APACVS April 6, 2018
|
|
|
- Lorena Copeland
- 5 years ago
- Views:
Transcription



1 APACVS April 6, 2018 Dejah R Judelson, MD Assistant Professor of Surgery Division of Vascular and Endovascular Surgery University of Massachusetts Medical School
2 I got a small stipend to be here I think I have the best job in the entire world I m married to the lead tech in our vascular lab so I think our vascular lab is the best one out there No other relevant disclosures

3 Be able to complete a thorough and focused vascular physical exam for pre-operative evaluation Understand appropriate vascular testing including ABIs, carotid duplex Recognize the indications for combined revascularizations (ie CEA-CABG)
4 Cardiothoracic surgery is inherently high risk Reduction of modifiable risk factors improves outcomes Patients with unidentified or untreated concomitant vascular disease can have worse outcomes and complications

5 Healing vein harvest sites Balloon pump placement Risk of stroke on-pump RIMA/LIMA inflow Risk of post-operative renal failure and mesenteric ischemia (Vascular Complications in the ICU, Sunday am)
6
7
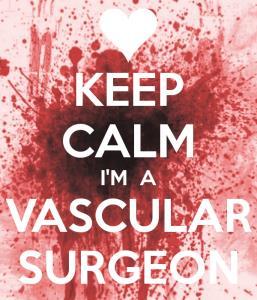
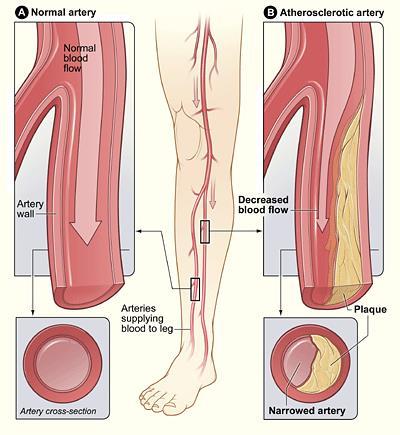
8 Carotid Disease Subclavian Disease Peripheral Arterial Disease Mesenteric Disease Renal artery occlusive disease

9 The prevalence of PAD in the lower limbs in a general population >55 years of age is between 10% and 25% and it increases with age Majority of affected population have asymptomatic disease. Peripheral arterial disease, whether symptomatic or asymptomatic, is a risk factor for non-fatal and fatal coronary disease and cerebrovascular events. Patients with PAD alone have the same relative risk of death from cardiovascular cause as those with coronary or cerebrovascular disease Circulation Research. 2015;116:

10 Circulation Research. 2015;116:
 concomitant PAD who participated in 7 clinical trials that employed serial intravascular ultrasound imaging JACC Vol. 57, No.")
11 The burden and progression of coronary atherosclerosis was investigated in 3,479 patients with coronary artery disease with (n = 216) and without (n = 3,263) concomitant PAD who participated in 7 clinical trials that employed serial intravascular ultrasound imaging JACC Vol. 57, No. 10, 2011
12
13
14 Global Registry of Acute Coronary Events (GRACE) increase of in-hospital mortality from 4.5 to 7.2% and a 6- month mortality from 3.9 to 8.8% in patients with lower extremity PVD CASS Registry 30 days post-cabg, patients with lower extremity PVD exhibited higher rates of mortality BARI: Bypass Angioplasty Revascularization Investigation Five-year mortality rates after CABG were five times higher in patients with symptomatic or asymptomatic ABI <0.9 compared with patients without PVD
15 Targeted History Vascular specific physical exam Pulses Skin changes Non-invasive vascular testing
16 Focus on what you need to get the patient through surgery safely and to reduce modifiable risk factors You probably aren t a vascular surgeon/vascular PA. And if you want to be one come talk to me later!
17 Few notable exceptions
18 Focus on symptoms! Be systematic Head to toe By organ system
19 What questions to ask/what are we focused on? Stroke symptoms Upper extremity symptoms Lower extremity symptoms Mesenteric ischemia symptoms Previous vascular procedures
20 Have they had a recent stroke or TIA (within the last 6 months)? Amaurosis fugax Expressive aphasia Lateralizing weakness/paresthesias Facial droop
21 Do they have a known history of different blood pressures in each arm? Most patients with subclavian stenosis are asymptomatic
22 Upper extremity fatigue can be very vague Early exhaustion when using one arm Upper extremity claudication History of syncope when using one arm Subclavian steal from reversal of flow in vertebral
23 3 classifications of symptoms Asymptomatic Claudication Critical Limb Ischemia Rest Pain Non-healing ulceration or lesion
24 Cramping when ambulating a set distance Discomfort relieved when patient stops moving (does not need to sit down) **It is (almost) always the same distance and occurs every time they walk** Pain occurs one level BELOW the level of disease Calf cramping femoral disease Thigh cramping aortoiliac disease
25 Leriche syndrome Specific constellation of symptoms associated with aortoiliac occlusive disease Men Buttock and thigh claudication Erectile dysfunction
26 Aka METATARSALGIA Pain that occurs while sleeping Across the metatarsal bones Often hard to describe Relieved by dangling their leg off the side of the bed Not the same as charley horse!
27 Have they had a history of non-healing or slow to heal ulcerations or lesions on their feet?
28 Post prandial abdominal pain Unintentional weight loss Food fear
29 Focus on reversible disease renal artery stenosis Difficult to control blood pressure on 4+ antihypertensives? Without another etiology

30
31 VITALS ARE VITAL Must get bilateral upper extremity blood pressure measurements High sensitivity for determining hemodynamically significant subclavian stenosis If SBP <20 point difference unlikely to have significant disease
32 4 Key things: 1. Pulses 2. Pulses 3. Pulses 4. Skin changes
33 Brachial Radial Femoral Dorsalis Pedis/Posterior Tibial If they have equal and palpable radial and pedal pulses unlikely significant disease!
34 But if you aren t completely sure. Do the complete pulse exam Strongly palpable brachial pulse that is symmetric unlikely to have significant subclavian stenosis (unless the patient is hypertensive or has bilateral disease) Strongly palpable femoral pulses unlikely to have aorto-iliac disease IABP can likely safely be placed Likely to heal vein harvest incisions
35 Skin changes Loss of hair on legs distally Lighter coloring of feet/toes Delayed capillary refill Be concerned for underlying PAD that may complicate healing of vein harvest
36 Things that I don t even do: Listen for carotid bruit Can be confused with aortic stenosis Neither sensitive nor specific for carotid stenosis Listen for abdominal bruit My patients are never skinny enough to appreciate RAS **for the record I do own and always use my stethoscope!**
37 Now you think there might be a vascular problem based on your history and exam what tests do you order to confirm it?
38 Lots of variability: tech dependent Radiology vs Vascular Surgery Registered Vascular Technicians vs Ultrasound Technicians Ask your vascular surgeons! Assuming you are at a place with an amazing reliable vascular lab like University of Massachusetts.
39 Direct Indirect
40 Doppler Duplex ultrasonography Laser doppler and skin perfusion Not used as frequently

41 Velocities are detected as frequency shifts in reflected ultrasound from the flowing red blood cells Arterial narrowing causes an increase in velocity at the site of the stenosis and dampening of the velocity waveform beyond

42 Handheld devices at the bedside transmit between 5-10MHz can only penetrate a few cm below the skin Probes have a receiving and transmitting piezoelectric crystal at the tip. Doppler output is a sound signature tells you if there is flow but not what direction it is going in


43 Normal peripheral arteries have a triphasic quality: brisk upstroke of forward flow in systole brief reversal in early diastole forward flow in late diastole Arterial obstruction leads to dampening of the waveforms with a monophasic output
44 Developed under Dr. Eugene Strandness at University of Washington 1967: Ultrasonic Flow Detection: A Useful Technic In The Evaluation of Peripheral Vascular Disease 1970s: combined B-mode with Doppler to create Duplex imaging Non-invasive and cost effective Pulsed doppler spectral analysis flow velocity distribution at a selected sample volume Provides information about peak velocity in sample


45 Combination of B mode (black and white) with color flow and doppler waveforms
46 ABI/TBI Segmental Pressures Pulse Volume Recording Transcutaneous Oxygen tissue measurement
47
48 ABI also has been shown to be linked to cardiovascular morbidity and mortality - ABI <0.5 found to have 5 yr survival of only 63% - ABI <0.67 independently associated with cardiac events and increased the risk for cardiac death by 2/3.

