Normal range of serum potassium is meq/l true hyperkalemia manifests clinically as : Clinical presentation : muscle and cardiac dysfunction
|
|
|
- Jewel Barrett
- 5 years ago
- Views:
Transcription
1 Potassium Disorders
2 hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of the nephron is mainly responsible for the excretion of potassium? What Is the normal range of potassium? How does hyperkalemia manifest clinically? What are the EGC changes associated with hyperkalemia? How is hyperkalemia acutely managed? How do you approach a case of hyperkalemia?
3 Normal range of serum potassium is meq/l true hyperkalemia manifests clinically as : Clinical presentation : muscle and cardiac dysfunction muscular symptoms myalgias muscle paralysis chest pain cardiac symptoms arrhythmias and palpitations nausea and vomiting paresthesia's


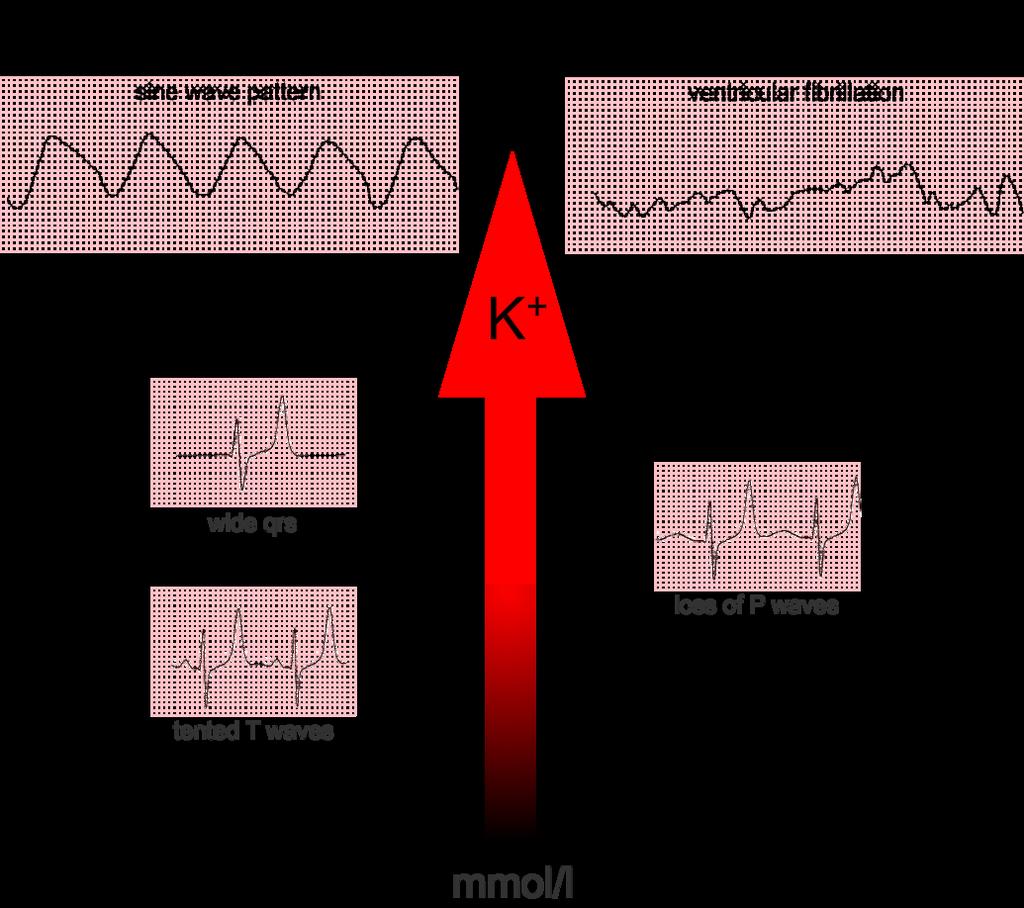
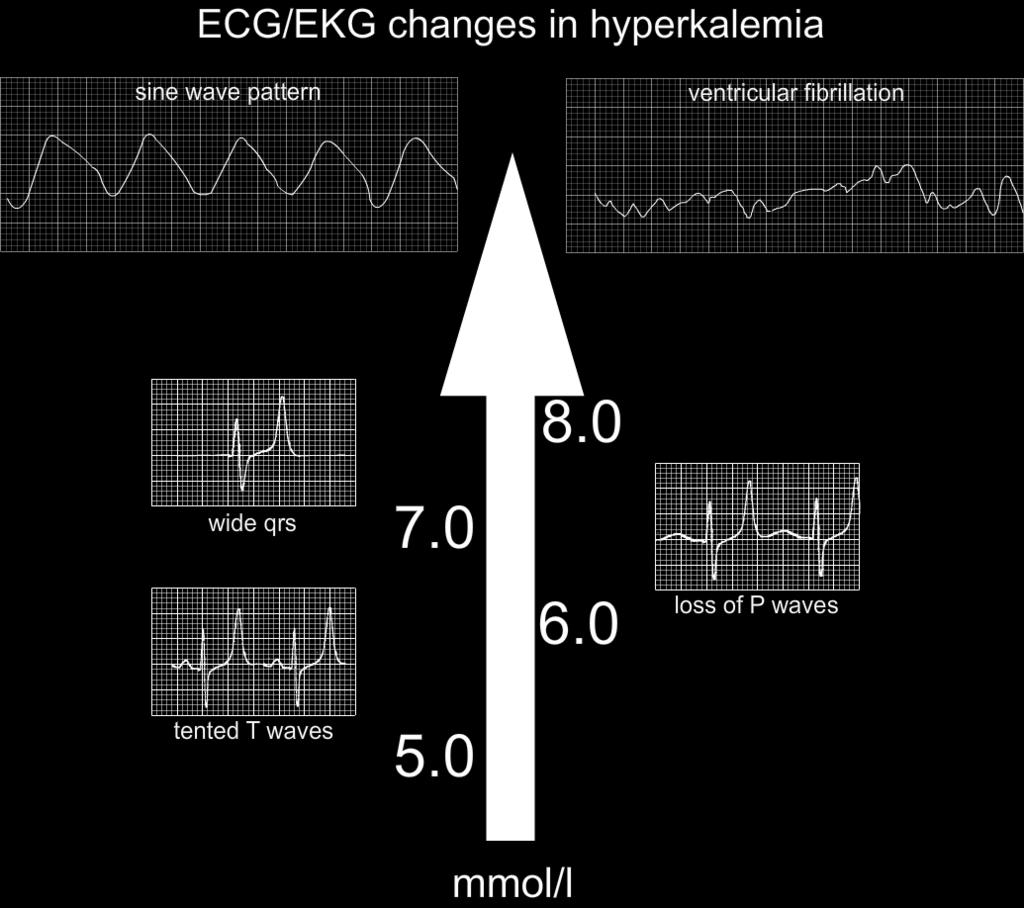
4 ECG changes 1. Tall 'tented' T waves


5 2- P wave changes Worsening hyperkalemia is associated with progressive flattening of P waves, prolongation of the PR interval (PR interval > 200 ms) and eventually disappearance of P waves. Bradycardia is common and AV block may complicate hyperkalemia.


6 3-Broad QRS complexes As serum K+ levels rise the QRS complex becomes wider eventually passing the upper limit of normal. At least think of hyperkalemia if you see this combination of wide QRS complexes and tall T waves.


7 4-Development of a sine wave pattern As K + levels rise further, the situation is becoming critical. The combination of broadening QRS complexes and tall T waves produces a sine wave pattern on the ECG readout. Cardiovascular collapse and death are imminent.

8 5- Ventricular fibrillation The end game for untreated hyperkalemia is chaotic depolarization of ventricular myocardium: ventricular fibrillation. No cardiac output is present. This situation is not compatible with life.
9
10 Acute management of hyperkalemia 1. Check for ECG CHANGES, if non, consider lab error, repeat sample without tourniquet, Otherwise, in the presence of symptoms, ECG changes or critically high potassium do the following 1. ABC s 2. Place on continuous ECG monitor 3. Stabilize the myocardium by? 4. Induce trans-cellular sift by? 5. Rid the body of excess potassium by? 6. Treat the underlying cause
11
12 1-IV calcium is indicated when the serum potassium is >6.5 meq/l regardless of whether ECG changes are present. 6 Given their poor sensitivity and specificity, ECG changes should not be used as diagnostic criteria for treatment of hyperkalemia. 7 The immediate goal of acute management in hyperkalemia is the stabilization of the membrane potential, which is often done with IV calcium. Calcium antagonizes the effects of hyperkalemia through effects on the threshold potential and the speed of impulse propagation at the cellular level. IV calcium can be given as 10 ml of a 10% calcium gluconate solution over 2 to 3 minutes 2-Insulin: Insulin accelerates the intracellular movement of potassium into muscle cells by binding to its receptor on skeletal muscle. Once this occurs, the abundance and activity of sodium-potassium adenosine triphosphatase (Na+/K+-ATPase) and glucose transporter on the cell membrane increase through independent signaling pathways. The most commonly recommended regimen is a bolus injection of short-acting insulin. If the blood glucose is <250 mg/dl, 25 g of glucose should also be given (50 ml of a 50% solution) to offset hypoglycemia due to insulin administration
13 3- Sodium bicarbonate works to shift potassium intracellularly but is not considered first-line management of hyperkalemia due to controversial data regarding efficacy and safety concerns. Boluses of 1 ml/kg of sodium bicarbonate 8.4% solution have been suggested. Studies have shown that sodium bicarbonate was not able to decrease serum potassium significantly or rapidly, with onset of action potentially taking hours. 4- Albuterol inhalation can be considered in nonacute situations to lower potassium. Albuterol stimulates Na+/K+-ATPase, which results in intracellular shift of potassium of albuterol has been shown to decrease serum potassium levels by 0.3 to 0.6 meq/l within 30 minutes; the decrease lasts for at least 2 hours.
14 5- Diuretics : In patients with adequate kidney function, loop diuretics (e.g., furosemide and bumetanide) in combination with thiazide diuretics can be used for the excretion of potassium. Onset of action is 15 to 60 minutes. However, it should be noted that although diuretic-induced volume depletion can lead to decreased distal nephron flow and reduced potassium excretion, volume-expanded patients will benefit from diuresis. 6- kayexalate or SPS is a cation-exchange polymer that exchanges sodium for potassium, in addition to other cations such as calcium, ammonium, and magnesium. SPS also contains a considerable amount of sodium content and should be used cautiously in patients with concomitant conditions such as congestive heart failure, edema, and severe hypertension.
15 it may be given as 15 to 30 g by mouth with cathartics (most commonly sorbitol) or as an enema. The rectal dose is 30 to 50 g but has been found to be less effective compared to an equivalent dose administered orally. What is the most important side effect of such a medication? 6- hemodialysis
