Acknowledgement This training package was created by Joseph Schar and Chantelle Skinner. Please direct any questions to your CSO or Team Leader.
|
|
|
- Morris O’Connor’
- 5 years ago
- Views:
Transcription


1 Post-ROSC Management Acknowledgement This training package was created by Joseph Schar and Chantelle Skinner. Please direct any questions to your CSO or Team Leader. Offline Reading Download as PDF Welcome Introduction Post-Cardiac Arrest Syndrome Post-ROSC Management Paediatric Post-ROSC Management References
2 Summative Assessment Details Download PDF for of ine reading
3 Section 1 of 8 Welcome Welcome to the Post-ROSC Management clinical development package. This package will provide an overview of the key principles and priorities following return of circulation that are reflected in the new paramedic Post-ROSC Management CPG. It will outline a stepwise ABCDE approach to the post- ROSC patient and provide evidence summaries and best practice principles regarding optimal management following ROSC. References are provided should you wish to expand your knowledge. Overview and learning outcomes: Review the pathophysiology of the post-cardiac arrest syndrome. Review the key principles of post-rosc management in a stepwise ABCDE approach. Introduce the new changes to paramedic practice, including treating adults with hypotension and an altered conscious state; and Code STEMI activation. A summative assessment. Objective Successful completion of the online package will require at least 80% correct responses to the 12 MCQ. Once issued with an authority to practice (ATP) following this online package AND completion
4 of the paramedic 2-day conference you will be able to use the Post-ROSC Management CPG. The package will take approximately 45 minutes to complete.
5 Section 2 of 8 Introduction Post-return of spontaneous circulation (ROSC) management is an important step in the continuum of resuscitation. The quality of treatment provided in the post-cardiac arrest period the final ring in the Chain of Survival significantly influences the patient s ultimate outcome. [1] Resuscitation councils, including ANZCOR, have separate post-rosc guidelines from cardiac arrest guidelines. This recognises the distinct importance of management in this period. While there is a paucity of robust post-rosc literature, particularly pre-hospitally, studies have indicated negative outcomes associated with sub-optimal ROSC management.2 Therefore, up to date guidance that supports our delivery of optimal post-rosc management is the motivation for the development of a CPG. While tailoring our post-rosc care to the individual patient needs takes precedence, general principles in the CPG will standardise the management and expectations across clinical levels and articulate what is considered best practice. A difficult, but essential, skill is to be able to adapt our thinking once ROSC is achieved. We should be expecting ROSC in our cardiac arrest patients and have a clear plan to manage the patient when it occurs. The post-rosc patient is now a very different patient with different needs and priorities to the one that was in cardiac arrest. As such, we need to have the ability to mentally re-dispatch ourselves to this new critically unwell patient who may now also be affected by the post-cardiac arrest syndrome. This e-learning package provides a background, evidence summaries and practical recommendations relevant to every dot point in the new Post-ROSC Management CPG. The CPG details are displayed in text boxes, followed by the rationale for their inclusion in this new guideline.
6 CPG-120-P - Post-ROSC Management (Paramedic) CPG
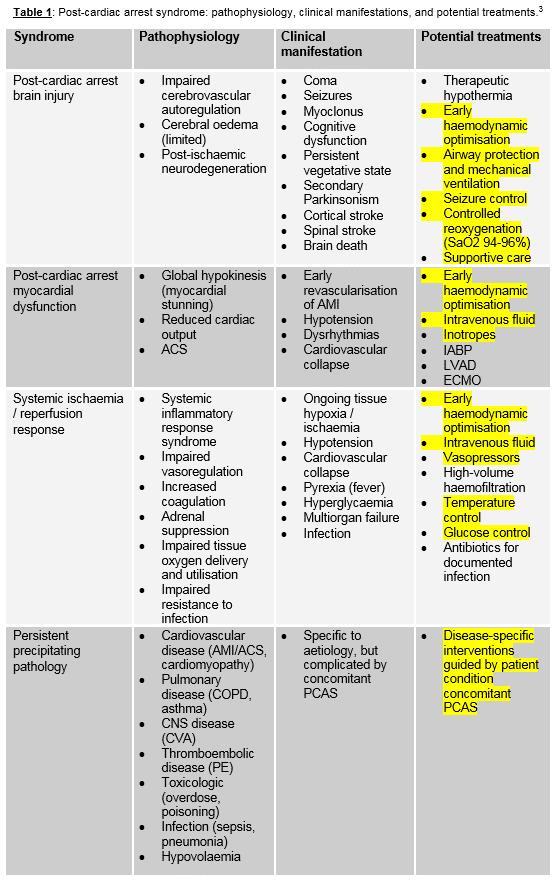
7 Section 3 of 8 Post-Cardiac Arrest Syndrome The International Liaison Committee on Resuscitation (ILCOR) in 2008 published a consensus statement detailing the post-cardiac arrest syndrome. The syndrome has 4 key components: 1 Post-cardiac arrest brain injury 2 Post-cardiac arrest myocardial dysfunction 3 Systemic ischaemia / reperfusion response, and 4 Persistent precipitating pathology. Patients who achieve ROSC following cardiac arrest have a high mortality rate that can be attributed to a unique pathophysiological process that involves multiple organs. These are often superimposed on the disease or injury that caused the cardiac arrest as well as underlying co-morbidities. Injury caused by global ischaemia during the cardiac arrest is compounded by additional damage that occurs during and after reperfusion. The severity of the post-cardiac arrest syndrome will vary between patients and depend on the time in cardiac arrest, the cause of the arrest and pre-morbid health. It may not occur at all if the cardiac arrest is brief. [3]
8 Table 1 illustrates the components of the post-cardiac arrest syndrome and their pathophysiology, clinical manifestations and potential treatments. Note: the potential treatments that are highlighted are what we can offer prior to hospital arrival.