49 Useful in diabetics where ABI is non-compressible due to extensive calcifications of tibial vessels Normal >0.7 Toe pressure > 50 Interpretation Able to heal wounds CLI < 30 CLI with inability to heal wounds

50 Allows for identification of levels of disease Pressure gradients >20mmHg are significant and indicate disease at the level above Segmental pressure measurements also do not detect disease in nonaxial vessels, such as the profunda femoris Inaccurate in patients with calcification

51 Records volume changes in leg and thigh with arterial pulse - blood moves into microcirculation during systole, leading to increased tissue perfusion and limb volume Air-containing cuffs are applied to legs as leg volume increases, air in cuff gets displaced and is recorded by a transducer Allows for noninvasive evaluation even in patients with significant calcification
52

53 An oximetry probe is used to measure tissue oxygen perfusion Reports absolute oxygen pressure and ratio of oxygen pressures Normal wound healing requires TcpO2 > 40 TcpO2 < 20 indicates critical ischemia with need for revascularization
54 Cerebrovascular Disease: Carotid Duplex Subclavian Disease: Carotid Duplex, Upper Extremity Arterial Duplex Peripheral Arterial Disease: ABIs Chronic Mesenteric Ischemia: Mesenteric Duplex Renal Artery Stenosis: Renal Artery Duplex

55
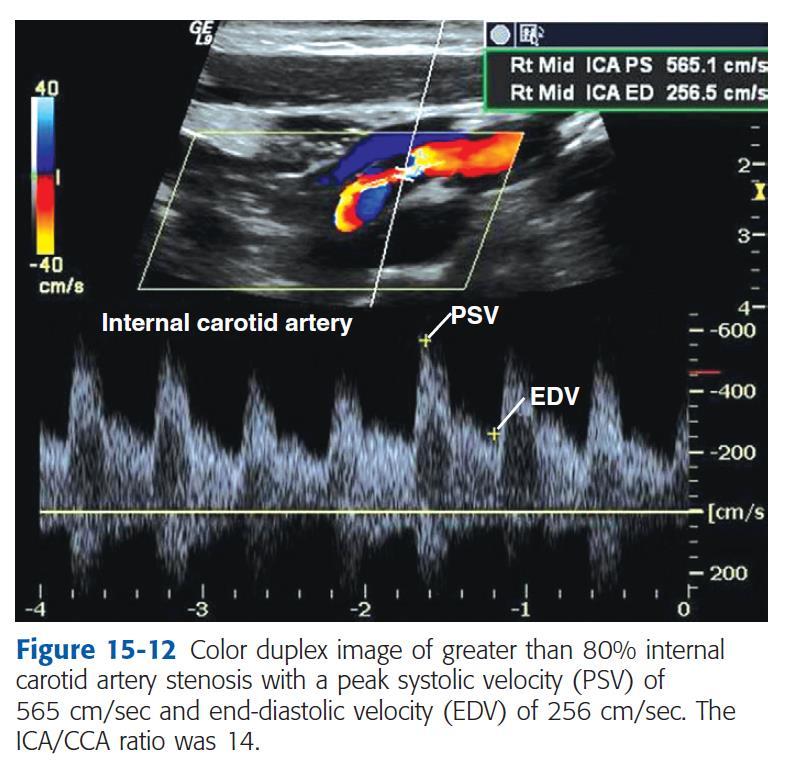
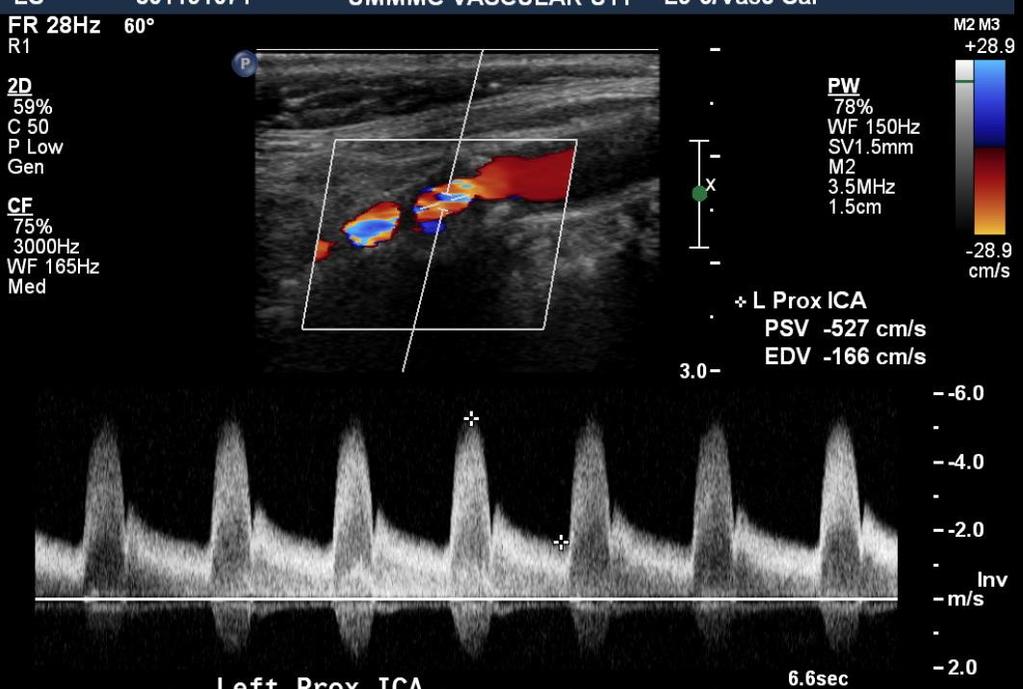
56 Most common clinical application is for the detection of proximal ICA atherosclerotic plaque and estimation of stenosis severity Can also identify subclavian stenosis (by retrograde flow in the vertebral) Huge variety in diagnostic criteria, no set standards Visualizes: Common carotid arteries Internal carotid arteries External carotid arteries Proximal Vertebral arteries
57 Inability to examine supraaortic trunks and distal cervical portions Quality and reliability is operator dependent Additional imaging may be indicated to visualize high bifurcations, tandem stenoses, proximal common or distal carotid disease May overestimate degree of stenosis if contralateral side occluded - elevated velocities as compensatory mechanism to maintain perfusion
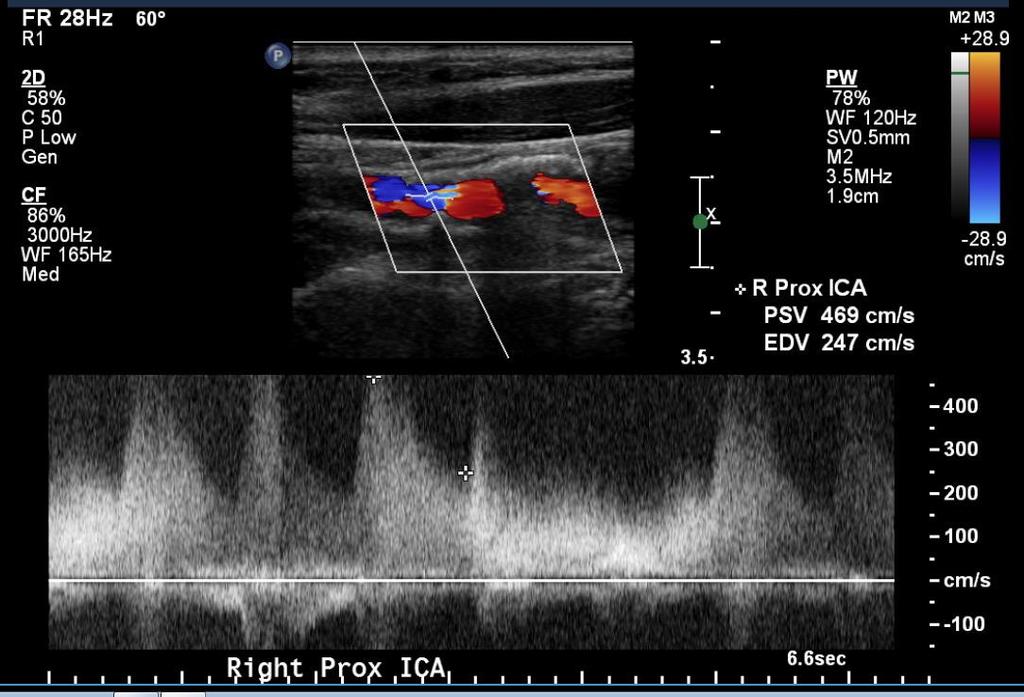
58 Stenoses reported in decile ranges 1-29% 30-49% 50-69% 70-79% 80-99% Occluded Stenosis determined by PSV, EDV, ratio
59
60
61 Used infrequently Direct visualization of subclavian, axillary, brachial, radial, ulnar arteries Looks at peak systolic velocity with focal increases to determine areas of stenosis Limitation: proximal left subclavian stenosis not visualized

62 ABIs/TBIs are sufficient to determine if there is significant PAD
63 Patient must be fasting ~90% accurate to detect >70% stenosis Visualizes celiac, SMA, IMA Criteria for >70% stenosis Celiac: PSV >200 cm/sec SMA: PSV >275 cm/sec IMA: no set criteria Must be accompanied by post stenotic turbulence and decreased velocities distal to the area of stenosis
64 >70% in 2+ mesenteric vessels Typically celiac and SMA Can be seen with SMA and IMA stenosis Isolated single mesenteric stenosis should not give you chronic mesenteric ischemia Acute mesenteric ischemia is a different story come back Sunday am!
65 Patient must be fasting PSV >180 cm/sec suggestive of >60% stenosis Renal/Aortic Velocity Ratio (RAR) RAR = PSV of renal artery/psv of suprarenal aorta <3.5 = normal >3.5 = Abnormal (>60% stenosis) Resistive Index = PSV-EDV/PSV <0.7 = normal 0.7= renal parenchymal disease
66
67 One of the most hotly debated topics in cardiac/vascular literature
68 Everyone s favorite vascular consult How many of you get carotid duplexes for: Every CABG and valve? All ascending aneurysms? Every open heart case?
69 Typically well tolerated vascular procedure Only moderate risk open vascular intervention At centers of excellence, stroke rates Asymptomatic disease: <1-3% Symptomatic disease: <3-5% Biggest complication: MI
70 Symptomatic disease (stroke or TIA within past 6 months) and stenosis >50% Asymptomatic disease >80% Some providers will perform CEA for low risk patients at stenosis >70%
71 Favored more by interventional radiologists and interventional cardiologists Vascular surgeons preferer CEA and reserve CAS for appropriate populations Biggest complication: risk of stroke Reduced cardiovascular complications

72 Case by case situation Is the risk of two surgeries greater than the risk of a combined case?



73
74 Should be performed if the risk of stroke during CABG is prohibitively increased if carotid revascularization isn t done in the same setting Symptomatic Disease Bilateral 80-99% stenosis (typically left) Unilateral occlusion and contralateral 80-99% Any other carotid stenosis >50% refer to vascular surgeon for outpatient evaluation
75 To heal a vein harvest site: need palpable femoral pulse and reasonable outflow To place an IABP: need palpable femoral pulse
76 Concern for symptomatic disease: claudication, rest pain, ulcers Non palpable femoral pulse Non palpable pedal pulse ABIs concerning for significant PAD
77 If you are planning on using a LIMA and there is a concern for subclavian stenosis Retrograde flow of vertebral on CDS Unequal upper extremity BP >20mm Hg Coronary angiogram concerning for subclavian stenosis
78 Patient endorses symptoms consistent with chronic mesenteric ischemia Mesenteric duplex with>70% in 1+ vessels
79 Worsening HTN refractory to 4+ meds Renal duplex with >60% stenosis

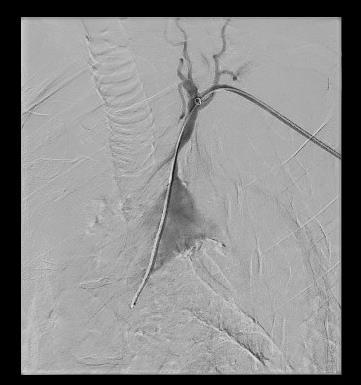
80 PAD case study Subclavian stenosis/carotid case study
81 61 male with history of hypertension, coronary artery disease s/p RCA plasty hyperlipidemia, ESRD on HD presented with chest pain during hemodialysis Coronary angiogram: severe three vessel coronary disease On preoperative evaluation patient endorses bilateral claudication, left >right
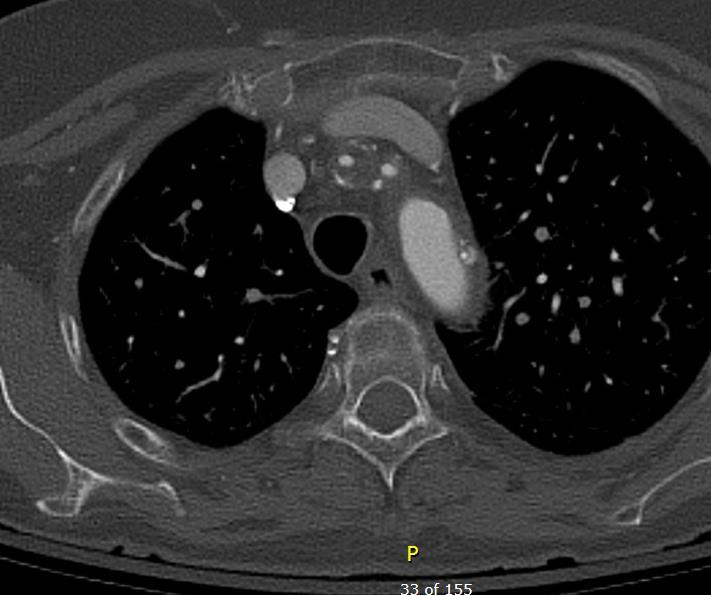
82 Vein mapping: Chronic superficial thrombophlebitis was found in the right great saphenous vein at the proximal calf. The left great saphenous vein was patent and continuous from the saphenofemoral junction to the ankle (0.09cm-0.57cm). Carotid Ultrasound: 30-49% stenosis of the right internal carotid artery % stenosis of the left internal carotid artery. STS mortality risk for an isolated CABG is 2.879
83 Emergent 4-vessel coronary artery bypass grafting Left endoscopic vein harvest LIMA to the mid LAD, GSV to RCA, GSV to ramus, GSV as a Y-graft off of the ramus graft going to D1 Immediate post op course uneventful

84 2 week post op with clear serous fluid draining from vein harvest site erythematous within a week or two started on PO ABx Presented one week later with small dehiscence at vein harvest site Duplex negative for fluid collection Sent out on antibiotics with HD


85 Two weeks later returned to the ED with increasing erythema at wound, unable to bear weight, contracture at knee CT leg showed air around the knee joint and significant vascular calcifications


86 Patient extensively debrided by plastic surgery

87 Post op noted foot was cool comparable to contralateral leg CT angiogram: common and external iliac occlusion, reconstitution of femoral artery


88 BEFORE AFTER Vascular surgery consult: Given extensive tissue loss, no option for limb salvage but needed revascularization to heal major amputation Underwent iliac stenting and then AKA Left common/external iliac occlusion Stenting left common/external iliac
89 If patient endorses lower extremity symptoms, work them up for PAD to determine extent of disease His leg pain was less significant (to him) than his chest pain and was hiding his rest pain!
90 73F with HTN, HLD had syncopal event positive stress test Cardiac cath: 3 vessel disease, arch branch disease, aorto-iliac occlusive disease Worked up for CABG CDS: bilateral 80-99% CAS with L CCA stenosis CTA findings: high grade innominate lesion moderate-severe L CCA stenosis high grade L SCA stenosis Celiac stenosis aorto-iliac occlusive disease
91
92

93
94 Left subclavian stent to preserve LIMA inflow Combined L CEA and L CCA stent with CABG Why left? Patient right handed speech center on the left Asymptomatic from celiac stenosis Intermittent claudication but weakly palpable femoral pulses

95

96

97 Thank You
Non-invasive examination
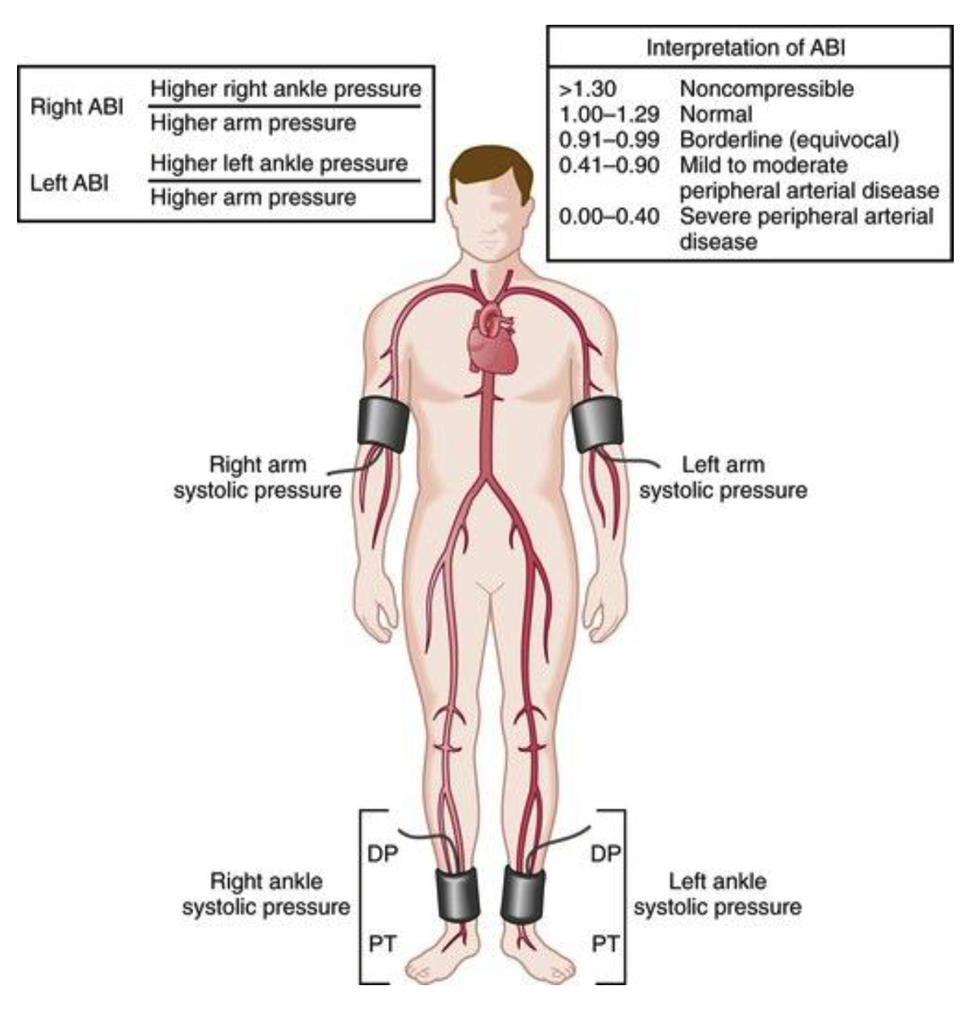
 Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
Role of ABI in Detecting and Quantifying Peripheral Arterial Disease
 Role of ABI in Detecting and Quantifying Peripheral Arterial Disease Difference in AAA size between US and Surgeon 2 1 0-1 -2-3 0 1 2 3 4 5 6 7 Mean AAA size between US and Surgeon Kathleen G. Raman MD,
Role of ABI in Detecting and Quantifying Peripheral Arterial Disease Difference in AAA size between US and Surgeon 2 1 0-1 -2-3 0 1 2 3 4 5 6 7 Mean AAA size between US and Surgeon Kathleen G. Raman MD,
Introduction to Peripheral Arterial Disease. Stacey Clegg, MD Interventional Cardiology August
 Introduction to Peripheral Arterial Disease Stacey Clegg, MD Interventional Cardiology August 20 2014 Outline (and for the ABIM board exam * ** ***) Prevalence* Definitions Lower Extremity: Aorta*** Claudication***
Introduction to Peripheral Arterial Disease Stacey Clegg, MD Interventional Cardiology August 20 2014 Outline (and for the ABIM board exam * ** ***) Prevalence* Definitions Lower Extremity: Aorta*** Claudication***
Ultrasound Imaging of The Posterior Circulation
 Ultrasound Imaging of The Posterior Circulation Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RDMS-RVT Clinical Manager General Ultrasound/Neurovascular Laboratory Cleveland
Ultrasound Imaging of The Posterior Circulation Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RDMS-RVT Clinical Manager General Ultrasound/Neurovascular Laboratory Cleveland
Introduction. Risk factors of PVD 5/8/2017
 PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
Duplex Ultrasound of the Renal Arteries. Duplex Ultrasound. In the Beginning
 Duplex Ultrasound of the Renal Arteries DIMENSIONS IN HEART AND VASCULAR CARE 2013 PENN STATE HEART AND VASCULAR INSTITUTE ROBERT G. ATNIP MD PROFESSOR OF SURGERY AND RADIOLOGY Duplex Ultrasound Developed
Duplex Ultrasound of the Renal Arteries DIMENSIONS IN HEART AND VASCULAR CARE 2013 PENN STATE HEART AND VASCULAR INSTITUTE ROBERT G. ATNIP MD PROFESSOR OF SURGERY AND RADIOLOGY Duplex Ultrasound Developed
Recommendations for Follow-up After Vascular Surgery Arterial Procedures SVS Practice Guidelines
 Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Imaging Strategy For Claudication
 Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Imaging for Peripheral Vascular Disease
 Imaging for Peripheral Vascular Disease James G. Jollis, MD Director, Rex Hospital Cardiovascular Imaging Imaging for Peripheral Vascular Disease 54 year old male with exertional calf pain in his right
Imaging for Peripheral Vascular Disease James G. Jollis, MD Director, Rex Hospital Cardiovascular Imaging Imaging for Peripheral Vascular Disease 54 year old male with exertional calf pain in his right
HD Scanning: Velocities and Volume Flow
 HD Scanning: Velocities and Volume Flow Non-Invasive Lab Symposium West Orange, NJ April 27, 2018 Volume Flow Cindy Sturt, MD, FACS, RVT 500,000 Americans on dialysis 20-25% annual mortality 65% 5 year
HD Scanning: Velocities and Volume Flow Non-Invasive Lab Symposium West Orange, NJ April 27, 2018 Volume Flow Cindy Sturt, MD, FACS, RVT 500,000 Americans on dialysis 20-25% annual mortality 65% 5 year
Perfusion Assessment in Chronic Wounds
 Perfusion Assessment in Chronic Wounds American Society of Podiatric Surgeons Surgical Conference September 22, 2018 Michael Maier, DPM, FACCWS Cardiovascular Medicine Cleveland Clinic Disclosures Speaker,
Perfusion Assessment in Chronic Wounds American Society of Podiatric Surgeons Surgical Conference September 22, 2018 Michael Maier, DPM, FACCWS Cardiovascular Medicine Cleveland Clinic Disclosures Speaker,
V.A. is a 62-year-old male who presents in referral
 , LLC an HMP Communications Holdings Company Clinical Case Update Latest Trends in Critical Limb Ischemia Imaging Amit Srivastava, MD, FACC, FABVM Interventional Cardiologist Bay Area Heart Center St.
, LLC an HMP Communications Holdings Company Clinical Case Update Latest Trends in Critical Limb Ischemia Imaging Amit Srivastava, MD, FACC, FABVM Interventional Cardiologist Bay Area Heart Center St.
Radiologic Evaluation of Peripheral Arterial Disease
 January 2003 Radiologic Evaluation of Peripheral Arterial Disease Grace Tye, Harvard Medical School Year III Patient D.M. CC: 44 y/o male with pain in his buttocks Occurs after walking 2 blocks. Pain is
January 2003 Radiologic Evaluation of Peripheral Arterial Disease Grace Tye, Harvard Medical School Year III Patient D.M. CC: 44 y/o male with pain in his buttocks Occurs after walking 2 blocks. Pain is
Practical Point in Holistic Diabetic Foot Care 3 March 2016
 Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
Subclavian artery Stenting
 Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Practical Point in Diabetic Foot Care 3-4 July 2017
 Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
No financial or commercial relationships to disclose
 Deanna New, RVT No financial or commercial relationships to disclose IAC REQUIREMENTS: The main duty of a sonographer is to make the physician or radiologists job easier by capturing images and doing
Deanna New, RVT No financial or commercial relationships to disclose IAC REQUIREMENTS: The main duty of a sonographer is to make the physician or radiologists job easier by capturing images and doing
Vascular Surgery Cases: Detours. Brian F. Stull, RDMS, RVT UNC REX Healthcare Vascular Specialists
 Vascular Surgery Cases: Detours Brian F. Stull, RDMS, RVT UNC REX Healthcare Vascular Specialists Brian.Stull@Unchealth.unc.edu Objectives Anatomy of a bypass graft Where does it connect, where does it
Vascular Surgery Cases: Detours Brian F. Stull, RDMS, RVT UNC REX Healthcare Vascular Specialists Brian.Stull@Unchealth.unc.edu Objectives Anatomy of a bypass graft Where does it connect, where does it
Current Status of Endovascular Therapies for Critical Limb Ischemia
 Current Status of Endovascular Therapies for Critical Limb Ischemia Bulent Arslan, MD Associate Professor of Radiology Director, Vascular & Interventional Radiology Rush University Medical Center bulent_arslan@rush.edu
Current Status of Endovascular Therapies for Critical Limb Ischemia Bulent Arslan, MD Associate Professor of Radiology Director, Vascular & Interventional Radiology Rush University Medical Center bulent_arslan@rush.edu
DISCLOSURE TEST YOUR WAVEFORM IQ. Partial volume artifact. 86 yo female with right arm swelling, picc line. AVF on left? Dx?
 Deborah Rubens University of Rochester Rochester, NY DISCLOSURE Neither I nor my immediate family have a financial relationship with a commercial organization that may have a direct or indirect interest
Deborah Rubens University of Rochester Rochester, NY DISCLOSURE Neither I nor my immediate family have a financial relationship with a commercial organization that may have a direct or indirect interest
Physician s Vascular Interpretation Examination Content Outline
 Physician s Vascular Interpretation Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 6 Cerebrovascular Abdominal Peripheral Arterial - Duplex Imaging Peripheral Arterial
Physician s Vascular Interpretation Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 6 Cerebrovascular Abdominal Peripheral Arterial - Duplex Imaging Peripheral Arterial
Arterial Studies And The Diabetic Foot Patient
 Arterial Studies And The Patient George L. Berdejo, BA, RVT, FSVU gberdejo@wphospital.org Disclosures I have nothing to disclose! Diabetes mellitus continues to grow in global prevalence and to consume
