HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long. Case Study 2
|
|
|
- Tracey Patrick
- 5 years ago
- Views:
Transcription
1 HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2
2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS
3 CLINICAL CASE MEDICAL HISTORY 59-year-old man Hypertension and hyperlipidemia (for 10 years) Obesity (BMI 30.1 kg/m²) Current smoking Anterior NSTEMI (2 years ago) Stable angina (CCS II) Paroxysmal AF (CHA 2 DS 2 VASc 3; HAS-BLED 1) Heart failure, recent LVEF 54% (last 6 months) Treatment before the admission: Nitroglycerin, Bisoprolol, Isosorbide dinitrate, Aspirin, Atorvastatin, Perindopril, Rivaroxaban.
4 CLINICAL CASE STATUS ON ADMISSION Symptoms: worsening of dyspnea for 1 week (NYHA III) irregular palpitations fatigue reduced exercise tolerance typical angina (CCS II) Clinical status: BP 165/95 mmhg, HR 120 bpm (Paroxysmal AF, last 12 hours) pulmonary congestion (confirmed on chest X-ray) ankle swelling weight gain Laboratory tests: Hb 14.2 g/dl egfr 68 ml/min/1.73m 2 NT-proBNP 1190 pg/ml ctnt 0.01 ng/ml LDL 2.0 mmol/l
5 CLINICAL CASE APPLIED TREATMENT Acute management: admitted to a coronary care unit i.v. amiodarone i.v. furosemide i.v. nitroglycerine Clinical status: conversion AF to sinus rhythm BP 136/90 mmhg, HR 69 bpm significant reduction in dyspnea significant reduction in pulmonary congestion
 program; 99,825 HF admissions from 305 hospitals between January 2005 and September 2013 Kapoor JR, et al.")
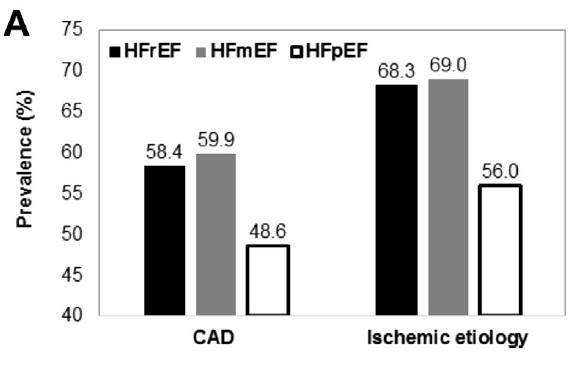
6 PRECIPITATING FACTORS FOR HEART FAILURE ADMISSION IN PATIENTS WITH HFREF, HFMREF AND HFPEF Database of the Get With The Guidelines-HF (GWTG-HF) program; 99,825 HF admissions from 305 hospitals between January 2005 and September 2013 Kapoor JR, et al. J Am Coll Cardiol HF 2016;4:464 72

7 PREVALENCE OF HEART FAILURE CHARACTERISTICS IN PATIENTS WITH HFREF, HFMREF AND HFPEF Database of the Get With The Guidelines-HF (GWTG-HF) program; 99,825 HF admissions from 305 hospitals between January 2005 and September 2013 Kapoor JR, et al. J Am Coll Cardiol HF 2016;4:464 72






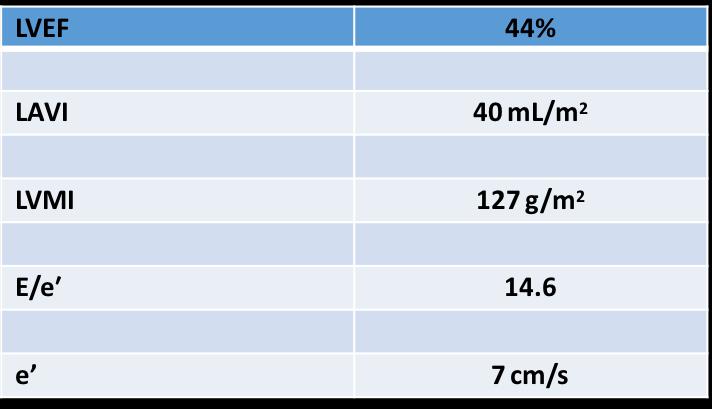
8 CLINICAL CASE ECHOCARDIOGRAPHY Key structural and functional alterations (2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure)
:2129-200.")
9 ESC HF GL 2016: DEFINITION OF HEART FAILURE WITH PRESERVED (HFPEF), MID-RANGE (HFMREF) AND REDUCED EJECTION FRACTION (HFREF) ESC 2016: Signs and symptoms of HF are often non-specific and do not discriminate well between HF and other clinical conditions Ponikowski et al., Eur Heart J Jul 14;37(27):

 With Preserved Ejection Fraction (pg/ml) NT-proBNP or BNP Sinus rhythm 300")
10 DIFFERENT THRESHOLDS OF NT-PROBNP FOR THE DIAGNOSIS OF HFPEF IN THE PRESENCE OF AF VS. THE ABSENCE OF AF Eur J Heart Fail 2014: 16, A Multicenter, Randomized, Double-blind, Parallel Group, Active- controlled Study to Evaluate the Efficacy and Safety of LCZ696 Compared to Valsartan, on Morbidity and Mortality in Heart Failure Patients (NYHA Class II-IV) With Preserved Ejection Fraction (pg/ml) NT-proBNP or BNP Sinus rhythm AF NT-proBNP (pg/ml) >900

 in the mid of")


