Managing Patients with Sepsis
|
|
|
- Hilary Pearson
- 5 years ago
- Views:
Transcription

1 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany
2 Male Patient, Age 43 Years During last 2-3 days feeling moderately unwell with signs of upper respiratory tract infection (cough), but mobile and going out of the house until yesterday morning. Yesterday feeling increasingly unwell with mounting weakness and dyspnea. Towards the evening increasingly confused with slurred speech, weakness; unable to walk; spouse called emergency services. Admitted to emergency room: Temperature 38.9 C; HR 110/min, BP 110/70 mmhg; CRP 12 mg/dl, rales on auscultation; chest X-ray with suspected pneumonia. Antibiotic therapy (piperacillin/combactam), admission to ward. Next morning development of hypotension, dyspnea/tachypnea and O 2 desaturation (80%) transfer to ICU


3 Vital parameters following ICU admission Temperature 40.6 C O 2 saturation 87% Heart rate 150/min Respiratory rate 26/min BP syst. 90 mmhg BP diast. 50 mmhg Urine output
4
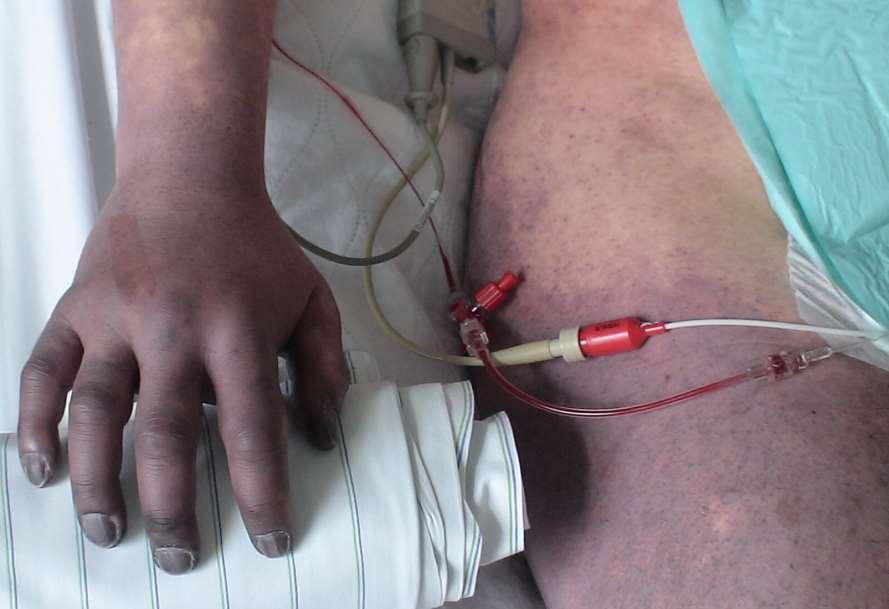
5

6


7 Labs Metabolic acidosis with respiratory compensation AKI Inflammation Liver enzymes Rhabdomyolysis Anemia Thrombopenia DIC

8 Sepsis A Disease Continuum Infection SIRS Sepsis Severe Sepsis At least 2 symptoms: Temp >38 C or < 36 C Heart rate > 90/min Respiratory rate > 20/min WBC > 11,500 oder < 4,000 or > 10% neutrophils SIRS with suspected or proven infectious origin Sepsis + organ dysfunction Circulation SHOCK! Kidney Lung BPsys <90 mmhg Liver MAD <65 mmhg Needs vasopressors Coagulation despite ml/kg CNS fluid resuscitation
 Obtain blood cultures prior to administration of antibiotics 3)")

9 SURVIVING SEPSIS CAMPAIGN CARE BUNDLES TO BE COMPLETED WITHIN 3 HOURS: 1) Measure lactate level 2) Obtain blood cultures prior to administration of antibiotics 3) Administer broad spectrum antibiotics 4) Administer 30 ml/kg crystalloid for hypotension or lactate 4 mmol/l Dellinger R et al. Critical Care Med. 2013; 41:
10 Initial resuscitation (first 6 hours): Begin resuscitation immediately in patients with hypotension or elevated serum lactate >4 mmol/l; do not delay pending ICU admission. Resuscitation goals: Central venous pressure (CVP) 8 12 mm Hg Mean arterial pressure 65 mm Hg Urine output 0.5 ml kg -1 hr -1 Central venous (superior vena cava) oxygen saturation 70%, or mixed venous 65% Dellinger R et al. Critical Care Med. 2013; 41:
.")
11 Prospective RCT in 263 patients with severe sepsis / septic shock upon hospital admission, six hours of early goal-directed therapy vs. standard therapy before admission to ICU In-hospital mortality was 30.5% in the group with early goal-directed therapy, vs. 46.5% with standard therapy (P=0.009). Rivers E et al, NEJM 2001; 345:
12 Total fluid administered over 72 h was not different between the groups, however: During the first 6 hours patients with early goaldirected therapy received significantly more fluid infusion early golden hours Rivers E et al, NEJM 2001; 345:
13 Prospective RCT, 1600 patients in 51 centers (mostly in Australia or New Zealand) presenting to the emergency department with early septic shock were randomized to EGDT vs. usual care Primary outcome was all-cause mortality within 90 days NEJM 2014; 371:
14 Prospective RCT, 1600 patients in 51 centers (mostly in Australia or New Zealand) presenting to the emergency department with early septic shock were randomized to EGDT vs. usual care Primary outcome was all-cause mortality within 90 days NEJM 2014; 371:
15 Prospective RCT, 1600 patients in 51 centers (mostly in Australia or New Zealand) presenting to the emergency department with early septic shock were randomized to EGDT vs. usual care Primary outcome was all-cause mortality within 90 days NEJM 2014; 371:
16 Prospective RCT, 1341 patients in 31 U.S. centers presenting to the emergency department with septic shock were randomized to EGDT vs. protocol-based standard therapy (no CVC placement, administration of inotropes, or blood transfusions) vs. usual care Primary outcome was in-hospital mortality within 60 days NEJM 2014; 370:
17 NEJM 2014; 370:
18 Surviving Sepsis Campaign Statement Regarding Hemodynamic and Oximetric Monitoring in Response to ProCESS and ARISE Trials (October 1, 2014) Required monitoring of CVP and ScvO 2 via a CVC as part of an early resuscitation strategy does not confer survival benefit in all patients with septic shock who have received timely antibiotics and fluid resuscitation compared with controls. Requiring measurement of CVP and ScvO 2 in all patients who have lactate results >4 mmol/l and/or persistent hypotension after initial fluid challenge and who have received timely antibiotics is not supported by the available scientific evidence. The results of the ProCESS and ARISE trials have not demonstrated any adverse outcomes in the groups that utilized CVP and ScvO 2 as end points for resuscitation. Therefore, no harm exists in keeping the current SSC bundles intact until a thorough appraisal of all available data has been performed.
19 Excessive Fluid Resuscitation Clinical consequences Impaired pulmonary function Impaired mental status Bowel dysfunction Intra-abdominal compartment syndrome Myocardial dysfunction Increased risk of decubital ulcers Delayed wound healing Muscle weakness / impaired mobilisation
 With RRT Fluid overload (>10% over baseline)")

20 Prospective observational study; 618 critically ill patients with AKI (5 UScentres) With RRT Fluid overload (>10% over baseline) independently associated with mortality but kidney function and renal recovery not improved Without RRT Bouchard et al., Kidney Int. 2009; 76: 422-7



21 Fluid Resuscitation Early interventions to achieve hemodynamic stability in patients with septic shock may reduce mortality Rapid fluid resuscitation of central importance Excessive fluid resuscitation and overhydration may lead to increased mortality and worse renal recovery
22 Crystalloids or Colloids?
23 Prospective, randomised study; 6,997 ICU patients in Australia and New Zealand Comparison of fluid resuscitation with 4% albumin vs. saline (28 days) 726 deaths in the albumin group, 729 deaths in the saline group (RR 0.99; 95 % CI, ; P=0.87). No difference regarding: ICU days (6.5 ± 6.6 with albumin vs. 6.2 ± 6.2 with saline, P=0.44) Hospital days (15.3 ± 9.6 vs /-9.6, P=0.30) Days on mechanical ventilation (4.5 ± 6.1 and 4.3 ± 5.7, P=0.74) Days on RRT (0.5 ± 2.3 and 0.4 ± 2.0, P=0.41). Finfer et al, N. Engl. J. Med. 2004; 350:
24 (CHEST) Crystalloid versus Hydroxyethyl Starch Trial 7,000 ICU patients (43% surgical) in AU/NZ randomised to FR with HES 130/0.4 (max. 50 ml/kg/day) or Saline 0.9% No difference in survival More patients in HES group required ARRT Myburgh et al, NEJM 2012; 367(20):
 increased renal failure among 8,725 patients (RR, 1.27; 95% CI 1.09-1.47) and increased use of renal replacement therapy among 9,258 patients (RR, 1.32; 95% CI, 1.15 to 1.")
25 Meta-analysis of 38 randomized controlled trials Hydroxyethyl starch was found to be associated with increased mortality among 10,290 patients (RR 1.09; 95% CI ) increased renal failure among 8,725 patients (RR, 1.27; 95% CI ) and increased use of renal replacement therapy among 9,258 patients (RR, 1.32; 95% CI, 1.15 to 1.50) Zarychanski R et al, JAMA 2013; 309 (7):
26 Fluid Therapy of Severe Sepsis We recommend crystalloids be used as the initial fluid of choice in the resuscitation of severe sepsis and septic shock (grade 1B). We recommend against the use of hydroxyethyl starches (HES) for fluid resuscitation of severe sepsis and septic shock (grade 1B). We suggest the use of albumin in the fluid resuscitation of severe sepsis and septic shock when patients require substantial amounts of crystalloids (grade 2C) Dellinger R et al. Critical Care Med. 2013; 41:
 as initial management for expansion of intravascular volume in patients at risk")
27 AKI Guideline 3.1. Hemodynamic monitoring and support for prevention and management of AKI 1. In the absence of hemorrhagic shock, we suggest using isotonic crystalloids rather than colloids (albumin or starches) as initial management for expansion of intravascular volume in patients at risk for AKI or with AKI. (2B) 2. We recommend the use of vasopressors in conjunction with fluids in patients with vasomotor shock with, or at risk for, AKI. (1C) 3. We suggest using protocol-based management of hemodynamic and oxygenation parameters to prevent development or worsening of AKI in high-risk patients in the perioperative setting (2C) or in patients with septic shock (2C). Kidney Int. Suppl. Volume 2, No 1 (March 2012)
28 When to initiate acute dialysis?

 Uraemic organ complications (e.g. pericarditis) Timely start: Serum urea concentration?")
29 When to initiate acute dialysis? Generally accepted indications Refractory hyperkalaemia (>6.5 mmol/l) Refractory volume overload Refractory metabolic acidosis (ph 7.1) Uraemic organ complications (e.g. pericarditis) Timely start: Serum urea concentration? Serum creatinine? AKI Stage?????


30 Most studies favour early start of RRT Paucity of randomized controlled trials, use of variable definitions of early RRT, and publication bias preclude definitive conclusions Seabra et al., AJKD 2008; 52:


31 Most studies favour early start of RRT The overall design and quality of studies comparing early versus late initiation of RRT in critically ill patients with AKI is low. Earlier initiation of RRT in critically ill patients with AKI may have a beneficial impact on survival Karvellas et al., Crit. Care 2011; 15: R72

32 Sepsis/Multiorgan Failure Should we start pre-emptive RRT?

33 Prospective multicenter RCT in 80 patients with sepsis/septic shock (study inclusion within 24h after first organ failure) CVVH for 96h with 25 ml/kg h vs. standard medical therapy Study stopped following Interim analysis! CVVH group: Higher number and severity of organ failure More/prolonged AKI (need for CVVH >96h) No reduction of plasma cytokines Payen D. et al., Crit. Care Med. 2009; 37:
34 Substudy of the FINNAKI (Finnish Acute Kidney Injury) study conducted in in 17 ICUs with 2901 patients Patients were classified as pre-emptive (no conventional indications) and classic (one or more indications) RRT recipients. Patients with classic RRT were further divided into classic-urgent (RRT initiated 12 hours from manifesting indications) and classic-delayed (RRT>12 hours from first indication). Additionally, 2450 patients treated without RRT were matched to patients with preemptive RRT. Of 239 patients treated with RRT, 134 fulfilled at least one conventional indication before commencing RRT. Vaara et al, CJASN 2014; 9:

35 Vaara et al, CJASN 2014; 9:

36 Patients on RRT after one or more conventional indications had higher crude and adjusted 90-day mortality compared with patients without conventional indications. Highest mortality in group with delayed RRT (>24 h) and classic indications Vaara et al, CJASN 2014; 9:

37 Timing of Acute Renal Replacement Therapy 1. Initiate RRT emergently when life-threatening changes in fluid, electrolyte, and acid-base balance exist. (Not Graded) 2. Consider the broader clinical context, the presence of conditions that can be modified with RRT, and trends of laboratory tests rather than single BUN and creatinine thresholds alone when making the decision to start RRT. (Not Graded) ARRT should be initiated once AKI is established and unavoidable but before overt complications have developed. The threshold for initiating RRT should be lowered when AKI occurs as part of multi-organ failure. The initiation of RRT may be deferred if the underlying clinical condition is improving and there are early signs of renal recovery. British Renal Association Standards Jörres A et al., Nephrol. Dial. Transplant. 2013; 28: KDIGO Group, Kidney Int. Suppl. Vol.2, No 1 (March 2012)
38 Acute Renal Replacement Therapy in Patients with AKI as Part of Multiorgan Failure Check for acute RRT indications Restore fluid status and circulation, correct electrolyte abnormalities Treat underlying problems If oliguria persists despite adequate fluid resuscitation and hemodynamic management, consider to start RRT without further delay (i.e. within hours) Prefer CRRT (or extended dialysis) over classic ihd Prescribe adequate RRT dose (e.g., 30 ml/kg/h in CRRT) in order to achieve the minimum recommended dose (20-25 ml/kg/h)
Timing, Dosing and Selecting of modality of RRT for AKI - the ERBP position statement
 Timing, Dosing and Selecting of modality of RRT for AKI - the ERBP position statement Prof. Dr. Achim Jörres Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Timing, Dosing and Selecting of modality of RRT for AKI - the ERBP position statement Prof. Dr. Achim Jörres Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Septic AKI in ICU patients
 Septic AKI in ICU patients Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany achim.joerres@charite.de Agenda Epidemiology
Septic AKI in ICU patients Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany achim.joerres@charite.de Agenda Epidemiology
Fluid Management in Critically Ill AKI Patients
 Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis
 How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis") Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Section 3: Prevention and Treatment of AKI
 http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes. Richard Beale
 Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
SURVIVING SEPSIS: Early Management Saves Lives
 SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
MAKING SENSE OF IT ALL AUGUST 17
 MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us?
 Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
What is sepsis? RECOGNITION. Sepsis I Know It When I See It 9/21/2017
 Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
SEPSIS 2015 DISCLOSURES FINANCIAL DISCLOSURES 9/1/2015. William M. Johnson, MD Nebraska Pulmonary Specialties. William Johnson
 SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
Diagnosis and Management of Sepsis. Disclosures
 Diagnosis and Management of Sepsis David Shimabukuro, MDCM Medical Director, 13 ICU Physician Lead, UCSF Sepsis Bundle Compliance and Mortality Reduction I have no disclosures Disclosures 1 The following
Diagnosis and Management of Sepsis David Shimabukuro, MDCM Medical Director, 13 ICU Physician Lead, UCSF Sepsis Bundle Compliance and Mortality Reduction I have no disclosures Disclosures 1 The following
Citrate Anticoagulation
 Strategies for Optimizing the CRRT Circuit Citrate Anticoagulation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany
Strategies for Optimizing the CRRT Circuit Citrate Anticoagulation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany
Sepsis care and the new core measures
 Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
Fluid balance and clinically relevant outcomes
 Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
EARLY GOAL DIRECTED THERAPY : seminaires iris. Etat des lieux en Daniel De Backer
 EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
Fluid Treatments in Sepsis: Meta-Analyses
 Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Update in Sepsis. Conflicts of Interest: None. Bill Janssen, M.D.
 Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it?
 Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Surviving Sepsis Campaign
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR
 Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Fluid assessment, monitoring and therapy for the acute nurse
 Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
JOURNAL CLUB: THE FLUIDS DEBATE. Veronica Ueckermann
 JOURNAL CLUB: THE FLUIDS DEBATE Veronica Ueckermann INTRODUCTION The selection and use of resuscitation fluids should be based on physiological principles. However, historically, clinical practice has
JOURNAL CLUB: THE FLUIDS DEBATE Veronica Ueckermann INTRODUCTION The selection and use of resuscitation fluids should be based on physiological principles. However, historically, clinical practice has
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the
 Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Blood purification in sepsis
 Blood purification in sepsis Joannes-Boyau O Dept of anesthesiology and intensive care, University Hospital of Bordeaux, France 1 Types of Blood Purification hemofilters regular pore size (MW < 40,000D)
Blood purification in sepsis Joannes-Boyau O Dept of anesthesiology and intensive care, University Hospital of Bordeaux, France 1 Types of Blood Purification hemofilters regular pore size (MW < 40,000D)
Early goal-directed therapy Where to from here? Rinaldo Bellomo ANZIC Research Centre Melbourne, Australia
 Early goal-directed therapy Where to from here? Rinaldo Bellomo ANZIC Research Centre Melbourne, Australia Early goal-directed therapy in septic shock 2001 Proof-of-concept EGDT trial published NEJM 16%
Early goal-directed therapy Where to from here? Rinaldo Bellomo ANZIC Research Centre Melbourne, Australia Early goal-directed therapy in septic shock 2001 Proof-of-concept EGDT trial published NEJM 16%
Advancements in Sepsis
 Objectives Advancements in Sepsis Brian Gilbert, PharmD PGY-1 Pharmacy Resident Jackson Memorial Hospital 3/13/2016 www.fshp.org Pharmacist objectives Review recent updates in resuscitation strategies
Objectives Advancements in Sepsis Brian Gilbert, PharmD PGY-1 Pharmacy Resident Jackson Memorial Hospital 3/13/2016 www.fshp.org Pharmacist objectives Review recent updates in resuscitation strategies
Guidelines are the Future of Sepsis Management Pro
 Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
LESSONS FROM EVIDENCE BASED MEDICINEIN THE CARE OF ARF AND ESRD. Prof. Dr. Adrian Covic University of Medicine Gr. T. Popa, Iaşi
 LESSONS FROM EVIDENCE BASED MEDICINEIN THE CARE OF ARF AND ESRD 2008 Prof. Dr. Adrian Covic University of Medicine Gr. T. Popa, Iaşi Effect of acute renal failure requiring renal replacement therapy on
LESSONS FROM EVIDENCE BASED MEDICINEIN THE CARE OF ARF AND ESRD 2008 Prof. Dr. Adrian Covic University of Medicine Gr. T. Popa, Iaşi Effect of acute renal failure requiring renal replacement therapy on
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Inflammatory Statements
 Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
Sepsis Care and the New Core Measures. Daniel S. Hagg, MD January 15, 2016
 Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
What s new in kidneys a renal update for Anaesthetists
 What s new in kidneys a renal update for Anaesthetists Thursday 11 th December 2014 Roslyn Simms Clinical Lecturer in Nephrology Renal update What s new/update AKI When to start RRT in AKI? Perioperative
What s new in kidneys a renal update for Anaesthetists Thursday 11 th December 2014 Roslyn Simms Clinical Lecturer in Nephrology Renal update What s new/update AKI When to start RRT in AKI? Perioperative
Sepsis. Reliability- can we achieve Dr Ron Daniels
 Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Fluid balance in Critical Care
 Fluid balance in Critical Care By Dr HP Shum Nephrologist and Critical Care Physician Department of Intensive Care, PYNEH Fluid therapy is a critical aspect of initial acute resuscitation in critically
Fluid balance in Critical Care By Dr HP Shum Nephrologist and Critical Care Physician Department of Intensive Care, PYNEH Fluid therapy is a critical aspect of initial acute resuscitation in critically
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign
 Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
What is the Role of Albumin in Sepsis? An Evidenced Based Affair. Justin Belsky MD PGY3 2/6/14
 What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
Approach to Severe Sepsis. Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore
 Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
Renal failure in sepsis and septic shock
 Renal failure in sepsis and septic shock Dr. Venugopal Reddy. MD, EDIC, FCARCSI Associate Professor of Anesthesiology and Critical Care medicine Department of Anaesthesia and CCM Penn State College of
Renal failure in sepsis and septic shock Dr. Venugopal Reddy. MD, EDIC, FCARCSI Associate Professor of Anesthesiology and Critical Care medicine Department of Anaesthesia and CCM Penn State College of
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL
 resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL") Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Actualités de la prise en charge hémodynamique initiale Daniel De Backer
 Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
6/5/2014. Sepsis Management and Hemodynamics. 2004: International group of experts,
 Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Fluids in ICU. JMO teaching 5th July 2016
 Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
SEPSIS & SEPTIC SHOCK
 SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
Last frontier of infection in critically ill patients
 Last frontier of infection in critically ill patients Nick Beeching Tropical & Infectious Disease Unit Royal Liverpool University Hospital Liverpool School of Tropical Medicine Liverpool School of Tropical
Last frontier of infection in critically ill patients Nick Beeching Tropical & Infectious Disease Unit Royal Liverpool University Hospital Liverpool School of Tropical Medicine Liverpool School of Tropical
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania
 AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania Who Am I? Except on few occasions, the patient appears
AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania Who Am I? Except on few occasions, the patient appears
3/14/2017. Pediatric Sepsis: From Goal Directed Therapy to Protocolized Care. Objectives. Developmental Response to Sepsis
 Pediatric Sepsis: From Goal Directed Therapy to Protocolized Care March 20, 2017 Reid WD Farris, MS MD Objectives Review the evolution & current state of the pediatric septic shock treatment guidelines
Pediatric Sepsis: From Goal Directed Therapy to Protocolized Care March 20, 2017 Reid WD Farris, MS MD Objectives Review the evolution & current state of the pediatric septic shock treatment guidelines
What is the right fluid to use?
 What is the right fluid to use? L McIntyre Associate Professor, University of Ottawa Senior Scientist, Ottawa Hospital Research Institute Centre for Transfusion Research CCCF, November 2, 2016 Disclosures
What is the right fluid to use? L McIntyre Associate Professor, University of Ottawa Senior Scientist, Ottawa Hospital Research Institute Centre for Transfusion Research CCCF, November 2, 2016 Disclosures