16 Causes of hyperkalemia- Approach?
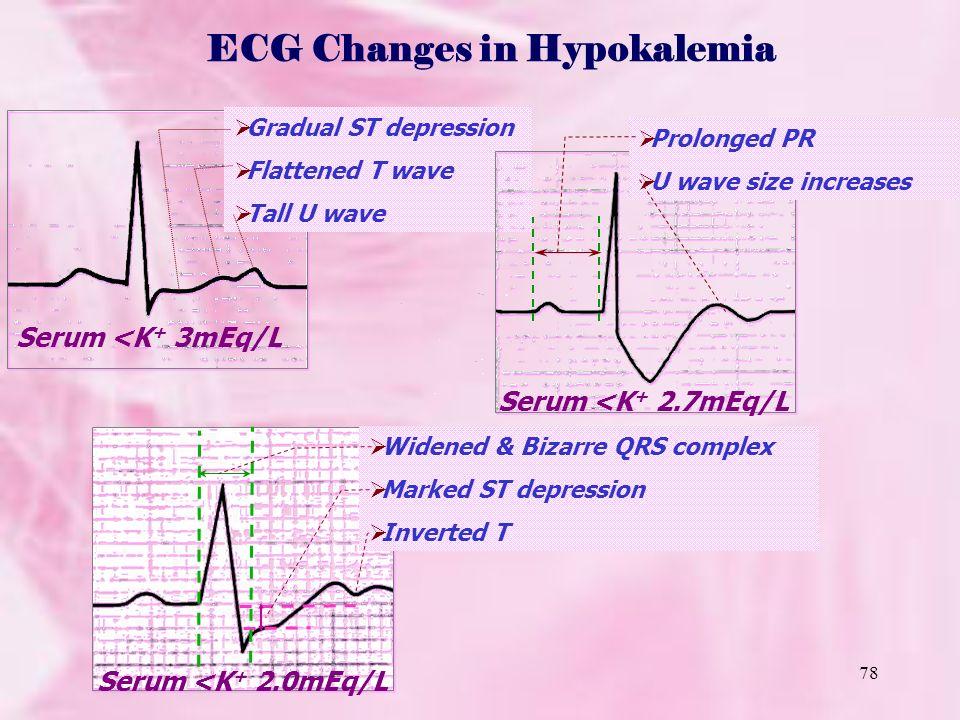
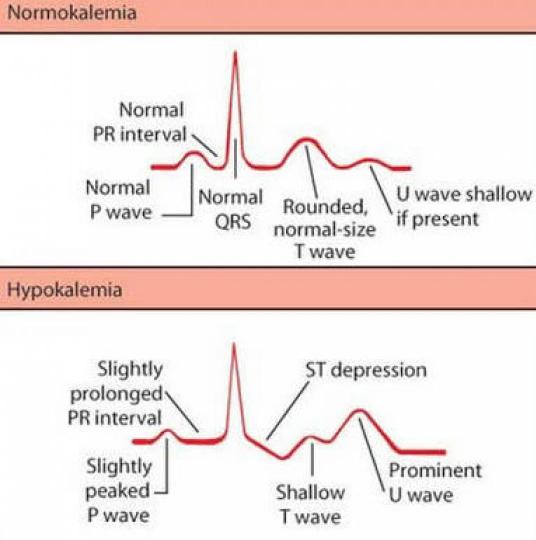
17 Hypokalemia ( potassium less than 3.5 meq/ L) Clinical presentation : Presentation muscle and cardiac dysfunction muscular symptoms muscle weakness and cramping cardiac symptoms Palpitations Paralytic ileus paresthesia nausea and vomiting Hypokalemic nephropathy ( which includes????)
18 ECG changes of hypokalemia :
19
20
21 Treatment of hypokalemia 1- ABC s 2- place on cardiac monitor 3 replace potassium Iv potassium chloride at a rate of no more than 20 meq/hour, and a concentration of no more than 40 meq/l, preferably via central line 4- treat the underlying cause
22 Approach to a patient with hypokalemia
A Mnemonic for the Treatment of Hyperkalemia. Nick Wolters, PGY1 Resident Grandview Medical Center
 A Mnemonic for the Treatment of Hyperkalemia Nick Wolters, PGY1 Resident Grandview Medical Center Hyperkalemia 30 YOF, ESRD, missed 2 dialysis sessions over the last week Potassium level came back at 7
A Mnemonic for the Treatment of Hyperkalemia Nick Wolters, PGY1 Resident Grandview Medical Center Hyperkalemia 30 YOF, ESRD, missed 2 dialysis sessions over the last week Potassium level came back at 7
Electrolyte Imbalance and Resuscitation. Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine
 Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Hyperkalemia Protect, Shift, and Eliminate
 Disclosure Michael C. Thomas reports no relevant financial relationships. Lytes Off in Vegas! The Acute Management of Potassium and Calcium Disorders Program Objectives Design a plan to replace and monitor
Disclosure Michael C. Thomas reports no relevant financial relationships. Lytes Off in Vegas! The Acute Management of Potassium and Calcium Disorders Program Objectives Design a plan to replace and monitor
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Potassium A NNA VINNIKOVA, M. D.
 Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
K+ Ann Crawford, RN, PhD, CNS, CEN
 Hyperkalemia: Management of a Critical Electrolyte Disturbance K+ Ann Crawford, RN, PhD, CNS, CEN Balancing Fluid Intracellular fluid (ICF) Extracellular fluid (ECF) Intravascular interstitial Hormonal
Hyperkalemia: Management of a Critical Electrolyte Disturbance K+ Ann Crawford, RN, PhD, CNS, CEN Balancing Fluid Intracellular fluid (ICF) Extracellular fluid (ECF) Intravascular interstitial Hormonal
Electrolytes and other equally exciting topics
 Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
PP-US-DSE Relypsa, Inc. All rights reserved. Relypsa and the Relypsa logo are trademarks of Relypsa, Inc.
 1 2 There are 4 main objectives that I d like to cover with you today: First, to review the definition, prevalence, and risk of hyperkalemia in certain populations Second, to review why RAASi are recommended
1 2 There are 4 main objectives that I d like to cover with you today: First, to review the definition, prevalence, and risk of hyperkalemia in certain populations Second, to review why RAASi are recommended
Hyperkalemia. Katarzyna Bigaj PGY -1
 Hyperkalemia Katarzyna Bigaj PGY -1 Definition Hyperkalaemia is defined as a potassium level > 5.5 meq/l Moderate hyperkalaemia is a serum potassium > 6.0 meq/l Severe hyperkalaemia is a serum potassium
Hyperkalemia Katarzyna Bigaj PGY -1 Definition Hyperkalaemia is defined as a potassium level > 5.5 meq/l Moderate hyperkalaemia is a serum potassium > 6.0 meq/l Severe hyperkalaemia is a serum potassium
Nephrology / Urology. Hyperkalemia Causes and Definition Lecturio Online Medical Library. Definition. Epidemiology of Hyperkalemia.