11 CLINICAL CASE CORONARY ANGIOGRAPHY, PCI Single-vessel disease with a stenosis (70%) in the mid of the left anterior descending coronary artery PCI and DES implantation Standard periprocedural therapy, then triple therapy (1 month)



12 J Am Coll Cardiol 2014; 63: HFpEF patients with angiographically-proven CAD NYHA functional class III 56% Angina 36% CCS II 34%
13 CLINICAL CASE OUTPATIENT FOLLOW-UP Outpatient visit 3 months post discharge Clinical status: dyspnea and fatigue during ordinary physical activity (NYHA II), no angina LVEF 52% BP 130/85 mmhg, HR 64 bpm no hospitalization in the past 3 months Current treatment: Amiodarone, Clopidogrel, Rivaroxaban, Atorvastatin, Perindopril, Spironolactone
14 TRANSITIONS BETWEEN LVEFS IN PATIENTS WITH HEART FAILURE HFrEF LVEF<40%) HFmrEF (LVEF 40-49%) HFpEF LVEF 50%)


15 % 30 Estimated Transition Probability Matrices at Several Points of Follow- Up for the Primary Model HFpEF to HFrEF HFrEF to HFpEF Circ Cardiovasc Qual Outcomes. 2013;6:
16 CONCLUSIONS Many demographic and clinical characteristics of HFmrEF are intermediate between HFrEF and HFpEF. The potential dynamism of HFmrEF raises the question of the better understanding of the role of precipitating factors and comorbidities, as well as of the correct time to categorize the LV systolic function. Large prospective randomized clinical trials on the middle child of HF are needed.

, iv.")
 or LA >34 ml/m 2 ) or diastolic")
 Questions: 1. What is the correct definition of LVEF?")
17 WE VE COME A LONG WAY Four elements of HFmrEF: i. Symptoms with or without signs of HF ii. LVEF of 40-49%. iii. elevated natriuretic peptides (BNP 35pg/mL or NT-proBNP 125pg/mL), iv. Relevant structural heart disease: LVMI 115 g/m 2 for males and 95 g/m 2 for females) or LA >34 ml/m 2 ) or diastolic dysfunction (E/e 13 and a mean e septal and lateral wall <9 cm/s) Questions: 1. What is the correct definition of LVEF? 2. What adds to LVEF? 3. The value of exercise testing
18 WHY A NEW CATEGORY HFMREF 40-49%? HF is now becoming a preventable and treatable disease Most clinical trials since 1990 selected patients on the basis of LVEF but no convincing data at EF 40% Identifying HFmREF as a separate group will stimulate research into underlying characteristics, pathophysiology, and treatment of this population. Ponikowski et al., Eur Heart J. 016 Jul 14;37(27):19-00.
19

20 HIGH PREVALENCE OF HFMREF IN CONTEMPORARY EUROPE
21 SURVIVAL COMPARABLY POOR IN HFMREF VS. HFREF

22 CAUSES OF DEATH IN HFMREF VS. HFREF, HFPEF
23 HFMREF MANAGEMENT WHAT DO THE GUIDELINES SAY? 1. Make a firm Diagnosis 2. Classify the patient Etiology and Comorbidities 3. General principles of management 4. Specific therapeutic approaches
 Clinical History Physical examination")

24 DIAGNOSTIC ALGORITHM FOR HF OF NON-ACUTE ONSET 1) Assess likelihood that HF like symptoms are of cardiac origin (heart failure) Clinical History Physical examination ECG 2) Consider other disease/comorbidities CAD COPD Obesity Sarcopenia Anemia 3) Measure BNP or NTproBNP Echocardiography Ponikowski et al., Eur Heart J Jul 14;37(27):
25 ESC 2016 KEY DIAGNOSTIC HFMREF CRITERIA LVEF: % Structural alterations: Functional alterations: LAVI >34 ml/m2or LVMI 115 (males) / 95 (females) mg/m2 E/é 13 é (mean septal and lateral) <9 cm/s NTproBNP: BNP: >125 pg/ml or (SR; increase with Afib!) >35 pg/ml
26 CAN YOU MAKE A HFMREF DIAGNOSIS IN OUR PATIENT? Which ONE option would you choose first? A. Yes because he has typical HF signs/symptoms B. Yes because his E/é is 14.6 C. Yes because his NTproBNP was 600 after conversion to SR D. Yes because EF was 44% E. All of the above
27 CAN YOU MAKE A HFMREF DIAGNOSIS IN OUR PATIENT? Which ONE option would you choose first? A. Yes because he has typical HF signs/symptoms B. Yes because his E/é is 14.6 C. Yes because his NTproBNP was 600 after conversion to SR D. Yes because EF was 44% E. All of the above
28 HFpEF Management What do the Guidelines Say? 1. Make a firm Diagnosis 2. Classify the patient Etiology and Comorbidities 3. General principles of management 4. Specific therapeutic approaches
29 ESC 2016: HFmrEF workup Screen cardiovascular comorbidities Arterial hypertension, AFib, pulmonary hypertension. Screen non-cardiovascular comorbidities - Diabetes, CKD, iron deficiency, anemia, COPD, obesity. Identify underlying aetiology

