Diagnosis & Management of Heparin-Induced Thrombocytopenia
|
|
|
- Godfrey Stewart
- 5 years ago
- Views:
Transcription

1 Diagnosis & Management of Heparin-Induced Thrombocytopenia An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric Tseng MD MScCH, University of Toronto Adam Cuker MD MS, University of Pennsylvania



2 Clinical Guidelines American Society of Hematology 2018 guidelines for management of venous thromboembolism: heparininduced thrombocytopenia Adam Cuker, Gowthami M. Arepally, Beng H. Chong, Douglas B. Cines, Andreas Greinacher, Yves Gruel, Lori A. Linkins, Stephen B. Rodner, Sixten Selleng, Theodore E. Warkentin, Ashleigh Wex, Reem A. Mustafa, Rebecca L. Morgan, and Nancy Santesso
3 ASH Clinical Practice Guidelines on VTE 1. Prevention of VTE in Surgical Hospitalized Patients 2. Prevention of VTE in Medical Hospitalized Patients 3. Treatment of Acute VTE (DVT and PE) 4. Optimal Management of Anticoagulation Therapy 5. Prevention and Treatment of VTE in Patients with Cancer 6. Heparin-Induced Thrombocytopenia (HIT) 7. Thrombophilia 8. Pediatric VTE 9. VTE in the Context of Pregnancy 10. Diagnosis of VTE
4 How were these ASH guidelines developed? PANEL FORMATION Each guideline panel was formed following these key criteria: Balance of expertise (including disciplines beyond hematology, and patients) Close attention to minimization and management of conflicts of interest CLINICAL QUESTIONS 10 to 20 clinicallyrelevant questions generated in PICO format (population, intervention, comparison, outcome) Example: PICO question In patients with suspected HIT and an intermediate probability 4Ts score, should non-heparin anticoagulants be provided at therapeutic or prophylactic intensity? EVIDENCE SYNTHESIS Evidence summary generated for each PICO question via systematic review of health effects plus: Resource use Feasibility Acceptability Equity Patient values and preferences MAKING RECOMMENDATIONS Recommendations made by guideline panel members based on evidence for all factors.
5 How patients and clinicians should use these recommendations For patients STRONG Recommendation ( The panel recommends ) Most individuals would want the intervention. CONDITIONAL Recommendation ( The panel suggests ) A majority would want the intervention, but many would not. For clinicians Most individuals should receive the intervention. Different choices will be appropriate for different patients, depending on their values and preferences. Use shared decision making.
6 Objectives By the end of this module, you should be able to 1. Describe a diagnostic algorithm for patients with suspected heparin-induced thrombocytopenia (HIT) 2. Compare non-heparin anticoagulants for the treatment of acute HIT 3. Describe recommendations for managing anticoagulation for cardiac surgery in patients with a previous history of HIT
7 HIT is a profoundly hypercoagulable state HIT is an iatrogenic disorder usually mediated by IgG antibodies that bind PF4-heparin complexes These antibodies cause a hypercoagulable state by activating platelets and procoagulant microparticles One-third to one-half of patients with HIT develop venous, arterial, or microvascular thrombosis Unfractionated heparin (UFH) associated with 10-fold increase in risk of HIT compared with LMWH
8 Case 1: Medical Inpatient Admission 82 year old male Past Medical History: Diabetes, hypertension, congestive heart failure Medications: Metformin, ramipril, aspirin, furosemide Admitted to: Internal Medicine ward with exacerbation of congestive heart failure, secondary to poor compliance with diet and diuretics Treated with: Intravenous furosemide, nitroglycerin patch Subcutaneous unfractionated heparin (UFH) 5,000 IU Q12H started on admission date for DVT prophylaxis
9 Case 1: Medical Inpatient Admission Bloodwork: Day 0 is admission date No fever, no other new medications. Normal blood pressure and heart rate. No signs or symptoms of venous thromboembolism. No bleeding or bruising No exposure to heparin in the 3 months prior to this admission Date Day Platelets (x 10 9 )
10 Considering your patient s progressive thrombocytopenia and heparin exposure, you are concerned about the possibility of HIT. Which of the following most accurately describes his clinical probability of HIT? A. Probably low probability, given overall clinical context B. Probably high probability, given overall clinical context C. Low probability, based on 4Ts score D. Intermediate probability, based on 4Ts score E. High probability, based on 4Ts score
11 Recommendation In patients with suspected HIT, the panel recommends using the 4Ts score to estimate the probability of HIT rather than a gestalt approach (strong recommendation, moderate certainty) Remarks: Missing or inaccurate information may lead to a faulty 4Ts score and inappropriate management Every effort should be made to obtain accurate and complete information necessary to calculate the 4Ts score. If key information is missing it may be prudent to err on the side of a higher 4Ts score. Reassess frequently. If there is a change in clinical picture, the 4Ts score should be recalculated.
12 The 4Ts Score: Clinical Probability Model Our patient: Platelets 67, > 50% drop. Onset of drop on day +6. No thrombosis. No other cause for thrombocytopenia. HIGH probability: 6-8 points INTERMEDIATE probability: 4-5 points LOW probability: 3 points Lo J Thromb Haemost 2006 ASH 2009 Clinical Guide
13 Your patient s 4Ts score indicates a high clinical probability for HIT. What diagnostic tests would you recommend at this point to confirm or exclude a diagnosis of HIT? A. None; patient is high probability and diagnosis is confirmed B. Immunoassay only (ex. HIT PF4/heparin ELISA) C. Functional test only (ex. serotonin release assay) D. Immunoassay, and if positive then perform functional test
14 Laboratory Diagnostic Testing for HIT HIT Immunoassay Tests Detect the presence of anti-pf4/heparin antibodies ELISA (detect IgG) ELISA (detect polyspecific antibodies) IgG-specific chemiluminescent assay Particle gel immunoassay (PaGIA) Latex agglutination assay Functional HIT Assays Assays that detect antibodies capable of binding and activating platelets Serotonin release assay (SRA) Heparin-induced platelet activation test (HIPA) Platelet aggregation test (PAT) Flow cytometry-based assays
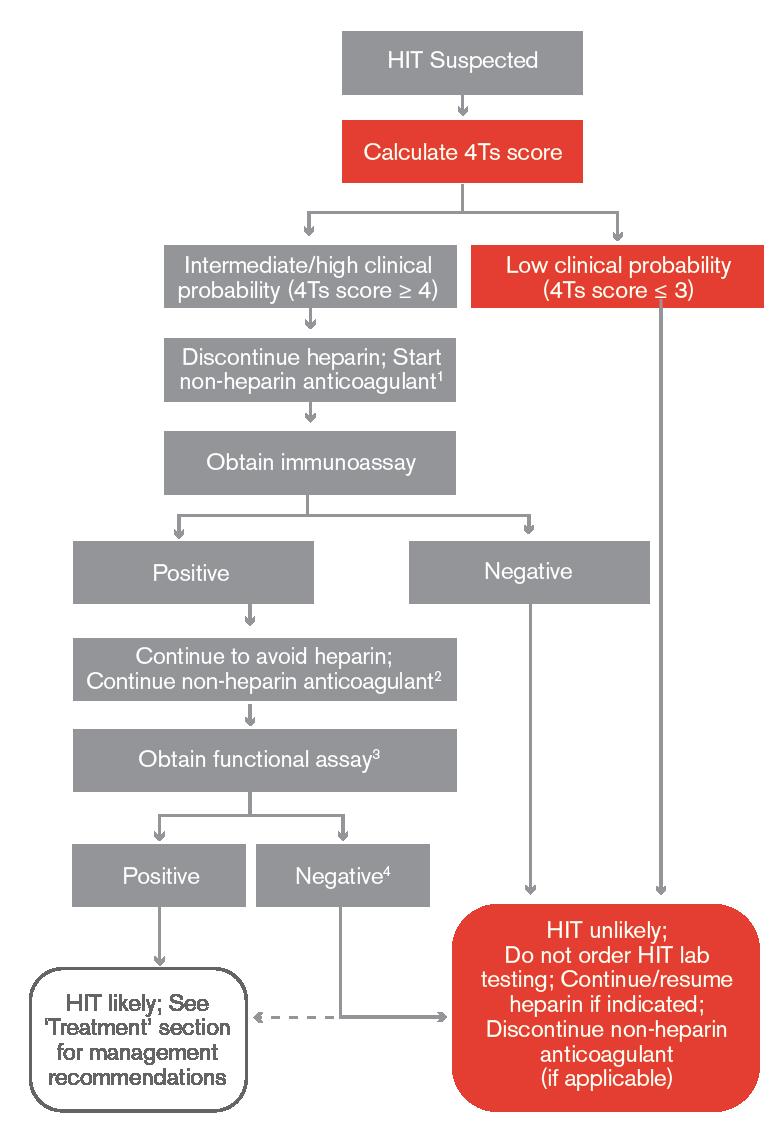
15 Recommendation If there is an intermediate- or high-probability 4Ts score, the panel recommends an immunoassay (strong recommendation, moderate certainty) If the immunoassay is positive and a functional assay is available (locally or as a send-out test to a reference laboratory), the panel suggests a functional assay (conditional recommendation, moderate certainty) Remark: Likelihood of HIT increases with a higher 4Ts score and a higher ELISA OD (Optical Density)
 A functional assay may not be necessary for patients with high probability 4Ts score and very strongly positive immunoassay (ELISA value of > 2.")
16 A diagnostic algorithm of intermediate/high 4Ts score, followed by immunoassay, followed by functional testing results in: Few false negatives (missed HIT diagnoses), and Few or no false positives (incorrect diagnoses of HIT) A functional assay may not be necessary for patients with high probability 4Ts score and very strongly positive immunoassay (ELISA value of > 2.0 OD units)
17 Your patient s 4Ts score indicates high probability for HIT, and you have sent off the HIT ELISA (result is pending). Currently, your patient is receiving subcutaneous UFH 5,000 units twice daily. What management strategy would you recommend while awaiting the HIT ELISA test results? A. Continue heparin as the diagnosis of HIT is not confirmed B. Stop heparin, wait for ELISA result C. Stop heparin, start non-heparin anticoagulant at prophylactic intensity D. Stop heparin, start non-heparin anticoagulant at therapeutic intensity E. Stop heparin, transfuse platelets
18 Recommendation In patients with suspected HIT and HIGH PROBABILITY 4Ts score: The panel recommends discontinuation of heparin and initiation of a non-heparin anticoagulant at therapeutic intensity (strong recommendation, moderate certainty) In patients with suspected HIT and INTERMEDIATE PROBABILITY 4Ts score: The panel recommends discontinuation of heparin (strong recommendation, moderate certainty) The panel suggests initiation of non-heparin anticoagulant at prophylactic intensity if patient is at high bleeding risk, therapeutic intensity if patient not at high bleeding risk In patients with INTERMEDIATE-risk 4Ts score who have high bleeding risk, there could be greater harm with therapeutic-intensity treatment (bleeding) with less potential benefit, because fewer such patients will have HIT
19 Therapeutic versus Prophylactic Intensity Non-heparin anticoagulant at therapeutic intensity is recommended over prophylactic intensity based on very low certainty of evidence 3 small studies comparing therapeutic versus prophylactic anticoagulation with Danaparoid, Lepirudin, or Fondaparinux Danaparoid showed 50% reduction in thrombosis with therapeutic dosing No difference in outcomes with Lepirudin and Fondaprainux However, strong recommendation based on likely large magnitude of benefit (prevention of thrombosis) Schindewolf Thromb Res 2012 Greinacher A Circulation 1999 Farner Thromb Haemost 2001
20 Recommendation In patients with HIT who are at average bleeding risk, the panel suggests against routine platelet transfusion (conditional recommendation, low certainty) Remark: Platelet transfusion may be an option for patients with active bleeding or at high bleeding risk Low certainty for beneficial or adverse effects of platelet transfusions in HIT Mixed results from observational studies One large database study (n = 6,332) suggested increase in arterial thrombotic events (adjusted odds ratio 3.4, 95% CI 1.2 to 9.5); other small cohort studies suggest no difference Goel Blood 2015 Refaai J Thromb Haemost 2010
21 Case 1: HIT Laboratory Test Results Your HIT immunoassay (ELISA) results are reported back that afternoon as optical density (OD) = 1.8 (NORMAL OD is < 0.4 at your lab). You ask your lab to send a sample to your local reference lab for a confirmatory functional assay (serotonin release assay). Your patient continues to be clinically stable with no symptoms or signs of pulmonary embolism, deep vein thrombosis, or arterial thrombosis.