9
10 AMI indicates acute myocardial infarction; ACS, acute coronary syndrome; IABP, intraaortic balloon pump; LVAD, left ventricular assist device; EMCO, extracorporeal membrane oxygenation; COPD, chronic obstructive pulmonary disease; CNS, central nervous system; CVA, cerebrovascular accident; PE, pulmonary embolism; and PCAS, post cardiac arrest syndrome. 1. Post-cardiac arrest brain injury A common cause of morbidity and mortality following cardiac arrest is brain injury. The brain has little tolerance to ischaemia and a unique response to reperfusion. The mechanisms of brain injury following cardiac arrest are complex and can continue for hours to days. It has been shown that an initial period of hyperaemia occurs in the first few minutes following ROSC due to elevated cerebral perfusion pressures and impaired cerebrovascular autoregulation, followed by vasospasm and hypoperfusion.3 Post-cardiac arrest brain injury may be exacerbated by hypotension, hypo/hypercarbia, hypo/hyperoxaemia, pyrexia, hypo/hyperglycaemia, and seizures. [1] These factors can be minimised, addressed or prevented by our meticulous attention to optimal post- ROSC management. 2. Post-cardiac arrest myocardial dysfunction Significant myocardial dysfunction is common after cardiac arrest, is usually responsive to treatment and is usually reversible. Transient increases in circulating catecholamine (e.g. adrenaline, noradrenaline) concentrations immediately following ROSC often result in increased HR and BP. Myocardial dysfunction can occur early in the post-rosc phase and is characterised by alterations in HR, rhythm and hypotension. It can occur despite preserved coronary blood flow, indicating a stunning phenomenon as opposed to infarction or permanent injury. 3. Systemic ischaemia / reperfusion syndrome The whole-body ischaemia that occurs during cardiac arrest and the reperfusion that occurs post- ROSC results in a number of processes that contribute to multiple organ failure. Thus, the post-
11 cardiac arrest syndrome has many similar pathophysiological processes to that of severe sepsis. Consequently, it shares many clinical manifestations such as intravascular volume depletion, vasodilation and impaired vasoregulation, impaired oxygen delivery and utilisation, and increased susceptibility to infection. [3] 4. Persistent precipitating pathology The precipitating pathology that caused / contributed to the cardiac arrest can complicate, and be complicated by, the simultaneous pathophysiology of the post-cardiac arrest syndrome. This needs to be rapidly identified and addressed. Having a high suspicion of the cause of the arrest can influence your management approach to the post-rosc patient. The most common pathology causing out of hospital cardiac arrest is acute coronary syndrome. Other common non-cardiac causes include pulmonary disease, CNS disease, PE, overdose/poisoning, sepsis, and trauma. Consider and correct where possible the reversible causes of cardiac arrest: Hypoxia Hypovolaemia Hyper / hypokalaemia / metabolic disorders Hypothermia / hyperthermia Tension pneumothorax Tamponade Toxins Thrombosis (pulmonary / coronary) Practice Question
12 Potential treatments to minimise and address components of the postcardiac arrest syndrome include: Airway protection and mechanical ventilation Early haemodynamic optimisation Seizure control Glucose control All of the other answers SUBMIT
13 Section 4 of 8 Post-ROSC Management Post cardiac arrest management can be defined in several phases: the immediate (0-20 mins) and early (20 min 6-12 hrs) phases, when early interventions may be most effective the intermediate (6-12 hrs 72 hrs) phase, when injury pathways are still active and aggressive treatment is often required the recovery (>72 hrs) phase, when prognostication is more reliable and the patient outcomes become more predictable. Click on the button to the right of this page to work through this section.

14 Page 1 of 17 Phases of post-cardiac arrest syndrome. Figure 1: Phases of post-cardiac arrest syndrome. [3] The immediate and early phases of post-rosc management aim to prevent cardiac arrest recurrence, provide organ support, and limit ongoing injury. Management priorities include requesting clinical support, treating precipitating causes, and preparing for rapid transport. For simplicity and consistency, the patient should be treated following the ABCDE approach. A full set of observations should be taken to establish a baseline condition and identify abnormalities that need to be addressed. Where the cause of the cardiac arrest is known, tailor your post-rosc management to the patient s particular dysfunction or disease by referring to relevant CPGs. This includes following a traumatic cardiac arrest, where management and treatment priorities may be determined by the patient s injuries.
15 Page 2 of 17 Airway Once ROSC is achieved, re-assessment of the airway should occur. If a supraglottic airway (SGA) is in place then this needs to be reviewed to ensure it is optimally positioned. After any movements, such as extrication, airway re-assessment should always be a priority to ensure the SGA remains optimally placed and with a good seal. Suctioning should occur as required. If a patient has neurological recovery post-rosc where they are gagging on the SGA or becoming significantly agitated because of its placement, it is reasonable to remove the SGA, consider another airway adjunct if tolerated, and continue oxygenation. Gagging and agitation will increase the patient s plasma catecholamine concentrations, which may provoke raised intracranial pressures, hypertension, or arrhythmias. [1]
16 Page 3 of 17 Breathing Clinical Practice Guideline Avoid hyperventilation. Start at 10 breaths / min and consider ventilation strategy. Continue waveform capnography monitoring. Avoid excessive ventilation volumes. Some patients will regain spontaneous respirations following ROSC. If these patients have an advanced airway in place and/or the bag-valve mask is being held over their face then gentle assistance with ventilations should occur. This is particularly important for paediatrics and patients with reduced ventilatory function. Following cardiac arrest, sub-optimal respiratory management has been associated with worse outcomes. [2] Post-ROSC, patients blood carbon dioxide levels and ph are controlled by ventilations. Ventilation strategy refers to the rate, volume and pressures delivered during IPPV. Optimal ventilation of the post-rosc patient balances the need to reverse hypoxia and acidosis with the potential deleterious effects of hyperventilation, hypocapnia and hyperoxia. [4] We will explore these individually.
![Page 4 of 17 Breathing - Hyperventilation Figure 2: Cerebral Blood flow dependence on PCO 2 [20] Hyperventilation (from excessive respiratory rates, tidal volumes, or both) is common and can have](/docs-images/92/109561150/images/17-0.jpg "adverse effects on haemodynamics and carbon dioxide levels in the blood (PaC0 2 ).")
17 Page 4 of 17 Breathing - Hyperventilation Figure 2: Cerebral Blood flow dependence on PCO 2 [20] Hyperventilation (from excessive respiratory rates, tidal volumes, or both) is common and can have adverse effects on haemodynamics and carbon dioxide levels in the blood (PaC0 2 ). Hyperventilating a patient post- ROSC can cause increases in intrathoracic pressure, which can decrease preload and result in reduced cardiac output and coronary perfusion pressure. [4] This could be deleterious in patients with haemodynamic compromise. Hyperventilation can also expel high concentration of carbon dioxide. This can lead to low carbon dioxide levels in the blood (hypocapnia). Hyperventilation causing hypocapnia can result in cerebral vasoconstriction, which can markedly reduce cerebral blood flow and lead to harmful cerebral ischaemia. Figure 2 shows the relationship between arterial PC0 2 and changes in cerebral blood flow. Note the significant percentage reduction of cerebral blood flow as blood carbon dioxide levels drop. An association between hypocapnia and poor neurological outcome is commonly reported in the literature. [1] Therefore, avoiding hypocapnia, and hyperventilation, is important.
18 While hyperventilation can cause hypocapnia, hypoventilation can result in further increases in a patient s blood carbon dioxide levels (hypercapnia). Hypercapnia can also contribute to secondary brain injury and may increase the likelihood of a further cardiac arrest.
19 Page 5 of 17 Breathing - Capnography Figure 3: Waveform capnography demonstrating loss of ROSC We are currently unable to measure a patient s blood carbon dioxide levels in the pre-hospital environment, as it requires arterial blood gas (ABG) testing. If the waveform capnography was attached during cardiac arrest then an end-tidal carbon dioxide (EtC0 2 ) number will be displayed. Capnography use for paramedics is outlined in the paramedic capnography e-learning package and will be further discussed at the paramedic conferences. The EtC0 2 number may give us an indication of a patient s blood carbon dioxide levels but there are many factors following cardiac arrest that cause alterations in EtC0 2 numbers that don t accurately correspond with blood carbon dioxide levels. Therefore, it is not recommended that paramedics use EtC0 2 numbers to guide ventilation strategy after cardiac arrest. Following ROSC, waveform capnography still has several important functions: Monitor ventilation rates. Monitor waveform trends. Display characteristic waveform patterns e.g. shark fin pattern indicating obstruction. A marker of cardiac output and loss of ROSC.
20 Figure 3 displays a waveform capnography pattern that occurs when a patient has a sudden loss in cardiac output eg. loss of ROSC. Any sudden change in waveform trend should be a prompt to re-check your patient s cardio-respiratory status.
21 Page 6 of 17 Breathing - Ventilation rates Following ROSC, ventilations should continue at a rate of 10 breaths / minute. This is considered a reasonable starting point (and may be continued thereafter if appropriate), which balances avoiding hyperventilation (and hypocapnia) and further increasing hypercapnia. For simplicity, one breath every 6 seconds will deliver a rate of 10 breaths / minute. This strategy has been recommended in guidelines5 and has been adopted by ambulance services in Australia and internationally. The optimal IPPV rate and volume following ROSC may differ between patients and many factors should be taken into consideration, including the cause of the arrest. For example, an asthmatic arrest who is now post- ROSC is likely to have a severely hyper-inflated chest and will require slow ventilation rates (and smaller tidal volumes) to allow for adequate chest deflation. This should occur according to the Asthma CPG.
22 Page 7 of 17 Breathing - Ventilation volumes Measuring and approximating ventilation volumes is difficult in our environment. The aim is to provide just enough volume to see rise and fall of the chest. Delivering high ventilation volumes, especially with an advanced airway in place, can cause lung injury as well as potentially effecting haemodynamics and carbon dioxide levels.
23 Page 8 of 17 Breathing - Oxygen Therapy Clinical Practice Guideline - Continue high-flow oxygen therapy: For patients requiring assisted ventilations, continue oxygen 15L/min. For patients not requiring assisted ventilations, re-assess and apply optimal oxygen to maintain Sp %. If Sp0 2 is unreliable, maintain high-flow oxygen. The optimal Sp0 2 range following ROSC has not been firmly established. Observational studies have frequently and consistently reported increased mortality and worse outcomes associated with hypoxemia (low PaO 2 ) following cardiac arrest.6 Maintaining Sp0 2 94% at all times is currently recommended. The administration of prolonged periods of high flow oxygen after ROSC has long been standard practice. Maximising oxygen delivery for several hours has been on the premise that patients have been severely hypoxic during the cardiac arrest and therefore might benefit from lots of oxygen post-rosc. Avoiding hypoxia has been, and still is, the most significant priority. Until recently there has been little evidence to support a change in this approach. However, recent studies have identified possible harm associated with excessive oxygen administration (hyperoxia) leading to very high Pa0 2 (hyperoxaemia). [7-8] No well powered randomised control trials have yet tested the pre-hospital titration of oxygen following ROSC on outcomes. However, SAAS has been, and will be, participating in important research in this area. The reduction of oxygen After Cardiac arrest (EXACT) study is a multi-centre, randomised, controlled trial (RCT) that will assess whether titrating oxygen to target saturations following ROSC improves outcome at hospital discharge. This study period will supersede standard oxygen administration guidelines. Outside of this study enrolment period, the current SAAS position is to continue high flow oxygen therapy in the immediate post- ROSC period. For patients who require assisted ventilations with the BVM (with or without an advanced airway), oxygen flow should remain at 15L/min. Patients who have had a brief cardiac arrest and have responded immediately to appropriate treatment may achieve return of normal cerebral function. These patients may not require oxygenation and ventilation through a BVM or advanced airway. Once a reliable Sp0 2 measurement occurs, optimal oxygen should be applied to maintain Sp %. The priority here is avoiding hypoxia, hence oxygen therapy must still be
24 initiated at high-flow and Sp02 measurements closely monitored. If a patient has a good neurological function, is maintaining their own airway, is self-ventilating with a reliable Sp0 2 > 98% on high flow oxygen, it is reasonable to titrate the oxygen to achieve a target saturation between 94-98%. This target saturation is recommended in ANZCOR Guideline [9] If at any point the Sp0 2 reading is considered to be an unreliable reading (eg poor peripheral perfusion, anaemic patient) or the Sp0 2 does not have a reliable trace, maintain or increase oxygen therapy to high flow. Preventing hypoxic episodes is considered more important than avoiding any potential risk of hyperoxia. [5]
25 Page 9 of 17 Breathing - Posture Clinical Practice Guideline: Optimise posture Following ROSC, consider the most appropriate posture for your patient. Raising the patient s head up to 30 may help prevent aspiration, improve lung mechanics and lower intracranial pressure (ICP).[4] However, this may not be appropriate in hypotensive patients or where C-spine precautions are applied. Raising the head up may be difficult to achieve on scene but is a consideration once the patient is on the stretcher. Ensure this does not obstruct your view of the patient.
26 Page 10 of 17 Breathing - Examination Clinical Practice Guideline: Perform chest examination, including auscultation of the lungs. Look at the patient s chest for symmetrical chest movement. Auscultate to ensure equal breath sounds bilaterally. If ribs have been fractured during chest compression (documented in up to 70% of OHCA receiving CPR) be aware of a potential pneumothorax. [1] Listen also for evidence of pulmonary oedema or other abnormalities.
27 Page 11 of 17 Circulation - Blood Pressure Management Clinical Practice Guideline - For adults with hypotension and altered conscious state: Administer sodium chloride 0.9% IV in 250 ml aliquots until a radial pulse is achieved or SBP=100 mmhg, to a maximum of 10 ml/kg up to 1000 ml. Reassess patient after each 250 ml and cease IV fluids if patient shows signs of pulmonary oedema. Consult with a SAAS Medical Practitioner via the EOC Clinician if hypotension persists. Haemodynamic instability is common post-rosc. Post-cardiac arrest myocardial dysfunction, impaired vasoregulation, and intravascular volume depletion can result in hypotension and arrhythmias.1 When considering BP goals post-rosc there is a balance between providing adequate perfusion to a brain that may have lost its autoregulatory ability with the potential for overstressing a post-ischaemic heart. [4] Adequate blood pressure for optimal organ perfusion will vary between post-cardiac arrest patients and will be influenced by individual pre-morbid pathophysiology and factors associated with resuscitation. A common cause of morbidity and mortality following cardiac arrest is brain injury. The brain has little tolerance to ischaemia and a unique response to reperfusion. [3] Post-cardiac arrest brain injury may be exacerbated by hypotension. [1] Hypotension, defined as a systolic blood pressure (SBP) < mmhg, has been associated with higher mortality and diminished functional recovery following out of hospital cardiac arrest. [10-13] Additionally, hypoxic-ischaemic brain injury (HIBI) can occur immediately following ROSC and can result in cerebrovascular autoregulation dysfunction in some patients. In these patients, cerebral perfusion pressures become dependent on systemic blood pressure. [14] Paramedics do not currently have capacity in their guidelines to treat post-rosc hypotension, unless it is covered in other specific CPGs. This has been rectified within the new Paramedic Post-ROSC Management CPG. In patients who have an altered conscious state and are hypotensive, there is a risk that their cerebral perfusion is inadequate and not treating their hypotension could result in further cerebral ischaemia. Therefore, maintaining a minimum BP target is important. Patients who have a brief cardiac arrest and a return of a GCS=15 indicate that their cerebral perfusion is adequate, and treating to a higher BP is not currently recommended. It is extremely important to auscultate the patient s chest before commencing fluid therapy and after each
28 250ml aliquot. If the patient shows any sign of pulmonary oedema then fluid therapy must be ceased. This can be a sign of cardiac failure that will require additional treatment, and continuing fluid therapy in these patients can be harmful.
29 Page 12 of 17 Circulation - Coronary Reperfusion Considerations Clinical Practice Guideline: If ST elevation diagnostic of STEMI persists on the 12 lead ECG, activate the receiving hospital PCI team using the Code STEMI line (refer to Ischaemic Chest Pain CPG) and notify the receiving hospital early. The majority of OHCA cases are reported to have a cardiac origin, with obstructive coronary artery disease being the most dominant aetiology. [15] As part of a comprehensive post-rosc plan, an emphasis of directing management toward the early treatment of the underlying cause of the arrest is important. Use of coronary angiography and percutaneous coronary intervention (PCI) following OHCA has been reportedly increasing over the last decade, with an associated trend in survival to discharge in patients with post-arrest ECG STsegment elevation (STE). [16] Approximately 70% of patients who do present with ST elevation following out-of-hospital cardiac arrest (OHCA) are found to have an acute coronary occlusion. [17] This is comparable to findings of acute coronary syndrome (ACS) patients (who have not had a cardiac arrest) who undergo coronary angiography. [18-19] Since 2016, paramedics can activate the receiving hospital PCI-team in stable patients with STEMI. Following cardiac arrest, these patients do not fit current paramedic criteria for calling a code STEMI. However, these patients are regarded as the highest risk patients who may require immediate angiography. Therefore, the new Post-ROSC Management CPG enables paramedics to call a code STEMI following a cardiac arrest if ST elevation diagnostic of STEMI persists on the 12 lead ECG. Caution needs to be taken when immediately analyzing a post-rosc ECG. A post-ischaemic heart that has potentially had large doses of adrenaline during the arrest may take some time to settle into a stable rhythm and morphology, and interpretation of the ECG for ST elevation should wait until this occurs. It is also important to note that patients commonly have a GCS=3 or similar following OHCA, and with the new CPG this is not a contraindication for Code STEMI notification. Post-cardiac arrest patients will be considered unstable at the receiving ED and will be required to go directly to the resus room. However, the Code STEMI notification will inform the receiving Interventional Cardiologist and preparations can begin prior to your arrival. By activating a Code STEMI we are not committing a patient
30 to a particular procedure but identifying a high-risk patient who meets criteria for consideration. Whether the patient is then directed to the catheterization lab will be a decision for the receiving Doctors and Cardiology team. A Code STEMI notification should not take priority over other critical post-rosc management interventions. If you are close proximity to hospital then it may be more appropriate to notify the receiving hospital with your observations.
31 Page 13 of 17 Disability and Exposure Assessing a patient s neurological function post-rosc will include a GCS and pupillary examination. Performing a rapid secondary survey ensures that nothing has been missed. To examine the patient properly full body exposure may be necessary. These actions may give insight as to the cause of the cardiac arrest.
32 Page 14 of 17 Other Considerations - Blood Glucose Control Clinical Practice Guideline - For adults with hypoglycaemia: Administer glucose (10%) IV titrated to achieve a BGL between 4-10 mmol/l. Sodium chloride 0.9% 100 ml IV flush must be given before and after glucose IV. Avoid hyperglycaemia. Hyperglycaemia is common after cardiac arrest. A strong association exists between high BGL after resuscitation and poor neurological outcome. [4,9] Additionally, in critically ill patients severe hypoglycaemia is associated with increased mortality. Comatose patients are at risk of unrecognised hypoglycaemia; recording a BGL should be included as one of the post-rosc observations. If treating hypoglycaemia, administer the minimum amount of IV glucose to achieve a BGL within normal values (4-10 mmol/l). [4,9]
33 Page 15 of 17 Other Considerations - Temperature Management Clinical Practice Guideline: Maintain temperature within normal range ( C). Animal studies indicate that early cooling post-rosc results in improved outcomes but this has yet to be demonstrated in human trials. [1] Pre-hospital cooling has not demonstrated benefit despite large numbers of patients studied. [9] Post-ROSC patients usually have drops in temperature within the first hour and hospital admission temperatures following OHCA are usually between C. Temperatures less than 36 C may not be desired in patients with significant shock, myocardial dysfunction, or excessive risk of bleeding. [1] Therefore, if a post-rosc patient is hypothermic, consider applying blankets and space blankets to prevent further heat loss. Although the effect of elevated temperature on outcome is not proven, hyperthermia may aggravate ischaemia-reperfusion injury and neuronal damage through raised metabolic activity. [3] Passive cooling is appropriate for these patients, removing blankets and clothes to manage the hyperthermia. The overall aim of pre-hospital temperature management is to attempt to maintain a temperature within normal range.
34 Page 16 of 17 Other Considerations - Seizure Control Seizures are common after cardiac arrest and occur in approximately 30% of patients who remain comatose after ROSC. [1] Myoclonus is the most common seizure type, but focal and generalised tonic-clonic can also occur. Seizures can increase the cerebral metabolic rate up to 3-fold and prolonged seizures can exacerbate brain injury caused by cardiac arrest. Be alert for any seizure activity following ROSC. Treatment of post-rosc seizures should occur following relevant CPGs.
35 Page 17 of 17 Other Considerations - History If a clear history has not been obtained it is important to gather a comprehensive history as quickly as possible. Those involved with the patient prior to the cardiac arrest may have valuable insight into symptoms reported or actions prior, as well as the patient s physiological baseline (before the cardiac arrest). This history can be significant when the patient arrives at hospital and decisions are being made regarding appropriate treatment for the patient. Valuable information relating to the cardiac arrest should also be obtained, including time of the cardiac arrest, whether it was a witnessed arrest, and whether CPR or defibrillation occurred prior to SAAS arrival.
36 Section 5 of 8 Paediatric Post-ROSC Management The principles of paediatric post-rosc care are based around minimization and management of the components of the post-cardiac arrest syndrome. While much of the post-rosc management for adults includes reasonably standardized targets, paediatric intervention strategies are unique and therefore dependent on individual age, weight and normal physiological ranges expected of the child. For timely management of the anticipated physiological abnormalities in a paediatric post-rosc patient, early clinical support from a SAAS Medical Practitioner, via the EOC clinician, must occur. Paediatric cardiac arrest and return of circulation form a particularly small percentage of total ROSC seen by SAAS each year. However, each of these patients is significant, and changes to our understanding and management of post-rosc paediatric care can have a significant impact on the final outcome. As always, reversible causes including the 4 Hs and 4 Ts must be considered and treated whenever possible. With an anticipated ease of extrication compared to adults, transport of post-rosc paediatric patients should not be delayed. Click on the button to the right of this page to work through this section.

37 Page 1 of 6 Airway Paediatric cardiac arrest is less likely to be precipitated by a cardiac cause and is most commonly secondary to prolonged global hypoxaemia and ischaemia. [21] For this reason, close attention to airway and oxygenation in these patients is paramount. Posturing a paediatric patient correctly can have an impact on your ability to ventilate effectively and is an important component of your airway re-evaluation. This is of particular importance after any movement, after extrication and again prior to transport. Hyperextension of the neck can cause airway obstruction in small infants and should be avoided.
, decompress the stomach via the SGA gastric drainage tube.")