30
31 HFMREF MANAGEMENT WHAT DO THE GUIDELINES SAY? 1. Make a firm Diagnosis 2. Classify the patient Etiology and Comorbidities 3. General principles of management 4. Specific therapeutic approaches
32 ESC 2016: GENERAL PRINCIPLES OF MANAGEMENT Treat underlying etiology! Ischemia, myocarditis.. Treat cardiovascular comorbidities Arterial hypertension, diabetes, pulmonary hypertension. Treat non-cardiovascular comorbidities - CKD, iron deficiency, COPD, obesity. Diuretics for symptom relieve
:2129-200.")
33 ESC 2016: RECOMMENDATIONS FOR HFMREF Ponikowski et al., Eur Heart J Jul 14;37(27):
34 WEIGHT LOSS AND EXERCISE TRAINING
35 EX-DHF PILOT: EXERCISE TRAINING IN ELDERLY HFMREF/HFPEF Primary Endpoint: peak VO2 Maximum Workload Edelmann et al., JACC 2011;58:
36 ESC 2016: RECOMMENDATIONS FOR EXERCISE TRAINING Combined endurance/resistance training for patients with HFmrEF appears safe improves exercise capacity, physical functioning score, and diastolic function
37 ESC 2016: HOW TO OPTIMIZE MANAGEMENT 1. Make a firm Diagnosis 2. Classify the patient Etiology and Comorbidities 3. General principles of management 4. Specific therapeutic approaches
38 ESC 2016: SPECIFIC HFMREF THERAPIES? No treatment has been shown, convincingly, to reduce morbiditiy and mortality in patients with HFpEF or HFmrEF Patients with HFmrEF have generally been included in trials of HFpEF.





39 OUTCOME TRIALS IN HFMREF - HFPEF CHARM-Preserved 1 PEP-CHF 2 EF >40% EF 40% I-PRESERVE 3 TOPCAT EF >45% EF >45% Yusuf et al., Lancet 2003; 362: Massie et al., N Engl J Med 2008; 359: Cleland et al., Eur Heart J 2006; 27:
40 ESC 2016: SPECIFIC HFMREF THERAPIES? Compared with HFrEF, only slightly fewer patients with HFmrEF appear to receive diuretics, betablockers, MRAs, ACEI, and ARBs. This may reflect comorbidities, CAD, or Afib, or extrapolation of results from trials in these conditions...or a belief that existing clinical trials provide some evidence of benefit with these agents

41 REGISTRY DATA: THERAPIES SIMILAR IN HFREF AND HFMREF
42 ESC 2016: SPECIFIC HFMREF THERAPIES? Compared with HFrEF, only slightly fewer patients with HFmrEF appear to receive diuretics, betablockers, MRAs, ACEI, and ARBs. This may reflect comorbidities, CAD, or Afib, or extrapolation of results from trials in these conditions...or a belief that existing clinical trials provide some evidence of benefit with these agents

43 SPECIFIC ETIOLOGIES: ACE INHIBITORS AFTER MYOCARDIAL INFARCTION

44 ESC 2016: ASYMPTOMATIC LVSD AFTER MI ACEI BB Ponikowski P et al., EHJ 2016
45 ESC 2016: SPECIFIC HFMREF THERAPIES? Compared with HFrEF, only slightly fewer patients with HFmrEF appear to receive diuretics, beta-blockers, MRAs, ACEI, and ARBs. This may reflect comorbidities, CAD, or Afib, or extrapolation of results from trials in these conditions...or a belief that existing clinical trials provide some evidence of benefit with these agents
46 RAAS INHIBITION IN HFMREF/HFPEF Meta-analysis: Renin-Angiotensin-Aldosterone Inhibitor Trials in HFmrEF/HFpEF TOPCAT CHARM-Preserved I-PRESERVE PEP-CHF OR (95% CI) % Weight Primary Event 0.89 (0.75, 1.06) (0.74, 1.04) (0.84, 1.08) (0.67, 1.26) 7.15 Overall 0.92 (0.84, 1.00) P = Primary Event P = CV Death or HHF Courtesy of S. Solomon, Boston

47 Spironolactone (N = 1722) Placebo (N = 1723) HR (95% CI) Hospitalization for Heart Failure 206 (12.0%) 3.8/100pt-yr 245 (14.2%) 4.6/100pt-yr 0.83 ( ) P=0.042 Multiple HF Hosp P<0.01 Conclusions: TOPCAT population with HFpEF Rx with spironolactone did not alter the 1 composite Reductions in heart failure were observed Use of spironolactone in these patients requires careful monitoring of K + and creatinine
48 HFMREF - WHAT DO THE GUIDELINES SAY? Make a firm diagnosis Establish underlying etiology, comorbidities, and current status on HF trajectory Apply established therapeutic measures for underlying causes and comorbidities Many of these patients will need Diuretics, ACE- Inhibitors/ARBs, BB, MR-Antagonists
49 OUR PATIENT HFMREF: WHAT DO THE GUIDELINES SAY? Recovered HFmrEF therapy: ACE Inhibitor (Perindopril) Spironolactone 25 mg o.d mg, check K+, Crea, BP) No BB since on Amiodarone No diuretics because patient recovered (EF 52%) & euvolemic Comorbidities: Oral anticoagulation for s.p. Afib (Rivaroxaban) Antiplatelet therapy for 6-12 months after DES Risk factor control: Statin (Atorvastatin) Lifestyle interventions (Exercise program if possible at all) Weight loss & smoking cessation

