Conflicts of Interest
|
|
|
- Kerry Marshall
- 5 years ago
- Views:
Transcription


1 Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania Conflicts of Interest 1
2 Upper Abdominal Surgery Focus on oncologic surgery Epidemiology i Preoperative assessment Intraoperative hemodynamic derangements Fluid management Respiratory complications Anesthesia / analgesia Operations Colon Cancer Pancreatic Cancer Renal Cell Carcinoma Hepatic Metastases Transhiatal esophagectomy Not the endocrine procedures 2

3 Surgeons/hospitals that do more of these procedures have lower mortality Related to lower complication rates. More so for cancer operations than CV % mortality procedures / yr 3




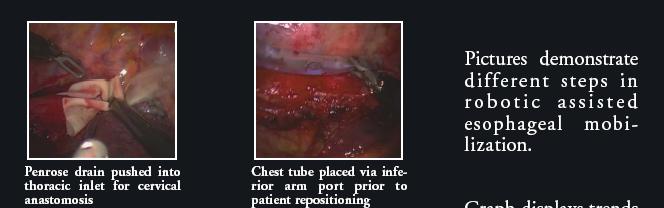
4 Does less-invasive surgery change these considerations? Conventional esophagectomy 4



5 Throracoscopic esophagectomy Robotic Assisted Transthoracic Esophagectomy. Society of American Gastrointestinal Endoscopic Surgeons, Denver, Colorado. April


6 Many patients are elderly With significant medical comorbidity 6
7 14 deaths (6%) in 226 patients. Preoperative variables Cholangitis creatinine > 1.3 mg/dl total bilirubin > 6 mg/dl Operative variables EBL > 3000 ml Vena cava resection 7
8 Can anesthetic management reduce complications and improve outcome? Preoperative Evaluation Maintaining vital organ perfusion Stress reduction and analgesia Fluid management Normovolemic hemodilution for hepatic resection Low CVP for hepatic resection Goal-directed fluid resuscitation Colloid vs. crystalloid How to monitor adequacy of resuscitation? 8

9 Normovolemic hemodilution Normovolemic Hemodilution 78 healthy patients with Aline, CVP, ST segs ANH via 8.5 F introducer Hct = 40.5 ± 2.7 to 23.5 ± 1.2% Average blood off = 2,020 ± 412 ml Hetastarch 20 ml/kg, 5% albumin via 2 large bore PIV 2,210 ±458 ml No significant changes in MAP, HR, ST segs 9
,")

10 Ann Surg 248(3), 2008, pp

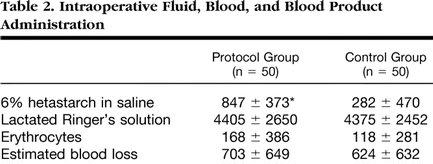
11 ANH for hepatic resection Patients randomized Goal: CVP < 5 mmhg o Fluid restriction o Morphine, NTG Arterial lines o ABG and Hct q 30 min Ann Surg 248(3), 2008, pp ANH Protocol Blood was withdrawn through central venous catheters into standard blood collection bags Baxter-HC/Fenwal Autologous Blood Collection Kit Stored at room temperature In the operating room Labeled with the patients': o name o medical record number o date of birth 11



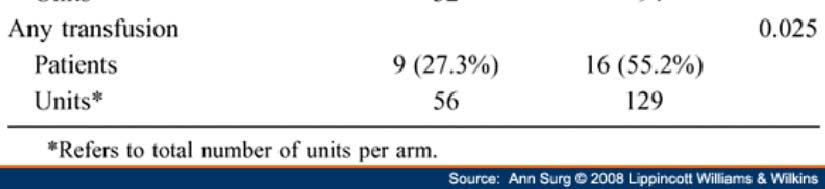
12 All patients Ann Surg 248(3), 2008, pp Patients EBL > 800 ml Ann Surg 248(3), 2008, pp
:360-369,")

13 Ann Surg 248(3): , 2008 Does transfusion promote metastases? 13


14 Local recurrence Busch OR, et al: Blood transfusions and local tumor recurrence in colorectal cancer: Evidence of a noncausal relationship. Ann Surg 1994; 220:791-7 Bigger tumors bleed more? Therefore, more transfusion? Or is the transfusion itself bad? 14


15 Anesthesiology:109(6)December 2008pp Anesthesiology:109(6)December 2008pp


16 Surgery is bad, transfusion is bad The combination is worse! Anesthesiology:109(6)December 2008pp





17 Does old blood cause hypoperfusion, tissue hypoxia? Bad old blood Exchange transfusion with RBC after 60% isovolemic hemodilution to Hct =18 % Stored RBCs (28 days in CPDA) Stored RBCs reduced microvascular flow by 63% Tissue oxygen levels: 3.5 for the stored and 14.4 mmhg for fresh RBCs. Tsai AG, et al. Transfusion 2004; 44:
18 Goals of low CVP Soften the liver Precludes vena caval distention Facilitates mobilization of the liver and dissection of the retrohepatic and major hepatic veins. Minimizes hepatic venous bleeding during parenchymal transection Facilitates control of inadvertent venous injury Reduce EBL Fluid restriction Large bore IVs Isoflurane in oxygen, fentanyl prn morphine for vasodilation prn NTG to lower CVP < 5 mmhg Why not just give everyone NTG?? Does fluid restriction reduce organ perfusion?? 18

19 Air emboli well described during hepatectomy Risk is likely to increase with low CVP anesthesia. Therefore, no nitrous oxide used 19


20 Mean EBL 645 ml. Median units PRBC = 2 67% of patients did not require transfusion during surgery and first 12 hours postop p Only 3% of the patients experienced a persistent and clinically significant increase in serum creatinine possibly attributable to the anesthetic 20



21 Normovolemic hemodilution 21


22 Not everyone is a candidate Hemodilution in the OR Whole blood collected Cordis Art Line 14 G PIV How long to sit unrefrigerated? Blood banking paperwork etc.. 22



23 Renal effects of insufflation 23

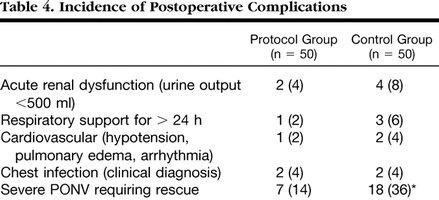
24 Does subtle hypovolemia cause harm? Hypothesis: Vital organ hypoperfusion is common during major cancer resection, and may produce vital organ dysfunction Goal-directed fluid therapy 100 major elective surgery patients Anticipated EBL > 500 ml randomized control group (n = 50) that received standard care protocol group (n = 50) received intraoperative plasma volume expansion guided by the esophageal Doppler monitor to maintain maximal stroke volume. 24



25 Days hospital First POD food Conventional Goal-directed 25

26 Flow time 26
27 Do we monitor vital organ perfusion? Renal Urine output Gut Gastric tonometry? Brain EEG? Cerebral oximetry? Heart ST segments TEE Postoperative Ventilation Contributing factors Underlying cardiopulmonary disease Large fluid volumes Airway edema / difficult ETT Transfusion Visceral edema Systemic inflammatory response Pain and splinting 27




28 Fluids to maintain BP? Dangers of excessive IV fluids 28
29 29
30 Problem Solving Ephedrine and/or dopamine were administered in both groups to achieve a mean arterial blood pressure above 60 mm Hg during operation. Cases of postoperative hypotension or low urinary output (<0.5 ml/kg/h) were always examined and the cause treated. Bleeding initiated administration of intravenous fluids as previously described. 30
31 31




32 102 patients 92 extubated in OR Only 3 required reintubation 10 patients to ICU with ETT 2 reintubated in OR for acute a/w obstruction Overall, ~5% require reintubation Don t put the ETT in the esophagus! Tube changer? 32
33 17% of postop laparotomy patients were hypoxemic JAMA. 2005;293: JAMA. 2005;293:

34 JAMA. 2005;293: Good analgesia improves outcome? 34



35 Epidurals for abdominal surgery From Ontario, Canada insurance data Retrospective analysis Matched cases with and without epidural N = 44,000 in each group! Published online August 11, Published online August 11,

36 Published online August 11, Published online August 11,
37 Our institution Much room for improvement! 37
38 Conclusions High mortality, though not so apparent to anesthesia care providers Anesthetic technique, adequate fluid resuscitation may improve outcome Does early extubation reduce pulmonary complications? Multimodal l analgesia and fast tracking? 38
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006.
 Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006 Introduction Laparoscopic surgery started in the mid 1950s. In recent
Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006 Introduction Laparoscopic surgery started in the mid 1950s. In recent
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
HEPATECTOMY. Surgical Potpourri Session. ACS NSQIP National Conference Salt Lake City 2012
 HEPATECTOMY Surgical Potpourri Session ACS NSQIP National Conference Salt Lake City 2012 Pascal Fuchshuber, MD, PhD, FACS Kaiser Permanente Medical Center Walnut Creek - California Hepatic Resection Is
HEPATECTOMY Surgical Potpourri Session ACS NSQIP National Conference Salt Lake City 2012 Pascal Fuchshuber, MD, PhD, FACS Kaiser Permanente Medical Center Walnut Creek - California Hepatic Resection Is
Perioperative Management To Prevent Allogeneic Blood Transfusion In Liver Surgery
 AEJ Perioperative Management To Prevent Allogeneic Blood Transfusion In Liver Surgery Robbin Rabbani, CRNA, MS Michele E. Gold, CRNA, PhD Affiliations: This article was written by Robbin as student at
AEJ Perioperative Management To Prevent Allogeneic Blood Transfusion In Liver Surgery Robbin Rabbani, CRNA, MS Michele E. Gold, CRNA, PhD Affiliations: This article was written by Robbin as student at
The Use of Dynamic Parameters in Perioperative Fluid Management
 The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Is the patient at risk for blood loss of 1000 mls? Avoid these Guidelines. Avoid these Guidelines. Yes. Yes. Yes. Yes. Yes
 Clinical Guidelines Acute rmovolemic Hemodilution Guidelines for Cardiac Surgery Department of Anesthesiology and Perioperative Medicine Date: 12-30-2012 Is the patient at risk for blood loss of 1000 mls?
Clinical Guidelines Acute rmovolemic Hemodilution Guidelines for Cardiac Surgery Department of Anesthesiology and Perioperative Medicine Date: 12-30-2012 Is the patient at risk for blood loss of 1000 mls?
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Fluid Balance in an Enhanced Recovery Pathway. Edwin Itenberg, DO, FACS, FASCRS St. Joseph Mercy Oakland MSQC/ASPIRE Meeting April 28, 2017
 Fluid Balance in an Enhanced Recovery Pathway Edwin Itenberg, DO, FACS, FASCRS St. Joseph Mercy Oakland MSQC/ASPIRE Meeting April 28, 2017 No Disclosures 2 Introduction The optimal intravenous fluid regimen
Fluid Balance in an Enhanced Recovery Pathway Edwin Itenberg, DO, FACS, FASCRS St. Joseph Mercy Oakland MSQC/ASPIRE Meeting April 28, 2017 No Disclosures 2 Introduction The optimal intravenous fluid regimen
General surgery. Thyroid surgery. Physiological response to pneumoperitoneum. Bowel resection
 General surgery Thyroid surgery Physiological response to pneumoperitoneum Bowel resection General surgery 3.D.9.1 James Mitchell (December 24, 2003) Thyroid surgery Preoperative Assessment Routine, plus
General surgery Thyroid surgery Physiological response to pneumoperitoneum Bowel resection General surgery 3.D.9.1 James Mitchell (December 24, 2003) Thyroid surgery Preoperative Assessment Routine, plus
ANESTHESIA EXAM (four week rotation)
") SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
LiverGroup.org. Case Report Form (CRF) for STAGED procedures
 for STAGED procedures") Case Report Form (CRF) for STAGED procedures Patient Characteristics Case number * Age * ( 18)y Gender * Male Female Race * Caucasian Asian African Other If other race, please specify Height * cm Weight
Case Report Form (CRF) for STAGED procedures Patient Characteristics Case number * Age * ( 18)y Gender * Male Female Race * Caucasian Asian African Other If other race, please specify Height * cm Weight
Role of IONM in reducing the incidence and severity in pediatric patients with AIS
 Role of IONM in reducing the incidence and severity in pediatric patients with AIS Mohamed Nassef M.D PGY 2 ANESTHESIA McMaster University DEC 9, 2015 Objectives: Literature Review on neurological complications
Role of IONM in reducing the incidence and severity in pediatric patients with AIS Mohamed Nassef M.D PGY 2 ANESTHESIA McMaster University DEC 9, 2015 Objectives: Literature Review on neurological complications
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Anesthetic Management of a Child with Malignant Hypertension Secondary to a Renal Paraganglioma and Concomitant Renal Artery Stenosis
 Anesthetic Management of a Child with Malignant Hypertension Secondary to a Renal Paraganglioma and Concomitant Renal Artery Stenosis Moderators: Joel Stockman, MD, Ellen Choi, MD Objectives: 1. Identify
Anesthetic Management of a Child with Malignant Hypertension Secondary to a Renal Paraganglioma and Concomitant Renal Artery Stenosis Moderators: Joel Stockman, MD, Ellen Choi, MD Objectives: 1. Identify
How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion
 How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Disclosure Slide No COI and no disclosures. Hospital Mortality rate : is it
How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Disclosure Slide No COI and no disclosures. Hospital Mortality rate : is it
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL
 Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
ICU Management of Minimally Invasive Cardiac Surgery
 ICU Management of Minimally Invasive Cardiac Surgery Benjamin A. Kohl, MD, FCCM Chief of Critical Care, Aria-Jefferson Health Professor of Anesthesiology Thomas Jefferson University Sidney Kimmel Medical
ICU Management of Minimally Invasive Cardiac Surgery Benjamin A. Kohl, MD, FCCM Chief of Critical Care, Aria-Jefferson Health Professor of Anesthesiology Thomas Jefferson University Sidney Kimmel Medical
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Fluid management. Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center
 Fluid management Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center Disclosure Consultant and research funding Edwards Lifesciences Goals of fluid therapy 1. Maintain
Fluid management Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center Disclosure Consultant and research funding Edwards Lifesciences Goals of fluid therapy 1. Maintain
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT.
 HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
Problem Based Learning. Problem. Based Learning
 Problem 2013 Based Learning Problem Based Learning Your teacher presents you with a problem in anesthesia, our learning becomes active in the sense that you discover and work with content that you determine
Problem 2013 Based Learning Problem Based Learning Your teacher presents you with a problem in anesthesia, our learning becomes active in the sense that you discover and work with content that you determine
Anesthesiology in advanced radical surgery. Bruno Carrara Ospedali Riuniti di Bergamo
 Anesthesiology in advanced radical surgery Bruno Carrara Ospedali Riuniti di Bergamo Anesthetic considerations Anesthesiology in advanced radical surgery Anesthesiologists's task is to minimize the contribution
Anesthesiology in advanced radical surgery Bruno Carrara Ospedali Riuniti di Bergamo Anesthetic considerations Anesthesiology in advanced radical surgery Anesthesiologists's task is to minimize the contribution
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Goal-Directed Fluid Therapy: A New Way of Thinking. Ji Su Jenny Kim & Logan D. MacLean SRNA, BSN, CCRN DNP Candidates
 Goal-Directed Fluid Therapy: A New Way of Thinking Ji Su Jenny Kim & Logan D. MacLean SRNA, BSN, CCRN DNP Candidates Goal-Directed Fluid Therapy Map History of Fluid Management Significance of Fluid Management
Goal-Directed Fluid Therapy: A New Way of Thinking Ji Su Jenny Kim & Logan D. MacLean SRNA, BSN, CCRN DNP Candidates Goal-Directed Fluid Therapy Map History of Fluid Management Significance of Fluid Management
Minimally Invasive Esophagectomy
 Minimally Invasive Esophagectomy M A R K B E R R Y, M D A S S O C I AT E P R O F E S S O R D E PA R T M E N T OF C A R D I O T H O R A C I C S U R G E R Y S TA N F O R D U N I V E R S I T Y S E P T E M
Minimally Invasive Esophagectomy M A R K B E R R Y, M D A S S O C I AT E P R O F E S S O R D E PA R T M E N T OF C A R D I O T H O R A C I C S U R G E R Y S TA N F O R D U N I V E R S I T Y S E P T E M
Hyperthermic Intra PEritoneal Chemotherapy:
 Hyperthermic Intra PEritoneal Chemotherapy: Does the anaesthesiological strategy differ from other extensive abdominal strategies? Dr V. Billard, Département d anesthésie Preoperative assessment Eligibility
Hyperthermic Intra PEritoneal Chemotherapy: Does the anaesthesiological strategy differ from other extensive abdominal strategies? Dr V. Billard, Département d anesthésie Preoperative assessment Eligibility
Effects of intraoperative epidural anesthesia during hepatectomy on intraoperative and post-operative patient outcomes
 Open Access International Journal of Clinical Anesthesia and Research Research Article Effects of intraoperative epidural anesthesia during hepatectomy on intraoperative and post-operative patient outcomes
Open Access International Journal of Clinical Anesthesia and Research Research Article Effects of intraoperative epidural anesthesia during hepatectomy on intraoperative and post-operative patient outcomes
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
Shock. William Schecter, MD
 Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
ANAESTHESIA FOR BLEEDING TONSIL
 ANAESTHESIA FOR BLEEDING TONSIL BY Dr.S.C.Ganeshprabu, MD., D.A., Professor of Anaesthesiology, Madurai Medical College & Govt. Rajaji Hospital, Madurai -652 020. A 5-year-old child who had tonsillectomy
ANAESTHESIA FOR BLEEDING TONSIL BY Dr.S.C.Ganeshprabu, MD., D.A., Professor of Anaesthesiology, Madurai Medical College & Govt. Rajaji Hospital, Madurai -652 020. A 5-year-old child who had tonsillectomy
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
The Surgical Patient. Objectives:
 The Surgical Patient Objectives: 1. Discuss the effect of surgery on the body systems. 2. Explain the etiological factors, nursing assessment, and management of potential problems during the postoperative
The Surgical Patient Objectives: 1. Discuss the effect of surgery on the body systems. 2. Explain the etiological factors, nursing assessment, and management of potential problems during the postoperative
POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO. MD (ANAESTHESIOLOGY) FINAL EXAMINATION AUGUST 2011 Time : 1.00 p.m p.m.
 FINAL EXAMINATION AUGUST 2011 Time : 1.00 p.m p.m.") POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO MD (ANAESTHESIOLOGY) FINAL EXAMINATION AUGUST 2011 Date : 5 th August 2011 Time : 1.00 p.m. 4.00 p.m. Answer any three questions. Answer each question
POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO MD (ANAESTHESIOLOGY) FINAL EXAMINATION AUGUST 2011 Date : 5 th August 2011 Time : 1.00 p.m. 4.00 p.m. Answer any three questions. Answer each question
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
University of Colorado Health Sciences Center, Denver Colorado ******************** ******************
 University of Colorado Health Sciences Center, Denver Colorado ******************** 1988-2005 ****************** Disclosures No disclosures Case 53 M presents with sudden onset of upper abdominal pain
University of Colorado Health Sciences Center, Denver Colorado ******************** 1988-2005 ****************** Disclosures No disclosures Case 53 M presents with sudden onset of upper abdominal pain
Postoperative Management of Patients Following Surgical Ablation
 Postoperative Management of Patients Following Surgical Ablation Harold G. Roberts, Jr. Department of Cardiovascular and Thoracic Surgery West Virginia University Morgantown, WV None Disclosures Postop
Postoperative Management of Patients Following Surgical Ablation Harold G. Roberts, Jr. Department of Cardiovascular and Thoracic Surgery West Virginia University Morgantown, WV None Disclosures Postop
Capnography: The Most Vital of Vital Signs. Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017
 Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
Cardiovascular Effects of Anesthesia for Cesarean Delivery in the Cardiac Patient
 Cardiovascular Effects of Anesthesia for Cesarean Delivery in the Cardiac Patient Katherine W. Arendt, M.D. Associate Professor of Anesthesiology Mayo Clinic, Rochester, Minnesota Cardiac Problems in Pregnancy
Cardiovascular Effects of Anesthesia for Cesarean Delivery in the Cardiac Patient Katherine W. Arendt, M.D. Associate Professor of Anesthesiology Mayo Clinic, Rochester, Minnesota Cardiac Problems in Pregnancy
Admission of patient CVICU and hemodynamic monitoring
 Admission of patient CVICU and hemodynamic monitoring Prepared by: Rami AL-Khatib King Fahad Medical City Pi Prince Salman Heart tcentre CVICU-RN Admission patient to CVICU Introduction All the patients
Admission of patient CVICU and hemodynamic monitoring Prepared by: Rami AL-Khatib King Fahad Medical City Pi Prince Salman Heart tcentre CVICU-RN Admission patient to CVICU Introduction All the patients
Interesting Cases - A Case Report: Renal Cell Carcinoma With Tumor Mass In IVC And Heart. O Wenker, L Chaloupka, R Joswiak, D Thakar, C Wood, G Walsh
 ISPUB.COM The Internet Journal of Thoracic and Cardiovascular Surgery Volume 3 Number 2 Interesting Cases - A Case Report: Renal Cell Carcinoma With Tumor Mass In IVC And Heart O Wenker, L Chaloupka, R
ISPUB.COM The Internet Journal of Thoracic and Cardiovascular Surgery Volume 3 Number 2 Interesting Cases - A Case Report: Renal Cell Carcinoma With Tumor Mass In IVC And Heart O Wenker, L Chaloupka, R
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Organ Donor Management Recommended Guidelines ADULT CARDIAC DEATH (DCD)
") Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
Actualités sur le remplissage peropératoire. Philippe Van der Linden MD, PhD
 Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Advances in Transfusion and Blood Conservation
 Advances in Transfusion and Blood Conservation Arman Kilic, MD Division of Cardiac Surgery, Department of Surgery, Johns Hopkins Hospital, Baltimore, MD No relevant financial relationships to disclose.
Advances in Transfusion and Blood Conservation Arman Kilic, MD Division of Cardiac Surgery, Department of Surgery, Johns Hopkins Hospital, Baltimore, MD No relevant financial relationships to disclose.
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Acute Kidney Injury for the General Surgeon
 Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit
 Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL
 resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL") Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Organ Donor Management Recommended Guidelines ADULT Brain Death (NDD)
") Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Neurological Determination of Death (NDD) has been performed by at least 2 licensed physicians Contact initiated with BC Transplant
Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Neurological Determination of Death (NDD) has been performed by at least 2 licensed physicians Contact initiated with BC Transplant
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Perioperative Fluid Management in ERPs
 Perioperative Fluid Management in ERPs Robert H. Thiele, M.D. Assistant Professor University of Virginia First Do No Harm Intravenous fluids should be considered a pharmacotherapeutic agent Just like all
Perioperative Fluid Management in ERPs Robert H. Thiele, M.D. Assistant Professor University of Virginia First Do No Harm Intravenous fluids should be considered a pharmacotherapeutic agent Just like all
Intraoperative Fluid Management. David G Hovord BA MB BChir FRCA Clinical Assistant Professor University of Michigan
 Intraoperative Fluid Management David G Hovord BA MB BChir FRCA Clinical Assistant Professor University of Michigan Objectives Examine impact of perioperative renal failure, and discuss structure and function
Intraoperative Fluid Management David G Hovord BA MB BChir FRCA Clinical Assistant Professor University of Michigan Objectives Examine impact of perioperative renal failure, and discuss structure and function
25. Fluid Management and Renal Function During a Laparoscopic Case Done Under CO 2 Pneumoperitoneum
 25. Fluid Management and Renal Function During a Laparoscopic Case Done Under CO 2 Pneumoperitoneum Gamal Mostafa, M.D. Frederick L. Greene, M.D. Minimally invasive surgery aims to attenuate the stress
25. Fluid Management and Renal Function During a Laparoscopic Case Done Under CO 2 Pneumoperitoneum Gamal Mostafa, M.D. Frederick L. Greene, M.D. Minimally invasive surgery aims to attenuate the stress
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
Recent reports have investigated the impact of
 Normal Saline Versus Lactated Ringer s Solution for Intraoperative Fluid Management in Patients Undergoing Abdominal Aortic Aneurysm Repair: An Outcome Study Jonathan H. Waters, MD, Alexandru Gottlieb,
Normal Saline Versus Lactated Ringer s Solution for Intraoperative Fluid Management in Patients Undergoing Abdominal Aortic Aneurysm Repair: An Outcome Study Jonathan H. Waters, MD, Alexandru Gottlieb,
Robotic Surgery for Esophageal Cancer
 Robotic Surgery for Esophageal Cancer Kemp H. Kernstine, MD PhD Division of Thoracic Surgery City of Hope Medical Center and Beckman Research Institute May 1, 2010 Esophageal Cancer on the Rise JNCI 2005,
Robotic Surgery for Esophageal Cancer Kemp H. Kernstine, MD PhD Division of Thoracic Surgery City of Hope Medical Center and Beckman Research Institute May 1, 2010 Esophageal Cancer on the Rise JNCI 2005,
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Perioperative Myocardial Infarction
 Perioperative Myocardial Infarction Which patient should UNDERGO CORONARY ANGIOGRAPHY? The Cardiologists view Hans Rickli, St.Gallen 1 Experience Standards Risk stratification Team approach.. Tightrope
Perioperative Myocardial Infarction Which patient should UNDERGO CORONARY ANGIOGRAPHY? The Cardiologists view Hans Rickli, St.Gallen 1 Experience Standards Risk stratification Team approach.. Tightrope
Post-Anesthesia Care In the ICU
 Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand?
 MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand? Ph Nafteux, MD Copenhagen, Nov 3rd 2011 Department of Thoracic Surgery, University Hospitals Leuven, Belgium W. Coosemans, H. Decaluwé, Ph.
MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand? Ph Nafteux, MD Copenhagen, Nov 3rd 2011 Department of Thoracic Surgery, University Hospitals Leuven, Belgium W. Coosemans, H. Decaluwé, Ph.
Acute And perioperative care of the burn-injured patient. Anesthesiology, V 122, No 2
 Acute And perioperative care of the burn-injured patient Anesthesiology, V 122, No 2 Reporter:R4 沈士鈞 Supervisor: 蔡欣怡醫師 Pathophysiology Initial evaluation and management Anesthetic managemen nt Pathophysiology
Acute And perioperative care of the burn-injured patient Anesthesiology, V 122, No 2 Reporter:R4 沈士鈞 Supervisor: 蔡欣怡醫師 Pathophysiology Initial evaluation and management Anesthetic managemen nt Pathophysiology
Declaring Brain Death. Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery
 Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
FOAM A New Style of Learning for a New Generation. Eric Einstein, M.D. Henry Ford Hospital Department of Emergency Medicine November 13, 2014
 FOAM A New Style of Learning for a New Generation Eric Einstein, M.D. Henry Ford Hospital Department of Emergency Medicine November 13, 2014 Objectives Define and discuss the basics Peer review a podcast
FOAM A New Style of Learning for a New Generation Eric Einstein, M.D. Henry Ford Hospital Department of Emergency Medicine November 13, 2014 Objectives Define and discuss the basics Peer review a podcast
6/5/2014. Sepsis Management and Hemodynamics. 2004: International group of experts,
 Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Trends In Hemodynamic Monitoring: A Review For Tertiary Care Providers
 ISPUB.COM The Internet Journal of Advanced Nursing Practice Volume 12 Number 1 Trends In Hemodynamic Monitoring: A Review For Tertiary Care Providers M E Zerlan Citation M E Zerlan.. The Internet Journal
ISPUB.COM The Internet Journal of Advanced Nursing Practice Volume 12 Number 1 Trends In Hemodynamic Monitoring: A Review For Tertiary Care Providers M E Zerlan Citation M E Zerlan.. The Internet Journal
Milestone Guide. CBD Anesthesia
 Table of Contents Department of Anesthesiology Foundations 1 Airway 1 Pharmacology 1 Physiology 1 Common Uncomplicated Anesthetics Practice 2 Obstetrics 2 Pain 2 Core 3 Perioperative Medicine 3 Complex
Table of Contents Department of Anesthesiology Foundations 1 Airway 1 Pharmacology 1 Physiology 1 Common Uncomplicated Anesthetics Practice 2 Obstetrics 2 Pain 2 Core 3 Perioperative Medicine 3 Complex
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
Edwards Critical Care Education. Perioperative Goal-Directed Therapy Protocol Summary
 Edwards Critical Care Education Perioperative Goal-Directed Therapy Protocol Summary Issue Date: November 2014 Evidence-based, Perioperative Goal-Directed Therapy (PGDT) protocols Note: This protocol summary
Edwards Critical Care Education Perioperative Goal-Directed Therapy Protocol Summary Issue Date: November 2014 Evidence-based, Perioperative Goal-Directed Therapy (PGDT) protocols Note: This protocol summary
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Colorectal non-inflammatory emergencies
 Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
SHOCK and the Trauma Victim. JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital.
 SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
Edwards Critical Care Education. Perioperative Goal-Directed Therapy Protocol Summary
 Edwards Critical Care Education Perioperative Goal-Directed Therapy Protocol Summary Issue Date: March 2013 Evidence-based, Perioperative Goal-Directed Therapy (PGDT) protocols Note: This protocol summary
Edwards Critical Care Education Perioperative Goal-Directed Therapy Protocol Summary Issue Date: March 2013 Evidence-based, Perioperative Goal-Directed Therapy (PGDT) protocols Note: This protocol summary
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq
 Dr.Ahmad farooq") Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH
 Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Hemodynamic Optimization HOW TO IMPLEMENT?
 Hemodynamic Optimization HOW TO IMPLEMENT? Why Hemodynamic Optimization? Are post-surgical complications exceptions? Patients undergoing surgery may develop post-surgical complications. The morbidity rate,
Hemodynamic Optimization HOW TO IMPLEMENT? Why Hemodynamic Optimization? Are post-surgical complications exceptions? Patients undergoing surgery may develop post-surgical complications. The morbidity rate,
INTRAVENOUS FLUID THERAPY. Tom Heaps Consultant Acute Physician
 INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal