomy for Severe Hypertension Bilateral T8-L3 Sympathectomy Ray BS. Ann Surg 1949

70 Renal Sympathetic Denervation Papademetriou et al. Int J Hypertens 2011

71 Renal Sympathetic Denervation for Resistant Hypertension Source: Medtronic 73
 Esler et al.")
72 Renal Sympathetic Denervation for Resistant Hypertension: SYMPLICITY HTN-2 RCT 6 month BP difference of 33/11 P< (n=106) Esler et al. Lancet
73 Renal Sympathetic Denervation: Safety Well tolerated one femoral pseudoaneurysm was the only adverse effect. Renal function similar at end of six months. Only half had ABPM measured; ABPM difference was 16/8 mm Hg between groups. Irreversible nature of the procedure Renal adverse effects? Stenosis, dilation Proteinuria Renal function
74 Renal Sympathetic Denervation: Key Point An emerging procedure Potential to be used in a large number of patients Long-term efficacy and safety data required.
75 Outline 1. Understand how to interpret ABPM. 2. Review the pros and cons of different methods to diagnose hypertension. 3. Discuss some current controversies in HTN management.
Disclosures. Funding: CIHR, HSF, AIHS, UHF. Research: Novo Nordisk, CVRx, Valencia. Consulting: Valeant
 Hypertension Update Raj Padwal Associate Professor General Internal Medicine and Clinical Pharmacology Director, Hypertension Clinic University of Alberta Disclosures Funding: CIHR, HSF, AIHS, UHF Research:
Hypertension Update Raj Padwal Associate Professor General Internal Medicine and Clinical Pharmacology Director, Hypertension Clinic University of Alberta Disclosures Funding: CIHR, HSF, AIHS, UHF Research:
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Objectives. JNC 7 Is Nice But What s Up With JNC 8? Why Do We Care? Hypertension Background: Prevalence
 JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
APPENDIX D: PHARMACOTYHERAPY EVIDENCE
 Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Masked Hypertension. Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre
 Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
Disclosures. Hypertension: Nationwide Dilemma. Learning Objectives. What s Currently Recommended? Specific Concerns 3/9/2012
 How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
Hypertension Update. Faculty/Presenter Disclosure
 Hypertension Update Who Gives a CHEP About Targets? Faculty/Presenter Disclosure Presenter: Raj Padwal Relationships that may introduce potential bias and/or conflict of interest: Grants/Research Support:
Hypertension Update Who Gives a CHEP About Targets? Faculty/Presenter Disclosure Presenter: Raj Padwal Relationships that may introduce potential bias and/or conflict of interest: Grants/Research Support:
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Talking about blood pressure
 Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Blood Pressure Monitoring in Chronic Kidney Disease
 Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS
 HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS Michael J. Scalese, PharmD, BCPS, CACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 14, 2018 DISCLOSURE/CONFLICT OF INTEREST
HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS Michael J. Scalese, PharmD, BCPS, CACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 14, 2018 DISCLOSURE/CONFLICT OF INTEREST
Hypertension Guidelines Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center
 Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
Patrick Kay, General and Interventional Cardiologist Auckland or healthpoint.co.nz
 Patrick Kay, General and Interventional Cardiologist Auckland ipatkay@hotmail.com or healthpoint.co.nz Rotorua 2015 Rotorua 2015 Graphical example of true mean and variation, and of regression to the
Patrick Kay, General and Interventional Cardiologist Auckland ipatkay@hotmail.com or healthpoint.co.nz Rotorua 2015 Rotorua 2015 Graphical example of true mean and variation, and of regression to the
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
The Evolution To Treatment Of Hypertension With Advanced Formulation
 The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Hypertension: What s new since JNC 7. Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF
 Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Thiazide or Thiazide Like? Choosing Wisely Academic Detailing Conference Digby Pines October 12-14
 Thiazide or Thiazide Like? Choosing Wisely Academic Detailing Conference Digby Pines October 12-14 Disclosures Pam McLean-Veysey, Team Leader Drug Evaluation Unit DEU funded by the Drug Evaluation Alliance
Thiazide or Thiazide Like? Choosing Wisely Academic Detailing Conference Digby Pines October 12-14 Disclosures Pam McLean-Veysey, Team Leader Drug Evaluation Unit DEU funded by the Drug Evaluation Alliance
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
AGING, BLOOD PRESSURE & CARDIOVASCULAR DISEASE EVENT RISK. Michael Smolensky, Ph.D. The University of Texas Austin & Houston
 AGING, BLOOD PRESSURE & CARDIOVASCULAR DISEASE EVENT RISK Michael Smolensky, Ph.D. The University of Texas Austin & Houston Disclosures Partner: Circadian Ambulatory Diagnostics Consultant: Spot On Sciences
AGING, BLOOD PRESSURE & CARDIOVASCULAR DISEASE EVENT RISK Michael Smolensky, Ph.D. The University of Texas Austin & Houston Disclosures Partner: Circadian Ambulatory Diagnostics Consultant: Spot On Sciences
MPharmProgramme. Hypertension (HTN)
") MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management?
 Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Slide notes: References:
 1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
NICE BHS Hypertension guidelines 2011 update
 NICE BHS Hypertension guidelines 2011 update Review for clinicians Sept 2011 Mark Thomas West Midlands Hypertension Centre Heart of England NHS Trust www.wmhc.co.uk mark.thomas@heartofengland.nhs.uk Full
NICE BHS Hypertension guidelines 2011 update Review for clinicians Sept 2011 Mark Thomas West Midlands Hypertension Centre Heart of England NHS Trust www.wmhc.co.uk mark.thomas@heartofengland.nhs.uk Full
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
RISE, FALL AND RESURRECTION OF RENAL DENERVATION. Michael A. Weber, MD State University of New York Downstate College of Medicine
 RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
HYPERTENSION IN THE ELDERLY A BALANCED APPROACH. Barry Goldlist October 31, 2014
 HYPERTENSION IN THE ELDERLY A BALANCED APPROACH Barry Goldlist October 31, 2014 DISCLOSURE I have not accepted any money for myself from any pharmaceutical company in the 21 st century I have accepted
HYPERTENSION IN THE ELDERLY A BALANCED APPROACH Barry Goldlist October 31, 2014 DISCLOSURE I have not accepted any money for myself from any pharmaceutical company in the 21 st century I have accepted
Hypertension 2015: Recent Evidence that Will Change Your Practice
 Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Challenges in Hypertension: Incorporating Evolving Clinical Data Into Practice
 Challenges in Hypertension: Incorporating Evolving Clinical Data Into Practice Faculty Jan Basile, MD Professor of Medicine Seinsheimer Cardiovascular Health Program Division of General Internal Medicine
Challenges in Hypertension: Incorporating Evolving Clinical Data Into Practice Faculty Jan Basile, MD Professor of Medicine Seinsheimer Cardiovascular Health Program Division of General Internal Medicine
Hypertension and Atrial Fibrillation
 Hypertension and Atrial Fibrillation Sheldon Tobe MD, MScCH (HPTE), FRCPC, FACP, FASH Hypertension and Nephrology HSF/NOSM Chair in Aboriginal and Rural Health Research Professor in Medicine, University
Hypertension and Atrial Fibrillation Sheldon Tobe MD, MScCH (HPTE), FRCPC, FACP, FASH Hypertension and Nephrology HSF/NOSM Chair in Aboriginal and Rural Health Research Professor in Medicine, University
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Volume 6; Number 1 January 2012 NICE CLINICAL GUIDELINE 127: HYPERTENSION CLINICAL MANAGEMENT OF PRIMARY HYPERTENSION IN ADULTS (AUGUST 2011)
") Volume 6; Number 1 January 2012 NICE CLINICAL GUIDELINE 127: HYPERTENSION CLINICAL MANAGEMENT OF PRIMARY HYPERTENSION IN ADULTS (AUGUST 2011) What s new in hypertension? NICE has issued an updated Clinical
Volume 6; Number 1 January 2012 NICE CLINICAL GUIDELINE 127: HYPERTENSION CLINICAL MANAGEMENT OF PRIMARY HYPERTENSION IN ADULTS (AUGUST 2011) What s new in hypertension? NICE has issued an updated Clinical
Importance of Ambulatory Blood Pressure Monitoring in Adolescents
 Importance of Ambulatory Blood Pressure Monitoring in Adolescents Josep Redon, MD, PhD, FAHA Internal Medicine Hospital Clinico Universitario de Valencia University of Valencia CIBERObn Instituto de Salud
Importance of Ambulatory Blood Pressure Monitoring in Adolescents Josep Redon, MD, PhD, FAHA Internal Medicine Hospital Clinico Universitario de Valencia University of Valencia CIBERObn Instituto de Salud
JNC-8. (Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure- 8) An Update on Hypertension Guidelines
 An Update on Hypertension Guidelines") JNC-8 (Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure- 8) An Update on Hypertension Guidelines Derrick Sorweide, DO Assistant Professor of Family Medicine,
JNC-8 (Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure- 8) An Update on Hypertension Guidelines Derrick Sorweide, DO Assistant Professor of Family Medicine,
Evaluation and Management of Hypertension in Women. Vesna D. Garovic, M.D. Moscow, Russia, December 2016
 Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Diabetes and Hypertension
 Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
A/Prof Gerard Wilkins. A/Proff of Medicine at Otago University Cardiac Services at Dunedin Hospital
 A/Prof Gerard Wilkins A/Proff of Medicine at Otago University Cardiac Services at Dunedin Hospital Hypertension Ambulatory BP Monitoring Gerard T Wilkins Assoc Professor of Medicine, Consultant Cardiologist,
A/Prof Gerard Wilkins A/Proff of Medicine at Otago University Cardiac Services at Dunedin Hospital Hypertension Ambulatory BP Monitoring Gerard T Wilkins Assoc Professor of Medicine, Consultant Cardiologist,
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA
 Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
Managing Hypertension in 2018
 MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
Individual management of arterial hypertension. Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki
 Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets
 Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets Robert J. Herman University of Calgary herman@ucalgary.ca Conflict of Interest Disclosure
Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets Robert J. Herman University of Calgary herman@ucalgary.ca Conflict of Interest Disclosure
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127
 Hypertension in adults: diagnosis and management Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Hypertension in adults: diagnosis and management Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
2/10/2014. Hypertension: Highlights of Hypertension Guidelines: Making the Most of Limited Evidence. Issues with contemporary guidelines
 Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Management of Hypertension in Women
 Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines. John Potter Professor Ageing & Stroke Medicine University of East Anglia
 Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
Hipertensión enmascarada. Alejandro de la Sierra Hospital Mútua Terrassa Universitat de Barcelona
 Hipertensión enmascarada Alejandro de la Sierra Hospital Mútua Terrassa Universitat de Barcelona HTA enmascarada Definición Prevalencia Características clínicas Riesgo derivado Asociación con LOD Progresión
Hipertensión enmascarada Alejandro de la Sierra Hospital Mútua Terrassa Universitat de Barcelona HTA enmascarada Definición Prevalencia Características clínicas Riesgo derivado Asociación con LOD Progresión
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Renal Denervation. by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School
 Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Overview. NOT A REPETION OF LOCAL GUIDELINE Dr Diviash Thakrar
 Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
Dr Diana R Holdright. MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION.
 Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Ambulatory BP Monitoring: Getting the Diagnosis of Hypertension Right. Anthony J. Viera, MD, MPH, FAHA Professor and Chair
 Ambulatory BP Monitoring: Getting the Diagnosis of Hypertension Right Anthony J. Viera, MD, MPH, FAHA Professor and Chair Objectives Review limitations of office BP in making a correct diagnosis of hypertension
Ambulatory BP Monitoring: Getting the Diagnosis of Hypertension Right Anthony J. Viera, MD, MPH, FAHA Professor and Chair Objectives Review limitations of office BP in making a correct diagnosis of hypertension
Updates in Cardiovascular Recommendations for Diabetic Patients
 Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Management of Hypertension in special groups. DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University
 Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH)
") Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations
 Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Update in Cardiology Pharmacologic Management of Cardiovascular Risk. Christopher C. Roe, MSN, ACNP
 Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts