Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham
|
|
|
- Benedict Lamb
- 5 years ago
- Views:
Transcription

1 Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham
2 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Chronic heart failure in adults: Diagnosis and management (NG106) September 2018
3 The Model of Care should ensure people receive the right care, at the right time, by the right team and in the right place
4 Compared with certain cancers, heart failure is associated with the second poorest survival rate The picture can't be displayed. In an observational study of 16,224 men and 14,842 women hospitalised with heart failure or different types of cancer: Median survival time of patients with heart failure was 16 months Only 25% of men and women survived 5 years Survival Women Breast 0.6 MI Bowel 0.4 Ovarian Heart failure 0.2 Lung Men MI Bladder Bowel Prostate Heart failure Lung Months of follow-up Months of follow-up MI, myocardial infarction. Stewart S et al. Eur J Heart Fail 2001;3:
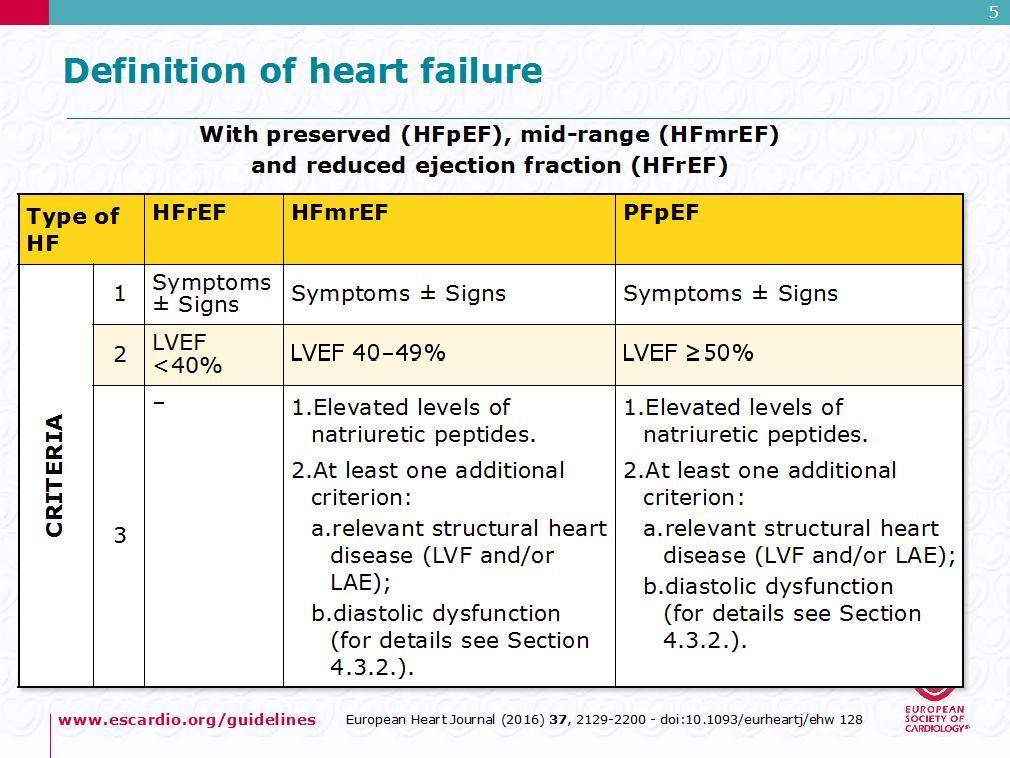
5 Classifying heart failure (NICE CHF Guideline NG106) u Heart failure with reduced ejection fraction Heart failure with an ejection fraction below 40%. u Heart failure with preserved ejection fraction This is usually associated with impaired left ventricular relaxation, rather than left ventricular contraction and is characterised by normal or preserved left ventricular ejection fraction.
6
7 Diagnosing Heart Failure NICE CHF Guidelines NG106
8 Diagnostic Algorithm Take a detailed history and perform a clinical examination Perform ECG. Consider chest x-ray, blood tests, urinalysis, peak flow or spirometry Measure NT probnp NT pro BNP >2000ng/l (>236pmol/l) Refer urgently to be seen within 2 weeks NT pro BNP ng/l (47-236pmol/l) Refer urgently to be seen within 6 weeks NT pro BNP <400ng/l (<47pmol/l) Specialist clinical assessment including echocardiography Exclude important valve disease, assess the systolic and diastolic function of the left ventricle, and detect intracardiacshunts Heart failure confirmed Heart failure not confirmed HF less likely Consider alternative causes for symptoms Assess HF severity Assess HF aetiology Identify precipitating factors and correctable causes HF unlikely If still concerned that symptoms might be related to heart failure, discuss with a specialist HFREF HFPEF Other abnormality
9 Diagnostic Algorithm Take a detailed history and perform a clinical examination Perform ECG. Consider chest x-ray, blood tests, urinalysis, peak flow or spirometry Measure NT probnp NT pro BNP >2000ng/l (>236pmol/l) NT pro BNP ng/l (47-236pmol/l) NT pro BNP <400ng/l (<47pmol/l) Refer urgently to be seen within 2 weeks Refer urgently to be seen within 6 weeks Specialist clinical assessment including echocardiography Exclude important valve disease, assess the systolic and diastolic function of the left ventricle, and detect intracardiacshunts HF less likely Consider alternative causes for symptoms If still concerned that symptoms might be related to heart failure, discuss with a specialist
10 Natriuretic peptides in Heart Failure ANP atria :BNP ventricles Increase in response to volume expansion and pressure overload in failing heart Promotes natriuresis dilates the afferent and constricts the efferent arteriole in the kidney resulting in decreased Na reabsorption and inhibits the secretion of renin and aldosterone Vasodilatation (arteries and veins)
11 other factors which may alter NT-proBNP levels May Reduce Serum NT-proBNP Obesity Diuretics ACE/ARB ARA s Beta blockers May Increase Serum NT-proBNP LVH Ischaemia Tachycardia/AF RV overload Hypoxaemia COPD Sepsis Diabetes Renal impairment Hepatic cirrhosis Over 70 s
 NT pro BNP 400-2000ng/l (47-236pmol/l) NT pro BNP <400ng/l (<47pmol/l) Refer")
12 Diagnostic Algorithm Take a detailed history and perform a clinical examination Perform ECG. Consider chest x-ray, blood tests, urinalysis, peak flow or spirometry Measure NT probnp NT pro BNP >2000ng/l (>236pmol/l) NT pro BNP ng/l (47-236pmol/l) NT pro BNP <400ng/l (<47pmol/l) Refer urgently to be seen within 2 weeks Refer urgently to be seen within 6 weeks Specialist clinical assessment including echocardiography Exclude important valve disease, assess the systolic and diastolic function of the left ventricle, and detect intracardiacshunts HF less likely Consider alternative causes for symptoms If still concerned that symptoms might be related to heart failure, discuss with a specialist
13 Team working in the management of heart failure NICE CHF Guideline NG106 The core specialist heart failure multidisciplinary team (MDT) should work in collaboration with the primary care team, and should include: ua lead physician with subspecialty training in heart failure (usually a consultant cardiologist) who is responsible for making the clinical diagnosis u a specialist heart failure nurse ua healthcare professional with expertise in specialist prescribing for heart failure. [2018]
14 Role of the Specialist Heart Failure MDT (NICE CHF Guideline NG106) The specialist heart failure MDT should: u diagnose heart failure u give information to people newly diagnosed with heart failure u manage newly diagnosed, recently decompensated or advanced heart failure (NYHA [New York Heart Association] class III to IV) u optimise treatment u start new medicines that need specialist supervision u continue to manage heart failure after an interventional procedure such as implantation of a cardioverter defibrillator or cardiac resynchronisation device u manage heart failure that is not responding to treatment. [2018]
15 Diagnostic Algorithm Take a detailed history and perform a clinical examination Perform ECG. Consider chest x-ray, blood tests, urinalysis, peak flow or spirometry Measure NT probnp NT pro BNP >2000ng/l (>236pmol/l) NT pro BNP ng/l (47-236pmol/l) NT pro BNP <400ng/l (<47pmol/l) Refer urgently to be seen within 2 weeks Refer urgently to be seen within 6 weeks Specialist clinical assessment including echocardiography Exclude important valve disease, assess the systolic and diastolic function of the left ventricle, and detect intracardiacshunts HF less likely Consider alternative causes for symptoms If still concerned that symptoms might be related to heart failure, discuss with a specialist
16 Specialist clinical assessment including echocardiography Exclude important valve disease, assess the systolic and diastolic function of the left ventricle, and detect intracardiac shunts Heart failure confirmed Heart failure not confirmed Assess HF severity Assess HF aetiology Identify precipitating factors and correctable causes HF unlikely HFREF HFPEF Other abnormality
17 NICE Chronic Heart Failure First consultations for people newly diagnosed with heart failure The specialist heart failure MDT should offer people newly diagnosed with heart failure an extended first consultation, followed by a second consultation to take place within 2 weeks if possible. At each consultation: u discuss the person's diagnosis and prognosis u explain heart failure terminology u discuss treatments u address the risk of sudden death, including any misconceptions about that risk u encourage the person and their family or carers to ask any questions they have. [2018]
18 Communication The specialist heart failure MDT should write a summary for each person with heart failure that includes: u diagnosis and aetiology u medicines prescribed, monitoring of medicines, when medicines should be reviewed and any support the person needs to take the medicines u functional abilities and any social care needs social circumstances, including carers' needs. [2018] u Summary should be the basis of a care plan and shared with the patient/carer/ appropriate health professionals
19 Managing Heart Failure NICE CHF Guideline NG106
20 Heart Failure diagnosed by the specialist Offer diuretics for the relief of congestive symptoms and fluid retention Heart Failure with Preserved Ejection Fraction (HFPEF) Manage co-morbid conditions such as high blood pressure, atrial fibrillation, ischaemic heart disease, and diabetes mellitus in line with NICE guidance Heart Failure with Reduced Ejection Fraction (HFREF) First line: Offer ACEI and BB Offer an MRA if symptoms continue All heart failure: Offer personalised, exercise-based cardiac rehabilitation programme, unless condition is unstable Specialist re-assessment Cardiac re-synchronisation therapy (CRT-P/D) in accordance with TA314 ICD in accordance with TA314 Replace ACEI (or ARB) by Sacubitril-Valsartan (if LVEF<35%) in accordance with TA388 If symptoms persist despite optimal first line therapy, seek specialist advice and consider one or more of the following options Add Ivabradine if in sinus rhythm with a HR of >75bpm and LVEF <35% in accordance with TA267 Add Hydralazine & nitrate (especially if of African/Caribbean descent) *Please refer to CG180 for recommendations on the use ofdigoxin in patients with atrial fibrillation Digoxin for worsening HF* Consider ARB if intolerant of ACEI Consider hydralazine & nitrate if intolerant of ACEI & ARB If the person s egfr is ml/min/1.73 m2, consider lower doses and/or slower titration of dose of ACE Inhibitors, ARBs, mineralocorticoid receptor antagonists,sacubitril-valsartan and digoxin. Ifthe person s egfr is <30 ml/min/1.73 m2, liaise with the renal physician.
21 Heart Failure diagnosed by the specialist Offer diuretics for the relief of congestive symptoms and fluid retention Heart Failure with Reduced Ejection Fraction (HFREF) First line: Offer ACEI and BB Offer an MRA if symptoms continue Consider ARB if intolerant of ACEI Specialist re-assessment Cardiac re-synchronisation therapy (CRT-P/D) in accordance with TA314 ICD in accordance with TA314 Replace ACEI (or ARB) by Sacubitril-Valsartan (if LVEF<35%) in accordance with TA388 If symptoms persist despite optimal first line therapy, seek specialist advice and consider one or more of the following options Add Ivabradine if in sinus rhythm with a HR of >75bpm and LVEF <35% in accordance with TA267 Add Hydralazine & nitrate (especially if of African/Caribbean descent) Consider hydralazine & nitrate if intolerant of ACEI & ARB Digoxin for worsening HF* *Please refer to CG180 for recommendations on the use ofdigoxin in patients with atrial fibrillation If the person s egfr is ml/min/1.73 m2, consider lower doses and/or slower titration of dose of ACE Inhibitors, ARBs, mineralocorticoid receptor antagonists,sacubitril-valsartan and digoxin. Ifthe person s egfr is <30 ml/min/1.73 m2, liaise with the renal physician.
22 Monitoring medication (NICE CHF Guideline NG106) Beta blockers vintroduce beta-blockers in a start low, go slow manner. Assess heart rate and clinical status after each titration. Measure blood pressure before and after each dose increment of a beta-blocker. [2010, amended 2018]
23 NICE CHF Guideline NG106 Mineralocorticoid receptor antagonists (MRAs) Offer a mineralocorticoid receptor antagonist (MRA), in addition to an ACE inhibitor (or ARB) and beta-blocker, to people who have heart failure with reduced ejection fraction if they continue to have symptoms of heart failure. [2018]
24 Heart Failure diagnosed by the specialist Offer diuretics for the relief of congestive symptoms and fluid retention Heart Failure with Reduced Ejection Fraction (HFREF) First line: Offer ACEI and BB Offer an MRA if symptoms continue Consider ARB if intolerant of ACEI Specialist re-assessment Cardiac re-synchronisation therapy (CRT-P/D) in accordance with TA314 ICD in accordance with TA314 Replace ACEI (or ARB) by Sacubitril-Valsartan (if LVEF<35%) in accordance with TA388 If symptoms persist despite optimal first line therapy, seek specialist advice and consider one or more of the following options Add Ivabradine if in sinus rhythm with a HR of >75bpm and LVEF <35% in accordance with TA267 Add Hydralazine & nitrate (especially if of African/Caribbean descent) Consider hydralazine & nitrate if intolerant of ACEI & ARB Digoxin for worsening HF* *Please refer to CG180 for recommendations on the use ofdigoxin in patients with atrial fibrillation If the person s egfr is ml/min/1.73 m2, consider lower doses and/or slower titration of dose of ACE Inhibitors, ARBs, mineralocorticoid receptor antagonists,sacubitril-valsartan and digoxin. Ifthe person s egfr is <30 ml/min/1.73 m2, liaise with the renal physician.
25 Heart Failure diagnosed by the specialist Offer diuretics for the relief of congestive symptoms and fluid retention Heart Failure with Reduced Ejection Fraction (HFREF) MDT OPTIMISATION First line: Offer ACEI and BB Offer an MRA if symptoms continue Consider ARB if intolerant of ACEI Specialist re-assessment Cardiac re-synchronisation therapy (CRT-P/D) in accordance with TA314 ICD in accordance with TA314 Replace ACEI (or ARB) by Sacubitril-Valsartan (if LVEF<35%) in accordance with TA388 If symptoms persist despite optimal first line therapy, seek specialist advice and consider one or more of the following options Add Ivabradine if in sinus rhythm with a HR of >75bpm and LVEF <35% in accordance with TA267 Add Hydralazine & nitrate (especially if of African/Caribbean descent) Consider hydralazine & nitrate if intolerant of ACEI & ARB Digoxin for worsening HF* *Please refer to CG180 for recommendations on the use ofdigoxin in patients with atrial fibrillation If the person s egfr is ml/min/1.73 m2, consider lower doses and/or slower titration of dose of ACE Inhibitors, ARBs, mineralocorticoid receptor antagonists,sacubitril-valsartan and digoxin. Ifthe person s egfr is <30 ml/min/1.73 m2, liaise with the renal physician.
26 RAAS Medication ACE or ARB and MRA Monitoring medication (NICE CHF Guideline NG106) v Once the target or maximum tolerated dose is reached, monitor treatment monthly for 3 months and then at least every 6 months, and at any time the person becomes acutely unwell.
27 National Heart Failure Audit 15/16 Pharmacotherapy
28 Patients journey of care following incident heart failure: diagnostic tests, treatments and care pathways in 93,000 patients N. Conrad EHJ 2018 u 93,000 Primary care patients CPRD u Primary care follow up decreased from 63% to 44% u Patients on ACE/ARB+ BB within 3 months of diagnosis increased from 18% to 63%.but in 2014 only 49% achieved target dose of ACE?ARB and 29% for BB and showed no signs of dose increment over the 12 months following there diagnosis of heart failure.

29 so what happens to your optimised patient now?
30 Managing heart failure Excellent Supportive care Functional status 2 3 Heart failure care 4 1 Death Time Sudden death event Transplant or ventricular assist device HF, heart failure; NYHA, New York Heart Association. Figure adapted from Goodlin SJ. J Am Coll Cardiol 2009;54:
31 Heart Failure diagnosed by the specialist Offer diuretics for the relief of congestive symptoms and fluid retention Heart Failure with Reduced Ejection Fraction (HFREF) Specialist re-assessment Cardiac re-synchronisation therapy (CRT-P/D) in accordance with TA314 ICD in accordance with TA314 Replace ACEI (or ARB) by Sacubitril-Valsartan (if LVEF<35%) in accordance with TA388 First line: Offer ACEI and BB Offer an MRA if symptoms continue Discharged back to Primary care If symptoms persist despite optimal first line therapy, seek specialist advice and consider one or more of the following options Add Ivabradine if in sinus rhythm with a HR of >75bpm and LVEF <35% in accordance with TA267 Add Hydralazine & nitrate (especially if of African/Caribbean descent) Consider ARB if intolerant of ACEI Consider hydralazine & nitrate if intolerant of ACEI & ARB Digoxin for worsening HF* *Please refer to CG180 for recommendations on the use ofdigoxin in patients with atrial fibrillation If the person s egfr is ml/min/1.73 m2, consider lower doses and/or slower titration of dose of ACE Inhibitors, ARBs, mineralocorticoid receptor antagonists,sacubitril-valsartan and digoxin. Ifthe person s egfr is <30 ml/min/1.73 m2, liaise with the renal physician.
32 Key recommendations for Primary care NICE CHF Guideline NG106
33 The role of primary care (NICE CHF Guideline NG106 ) The primary care team working within the specialist heart failure MDT should take over routine management of heart failure as soon as it has been stabilised and its management optimised. [2018]
34 The role of primary care (NICE CHF Guideline NG106 ) The primary care team should carry out the following for people with heart failure at all times, including periods when the person is also receiving specialist heart failure care from the MDT: u ensure effective communication links between different care settings and clinical services involved in the person's care u lead a full review of the person's heart failure care, which may form part of a long-term conditions review u recall the person at least every 6 months and update the clinical record u ensure that changes to the clinical record are understood and agreed by the person with heart failure and shared with the specialist heart failure MDT u arrange access to specialist heart failure services if needed. [2018]
35 Clinical review (NICE CHF Guideline NG106) All people with chronic heart failure need monitoring. This monitoring should include: u a clinical assessment of functional capacity, fluid status, cardiac rhythm (minimum of examining the pulse), cognitive status and nutritional status u a review of medication, including need for changes and possible side effects u an assessment of renal function [2010, amended 2018] u The frequency of monitoring should depend on the clinical status and stability of the person. The monitoring interval should be short (days to 2 weeks) if the clinical condition or medication has changed, but is needed at least 6-monthly for stable people with proven heart failure. [2003]
36 Reviewing Heart Failure Patients in Primary Care u Stoke Road Practice,Bishops Cleeve,Cheltenham u Total Population u Number of patients with a diagnosis of heart failure 112 u Number of HF patients not seen routinely in a Chronic Disease Clinic 14

37 Long Term Condition templates
38 Long Term Condition templates - Heart Failure
39 why is it important that HF is monitored at a LTC u Raises the profile of heart failure amongst all clinical staff - increased awareness of symptoms - earlier diagnosis - monitoring should lead to earlier re-referral - reduced hospital admissions - improved communication MDT-patient-Primary care - improved overall care and better supported patients - reduced costs
40 Managing heart failure Excellent Supportive care Functional status 2 3 Heart failure care 4 1 Death Time Sudden death event Transplant or ventricular assist device HF, heart failure; NYHA, New York Heart Association. Figure adapted from Goodlin SJ. J Am Coll Cardiol 2009;54:
41 Heart Failure diagnosed by the specialist Offer diuretics for the relief of congestive symptoms and fluid retention Heart Failure with Reduced Ejection Fraction (HFREF) First line: Offer ACEI and BB Offer an MRA if symptoms continue Consider ARB if intolerant of ACEI Specialist re-assessment Cardiac re-synchronisation therapy (CRT-P/D) in accordance with TA314 ICD in accordance with TA314 Replace ACEI (or ARB) by Sacubitril-Valsartan (if LVEF<35%) in accordance with TA388 If symptoms persist despite optimal first line therapy, seek specialist advice and consider one or more of the following options Add Ivabradine if in sinus rhythm with a HR of >75bpm and LVEF <35% in accordance with TA267 Add Hydralazine & nitrate (especially if of African/Caribbean descent) Consider hydralazine & nitrate if intolerant of ACEI & ARB Digoxin for worsening HF* *Please refer to CG180 for recommendations on the use ofdigoxin in patients with atrial fibrillation If the person s egfr is ml/min/1.73 m2, consider lower doses and/or slower titration of dose of ACE Inhibitors, ARBs, mineralocorticoid receptor antagonists,sacubitril-valsartan and digoxin. Ifthe person s egfr is <30 ml/min/1.73 m2, liaise with the renal physician.