Arterial Studies And The Patient George L. Berdejo, BA, RVT, FSVU gberdejo@wphospital.org Disclosures I have nothing to disclose! Diabetes mellitus continues to grow in global prevalence and to consume
Introduction History Preceded by Arterial Doppler and ABI Indications
 Elise Brady, RVT, RDMS Introduction History Preceded by Arterial Doppler and ABI Indications 1) Abnormal ABI (within 2weeks of duplex) 2) Abnormal Doppler waveforms 3) Claudication 4) History of PVD 5)
Elise Brady, RVT, RDMS Introduction History Preceded by Arterial Doppler and ABI Indications 1) Abnormal ABI (within 2weeks of duplex) 2) Abnormal Doppler waveforms 3) Claudication 4) History of PVD 5)
Peripheral Arterial Disease: A Practical Approach
 Peripheral Arterial Disease: A Practical Approach Sanjoy Kundu BSc, MD, FRCPC, DABR, FASA, FCIRSE, FSIR The Scarborough Hospital Toronto Endovascular Centre The Vein Institute of Toronto Scarborough Vascular
Peripheral Arterial Disease: A Practical Approach Sanjoy Kundu BSc, MD, FRCPC, DABR, FASA, FCIRSE, FSIR The Scarborough Hospital Toronto Endovascular Centre The Vein Institute of Toronto Scarborough Vascular
Vascular Sonography Examination
 Vascular Sonography Examination The purpose of The American Registry of Radiologic Technologists (ARRT ) Vascular Sonography Examination is to assess the knowledge and cognitive skills underlying the intelligent
Vascular Sonography Examination The purpose of The American Registry of Radiologic Technologists (ARRT ) Vascular Sonography Examination is to assess the knowledge and cognitive skills underlying the intelligent
DON T LET LEG PAIN BECOME A REAL THREAT.
 DON T LET LEG PAIN BECOME A REAL THREAT. These three words have the power to change lives. Between 8 to 10 million Americans are estimated to suffer from poor blood flow to the legs and feet potentially
DON T LET LEG PAIN BECOME A REAL THREAT. These three words have the power to change lives. Between 8 to 10 million Americans are estimated to suffer from poor blood flow to the legs and feet potentially
Peripheral Arterial Disease Extremity
 Peripheral Arterial Disease Lower Extremity 05 Contributor Dr Steven Chong Advisors Dr Ashish Anil Dr Tay Jam Chin Introduction Risk Factors Clinical Presentation Classification History PHYSICAL examination
Peripheral Arterial Disease Lower Extremity 05 Contributor Dr Steven Chong Advisors Dr Ashish Anil Dr Tay Jam Chin Introduction Risk Factors Clinical Presentation Classification History PHYSICAL examination
Critical Limb Ischemia A Collaborative Approach to Patient Care. Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017
 Critical Limb Ischemia A Collaborative Approach to Patient Care Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017 Surgeons idea Surgeons idea represents the final stage of peripheral
Critical Limb Ischemia A Collaborative Approach to Patient Care Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017 Surgeons idea Surgeons idea represents the final stage of peripheral
Peripheral Vascular Disease
 Peripheral artery disease (PAD) results from the buildup of plaque (atherosclerosis) in the arteries of the legs. For people with PAD, symptoms may be mild, requiring no treatment except modification of
Peripheral artery disease (PAD) results from the buildup of plaque (atherosclerosis) in the arteries of the legs. For people with PAD, symptoms may be mild, requiring no treatment except modification of
Pedal Bypass With Deep Venous Arterialization:
 Pedal Bypass With Deep Venous Arterialization: Long Term Result For Critical Limb Ischemia With Unreconstructable Distal Arteries Pramook Mutirangura Professor of Vascular Surgery Faculty of Medicine Siriraj
Pedal Bypass With Deep Venous Arterialization: Long Term Result For Critical Limb Ischemia With Unreconstructable Distal Arteries Pramook Mutirangura Professor of Vascular Surgery Faculty of Medicine Siriraj
Aortoiliac occlusive disease
 Role of endovascular therapy in TASC II C & D inflow disease Per the TASC II Document: Surgery is the treatment of choice for type D lesions Aortoiliac occlusive disease Bala Ramanan, MBBS 1 st year vascular
Role of endovascular therapy in TASC II C & D inflow disease Per the TASC II Document: Surgery is the treatment of choice for type D lesions Aortoiliac occlusive disease Bala Ramanan, MBBS 1 st year vascular
Disclosures. Carotid artery stenting. Surveillance after Endovascular Intervention: When to Re-Intervene and What s the Evidence
 Disclosures Surveillance after Endovascular Intervention: When to Re-Intervene and What s the Evidence None 2015 UCSF Vascular Symposium Warren Gasper, MD Assistant Professor of Surgery UCSF Division of
Disclosures Surveillance after Endovascular Intervention: When to Re-Intervene and What s the Evidence None 2015 UCSF Vascular Symposium Warren Gasper, MD Assistant Professor of Surgery UCSF Division of
STRUCTURED EDUCATION REQUIREMENTS IMPLEMENTATION DATE: JULY 1, 2016
 STRUCTURED EDUCATION REQUIREMENTS Vascular Sonography The purpose of structured education is to provide the opportunity for individuals to develop mastery of discipline-specific knowledge that, when coupled
STRUCTURED EDUCATION REQUIREMENTS Vascular Sonography The purpose of structured education is to provide the opportunity for individuals to develop mastery of discipline-specific knowledge that, when coupled
Image Formation (10) 2 Evaluation and Selection of Representative Images (10)
 2 Evaluation and Selection of Representative Images (10)") STRUCTURED SELF ASSESSMENT CONTENT SPECIFICATIONS SSA LAUNCH DATE: JANUARY 1, 2018 Vascular Sonography The purpose of continuing qualifications requirements (CQR) is to assist registered technologists
STRUCTURED SELF ASSESSMENT CONTENT SPECIFICATIONS SSA LAUNCH DATE: JANUARY 1, 2018 Vascular Sonography The purpose of continuing qualifications requirements (CQR) is to assist registered technologists
Disclosures. Critical Limb Ischemia. Vascular Testing in the CLI Patient. Vascular Testing in Critical Limb Ischemia UCSF Vascular Symposium
 Disclosures Vascular Testing in the CLI Patient None 2015 UCSF Vascular Symposium Warren Gasper, MD Assistant Professor of Surgery UCSF Division of Vascular Surgery Critical Limb Ischemia Chronic Limb
Disclosures Vascular Testing in the CLI Patient None 2015 UCSF Vascular Symposium Warren Gasper, MD Assistant Professor of Surgery UCSF Division of Vascular Surgery Critical Limb Ischemia Chronic Limb
Lower Extremity Arterial Disease
 Lower Extremity Arterial Disease Circulating the Facts About Peripheral Disease Brought to you by the Education Committee of the Society for 1 www.svnnet.org Peripheral Artery Disease (PAD) Many people
Lower Extremity Arterial Disease Circulating the Facts About Peripheral Disease Brought to you by the Education Committee of the Society for 1 www.svnnet.org Peripheral Artery Disease (PAD) Many people
Surgical Options for revascularisation P E T E R S U B R A M A N I A M
 Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
National Vascular Registry
 National Vascular Registry Bypass Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or postcode.
National Vascular Registry Bypass Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or postcode.
Carotid Duplex: Beyond Stenosis Ido Weinberg, MD Vascular Medicine Massachusetts General Hospital Assistant Professor of Medicine Harvard Medical
 Carotid Duplex: Beyond Stenosis Ido Weinberg, MD Vascular Medicine Massachusetts General Hospital Assistant Professor of Medicine Harvard Medical School Boston, Massachusetts Disclosures I do not have