50 Main purpose: to stimulate research into the underlying characteristics, pathophysiology and treatment of this group of patients. Moreover, recent data from TOPCAT2 and CHARM-Preserved3 have shown that patients with HFmrEF behave similarly to those with HFrEF, in terms of both prognosis and response to therapy. Nevertheless, we should resist the temptation to fuss over names or become overly rigid in our partitioning. After all, all of the heart failure children are part of the same family.
51 TAKE HOME MESSAGES: GAPS IN EVIDENCE Difficult to define accurately EF More trials needed with strict cut off values Imaging modalities will have a positive value We should resist the temptation to fuss over names or become overly rigid in our partitioning. After all, all of the heart failure children are part of the same family. CSP Lam & SC Solomon, Circulation 4 th April 017
52 THANK YOU
HFpEF: How to optimise management
 HFpEF: How to optimise management Burkert Pieske M.D. Berlin, Germany Department of Internal Medicine and Cardiology, Campus Virchow Klinikum, Charité University Medicine Berlin, and Department of Internal
HFpEF: How to optimise management Burkert Pieske M.D. Berlin, Germany Department of Internal Medicine and Cardiology, Campus Virchow Klinikum, Charité University Medicine Berlin, and Department of Internal
Heart Failure with preserved ejection fraction (HFpEF)
") Heart Failure with preserved ejection fraction (HFpEF) Dr. Pierpaolo Pellicori Hull York Medical School Kingston-upon-Hull United Kingdom Conflict of interest: none Heart failure is a contemporary problem
Heart Failure with preserved ejection fraction (HFpEF) Dr. Pierpaolo Pellicori Hull York Medical School Kingston-upon-Hull United Kingdom Conflict of interest: none Heart failure is a contemporary problem
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
HFpEF, Mito or Realidad?
 HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016
 SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
HFpEF 2016 : Comorbidities and Outcomes
 HFpEF 2016 : Comorbidities and Outcomes Christopher M. O Connor, MD, FACC CEO and Executive Director, Inova Heart and Vascular Institute Professor of Medicine, Duke University Editor in Chief, JACC: Heart
HFpEF 2016 : Comorbidities and Outcomes Christopher M. O Connor, MD, FACC CEO and Executive Director, Inova Heart and Vascular Institute Professor of Medicine, Duke University Editor in Chief, JACC: Heart
Drugs acting on the reninangiotensin-aldosterone
 Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
The Approach to Patients with Heart Failure and Mid-Range (40-50%) Ejection Fraction (HFmrEF)
 Ejection Fraction (HFmrEF)") The Approach to Patients with Heart Failure and Mid-Range (40-50%) Ejection Fraction (HFmrEF) 22 nd Annual Heart Failure 2018 an Update on Therapy April 21, 2018 Los Angeles, CA Barry Greenberg, M.D. Distinguished
The Approach to Patients with Heart Failure and Mid-Range (40-50%) Ejection Fraction (HFmrEF) 22 nd Annual Heart Failure 2018 an Update on Therapy April 21, 2018 Los Angeles, CA Barry Greenberg, M.D. Distinguished
2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland
 2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland Disclosures Consultancy fees and speaker s honoraria from: Amgen, Servier, Novartis, Johnson & Johnson, Merck, Berlin Chemie,
2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland Disclosures Consultancy fees and speaker s honoraria from: Amgen, Servier, Novartis, Johnson & Johnson, Merck, Berlin Chemie,
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Heart Failure Update. Bibiana Cujec MD May 2015
 Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
The NEW Heart Failure Guidelines
 The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
HF-Preserved Ejection Fraction
 HF-Preserved Ejection Fraction Justin A. Ezekowitz, MBBCh MSc FRCPC FACC FESC FAHA Associate Professor, University of Alberta Co-Director, Canadian VIGOUR Centre Cardiologist, Mazankowski Alberta Heart
HF-Preserved Ejection Fraction Justin A. Ezekowitz, MBBCh MSc FRCPC FACC FESC FAHA Associate Professor, University of Alberta Co-Director, Canadian VIGOUR Centre Cardiologist, Mazankowski Alberta Heart
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Heart Failure A Disease for the Internist?
 Heart Failure A Disease for the Internist? Dr Chris Davidson Sussex Cardiac Centre BRIGHTON UK Hot Topics in Heart Failure Drug treatments Valsartan / neprilysin inhib Investigations BNP and others Devices
Heart Failure A Disease for the Internist? Dr Chris Davidson Sussex Cardiac Centre BRIGHTON UK Hot Topics in Heart Failure Drug treatments Valsartan / neprilysin inhib Investigations BNP and others Devices
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure
 ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
8:30-10:30 WS #4: Cardiology :00-13:00 WS #11: Cardiology 101 (Repeated)
") Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA
 Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Heart Failure with Preserved EF (HFPEF) Epidemiology and management
 Epidemiology and management") Heart Failure with Preserved EF (HFPEF) Epidemiology and management Karl Swedberg Senior Professor of Medicine Sahlgrenska Academy University of Gothenburg Gothenburg, Sweden e-mail: karl.swedberg@gu.se