 Nephrology / Urology Hyperkalemia Causes and Definition Lecturio Online Medical Library See online here Hyperkalemia is defined by the serum potassium level when it is higher than 5.5mEq/L. It is usually
Nephrology / Urology Hyperkalemia Causes and Definition Lecturio Online Medical Library See online here Hyperkalemia is defined by the serum potassium level when it is higher than 5.5mEq/L. It is usually
HYPERKALEMIA. Best Practices in Managing. in Chronic Kidney Disease
 + Best Practices in Managing HYPERKALEMIA in Chronic Kidney Disease Hyperkalemia in Chronic Kidney Disease (CKD) Treatment with RAAS Inhibitors (RAASi) in CKD Diagnosis and Evaluation of Hyperkalemia Treatment
+ Best Practices in Managing HYPERKALEMIA in Chronic Kidney Disease Hyperkalemia in Chronic Kidney Disease (CKD) Treatment with RAAS Inhibitors (RAASi) in CKD Diagnosis and Evaluation of Hyperkalemia Treatment
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Potassium secretion. E k = -61 log ([k] inside / [k] outside).
![Potassium secretion. E k = -61 log ([k] inside / [k] outside).](/thumbs/80/80478709.jpg "Potassium secretion. E k = -61 log ([k] inside / [k] outside).") 1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis.
 Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
The Crushing Truth. Crush Injury Syndrome Compartment Syndrome Acute Traumatic Ischemia. Carson City Fire Department
 The Crushing Truth Crush Injury Syndrome Compartment Syndrome Acute Traumatic Ischemia Carson City Fire Department John Mohler, RN, BSN, CFRN, CCRN REMSA Care Flight Carson City Fire Department 1 Crushing
The Crushing Truth Crush Injury Syndrome Compartment Syndrome Acute Traumatic Ischemia Carson City Fire Department John Mohler, RN, BSN, CFRN, CCRN REMSA Care Flight Carson City Fire Department 1 Crushing
Fluids & Electrolytes
 Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
Electrolyte abnormalities are commonly associated with
 Electrolyte abnormalities are commonly associated with cardiovascular emergencies. These abnormalities may cause or contribute to cardiac arrest and may hinder resuscitative efforts. In some cases therapy
Electrolyte abnormalities are commonly associated with cardiovascular emergencies. These abnormalities may cause or contribute to cardiac arrest and may hinder resuscitative efforts. In some cases therapy
Medical therapy of AKI complications. Refik Gökmen AKI Academy 18 October 2014
 Medical therapy of AKI complications Refik Gökmen AKI Academy 18 October 2014 Medical therapy of AKI complications Hyperkalaemia Volume status, fluid therapy Acidosis Calcium & phosphate Bleeding risk
Medical therapy of AKI complications Refik Gökmen AKI Academy 18 October 2014 Medical therapy of AKI complications Hyperkalaemia Volume status, fluid therapy Acidosis Calcium & phosphate Bleeding risk
PRODUCT INFORMATION RESONIUM A. Na m
 PRODUCT INFORMATION RESONIUM A NAME OF THE MEDICINE Non-proprietary Name Sodium polystyrene sulfonate Chemical Structure CH - 2 CH SO 3 Na + n CAS Number 28210-41-5 [9003-59-2] CH 2 CH SO - 3 m DESCRIPTION
PRODUCT INFORMATION RESONIUM A NAME OF THE MEDICINE Non-proprietary Name Sodium polystyrene sulfonate Chemical Structure CH - 2 CH SO 3 Na + n CAS Number 28210-41-5 [9003-59-2] CH 2 CH SO - 3 m DESCRIPTION
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
HEART FAILURE PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
Hyponatremia and Hypokalemia
 Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
CSI (Clinical Scenario Investigation): Hyperkalemia
: Hyperkalemia") CSI (Clinical Scenario Investigation): Hyperkalemia Alison Thomas, RN(EC), MN, CNeph(C) Ann Jones, RN(EC), MSN, CNeph(C) Joyce Hunter, RN, Vascular Access Co-ordinator Simcoe Muskoka Regional Kidney Care
CSI (Clinical Scenario Investigation): Hyperkalemia Alison Thomas, RN(EC), MN, CNeph(C) Ann Jones, RN(EC), MSN, CNeph(C) Joyce Hunter, RN, Vascular Access Co-ordinator Simcoe Muskoka Regional Kidney Care
Acid-Base Balance 11/18/2011. Regulation of Potassium Balance. Regulation of Potassium Balance. Regulatory Site: Cortical Collecting Ducts.
 Influence of Other Hormones on Sodium Balance Acid-Base Balance Estrogens: Enhance NaCl reabsorption by renal tubules May cause water retention during menstrual cycles Are responsible for edema during
Influence of Other Hormones on Sodium Balance Acid-Base Balance Estrogens: Enhance NaCl reabsorption by renal tubules May cause water retention during menstrual cycles Are responsible for edema during
ELECTROLYTES RENAL SHO TEACHING
 ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
PRODUCT MONOGRAPH K-DUR. (Potassium Chloride) Sustained Release Tablets mg - 20 mmol (meq)
 Sustained Release Tablets mg - 20 mmol (meq)") PRODUCT MONOGRAPH K-DUR (Potassium Chloride) Sustained Release Tablets 1500 mg - 20 mmol (meq) Merck Canada Inc. 16750 route Transcanadienne Kirkland, Quebec H9H 4M7 DATE OF PREPARATION: March 2, 2011
PRODUCT MONOGRAPH K-DUR (Potassium Chloride) Sustained Release Tablets 1500 mg - 20 mmol (meq) Merck Canada Inc. 16750 route Transcanadienne Kirkland, Quebec H9H 4M7 DATE OF PREPARATION: March 2, 2011
THE HYPERKALEMIC SYNDROMES
 THE HYPERKALEMIC SYNDROMES K + BALANCE Cells (3400 meq) ECF (60 meq) External K Pump insulin catechols Na intake Leak K ph; osmolality membrane integrity distal Na + renal { delivery output aldosterone