22 Your patient has acute isolated HIT (without thrombosis), and platelet count is currently 67. Which of the following non-heparin anticoagulants would NOT be appropriate at this point? A. Argatroban B. Warfarin (vitamin K antagonist) C. Rivaroxaban D. Fondaparinux E. Danaparoid
23 Recommendation In patients with acute HITT or acute isolated HIT, the panel recommends against initiation of a VKA prior to platelet count recovery (platelets 150 x 10 9 /L) (strong recommendation, moderate certainty) Remarks: Also applies to those taking VKA at onset of acute HITT or acute isolated HIT In these patients, VKA would be discontinued and intravenous Vitamin K administered concomitant with initiation of a non-heparin anticoagulant In case series, early initiation of VKA associated: Warfarin-induced skin necrosis Venous limb gangrene Recurrent thrombosis Limb amputation
24 Recommendation In patients with acute HIT complicated by thrombosis (HITT) or acute HIT without thrombosis (isolated HIT), the panel recommends discontinuation of heparin and initiation of a non-heparin anticoagulant (strong recommendation, moderate certainty) The panel suggests argatroban, bivalirudin, danaparoid, fondaparinux or a direct oral anticoagulant (DOAC)
25 Rationale for Anticoagulant Selection Using a non-heparin anticoagulant (compared with stopping heparin +/- starting VKA) associated with: Fewer thrombotic events BUT probably increase in risk of major bleeding No direct comparisons of DOACs vs. parenteral anticoagulants in HIT Small numbers of patients treated with DOACs in case series Few thrombotic events (rivaroxaban 1/46, apixaban 0/12, dabigatran 1/11) Benefits and harms of DOACs compare favorably to parenteral agents
26 Rationale for Anticoagulant Selection Clinical Context Critical illness Increased bleeding risk Possible urgent procedures Life- or limb-threatening VTE (massive PE or venous limb gangrene) Clinically stable patients at average bleeding risk Implications for Anticoagulant Selection Argatroban or Bivalirudin (shorter duration of effect) If moderate or severe hepatic dysfunction (Childs-Pugh B or C), may be advisable to avoid argatroban or use a reduced dose Parenteral non-heparin anticoagulant preferred (Argatroban, Bivalirudin, Danaparoid, Fondaparinux) Few such patients treated with DOACs Fondaparinux or DOACs reasonable Most published DOAC experience with Rivaroxaban
27 Anticoagulant (mechanism, route) Argatroban (direct thrombin inhibitor) IV Bivalirudin (direct thrombin inhibitor) IV Danaparoid (indirect Xa inhibitor) IV Fondaparinux (indirect Xa inhibitor) SC Rivaroxaban (direct Xa inhibitor) PO Dosing Bolus: None Infusion: STANDARD (2 mcg/kg/min), REDUCED DOSE for liver dysfunction, CHF, post-cardiac surgery ( mcg/kg/min) Bolus: None Infusion: STANDARD (0.15 mg/kg/hr); consider REDUCED DOSE for renal or liver dysfunction Bolus: Weight-based ( units) Infusion: INITIAL ACCELERATED (400 units/hr x 4 hr, then 300 units/hr x 4 hr), then MAINTENANCE ( units/hr) < 50 kg 5 kg daily kg 7.5 mg daily > 100 kg 10 mg daily HITT: 15 mg twice daily x 3 weeks, then 20 mg daily Isolated HIT: 15 mg twice daily until platelet count recovery ( 150) Clearance & Monitoring Hepatobiliary clearance Adjusted to aptt times baseline Enzymatic clearance Adjusted to aptt times baseline Renal clearance Adjusted to anti-xa activity units/ml Renal clearance No monitoring Renal clearance No monitoring
28 Case 1: Treatment You decide to start your patient on rivaroxaban 15 mg PO BID and discontinue subcutaneous UFH. Over the next 8 days, your patient s platelet count gradually rises from 67 to 165, and there is no evidence of bleeding.
29 Your patient has no symptoms of deep vein thrombosis or pulmonary embolism. Which of the following tests would you suggest to screen for asymptomatic VTE? A. There are no symptoms, so imaging is not indicated B. Bilateral upper extremity compression ultrasound (US) C. Bilateral lower extremity compression ultrasound (US) D. CT pulmonary angiogram E. Choices C & D
30 Recommendation In patients with acute isolated HIT, the panel suggests: Bilateral lower extremity compression US to screen for asymptomatic proximal DVT (conditional recommendation, very low certainty) Upper-extremity US in patients with an upper extremity central venous catheter, in the limb with the catheter, to screen for asymptomatic DVT (conditional recommendation, very low certainty) Ultrasound studies have identified silent lower extremity DVT in 12-44% of asymptomatic patients with HIT
31 Case 1: HITT He is found to have an occlusive left popliteal vein DVT. He continues rivaroxaban 15 mg BID for 3 weeks, then takes rivaroxaban 20 mg daily for a total of 3 months. At 3 months, his platelet count is normal (205 x 10 9 /L) and he is at his baseline health status. You ask him to stop rivaroxaban. 15 months later, he returns to hospital with CHF again and is found to have severe aortic stenosis, with an aortic valve area of 0.6 cm 2. He requires a valve replacement.
32 Your patient with a history of HITT requires open heart surgery, with intraoperative anticoagulation while on pump. His platelet count is normal. You repeat his HIT ELISA and OD is 0.2 (NORMAL < 0.4). What would you suggest that your patient receive for intraoperative anticoagulation? A. Preoperative plasma exchange and intraoperative heparin B. Intraoperative heparin only C. Intraoperative heparin with an antiplatelet agent D. Intraoperative bivalirudin only E. Intraoperative bivalirudin with an antiplatelet agent
33 Five Phases of HIT Phase Platelet count Immunoassay Functional assay Suspected HIT Decreased?? Acute HIT Decreased + + Subacute HIT A Normal + + Subacute HIT B Normal + Remote HIT Normal
34 Recommendation In patients with subacute HIT B or remote HIT who require cardiovascular surgery, the panel suggests intraoperative anticoagulation with heparin rather than treatment with a non-heparin anticoagulant, plasma exchange and heparin, or heparin combined with antiplatelet agent (conditional recommendation, very low certainty) Remarks: Treatment with heparin would be limited to the intraoperative setting, and avoided before and after surgery Postoperative platelet count monitoring for HIT may be necessary, even when postoperative heparin is not given, because delayed-onset (autoimmune) HIT beginning 5 to 10 days after intraoperative heparin exposure has been reported
35 Case 2: Medical Inpatient Admission 82 year old male Past Medical History: Diabetes, hypertension, congestive heart failure Medications: Metformin, ramipril, aspirin, furosemide Admitted to: Internal Medicine ward with exacerbation of congestive heart failure, secondary to poor compliance with diet and diuretics Treated with: Intravenous furosemide, nitroglycerin patch Subcutaneous unfractionated heparin (UFH) 5,000 IU Q12H started on admission date for DVT prophylaxis
36 Case 2: Medical Inpatient Admission Bloodwork: Day 0 is admission date No fever, no other new medications. Normal blood pressure and heart rate. No signs or symptoms of venous thromboembolism No bruising or bleeding No exposures to heparin in the 3 months prior to this admission Date Day Platelets (x 10 9 )
37 Considering your patient s progressive thrombocytopenia and heparin exposure, you are concerned about the possibility of HIT. Which of the following most accurately describes his clinical probability of HIT? A. Probably low probability, given overall clinical context B. Probably high probability, given overall clinical context C. Low probability, based on 4Ts score D. Intermediate probability, based on 4Ts score E. High probability, based on 4Ts score
38 The 4Ts Score: Clinical Probability Model Our patient: Platelets 125, 30-50% drop Drop at Day +2 No thrombosis No other cause for thrombocytopenia HIGH probability: 6-8 points INTERMEDIATE probability: 4-5 points LOW probability: 3 points Lo J Thromb Haemost 2006 ASH 2009 Clinical Guide
39 Your patient s 4Ts score (3) indicates a low clinical probability for HIT. What diagnostic tests would you recommend at this point to confirm or exclude a diagnosis of HIT? A. None; patient is low probability and HIT is highly unlikely B. Immunoassay only (ex. HIT PF4/heparin ELISA) C. Functional test only (ex. serotonin release assay) D. Immunoassay, and if positive then perform functional test
40 Recommendation In patients with suspected HIT and low probability 4Ts score, the panel recommends against HIT laboratory testing (strong recommendation, moderate certainty) Remark: HIT laboratory testing may be appropriate for patients with a low probability 4Ts score if there is uncertainty about the 4Ts score (for example, due to missing data)
41
42 Case 2: Resolution Given his low clinical probability, you elect not to send his HIT ELISA assay or functional assay. He continues to receive SC heparin. With treatment for CHF, his thrombocytopenia improves. He is discharged with a follow-up outpatient CBC to ensure resolution of thrombocytopenia Date Day Platelets (x 10 9 ) Date Platelets (x 10 9 )
43 Additional Topics in these Guidelines Platelet count monitoring in patients receiving heparin Prophylactic IVC filter insertion in the setting of acute HIT Duration of non-heparin anticoagulant therapy in acute isolated HIT Anticoagulant management for percutaneous coronary intervention in patients with acute HIT or previous history of HIT Anticoagulant therapy for HIT in renal replacement therapy
44 Areas of Future Investigation Development of novel HIT immunoassays and functional assays Outcomes from treatment of acute HIT with DOACs Comparisons of DOACs and parenteral non-heparin anticoagulants Role of concomitant antiplatelet and anticoagulant therapy in HIT Impact of screening for asymptomatic DVT in acute isolated HIT Optimal duration of anticoagulation in acute isolated HIT Intraoperative anticoagulant management for cardiovascular surgery
45 In Summary: Back to our Objectives 1. Describe a diagnostic algorithm for patients with suspected heparin-induced thrombocytopenia (HIT) 4Ts score, immunoassay, functional assay 2. Compare non-heparin anticoagulants for treatment of acute HIT DOACs or parenteral options (Argatroban, Fondaparinux, Danaparoid, Bivalirudin) 3. Describe recommendations for managing anticoagulation for cardiac surgery in patients with a previous history of HIT Determination of HIT clinical status with ELISA and/or functional assay helps to determine intraoperative anticoagulation plan
46 Acknowledgements ASH Guideline Panel team members Knowledge Synthesis team members McMaster University GRADE Centre Author of ASH VTE Slide Sets: Eric Tseng MD MScCH, University of Toronto and Paul Monagle MD MBBS MSc, University of Melbourne, Royal Children s Hospital See more about the ASH VTE guidelines at Don t miss our updated HIT Pocket Guide!
Diagnosis and Management of Heparin-Induced Thrombocytopenia (HIT)
") ASH CLINICAL PRACTICE GUIDELINES VENOUS THROMBOEMBOLISM (VTE) POCKET GUIDE Diagnosis and Management of Heparin-Induced Thrombocytopenia (HIT) A POCKET GUIDE FOR THE CLINICIAN DECEMBER 08 Allyson M. Pishko,
ASH CLINICAL PRACTICE GUIDELINES VENOUS THROMBOEMBOLISM (VTE) POCKET GUIDE Diagnosis and Management of Heparin-Induced Thrombocytopenia (HIT) A POCKET GUIDE FOR THE CLINICIAN DECEMBER 08 Allyson M. Pishko,
HEPARIN-INDUCED THROMBOCYTOPENIA (HIT)
") HEPARIN-INDUCED THROMBOCYTOPENIA (HIT) OBJECTIVE: To assist clinicians with the investigation and management of suspected and documented heparin-induced thrombocytopenia (HIT). BACKGROUND: HIT is a transient,
HEPARIN-INDUCED THROMBOCYTOPENIA (HIT) OBJECTIVE: To assist clinicians with the investigation and management of suspected and documented heparin-induced thrombocytopenia (HIT). BACKGROUND: HIT is a transient,
ASH Draft Recommendations for Heparin-Induced Thrombocytopenia. Draft
 ASH Recommendations for Heparin-Induced Thrombocytopenia INTRODUCTION American Society of Hematology (ASH) guidelines are based on a systematic review of available evidence. Through a structured process,
ASH Recommendations for Heparin-Induced Thrombocytopenia INTRODUCTION American Society of Hematology (ASH) guidelines are based on a systematic review of available evidence. Through a structured process,
Heparin-Induced Thrombocytopenia (HIT)
") Heparin-Induced Thrombocytopenia (HIT) Joshua Ononuju, Pharm. D. Owensboro Medical Health Systems Objectives Overview Pathogenesis Risk factors Clinical Presentation and Diagnosis Treatment goals and options
Heparin-Induced Thrombocytopenia (HIT) Joshua Ononuju, Pharm. D. Owensboro Medical Health Systems Objectives Overview Pathogenesis Risk factors Clinical Presentation and Diagnosis Treatment goals and options
Prophylaxis for Hospitalized and Non-Hospitalized Medical Patients
 Prophylaxis for Hospitalized and Non-Hospitalized Medical Patients An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric
Prophylaxis for Hospitalized and Non-Hospitalized Medical Patients An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric
Obesity, renal failure, HIT: which anticoagulant to use?
 Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Heparin induced thrombocytopenia in the critically ill: How to interpret anti- PF4 antibody test results
 Heparin induced thrombocytopenia in the critically ill: How to interpret anti- PF4 antibody test results Daniel H. Kett, M.D. Professor of Clinical Medicine Director MICU, Jackson Memorial Hospital University
Heparin induced thrombocytopenia in the critically ill: How to interpret anti- PF4 antibody test results Daniel H. Kett, M.D. Professor of Clinical Medicine Director MICU, Jackson Memorial Hospital University
Heparin-Induced Thrombocytopenia. Steven Baroletti, PharmD., M.B.A., BCPS Brigham and Women s Hospital
 Heparin-Induced Thrombocytopenia Steven Baroletti, PharmD., M.B.A., BCPS Brigham and Women s Hospital Heparin-induced thrombocytopenia (HIT) A serious concern associated with thrombosis development following
Heparin-Induced Thrombocytopenia Steven Baroletti, PharmD., M.B.A., BCPS Brigham and Women s Hospital Heparin-induced thrombocytopenia (HIT) A serious concern associated with thrombosis development following
10/24/2013. Heparin-Induced Thrombocytopenia (HIT) Anticoagulation Management in ECMO Therapy:
 Anticoagulation Management in ECMO Therapy:") Anticoagulation Management in ECMO Therapy: Heparin-Induced (HIT) Michael H. Creer, MD Professor of Pathology Director, Clinical Laboratories, Medical Co- Director, Hematopathology and Chief, Division
Anticoagulation Management in ECMO Therapy: Heparin-Induced (HIT) Michael H. Creer, MD Professor of Pathology Director, Clinical Laboratories, Medical Co- Director, Hematopathology and Chief, Division
A Great Clinical Paradox. Narendranath Epperla MD Sowjanya Bapani MD Steven Yale MD, FACP
 A Great Clinical Paradox Narendranath Epperla MD Sowjanya Bapani MD Steven Yale MD, FACP Initial Presentation 61 y/o Vietnam veteran with a past H/O hypertension, back pain and depression on Lisinopril,
A Great Clinical Paradox Narendranath Epperla MD Sowjanya Bapani MD Steven Yale MD, FACP Initial Presentation 61 y/o Vietnam veteran with a past H/O hypertension, back pain and depression on Lisinopril,
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
What You Should Know
 1 New 2018 ASH Clinical Practice Guidelines on Venous Thromboembolism: What You Should Know New 2018 ASH Clinical Practice Guidelines on Venous Thromboembolism: What You Should Know The American Society
1 New 2018 ASH Clinical Practice Guidelines on Venous Thromboembolism: What You Should Know New 2018 ASH Clinical Practice Guidelines on Venous Thromboembolism: What You Should Know The American Society
Heparin-Induced Thrombocytopenia and Thrombosis: HITT Syndrome Update
 Heparin-Induced Thrombocytopenia and Thrombosis: HITT Syndrome Update Surgery Grand Rounds February 18, 2011 Anne T. Neff, MD Director, Hemostasis & Thrombosis Clinic Case Presentation #1 43 yo male with
Heparin-Induced Thrombocytopenia and Thrombosis: HITT Syndrome Update Surgery Grand Rounds February 18, 2011 Anne T. Neff, MD Director, Hemostasis & Thrombosis Clinic Case Presentation #1 43 yo male with
Treatment and Prevention of Heparin-Induced Thrombocytopenia
 CHEST Supplement ANTITHROMBOTIC THERAPY AND PREVENTION OF THROMBOSIS, 9TH ED: ACCP GUIDELINES Treatment and Prevention of Heparin-Induced Thrombocytopenia Antithrombotic Therapy and Prevention of Thrombosis,
CHEST Supplement ANTITHROMBOTIC THERAPY AND PREVENTION OF THROMBOSIS, 9TH ED: ACCP GUIDELINES Treatment and Prevention of Heparin-Induced Thrombocytopenia Antithrombotic Therapy and Prevention of Thrombosis,
Treatment of Pediatric Venous Thromboembolism
 Treatment of Pediatric Venous Thromboembolism An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric Tseng MD, MScCH, University
Treatment of Pediatric Venous Thromboembolism An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric Tseng MD, MScCH, University
10 Key Things the Vascular Community Should Know about the DOACs Heather Gornik, MD, RVT, RPVI
 10 Key Things the Vascular Community Should Know about the DOACs Heather Gornik, MD, RVT, RPVI Cleveland Clinic Heart and Vascular Institute Heather L. Gornik, MD has the following relationships to disclose:
10 Key Things the Vascular Community Should Know about the DOACs Heather Gornik, MD, RVT, RPVI Cleveland Clinic Heart and Vascular Institute Heather L. Gornik, MD has the following relationships to disclose:
Objectives. Heparin. Heparin & HIT: State of the Art. Acknowledge Heparin (almighty) HIT? Why care? Is it HIT? It is HIT. Now what?
 HIT? Why care? Is it HIT? It is HIT. Now what?") Heparin & HIT: State of the Art Erika R. Ketteler, MD MA NMVAHCS, Vascular Surgery Assistant Professor of Surgery, UNM Objectives Acknowledge Heparin (almighty) HIT? Why care? Is it HIT? It is HIT. Now
Heparin & HIT: State of the Art Erika R. Ketteler, MD MA NMVAHCS, Vascular Surgery Assistant Professor of Surgery, UNM Objectives Acknowledge Heparin (almighty) HIT? Why care? Is it HIT? It is HIT. Now
Diagnosis of Venous Thromboembolism
 Diagnosis of Venous Thromboembolism An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric Tseng MD MScCH, University of
Diagnosis of Venous Thromboembolism An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric Tseng MD MScCH, University of
Treatment and Prevention of Heparin-Induced Thrombocytopenia*
 Supplement ANTITHROMBOTIC AND THROMBOLYTIC THERAPY 8TH ED: ACCP GUIDELINES Treatment and Prevention of Heparin-Induced Thrombocytopenia* American College of Chest Physicians Evidence-Based Clinical Practice
Supplement ANTITHROMBOTIC AND THROMBOLYTIC THERAPY 8TH ED: ACCP GUIDELINES Treatment and Prevention of Heparin-Induced Thrombocytopenia* American College of Chest Physicians Evidence-Based Clinical Practice
HIT Me With Your Best Shot A Review of Heparin-Induced Thrombocytopenia
 HIT Me With Your Best Shot A Review of Heparin-Induced Thrombocytopenia Presented by: Melissa Hawkins & Natalie LeBlanc Pharmacy Residents Horizon Health Network The Moncton Hospital November 6 th, 2010
HIT Me With Your Best Shot A Review of Heparin-Induced Thrombocytopenia Presented by: Melissa Hawkins & Natalie LeBlanc Pharmacy Residents Horizon Health Network The Moncton Hospital November 6 th, 2010
Venous Thromboembolism National Hospital Inpatient Quality Measures
 Venous Thromboembolism National Hospital Inpatient Quality Measures Presentation Overview Review venous thromboembolism as a new mandatory measure set Outline measures with exclusions and documentation
Venous Thromboembolism National Hospital Inpatient Quality Measures Presentation Overview Review venous thromboembolism as a new mandatory measure set Outline measures with exclusions and documentation
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY
 ASWAN UNIVERSITY") New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
Venous Thromboembolism Prophylaxis
 Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
The Perioperative Management of Heparin Induced Thrombocytopenia. Chaitan K. Narsule, M.D. March 5, 2008
 The Perioperative Management of Heparin Induced Thrombocytopenia Chaitan K. Narsule, M.D. March 5, 2008 Overview Case Presentation Incidence of HIT Pathophysiology Clinical Presentation Laboratory Diagnosis
The Perioperative Management of Heparin Induced Thrombocytopenia Chaitan K. Narsule, M.D. March 5, 2008 Overview Case Presentation Incidence of HIT Pathophysiology Clinical Presentation Laboratory Diagnosis
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Slide 1. Slide 2. Slide 3. Outline of This Presentation
 Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Page 1 of 6. Low 1 (score 0-3) Monitor platelets and signs and symptoms of thrombosis and continue heparin
 Monitor platelets and signs and symptoms of thrombosis and continue heparin") Page 1 of 6 Estimate probability of HIT using the Four T s 1 Low 1 (score 0-3) Intermediate 1 (score 4-5) or High 1 (score 6-8) Monitor platelets and signs and symptoms of thrombosis and continue heparin
Page 1 of 6 Estimate probability of HIT using the Four T s 1 Low 1 (score 0-3) Intermediate 1 (score 4-5) or High 1 (score 6-8) Monitor platelets and signs and symptoms of thrombosis and continue heparin
Venous Thromboembolism (VTE) in Myeloma. Christine Chen May 2017
 in Myeloma. Christine Chen May 2017") Venous Thromboembolism (VTE) in Myeloma Christine Chen May 2017 Objectives 1. Review the magnitude of the problem and why myeloma patients are at risk of VTE 2. Discuss thromboprophylaxis approaches in
Venous Thromboembolism (VTE) in Myeloma Christine Chen May 2017 Objectives 1. Review the magnitude of the problem and why myeloma patients are at risk of VTE 2. Discuss thromboprophylaxis approaches in
Clinical issues which drug for which patient
 Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Heparin-induced thrombocytopenia (HIT) is an antibody-mediated,
 is an antibody-mediated,") Heparin-Induced Thrombocytopenia: Recognition, Treatment, and Prevention The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Theodore E. Warkentin, MD, Chair; and Andreas Greinacher,
Heparin-Induced Thrombocytopenia: Recognition, Treatment, and Prevention The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Theodore E. Warkentin, MD, Chair; and Andreas Greinacher,
WMC PHARMACY ANTICOAGULATION PROTOCOL Current Revision: July 2017 GENERAL ORDER PROCESSING AND MANAGEMENT
 WMC PHARMACY ANTICOAGULATION PROTOCOL Current Revision: July 2017 GENERAL ORDER PROCESSING AND MANAGEMENT - Entering orders for anticoagulation in Cerner Providers will enter individual orders (oneoffs)
WMC PHARMACY ANTICOAGULATION PROTOCOL Current Revision: July 2017 GENERAL ORDER PROCESSING AND MANAGEMENT - Entering orders for anticoagulation in Cerner Providers will enter individual orders (oneoffs)
Updates in venous thromboembolism. Cecilia Becattini University of Perugia
 Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Venous thrombosis is common and often occurs spontaneously, but it also frequently accompanies medical and surgical conditions, both in the community
 Venous Thrombosis Venous Thrombosis It occurs mainly in the deep veins of the leg (deep vein thrombosis, DVT), from which parts of the clot frequently embolize to the lungs (pulmonary embolism, PE). Fewer
Venous Thrombosis Venous Thrombosis It occurs mainly in the deep veins of the leg (deep vein thrombosis, DVT), from which parts of the clot frequently embolize to the lungs (pulmonary embolism, PE). Fewer
Optimal Management of Anticoagulation Therapy
 Optimal Management of Anticoagulation Therapy An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric Tseng MD MScCH, University
Optimal Management of Anticoagulation Therapy An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric Tseng MD MScCH, University
Medical Patients: A Population at Risk
 Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Clinical Guideline for Anticoagulation in VTE
 Clinical Guideline for Anticoagulation in VTE These clinical guidelines are intended to provide evidence-based recommendations regarding the anticoagulation in patients with DVT and PE. Please note that
Clinical Guideline for Anticoagulation in VTE These clinical guidelines are intended to provide evidence-based recommendations regarding the anticoagulation in patients with DVT and PE. Please note that
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel)
") New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
Disclosures. Learning Objectives. Financial: none. Off label discussion: Recommendations in lieu of data
 Kathryn Hassell, MD Professor of Medicine, Division of Hematology University of Colorado Denver Disclosures Financial: none Off label discussion: Prothormbin complex concentrates for DOAC reversal Use
Kathryn Hassell, MD Professor of Medicine, Division of Hematology University of Colorado Denver Disclosures Financial: none Off label discussion: Prothormbin complex concentrates for DOAC reversal Use
ADMINISTRATIVE CLINICAL Page 1 of 6
 ADMINISTRATIVE CLINICAL Page 1 of 6 Anticoagulant Guidelines #2: REVERSAL OF OR MANAGEMENT OF BLEEDING WITH ANTICOAGULANTS Origination Date: Revision Date: Reviewed Date: 09/12 09/12, 01/13, 11/13, 11/15
ADMINISTRATIVE CLINICAL Page 1 of 6 Anticoagulant Guidelines #2: REVERSAL OF OR MANAGEMENT OF BLEEDING WITH ANTICOAGULANTS Origination Date: Revision Date: Reviewed Date: 09/12 09/12, 01/13, 11/13, 11/15
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE)
") DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
Heparin Induced Thrombocytopenia (HIT) without Thrombocytopenia-A case report and a literature review
 without Thrombocytopenia-A case report and a literature review") ISPUB.COM The Internet Journal of Hematology Volume 5 Number 2 Heparin Induced Thrombocytopenia (HIT) without Thrombocytopenia-A case report and a literature review I Ahmed, M Naglak, H Rashid Citation
ISPUB.COM The Internet Journal of Hematology Volume 5 Number 2 Heparin Induced Thrombocytopenia (HIT) without Thrombocytopenia-A case report and a literature review I Ahmed, M Naglak, H Rashid Citation
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE VENOUS THROMBOEMBOLISM PROPHYLAXIS SCOPE Provincial Acute and Sub-Acute Care Facilities APPROVAL AUTHORITY Alberta Health Services Executive Committee SPONSOR Vice President, Quality and Chief Medical
TITLE VENOUS THROMBOEMBOLISM PROPHYLAXIS SCOPE Provincial Acute and Sub-Acute Care Facilities APPROVAL AUTHORITY Alberta Health Services Executive Committee SPONSOR Vice President, Quality and Chief Medical
With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis
 BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients
 4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients Assess Thrombosis risk: baseline risk in an individual patient plus additional thrombotic risk
4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients Assess Thrombosis risk: baseline risk in an individual patient plus additional thrombotic risk
Anticoagulation Overview Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita
 Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
Heparin-induced thrombocytopenia (HIT; sometimes
 Contemporary Reviews in Cardiovascular Medicine When Heparins Promote Thrombosis Review of Heparin-Induced Thrombocytopenia Ik-Kyung Jang, MD, PhD; Marcie J. Hursting, PhD Heparin-induced thrombocytopenia
Contemporary Reviews in Cardiovascular Medicine When Heparins Promote Thrombosis Review of Heparin-Induced Thrombocytopenia Ik-Kyung Jang, MD, PhD; Marcie J. Hursting, PhD Heparin-induced thrombocytopenia
HIT in ECMO: a challenging complication
 HIT in ECMO: a challenging complication Blanca Martinez SOC Anestesia e Rianimazione 2 Direttore R. Muzzi Azienda Ospedaliero-Universitaria SM della Misericordia di Udine martinez.blanca@aoud.sanita.fvg.it
HIT in ECMO: a challenging complication Blanca Martinez SOC Anestesia e Rianimazione 2 Direttore R. Muzzi Azienda Ospedaliero-Universitaria SM della Misericordia di Udine martinez.blanca@aoud.sanita.fvg.it
Disclosures. DVT: Diagnosis and Treatment. Questions To Ask. Dr. Susanna Shin - DVT: Diagnosis and Treatment. Acute Venous Thromboembolism (VTE) None
 None") Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
DOAC and NOAC are terms for a novel class of directly acting oral anticoagulant drugs including Rivaroxaban, Apixaban, Edoxaban, and Dabigatran.
 Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
Novel Anticoagulant Drugs. by: Dr. M. Kamandi Fellowship of hematology and Oncology
 Novel Anticoagulant Drugs by: Dr. M. Kamandi Fellowship of hematology and Oncology A-Novel Oral Anticoagulants A drug that is: safe and effective has predictable pharmacology has few drug drug and drug
Novel Anticoagulant Drugs by: Dr. M. Kamandi Fellowship of hematology and Oncology A-Novel Oral Anticoagulants A drug that is: safe and effective has predictable pharmacology has few drug drug and drug
New Oral Anticoagulant Drugs in the Prevention of DVT
 New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
New Oral Anticoagulant Drugs in the Prevention of DVT Targets for Anticoagulants ORAL DIRECT VKAs inhibit the hepatic synthesis of several coagulation factors Rivaroxaban Apixaban Edoxaban Betrixaban X
Objectives. Venous Thromboembolism (VTE) Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?
 Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?") Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM. Gordon Lowe Professor of Vascular Medicine University of Glasgow
 CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism
 Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Bridging anticoagulation definition
 Bridging anticoagulation definition Giving a short-acting anticoagulant, consisting of sc LMWH or ev UFH for 10 to 12 day period during interruption of VKA therapy when the INR is not within therapeutic
Bridging anticoagulation definition Giving a short-acting anticoagulant, consisting of sc LMWH or ev UFH for 10 to 12 day period during interruption of VKA therapy when the INR is not within therapeutic
Misunderstandings of Venous thromboembolism prophylaxis
 Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY
 INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
a. A pharmacist may order a baseline SCr per protocol
 UNITYPOINT HEALTH - MARSHALLTOWN Marshalltown, Iowa PHARMACY POLICY AND PROCEDURE Subject: Anticoagulant Therapy Per Practice Protocol (Formerly Anticoagulant therapy #NPSG.03.05.01) Inpatient Warfarin
UNITYPOINT HEALTH - MARSHALLTOWN Marshalltown, Iowa PHARMACY POLICY AND PROCEDURE Subject: Anticoagulant Therapy Per Practice Protocol (Formerly Anticoagulant therapy #NPSG.03.05.01) Inpatient Warfarin
Treatment Options and How They Work
 Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Heparin-induced thrombocytopenia (HIT)
") Heparin-induced thrombocytopenia: Principles for early recognition and management JOHN R. BARTHOLOMEW, MD; SUSAN M. BEGELMAN, MD; AND AMJAD ALMAHAMEED, MD ABSTRACT Heparin-induced thrombocytopenia (HIT)
Heparin-induced thrombocytopenia: Principles for early recognition and management JOHN R. BARTHOLOMEW, MD; SUSAN M. BEGELMAN, MD; AND AMJAD ALMAHAMEED, MD ABSTRACT Heparin-induced thrombocytopenia (HIT)
Are guidelines for anticoagulation useful in cancer patients?
 Session 3 Striking a Balance Between Bleeding and the Risk of Thrombosis in Cancer Patients Are guidelines for anticoagulation useful in cancer patients? Sebastian Szmit Department of Pulmonary Circulation
Session 3 Striking a Balance Between Bleeding and the Risk of Thrombosis in Cancer Patients Are guidelines for anticoagulation useful in cancer patients? Sebastian Szmit Department of Pulmonary Circulation
10/8/2012. Disclosures. Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines. Goals and Objectives. Outline
 Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
Disclosures. Overview. Have you ever. The Perioperative Management of Anticoagulants. No financial conflicts of interest to disclose
 Disclosures No financial conflicts of interest to disclose The Perioperative Management of Anticoagulants Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical
Disclosures No financial conflicts of interest to disclose The Perioperative Management of Anticoagulants Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical
Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1
 CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
DOAC for VTE. Direct Oral Anticoagulants Clint Shedd DNP, FNP-BC Emory University
 DOAC for VTE Direct Oral Anticoagulants Clint Shedd DNP, FNP-BC Emory University No disclosures Direct Oral Anticoagulants Understand VTE and the ACCP s position on it List the DOACs available in the US
DOAC for VTE Direct Oral Anticoagulants Clint Shedd DNP, FNP-BC Emory University No disclosures Direct Oral Anticoagulants Understand VTE and the ACCP s position on it List the DOACs available in the US
Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol
 Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol Page Platelet Inhibitors 2 Aspirin, Clopidogrel (Plavix), Prasugrel (Effient) & Ticagrelor
Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol Page Platelet Inhibitors 2 Aspirin, Clopidogrel (Plavix), Prasugrel (Effient) & Ticagrelor
CLINICIAN UPDATE. Heparin-induced thrombocytopenia. Diagnosis and Management. Theodore E. Warkentin, MD
 CLINICIAN UPDATE Heparin-Induced Thrombocytopenia Diagnosis and Management Theodore E. Warkentin, MD Heparin-induced thrombocytopenia (HIT) is an adverse drug reaction characterized by thrombocytopenia
CLINICIAN UPDATE Heparin-Induced Thrombocytopenia Diagnosis and Management Theodore E. Warkentin, MD Heparin-induced thrombocytopenia (HIT) is an adverse drug reaction characterized by thrombocytopenia
Anticoagulation. MPharm Programme & OSPAP Programme. Tania Jones Senior Lecturer in Pharmacy Practice & Therapeutics
 MPharm Programme & OSPAP Programme Anticoagulation Tania Jones Senior Lecturer in Pharmacy Practice & Therapeutics tania.jones@sunderland.ac.uk Lecture MPHM13 / MPHM14 2017-2018 MPHM13 & MPHM14 Objectives
MPharm Programme & OSPAP Programme Anticoagulation Tania Jones Senior Lecturer in Pharmacy Practice & Therapeutics tania.jones@sunderland.ac.uk Lecture MPHM13 / MPHM14 2017-2018 MPHM13 & MPHM14 Objectives
Challenges in Anticoagulation and Thromboembolism
 Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture
 Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
New Age Anticoagulants: Bleeding Considerations
 Ontario Regional Blood Coordinating Network March 23, 2012 New Age Anticoagulants: Bleeding Considerations Bill Geerts, MD, FRCPC Thromboembolism Specialist, Sunnybrook HSC Professor of Medicine, University
Ontario Regional Blood Coordinating Network March 23, 2012 New Age Anticoagulants: Bleeding Considerations Bill Geerts, MD, FRCPC Thromboembolism Specialist, Sunnybrook HSC Professor of Medicine, University
Pulmonary Thromboembolism
 Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales
 John Fletcher Wound Care Association of New South Wales") Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales Merimbula, 6 th November 2010 University of Sydney Department of Surgery Westmead Hospital
Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales Merimbula, 6 th November 2010 University of Sydney Department of Surgery Westmead Hospital
New Oral Anticoagulants Prevention and Treatment of DVT and PE
 New Oral Anticoagulants Prevention and Treatment of DVT and PE Grigoris T Gerotziafas Groupe de Thrombose Equipe de recherche ER2UPMC Interactions cellulaires tumorales et leur environnement et réponses
New Oral Anticoagulants Prevention and Treatment of DVT and PE Grigoris T Gerotziafas Groupe de Thrombose Equipe de recherche ER2UPMC Interactions cellulaires tumorales et leur environnement et réponses
Shared Care Protocol for the Prescription and Supply of Low Molecular Weight Heparins
 Tameside Hospital NHS Foundation Trust and NHS Tameside and Glossop Shared Care Protocol for the Prescription and Supply of Low Molecular Weight Heparins Version 5.2 Version: 5.2 Authorised by: Joint Medicines
Tameside Hospital NHS Foundation Trust and NHS Tameside and Glossop Shared Care Protocol for the Prescription and Supply of Low Molecular Weight Heparins Version 5.2 Version: 5.2 Authorised by: Joint Medicines
Drug Class Review Newer Oral Anticoagulant Drugs
 Drug Class Review Newer Oral Anticoagulant Drugs Final Original Report May 2016 The purpose of reports is to make available information regarding the comparative clinical effectiveness and harms of different
Drug Class Review Newer Oral Anticoagulant Drugs Final Original Report May 2016 The purpose of reports is to make available information regarding the comparative clinical effectiveness and harms of different
Choosing and Managing Direct Oral Anticoagulants (DOACs)
") Choosing and Managing Direct Oral Anticoagulants (DOACs) Ana G. Antun, MD, MSc Assistant Professor, Department of Hematology and Medical Oncology Winship Cancer Institute of Emory University 1 Outline
Choosing and Managing Direct Oral Anticoagulants (DOACs) Ana G. Antun, MD, MSc Assistant Professor, Department of Hematology and Medical Oncology Winship Cancer Institute of Emory University 1 Outline
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Blood Thinner Agent. Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy
 Blood Thinner Agent Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy Outline: Blood thinner agent definition. anticoagulants drugs. Thrombolytics. Blood thinner agent Therapeutic interference
Blood Thinner Agent Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy Outline: Blood thinner agent definition. anticoagulants drugs. Thrombolytics. Blood thinner agent Therapeutic interference
Venous Thromboembolism. Prevention
 Venous Thromboembolism Prevention August 2010 Venous Thromboembloism Prevention 1 1 Expected Practice Assess all patients upon admission to the ICU for risk factors of venous thromboembolism (VTE) and
Venous Thromboembolism Prevention August 2010 Venous Thromboembloism Prevention 1 1 Expected Practice Assess all patients upon admission to the ICU for risk factors of venous thromboembolism (VTE) and
Appendix IV - Prescribing Guidance for Apixaban
 Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015
 Clinical Practice Guideline August 2015") Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015 General Principles: There is compelling data in the medical literature to support
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015 General Principles: There is compelling data in the medical literature to support
Acute and long-term treatment of PE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
Reversal of Novel Oral Anticoagulants. Angelina The, MD March 22, 2016
 Reversal of Novel Oral Anticoagulants Angelina The, MD March 22, 2016 Argatroban Bivalirudin Enoxaparin Lepirudin Heparin Dabigatran Apixaban 1939 1954 1998 2000 1999 2001 10/2010 7/2011 12/2012 1/2015
Reversal of Novel Oral Anticoagulants Angelina The, MD March 22, 2016 Argatroban Bivalirudin Enoxaparin Lepirudin Heparin Dabigatran Apixaban 1939 1954 1998 2000 1999 2001 10/2010 7/2011 12/2012 1/2015
Acute Pulmonary Embolism and Deep Vein Thrombosis. Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center COPYRIGHT
 Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Perioperative Management of the Anticoagulated Patient
 Perioperative Management of the Anticoagulated Patient Citywide Resident Perioperative Medical Consultation Conference 5/5/17 Matthew Eisen, MD Director, Anticoagulation Services MetroHealth Medical Center
Perioperative Management of the Anticoagulated Patient Citywide Resident Perioperative Medical Consultation Conference 5/5/17 Matthew Eisen, MD Director, Anticoagulation Services MetroHealth Medical Center
3/19/2012. What is the indication for anticoagulation? Has the patient previously been on warfarin? If so, what % of the time was the INR therapeutic?
 Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
DVT - initial management NSCCG
 Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Venous Thromboembolism Prophylaxis - Why Should We Care? Harry Gibbs FRACP FCSANZ Vascular Physician The Alfred Hospital
 Venous Thromboembolism Prophylaxis - Why Should We Care? Harry Gibbs FRACP FCSANZ Vascular Physician The Alfred Hospital VTE is common and dangerous 5 VTE is Common VTE Incidence: 1.5 / 1000 per year
Venous Thromboembolism Prophylaxis - Why Should We Care? Harry Gibbs FRACP FCSANZ Vascular Physician The Alfred Hospital VTE is common and dangerous 5 VTE is Common VTE Incidence: 1.5 / 1000 per year
CANCER ASSOCIATED THROMBOSIS. Pankaj Handa Department of General Medicine Tan Tock Seng Hospital
 CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
Cancer and Thrombosis
 Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
Clinical Policy: Dalteparin (Fragmin) Reference Number: ERX.SPA.207 Effective Date:
 Reference Number: ERX.SPA.207 Effective Date:") Clinical Policy: (Fragmin) Reference Number: ERX.SPA.207 Effective Date: 01.11.17 Last Review Date: 02.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Fragmin) Reference Number: ERX.SPA.207 Effective Date: 01.11.17 Last Review Date: 02.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders
 SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is
SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban
 Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement. Marilyn Szekendi, PhD, RN
 Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement Marilyn Szekendi, PhD, RN ANA 7 th Annual Nursing Quality Conference, February 2013 Research Team Banafsheh Sadeghi,
Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement Marilyn Szekendi, PhD, RN ANA 7 th Annual Nursing Quality Conference, February 2013 Research Team Banafsheh Sadeghi,