42 Role of the Specialist Heart Failure MDT (NICE CHF Guideline NG106) The specialist heart failure MDT should: u diagnose heart failure u give information to people newly diagnosed with heart failure u manage newly diagnosed, recently decompensated or advanced heart failure (NYHA [New York Heart Association] class III to IV) u optimise treatment u start new medicines that need specialist supervision u continue to manage heart failure after an interventional procedure such as implantation of a cardioverter defibrillator or cardiac resynchronisation device u manage heart failure that is not responding to treatment. [2018]
43 Sacubitril/Valsartan
: 1 Entresto is recommended as an option for treating symptomatic chronic heart failure with reduced ejection fraction, only in people: 1 With NYHA class")
44 What is the NICE recommendation for Entresto? 1 NICE Technology Appraisal Guidance (TA388): 1 Entresto is recommended as an option for treating symptomatic chronic heart failure with reduced ejection fraction, only in people: 1 With NYHA class II to IV symptoms and With a left ventricular ejection fraction of 35% or less, and Who are already taking a stable dose of ACE inhibitors or ARBs ACE, angiotensin converting enzyme; ARB, angiotensin II receptor blocker; NICE, National Institute for Health and Care Excellence; NYHA, New York Heart Association 1. NICE. Technology Appraisal Guidance (TA388). Sacubitril valsartan for treating symptomatic chronic heart failure with reduced ejection fraction. April Last accessed October 2018
45 Heart Failure diagnosed by the specialist Offer diuretics for the relief of congestive symptoms and fluid retention Heart Failure with Reduced Ejection Fraction (HFREF) First line: Offer ACEI and BB Offer an MRA if symptoms continue Consider ARB if intolerant of ACEI Specialist re-assessment Cardiac re-synchronisation therapy (CRT-P/D) in accordance with TA314 ICD in accordance with TA314 Replace ACEI (or ARB) by Sacubitril-Valsartan (if LVEF<35%) in accordance with TA388 If symptoms persist despite optimal first line therapy, seek specialist advice and consider one or more of the following options Add Ivabradine if in sinus rhythm with a HR of >75bpm and LVEF <35% in accordance with TA267 Add Hydralazine & nitrate (especially if of African/Caribbean descent) Consider hydralazine & nitrate if intolerant of ACEI & ARB Digoxin for worsening HF* *Please refer to CG180 for recommendations on the use ofdigoxin in patients with atrial fibrillation If the person s egfr is ml/min/1.73 m2, consider lower doses and/or slower titration of dose of ACE Inhibitors, ARBs, mineralocorticoid receptor antagonists,sacubitril-valsartan and digoxin. Ifthe person s egfr is <30 ml/min/1.73 m2, liaise with the renal physician.
46 Ivabradine in Heart Failure
47 NICE TA 267 Ivabradine for treating Chronic Heart Failure Ivabradine is recommended as an option for treating chronic heart failure for people: u with New York Heart Association (NYHA) class II to IV stable chronic heart failure with systolic dysfunction and u who are in sinus rhythm with a heart rate of 75 beats per minute (bpm) or more and u who are given ivabradine in combination with standard therapy including beta-blocker therapy, angiotensin-converting enzyme (ACE) inhibitors and aldosterone antagonists, or when betablocker therapy is contraindicated or not tolerated and u with a left ventricular ejection fraction of 35% or less.
48 Heart Failure diagnosed by the specialist Offer diuretics for the relief of congestive symptoms and fluid retention Heart Failure with Reduced Ejection Fraction (HFREF) First line: Offer ACEI and BB Offer an MRA if symptoms continue Consider ARB if intolerant of ACEI Specialist re-assessment Cardiac re-synchronisation therapy (CRT-P/D) in accordance with TA314 ICD in accordance with TA314 Replace ACEI (or ARB) by Sacubitril-Valsartan (if LVEF<35%) in accordance with TA388 If symptoms persist despite optimal first line therapy, seek specialist advice and consider one or more of the following options Add Ivabradine if in sinus rhythm with a HR of >75bpm and LVEF <35% in accordance with TA267 Add Hydralazine & nitrate (especially if of African/Caribbean descent) Consider hydralazine & nitrate if intolerant of ACEI & ARB Digoxin for worsening HF* *Please refer to CG180 for recommendations on the use ofdigoxin in patients with atrial fibrillation If the person s egfr is ml/min/1.73 m2, consider lower doses and/or slower titration of dose of ACE Inhibitors, ARBs, mineralocorticoid receptor antagonists,sacubitril-valsartan and digoxin. Ifthe person s egfr is <30 ml/min/1.73 m2, liaise with the renal physician.
49 A-HeFT trial 2004 u 1050 self identified black patients u NYHA advanced HF u ISDN ( target 120mg daily )/Hydrallazine (target 225mg daily) in addition to standard therapy u Stopped early u Primary outcome all cause mortality +HF hospitalization + QOL u 43% RR reduction in all cause mortality ;33%RR reduction in first hospitalisation u Subsequent echo analysis showed significant effect on LV remodeling
50 Digoxin v Given for symptomatic benefit v No prognostic benefit v AF with LVSD (use in conjunction with beta blockers for rate control) v Indicated in SR if still symptomatic v Positive inotrope
51 Heart Failure diagnosed by the specialist Offer diuretics for the relief of congestive symptoms and fluid retention Heart Failure with Reduced Ejection Fraction (HFREF) First line: Offer ACEI and BB Offer an MRA if symptoms continue Consider ARB if intolerant of ACEI Specialist re-assessment Cardiac re-synchronisation therapy (CRT-P/D) in accordance with TA314 ICD in accordance with TA314 Replace ACEI (or ARB) by Sacubitril-Valsartan (if LVEF<35%) in accordance with TA388 If symptoms persist despite optimal first line therapy, seek specialist advice and consider one or more of the following options Add Ivabradine if in sinus rhythm with a HR of >75bpm and LVEF <35% in accordance with TA267 Add Hydralazine & nitrate (especially if of African/Caribbean descent) Consider hydralazine & nitrate if intolerant of ACEI & ARB Digoxin for worsening HF* *Please refer to CG180 for recommendations on the use ofdigoxin in patients with atrial fibrillation If the person s egfr is ml/min/1.73 m2, consider lower doses and/or slower titration of dose of ACE Inhibitors, ARBs, mineralocorticoid receptor antagonists,sacubitril-valsartan and digoxin. Ifthe person s egfr is <30 ml/min/1.73 m2, liaise with the renal physician.
52 Managing Heart Failure with Preserved Ejection Fraction NICE CHF Guideline NG106
53 Heart Failure diagnosed by the specialist Offer diuretics for the relief of congestive symptoms and fluid retention Heart Failure with Preserved Ejection Fraction (HFPEF) Manage co-morbid conditions such as high blood pressure, atrial fibrillation, ischaemic heart disease, and diabetes mellitus in line with NICE guidance
54 Heart Failure diagnosed by the specialist Offer diuretics for the relief of congestive symptoms and fluid retention Heart Failure with Preserved Ejection Fraction (HFPEF) Manage co-morbid conditions such as high blood pressure, atrial fibrillation, ischaemic heart disease, and diabetes mellitus in line with NICE guidance Heart Failure with Reduced Ejection Fraction (HFREF) First line: Offer ACEI and BB Offer an MRA if symptoms continue All heart failure: Offer personalised, exercise-based cardiac rehabilitation programme, unless condition is unstable Specialist re-assessment Cardiac re-synchronisation therapy (CRT-P/D) in accordance with TA314 ICD in accordance with TA314 Replace ACEI (or ARB) by Sacubitril-Valsartan (if LVEF<35%) in accordance with TA388 If symptoms persist despite optimal first line therapy, seek specialist advice and consider one or more of the following options Add Ivabradine if in sinus rhythm with a HR of >75bpm and LVEF <35% in accordance with TA267 Add Hydralazine & nitrate (especially if of African/Caribbean descent) *Please refer to CG180 for recommendations on the use ofdigoxin in patients with atrial fibrillation Digoxin for worsening HF* Consider ARB if intolerant of ACEI Consider hydralazine & nitrate if intolerant of ACEI & ARB If the person s egfr is ml/min/1.73 m2, consider lower doses and/or slower titration of dose of ACE Inhibitors, ARBs, mineralocorticoid receptor antagonists,sacubitril-valsartan and digoxin. Ifthe person s egfr is <30 ml/min/1.73 m2, liaise with the renal physician.
55 NICE - Cardiac Rehabilitation Offer people with heart failure a personalised, exercise-based cardiac rehabilitation programme, unless their condition is unstable. The programme: Should be preceded by an assessment to ensure that it is suitable for the person Should be provided in a format and setting (at home, in the community or in the hospital) that is easily accessible for the person Should include a psychological and educational component May be incorporated within an existing cardiac rehabilitation programme Should be accompanied by information about support available from healthcare professionals when the person is doing the programme

56 NICE Resource Impact -Cardiac Rehabilitation

57 NICE Resource Impact -Cardiac Rehabilitation
58 NICE Chronic Heart Failure Coronary revascularisation u1.8.1 Do not routinely offer coronary revascularisation to people who have heart failure with reduced ejection fraction and coronary artery disease. [2018]
59 NICE Chronic Heart Failure Salt and fluid restriction u Do not routinely advise people with heart failure to restrict their sodium or fluid consumption. Ask about salt and fluid consumption and, if needed, advise as follows: u restricting fluids for people with dilutional hyponatraemia u reducing intake for people with high levels of salt and/or fluid consumption. Continue to review the need to restrict salt or fluid. [2018] u Advise people with heart failure to avoid salt substitutes that contain potassium. [2018]
60 Clinical review (NICE CHF Guideline NG106) All people with chronic heart failure need monitoring. This monitoring should include: u a clinical assessment of functional capacity, fluid status, cardiac rhythm (minimum of examining the pulse), cognitive status and nutritional status u a review of medication, including need for changes and possible side effects u an assessment of renal function [2010, amended 2018] u The frequency of monitoring should depend on the clinical status and stability of the person. The monitoring interval should be short (days to 2 weeks) if the clinical condition or medication has changed, but is needed at least 6-monthly for stable people with proven heart failure. [2003]
61 Primary Care Cardiovascular Society wwww.pccsuk.org
62 How to register for Membership Annual Subscription GPs 50 Pharmacists, GP Registrars and Nurses 25 How to Register To register for membership please follow this link Or call Or

63 Thank you!... any questions?
NICE Chronic Heart Failure Guidelines in Adults 2018
 NICE Chronic Heart Failure Guidelines in Adults 2018 The Whys, Whats and Hows of the importance of effectively managing heart failure in Primary Care and the community. Foreword Dr Clare J Taylor, General
NICE Chronic Heart Failure Guidelines in Adults 2018 The Whys, Whats and Hows of the importance of effectively managing heart failure in Primary Care and the community. Foreword Dr Clare J Taylor, General
Chronic heart failure in adults: diagnosis and management
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Chronic heart failure in adults: diagnosis and management NICE guideline: short version Draft for consultation, March 0 This guideline covers diagnosing
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Chronic heart failure in adults: diagnosis and management NICE guideline: short version Draft for consultation, March 0 This guideline covers diagnosing
New NICE Heart Failure Guidelines What do they mean for primary and secondary care, and patients?
 New NICE Heart Failure Guidelines 2018 - What do they mean for primary and secondary care, and patients? Prof Ahmet Fuat PhD FRCGP FRCP PG Dip (Cardiology) GP & GPSI Cardiology Darlington Professor of
New NICE Heart Failure Guidelines 2018 - What do they mean for primary and secondary care, and patients? Prof Ahmet Fuat PhD FRCGP FRCP PG Dip (Cardiology) GP & GPSI Cardiology Darlington Professor of
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
NCAP NATIONAL CARDIAC AUDIT PROGR AMME NATIONAL HEART FAILURE AUDIT 2016/17 SUMMARY REPORT
 NCAP NATIONAL CARDIAC AUDIT PROGR AMME NATIONAL HEART FAILURE AUDIT 2016/17 SUMMARY REPORT CONTENTS PATIENTS ADMITTED WITH HEART FAILURE...4 Demographics... 4 Trends in Symptoms... 4 Causes and Comorbidities
NCAP NATIONAL CARDIAC AUDIT PROGR AMME NATIONAL HEART FAILURE AUDIT 2016/17 SUMMARY REPORT CONTENTS PATIENTS ADMITTED WITH HEART FAILURE...4 Demographics... 4 Trends in Symptoms... 4 Causes and Comorbidities
Heart Failure from a GP perspective
 Heart Failure from a GP perspective Jane Gilmour, Alison Wright Clinical Nurse Specialists for Heart Failure The Heart failure Team Dr Ganesan Kumar- Consultant Cardiologist Dr D Maras- Staff Grade Cardiology
Heart Failure from a GP perspective Jane Gilmour, Alison Wright Clinical Nurse Specialists for Heart Failure The Heart failure Team Dr Ganesan Kumar- Consultant Cardiologist Dr D Maras- Staff Grade Cardiology
Chronic heart failure
 Chronic heart failure Management of chronic heart failure in adults in primary and secondary care Issued: August 2010 NICE clinical guideline 108 guidance.nice.org.uk/cg108 NICE has accredited the process
Chronic heart failure Management of chronic heart failure in adults in primary and secondary care Issued: August 2010 NICE clinical guideline 108 guidance.nice.org.uk/cg108 NICE has accredited the process
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary
 Prior Authorization and Quantity Limit Program Summary") Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Heart Failure (HF) - Primary Care Flow Charts. Pre diagnosis Symptoms or signs suggestive of HF
 - Primary Care Flow Charts. Pre diagnosis Symptoms or signs suggestive of HF") Heart Failure (HF) - Primary Care Flow Charts Pre diagnosis Symptoms or signs suggestive of HF 12 lead ECG Normal examination and 12 lead ECG HF highly unlikely Abnormal 12 lead ECG HF Possible Arrange
Heart Failure (HF) - Primary Care Flow Charts Pre diagnosis Symptoms or signs suggestive of HF 12 lead ECG Normal examination and 12 lead ECG HF highly unlikely Abnormal 12 lead ECG HF Possible Arrange
Heart Failure (HF) - Primary Care Flow Charts. Symptoms or signs suggestive of HF. Pre diagnosis. Refer to the Heart Failure Clinic at VHK for
 - Primary Care Flow Charts. Symptoms or signs suggestive of HF. Pre diagnosis. Refer to the Heart Failure Clinic at VHK for") Heart Failure (HF) - Primary Care Flow Charts Pre diagnosis Symptoms or signs suggestive of HF 12 lead ECG Normal examination and 12 lead ECG HF highly unlikely Abnormal 12 lead ECG HF Possible Arrange
Heart Failure (HF) - Primary Care Flow Charts Pre diagnosis Symptoms or signs suggestive of HF 12 lead ECG Normal examination and 12 lead ECG HF highly unlikely Abnormal 12 lead ECG HF Possible Arrange
Clinical guideline Published: 25 August 2010 nice.org.uk/guidance/cg108
 Chronic heart failure in adults: management Clinical guideline Published: 25 August 2010 nice.org.uk/guidance/cg108 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Chronic heart failure in adults: management Clinical guideline Published: 25 August 2010 nice.org.uk/guidance/cg108 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Heart Failure Management. Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist
 Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Frimley Health Area Prescribing Committee
 Frimley Health Area Prescribing Committee Frimley Health NHS Foundation Trust North East Hampshire and Farnham CCG East Berkshire CCG Surrey Heath CCG Buckinghamshire CCG SHARED CARE Guideline Amber Traffic
Frimley Health Area Prescribing Committee Frimley Health NHS Foundation Trust North East Hampshire and Farnham CCG East Berkshire CCG Surrey Heath CCG Buckinghamshire CCG SHARED CARE Guideline Amber Traffic
A patient with decompensated HF
 A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA
 Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Heart Failure 101 The Basic Principles of Diagnosis & Management
 Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Heart Failure in 2012 with reference to NICE Guidance Dr Maurice Pye Consultant Cardiologist York District Hospital
 Heart Failure in 2012 with reference to NICE Guidance 2010 Dr Maurice Pye Consultant Cardiologist York District Hospital A little over elaborate,do not include ECG or CXR If clinical suspicion is high
Heart Failure in 2012 with reference to NICE Guidance 2010 Dr Maurice Pye Consultant Cardiologist York District Hospital A little over elaborate,do not include ECG or CXR If clinical suspicion is high
1000 Lives Key Components of Reliable, Evidence-Based Chronic Heart Failure Care how do we compare?
 1000 Lives Key Components of Reliable, Evidence-Based Chronic Heart Failure Care how do we compare? Dr Nerys Davies, GPST Ms B. Davies, Specialist Nurse (Heart Failure) Dr J. Taylor, Consultant Cardiologist
1000 Lives Key Components of Reliable, Evidence-Based Chronic Heart Failure Care how do we compare? Dr Nerys Davies, GPST Ms B. Davies, Specialist Nurse (Heart Failure) Dr J. Taylor, Consultant Cardiologist
Innovation therapy in Heart Failure
 Innovation therapy in Heart Failure P. Laothavorn September 2015 Topics of discussion Basic Knowledge about heart failure Standard therapy New emerging therapy References: standard Therapy in Heart Failure
Innovation therapy in Heart Failure P. Laothavorn September 2015 Topics of discussion Basic Knowledge about heart failure Standard therapy New emerging therapy References: standard Therapy in Heart Failure
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Chronic heart failure
 Issue date: August 2010 Chronic heart failure Management of chronic heart failure in adults in primary and secondary care This updates and replaces NICE clinical guideline 5 NICE clinical guideline 108
Issue date: August 2010 Chronic heart failure Management of chronic heart failure in adults in primary and secondary care This updates and replaces NICE clinical guideline 5 NICE clinical guideline 108
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update)
") Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update) NICE guideline Draft for consultation, January 2010 If you wish to comment on this version
Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update) NICE guideline Draft for consultation, January 2010 If you wish to comment on this version
Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update)
") Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update) NICE guideline Apendix C The algorithms Draft for consultation, January 2010 Chronic
Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update) NICE guideline Apendix C The algorithms Draft for consultation, January 2010 Chronic
CLINICAL PRACTICE GUIDELINE
 CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
eplerenone 25, 50mg film-coated tablets (Inspra ) SMC No. (793/12) Pfizer Ltd
 SMC No. (793/12) Pfizer Ltd") eplerenone 25, 50mg film-coated tablets (Inspra ) SMC No. (793/12) Pfizer Ltd 08 June 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS Boards
eplerenone 25, 50mg film-coated tablets (Inspra ) SMC No. (793/12) Pfizer Ltd 08 June 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS Boards
State-of-the-Art Management of Chronic Systolic Heart Failure
 State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
National Horizon Scanning Centre. Irbesartan (Aprovel) for heart failure with preserved systolic function. August 2008
 for heart failure with preserved systolic function. August 2008") Irbesartan (Aprovel) for heart failure with preserved systolic function August 2008 This technology summary is based on information available at the time of research and a limited literature search. It
Irbesartan (Aprovel) for heart failure with preserved systolic function August 2008 This technology summary is based on information available at the time of research and a limited literature search. It
Heart Failure Medical and Surgical Treatment
 Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
8:30-10:30 WS #4: Cardiology :00-13:00 WS #11: Cardiology 101 (Repeated)
") Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Online Appendix (JACC )
") Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
The CCS Heart Failure Companion: Bridging Guidelines to your Practice
 The CCS Heart Failure Companion: Bridging Guidelines to your Practice Looking for practical answers concerning optimal heart failure care? The CCS Heart Failure Guidelines Companion can help. The Canadian
The CCS Heart Failure Companion: Bridging Guidelines to your Practice Looking for practical answers concerning optimal heart failure care? The CCS Heart Failure Guidelines Companion can help. The Canadian
What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE. Marc Ferrini (Lyon Fr)
") What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE Marc Ferrini (Lyon Fr) Palermo (I) 1 04 2017 Consulting Fees, Honoraria: BAYER PHARMA BOEHRINGER INGELHEIM BRISTOL MEYERS
What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE Marc Ferrini (Lyon Fr) Palermo (I) 1 04 2017 Consulting Fees, Honoraria: BAYER PHARMA BOEHRINGER INGELHEIM BRISTOL MEYERS
Enhancing the Quality of Heart Failure Care
 Enhancing the Quality of Heart Failure Care 2 Enhancing the quality of Heart Failure care Contents 2 Heart failure care in the UK: Case for change Heart failure in the UK: Case for change Heart failure
Enhancing the Quality of Heart Failure Care 2 Enhancing the quality of Heart Failure care Contents 2 Heart failure care in the UK: Case for change Heart failure in the UK: Case for change Heart failure
Heart Failure: Guideline-Directed Management and Therapy
 Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Heart Failure Acute and Chronic
 Heart Failure Acute and Chronic Cardiac Services in Wales Acute Heart Failure standards Chronic Heart Failure standards NWIS admissions/readmission data NHFA data 2016-17 Echo accessibility BNP availability
Heart Failure Acute and Chronic Cardiac Services in Wales Acute Heart Failure standards Chronic Heart Failure standards NWIS admissions/readmission data NHFA data 2016-17 Echo accessibility BNP availability
Heart Failure. Optimising treatment and balancing co-morbidity in the community. Andrew Ludman Cardiologist
 Heart Failure Optimising treatment and balancing co-morbidity in the community Andrew Ludman Cardiologist What is heart failure? A structural cardiac abnormality leading to failure of the heart to provide
Heart Failure Optimising treatment and balancing co-morbidity in the community Andrew Ludman Cardiologist What is heart failure? A structural cardiac abnormality leading to failure of the heart to provide
Guideline-Directed Medical Therapy
 Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Inverclyde CHP Protected Learning Event- Heart Failure
 Inverclyde CHP Protected Learning Event- Heart Failure 14:00 14:05 14:05 14:20 14:20 14:30 14:30 15:10 15:10 15:30 15:30 15:50 15:50 16:05 16:05 16:35 Welcome & Introduction Paul Forsyth (HF Pharmacist)
Inverclyde CHP Protected Learning Event- Heart Failure 14:00 14:05 14:05 14:20 14:20 14:30 14:30 15:10 15:10 15:30 15:30 15:50 15:50 16:05 16:05 16:35 Welcome & Introduction Paul Forsyth (HF Pharmacist)
Long-Term Care Updates
 Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Heart Failure: Current Management Strategies
 Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
PRESS RELEASE. New NICE guidance will improve diagnosis and treatment of chronic heart failure
 Tel: 0845 003 7782 www.nice.org.uk Ref: 2010/118 ISSUED: WEDNESDAY, 25 AUGUST 2010 PRESS RELEASE New NICE guidance will improve diagnosis and treatment of chronic heart failure The National Institute for
Tel: 0845 003 7782 www.nice.org.uk Ref: 2010/118 ISSUED: WEDNESDAY, 25 AUGUST 2010 PRESS RELEASE New NICE guidance will improve diagnosis and treatment of chronic heart failure The National Institute for
Combination of renin-angiotensinaldosterone. how to choose?
 Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Heart Failure. GP Update Refresher 18 th January 2018
 GP Update Refresher 18 th January 2018 Heart Failure Dr. Alexander Lyon Senior Lecturer and Consultant Cardiologist Clinical Lead in Cardio-Oncology Royal Brompton Hospital, London UK President of British
GP Update Refresher 18 th January 2018 Heart Failure Dr. Alexander Lyon Senior Lecturer and Consultant Cardiologist Clinical Lead in Cardio-Oncology Royal Brompton Hospital, London UK President of British
Heart Failure Medications: Who Needs What Drug Now? Disclosures
 Heart Failure Medications: Who Needs What Drug Now? Simon Jackson MD FRCPC MMedEd Professor of Medicine (Cardiology) Dalhousie 1 Disclosures Honoraria and educational grants from: Actelion (medications
Heart Failure Medications: Who Needs What Drug Now? Simon Jackson MD FRCPC MMedEd Professor of Medicine (Cardiology) Dalhousie 1 Disclosures Honoraria and educational grants from: Actelion (medications
Management Strategies for Advanced Heart Failure
 Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
The NEW Heart Failure Guidelines
 The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital
 What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
Heart Failure in Women: Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre
 Heart Failure in Women: More than EF? Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre Overview Review pathophysiology as it relates to diagnosis and management Rational approach to workup:
Heart Failure in Women: More than EF? Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre Overview Review pathophysiology as it relates to diagnosis and management Rational approach to workup:
Advanced Heart Failure Management. Dr Andrew Hannah Consultant Cardiologist Aberdeen Royal Infirmary
 Advanced Heart Failure Management Dr Andrew Hannah Consultant Cardiologist Aberdeen Royal Infirmary Grading of heart failure Mr WY age 73 3/12 dyspnoea, fatigue and some ankle oedema PMH: hypertension
Advanced Heart Failure Management Dr Andrew Hannah Consultant Cardiologist Aberdeen Royal Infirmary Grading of heart failure Mr WY age 73 3/12 dyspnoea, fatigue and some ankle oedema PMH: hypertension
Disclosure Statement. Heart Failure: Refreshers and Updates. Objectives. CHF: Chronic Heart Failure. Definitions. Definitions 2/19/2018
 Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure
 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
Performance and Quality Measures 1. NQF Measure Number. Coronary Artery Disease Measure Set
 Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Heart Failure Update John Coyle, M.D.
 Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Heart Failure Guidelines For your Daily Practice
 Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Heart Failure Treatments
 Heart Failure Treatments Past & Present www.philippelefevre.com Background Background Chronic heart failure Drugs Mechanical Electrical Background Chronic heart failure Drugs Mechanical Electrical Sudden
Heart Failure Treatments Past & Present www.philippelefevre.com Background Background Chronic heart failure Drugs Mechanical Electrical Background Chronic heart failure Drugs Mechanical Electrical Sudden
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Heart Failure Update. Bibiana Cujec MD May 2015
 Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Heart Failure New Drugs- Updated Guidelines
 Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Patient details GP details Specialist details Name GP Name Dr Specialist Name Dr R. Horton
 Rationale for Initiation, Continuation and Discontinuation (RICaD) Sacubitril/Valsartan (Entresto) For the treatment of symptomatic heart failure with reduced ejection fraction (NICE TA388) This document
Rationale for Initiation, Continuation and Discontinuation (RICaD) Sacubitril/Valsartan (Entresto) For the treatment of symptomatic heart failure with reduced ejection fraction (NICE TA388) This document
Optimal blockade of the Renin- Angiotensin-Aldosterone. in chronic heart failure
 Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
21/06/2018. MEASURING PERFORMANCE (AUDIT AND QUALITY IMPROVEMENT) Towards Reducing Inequity. What should we be measuring?