Carotid Duplex: Beyond Stenosis Ido Weinberg, MD Vascular Medicine Massachusetts General Hospital Assistant Professor of Medicine Harvard Medical School Boston, Massachusetts Disclosures I do not have
RadRx Your Prescription for Accurate Coding & Reimbursement Copyright All Rights Reserved.
 Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of November 19, 2018 Abdominal Aortogram, Bilateral Runoff
Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of November 19, 2018 Abdominal Aortogram, Bilateral Runoff
Garland Green, MD Interventional Cardiologist. Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management
 Garland Green, MD Interventional Cardiologist Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management Peripheral Arterial Disease Affects over 8 million Americans Affects 12% of the general
Garland Green, MD Interventional Cardiologist Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management Peripheral Arterial Disease Affects over 8 million Americans Affects 12% of the general
Resident Teaching Conference 3/12/2010
 Resident Teaching Conference 3/12/2010 Goals Definition and Classification of Acute Limb Ischemia Clinical Assessment of the Vascular Patient History and Physical Diagnostic Modalities Management of Acute
Resident Teaching Conference 3/12/2010 Goals Definition and Classification of Acute Limb Ischemia Clinical Assessment of the Vascular Patient History and Physical Diagnostic Modalities Management of Acute
EVALUATION OF THE VASCULAR STATUS OF DIABETIC WOUNDS Travis Littman, MD NorthWest Surgical Specialists
 EVALUATION OF THE VASCULAR STATUS OF DIABETIC WOUNDS Travis Littman, MD NorthWest Surgical Specialists Nothing To Disclosure DISCLOSURES I have no outside conflicts of interest, financial incentives, or
EVALUATION OF THE VASCULAR STATUS OF DIABETIC WOUNDS Travis Littman, MD NorthWest Surgical Specialists Nothing To Disclosure DISCLOSURES I have no outside conflicts of interest, financial incentives, or
Peripheral Vascular Examination. Dr. Gary Mumaugh Western Physical Assessment
 Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
Carotid Imaging IT S ABOUT MORE THAN JUST OBTAINING THE IMAGES
 Carotid Imaging IT S ABOUT MORE THAN JUST OBTAINING THE IMAGES No financial or commercial relationships to disclose Carotid artery disease: Stroke is one of the most serious causes of mortality and morbidity
Carotid Imaging IT S ABOUT MORE THAN JUST OBTAINING THE IMAGES No financial or commercial relationships to disclose Carotid artery disease: Stroke is one of the most serious causes of mortality and morbidity
Peripheral Arterial Disease: Who has it and what to do about it?
 Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS
 VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
National Vascular Registry
 National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
PUT YOUR BEST FOOT FORWARD
 PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
The Role of US in Chronic Mesenteric Ischemia. Sagar S. Gandhi, MD Vascular Health Alliance Greenville Health System
 The Role of US in Chronic Mesenteric Ischemia Sagar S. Gandhi, MD Vascular Health Alliance Greenville Health System No Disclosures Mesenteric Ischemia Anatomy Presentation Diagnostic tools Treatment Celiac
The Role of US in Chronic Mesenteric Ischemia Sagar S. Gandhi, MD Vascular Health Alliance Greenville Health System No Disclosures Mesenteric Ischemia Anatomy Presentation Diagnostic tools Treatment Celiac
Will it heal? How to assess the probability of wound healing
 Will it heal? How to assess the probability of wound healing Richard F. Neville, M.D. Professor of Surgery Chief, Division of Vascular Surgery George Washington University Limb center case 69 yr old male
Will it heal? How to assess the probability of wound healing Richard F. Neville, M.D. Professor of Surgery Chief, Division of Vascular Surgery George Washington University Limb center case 69 yr old male
Larry Diaz, MD, FSCAI Mehdi H. Shishehbor, DO, FSCAI
 PAD Diagnosis Larry Diaz, MD, FSCAI Metro Health / University of Michigan Health, Wyoming, MI Mehdi H. Shishehbor, DO, FSCAI University Hospitals Harrington Heart & Vascular Institute, Cleveland, OH PAD:
PAD Diagnosis Larry Diaz, MD, FSCAI Metro Health / University of Michigan Health, Wyoming, MI Mehdi H. Shishehbor, DO, FSCAI University Hospitals Harrington Heart & Vascular Institute, Cleveland, OH PAD:
The Peripheral Vascular System
 The Peripheral Vascular System Anatomy and Physiology Arteries Arteries contain 3 concentric layers of tissue: - the intima - the media - the adventitia The intima The endothelium of the intima has metabolic
The Peripheral Vascular System Anatomy and Physiology Arteries Arteries contain 3 concentric layers of tissue: - the intima - the media - the adventitia The intima The endothelium of the intima has metabolic
11 TH ANNUAL VASCULAR NONINVASIVE TESTING SYMPOSIUM NOVEMBER 10, 2018
 11 TH ANNUAL VASCULAR NONINVASIVE TESTING SYMPOSIUM NOVEMBER 10, 2018 RENAL ARTERY DISEASE AND RENOVASCULAR HYPERTENSION 1 WHAT IS RENOVASCULAR HYPERTENSION? https://my.clevelandclinic.org/health/diseases/16459-renovascular-hypertension
11 TH ANNUAL VASCULAR NONINVASIVE TESTING SYMPOSIUM NOVEMBER 10, 2018 RENAL ARTERY DISEASE AND RENOVASCULAR HYPERTENSION 1 WHAT IS RENOVASCULAR HYPERTENSION? https://my.clevelandclinic.org/health/diseases/16459-renovascular-hypertension
Objectives. Abdominal Aortic Aneuryms 11/16/2017. The Vascular Patient: Diagnosis and Conservative Treatment
 The Vascular Patient: Diagnosis and Conservative Treatment Ferrell-Duncan Clinic Zachary C. Schmittling, M.D., F.A.C.S. Vascular and General Surgery Ferrell-Duncan Clinic Cox Health Systems Objectives
The Vascular Patient: Diagnosis and Conservative Treatment Ferrell-Duncan Clinic Zachary C. Schmittling, M.D., F.A.C.S. Vascular and General Surgery Ferrell-Duncan Clinic Cox Health Systems Objectives
Contemporary management of brachiocephalic occlusive disease. TM Sullivan Minneapolis, MN
 Contemporary management of brachiocephalic occlusive disease TM Sullivan Minneapolis, MN WL Gore & Associates Disclosures Meeting organizer (SOAR) CR Bard Chair, CEC Bolster trial Veryan National PI, MIMICS
Contemporary management of brachiocephalic occlusive disease TM Sullivan Minneapolis, MN WL Gore & Associates Disclosures Meeting organizer (SOAR) CR Bard Chair, CEC Bolster trial Veryan National PI, MIMICS
UC SF. Disclosures. Vascular Assessment of the Diabetic Foot. What are the best predictors of wound healing? None. Non-Invasive Vascular Studies
 Disclosures Vascular Assessment of the Diabetic Foot What are the best predictors of wound healing? None Shant Vartanian MD Assistant Professor of Vascular Surgery UCSF Vascular Symposium April 20, 2013
Disclosures Vascular Assessment of the Diabetic Foot What are the best predictors of wound healing? None Shant Vartanian MD Assistant Professor of Vascular Surgery UCSF Vascular Symposium April 20, 2013
Indications: following: embolization. artery that has diseases 5. The evaluation. of suspected. such entities. a cold hand. biopsy
 Peripheral Arterial Ultrasound Protocol Using Color and Spectral Doppler Reviewed by: Mark Yuhasz, MD Last Review Date: January 2015 Contact: (866) 761 4200, Option 1 Indications: The indications for peripheral
Peripheral Arterial Ultrasound Protocol Using Color and Spectral Doppler Reviewed by: Mark Yuhasz, MD Last Review Date: January 2015 Contact: (866) 761 4200, Option 1 Indications: The indications for peripheral
9/7/2018. Disclosures. CV and Limb Events in PAD. Challenges to Revascularization. Challenges. Answering the Challenge