THE HYPERKALEMIC SYNDROMES K + BALANCE Cells (3400 meq) ECF (60 meq) External K Pump insulin catechols Na intake Leak K ph; osmolality membrane integrity distal Na + renal { delivery output aldosterone
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
ECG & ELECTROLYTES IMBALANCE
 ECG & ELECTROLYTES IMBALANCE Ayman Khairy, MD Ass. Prof. of Cardiovascular Medicine Assiut University, EGYPT Mohamed Aboel-Kassem, MD Lecturer of Cardiovascular Medicine Assiut University, EGYPT Systematic
ECG & ELECTROLYTES IMBALANCE Ayman Khairy, MD Ass. Prof. of Cardiovascular Medicine Assiut University, EGYPT Mohamed Aboel-Kassem, MD Lecturer of Cardiovascular Medicine Assiut University, EGYPT Systematic
A case of nonfatal non-collapsed patient with extreme hyperkalaemia
 Hong Kong Journal of Emergency Medicine A case of nonfatal non-collapsed patient with extreme hyperkalaemia YH Lim and J Hendricks This is a report of a non-collapsed patient with nonfatal, extreme hyperkalaemia
Hong Kong Journal of Emergency Medicine A case of nonfatal non-collapsed patient with extreme hyperkalaemia YH Lim and J Hendricks This is a report of a non-collapsed patient with nonfatal, extreme hyperkalaemia
Virtual Mentor American Medical Association Journal of Ethics April 2007, Volume 9, Number 4:
 Virtual Mentor American Medical Association Journal of Ethics April 2007, Volume 9, Number 4: 295-299. Clinical pearl Hyperkalemia: newer considerations by Amar D. Bansal and David S. Goldfarb, MD Maintenance
Virtual Mentor American Medical Association Journal of Ethics April 2007, Volume 9, Number 4: 295-299. Clinical pearl Hyperkalemia: newer considerations by Amar D. Bansal and David S. Goldfarb, MD Maintenance
5/18/2017. Specific Electrolytes. Sodium. Sodium. Sodium. Sodium. Sodium
 Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
SODIUM POLYSTYRENE SULFONATE Suspension, USP
 SODIUM POLYSTYRENE SULFONATE Suspension, USP DESCRIPTION Sodium Polystyrene Sulfonate Suspension, USP can be administered orally or in an enema. It is a cherryflavored suspension containing 15 grams of
SODIUM POLYSTYRENE SULFONATE Suspension, USP DESCRIPTION Sodium Polystyrene Sulfonate Suspension, USP can be administered orally or in an enema. It is a cherryflavored suspension containing 15 grams of
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE. Jules B. Puschett, M.D.
 DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
SUMMARY OF PRODUCT CHARACTERISTICS 2. QUALITATIVE AND QUANTITATIVE COMPOSITION
 SUMMARY OF PRODUCT CHARACTERISTICS PRODUCT SUMMARY 1. NAME OF THE MEDICINAL PRODUCT Sterile Potassium Chloride Concentrate 15%. 2. QUALITATIVE AND QUANTITATIVE COMPOSITION 15% of Potassium Chloride in
SUMMARY OF PRODUCT CHARACTERISTICS PRODUCT SUMMARY 1. NAME OF THE MEDICINAL PRODUCT Sterile Potassium Chloride Concentrate 15%. 2. QUALITATIVE AND QUANTITATIVE COMPOSITION 15% of Potassium Chloride in
Major intra and extracellular ions Lec: 1
 Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
K+ Na+ Na+ Na+ 4/28/2018. What does Potassium do for you? Regulation of Muscle and Nerve Function. Regulation of Muscle and Nerve Function
 What does Potassium do for you? Aids in the conversion of glucose into glycogen Assists in carbohydrate and protein metabolism 2018 Spring Fling EMS Conference Maintains balance between cells and body
What does Potassium do for you? Aids in the conversion of glucose into glycogen Assists in carbohydrate and protein metabolism 2018 Spring Fling EMS Conference Maintains balance between cells and body
Chapter 21. Diuretic Agents. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Conflict of interest
 Hyperkalemia in Heart and Kidney patients: Rescue is here Wajeh Qunibi, MD, FACP Professor of Medicine University of Texas Health Science Center San Antonio, TX CARDIORENAL CONNECTION April 28, 2017 Conflict
Hyperkalemia in Heart and Kidney patients: Rescue is here Wajeh Qunibi, MD, FACP Professor of Medicine University of Texas Health Science Center San Antonio, TX CARDIORENAL CONNECTION April 28, 2017 Conflict
Prevention of Electrolyte Disorders Refeeding Syndrome พญ.น นทพร เต มพรเล ศ
 Prevention of Electrolyte Disorders Refeeding Syndrome พญ.น นทพร เต มพรเล ศ Outline Refeeding Syndrome What is refeeding syndrome? What Electrolytes and minerals are involved? Who is at risk? How to manage
Prevention of Electrolyte Disorders Refeeding Syndrome พญ.น นทพร เต มพรเล ศ Outline Refeeding Syndrome What is refeeding syndrome? What Electrolytes and minerals are involved? Who is at risk? How to manage
POTASSIUM DIHYDROGEN PHOSPHATE 13.6% CONCENTRATED INJECTION
 POTASSIUM DIHYDROGEN PHOSPHATE 13.6% CONCENTRATED INJECTION NAME OF THE MEDICINE Potassium Dihydrogen Phosphate Synonyms: potassium biphosphate, potassium acid phosphate, monopotassium phosphate, or monoibasic
POTASSIUM DIHYDROGEN PHOSPHATE 13.6% CONCENTRATED INJECTION NAME OF THE MEDICINE Potassium Dihydrogen Phosphate Synonyms: potassium biphosphate, potassium acid phosphate, monopotassium phosphate, or monoibasic
Drugs Used in Heart Failure. Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia
 Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to
Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
Hello, and thank you for joining us for this presentation on novel approaches to understanding risks and treatment of hyperkalemia.
 Hello, and thank you for joining us for this presentation on novel approaches to understanding risks and treatment of hyperkalemia. PP-US-DSE-00032. 2015 Relypsa, Inc. All rights reserved. Relypsa and
Hello, and thank you for joining us for this presentation on novel approaches to understanding risks and treatment of hyperkalemia. PP-US-DSE-00032. 2015 Relypsa, Inc. All rights reserved. Relypsa and
VanderbiltEM.com. ACEP 2013 Electrolyte Emergencies. Mastering Emergency Medicine. Electrolyte Emergency Questions. Electrolyte Emergency Questions
 ACEP 2013 Electrolyte Emergencies VanderbiltEM.com Camiron L. Pfennig, M.D. Corey M. Slovis, M.D. Vanderbilt University Medical Center Nashville, TN Mastering Emergency Medicine Secure the ABC s Consider
ACEP 2013 Electrolyte Emergencies VanderbiltEM.com Camiron L. Pfennig, M.D. Corey M. Slovis, M.D. Vanderbilt University Medical Center Nashville, TN Mastering Emergency Medicine Secure the ABC s Consider
RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University
 RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University OBJECTIVES By the end of this lecture each student should be able to: Define acute & chronic kidney disease(ckd)
RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University OBJECTIVES By the end of this lecture each student should be able to: Define acute & chronic kidney disease(ckd)
3.Which is not a cause of hypokalemia? a) insulin administration b) adrenaline infusion c) alkalosis d) toluene toxicity e) digoxin OD
 insulin administration b) adrenaline infusion c) alkalosis d) toluene toxicity e) digoxin OD") Fluids and Electrolytes MCQs 1Which is incorrect with regards to the fluid and its content? a) Normal Saline 150mmol Na+/L b) Hartmans 131mmol Na+/L c) Hartmans 131mmolCl-/L d) D5W- 50gm glucose/l e) Hartmans-
Fluids and Electrolytes MCQs 1Which is incorrect with regards to the fluid and its content? a) Normal Saline 150mmol Na+/L b) Hartmans 131mmol Na+/L c) Hartmans 131mmolCl-/L d) D5W- 50gm glucose/l e) Hartmans-
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari
![Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari](/thumbs/90/104323364.jpg "Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari") Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Electrolyte Emergencies
 Electrolyte Emergencies Hyponatremia/hypernatremia Hypokalemia/hyperkalemia Hypocalcemia/hypercalcemia Hypomagnesemia/hypermagnesemia Hypophosphatemia/hyperphosphatemia Hyponatremia Symptomatic: headaches,
Electrolyte Emergencies Hyponatremia/hypernatremia Hypokalemia/hyperkalemia Hypocalcemia/hypercalcemia Hypomagnesemia/hypermagnesemia Hypophosphatemia/hyperphosphatemia Hyponatremia Symptomatic: headaches,
You Don t Want to Miss This One! Focus on can t miss EKG tracings
 You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
*Excess sodium loss through N-V-D, skin and kidneys *Excess diuretic dosage *Liver Failure *CHF *Increased hypotonic IV fluids
 I. Blood Chemistries Sodium: Hyponatremia Normal: 135-145 meq/l Patho Ranges Causes Treatments Nsg. Considerations Serum below 135mEq/L *Most abundant cation in EXTRAcellular fluid *Maintains osmotic pressure
I. Blood Chemistries Sodium: Hyponatremia Normal: 135-145 meq/l Patho Ranges Causes Treatments Nsg. Considerations Serum below 135mEq/L *Most abundant cation in EXTRAcellular fluid *Maintains osmotic pressure
Saint-Antoine Hospital, Paris. Medical Intensive Unit Care. Hafid Ait-Oufella, MD.PhD. Dyscalcemia. Dyskalemia
 Dyskalemia Dyscalcemia Hafid Ait-Oufella, MD.PhD. Medical Intensive Unit Care Saint-Antoine Hospital, Paris Potassium K + Molecular weight: 39 1gr K + =2.5mmol Potassium disorders in ICU : Our experience
Dyskalemia Dyscalcemia Hafid Ait-Oufella, MD.PhD. Medical Intensive Unit Care Saint-Antoine Hospital, Paris Potassium K + Molecular weight: 39 1gr K + =2.5mmol Potassium disorders in ICU : Our experience
Salicylate (Aspirin) Ingestion California Poison Control Background 1. The prevalence of aspirin-containing analgesic products makes
 Ingestion California Poison Control Background 1. The prevalence of aspirin-containing analgesic products makes") Salicylate (Aspirin) Ingestion California Poison Control 1-800-876-4766 Background 1. The prevalence of aspirin-containing analgesic products makes these agents, found in virtually every household, common
Salicylate (Aspirin) Ingestion California Poison Control 1-800-876-4766 Background 1. The prevalence of aspirin-containing analgesic products makes these agents, found in virtually every household, common
NHS Grampian Staff Guideline for the Management of Acute Hypokalaemia in Adults
 NHS Grampian Staff Guideline for the Management of Acute Hypokalaemia in Adults Co-ordinators: Medicines Information Pharmacist Consultation Group: See relevant page in guidance Approver: Medicine Guidelines
NHS Grampian Staff Guideline for the Management of Acute Hypokalaemia in Adults Co-ordinators: Medicines Information Pharmacist Consultation Group: See relevant page in guidance Approver: Medicine Guidelines
PRINCIPLES OF DIURETIC ACTIONS:
 DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
Diuretic Use in Neonates
 Neonatal Nursing Education Brief: Diuretic Use in the Neonate http://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/ Diuretics
Neonatal Nursing Education Brief: Diuretic Use in the Neonate http://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/ Diuretics
Medication Review. Renal Drugs. Pharmacy Technician Training Systems Passassured, LLC
 Medication Review Renal Drugs Pharmacy Technician Training Systems Passassured, LLC Medication Review, Renal Drugs PassAssured's Pharmacy Technician Training Program Medication Review Renal Drugs Click
Medication Review Renal Drugs Pharmacy Technician Training Systems Passassured, LLC Medication Review, Renal Drugs PassAssured's Pharmacy Technician Training Program Medication Review Renal Drugs Click
Diabetic Ketoacidosis
 Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Important Prescribing Information
 Important Prescribing Information Subject: Temporary importation of Potassium Chloride (KCl) Injection, Concentrate, 2 meq/ml to address drug shortage issues July 11, 2018 Dear Healthcare Professional,
Important Prescribing Information Subject: Temporary importation of Potassium Chloride (KCl) Injection, Concentrate, 2 meq/ml to address drug shortage issues July 11, 2018 Dear Healthcare Professional,
PACKAGE LEAFLET: INFORMATION FOR THE USER. CALCICLO STEROP 11 meq 10 ml Solution for injection. Dihydrated Calcium Chloride
 PACKAGE LEAFLET: INFORMATION FOR THE USER CALCICLO STEROP 11 meq 10 ml Solution for injection Dihydrated Calcium Chloride Read all of this leaflet carefully before you start using this medicine because
PACKAGE LEAFLET: INFORMATION FOR THE USER CALCICLO STEROP 11 meq 10 ml Solution for injection Dihydrated Calcium Chloride Read all of this leaflet carefully before you start using this medicine because
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
A case of DYSELECTROLYTEMIA. Dr. Prathyusha Dr. Lalitha janakiraman s unit
 A case of DYSELECTROLYTEMIA Dr. Prathyusha Dr. Lalitha janakiraman s unit CASE SUMMARY 4 month old, female infant 1 st born to NC parents, term, b.wt: 3.25kg No neonatal hospitalization Attained head control
A case of DYSELECTROLYTEMIA Dr. Prathyusha Dr. Lalitha janakiraman s unit CASE SUMMARY 4 month old, female infant 1 st born to NC parents, term, b.wt: 3.25kg No neonatal hospitalization Attained head control
Chapter 20 8/23/2016. Fluids and Electrolytes. Fluid (Water) Fluid (Water) (Cont.) Functions
 Fluid (Water) (Cont.) Functions") Chapter 20 Fluids and Electrolytes All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Fluid (Water) Functions Provides an extracellular transportation
Chapter 20 Fluids and Electrolytes All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Fluid (Water) Functions Provides an extracellular transportation
Case Report WenckebachBlockduetoHyperkalemia:ACaseReport
 Emergency Medicine International Volume 2010, Article ID 879751, 4 pages doi:10.1155/2010/879751 Case Report WenckebachBlockduetoHyperkalemia:ACaseReport Aparajita Sohoni, Berenice Perez, and Amandeep
Emergency Medicine International Volume 2010, Article ID 879751, 4 pages doi:10.1155/2010/879751 Case Report WenckebachBlockduetoHyperkalemia:ACaseReport Aparajita Sohoni, Berenice Perez, and Amandeep
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
K-TAB (potassium chloride extended-release tablets, USP)
") K-TAB (potassium chloride extended-release tablets, USP) DESCRIPTION K-TAB (potassium chloride extended-release tablets) is a solid oral dosage form of potassium chloride containing 8 meq, 10 meq and 20
K-TAB (potassium chloride extended-release tablets, USP) DESCRIPTION K-TAB (potassium chloride extended-release tablets) is a solid oral dosage form of potassium chloride containing 8 meq, 10 meq and 20
Electrolyte Abnormalities in the Transplant Recipient
 Electrolyte Abnormalities in the Transplant Recipient Michael J. Goldstein, MD Assistant Professor of Surgery Overview Sodium Potassium Calcium Magnesium Phosphorus Sodium Balance Na + determines extracellular
Electrolyte Abnormalities in the Transplant Recipient Michael J. Goldstein, MD Assistant Professor of Surgery Overview Sodium Potassium Calcium Magnesium Phosphorus Sodium Balance Na + determines extracellular
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!!
 Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Chapter 26. Media Directory. Dysrhythmias. Diagnosis/Treatment of Dysrhythmias. Frequency in Population Difficult to Predict
 Chapter 26 Drugs for Dysrythmias Slide 33 Slide 35 Media Directory Propranolol Animation Amiodarone Animation Upper Saddle River, New Jersey 07458 All rights reserved. Dysrhythmias Abnormalities of electrical
Chapter 26 Drugs for Dysrythmias Slide 33 Slide 35 Media Directory Propranolol Animation Amiodarone Animation Upper Saddle River, New Jersey 07458 All rights reserved. Dysrhythmias Abnormalities of electrical
PRODUCT MONOGRAPH UROCIT -K. (Potassium Citrate Extended-Release Tablets, USP)
") PRODUCT MONOGRAPH UROCIT -K (Potassium Citrate Extended-Release Tablets, USP) Renal Stone treatment in patients with hypocitraturia or uric acid lithiasis Mission Pharmacal Company Date of Revision: 10999
PRODUCT MONOGRAPH UROCIT -K (Potassium Citrate Extended-Release Tablets, USP) Renal Stone treatment in patients with hypocitraturia or uric acid lithiasis Mission Pharmacal Company Date of Revision: 10999
Should we be moving away from Kayexalate (Sodium Polystyrene Sulfonate)?
?") Should we be moving away from Kayexalate (Sodium Polystyrene Sulfonate)? Shermaine Ngo, LMPS Pharmacy Resident Preceptor: Joanie Tulloch, Emergency Medicine Rotation May 2017 1 Learning Objectives Describe
Should we be moving away from Kayexalate (Sodium Polystyrene Sulfonate)? Shermaine Ngo, LMPS Pharmacy Resident Preceptor: Joanie Tulloch, Emergency Medicine Rotation May 2017 1 Learning Objectives Describe
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1
 K E M I A D E Y E R I, P G Y - 1") DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
Metabolic Abnormalities in Critically Ill Patients
 CHAPTER 66 Metabolic Abnormalities in Critically Ill Patients A. M. Bhagwati Introduction Critically ill patients have a unique set of problems, ranging from metabolic, endocrine, nutritional, respiratory
CHAPTER 66 Metabolic Abnormalities in Critically Ill Patients A. M. Bhagwati Introduction Critically ill patients have a unique set of problems, ranging from metabolic, endocrine, nutritional, respiratory
KEVEYIS (dichlorphenamide) oral tablet
 oral tablet") KEVEYIS (dichlorphenamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
KEVEYIS (dichlorphenamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
Kidneycentric. Follow this and additional works at:
 Washington University School of Medicine Digital Commons@Becker All Kidneycentric 2014 Gitelman syndrome David Steflik Washington University School of Medicine in St. Louis Follow this and additional works
Washington University School of Medicine Digital Commons@Becker All Kidneycentric 2014 Gitelman syndrome David Steflik Washington University School of Medicine in St. Louis Follow this and additional works
Fluid & Electrolyte Balances in Term & Preterm Infants. Carolyn Abitbol, M.D. University of Miami/ Holtz Children s Hospital
 Fluid & Electrolyte Balances in Term & Preterm Infants Carolyn Abitbol, M.D. University of Miami/ Holtz Children s Hospital Objectives Review maintenance fluid & electrolyte requirements in neonates Discuss
Fluid & Electrolyte Balances in Term & Preterm Infants Carolyn Abitbol, M.D. University of Miami/ Holtz Children s Hospital Objectives Review maintenance fluid & electrolyte requirements in neonates Discuss
FLUIDS/ELECTROLYTES. Sahir Kalim, MD MMSc. Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School
 FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
5AB Dysrhythmia Interpretation and Management 2016
 5AB Dysrhythmia Interpretation and Management 2016 How to complete your biennial ECG review: A website has been created that contains the basic review information. Use this as a reference during your review.
5AB Dysrhythmia Interpretation and Management 2016 How to complete your biennial ECG review: A website has been created that contains the basic review information. Use this as a reference during your review.
A case of severe hyperkalaemia presenting with cardiac arrythmias: An uncommon initial manifestation of chronic kidney disease
 Case Report A case of severe hyperkalaemia presenting with cardiac arrythmias: An uncommon initial manifestation of chronic kidney disease D H Sudusinghe 1, J indrakumar 2 1 Department of Physiology, Faculty
Case Report A case of severe hyperkalaemia presenting with cardiac arrythmias: An uncommon initial manifestation of chronic kidney disease D H Sudusinghe 1, J indrakumar 2 1 Department of Physiology, Faculty
Fundamentals of Pharmacology for Veterinary Technicians Chapter 8
 Figure 8-1 Figure 8-2 Figure 8-3 Figure 8-4 Figure 8-5 Figure 8-7 Figure 8-8 Figure 8-9 TABLE 8-1 Blood Flow Through the Heart The right atrium receives blood from all tissues, except the lungs, through
Figure 8-1 Figure 8-2 Figure 8-3 Figure 8-4 Figure 8-5 Figure 8-7 Figure 8-8 Figure 8-9 TABLE 8-1 Blood Flow Through the Heart The right atrium receives blood from all tissues, except the lungs, through
Proceedings of the Southern European Veterinary Conference - SEVC -
 Close this window to return to IVIS www.ivis.org Proceedings of the Southern European Veterinary Conference - SEVC - Sep. 30-Oct. 3, 2010, Barcelona, Spain Next SEVC Conference: Sep. 30-Oct. 2, 2011 -
Close this window to return to IVIS www.ivis.org Proceedings of the Southern European Veterinary Conference - SEVC - Sep. 30-Oct. 3, 2010, Barcelona, Spain Next SEVC Conference: Sep. 30-Oct. 2, 2011 -
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Low Efficacy Diuretics. Potassium sparing diuretics. Carbonic anhydrase inhibitors. Osmotic diuretics. Miscellaneous
 University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
Electrolyte Disorders in ICU. Debashis Dhar
 Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries
Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries
Fluid & Elyte Case Discussion. Hooman N IUMS 2013
 Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
Full file at
 MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) What electrical event must occur for atrial kick to occur? 1) A) Atrial repolarization B) Ventricular
MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) What electrical event must occur for atrial kick to occur? 1) A) Atrial repolarization B) Ventricular
Composition: Each Tablet contains. Pharmacokinetic properties:
 Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
The CKD patient in the office or ER. Dr. Vincent Cheung Nephrologist Peterborough Regional Renal Program November 9 th, 2016
 The CKD patient in the office or ER Dr. Vincent Cheung Nephrologist Peterborough Regional Renal Program November 9 th, 2016 Presenter Disclosure Dr. Vincent Cheung Relationships with commercial interests
The CKD patient in the office or ER Dr. Vincent Cheung Nephrologist Peterborough Regional Renal Program November 9 th, 2016 Presenter Disclosure Dr. Vincent Cheung Relationships with commercial interests
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Nursing Process Focus: Patients Receiving Dextran 40 (Gentran 40)
") Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Table 1. Diuretics. Drugs Mechanisms of Action Indications Adverse Drug Effects. Table 2. Electrolyte Modifiers.
 Table 1. Diuretics. hydrochlorothiazide 23 furosemide 23 triamterene 23 Inhibits sodium reabsorption at the distal convoluted tubule Inhibits sodium reabsorption at the loop of Henle Competitive inhibitor
Table 1. Diuretics. hydrochlorothiazide 23 furosemide 23 triamterene 23 Inhibits sodium reabsorption at the distal convoluted tubule Inhibits sodium reabsorption at the loop of Henle Competitive inhibitor
Heart Failure. Dr. Alia Shatanawi
 Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
50% Concentrated Injection
 NAME OF THE MEDICINE. The molecular weight of the compound is 246.5 and the CAS registry number is 10034-99-8. The molecular formula is MgSO4, 7H2O. DESCRIPTION MAGNESIUM SULFATE HEPTAHYDRATE 50% CONCENTRATED
NAME OF THE MEDICINE. The molecular weight of the compound is 246.5 and the CAS registry number is 10034-99-8. The molecular formula is MgSO4, 7H2O. DESCRIPTION MAGNESIUM SULFATE HEPTAHYDRATE 50% CONCENTRATED
Water Reabsorption and the Effect of Diuretics on Urine Formation Patricia J. Clark, Ph.D. Department of Biology, IUPUI
 Water Reabsorption and the Effect of Diuretics on Urine Formation Patricia J. Clark, Ph.D. Department of Biology, IUPUI This activity may be done in conjunction with a more traditional urinalysis lab.
Water Reabsorption and the Effect of Diuretics on Urine Formation Patricia J. Clark, Ph.D. Department of Biology, IUPUI This activity may be done in conjunction with a more traditional urinalysis lab.
Wk 10. Management of Clients with Diabetes Mellitus
 Wk 10. Management of Clients with Diabetes Mellitus 2. Acute complications of DM 1) Hyperglycemia and diabetic ketoacidosis Hyperglycemia: glycogenolysis gluconeogenesis 1) Etiology and Risk Factors Taking
Wk 10. Management of Clients with Diabetes Mellitus 2. Acute complications of DM 1) Hyperglycemia and diabetic ketoacidosis Hyperglycemia: glycogenolysis gluconeogenesis 1) Etiology and Risk Factors Taking