Heart Failure with Preserved EF (HFPEF) Epidemiology and management Karl Swedberg Senior Professor of Medicine Sahlgrenska Academy University of Gothenburg Gothenburg, Sweden e-mail: karl.swedberg@gu.se
Diagnosis is it really Heart Failure?
 ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University
ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University
Heart Failure: Current Management Strategies
 Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
The Hearth Rate modulators. How to optimise treatment
 The Hearth Rate modulators How to optimise treatment Munich, ESC Congress 2012 Prof. Luigi Tavazzi GVM Care&Research E.S. Health Science Foundation Cotignola, IT Disclosure Cooperation with: Servier, Medtronic,
The Hearth Rate modulators How to optimise treatment Munich, ESC Congress 2012 Prof. Luigi Tavazzi GVM Care&Research E.S. Health Science Foundation Cotignola, IT Disclosure Cooperation with: Servier, Medtronic,
ACE inhibitors: still the gold standard?
 ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
Objectives. Systolic Heart Failure: Definitions. Heart Failure: Historical Perspective 2/7/2009
 Objectives Diastolic Heart Failure and Indications for Echocardiography in the Asian Population Damon M. Kwan, MD UCSF Asian Heart & Vascular Symposium 02.07.09 Define diastolic heart failure and differentiate
Objectives Diastolic Heart Failure and Indications for Echocardiography in the Asian Population Damon M. Kwan, MD UCSF Asian Heart & Vascular Symposium 02.07.09 Define diastolic heart failure and differentiate
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
Outline. Classification by LVEF Conventional Therapy New Therapies. Ivabradine Sacubitril/valsartan
 New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
Heart Failure in Women
 Heart Failure in Women Disclosure Professor Sindone has received honoraria, speaker fees, consultancy fees, is a member of advisory boards or has appeared on expert panels for: Professor Andrew Sindone
Heart Failure in Women Disclosure Professor Sindone has received honoraria, speaker fees, consultancy fees, is a member of advisory boards or has appeared on expert panels for: Professor Andrew Sindone
A patient with decompensated HF
 A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
Ejection Fraction in Patients With Chronic Heart Failure. Diastolic Heart Failure or Heart Failure with Preserved Ejection Fraction
 Diastolic Heart Failure or Heart Failure with Preserved Ejection Fraction Keith Miller MD Diastolic Heart Failure Risk Factors Common Risk Factors Aging Female gender Obesity Hypertension Diabetes mellitus
Diastolic Heart Failure or Heart Failure with Preserved Ejection Fraction Keith Miller MD Diastolic Heart Failure Risk Factors Common Risk Factors Aging Female gender Obesity Hypertension Diabetes mellitus
Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study
 Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study Dr. Antonio Magaña M.D. (on behalf I-PREFER investigators group) Stockholm, Sweden, August
Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study Dr. Antonio Magaña M.D. (on behalf I-PREFER investigators group) Stockholm, Sweden, August
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό
 Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
2/15/2017. Disclosures. Heart Failure = Big Problem. Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017
 Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017 Julio A. Barcena, M.D. South Miami Heart Specialists Disclosures I have no relevant commercial relationships to
Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017 Julio A. Barcena, M.D. South Miami Heart Specialists Disclosures I have no relevant commercial relationships to
The new Guidelines: Focus on Chronic Heart Failure
 The new Guidelines: Focus on Chronic Heart Failure Petros Nihoyannopoulos MD, FRCP, FESC Professor of Cardiology Imperial College London and National & Kapodistrian University of Athens 2 3 4 The principal
The new Guidelines: Focus on Chronic Heart Failure Petros Nihoyannopoulos MD, FRCP, FESC Professor of Cardiology Imperial College London and National & Kapodistrian University of Athens 2 3 4 The principal
Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham
 Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Chronic heart failure
Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Chronic heart failure
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0.
 New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
Management of atrial fibrillation in heart failure
 Nationale hartfalendag 2017 Zeist Management of atrial fibrillation in heart failure Isabelle C Van Gelder University of Groningen University Medical Center Groningen The Netherlands Disclosures Grant
Nationale hartfalendag 2017 Zeist Management of atrial fibrillation in heart failure Isabelle C Van Gelder University of Groningen University Medical Center Groningen The Netherlands Disclosures Grant
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Is there a mortality risk associated with aspirin use in heart failure? Results from a large community based cohort Margaret Bermingham, Mary-Kate Shanahan, Saki Miwa,