 Towards Reducing Inequity. What should we be measuring?") MEASURING PERFORMANCE (AUDIT AND QUALITY IMPROVEMENT) Towards Reducing Inequity Dr Raewyn Fisher Cardiologist Director of Waikato Integrated Heart Failure Service What should we be measuring? At risk,
MEASURING PERFORMANCE (AUDIT AND QUALITY IMPROVEMENT) Towards Reducing Inequity Dr Raewyn Fisher Cardiologist Director of Waikato Integrated Heart Failure Service What should we be measuring? At risk,
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
ARxCH. Annual Review of Changes in Healthcare. Entresto: An Overview for Pharmacists
 Entresto: An Overview for Pharmacists David Comshaw, PharmD Candidate 2019 1 Gyen Musgrave, PharmD Candidate 2019 1 Suzanne Surowiec, PharmD, BCACP 1 Jason Guy, PharmD 1 1 University of Findlay College
Entresto: An Overview for Pharmacists David Comshaw, PharmD Candidate 2019 1 Gyen Musgrave, PharmD Candidate 2019 1 Suzanne Surowiec, PharmD, BCACP 1 Jason Guy, PharmD 1 1 University of Findlay College
Cardiac resynchronisation therapy (biventricular pacing) for the treatment of heart failure
 for the treatment of heart failure") NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal for the treatment of heart failure Final scope Appraisal objective To appraise the clinical and cost effectiveness of cardiac
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Health Technology Appraisal for the treatment of heart failure Final scope Appraisal objective To appraise the clinical and cost effectiveness of cardiac
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Neprilysin Inhibitor (Entresto ) Page 1 of 6 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Neprilysin Inhibitor (Entresto ) Prime Therapeutics will review Prior
Neprilysin Inhibitor (Entresto ) Page 1 of 6 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Neprilysin Inhibitor (Entresto ) Prime Therapeutics will review Prior
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Overview & Update on the Utilization of the Natriuretic Peptides in Heart Failure
 June 28, 2016 Overview & Update on the Utilization of the Natriuretic Peptides in Heart Failure Linda C. Rogers, PhD, DABCC, FACB. Agenda Overview of the Natriuretic Peptides and Efficacy studies Similarities
June 28, 2016 Overview & Update on the Utilization of the Natriuretic Peptides in Heart Failure Linda C. Rogers, PhD, DABCC, FACB. Agenda Overview of the Natriuretic Peptides and Efficacy studies Similarities
ESC Guidelines. ESC Guidelines Update For internal training purpose. European Heart Journal, doi: /eurheart/ehn309
 ESC Guidelines Update 2008 ESC Guidelines Heart failure update 2008 For internal training purpose. 0 Agenda Introduction Classes of recommendations Level of evidence Treatment algorithm Changes to ESC
ESC Guidelines Update 2008 ESC Guidelines Heart failure update 2008 For internal training purpose. 0 Agenda Introduction Classes of recommendations Level of evidence Treatment algorithm Changes to ESC
DISCLOSURES ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION NONE
 ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
Summary Protocol ISRCTN / NCT REVIVED-BCIS2 Summary protocol version 4, May 2015 Page 1 of 6
 Summary Protocol REVIVED-BCIS2 Summary protocol version 4, May 2015 Page 1 of 6 Background: Epidemiology In 2002, it was estimated that approximately 900,000 individuals in the United Kingdom had a diagnosis
Summary Protocol REVIVED-BCIS2 Summary protocol version 4, May 2015 Page 1 of 6 Background: Epidemiology In 2002, it was estimated that approximately 900,000 individuals in the United Kingdom had a diagnosis
NT-proBNP: Evidence-based application in primary care
 NT-proBNP: Evidence-based application in primary care Associate Professor Rob Doughty The University of Auckland, Auckland City Hospital, Auckland Heart Group NT-proBNP: Evidence in Primary Care The problem
NT-proBNP: Evidence-based application in primary care Associate Professor Rob Doughty The University of Auckland, Auckland City Hospital, Auckland Heart Group NT-proBNP: Evidence in Primary Care The problem
Topic Page: congestive heart failure
 Topic Page: congestive heart failure Definition: congestive heart f ailure from Merriam-Webster's Collegiate(R) Dictionary (1930) : heart failure in which the heart is unable to maintain an adequate circulation
Topic Page: congestive heart failure Definition: congestive heart f ailure from Merriam-Webster's Collegiate(R) Dictionary (1930) : heart failure in which the heart is unable to maintain an adequate circulation
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure
 ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Implantable cardioverter defibrillators for the treatment of arrhythmias and cardiac resynchronisation therapy for the treatment of heart failure (review
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Implantable cardioverter defibrillators for the treatment of arrhythmias and cardiac resynchronisation therapy for the treatment of heart failure (review
Cardiology. Presented by: Dr Paul Bethell GP Lead for Planned Care
 Cardiology Presented by: Dr Paul Bethell GP Lead for Planned Care 16 th April 2015 Integrated Cardiology Service for Ipswich and East Suffolk CCG IHT 6 consultants - all with specialist areas PCI CoW rapid
Cardiology Presented by: Dr Paul Bethell GP Lead for Planned Care 16 th April 2015 Integrated Cardiology Service for Ipswich and East Suffolk CCG IHT 6 consultants - all with specialist areas PCI CoW rapid
Congestive Heart Failure or Heart Failure
 Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
Heart Failure. Jay Shavadia
 Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
Heart.org/HFGuidelinesToolkit
 2017 /H/HFS Focused Update of the 2013 F/H 6.3.1 Biomarkers for Prevention: Recommendation OR LOE Recommendation a For patients at risk of developing HF, natriuretic peptide biomarker-based screening followed
2017 /H/HFS Focused Update of the 2013 F/H 6.3.1 Biomarkers for Prevention: Recommendation OR LOE Recommendation a For patients at risk of developing HF, natriuretic peptide biomarker-based screening followed
Introduction to Heart Failure. Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL
 Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
Sacubitril valsartan (Entresto ) for patients with symptomatic chronic heart failure
 for patients with symptomatic chronic heart failure") North Central London Joint Formulary Committee Sacubitril valsartan (Entresto ) for patients with symptomatic chronic heart failure North East and North Central London Position statement for the period
North Central London Joint Formulary Committee Sacubitril valsartan (Entresto ) for patients with symptomatic chronic heart failure North East and North Central London Position statement for the period
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Saudi Heart Failure Guidelines. Waleed AlHabeeb, MD, MHA Consultant Heart Failure Cardiologist President of the Saudi Heart Failure Group
 Saudi Heart Failure Guidelines Waleed AlHabeeb, MD, MHA Consultant Heart Failure Cardiologist President of the Saudi Heart Failure Group Heart Failure Expert committee The Heart Failure Expert Committee,
Saudi Heart Failure Guidelines Waleed AlHabeeb, MD, MHA Consultant Heart Failure Cardiologist President of the Saudi Heart Failure Group Heart Failure Expert committee The Heart Failure Expert Committee,
2017 Summer MAOFP Update
 2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases