IMET 2000 PAL International Medical Education Trust Palestine What the GP Should Know about Hypertension
|
|
|
- Theodore Fletcher
- 5 years ago
- Views:
Transcription
1 What the GP Should Know about Hypertension Raed Abu Sham a, M.D Internist and Cardiologist Cardiac Pacing and Electrophysiologist
2 Impact of Age on Blood Pressure

3 Prevalence of HTN according to Age

4 Fast Facts about HTN in USA 69%

5 Control in % Hypertension Control in Europe and North America 30% 25% 26.8% 20% 15% 10% 5% 13.0% 9.3% 5.7% 7.7% 5.0% 11.6% 0% USA Canada England Finland Germany Spain Italy Wolf-Maier K et al, Hypertension 2004;43:10-17

6
7
8
9 Proportion of deaths attributable to leading risk factors worldwide (2000) High mortality, developing region Lower mortality, developing region Developed region Attributable Mortality (In millions; total 55,861,000) Ezzati et al. WHO 2000 Report. Lancet. 2002;360:
10 Hypertension as a Risk Factor Hypertension is a significant risk factor for: Cerebrovascular disease Coronary artery disease Congestive heart failure Renal failure Peripheral vascular disease Dementia Atrial fibrillation

11 Hypertension and Heart Failure
12 CVD Risk Factors HTN Inactivity Diabetes Age: Obesity >55 in men Dyslipidemia Cigarette Smoking >65 in women Family history of premature CVD
13

14 Classification of HTN in Adults

15 Classification of HTN in Adults Classification SBP (mmhg) DBP (mmhg) Normal Less than 120 and Less than 80 Prehypertension or Stage 1 hypertension Stage 2 hypertension or > 160 or > 100 Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003;42(6):
16 Classification of Hypertension Category Systolic Diastolic Optimal <120 and / or <80 Normal <130 and / or <85 High-Normal and / or Grade 1 (mild hypertension ) and / or Grade 2 (moderate HTN) and / or Grade 3 (severe HTN) 180 and / or 110 Isolated Systolic HTN (ISH) 140 and / or < 90 The category pertains to the highest risk blood pressure *ISH=Isolated Systolic Hypertension. J Hypertens 2007;25:
17 Classification for Adults Classification based on average of > 2 properly measured seated BP measurements from > 2 clinical encounters If systolic & diastolic blood pressure values give different classifications, classify by highest category > 130/80 mmhg: above goal for patients with diabetes or chronic kidney disease 17

18 How We Measure BP Appropriately?

19 Tips for Blood Pressure Measurement NO coffee or cigarette smoking for 30 minutes before the measurement. The patient should sit down for five minutes before test. The measurement should be done in a seating position. Set the patient s arm on a table. The measurement should be done when the arm is exposed.

20
21 Tips for BP Measurement Get 2 readings from both arms at first visit with five minutes apart. Tell your patients which is the arm of the higher reading. Always record from the highest arm thereafter. Tell your patient the result in numbers.


22 FACT Inaccurate blood pressure tests could affect millions
23 Training and measurement differences in blood pressure
 monitors Always used")
24 BP measurement 1. Auscultation method: [mercury] Should be available in all clinical areas Taught to all healthcare workers Used to check oscillometric (automatic) monitors Always used in certain clinical conditions: arrhythmias; preeclampsia; certain vascular disorders 2. Non-mercury auscultation method: Available in all clinical areas
: Not suitable for diagnosis of HTN Not suitable for Arrythmias; pre-eclampsia; certain vascular diseases 4.")
25 BP measurement 3. Oscillometric monitors (automatic): Not suitable for diagnosis of HTN Not suitable for Arrythmias; pre-eclampsia; certain vascular diseases 4. Aneroid monitors: Aneroid dial gauges easily prone to damage from dropping, causing significant errors in zero & calibration Suitable for HBPM








26 X X X

27 Calibrating Manometers Against the Mercury Column


28 Blood Pressure Measurement Myths & Facts


29 what size cuff? Size does matter Using too small a cuff/bladder can overestimate the blood pressure Bladder should encircle arm by % For cuff size follow manufacturer s recommendations

30 Too tight clothing if the sleeves are too tight or bulky they act as a tourniquet giving inaccurate readings

31 MYTH: Mercury sphygmomanometer should be positioned level with the patients heart? It should be level with the examiner s eye 9
32 MYTH: The position of the arm is unimportant During BP measurement? FACT: The arm should be well supported at HEART level (both sitting & standing) An unsupported arm is performing isometric exercise thus raising BP 4

33 At what rate should the cuff be deflated on a mercury or Greenlight sphygmomanometer? FACT: 2mm/Hg per second

34 How we evaluate a patient with Newly Diagnosed HTN?

35 Objectives of Patient Evaluation 1. Assess lifestyle and identify other CV risk factors 2. Reveal identifiable causes of high BP 3. Assess the presence or absence of target organ damage and CVD

36 Routine investigations Urine tests for protein and blood Serum creatinine and electrolytes Fasting blood glucose Lipid profile Electrocardiogram Chest x-ray no longer routinely indicated
37 Etiology Essential hypertension: > 90% of cases hereditary component Secondary hypertension: < 10% of cases common causes: CKD, renovascular disease other causes: drugs, natural products, food 37
38 Identifiable Causes of Hypertension Obstructive Sleep Apnea Syndrome Chronic kidney disease Renovascular disease Drug-induced Cushing s syndrome Thyroid or parathyroid disease Primary aldosteronism Pheochromocytoma Coarctation of the aorta
39 Causes of 2 Hypertension Prescription drugs: NSAIDs, COX-2 inhibitors Prednisone, Triamcinolone Decongestants Estrogens: oral contraceptives Amphetamines/Anorexiants Cyclosporine, Tacrolimus Erythropoietin 39
40 Causes of 2 Hypertension Food substances: Sodium Ethanol Licorice 40
41 Causes of 2 Hypertension Street drugs, other natural products: Herbal ecstasy Nicotine withdrawal Cocaine abuse and cocaine withdrawal Narcotic withdrawal 41

42 Clinical Features of OSAS

43 Acute BP changes during and immediately following an obstructive apneic episode


44 Incidence of CVD events during 7 years of follow-up in healthy middle-aged men at baseline
45 Home Blood Pressure Measurement HBPM
46 AHA call to action statement HBPM should become a routine component of BP measurement for the majority of patients with known or suspected hypertension using validated oscillometric monitors that measure BP on the upper arm with an appropriate cuff size.
47 Why We Need HBPM? 1. Better predictor of TOD 2. Helps reduce the white coat effect 3. Determine the presence of masked hypertension 2 to 3 readings should be taken while the subject is resting in the seated position, both in the morning and the evening, over 1 week. An average total of 12 readings is recommended for making clinical decisions. Discard first 24 hours of readings
48 Interpretation of the Results The levels of average HBPM considered as definite hypertension by the majority of the guidelines is 135/85 mm Hg. The WHO Guidelines recommended an upper limit of normality as 125/80 mmhg
49 Appropriateness of HBPM Most patients are suitable for HBPM but do need instruction in the methods. Those unsuitable include patients with atrial fibrillation and other significant cardiac arrhythmias.

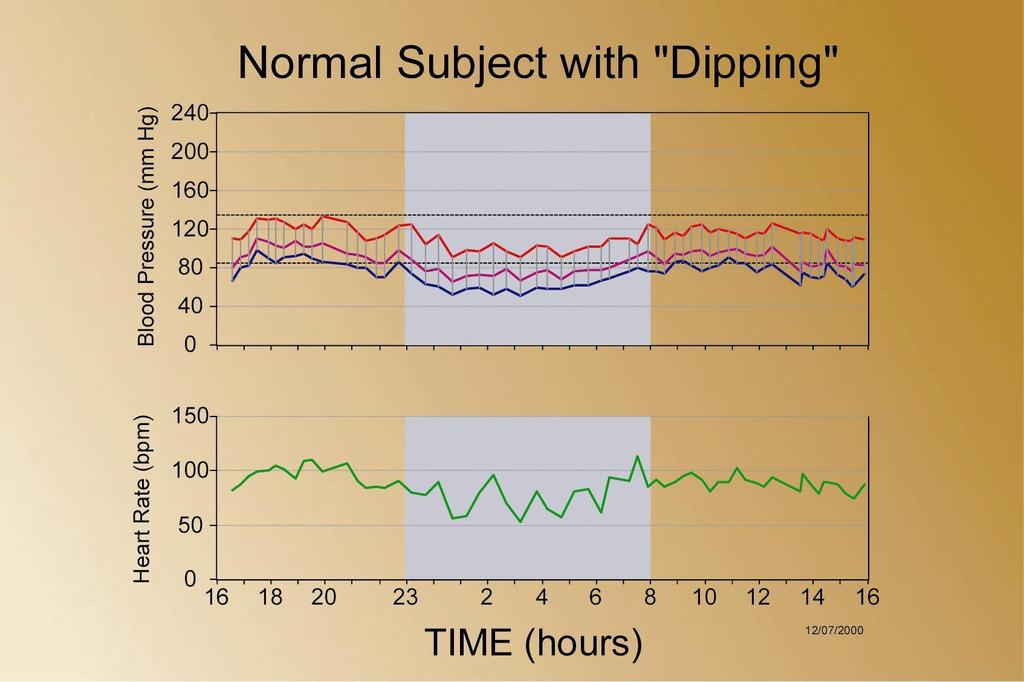
50 Ambulatory Blood Pressure Measurement [ABPM]
51
52 Indications for ABPM 1. Unusual variability 2. Possible white coat hypertension 3. Informing equivocal treatment decisions 4. Evaluation of nocturnal hypertension 5. Evaluation of drug-resistant hypertension 6. Determining the efficacy of drug treatment over 24 hours 7. Diagnoses and treatment of hypertension in pregnancy 8. Evaluation of symptomatic hypotension
53 Why we need to treat HTN?

54 The Natural History of Untreated HTN
55 BP and Risk of Stroke Mortality Lancet 2002;360:
56 BP and Risk of IHD Mortality Lancet 2002;360:
57 Treatment goals Reduce blood pressure Reduce mortality Reduce stroke Reduce congestive heart failure Reduce coronary artery disease Reduce nephropathy Reduce retinopathy Short term goal Long term goal

58 Are these Risks Only in Patients with True Hypertension?
59 Home/Ambulatory SBP mmhg The Concept of Masked HTN Masked HTN True hypertensive True Normotensive White Coat HTN Office SBP mmhg Derived from Pickering et al. Hypertension 2002: 40:
60 Odds Ratio of a Cardiovascular Event The Prognosis of White Coat and Masked Hypertension Prevalence is approximately 10% in hypertensive patients Normal BP White coat hypertension Masked Hypertension Hypertension J Hypertension 2007;25:
61 Cumulative hazard of stroke (%) Cumulative hazard for stroke in 3 groups of subjects: Normotensive, White-Coat Hypertension, and Ambulatory hypertension White-coat hypertension Ambulatory hypertension 5 4 Normotensive group p = Time to stroke (years) Hypertension. 2005;45(2):

62 Is there a Difference Between Systolic and Diastolic Hypertension?
63 Effect of SBP and DBP on Age-Adjusted CAD Mortality: MRFIT CAD Death Rate per 10,000 Person-years <70 Diastolic BP (mmhg) < Systolic BP (mmhg) Neaton et al. Arch Intern Med 1992; 152:56-64.
64 HOT Study: Significant Benefit From Intensive Treatment in the Diabetic Subgroup Major cardiovascular events/1,000 patient-years p=0.005 for trend mm Hg Target Diastolic Blood Pressure Hansson L et al. Lancet. 1998;351:
65 Benefits of Lowering BP Diseases Reduction Average Percent Stroke 35-40% Myocardial Infarction 20-25% Heart Failure 50% 7 Th Joint National Committee on High Blood Pressure
66 90% of Hypertensives have other Cardiovascular Risk factors 10% Reduction in BP + 10% Reduction in Total-C = 45% Reduction in CVD Emberson et al. Eur Heart J. 2004;25:
67 Failures of Patient Education 50% of patients discontinue their anti-hypertensive within 1 year of initiating treatment. Can J Cardiol 2005;21:589-93
68 When to Treat? 1. Medication Required if: Sustained raised BP > 140/90 mmhg Any reading > 160/100 mmhg (despite non-pharmacological treatment) 2. OR if: BP > 140/90 mmhg AND patient has: 1. Target Organ Damage, or 2. CVD, or year CVD risk > 20%
69 Target-Organ Damage Brain: stroke, TIA, dementia Eyes: retinopathy Heart: left ventricular hypertrophy, angina, HF Kidney: chronic kidney disease Blood Vessels: peripheral arterial disease 69
70 Treatment Goals Reduce morbidity & mortality Select drug therapy based on evidence demonstrating risk reduction Patient Population Most patients Diabetes mellitus Chronic kidney disease Target Blood Pressure < 140/90 mmhg < 130/80 mmhg <130/80 mmhg Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003;42(6):
71 2007 AHA Recommendations More aggressive BP lowering for high risk patients Most patients for general prevention <140/90 mmhg Patients with diabetes (CAD risk equivalent), Significant CKD Known CAD (MI, stable angina, unstable angina), <130/80 mmhg Noncoronary atherosclerosis (stroke, TIA, PAD, AAA) Framingham risk score > 10% Patients with left ventricular dysfunction (HF) <120/80 mmhg Rosendorff C, Black HR, Cannon CP, et al. Treatment of hypertension in the prevention and management of ischemic heart disease: A scientific statement from the American Heart Association Council for High Blood Pressure Research and the Councils on Clinical Cardiology and Epidemiology and Prevention. Circulation 2007;115(21):
72 JNC 7: Treatment Algorithm Lifestyle modifications Not at goal blood pressure (<140/90 mm Hg) (<130/80 mm Hg for those with diabetes or chronic kidney disease) Initial drug choices Without compelling indications With compelling indications Stage 1 hypertension (SBP or DBP mm Hg) Thiazide-type diuretic for most. May consider ACEI, ARB, BB, CCB, or combination. Stage 2 hypertension (SBP 160 or DBP 100 mm Hg) Two-drug combination for most (usually thiazide-type diuretic and ACEI or ARB or BB or CCB). Drugs for compelling indications Other antihypertensive drugs (diuretic, ACEI, ARB, BB, CCB) as needed. Not at goal blood pressure Optimize dosages or add additional drugs until goal blood pressure is achieved. Consider consultation with hypertension specialist. JNC 7. May NIH publication
73 Key Diet History Questions Do you use a salt shaker? Do you taste your food before you add salt? How often do you eat salty foods, such as chips, salted nuts, canned and smoked foods? Do you read labels for sodium content? How many servings of fruits and vegetables do you eat everyday? How often do you eat or drink dairy products? What kind? How often do you eat out? What kinds of restaurants? How often do you exercise, including walking?
74 FACT: Lifestyle intervention for blood pressure reduction Intervention Recommendation Expected SBP reduction Weight reduction Maintain ideal body mass index (20-25kg/M²) 5-10 mmhg per 10kg loss DASH eating plan Eat diet rich in fruit, vegetables, low-fat dairy products. Eat less saturated and total fat 8-14 mmhg Sodium restriction Reduce dietary sodium intake to <100mmol/day <2.4g sodium or <6 g salt (sodium chloride) 2-8mmHg Physical activity Regular aerobic physical activity, e.g. brisk walking for at least 30 min most days 4-9 mmhg Alcohol moderation Men 21 units per week Women 14 units per week 2-4 mmhg

75
76 Compelling Indications Heart Failure: Post- MI: High CVD risk: DM: CRF ACEi, ARB, Diuretics, BB, Aldosterone antagonist BB, ACEi, Aldosterone antagonist Thiazide, ACE, BB, Ca channel blocker ACE, ARB, CCB, Thiazide, BB S/P CVA ACE, ARB. For creatinine 2-3 try loop diuretic Thiazide, ACE inhibitor
77 Change in LV mass index (%) Reversal of LV Hypertrophy By Antihypertensive Treatment 0 Diuretics -blockers Calcium channel blockers ACE inhibitors % 6% 9% % p<.01 p<.01 Schmieder RE et al. JAMA. 1996;275:
78 TIPS on drugs for HTN Most patients should start with a diuretic as they enhance the effectiveness of other agents. Most patients will require more than one agent. Add a baby aspirin to improve cardiovascular outcomes.
79 TIPS on drugs for HTN CCB for isolated systolic hypertension For DM: ACEi or ARB with or without diuretic, then add CCB and then BB. When ACEi causes cough, substitute ARB Don t use short acting CCB (increase mortality).

80 Combination Therapy
81 Rules of Combination Therapy 1. Most patients require > 2 drugs 2. A thiazide-type diuretic should be one of these agents unless contraindicated 3. Combination regimens should include a diuretic (preferably a thiazide) 4. If BP is >20/10 mmhg above goal, initiate therapy with two agents. 81
82 Reasons for Inadequate Control of BP? 1. Ineffective drugs? 2. Resistant hypertension? 3. Drug costs? 4. Drug side-effects? 5. Poor adherence/compliance? 6. Physician inertia?
83 Hypertension Emergencies Hypertensive Crises
84 Hypertensive Crisis BP > 180/120 mmhg reduce gradually Hypertensive urgency elevated BP no acute or progressing target-organ injury Hypertensive emergency acute or progressing target-organ damage encephalopathy, intracranial hemorrhage, acute left ventricular failure with pulmonary edema, dissecting aortic aneurysm, unstable angina, eclampsia 84
85 Hypertensive Crises They represent about 1% of patients who present for evaluation of hypertension. They account for up to 25% of all emergency department visits The clinical outcome for untreated patients with a hypertensive emergency: 1-year mortality rate is 70% to 90% 5-year mortality rate is nearly 100%
86 Hypertensive Emergencies and Urgencies Hypertensive emergency combines a severe elevation in BP with acute, ongoing target organ damage. Hypertensive urgencies, may be better termed severe elevations in BP. without acute target organ damage.
87 Hypertensive Emergency It is associated with severe elevation in BP, accompanied by progressive TOD. It is not the degree of BP elevation, but the clinical status of the patient that defines it as an emergency. Patients with hypertensive emergencies need to be treated with parenteral medications.
88 Hypertensive Emergencies 1. Hypertensive encephalopathy 2. Malignant hypertension: [acute retinopathy] 3. Intracranial hemorrhage or brain infarction 4. Acute coronary syndromes 5. Acute pulmonary edema 6. Acute aortic dissection 7. Rapidly progressive renal failure 8. Eclampsia 9. Life-threatening arterial bleeding 10. Head trauma
89 Severe Blood Pressure Elevation (Hypertensive Urgency) Severe elevations in BP without progressive TOD. Examples include Severe BP Elevation with: severe headache shortness of breath Epistaxis severe anxiety Even though these patients may have signs of chronic target organ damage
90 Severe Blood Pressure Elevation (Hypertensive Urgency) Most of these patients are not adherent to drug therapy or have inadequately treated hypertension. These patients require neither hospital admission nor acute lowering of BP, and they can safely be treated in the outpatient setting with oral medications.
91 EVALUATION Therapy may need to be initiated before all test results are obtained or before the underlying cause of the emergency becomes known.
92 EVALUATION 1. A focused history and examination. 2. CBC 3. BUN, creatinine, electrolytes 4. Urinalysis 5. Electrocardiogram 6. CXR 7. Brain CT scan for patients with neurologic signs and symptoms
93 Treatment of Hypertensive Emergencies These patients require immediate admission to an ICU or monitored bed for IV therapy. BP should not be rapidly lowered into the normal range The initial goal of therapy is to reduce mean arterial BP to no more than 25% within the first 2 hours.
94 Treatment of Hypertensive Emergencies Over the next 2 to 6 hours, BP should be reduced slowly toward 160/100 mm Hg. If this is well tolerated, further gradual reductions toward normal over the next 24 to 48 hours. The most notable exceptions: Acute aortic dissection (SBP target: <120 mm Hg over 20 minutes) Acute stroke in evolution (BP lowering is not recommended).
95 Treatment of Hypertensive Emergencies It is unclear which drugs is superior to another. Parenteral agents should be used initially. Oral agents can be started as the parenteral agent is tapered. Typically, patients with hypertensive emergencies are volume depleted, so loop diuretics are not recommended unless there is evidence of volume overload. The use of diuretics may be necessary after 12 hours of intravenous vasodilator therapy.
96 Treatment of Hypertensive urgencies First of all, rule out a true hypertensive emergency Address the cause Patients should be treated with oral agents, with the intent to decrease the BP over the next 24 to 48 hours. Sometimes, antihypertensive drug treatment carries an even greater risk. Short-acting nifedipine is contraindicated.
97 Pay attention please... Some patients present with severely elevated BPs that can be attributed to: pain anxiety and fear These patients should be treated with analgesics or anxiolytics before antihypertensive agents are considered.
98 When Shall You Refer Your Patient to an Internist or Hypertension Specialist?
99 Indications for Specialist Referral Urgent treatment needed Accelerated hypertension (severe HTN and grade III-IV retinopathy) Severe hypertension (>220/120mmHg) Impending complications (e.g. TIA, LVF)
100 Indications for Specialist Referral Possible underlying cause Any clue in history or examination of a secondary cause Raised serum creatinine Proteinuria or haematuria Sudden onset or worsening of hypertension Resistant to multi-drug regimen (> 3 drugs) Young age Any hypertension <20 years; needing treatment <30 years
101 Indications for Specialist Referral Therapeutic problems Multiple drug intolerance Multiple drug contraindications Non-adherence or non-compliance Special situations Unusual blood pressure variability Possible white coat hypertension Hypertension in pregnancy
102
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
What is hypertension?
 HYPERTENSION What is hypertension? Abnormally elevated arterial blood pressure that is usually indicated by an adult systolic blood pressure of 140 mm Hg or greater or a diastolic blood pressure of 90
HYPERTENSION What is hypertension? Abnormally elevated arterial blood pressure that is usually indicated by an adult systolic blood pressure of 140 mm Hg or greater or a diastolic blood pressure of 90
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Hypertension Update Background
 Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Hypertension Update. Aaron J. Friedberg, MD
 Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to
 Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans
 Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
major public health burden
 HYPERTENSION INTRODUCTION Hypertension is one of the major public health burden in the recent times. Hypertension remains a challenging medical condition among the noncommunicable diseases of ever growing
HYPERTENSION INTRODUCTION Hypertension is one of the major public health burden in the recent times. Hypertension remains a challenging medical condition among the noncommunicable diseases of ever growing
From the desk of the: THE VIRTUAL NEPHROLOGIST
 Hypertension, also referred to as high blood pressure or HTN, is a medical condition in which the blood pressure is chronically elevated. It is a very common illness. One out of three American adults has
Hypertension, also referred to as high blood pressure or HTN, is a medical condition in which the blood pressure is chronically elevated. It is a very common illness. One out of three American adults has
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Genetic factors. A number of genetic factors or interactions between genes play a major role in essential hypertension.
 Hypertension Blood pressure is a measurement of the force against the walls of your arteries as your heart pumps blood through your body. Hypertension is another term used to describe high blood pressure.
Hypertension Blood pressure is a measurement of the force against the walls of your arteries as your heart pumps blood through your body. Hypertension is another term used to describe high blood pressure.
SAURIN GANDHI, AZCOM Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8)
") 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8) Background HTN is the most common condition seen in primary care and leads to MI, stroke, renal failure, and death
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8) Background HTN is the most common condition seen in primary care and leads to MI, stroke, renal failure, and death
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Hypertension. Most important public health problem in developed countries
 Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Blood Pressure Treatment in 2018
 Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
HYPERTENSION: ARE WE GOING TOO LOW?
 HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
Summary of recommendations
 Summary of recommendations Measuring blood pressure (BP) Use the recommended technique at every BP reading to ensure accurate measurements and avoid common errs. Pay particular attention to the following:
Summary of recommendations Measuring blood pressure (BP) Use the recommended technique at every BP reading to ensure accurate measurements and avoid common errs. Pay particular attention to the following:
Management of Hypertension in special groups. DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University
 Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
New Hypertension Guidelines. Kofi Osei, MD
 New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Agenda. Management of Accelerated Hypertension (Updated in 2017) Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 2/27/2017
 Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 2/27/2017") Management of Accelerated Hypertension (Updated in 2017) By Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 Agenda Definition of Accelerated HTN Pathophysiology & Etiology Prognosis
Management of Accelerated Hypertension (Updated in 2017) By Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 Agenda Definition of Accelerated HTN Pathophysiology & Etiology Prognosis
CHALLENGES OF HYPERTENSION IN THE COALFACE
 CHALLENGES OF HYPERTENSION IN THE COALFACE Y VERIAVA CENTRE FOR RURAL HEALTH SCHOOL OF CLINICAL MEDICINE FACULTY OF HEALTH SCIENCES UNIVERSITY OF WITWATERSRAND SYSTOLIC AND DIASTOLIC BLOOD PRESSURES (BP)
CHALLENGES OF HYPERTENSION IN THE COALFACE Y VERIAVA CENTRE FOR RURAL HEALTH SCHOOL OF CLINICAL MEDICINE FACULTY OF HEALTH SCIENCES UNIVERSITY OF WITWATERSRAND SYSTOLIC AND DIASTOLIC BLOOD PRESSURES (BP)
7/6/2012. University Pharmacy 5254 Anthony Wayne Drive Detroit, MI (313)
") University Pharmacy 5254 Anthony Wayne Drive Detroit, MI 48202 (313) 831-2008 Be able to identify the signs of a heart attack or stoke Identify what puts you at a higher risk for cardiovascular disease,
University Pharmacy 5254 Anthony Wayne Drive Detroit, MI 48202 (313) 831-2008 Be able to identify the signs of a heart attack or stoke Identify what puts you at a higher risk for cardiovascular disease,
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Hypertension JNC 8 (2014)
") Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Renal Disease through the Ages: From Childbearing years to Old Age. Dr Elizabeth Jarvis, Renal Physician, General Physician, Obstetric Physician.
 Renal Disease through the Ages: From Childbearing years to Old Age Dr Elizabeth Jarvis, Renal Physician, General Physician, Obstetric Physician. Learning Outcomes: Understand the presentation of renal
Renal Disease through the Ages: From Childbearing years to Old Age Dr Elizabeth Jarvis, Renal Physician, General Physician, Obstetric Physician. Learning Outcomes: Understand the presentation of renal
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension.
 / International Society of Hypertension (ISH) Statement on Management of Hypertension.") 2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL
 CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL Douglas G. Kelling Jr., MD Carmella Gismondi-Eagan, MD, FACP George C. Monroe, III, MD Revised, April 8, 2012 The information contained in this protocol
CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL Douglas G. Kelling Jr., MD Carmella Gismondi-Eagan, MD, FACP George C. Monroe, III, MD Revised, April 8, 2012 The information contained in this protocol
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Dr Doris M. W Kinuthia
 Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
MPharmProgramme. Hypertension (HTN)
") MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
SBP in range of 120 to 140 :no progression or regression of CAD. Sipahi et al., 2006
 Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
HypertensionTreatment Guidelines. Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC
 HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
How Low Do We Go? Update on Hypertension
 How Low Do We Go? Update on Beth L. Abramson, MD, FRCPC, FACC As presented at the University of Toronto s Saturday at the University Session (September 2003) Arecent World Health Organization report states
How Low Do We Go? Update on Beth L. Abramson, MD, FRCPC, FACC As presented at the University of Toronto s Saturday at the University Session (September 2003) Arecent World Health Organization report states
MANAGEMENT OF HYPERTENSION IN EGYPT AND DEVELOPING COUNTRIES
 EGYPTIAN HYPERTENSION SOCIETY GUIDELINES MANAGEMENT OF HYPERTENSION IN EGYPT AND DEVELOPING COUNTRIES 2003 EXECUTIVE SUMMARY PREPARED BY M. MOHSEN IBRAHIM, MD PROFESSOR OF CARDIOLOGY- CAIRO UNIVERSITY
EGYPTIAN HYPERTENSION SOCIETY GUIDELINES MANAGEMENT OF HYPERTENSION IN EGYPT AND DEVELOPING COUNTRIES 2003 EXECUTIVE SUMMARY PREPARED BY M. MOHSEN IBRAHIM, MD PROFESSOR OF CARDIOLOGY- CAIRO UNIVERSITY
ESSENTIAL HYPERTENSION
 E S S E N T I A L H Y P E R T E N S I O N Elevated blood pressure is one of the most important causes of cardiovascular disease. J A Ker MB ChB, MMed, MD Professor and Deputy Dean Faculty of Health Sciences
E S S E N T I A L H Y P E R T E N S I O N Elevated blood pressure is one of the most important causes of cardiovascular disease. J A Ker MB ChB, MMed, MD Professor and Deputy Dean Faculty of Health Sciences
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Categories of HTN. Overview of Hypertension. Types of Hypertension
 Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
CLINICAL GUIDELINE. Document No:CG38 *All Sites Management of adult patients referred to South Tees University Hospitals for hypertension.
 GUIDELINE CLINICAL GUIDELINE Document No:CG38 *All Sites Management of adult patients referred to South Tees University Hospitals for hypertension. TITLE Management of adult patients referred to South
GUIDELINE CLINICAL GUIDELINE Document No:CG38 *All Sites Management of adult patients referred to South Tees University Hospitals for hypertension. TITLE Management of adult patients referred to South
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Essential Hypertension Management Considerations By Elaine Lewis, ND
 Essential Hypertension Management Considerations By Elaine Lewis, ND Elaine Lewis, ND Research Resident, Canadian College of Naturopathic Medicine 1255 Sheppard Avenue East North York, Ontario Back To
Essential Hypertension Management Considerations By Elaine Lewis, ND Elaine Lewis, ND Research Resident, Canadian College of Naturopathic Medicine 1255 Sheppard Avenue East North York, Ontario Back To
Hypertension in the very old. Objectives: Clinical Perspective
 Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
CLINICAL PRACTICE GUIDELINE
 CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
TIP. Documentation and coding guide. Disease definitions* Prevalence and statistics associated with HTN**
 Documentation and coding guide Disease definitions* HTN is diagnosed when the average of two or more (systolic of diastolic) blood pressure readings are found to be elevated on two or more office visits
Documentation and coding guide Disease definitions* HTN is diagnosed when the average of two or more (systolic of diastolic) blood pressure readings are found to be elevated on two or more office visits
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Overview. NOT A REPETION OF LOCAL GUIDELINE Dr Diviash Thakrar
 Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
Hypertension Clinical case scenarios for primary care
 Hypertension Clinical case scenarios for primary care Implementing NICE guidance August 2011 NICE clinical guideline 127 What this presentation covers Five clinical case scenarios, including: presentation
Hypertension Clinical case scenarios for primary care Implementing NICE guidance August 2011 NICE clinical guideline 127 What this presentation covers Five clinical case scenarios, including: presentation
Hypertension and the Challenge of Adherence. Geneva Clark Briggs, Pharm.D., BCPS
 Hypertension and the Challenge of Adherence Geneva Clark Briggs, Pharm.D., BCPS Outline Brief overview of HTN and pharmacologic therapies Role of pharmacists in collaboration with patients and physicians
Hypertension and the Challenge of Adherence Geneva Clark Briggs, Pharm.D., BCPS Outline Brief overview of HTN and pharmacologic therapies Role of pharmacists in collaboration with patients and physicians
Controlling Hypertension in Primary Care: Hitting a moving target?
 Controlling Hypertension in Primary Care: Hitting a moving target? David J. Hyman, MD,MPH Professor of Medicine and Family & Community Medicine Chief, Section General Medicine Baylor College of Medicine
Controlling Hypertension in Primary Care: Hitting a moving target? David J. Hyman, MD,MPH Professor of Medicine and Family & Community Medicine Chief, Section General Medicine Baylor College of Medicine
Dr Narender Goel MD (Internal Medicine and Nephrology) Financial Disclosure: None, Conflict of Interest: None
 Financial Disclosure: None, Conflict of Interest: None") Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups. Lisa Ivy APRN
 Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups Lisa Ivy APRN The 2017 Guideline is an Update to JNC7 New information regarding BP related risk of CVD Ambulatory BP monitoring
Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups Lisa Ivy APRN The 2017 Guideline is an Update to JNC7 New information regarding BP related risk of CVD Ambulatory BP monitoring
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Blood Pressure LIMBO How Low To Go?
 Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Hypertension Management Focus on new RAAS blocker. Disclosure
 Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
2/11/2019 CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES DUALITY OF INTEREST
 CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES George L. Bakris, M.D.,F.A.S.N., F.A.H.A. Professor of Medicine Director, Am Heart Assoc. Comprehensive Hypertension Center University of Chicago Medicine
CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES George L. Bakris, M.D.,F.A.S.N., F.A.H.A. Professor of Medicine Director, Am Heart Assoc. Comprehensive Hypertension Center University of Chicago Medicine
Antihypertensive drugs: I. Thiazide and other diuretics:
 Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Objectives. JNC 7 Is Nice But What s Up With JNC 8? Why Do We Care? Hypertension Background: Prevalence
 JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
What s New? Hypertension Canada Guidelines for the Management of Hypertension
 What s New? 2017 Hypertension Canada Guidelines for the Management of Hypertension What s New? About This Booklet This booklet highlights key advancements and important, enduring aspects of the Hypertension
What s New? 2017 Hypertension Canada Guidelines for the Management of Hypertension What s New? About This Booklet This booklet highlights key advancements and important, enduring aspects of the Hypertension
Clinical Recommendations: Patients with Periodontitis
 The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
Presentation of hypertensive emergency
 Presentation of hypertensive emergency Definitions surrounding hypertensive emergency Hypertension: elevated blood pressure (BP), usually defined as BP >140/90; pathological both in isolation and in association
Presentation of hypertensive emergency Definitions surrounding hypertensive emergency Hypertension: elevated blood pressure (BP), usually defined as BP >140/90; pathological both in isolation and in association
Patrick Kay, General and Interventional Cardiologist Auckland or healthpoint.co.nz
 Patrick Kay, General and Interventional Cardiologist Auckland ipatkay@hotmail.com or healthpoint.co.nz Rotorua 2015 Rotorua 2015 Graphical example of true mean and variation, and of regression to the
Patrick Kay, General and Interventional Cardiologist Auckland ipatkay@hotmail.com or healthpoint.co.nz Rotorua 2015 Rotorua 2015 Graphical example of true mean and variation, and of regression to the
Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study
 Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study Dr. Antonio Magaña M.D. (on behalf I-PREFER investigators group) Stockholm, Sweden, August
Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study Dr. Antonio Magaña M.D. (on behalf I-PREFER investigators group) Stockholm, Sweden, August
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Hypertensive Crises. Controlling high blood pressure prevents disease. Recognition and Management of Acute Hypertensive Emergencies
 Controlling high blood pressure prevents disease Recognition and Management of Acute Hypertensive Emergencies David idweiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Functional Genomics
Controlling high blood pressure prevents disease Recognition and Management of Acute Hypertensive Emergencies David idweiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Functional Genomics