DECLARATION OF CONFLICT OF INTEREST Is there a mortality risk associated with aspirin use in heart failure? Results from a large community based cohort Margaret Bermingham, Mary-Kate Shanahan, Saki Miwa,
ST2 in Heart Failure. ST2 as a Cardiovascular Biomarker. Competitive Model of ST2/IL-33 Signaling. ST2 and IL-33: Cardioprotective
 ST2 as a Cardiovascular Biomarker Lori B. Daniels, MD, MAS, FACC Professor of Medicine Director, Coronary Care Unit University of California, San Diego ST2 and IL-33: Cardioprotective ST2: member of the
ST2 as a Cardiovascular Biomarker Lori B. Daniels, MD, MAS, FACC Professor of Medicine Director, Coronary Care Unit University of California, San Diego ST2 and IL-33: Cardioprotective ST2: member of the
Optimal blockade of the Renin- Angiotensin-Aldosterone. in chronic heart failure
 Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Performance and Quality Measures 1. NQF Measure Number. Coronary Artery Disease Measure Set
 Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Heart Failure Management. Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist
 Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
HFpEF: Pathophysiology & Treatment
 HFpEF: Pathophysiology & Treatment Barry A. Borlaug, MD Mayo Clinic, Rochester, MN borlaug.barry@mayo.edu Disclosure Financial Relationships Research Support: Aires Pharmaceuticals, Medtronic, GSK Consulting/Advisory
HFpEF: Pathophysiology & Treatment Barry A. Borlaug, MD Mayo Clinic, Rochester, MN borlaug.barry@mayo.edu Disclosure Financial Relationships Research Support: Aires Pharmaceuticals, Medtronic, GSK Consulting/Advisory
New in Heart Failure SGK autumn session 2012
 New in Heart Failure SGK autumn session 2012 Roger Hullin Cardiology Department of Internal Medicine Centre Universitaire Hospitaler Vaudois University of Lausanne ESC Heart Failure Guidelines 2012 Classes
New in Heart Failure SGK autumn session 2012 Roger Hullin Cardiology Department of Internal Medicine Centre Universitaire Hospitaler Vaudois University of Lausanne ESC Heart Failure Guidelines 2012 Classes
DIASTOLIC HEART FAILURE
 DIASTOLIC HEART FAILURE M Mohsen Ibrahim, MD Alexandria, Proposed Criteria for Diastolic Heart Failure ESC Working Group (EHJ 1998) CHF signs/symptoms EF 45% Hemodynamic or echo evidence of diastolic dysfunction
DIASTOLIC HEART FAILURE M Mohsen Ibrahim, MD Alexandria, Proposed Criteria for Diastolic Heart Failure ESC Working Group (EHJ 1998) CHF signs/symptoms EF 45% Hemodynamic or echo evidence of diastolic dysfunction
UPDATES IN MANAGEMENT OF HF
 UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
Sleep Disordered Breathing and HH with Preserved Ejection Fraction:
 Sleep Disordered Breathing and HH with Preserved Ejection Fraction: Pr Thibaud DAMY Heart Failure Unit Department of Cardiology CHU Mondor, Créteil, France Definition of HF-PEF The diagnosis of HF-PEF
Sleep Disordered Breathing and HH with Preserved Ejection Fraction: Pr Thibaud DAMY Heart Failure Unit Department of Cardiology CHU Mondor, Créteil, France Definition of HF-PEF The diagnosis of HF-PEF
What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE. Marc Ferrini (Lyon Fr)
") What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE Marc Ferrini (Lyon Fr) Palermo (I) 1 04 2017 Consulting Fees, Honoraria: BAYER PHARMA BOEHRINGER INGELHEIM BRISTOL MEYERS
What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE Marc Ferrini (Lyon Fr) Palermo (I) 1 04 2017 Consulting Fees, Honoraria: BAYER PHARMA BOEHRINGER INGELHEIM BRISTOL MEYERS
Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2014 Update on Randomized Trials
 AHA Nov 18, 2014 Update on Randomized Trials") Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2014 Update on Randomized Trials Marc A. Pfeffer, MD, PhD; Brian Claggett, PhD; Susan F. Assmann,
Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2014 Update on Randomized Trials Marc A. Pfeffer, MD, PhD; Brian Claggett, PhD; Susan F. Assmann,
Heart failure in diabetes: consequences for diagnosis and therapy
 Heart failure in diabetes: consequences for diagnosis and therapy Arno W. Hoes, MD, PhD (no potential conflict of interest regarding this presentation) Hartfalen werkgroep, Amersfoort, Maart 2017 Pathophysiology:
Heart failure in diabetes: consequences for diagnosis and therapy Arno W. Hoes, MD, PhD (no potential conflict of interest regarding this presentation) Hartfalen werkgroep, Amersfoort, Maart 2017 Pathophysiology:
ESC Guidelines for diagnosis and management of HF 2012: What s new? John Parissis, MD Athens, GR
 ESC Guidelines for diagnosis and management of HF 2012: What s new? John Parissis, MD Athens, GR Disclosures ALARM INVESTIGATOR RESEARCH GRANTS BY ABBOTT USA AND ORION PHARMA The principal changes from
ESC Guidelines for diagnosis and management of HF 2012: What s new? John Parissis, MD Athens, GR Disclosures ALARM INVESTIGATOR RESEARCH GRANTS BY ABBOTT USA AND ORION PHARMA The principal changes from
Update on pharmacological treatment of heart failure. Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy
 Update on pharmacological treatment of heart failure Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Presenter Disclosures Dr. Maggioni : Serving in Committees of studies sponsored
Update on pharmacological treatment of heart failure Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Presenter Disclosures Dr. Maggioni : Serving in Committees of studies sponsored
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Systolic and Diastolic Dysfunction: Four Upcoming Challenges
 Systolic and Diastolic Dysfunction: Four Upcoming Challenges Promoting Early Detection HFrEF: Beyond Neprilysin/Enalapril HFmrEF: What Is It and How Does One Manage It? HFpEF: Etiopathogenetic Role and
Systolic and Diastolic Dysfunction: Four Upcoming Challenges Promoting Early Detection HFrEF: Beyond Neprilysin/Enalapril HFmrEF: What Is It and How Does One Manage It? HFpEF: Etiopathogenetic Role and
THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION
 THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine Disclosures Data
THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine Disclosures Data
Heart Failure. GP Update Refresher 18 th January 2018
 GP Update Refresher 18 th January 2018 Heart Failure Dr. Alexander Lyon Senior Lecturer and Consultant Cardiologist Clinical Lead in Cardio-Oncology Royal Brompton Hospital, London UK President of British
GP Update Refresher 18 th January 2018 Heart Failure Dr. Alexander Lyon Senior Lecturer and Consultant Cardiologist Clinical Lead in Cardio-Oncology Royal Brompton Hospital, London UK President of British
Heart Failure in Women: Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre
 Heart Failure in Women: More than EF? Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre Overview Review pathophysiology as it relates to diagnosis and management Rational approach to workup:
Heart Failure in Women: More than EF? Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre Overview Review pathophysiology as it relates to diagnosis and management Rational approach to workup:
Mihai Gheorghiade MD
 Mihai Gheorghiade MD Center for Cardiovascular Innovation, Northwestern University Feinberg School of Medicine, Chicago, Illinois On behalf of: Stephen J Greene MD; Javed Butler MD MPH MBA; Gerasimos Filippatos
Mihai Gheorghiade MD Center for Cardiovascular Innovation, Northwestern University Feinberg School of Medicine, Chicago, Illinois On behalf of: Stephen J Greene MD; Javed Butler MD MPH MBA; Gerasimos Filippatos
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing
 Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Heart Failure Guidelines For your Daily Practice
 Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
Online Appendix (JACC )
") Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
Pravin Manga Division of Cardiology Department of Medicine University of Witwatersrand
 Pravin Manga Division of Cardiology Department of Medicine University of Witwatersrand Overview Definition Epidemiology Biomarkers Treatment Clinical Heart Failure: Syndrome in which patients have typical
Pravin Manga Division of Cardiology Department of Medicine University of Witwatersrand Overview Definition Epidemiology Biomarkers Treatment Clinical Heart Failure: Syndrome in which patients have typical
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
12 th Annual Biomarkers in Heart Failure and Acute Coronary Syndromes: Diagnosis, Treatment and Devices. Heart Rate as a Cardiovascular Biomarker
 12 th Annual Biomarkers in Heart Failure and Acute Coronary Syndromes: Diagnosis, Treatment and Devices Heart Rate as a Cardiovascular Biomarker Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine,
12 th Annual Biomarkers in Heart Failure and Acute Coronary Syndromes: Diagnosis, Treatment and Devices Heart Rate as a Cardiovascular Biomarker Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine,
Vitals HR 90 BP 125/58 Tmax 98.7F O2 Sat 97% on NC 2L/min BMP SCr 1.78 K 3.9 Gluc 194 A1c 7.5 Cardiac LVEF 55% NTproBNP 9,200 Troponin 0.
 ALDOSTERONE ANTAGONIST IN HEART FAILURE WITH PRESERVED EJECTION FRACTION ABBREVIATIONS BMP: basic metabolic panel HPI: history of present illness CAD: coronary artery disease HR: heart rate PINHUI (JUDY)
ALDOSTERONE ANTAGONIST IN HEART FAILURE WITH PRESERVED EJECTION FRACTION ABBREVIATIONS BMP: basic metabolic panel HPI: history of present illness CAD: coronary artery disease HR: heart rate PINHUI (JUDY)
The right heart: the Cinderella of heart failure
 The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
Combination of renin-angiotensinaldosterone. how to choose?
 Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Overview & Update on the Utilization of the Natriuretic Peptides in Heart Failure
 June 28, 2016 Overview & Update on the Utilization of the Natriuretic Peptides in Heart Failure Linda C. Rogers, PhD, DABCC, FACB. Agenda Overview of the Natriuretic Peptides and Efficacy studies Similarities
June 28, 2016 Overview & Update on the Utilization of the Natriuretic Peptides in Heart Failure Linda C. Rogers, PhD, DABCC, FACB. Agenda Overview of the Natriuretic Peptides and Efficacy studies Similarities
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC
 2016: ACC / AHA and ESC") Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
Heart Failure 101 The Basic Principles of Diagnosis & Management
 Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Faiez Zannad. Institut Lorrain du Coeur et des Vaisseaux. CIC - Inserm
 Faiez Zannad Institut Lorrain du Coeur et des Vaisseaux CIC - Inserm Disclosure Faiez Zannad Grants BG Medicine, Roche Diagnostics. Consultant/Steering committees/event committees/ Data safety Monitoring
Faiez Zannad Institut Lorrain du Coeur et des Vaisseaux CIC - Inserm Disclosure Faiez Zannad Grants BG Medicine, Roche Diagnostics. Consultant/Steering committees/event committees/ Data safety Monitoring
Heart Failure. Guillaume Jondeau Hôpital Bichat, Paris, France
 Heart Failure Guillaume Jondeau Hôpital Bichat, Paris, France Epidemiology Importance of PEF Europe I-PREFER study. Abstract: 2835 Prevalence of HF Preserved LV systolic Function older (65 vs 62 y, p
Heart Failure Guillaume Jondeau Hôpital Bichat, Paris, France Epidemiology Importance of PEF Europe I-PREFER study. Abstract: 2835 Prevalence of HF Preserved LV systolic Function older (65 vs 62 y, p
RAS Blockade Across the CV Continuum
 A Summary of Recent International Meetings RAS Blockade Across the CV Continuum Copyright New Evidence Presented at the 2009 Congress of the European Society of Cardiology (August 29-September 2, Barcelona)
A Summary of Recent International Meetings RAS Blockade Across the CV Continuum Copyright New Evidence Presented at the 2009 Congress of the European Society of Cardiology (August 29-September 2, Barcelona)
NCAP NATIONAL CARDIAC AUDIT PROGR AMME NATIONAL HEART FAILURE AUDIT 2016/17 SUMMARY REPORT
 NCAP NATIONAL CARDIAC AUDIT PROGR AMME NATIONAL HEART FAILURE AUDIT 2016/17 SUMMARY REPORT CONTENTS PATIENTS ADMITTED WITH HEART FAILURE...4 Demographics... 4 Trends in Symptoms... 4 Causes and Comorbidities
NCAP NATIONAL CARDIAC AUDIT PROGR AMME NATIONAL HEART FAILURE AUDIT 2016/17 SUMMARY REPORT CONTENTS PATIENTS ADMITTED WITH HEART FAILURE...4 Demographics... 4 Trends in Symptoms... 4 Causes and Comorbidities
NT-proBNP: Evidence-based application in primary care
 NT-proBNP: Evidence-based application in primary care Associate Professor Rob Doughty The University of Auckland, Auckland City Hospital, Auckland Heart Group NT-proBNP: Evidence in Primary Care The problem
NT-proBNP: Evidence-based application in primary care Associate Professor Rob Doughty The University of Auckland, Auckland City Hospital, Auckland Heart Group NT-proBNP: Evidence in Primary Care The problem
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Cardiovascular Pharmacotherapy
 Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists
 I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists Alessandro Fucili (Ferrara, IT) Massimo F Piepoli (Piacenza, IT) Clinical Case: 82 year old woman
I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists Alessandro Fucili (Ferrara, IT) Massimo F Piepoli (Piacenza, IT) Clinical Case: 82 year old woman
New evidences in heart failure: the GISSI-HF trial. Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy
 New evidences in heart failure: the GISSI-HF trial Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy % Improving survival in chronic HF and LV systolic dysfunction: 1 year all-cause mortality 20
New evidences in heart failure: the GISSI-HF trial Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy % Improving survival in chronic HF and LV systolic dysfunction: 1 year all-cause mortality 20
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Heart Failure Background, recognition, diagnosis and management
 Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Introduction to Heart Failure. Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL
 Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
Heart Failure A Team Approach Background, recognition, diagnosis and management
 Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
Program Metrics. New Unique ID. Old Unique ID. Metric Set Metric Name Description. Old Metric Name
 Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Value of echocardiography in chronic dyspnea
 Value of echocardiography in chronic dyspnea Jahrestagung Schweizerische Gesellschaft für /Schweizerische Gesellschaft für Pneumologie B. Kaufmann 16.06.2016 Chronic dyspnea Shortness of breath lasting
Value of echocardiography in chronic dyspnea Jahrestagung Schweizerische Gesellschaft für /Schweizerische Gesellschaft für Pneumologie B. Kaufmann 16.06.2016 Chronic dyspnea Shortness of breath lasting
heart failure John McMurray University of Glasgow.
 A to Z of RAAS blockade in heart failure John McMurray BHF Cardiovascular Research Centre University of Glasgow. RAAS inhibition in CHF ACE inhibition in patients with low LVEF CHF CONSENSUS Enalapril
A to Z of RAAS blockade in heart failure John McMurray BHF Cardiovascular Research Centre University of Glasgow. RAAS inhibition in CHF ACE inhibition in patients with low LVEF CHF CONSENSUS Enalapril
Trial to Reduce. Aranesp* Therapy. Cardiovascular Events with
 Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Diastolic Heart Failure Uri Elkayam, MD
 Diastolic Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu Diastolic Heart Failure Clinical Definition A
Diastolic Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu Diastolic Heart Failure Clinical Definition A