38 Page 2 of 6 Breathing Paediatric Drug Chart Clinical Practice Guideline: For paediatric patients, ventilate at a normal age-appropriate respiratory rate, refer to SAAS paediatric RDR chart. If gastric distension is impeding effective ventilations (e.g. in paediatrics), decompress the stomach via the SGA gastric drainage tube. Particular attention must be paid to ventilation rate and volume in paediatric patients, with careful consideration to avoid hyperventilation and subsequent hyperinflation of the lungs. Only deliver ventilation volumes that achieve normal visible chest movement. Gastric insufflation can be a risk in a non-intubated, ventilated patient, especially with a poorly sealed airway. If the abdomen becomes distended, ventilation and circulation may be impeded. With the new post-rosc guideline and the introduction of i-gels, comes the
39 ability to decompress the stomach with an orogastric tube via the i-gel gastric drainage tube. This will be expanded upon in the paramedic conferences. The SAAS paediatric RDR chart or drug dose chart must be used to help determine the age-appropriate respiratory rate.
40 Page 3 of 6 Breathing - Oxygenation Recall the OxyHaemoglobin Dissociation Curve Much of the evidence regarding oxygenation in a post-rosc paediatric patient is centred around in-hospital care, arterial blood gas analysis and the ability to adjust oxygenation to achieve a desired partial pressure of oxygen in arterial blood (PaO 2 ). In the prehospital environment, without ABG availability, it is appropriate to maintain high flow oxygen in patients who require assisted ventilations. Hypoxaemia and hyperoxaemia can both cause harm. Similar to the adult approach, in patients that do not require assisted ventilations, and the Sp0 2 reading is considered reliable, then it may be appropriate to titrate the concentration of inspired oxygen to achieve and maintain SpO %. An Sp0 2 of 90%, although only 10% below normal haemoglobin-oxygen saturation, represents a partial pressure of oxygen in arterial blood of 60mmHg which is 40mmHg below normal. ANZCOR 2016 Early clinical support must be sought with a SAAS Medical Practitioner via the EOC Clinician to discuss appropriate management of paediatric patients whose cardiac arrest may have been caused by a long-term cardiac condition. Examples of these may include chronic lung disease or cyanotic heart disease.
41 Page 4 of 6 Circulation Clinical Practice Guideline - For paediatrics with hypotension (refer to SAAS paediatric RDR chart): Consult with a SAAS Medical Practitioner via the EOC Clinician for sodium chloride 0.9% IV Peripheral circulatory failure is common after ROSC. Prior to any circulatory intervention in a paediatric post- ROSC patient, clinical support with a SAAS Medical Practitioner via the EOC Clinician must be sought. Consideration for sodium chloride 0.9% in hypotensive paediatric patients with an altered conscious state is based on maintenance of cerebral perfusion.
42 Page 5 of 6 Other Considerations - Blood Glucose Control Clinical Practice Guideline -For paediatrics with hypoglycaemia Consult with a SAAS Medical Practitioner via the EOC Clinician for glucose (10%) IV starting at 2 ml/kg titrated to achieve a BGL between 4-10 mmol/l. Sodium chloride 0.9% 1 ml/kg IV flush must be given before and after glucose IV. Post-ROSC paediatric patients are at increased risk of hypoglycaemia. If this is determined, it must be treated efficiently in order to maintain normal levels appropriate for age. Any management of paediatric post-rosc hypoglycaemia must be in consultation with a SAAS Medical Practitioner for use of glucose (10%) IV. When appropriate, reassessment of blood glucose levels, even if initial reading is within normal limits, must be done.
43 Page 6 of 6 Other Considerations - Temperature The recommendation of temperature management in paediatric post-rosc patients is maintenance of normothermia. The same strategies described with adult patients can be applied to paediatrics. Hyperthermia (>37.5 C) may be associated with worse neurological outcomes and must be avoided where possible.
44 Section 6 of 8 References Reference-Post-ROSC.pdf 46.1 KB
45 Section 7 of 8 Summative Assessment Details Successful completion of the online package will require at least 80% correct responses to the 12 MCQs. You are allowed three attempts for the quiz. Please speak to your team leader if you have used up all three attempts. Once you have passed the quiz, you can obtain your certificate of completion by returning to your portal. Go to quiz
46 Section 8 of 8 Download PDF for offline reading Download PDF
INFORMAL COPY WHEN PRINTED
 Doc Control Ref: TEM-003 Version 2.0 (Admin use only) Version no: (Admin use only) Effective Date: (Admin use only) 1. Principle Post-return of spontaneous circulation (ROSC) management is an important
Doc Control Ref: TEM-003 Version 2.0 (Admin use only) Version no: (Admin use only) Effective Date: (Admin use only) 1. Principle Post-return of spontaneous circulation (ROSC) management is an important
Intensive Care Paramedic
 Doc Control Ref: TEM-003 Version 2.0 (Admin use only) Version no: (Admin use only) Effective Date: (Admin use only) 1. Principle Post-return of spontaneous circulation (ROSC) management is an important
Doc Control Ref: TEM-003 Version 2.0 (Admin use only) Version no: (Admin use only) Effective Date: (Admin use only) 1. Principle Post-return of spontaneous circulation (ROSC) management is an important
Resuscitation Checklist
 Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
Post Resuscitation (ROSC) Care
 Care") Standard Operating Procedure 2.10 Post Resuscitation (ROSC) Care Position Responsible: Medical Director Approved: Clinical Governance Committee Related Documents: This document is the intellectual property
Standard Operating Procedure 2.10 Post Resuscitation (ROSC) Care Position Responsible: Medical Director Approved: Clinical Governance Committee Related Documents: This document is the intellectual property
Advanced Cardiac Life Support (ACLS) Science Update 2015
 Science Update 2015") 1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
ILCOR, ARC & NZRC PAEDIATRIC RESUSCITATION RECOMMENDATIONS 2010
 ILCOR, ARC & NZRC PAEDIATRIC RESUSCITATION RECOMMENDATIONS 2010 Jim Tibballs Officer, RCH Convenor, Paediatric Sub-Committee, (ARC) ARC Paediatric Representative International Liaison Committee on (ILCOR)
ILCOR, ARC & NZRC PAEDIATRIC RESUSCITATION RECOMMENDATIONS 2010 Jim Tibballs Officer, RCH Convenor, Paediatric Sub-Committee, (ARC) ARC Paediatric Representative International Liaison Committee on (ILCOR)
The ALS Algorithm and Post Resuscitation Care
 The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC
 SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Prehospital Care Bundles
 Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Advanced Life Support
 Standard Operating Procedure 2.1 Advanced Life Support Position Responsible: Head of Operations CGC Approved: October 2017 Related Documents Further Information 1.0 Background Magpas Resuscitation Policy
Standard Operating Procedure 2.1 Advanced Life Support Position Responsible: Head of Operations CGC Approved: October 2017 Related Documents Further Information 1.0 Background Magpas Resuscitation Policy
Maternal Collapse Guideline
 Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
In-hospital Care of the Post-Cardiac Arrest Patient. David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine
 In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
Cardiopulmonary Resuscitation in Adults
 Cardiopulmonary Resuscitation in Adults Fatma Özdemir, MD Emergency Deparment of Uludag University Faculty of Medicine OVERVIEW Introduction Pathophysiology BLS algorithm ALS algorithm Post resuscitation
Cardiopulmonary Resuscitation in Adults Fatma Özdemir, MD Emergency Deparment of Uludag University Faculty of Medicine OVERVIEW Introduction Pathophysiology BLS algorithm ALS algorithm Post resuscitation
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
Routine Patient Care Guidelines - Adult
 Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
Consider Treatable Underlying Causes Early
 Page 1 of 8 Cardiac Arrest Timeout Checklist Assign roles for Pit Crew CPR o Compressors x 2 o Airway o Lead responsible for coordinating team, making decisions o Medications Continuous compressions at
Page 1 of 8 Cardiac Arrest Timeout Checklist Assign roles for Pit Crew CPR o Compressors x 2 o Airway o Lead responsible for coordinating team, making decisions o Medications Continuous compressions at
Prehospital Post Arrest Care AHA Strive to Revive 2017 November 3, 2017
 Prehospital Post Arrest Care AHA Strive to Revive 2017 November 3, 2017 Jon Rittenberger, MD, MS Department of University of Pittsburgh Employers: Disclosures - Rittenberger University of Pittsburgh UPMC
Prehospital Post Arrest Care AHA Strive to Revive 2017 November 3, 2017 Jon Rittenberger, MD, MS Department of University of Pittsburgh Employers: Disclosures - Rittenberger University of Pittsburgh UPMC
CPR What Works, What Doesn t
 Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines
 Updated Guidelines") Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Post-Arrest Care: Beyond Hypothermia
 Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
TEACHING BASIC LIFE SUPPORT (& ALS)
") TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
Management of Post Cardiac Arrest Syndrome
 Management of Post Cardiac Arrest Syndrome Wilhelm Behringer Associated Professor of Emergency Medicine Medical University of Vienna, Austria Patients % What happens after ROSC? 35 30 25 20 15 10 5 ROSC
Management of Post Cardiac Arrest Syndrome Wilhelm Behringer Associated Professor of Emergency Medicine Medical University of Vienna, Austria Patients % What happens after ROSC? 35 30 25 20 15 10 5 ROSC
Post-Resuscitation Care. Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena
 Post-Resuscitation Care Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena Conflict of interest Emcools Shareholder and founder, honoraria Zoll: honoraria Bard: honoraria, nephew works
Post-Resuscitation Care Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena Conflict of interest Emcools Shareholder and founder, honoraria Zoll: honoraria Bard: honoraria, nephew works
Capnography 101. James A Temple BA, NRP, CCP
 Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Insight. Resuscitation Guidelines Summary of Key Changes
 Insight Resuscitation Guidelines 2015 - Summary of Key Changes Introduction Our 2020 Vision is to help save 500,000 more lives every year and therefore it seems fitting that we should help disseminate
Insight Resuscitation Guidelines 2015 - Summary of Key Changes Introduction Our 2020 Vision is to help save 500,000 more lives every year and therefore it seems fitting that we should help disseminate
Future of Cardiac Arrest Management for Paramedics
 Future of Cardiac Arrest Management for Paramedics EMS TODAY 2013 Mark Whitbread Consultant Paramedic London Ambulance Service London Ambulance Service NHS Trust 620 sq miles 8.2 million population 2011/12
Future of Cardiac Arrest Management for Paramedics EMS TODAY 2013 Mark Whitbread Consultant Paramedic London Ambulance Service London Ambulance Service NHS Trust 620 sq miles 8.2 million population 2011/12
EZ-IO. Offline Reading Download as PDF. Welcome. Introduction. Anatomy and Physiology. Indications. Paediatric Considerations.
 EZ-IO Acknowledgement This training package was created by David Funnell, Joseph Schar, and Jordan Pring. Please direct any questions to your CSO or Team Leader. Offline Reading Download as PDF Welcome
EZ-IO Acknowledgement This training package was created by David Funnell, Joseph Schar, and Jordan Pring. Please direct any questions to your CSO or Team Leader. Offline Reading Download as PDF Welcome
Head Trauma Protocol
 Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
ACLS Review. Pulse Oximetry to be between 94 99% to avoid hyperoxia (high oxygen tension can lead to tissue death
 ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
Lecture. ALS Algorithm
 Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
Capnography: The Most Vital Sign
 Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
1.1.2 CPAP therapy is used for patients who are suffering from an acute type 1 respiratory failure (Pa02 <8kPa with a normal or low Pac02).
.") Guidelines for initiating and managing CPAP (Continuous Positive Airway Pressure) on a general ward. B25/2006 1.Introduction and Who Guideline applies to 1.1.1 This document provides guidance for Healthcare
Guidelines for initiating and managing CPAP (Continuous Positive Airway Pressure) on a general ward. B25/2006 1.Introduction and Who Guideline applies to 1.1.1 This document provides guidance for Healthcare
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist
 Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
June 2011 Bill Streett-Training Section Chief
 Capnography 102 June 2011 Bill Streett-Training Section Chief Terminology Capnography: the measurement and numerical display of end-tidal CO2 concentration, at the patient s airway, during a respiratory
Capnography 102 June 2011 Bill Streett-Training Section Chief Terminology Capnography: the measurement and numerical display of end-tidal CO2 concentration, at the patient s airway, during a respiratory
Lesson 4-3: Cardiac Emergencies. CARDIAC EMERGENCIES Angina, AMI, CHF and AED
 Lesson 4-3: Cardiac Emergencies CARDIAC EMERGENCIES Angina, AMI, CHF and AED THREE FAMILIAR CARDIAC CONDITIONS Angina Pectoris Acute Myocardial Infarction Congestive Heart Failure ANGINA PECTORIS Chest
Lesson 4-3: Cardiac Emergencies CARDIAC EMERGENCIES Angina, AMI, CHF and AED THREE FAMILIAR CARDIAC CONDITIONS Angina Pectoris Acute Myocardial Infarction Congestive Heart Failure ANGINA PECTORIS Chest
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH
 Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
ACLS/ACS Updates 2015
 ACLS/ACS Updates 2015 Advanced Cardiovascular Life Support by: Fareed Al Nozha, JBIM, ABIM, FKFSH&RC(Cardiology) Consultant Cardiologist Faculty, National CPR Committee, ACLS Program Head, SHA Dr Abdulhalim
ACLS/ACS Updates 2015 Advanced Cardiovascular Life Support by: Fareed Al Nozha, JBIM, ABIM, FKFSH&RC(Cardiology) Consultant Cardiologist Faculty, National CPR Committee, ACLS Program Head, SHA Dr Abdulhalim
Pediatric Cardiac Arrest General
 Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
IFT1 Interfacility Transfer of STEMI Patients. IFT2 Interfacility Transfer of Intubated Patients. IFT3 Interfacility Transfer of Stroke Patients
 IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
Skills: Recall the incidence of seizures Recall the causes of seizures Describe types of seizures List signs and symptoms of seizure patients
 Medical 1 Resuscitation Describe the morbidity and mortality associated with sudden cardiac arrest List the chain of survival for sudden cardiac arrest as identified by the American Heart Association Discuss
Medical 1 Resuscitation Describe the morbidity and mortality associated with sudden cardiac arrest List the chain of survival for sudden cardiac arrest as identified by the American Heart Association Discuss
Department of Paediatrics Clinical Guideline. Advanced Paediatric Life Support. Sequence of actions. 1. Establish basic life support
 Advanced Paediatric Life Support Sequence of actions 1. Establish basic life support 2. Oxygenate, ventilate, and start chest compression: - Provide positive-pressure ventilation with high-concentration
Advanced Paediatric Life Support Sequence of actions 1. Establish basic life support 2. Oxygenate, ventilate, and start chest compression: - Provide positive-pressure ventilation with high-concentration
Emergency Cardiac Care Guidelines 2015
 Emergency Cardiac Care Guidelines 2015 VACEP 2016 William Brady, MD University of Virginia Guidelines 2015 Basic Life Support & Advanced Cardiac Life Support Acute Coronary Syndrome Pediatric Advanced
Emergency Cardiac Care Guidelines 2015 VACEP 2016 William Brady, MD University of Virginia Guidelines 2015 Basic Life Support & Advanced Cardiac Life Support Acute Coronary Syndrome Pediatric Advanced
How it Works. CO 2 is the smoke from the flames of metabolism 10/21/18. -Ray Fowler, MD. Metabolism creates ETC0 2 for excretion
 CO 2 is the smoke from the flames of metabolism -Ray Fowler, MD How it Works Metabolism creates ETC0 2 for excretion ETC02 and Oxygen are exchanged at the alveolar level in the lungs with each breath.
CO 2 is the smoke from the flames of metabolism -Ray Fowler, MD How it Works Metabolism creates ETC0 2 for excretion ETC02 and Oxygen are exchanged at the alveolar level in the lungs with each breath.
A silent chest is. Pediatrics II Asthma, seizures and cardiac arrest. Children are different. Cough variant asthma. Symptoms of severe distress
 Asthma ~21% of all asthma cases are school aged Pediatrics II Asthma, seizures and cardiac arrest Identify 3 symptoms of an asthma exacerbation Bronchospasm Edema of the bronchi Increased mucus production
Asthma ~21% of all asthma cases are school aged Pediatrics II Asthma, seizures and cardiac arrest Identify 3 symptoms of an asthma exacerbation Bronchospasm Edema of the bronchi Increased mucus production
3/30/12. Luke J. Gasowski BS, BSRT, NREMT-P, FP-C, CCP-C, RRT-NPS
 Luke J. Gasowski BS, BSRT, NREMT-P, FP-C, CCP-C, RRT-NPS 1) Define and describe ETCO 2 2) Explain methods of measuring ETCO 2 3) Describe various clinical applications of ETCO 2 4) Describe the relationship
Luke J. Gasowski BS, BSRT, NREMT-P, FP-C, CCP-C, RRT-NPS 1) Define and describe ETCO 2 2) Explain methods of measuring ETCO 2 3) Describe various clinical applications of ETCO 2 4) Describe the relationship
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Approach to type 2 Respiratory Failure
 Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Traumatic Cardiac Arrest Protocol
 Traumatic Cardiac Arrest Protocol Background: Major Trauma continues to be the leading worldwide cause of death in young adults. Mortality remains high but there are reports of good neurological outcomes
Traumatic Cardiac Arrest Protocol Background: Major Trauma continues to be the leading worldwide cause of death in young adults. Mortality remains high but there are reports of good neurological outcomes
Pediatric advanced life support. Management of decreased conscious level in children. Virgi ija Žili skaitė 2017
 Pediatric advanced life support. Management of decreased conscious level in children Virgi ija Žili skaitė 2017 Life threatening conditions: primary assessment, differential diagnostics and emergency care.
Pediatric advanced life support. Management of decreased conscious level in children Virgi ija Žili skaitė 2017 Life threatening conditions: primary assessment, differential diagnostics and emergency care.
Thanks to Ben Taylor for his Grand Rounds talk which looks at the problems that may result from whacking on a bit of oxygen.
 EMERGENCY MEDICINE Liverpool Hospital The Weekly Probe 4 th July, 2012 Volume 15, Issue 20 THIS WEEK: 1. Hyperoxia and the perils of oxygen therapy 2. Next week s case 3. Joke of the Week Hyperoxia The
EMERGENCY MEDICINE Liverpool Hospital The Weekly Probe 4 th July, 2012 Volume 15, Issue 20 THIS WEEK: 1. Hyperoxia and the perils of oxygen therapy 2. Next week s case 3. Joke of the Week Hyperoxia The
Post Resuscitation Care
 Princess Margaret Hospital f Children PAEDIATRIC ACUTE CARE GUIDELINE Post Resuscitation Care Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Princess Margaret Hospital f Children PAEDIATRIC ACUTE CARE GUIDELINE Post Resuscitation Care Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care
 Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post-resuscitation Therapy in Adult Advanced Life Support. ARC and NZRC Guideline 2010
 Emergency Medicine Australasia (2011) 23, 292 296 doi: 10.1111/j.1742-6723.2011.01422_15.x POST-RESUSCITATION THERAPY Post-resuscitation Therapy in Adult Advanced Life Support. ARC and NZRC Guideline 2010
Emergency Medicine Australasia (2011) 23, 292 296 doi: 10.1111/j.1742-6723.2011.01422_15.x POST-RESUSCITATION THERAPY Post-resuscitation Therapy in Adult Advanced Life Support. ARC and NZRC Guideline 2010
Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket
 BLS BASICS: Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket facemask or AMBU bag) Adults call it in, start CPR, get AED Child CPR First, Phone call second
BLS BASICS: Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket facemask or AMBU bag) Adults call it in, start CPR, get AED Child CPR First, Phone call second
New and Future Trends in EMS. Ron Brown, MD, FACEP Paramedic Lecture Series 2018
 New and Future Trends in EMS Ron Brown, MD, FACEP Paramedic Lecture Series 2018 New technologies and protocols DSD Mechanical Compression ITD BiPAP Ultrasound Double Sequential Defibrillation Two defibrillators
New and Future Trends in EMS Ron Brown, MD, FACEP Paramedic Lecture Series 2018 New technologies and protocols DSD Mechanical Compression ITD BiPAP Ultrasound Double Sequential Defibrillation Two defibrillators
Appendix (i) The ABCDE approach to the sick patient
 The ABCDE approach to the sick patient") Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
R Adams Cowley Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland.
 R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
Don t let your patients turn blue! Isn t it about time you used etco 2?
 Don t let your patients turn blue! Isn t it about time you used etco 2? American Association of Critical Care Nurses National Teaching Institute Expo Ed 2013 Susan Thibeault MS, CRNA, APRN, CCRN, EMT-P
Don t let your patients turn blue! Isn t it about time you used etco 2? American Association of Critical Care Nurses National Teaching Institute Expo Ed 2013 Susan Thibeault MS, CRNA, APRN, CCRN, EMT-P
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
Cardiac Emergencies. Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington
 Cardiac Emergencies Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington The Heart -------Aorta Pulmonary Veins---- Superior Vena Cava------ Right Atrium-----
Cardiac Emergencies Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington The Heart -------Aorta Pulmonary Veins---- Superior Vena Cava------ Right Atrium-----
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to
 1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
Capnography (ILS/ALS)
") Capnography (ILS/ALS) Clinical Indications: 1. Capnography shall be used as soon as possible in conjunction with any airway management adjunct, including endotracheal, Blind Insertion Airway Devices (BIAD)
Capnography (ILS/ALS) Clinical Indications: 1. Capnography shall be used as soon as possible in conjunction with any airway management adjunct, including endotracheal, Blind Insertion Airway Devices (BIAD)
EMT. Chapter 14 Review
 EMT Chapter 14 Review Review 1. All of the following are common signs and symptoms of cardiac ischemia, EXCEPT: A. headache. B. chest pressure. C. shortness of breath. D. anxiety or restlessness. Review
EMT Chapter 14 Review Review 1. All of the following are common signs and symptoms of cardiac ischemia, EXCEPT: A. headache. B. chest pressure. C. shortness of breath. D. anxiety or restlessness. Review
Resuscitation Science : Advancing Care for the Sickest Patients
 Resuscitation Science : Advancing Care for the Sickest Patients William Hallinan University of Rochester What is resuscitation science? Simply the science of resuscitation : Pre arrest Arrest care Medical
Resuscitation Science : Advancing Care for the Sickest Patients William Hallinan University of Rochester What is resuscitation science? Simply the science of resuscitation : Pre arrest Arrest care Medical
Chapter 40 Advanced Airway Management
 1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
Capnography- A Review and Renewed Perspective of its Uses and Limitations
 Capnography- A Review and Renewed Perspective of its Uses and Limitations Prepared and Presented by: Christine Hardie and Dr. Matt Davis December 2014 Learning Objectives Upon completion of this webinar
Capnography- A Review and Renewed Perspective of its Uses and Limitations Prepared and Presented by: Christine Hardie and Dr. Matt Davis December 2014 Learning Objectives Upon completion of this webinar
Nassau Regional Emergency Medical Services. Advanced Life Support Pediatric Protocol Manual
 Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Final Written Exam ASHI ACLS
 Final Written Exam ASHI ACLS Instructions: Identify the choice that best completes the statement or answers the question. Questions 1 and 2 pertain to the following scenario: A 54-year-old man has experienced
Final Written Exam ASHI ACLS Instructions: Identify the choice that best completes the statement or answers the question. Questions 1 and 2 pertain to the following scenario: A 54-year-old man has experienced
Post-resuscitation care for adults. Jerry Nolan Royal United Hospital Bath
 Post-resuscitation care for adults Jerry Nolan Royal United Hospital Bath Post-resuscitation care for adults Titration of inspired oxygen concentration after ROSC Urgent coronary catheterisation and percutaneous
Post-resuscitation care for adults Jerry Nolan Royal United Hospital Bath Post-resuscitation care for adults Titration of inspired oxygen concentration after ROSC Urgent coronary catheterisation and percutaneous
Interesting Capnography Cases
 Interesting Capnography Cases Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com Outline
Interesting Capnography Cases Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com Outline
2015 AHA Guidelines: Pediatric Updates
 2015 AHA Guidelines: Pediatric Updates Advances in Pediatric Emergency Medicine December 9, 2016 Karen O Connell, MD, MEd Associate Professor of Pediatrics and Emergency Medicine Emergency Medicine and
2015 AHA Guidelines: Pediatric Updates Advances in Pediatric Emergency Medicine December 9, 2016 Karen O Connell, MD, MEd Associate Professor of Pediatrics and Emergency Medicine Emergency Medicine and
Airway Management Essentials Self-Study Guide
 Airway Management Essentials Self-Study Guide Fourth Quarter 2010 Self-Study Guide Learning Objectives Cognitive Domain 1. Describe the various conditions that cause concern during treatment in the field
Airway Management Essentials Self-Study Guide Fourth Quarter 2010 Self-Study Guide Learning Objectives Cognitive Domain 1. Describe the various conditions that cause concern during treatment in the field
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
Out-of-hospital Cardiac Arrest. Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland
 Out-of-hospital Cardiac Arrest Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland Conflict of Interest I have no conflict of interest to disclose regarding this presentation.
Out-of-hospital Cardiac Arrest Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland Conflict of Interest I have no conflict of interest to disclose regarding this presentation.
Science Behind Resuscitation. Vic Parwani, MD ED Medical Director CarolinaEast Health System August 6 th, 2013
 Science Behind Resuscitation Vic Parwani, MD ED Medical Director CarolinaEast Health System August 6 th, 2013 Conflict of Interest No Financial or Industrial Conflicts Slides: Drs. Nelson, Cole and Larabee
Science Behind Resuscitation Vic Parwani, MD ED Medical Director CarolinaEast Health System August 6 th, 2013 Conflict of Interest No Financial or Industrial Conflicts Slides: Drs. Nelson, Cole and Larabee
Waitin In The Wings. Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider
 Indications and Use for the Pre-Hospital Provider") Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
Oxygen: Is there a problem? Tom Heaps Acute Physician
 Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
ANZCOR Guideline 11.2 Protocols for Adult Advanced Life Support
 ANZCOR Guideline 11.2 Protocols for Adult Advanced Life Support Summary Who does this guideline apply to? This guideline applies to adults who require advanced life support (ALS). Who is the audience for
ANZCOR Guideline 11.2 Protocols for Adult Advanced Life Support Summary Who does this guideline apply to? This guideline applies to adults who require advanced life support (ALS). Who is the audience for
They aren t the same thing. Daniel Dunham
 They aren t the same thing Daniel Dunham Capnometry Displays the value (as a number) of the partial pressure of CO2 Capnography Waveform capnography shows (as a wave) the change in CO2 over time Both are
They aren t the same thing Daniel Dunham Capnometry Displays the value (as a number) of the partial pressure of CO2 Capnography Waveform capnography shows (as a wave) the change in CO2 over time Both are
PALS NEW GUIDELINES 2010
 PALS NEW GUIDELINES 2010 DR WALEED ALAMRI PEDIATRIC EMERGENCY CONSULTANT FEB 24, 2011 Pediatric Basic Life Support Change in CPR Sequence (C-A-B Rather Than A-B-C) 2010 (New): Initiate CPR for infants
PALS NEW GUIDELINES 2010 DR WALEED ALAMRI PEDIATRIC EMERGENCY CONSULTANT FEB 24, 2011 Pediatric Basic Life Support Change in CPR Sequence (C-A-B Rather Than A-B-C) 2010 (New): Initiate CPR for infants
WESTMEAD Cardiac QUESTIONS PRACTICE SAQ
 QUESTION 1 A 65-year-old man presents to the emergency department with a history of palpitations. His vital signs are: BP 105/60 mmhg HR 156 beats/min RR 26 /min Temperature 36.2 o C His ECG is on the
QUESTION 1 A 65-year-old man presents to the emergency department with a history of palpitations. His vital signs are: BP 105/60 mmhg HR 156 beats/min RR 26 /min Temperature 36.2 o C His ECG is on the
Blood transfusions in sepsis, the elderly and patients with TBI
 Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
ITLS Advanced Pre-Test Annotated Key 8 th Edition
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Resuscitation in infants and children
 Resuscitation in infants and children The importance of respiratory support Dr. Simon Erickson Paediatric Intensive Care Princess Margaret Hospital for Children Paediatric cardiac arrests uncommon (~20/100,000)
Resuscitation in infants and children The importance of respiratory support Dr. Simon Erickson Paediatric Intensive Care Princess Margaret Hospital for Children Paediatric cardiac arrests uncommon (~20/100,000)
1 Pediatric Advanced Life Support Science Update What s New for 2010? 3 CPR. 4 4 Steps of BLS Survey 5 CPR 6 CPR.
 1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση. Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας
 Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας ACUTE HEART FAILURE AND CAD: ACS / LV ischaemic dysfunction Mechanical complications
Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας ACUTE HEART FAILURE AND CAD: ACS / LV ischaemic dysfunction Mechanical complications
Adult Basic Life Support
 Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
CHEST INJURY PULMONARY CONTUSION
 CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
Medical NREMT-PTE. NREMT Paramedic Trauma Exam.
 Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Airway and Ventilation. Emergency Medical Response
 Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report