 Disclosures State-of-the-Art Endovascular Lower Extremity Revascularization Promotional Speaker Jansen Pharmaceutical Promotional Speaker Amgen Pharmaceutical C. Michael Brown, MD, FACC al Cardiology Associate
Disclosures State-of-the-Art Endovascular Lower Extremity Revascularization Promotional Speaker Jansen Pharmaceutical Promotional Speaker Amgen Pharmaceutical C. Michael Brown, MD, FACC al Cardiology Associate
2015 ARDMS Physicians Vascular Interpretation Job Task Analysis Summary Report
 P a g e 1 2015 ARDMS Physicians Vascular Interpretation Job Task Analysis Summary Report American Registry for Diagnostic Medical Sonography (ARDMS) P a g e 2 Table of Contents ABOUT THE REPORT... 3 METHODOLOGY...
P a g e 1 2015 ARDMS Physicians Vascular Interpretation Job Task Analysis Summary Report American Registry for Diagnostic Medical Sonography (ARDMS) P a g e 2 Table of Contents ABOUT THE REPORT... 3 METHODOLOGY...
Lower Extremity Artery: Physiologic Testing
 Master Title Ultrasound for Initial Evaluation of Lower Extremity Arterial Occlusive Disease: WHY? Gregory L. Moneta MD Professor and Chief Knight Cardiovascular Institute Division of Vascular Surgery
Master Title Ultrasound for Initial Evaluation of Lower Extremity Arterial Occlusive Disease: WHY? Gregory L. Moneta MD Professor and Chief Knight Cardiovascular Institute Division of Vascular Surgery
Peripheral Arterial Disease. Westley Smith MD Vascular Fellow
 Peripheral Arterial Disease Westley Smith MD Vascular Fellow Background (per 10,000) Goodney P, et al. Regional intensity of vascular care and lower extremity amputation rates. JVS. 2013; 6: 1471-1480.
Peripheral Arterial Disease Westley Smith MD Vascular Fellow Background (per 10,000) Goodney P, et al. Regional intensity of vascular care and lower extremity amputation rates. JVS. 2013; 6: 1471-1480.
Peripheral Arterial Disease: Objectives. Disclosure. Definition: Peripheral Arterial Disease (PAD)
") Geriatric Grand Rounds Tuesday, April 21, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
Geriatric Grand Rounds Tuesday, April 21, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Due to Perimed s commitment to continuous improvement of our products, all specifications are subject to change without notice.
 A summary Disclaimer The information contained in this document is intended to provide general information only. It is not intended to be, nor does it constitute, medical advice. Under no circumstances
A summary Disclaimer The information contained in this document is intended to provide general information only. It is not intended to be, nor does it constitute, medical advice. Under no circumstances
Intercepting PAD. Playbook for Cardiovascular Care 2018 February 24, Jonathan D Woody, MD, FACS. University Surgical Vascular
 Intercepting PAD Playbook for Cardiovascular Care 2018 February 24, 2018 Jonathan D Woody, MD, FACS University Surgical Vascular Attending Vascular Surgeon - Piedmont Athens Regional Adjunct Clinical Associate
Intercepting PAD Playbook for Cardiovascular Care 2018 February 24, 2018 Jonathan D Woody, MD, FACS University Surgical Vascular Attending Vascular Surgeon - Piedmont Athens Regional Adjunct Clinical Associate
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/30/2012 Radiology Quiz of the Week # 79 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/30/2012 Radiology Quiz of the Week # 79 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Artery 1 Head and Thoracic Arteries. Arrange the parts in the order blood flows through them.
 Artery 1 Head and Thoracic Arteries 1. Given the following parts of the aorta: 1. abdominal aorta 2. aortic arch 3. ascending aorta 4. thoracic aorta Arrange the parts in the order blood flows through
Artery 1 Head and Thoracic Arteries 1. Given the following parts of the aorta: 1. abdominal aorta 2. aortic arch 3. ascending aorta 4. thoracic aorta Arrange the parts in the order blood flows through
Current Vascular and Endovascular Management in Diabetic Vasculopathy
 Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Carotid Abnormalities Coils, Kinks and Tortuosity David Lorelli M.D., RVT, FACS Michigan Vascular Association Conference Saturday, October 20, 2012
 Carotid Abnormalities Coils, Kinks and Tortuosity David Lorelli M.D., RVT, FACS Michigan Vascular Association Conference Saturday, October 20, 2012 Page 1 Table of Contents Carotid Anatomy Carotid Duplex
Carotid Abnormalities Coils, Kinks and Tortuosity David Lorelli M.D., RVT, FACS Michigan Vascular Association Conference Saturday, October 20, 2012 Page 1 Table of Contents Carotid Anatomy Carotid Duplex
Boca Raton Regional Hospital Grand Rounds September 13, 2016
 Boca Raton Regional Hospital Grand Rounds September 13, 2016 W. Anthony Lee, MD, FACS Chief, BocaCare Vascular Surgery Christine E. Lynn Heart and Vascular Institute Boca Raton, Florida Disclosures No
Boca Raton Regional Hospital Grand Rounds September 13, 2016 W. Anthony Lee, MD, FACS Chief, BocaCare Vascular Surgery Christine E. Lynn Heart and Vascular Institute Boca Raton, Florida Disclosures No
Lower Extremity Arterial Duplex Evaluation
 VASCULAR TECHNOLOGY PROFESSIONAL PERFORMANCE GUIDELINES Lower Extremity Arterial Duplex Evaluation This Guideline was prepared by the Professional Guidelines Subcommittee of the Society for Vascular Ultrasound
VASCULAR TECHNOLOGY PROFESSIONAL PERFORMANCE GUIDELINES Lower Extremity Arterial Duplex Evaluation This Guideline was prepared by the Professional Guidelines Subcommittee of the Society for Vascular Ultrasound
Coral Reef Aorta- Treatment Options?
 Chronic mesenteric ischemia (CMI) Coral Reef Aorta- Treatment Options? Bala Ramanan Vascular Fellow, UCSF CMI is a life-threatening problem that can result in death from inanition or bowel infarction Incidence
Chronic mesenteric ischemia (CMI) Coral Reef Aorta- Treatment Options? Bala Ramanan Vascular Fellow, UCSF CMI is a life-threatening problem that can result in death from inanition or bowel infarction Incidence
Clinical Approach to CLI and Related Diagnostics: What You Need to Know
 Clinical Approach to CLI and Related Diagnostics: What You Need to Know Ido Weinberg, MD Assistant Professor of Medicine Harvard Medical School Massachusetts General Hospital None Disclosures Critical
Clinical Approach to CLI and Related Diagnostics: What You Need to Know Ido Weinberg, MD Assistant Professor of Medicine Harvard Medical School Massachusetts General Hospital None Disclosures Critical
A Healthy Heart. IN BRIEF: Your Guide to
 IN BRIEF: Your Guide to A Healthy Heart If you re like most people, you may think of heart disease as a problem for other folks. If you re a woman, you may believe that being female protects you from heart
IN BRIEF: Your Guide to A Healthy Heart If you re like most people, you may think of heart disease as a problem for other folks. If you re a woman, you may believe that being female protects you from heart
SCAI Fall Fellows Course Subclavian/Innominate Case Presentation
 SCAI Fall Fellows Course 2012 Subclavian/Innominate Case Presentation Daniel J. McCormick DO, FACC, FSCAI Director, Cardiovascular Interventional Therapy Pennsylvania Hospital University of Pennsylvania
SCAI Fall Fellows Course 2012 Subclavian/Innominate Case Presentation Daniel J. McCormick DO, FACC, FSCAI Director, Cardiovascular Interventional Therapy Pennsylvania Hospital University of Pennsylvania
Surveillance of Peripheral Arterial Disease Cases Using Natural Language Processing of Clinical Notes
 Surveillance of Peripheral Arterial Disease Cases Using Natural Language Processing of Clinical Notes Naveed Afzal, Sunghwan Sohn, Christopher G. Scott, Hongfang Liu, Iftikhar J. Kullo, Adelaide M. Arruda-Olson
Surveillance of Peripheral Arterial Disease Cases Using Natural Language Processing of Clinical Notes Naveed Afzal, Sunghwan Sohn, Christopher G. Scott, Hongfang Liu, Iftikhar J. Kullo, Adelaide M. Arruda-Olson
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI?
 Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
The Struggle to Manage Stroke, Aneurysm and PAD
 The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
Abdominal Exam: The examination of the abdomen used by physicians to detect an abdominal aortic aneurysm.
 Glossary of Terms Abdominal Exam: The examination of the abdomen used by physicians to detect an abdominal aortic aneurysm. Angiogram: A diagnostic test requiring the insertion of a catheter into an artery
Glossary of Terms Abdominal Exam: The examination of the abdomen used by physicians to detect an abdominal aortic aneurysm. Angiogram: A diagnostic test requiring the insertion of a catheter into an artery
Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI
 Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI 1 Disclosures I have no financial disclosures related to this talk Objectives 1. Discuss indications for intervention
Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI 1 Disclosures I have no financial disclosures related to this talk Objectives 1. Discuss indications for intervention
Peripheral Arterial Disease
 UFS Peripheral Arterial Disease A problem of supply and demand Larry Rhoads, Associate Chief Underwriter November 8, 2011 PAD Two categories of these circulation disorders: Functional peripheral vascular
UFS Peripheral Arterial Disease A problem of supply and demand Larry Rhoads, Associate Chief Underwriter November 8, 2011 PAD Two categories of these circulation disorders: Functional peripheral vascular
Schedule of Benefits. for Professional Fees Vascular Procedures
 Schedule of Benefits for Professional Fees 2018 Vascular Procedures ANASTOMOSIS RULES 820 Arteriovenous anastomosis in arm 1453 Arteriovenous anastomosis, open by basilic vein transposition 1465 Splenorenal
Schedule of Benefits for Professional Fees 2018 Vascular Procedures ANASTOMOSIS RULES 820 Arteriovenous anastomosis in arm 1453 Arteriovenous anastomosis, open by basilic vein transposition 1465 Splenorenal
USWR 23: Outcome Measure: Non Invasive Arterial Assessment of patients with lower extremity wounds or ulcers for determination of healing potential
 USWR 23: Outcome Measure: Non Invasive Arterial Assessment of patients with lower extremity wounds or ulcers for determination of healing potential MEASURE STEWARD: The US Wound Registry [Note: This measure
USWR 23: Outcome Measure: Non Invasive Arterial Assessment of patients with lower extremity wounds or ulcers for determination of healing potential MEASURE STEWARD: The US Wound Registry [Note: This measure
8/20/18. The Doppler Effect. Objectives. What is the Doppler Effect. Doppler principles. Spectral Waveform. Image recognition. Vascular Ultrasound
 Vascular Ultrasound: Physics and Haemodynamics Objectives Doppler principles Spectral Waveform Key factors Haemodynamics: Stenosis Waveforms Image recognition Vascular Ultrasound: A flawed paradigm What
Vascular Ultrasound: Physics and Haemodynamics Objectives Doppler principles Spectral Waveform Key factors Haemodynamics: Stenosis Waveforms Image recognition Vascular Ultrasound: A flawed paradigm What
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease
 Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine
BC Vascular Surgery Day
 BC Vascular Surgery Day November 4, 2017 1 Table of Contents Abdominal Aortic Aneurysm 3 4 Acute DVT 5 6 Peripheral Arterial Disease 7 9 Varicose Veins 10 11 Diabetic Foot Ulcers 12 13 Carotid Stenosis
BC Vascular Surgery Day November 4, 2017 1 Table of Contents Abdominal Aortic Aneurysm 3 4 Acute DVT 5 6 Peripheral Arterial Disease 7 9 Varicose Veins 10 11 Diabetic Foot Ulcers 12 13 Carotid Stenosis
EDUCATION. Peripheral Artery Disease
 EDUCATION Peripheral Artery Disease Peripheral Artery Disease You may have circulation problems that have to do with your blood vessels. You may feel aches, pains, cramps, numbness or muscle fatigue when
EDUCATION Peripheral Artery Disease Peripheral Artery Disease You may have circulation problems that have to do with your blood vessels. You may feel aches, pains, cramps, numbness or muscle fatigue when
CPT Code Details
 CPT Code 93925 Details Code Descriptor Duplex scan of lower extremity arteries or arterial bypass grafts; complete bilateral study Lay Term The provider performs a duplex ultrasound scan of the lower extremity
CPT Code 93925 Details Code Descriptor Duplex scan of lower extremity arteries or arterial bypass grafts; complete bilateral study Lay Term The provider performs a duplex ultrasound scan of the lower extremity
Guidelines for Ultrasound Surveillance
 Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
Lower Extremity Arterial Doppler
 Lower Extremity Arterial Doppler 1. Spectral Doppler waveform should be taken in distal aorta and common iliac arteries. 2. R/L common femoral artery (CFA) color Doppler with velocity and B-mode. 3. R/L
Lower Extremity Arterial Doppler 1. Spectral Doppler waveform should be taken in distal aorta and common iliac arteries. 2. R/L common femoral artery (CFA) color Doppler with velocity and B-mode. 3. R/L
Subclavian Revascularization. Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014
 Subclavian Revascularization Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014 Disclosure Information Douglas E. Drachman, MD, FACC Abbott Vascular, Inc.:
Subclavian Revascularization Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014 Disclosure Information Douglas E. Drachman, MD, FACC Abbott Vascular, Inc.:
Radial Artery Assessment for Coronary Artery Bypass
 VASCULAR TECHNOLOGY PROFESSIONAL PERFORMANCE GUIDELINES Radial Artery Assessment for Coronary Artery Bypass This Guideline was prepared by the Professional Guidelines Subcommittee of the Society for Vascular
VASCULAR TECHNOLOGY PROFESSIONAL PERFORMANCE GUIDELINES Radial Artery Assessment for Coronary Artery Bypass This Guideline was prepared by the Professional Guidelines Subcommittee of the Society for Vascular
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES
 NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
Cath Lab Essentials : Peripheral Vascular Disease in Patients with CAD
 Cath Lab Essentials : Peripheral Vascular Disease in Patients with CAD Pranav M. Patel, MD, FACC, FSCAI Interim Chief & Associate Professor of Medicine Director, Cardiac Catheterization Lab University
Cath Lab Essentials : Peripheral Vascular Disease in Patients with CAD Pranav M. Patel, MD, FACC, FSCAI Interim Chief & Associate Professor of Medicine Director, Cardiac Catheterization Lab University
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship
 Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Endovascular Should Be Considered First Line Therapy
 Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
How to Determine Tolerance for Branch Vessel Coverage
 How to Determine Tolerance for Branch Vessel Coverage Venita Chandra, MD Clinical Assistant Professor of Surgery Division of Stanford Medical School, Stanford, CA PNEC May 25 th, 2017 DISCLOSURES Venita
How to Determine Tolerance for Branch Vessel Coverage Venita Chandra, MD Clinical Assistant Professor of Surgery Division of Stanford Medical School, Stanford, CA PNEC May 25 th, 2017 DISCLOSURES Venita