NEONATAL HYBRID PROCEDURES STRATEGIES TO REDUCE MORBIDITY AND MORTALITY
|
|
|
- Olivia Hubbard
- 5 years ago
- Views:
Transcription

1 NEONATAL HYBRID PROCEDURES STRATEGIES TO REDUCE MORBIDITY AND MORTALITY FOTIOS A. MITROPOULOS, MD, PHD DEPARTMENT OF PEDIATRIC AND ADULT CONGENITAL HEART SURGERY MITERA HYGEIA HOSPITALS, ATHENS, GREECE
2 HYBRID PROCEDURES - BACKGROUND 1. CHD is the most common congenital anomaly and cardiac disease is the most common cause of death in infants and children 2. Progress in CHD surgery has increased the pool of complex and multioperated patients 3. Repetitive surgical trauma and bypass may affect the outcome of patients 4. Percutaneous interventions may be associated with an increased risk due to occluded vessels or vascular access small for the purpose, especially in neonates Combining operative and interventional approaches with direct puncture of the heart or the great vessels may facilitate completing the procedure and implanting large devices and stents.
3 HYBRID PROCEDURES 1972: First combined hybrid procedure by Bhati et al 1. Introduced in the settings where routine cardiac surgery or cardiac interventions would not bring satisfactory results 2. Hybrid procedures in children and adults with congenital heart defects combine the experience of cardiac surgery and interventional cardiology as each technique has its own limitations, which could impair the anticipated result 3. Additional alternative option for selected group of borderline patients 4. Hybrid procedures shorten cardiopulmonary bypass, reduce morbidity of surgery and reduce duration of stay in the intensive care unit and the hospital Di Bernardo S. Hybrid procedures in congenital heart disease. Rev Med Suisse. 2008

4 HYBRID PROCEDURES IN NEONATES WITH CONGENITAL HEART DISEASE 1. Premature birth with low birth weight 2. Genetic Syndromes 3. Inability to go on bypass 4. Congenital diaphragmatic hernia
5 HYBRID PROCEDURES 1. Hypoplastic left heart syndrome (Selective RPA and LPA banding + PDA stenting ) 2. RVOT and Branch Pulmonary artery stenting 3. Hybrid transventricular closure of mvsd 4. Hybrid transatrial closure of ASD I 5. Valvuloplasty / valvotomy 6. Hybrid transcatheter valve implantation (Melody or Sapien valves)
6 HYBRID PROCEDURES Single - ventricle circulation in 60% of the procedures 1. Patent ductus arteriosus (PDA) stent placement (n = 55) 2. Vascular rehabilitation (n = 25) 3. Ventricular septal defect (VSD) device closure (n = 7) 4. Valvotomy (n = 3) 5. Diagnostic hybrid procedures (n = 38) Adverse events 1. Arrhythmias (n = 6) 2. Hypoxia or hypotension (n = 3) 3. Vessel or cardiac trauma (n = 2) 4. Other events (n = 5). The incidence of AE related to PDA stent placement with surgical exposure (5/50, 10%) was significantly lower when compared with PDA stent placement performed percutaneously (4/5, 80%, P=.002). Holzer R. Hybrid procedures: adverse events and procedural characteristics: results of a multi-institutional registry. Congenit Heart Dis. 2010
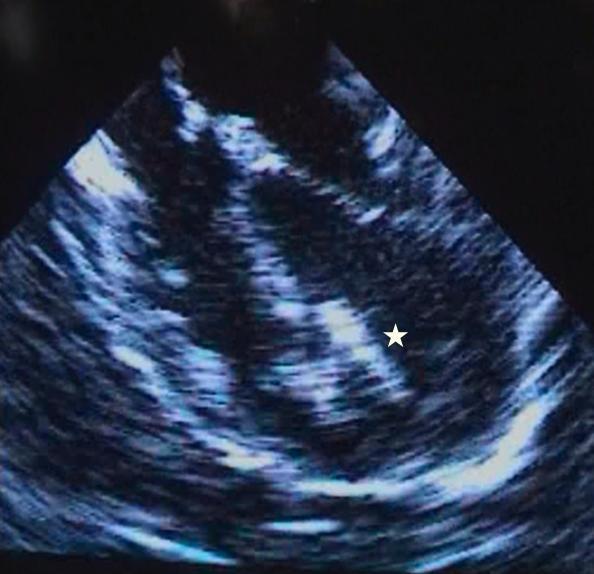
7 HYBRID PROCEDURE FOR HLHS Branch PA banding PDA stenting Atrial septostomy HLHS with INTACT SEPTUM Surgical septectomy F/B PDA stenting and PA banding in cath lab


8 HYBRID PROCEDURE FOR HLHS

9 HYBRID PROCEDURES / HLHS

10 HYBRID PROCEDURE FOR HLHS

11 STAGE II POST INITIAL HYBRID
12 HYBRID APPROACH FOR HLHS Long-term results of biventricular repair after initial Giessen hybrid approach for hypoplastic left heart variants. (2015, Yerebakan et al. J Thorac Cardiovasc Surg 2015;149: ) This article presents the long-term results of our 154 patients with a diagnosis of hypoplastic left heart syndrome (HLHS), hypoplastic left heart complex (HLHC), and variants who received a biventricular repair following hybrid stage I with ductal stenting and bilateral pulmonary artery banding. All patients survived hybrid stage I. Median survival after biventricular correction is 7.9 years. Overall mortality was 10% at 4 weeks, 5 weeks, 6 weeks, and 4 months after biventricular correction, respectively. One patient had to be switched to univentricular circulation and another patient underwent orthotopic heart transplantation 3 and 4 months after biventricular correction, respectively. The Giessen hybrid approach is an alternative to the conventional strategy to treat neonates with HLHS, HLHC, and variants. Biventricular repair after hybrid stage I is feasible and can be performed with satisfactory long-term survival.
13 HYBRID APPROACH TO BPAB Bilateral pulmonary arterial banding results in an increased need for subsequent pulmonary artery interventions. (2014, Davies et al. J Thorac Cardiovasc Surg 2014;147:706-12) ) Despite increasing use of bilateral branch pulmonary artery banding (bpab), both as a temporary stabilizing treatment and as part of comprehensive hybrid management of hypoplastic left heart syndrome, little is known about the long-term outcomes of the pulmonary arteries (PAs) in banded patients. A retrospective review of all patients with ductal-dependent systemic circulation ( ) undergoing bpab placement at a single institution (bpab, n = 50); patients who underwent a stage I Norwood procedure were used for comparison. The need for PA interventions (surgical arterioplasty, balloon angioplasty, and stent implantation) and PA growth were assessed. CONCLUSIONS: Patients with bpab require additional interventions at earlier time points than Norwood patients. Patients with smaller bands and longer duration of banding are at high risk. Despite stenoses requiring additional interventions, Fontan candidacy is maintained.
14 BRANCH PULMONARY ARTERY STENTING AND RVOT STENTING
15 HYBRID PROCEDURES FOR PA STENOSIS / OCCLUSION Pulmonary venous wedge angiograms are used to delineate the distal PA anatomy and serve to guide the recanalization process. Creation of a track is performed with small diameter balloons after passage of a or guide wire Establishment of a vessel lumen is achieved with the placement of premounted stents.

16 LPA occlusion: recanalization post Fallot repair with Contegra conduit. HYBRID APPROACH

17 Occluded LPA in Fallot with pulmonary atresia post RtBTS and LPA patch augmentation. LPA recanalization through BT shunt. PERCUTANEOUS APPROACH

18 LPA stenting: Small diameter stents HYBRID APPROACH LPA stenting Large diameter stents
19 HYBRID APPROACH FOR RVOT Perforation and right ventricular outflow tract stenting: Alternative palliation for infants with pulmonary atresia/ventricular septal defect. ( 2018, Aurigemma et al.) RVOT stenting in conjunction with radiofrequency perforation as a means for establishing reliable pulmonary blood flow in patients with PA/VSD has not previously been reported. The aim is to report experience with using perforation of plate-like pulmonary valve atresia combined with stenting of RVOT as an alternative and equally efficacious intervention for infants with PA/VSD, as compared to a surgical pulmonary artery shunt (SPS). Twenty-seven patients received palliation for PA/VSD. Five underwent RVOT stenting and 22 underwent surgical SPS. Of the patients who received an RVOT stent, 3 underwent guidewire perforation and balloon dilation of the plate-like pulmonary valve, and 2 underwent radiofrequency perforation of the pulmonary plate, followed by balloon dilation. Post procedure saturations averaged 93% in the stent group and 89% in the shunt group. One of the patients who underwent RVOT stenting required additional stenting of the PDA for isolation of the LPA, but none required re-intervention. Four patients in the SPS cohort required re-intervention (18%). Two required stenting of the shunt, and 2 required surgical revision of the shunt. There was one death in the stent group, however this was secondary to withdrawal of support given an underlying genetic diagnosis (trisomy 13). There was one fatality in the SPS cohort prior to hospital discharge. CONCLUSIONS: Perforation followed by RVOT stenting may be a safe and effective alternative to surgical SPS in infants with PA/VSD.
20 HYBRID APPROACH FOR RVOT Hybrid approach for pulmonary atresia with intact ventricular septum: early single center results and comparison to the standard surgical approach. (2014, Zampi et al.) A subset of PA-IVS patients with the prospect of biventricular circulation typically undergo surgical or transcatheter right ventricular (RV) outflow tract opening. A recently described hybrid procedure, involving perventricular pulmonary valve perforation, was shown to be safe and effective in single-center series. Seven patients with PA-IVS underwent a hybrid procedure; the procedure was technically successful in all attempts, and none required CPB. No patients required surgical re-intervention prior to hospital discharge, and none died during the study period. Surgical RV decompression was performed in 17 patients with a median CPB time of 80 min. Patient outcomes were nearly identical between cohorts. By systematic review, the transcatheter approach has a procedural success of 75-95% but up to 75% of patients require operation in the neonatal period. The hybrid approach is a safe and feasible alternative to the standard surgical and transcatheter approaches to PA-IVS. Acute and mid-term patient outcomes are comparable with those treated with a standard surgical approach and neonatal CPB is completely avoided.
21 HYBRID APPROACH FOR RVOT Evolution of Approach to Right Ventricular Outflow Tract Stenting in Infants 2Kgs (2018,Niall Linnane et al.) Surgical palliation or repair of symptomatic Tetralogy of Fallot in the neonatal period is associated with a relatively high mortality rate. Stenting of the right ventricular outflow tract is a newer procedure that has evolved to allow its performance in low birth weight neonates. Although a successful outcome with a transcutaneous approach is possible, complications may occur and are poorly tolerated. A hybrid approach provides the most direct route to the RVOT with the least hemodynamic instability, providing concurrent angiography through the delivery sheath to facilitate optimal stent position. This small case series may not provide sufficient experience to support a perventricular approach as first-line for all infants 2 kg requiring RVOT stenting. However, early conversion to this approach should be considered in those infants who do not tolerate attempts at percutaneous stent delivery.
22 HYBRID TRANSCATHETER VALVE IMPLANTATION
23
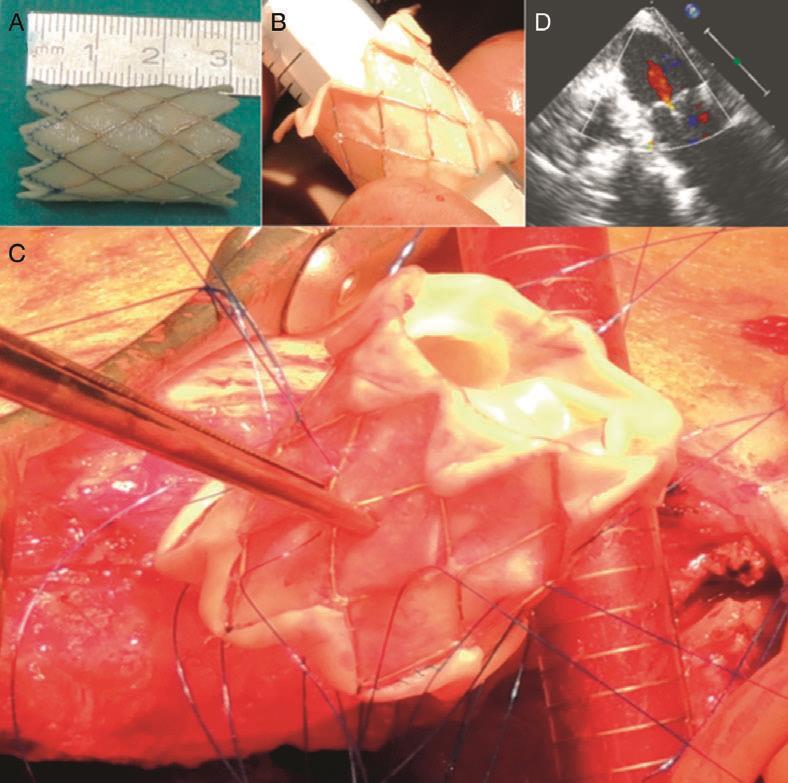
24 HYBRID APPROACH TO MITRAL VALVE REPAIR MELODY VALVE Pediatric Melody mitral valve replacement in acute endocarditis alternative surgical-hybrid technique (2017, Haponiuk et al.) Background: Emergency mitral valve replacement with the use of Melody balloon expandable stented bioprosthesis in a two-year-old patient with AE and subsequent mitral (bicuspid) valve incompetence after aggressive infective destruction with the symptoms of critical multi-organ failure. Results: The patient, with a history of rapid deterioration after two-week-long septicaemia in the course of AE, was operated urgently after initial antibiotic treatment because of huge vegetations into the mitral valve orifice. A Melody TVP 22 valve was expanded over a 16-mm TyShak balloon and implanted into a mitral position (Melody-MVR) with good result. Conclusions: Infected mitral valve in children should be primarily repaired; nevertheless, the Melody valve could be reasonably considered as a mitral prosthesis in such conditions.
25
26
27

28 Courtesy G Butera, Milan

29 Courtesy G Butera, Milan

30 Courtesy G Butera, Milan
31 Courtesy G Butera, Milan

32 Courtesy G Butera, Milan

33 Courtesy G Butera, Milan
34 Courtesy G Butera, Milan
35
36
37 HYBRID APPROACH FOR NEONATAL AORTIC STENOSIS Hybrid balloon valvuloplasty through the ascending aorta via median sternotomy in infants with severe congenital valvular aortic stenosis: feasibility of a new method. (2015, Pan et al.) Eighteen infants (<90 days of age) with severe congenital aortic stenosis were included in this study. Hybrid balloon valvuloplasty procedures were performed in a hybrid operating room. Patients were followed up at 3 months, 6 months, 1 year and then annually following the procedure. The hybrid balloon valvuloplasty procedure was successful in all patients. Eight patients were successfully rescued from left ventricular systolic dysfunction by cardiac compression under direct vision. The aortic valve pressure gradient decreased from 80.3 ± 20.8 mmhg preoperatively to 16.0 ± 3.6 mmhg immediately postoperatively (P < 0.001). None of the patients developed significant aortic insufficiency. The fluoroscopy time was 6.2 ± 2.9 min. Intraoperative blood transfusions and pacing were not required. The patients were all alive and healthy at the end of the follow-up period (mean 21.3 months; range 3-41 months), and the aortic valve pressure gradient remained low (21.7 ± 5.3 mmhg). Reintervention was not required in any of the patients. CONCLUSIONS: Hybrid balloon valvuloplasty through the ascending aorta via median sternotomy is an effective and safe procedure for infants with severe congenital aortic stenosis.
38 HYBRID APPROACH FOR NEONATAL AORTIC STENOSIS Hybrid approach as bridge to biventricular repair in a neonate with critical aortic stenosis and borderline left ventricle. (2009, Brown et al.) A newborn presented with severe aortic valve stenosis and a borderline hypoplastic left ventricle due to disproportionate left ventricular hypertrophy (maternal diabetes). The aortic valve was balloon dilated and the infant tolerated a biventricular circulation. However, severe retrograde pulmonary hypertension and mitral regurgitation developed, indicating that biventricular circulation was not possible at that stage. A hybrid approach with ductal stenting, atrial septostomy and bilateral dilatable pulmonary artery band placement was followed on day 25. This allowed the left ventricle several months to adapt to lower pressure and normoglycemic conditions. At re-evaluation after 8 months biventricular repair appeared possible: the ductus was closed with Amplatzer occluders and the pulmonary artery bands were opened up with bilateral balloon angioplasty of the dilatable bands. At the age of 3 years, the infant is doing well with a biventricular circulation and normal pulmonary artery pressure. The hybrid approach allowed adequate time (months) for careful consideration and acted as a bridge to biventricular repair in this infant.
39 HYBRID APPROACH FOR NEONATAL AORTIC STENOSIS Severe Aortic Stenosis and Severe Coarctation of the Aorta: A Hybrid Approach to Treatment. (2017, McLennan et al.) Here is a case of a patient with aortic stenosis (AS) and coarctation of the aorta (CoA). Case: a 1-month-old baby presented with severe AS and CoA. The decision was made to perform a hybrid surgical procedure. The patient underwent a lateral thoracotomy for repair of the CoA and carotid cutdown for aortic balloon valvuloplasty (Above). Optimal treatment has long been difficult to achieve. Using a hybrid technique by performing AoVP, surgical resection, and end-to-end anastomosis, the best treatment option for each lesion was provided. Known procedure-related complications were avoided with the use of surgical carotid cutdown. Long-term risks of neurological and developmental impairment were reduced with the avoidance of cardiac bypass and DHCA.
40 HYBRID APPROACH FOR VSD CLOSURE Hybrid approach for closure of muscular ventricular septal defects (2013, Haponiuk et al.) Background: Hybrid therapies aim to combine the advantages of surgical and interventional techniques in an effort to reduce the invasiveness. The aim of this study was to present an approach with mvsd patients and initial results in the development of a mini-invasive hybrid procedure. Results: The implants of choice were Amplatzer VSD Occluder and Amplatzer Duct Occluder II (AGA Med. Corp, USA). The position of the implants was checked carefully before releasing the device with both transesophageal echocardiography and epicardial echocardiography. All patients survived and their general condition improved. No complications occurred. The closure of mvsd was complete in all children. Conclusions: Hybrid procedures of periventricular muscular VSD closure appear feasible and effective for patients with septal defects with morphology unsuitable for classic surgical or interventional procedures. The modern strategy of joint cardiac surgical and interventional techniques provides the benefits of close cooperation between cardiac surgeon and interventional cardiologist for selected patients in difficult clinical settings.
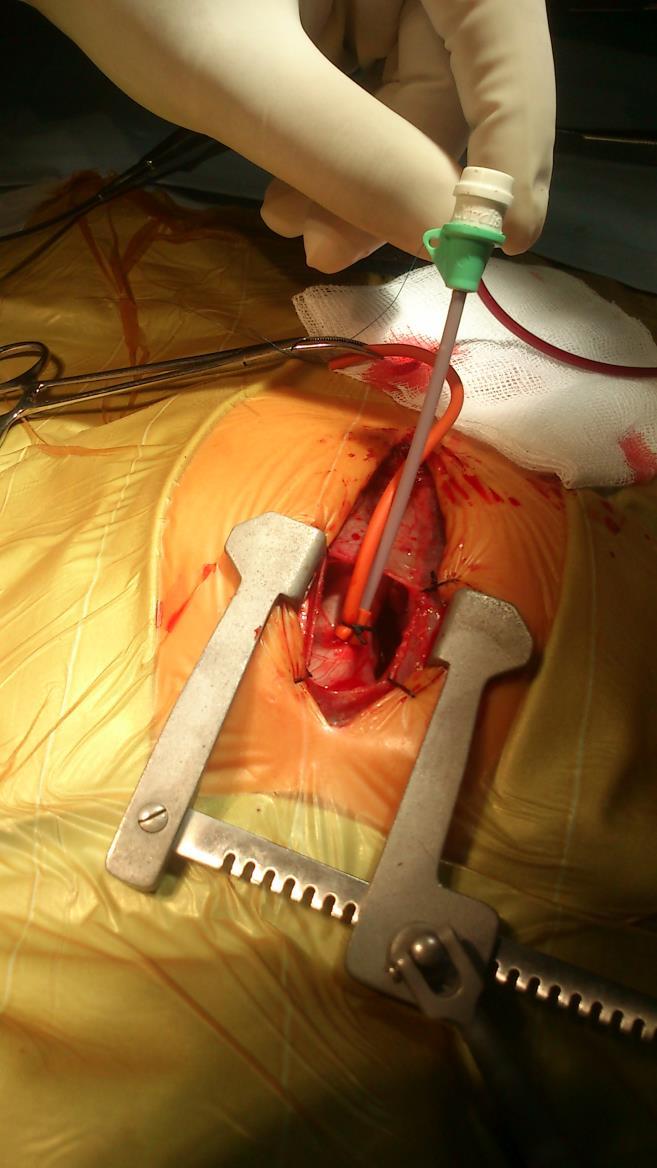
41 HYBRID VSD CLOSURE 2 patients 4 and 6 months of age Sizeable muscular ventricular septal defect Median sternotomy, off-pump Intraoperative device closure with the use of an Amplatzer occluding device Right perventricular approach Intraoperative TOE

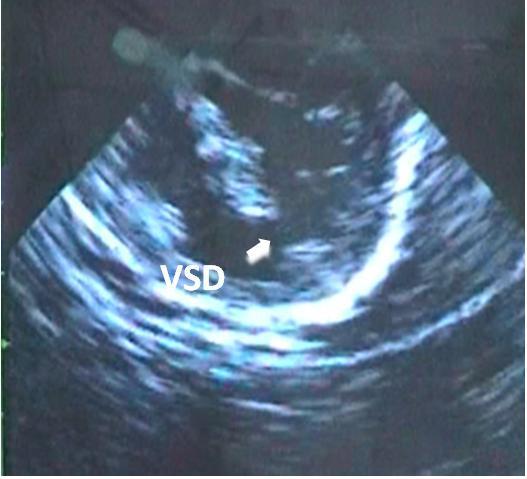
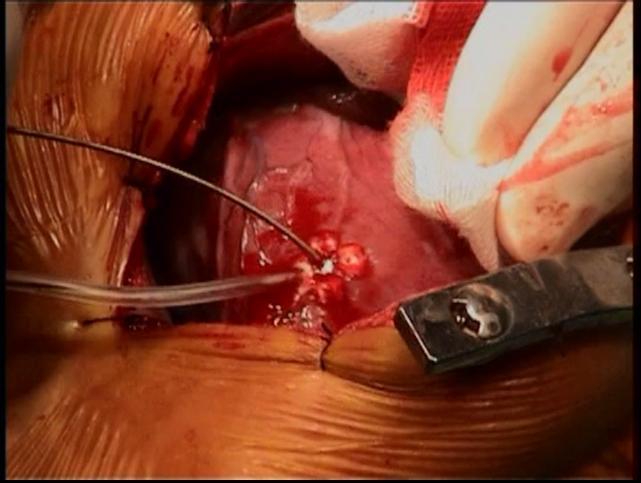
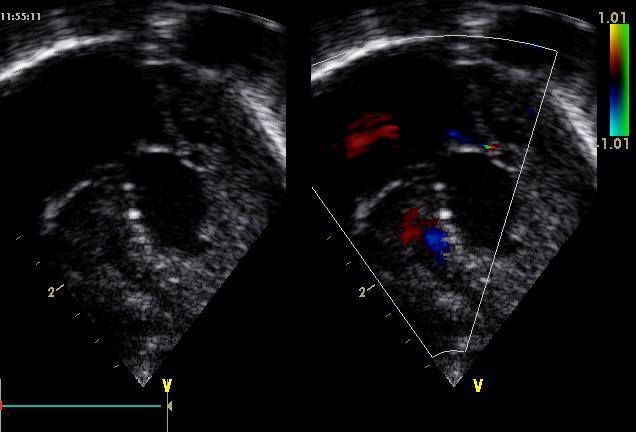
42 VSD DEVICE CLOSURE
43 RESULTS No Intraoperative death or postoperative complication ICU stay: 1 and 2 days respectively Hospital stay: 5 and 10 days respectively Echo prior to discharge: no residual VSD At 48 and 56 months of follow-up: intact ventricular septum both patients are asymptomatic
44 Acute and midterm results following perventricular device closure of muscular ventricular septal defects: A multicenter PICES investigation. Gray RG 1, Menon SC 1, Johnson JT 2, Armstrong AK 3, Bingler MA 4, Breinholt JP 5, Kenny D 6, Lozier J 7, Murphy JJ 8, Sathanandam SK 9, Taggart NW 10, Trucco SM 11, Goldstein BH 12, Gordon BM 13. Catheter Cardiovasc Interv Aug 1;90(2): This is a multicenter retrospective cohort study of patients undergoing hybrid perventricular mvsd device closure from 1/2004 to 1/2014. Procedural details, adverse events, outcomes, and follow-up data were collected. Patients were divided into two groups: (1) simple (mvsd closure alone) and (2) complex (mvsd closure with concomitant cardiac surgery). RESULTS: Forty-seven patients (60% female) underwent perventricular mvsd device closure at a median age of 5.2 months (IQR ) and weight of 5.1 kg (IQR ). Procedural success was 91% [100% (n = 22) simple and 84% (n = 21/25) complex]. Adverse events occurred in 19% (9/47) [9% (2/22) simple and 28% (7/25) complex]. Hospital length of stay (LOS) was shorter in the simple vs. complex group (4 vs. 14 days, P < 0.01). At mid-term follow-up of 19.2 months (IQR ) 90% of pts had complete mvsd closure; none developed late heart block, increased atrioventricular (AV) valve insufficiency or ventricular dysfunction. CONCLUSIONS: Perventricular device closure of simple mvsd was associated with a high rate of procedural success, few adverse events, and short hospital LOS. Procedural adverse events were associated with the presence of concomitant complex surgery. Residual mvsd, AV valve insufficiency, or ventricular dysfunction were uncommon at mid-term follow-up.


45 VSD closure HYBRID APPROACH
46 A novel hybrid technique for transcatheter pulmonary valve implantation within a dilated native right ventricular outflow tract Frances C. Travelli, MD, Cynthia S. Herrington, MD, Frank F. Ing, MD The Journal of Thoracic and Cardiovascular Surgery Volume 148, Issue 2, Pages e145-e146 (August 2014) DOI: /j.jtcvs



47 HYBRID IMPLANTATION OF PULMONARY VALVE IN EXTREMELY DILATED RV / MPA WITH POOR FUNCTION Dittrich S et al. Annals Thoracic Surgery 2008


48 Figure 1 The Journal of Thoracic and Cardiovascular Surgery , e145-e146doi: ( /j.jtcvs )

49 Figure 2 The Journal of Thoracic and Cardiovascular Surgery , e145-e146doi


50 Hybrid pulmonary artery plication followed by transcatheter pulmonary valve replacement: Comparison with surgical PVR Sosnowski C. Catheter Cardiovasc Interv 2016 Hybrid PV implantation due to occluded vessels

51 29-MM EDWARDS SAPIEN XT PROSTHESIS WITHIN AN ANDRAMED AS43XXL STENT IMPLANTED IN THE PULMONARY POSITION Rapetto F et al. Hybrid Surgery Options for Complex Clinical Scenarios in Adult Patients with Congenital Heart Disease, 2017
52 CONCLUSIONS As disease complexity and patient pathology are increasing, the neonatal population suitable for hybrid procedures broadens Hybrid procedures allow Surgeons and Cardiologists to achieve complex procedures that would not be possible in another way. In some case the combined approach might reduce the total number of interventions Possible Reduction total hospital stay, morbidity, mortality and cost
Introduction. Study Design. Background. Operative Procedure-I
 Risk Factors for Mortality After the Norwood Procedure Using Right Ventricle to Pulmonary Artery Shunt Ann Thorac Surg 2009;87:178 86 86 Addressor: R1 胡祐寧 2009/3/4 AM7:30 SICU 討論室 Introduction Hypoplastic
Risk Factors for Mortality After the Norwood Procedure Using Right Ventricle to Pulmonary Artery Shunt Ann Thorac Surg 2009;87:178 86 86 Addressor: R1 胡祐寧 2009/3/4 AM7:30 SICU 討論室 Introduction Hypoplastic
Surgical options for tetralogy of Fallot
 Surgical options for tetralogy of Fallot Serban Stoica FRCS(CTh) MD ACHD study day, 19 September 2017 Anatomy Physiology Children Adults Complications Follow up Anatomy Etienne Fallot (1850-1911) VSD Overriding
Surgical options for tetralogy of Fallot Serban Stoica FRCS(CTh) MD ACHD study day, 19 September 2017 Anatomy Physiology Children Adults Complications Follow up Anatomy Etienne Fallot (1850-1911) VSD Overriding
Perventricular Closure of Muscular VSD s
 Perventricular Closure of Muscular VSD s Dr Damien Kenny, MB, MD Assistant Professor of Pediatrics Director of the Cardiac Catheterization Hybrid Suite Co-Director of the Rush Adult Congenital Heart Disease
Perventricular Closure of Muscular VSD s Dr Damien Kenny, MB, MD Assistant Professor of Pediatrics Director of the Cardiac Catheterization Hybrid Suite Co-Director of the Rush Adult Congenital Heart Disease
CONGENITAL HEART DEFECTS IN ADULTS
 CONGENITAL HEART DEFECTS IN ADULTS THE ROLE OF CATHETER INTERVENTIONS Mario Carminati CONGENITAL HEART DEFECTS IN ADULTS CHD in natural history CHD with post-surgical sequelae PULMONARY VALVE STENOSIS
CONGENITAL HEART DEFECTS IN ADULTS THE ROLE OF CATHETER INTERVENTIONS Mario Carminati CONGENITAL HEART DEFECTS IN ADULTS CHD in natural history CHD with post-surgical sequelae PULMONARY VALVE STENOSIS
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Hybrid Therapy for Hypoplastic Left Heart Syndrome Myth, Alternative or Standard?
 Hybrid Therapy for Hypoplastic Left Heart Syndrome Myth, Alternative or Standard? Can Yerebakan, Klaus Valeske, Hatem Elmontaser, Matthias Mueller, Juergen Bauer, Josef Thul, Dietmar Schranz, Hakan Akintuerk
Hybrid Therapy for Hypoplastic Left Heart Syndrome Myth, Alternative or Standard? Can Yerebakan, Klaus Valeske, Hatem Elmontaser, Matthias Mueller, Juergen Bauer, Josef Thul, Dietmar Schranz, Hakan Akintuerk
LEFT VENTRICULAR OUTFLOW OBSTRUCTION WITH A VSD: OPTIONS FOR SURGICAL MANAGEMENT
 LEFT VENTRICULAR OUTFLOW OBSTRUCTION WITH A VSD: OPTIONS FOR SURGICAL MANAGEMENT 10-13 March 2017 Ritz Carlton, Riyadh, Saudi Arabia Zohair AlHalees, MD Consultant, Cardiac Surgery Heart Centre LEFT VENTRICULAR
LEFT VENTRICULAR OUTFLOW OBSTRUCTION WITH A VSD: OPTIONS FOR SURGICAL MANAGEMENT 10-13 March 2017 Ritz Carlton, Riyadh, Saudi Arabia Zohair AlHalees, MD Consultant, Cardiac Surgery Heart Centre LEFT VENTRICULAR
Hybrid Muscular VSD Closure in Small Weight Children
 Hybrid Muscular VSD Closure in Small Weight Children Shakeel A Qureshi, on behalf of: John P. Cheatham, MD George H. Dunlap Endowed Chair in Interventional Cardiology Director Cardiac Catheterization &
Hybrid Muscular VSD Closure in Small Weight Children Shakeel A Qureshi, on behalf of: John P. Cheatham, MD George H. Dunlap Endowed Chair in Interventional Cardiology Director Cardiac Catheterization &
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
Hybrid Stage I Palliation / Bilateral PAB
 Hybrid Stage I Palliation / Bilateral PAB Jeong-Jun Park Dept. of Thoracic & Cardiovascular Surgery Asan Medical Center, University of Ulsan CASE 1 week old neonate with HLHS GA 38 weeks Birth weight 3.0Kg
Hybrid Stage I Palliation / Bilateral PAB Jeong-Jun Park Dept. of Thoracic & Cardiovascular Surgery Asan Medical Center, University of Ulsan CASE 1 week old neonate with HLHS GA 38 weeks Birth weight 3.0Kg
Foetal Cardiology: How to predict perinatal problems. Prof. I.Witters Prof.M.Gewillig UZ Leuven
 Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Perimembranous VSD: When Do We Ask For A Surgical Closure? LI Xin. Department of Cardiothoracic Surgery Queen Mary Hospital Hong Kong
 Perimembranous VSD: When Do We Ask For A Surgical Closure? LI Xin Department of Cardiothoracic Surgery Queen Mary Hospital Hong Kong Classification (by Kirklin) I. Subarterial (10%) Outlet, conal, supracristal,
Perimembranous VSD: When Do We Ask For A Surgical Closure? LI Xin Department of Cardiothoracic Surgery Queen Mary Hospital Hong Kong Classification (by Kirklin) I. Subarterial (10%) Outlet, conal, supracristal,
The complications of cardiac surgery:
 The complications of cardiac surgery: a walk on the Dark Side? Prof Rik De Decker Red Cross Children s Hospital CME Nov/Dec 2011 http://www.cmej.org.za Why should you care? You are about to leave your
The complications of cardiac surgery: a walk on the Dark Side? Prof Rik De Decker Red Cross Children s Hospital CME Nov/Dec 2011 http://www.cmej.org.za Why should you care? You are about to leave your
Index. interventional.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Alagille syndrome, pulmonary artery stenosis in, 143 145, 148 149 Amplatz devices for atrial septal defect closure, 42 46 for coronary
Index Note: Page numbers of article titles are in boldface type. A Alagille syndrome, pulmonary artery stenosis in, 143 145, 148 149 Amplatz devices for atrial septal defect closure, 42 46 for coronary
Children with Single Ventricle Physiology: The Possibilities
 Children with Single Ventricle Physiology: The Possibilities William I. Douglas, M.D. Pediatric Cardiovascular Surgery Children s Memorial Hermann Hospital The University of Texas Health Science Center
Children with Single Ventricle Physiology: The Possibilities William I. Douglas, M.D. Pediatric Cardiovascular Surgery Children s Memorial Hermann Hospital The University of Texas Health Science Center
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
For Personal Use. Copyright HMP 2013
 12-00415 Case Report J INVASIVE CARDIOL 2013;25(4):E69-E71 A Concert in the Heart. Bilateral Melody Valve Implantation in the Branch Pulmonary Arteries Nicola Maschietto, MD, PhD and Ornella Milanesi,
12-00415 Case Report J INVASIVE CARDIOL 2013;25(4):E69-E71 A Concert in the Heart. Bilateral Melody Valve Implantation in the Branch Pulmonary Arteries Nicola Maschietto, MD, PhD and Ornella Milanesi,
Outline. Congenital Heart Disease. Special Considerations for Special Populations: Congenital Heart Disease
 Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE
 SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
Transcather Pulmonary Valve Replacement Using The Melody Valve: Indications, Techniques, Outcomes
 Transcather Pulmonary Valve Replacement Using The Melody Valve: Indications, Techniques, Outcomes Matthew J. Gillespie MD The Children s Hospital of Philadelphia SCAI Fall Fellows Course 2014 December
Transcather Pulmonary Valve Replacement Using The Melody Valve: Indications, Techniques, Outcomes Matthew J. Gillespie MD The Children s Hospital of Philadelphia SCAI Fall Fellows Course 2014 December
9/8/2009 < 1 1,2 3,4 5,6 7,8 9,10 11,12 13,14 15,16 17,18 > 18. Tetralogy of Fallot. Complex Congenital Heart Disease.
 Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
What is the Definition of Small Systemic Ventricle. Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University
 What is the Definition of Small Systemic Ventricle Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University Contents Introduction Aortic valve stenosis Aortic coarctation
What is the Definition of Small Systemic Ventricle Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University Contents Introduction Aortic valve stenosis Aortic coarctation
Congenital heart disease: When to act and what to do?
 Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment
 Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
INTEGRATING ECHOCARDIOGRAPHY WITH CATHETER INTERVENTIONS FOR CONGENITAL HEART DISEASE. Krishna Kumar SevenHills Hospital, Mumbai, India
 INTEGRATING ECHOCARDIOGRAPHY WITH CATHETER INTERVENTIONS FOR CONGENITAL HEART DISEASE Krishna Kumar SevenHills Hospital, Mumbai, India Why talk about it? What is the big deal? Are we not stating the obvious?
INTEGRATING ECHOCARDIOGRAPHY WITH CATHETER INTERVENTIONS FOR CONGENITAL HEART DISEASE Krishna Kumar SevenHills Hospital, Mumbai, India Why talk about it? What is the big deal? Are we not stating the obvious?
Atrial Septostomy in HLHS and ECMO: Indications, Technique and Outcome
 Atrial Septostomy in HLHS and ECMO: Indications, Technique and Outcome Dr Damien Kenny, MB, MD Assistant Professor of Pediatrics Director of the Cardiac Catheterization Hybrid Suite Co-Director of the
Atrial Septostomy in HLHS and ECMO: Indications, Technique and Outcome Dr Damien Kenny, MB, MD Assistant Professor of Pediatrics Director of the Cardiac Catheterization Hybrid Suite Co-Director of the
Down Syndrome Medical Interest Group Friday, 12 June Cardiac Surgery in patients with Down Syndrome
 Down Syndrome Medical Interest Group Friday, 12 June 2015 Cardiac Surgery in patients with Down Syndrome Mr. Attilio Lotto, FRCS CTh Congenital Cardiac Surgeon Cardiac surgery in patients with Down syndrome
Down Syndrome Medical Interest Group Friday, 12 June 2015 Cardiac Surgery in patients with Down Syndrome Mr. Attilio Lotto, FRCS CTh Congenital Cardiac Surgeon Cardiac surgery in patients with Down syndrome
Paediatrics Revision Session Cardiology. Emma Walker 7 th May 2016
 Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
PULMONARY ARTERY STENTING AFfER TOTAL SURGICAL CORRECTION OF RIGHT VENTRICULAR OUTFLOW TRACT OBSTRUCTIVE LESIONS
 Articles 5 PULMONARY ARTERY STENTING AFfER TOTAL SURGICAL CORRECTION OF RIGHT VENTRICULAR OUTFLOW TRACT OBSTRUCTIVE LESIONS SAMEH ARAB, MD; ERIC ROSENTHAL, MD, MRCP; SHAKEEL QURESHI, MB, MRCP; MICHAEL
Articles 5 PULMONARY ARTERY STENTING AFfER TOTAL SURGICAL CORRECTION OF RIGHT VENTRICULAR OUTFLOW TRACT OBSTRUCTIVE LESIONS SAMEH ARAB, MD; ERIC ROSENTHAL, MD, MRCP; SHAKEEL QURESHI, MB, MRCP; MICHAEL
Adults with Congenital Heart Disease. Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP
 Adults with Congenital Heart Disease Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP Outline History of CHD Statistics Specific lesions (TOF, TGA, Single ventricle) Erythrocytosis Pregnancy History
Adults with Congenital Heart Disease Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP Outline History of CHD Statistics Specific lesions (TOF, TGA, Single ventricle) Erythrocytosis Pregnancy History
Intraoperative Stents to Rehabilitate Severely Stenotic Pulmonary Vessels
 Intraoperative Stents to Rehabilitate Severely Stenotic Pulmonary Vessels Ross M. Ungerleider, MD, Troy A. Johnston, MD, Martin P. O Laughlin, MD, James J. Jaggers, MD, and Peter R. Gaskin, MD Division
Intraoperative Stents to Rehabilitate Severely Stenotic Pulmonary Vessels Ross M. Ungerleider, MD, Troy A. Johnston, MD, Martin P. O Laughlin, MD, James J. Jaggers, MD, and Peter R. Gaskin, MD Division
TRANSCATHETER REPLACEMENT OF THE PULMONARY VALVE (PPVI)
") TRANSCATHETER REPLACEMENT OF THE PULMONARY VALVE (PPVI) BASIL D. THANOPOULOS MD, PhD Director Interventional Cardiology of CHD Euroclinic ATHENS - GREECE TRANSCATHETER REPLACEMENT OF THE PULMONARY VALVE
TRANSCATHETER REPLACEMENT OF THE PULMONARY VALVE (PPVI) BASIL D. THANOPOULOS MD, PhD Director Interventional Cardiology of CHD Euroclinic ATHENS - GREECE TRANSCATHETER REPLACEMENT OF THE PULMONARY VALVE
Index. interventional.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Ablation, of mitral leaflets, 80 Accucinch Annuloplasty system, for mitral regurgitation, 79, 94 95 Accutrak delivery system, for CoreValve
Index Note: Page numbers of article titles are in boldface type. A Ablation, of mitral leaflets, 80 Accucinch Annuloplasty system, for mitral regurgitation, 79, 94 95 Accutrak delivery system, for CoreValve
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
7th Congress of the Asia-Pacific Pediatric Cardiac Society
 7th Congress of APPCS Wednesday, August 29, 2018 Thursday, August 30, 2018 Time Counter Ballroom 1 Ballroom 2 Ballroom 3 Junior Ballroom 2 Room 1 Room 2 Prefunction Area Level 1 07:00-07:30 08:00-20:00
7th Congress of APPCS Wednesday, August 29, 2018 Thursday, August 30, 2018 Time Counter Ballroom 1 Ballroom 2 Ballroom 3 Junior Ballroom 2 Room 1 Room 2 Prefunction Area Level 1 07:00-07:30 08:00-20:00
The Double Switch Using Bidirectional Glenn and Hemi-Mustard. Frank Hanley
 The Double Switch Using Bidirectional Glenn and Hemi-Mustard Frank Hanley No relationships to disclose CCTGA Interesting Points for Discussion What to do when. associated defects must be addressed surgically:
The Double Switch Using Bidirectional Glenn and Hemi-Mustard Frank Hanley No relationships to disclose CCTGA Interesting Points for Discussion What to do when. associated defects must be addressed surgically:
CMR for Congenital Heart Disease
 CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
CARDIAC INTERVENTIONS IN PEDIATRIC CARDIOLOGY: THE FUTURE
 CARDIAC INTERVENTIONS IN PEDIATRIC CARDIOLOGY: THE FUTURE Vikas Kohli From the: Senior Consultant Pediatric Cardiology, Apollo Centre of Advance Pediatrics, Indraprastha Apollo Hospitals, New Delhi-110044.
CARDIAC INTERVENTIONS IN PEDIATRIC CARDIOLOGY: THE FUTURE Vikas Kohli From the: Senior Consultant Pediatric Cardiology, Apollo Centre of Advance Pediatrics, Indraprastha Apollo Hospitals, New Delhi-110044.
Perventricular Closure of Muscular VSD
 Perventricular Closure of Muscular VSD John P. Cheatham, MD, MSCAI George H. Dunlap Endowed Chair in Interventional Cardiology Co-Director, The Heart Center, Nationwide Children s Hospital Professor, Pediatrics
Perventricular Closure of Muscular VSD John P. Cheatham, MD, MSCAI George H. Dunlap Endowed Chair in Interventional Cardiology Co-Director, The Heart Center, Nationwide Children s Hospital Professor, Pediatrics
Hemodynamic assessment after palliative surgery
 THERAPY AND PREVENTION CONGENITAL HEART DISEASE Hemodynamic assessment after palliative surgery for hypoplastic left heart syndrome PETER LANG, M.D., AND WILLIAM I. NORWOOD, M.D., PH.D. ABSTRACT Ten patients
THERAPY AND PREVENTION CONGENITAL HEART DISEASE Hemodynamic assessment after palliative surgery for hypoplastic left heart syndrome PETER LANG, M.D., AND WILLIAM I. NORWOOD, M.D., PH.D. ABSTRACT Ten patients
Tetralogy of Fallot Latest data in risk stratification and replacement of pulmonic valve
 Tetralogy of Fallot Latest data in risk stratification and replacement of pulmonic valve Alexandra A Frogoudaki Adult Congenital Heart Clinic Second Cardiology Department ATTIKON University Hospital No
Tetralogy of Fallot Latest data in risk stratification and replacement of pulmonic valve Alexandra A Frogoudaki Adult Congenital Heart Clinic Second Cardiology Department ATTIKON University Hospital No
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Outcomes Associated with the Off-label Use of Medical Devices in Congenital Heart Disease at a Single Institute
 Original Article Print ISSN 1738-5520 On-line ISSN 1738-5555 Korean Circulation Journal Outcomes Associated with the Off-label Use of Medical Devices in Congenital Heart Disease at a Single Institute Young
Original Article Print ISSN 1738-5520 On-line ISSN 1738-5555 Korean Circulation Journal Outcomes Associated with the Off-label Use of Medical Devices in Congenital Heart Disease at a Single Institute Young
Native valve, Conduit stenosis or leakage? How can the interventionalist help?
 Complications in Congenital Heart Diseases -with a little help of our friends Native valve, Conduit stenosis or leakage? How can the interventionalist help? P. Ewert German Heart Center Munich Lausanne
Complications in Congenital Heart Diseases -with a little help of our friends Native valve, Conduit stenosis or leakage? How can the interventionalist help? P. Ewert German Heart Center Munich Lausanne
Deborah Kozik, DO Assistant Professor Division of Cardiothoracic Surgery s present: Early Repair Era
 Deborah Kozik, DO Assistant Professor Division of Cardiothoracic Surgery 1954 1960: Experimental Era 1960 s 1980 s: Palliation Era 1980 s present: Early Repair Era 2010 2030 s: Fetal Interventions Hybrid
Deborah Kozik, DO Assistant Professor Division of Cardiothoracic Surgery 1954 1960: Experimental Era 1960 s 1980 s: Palliation Era 1980 s present: Early Repair Era 2010 2030 s: Fetal Interventions Hybrid
"Giancarlo Rastelli Lecture"
 "Giancarlo Rastelli Lecture" Surgical treatment of Malpositions of the Great Arteries Pascal Vouhé Giancarlo Rastelli (1933 1970) Cliquez pour modifier les styles du texte du masque Deuxième niveau Troisième
"Giancarlo Rastelli Lecture" Surgical treatment of Malpositions of the Great Arteries Pascal Vouhé Giancarlo Rastelli (1933 1970) Cliquez pour modifier les styles du texte du masque Deuxième niveau Troisième
Risk Factors in ACHD Redo Surgery: Strategies to Optimize Outcomes
 Risk Factors in ACHD Redo Surgery: Strategies to Optimize Outcomes David N. Campbell MD Professor of CV Surgery University of Colorado, Denver Children s Hospital Colorado ACHD 2017 Symposium, Nov 30-Dec
Risk Factors in ACHD Redo Surgery: Strategies to Optimize Outcomes David N. Campbell MD Professor of CV Surgery University of Colorado, Denver Children s Hospital Colorado ACHD 2017 Symposium, Nov 30-Dec
Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada
 PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions
 Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
Case submission for CSI Asia-Pacific Case 2
 Case submission for CSI Asia-Pacific 2018- Case 2 Title Page Case category: Coarctation and ducts, valves Title: Simultaneous balloon aortic valvuloplasty with transcatheter closure of large hypertensive
Case submission for CSI Asia-Pacific 2018- Case 2 Title Page Case category: Coarctation and ducts, valves Title: Simultaneous balloon aortic valvuloplasty with transcatheter closure of large hypertensive
Congenital Heart Disease An Approach for Simple and Complex Anomalies
 Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Role of Balloons and Stents in Congenital Heart Disease
 Role of Balloons and Stents in Congenital Heart Disease Rui Anjos Lisbon, Portugal No conflict of interest Balloon dilatation in Congenital Heart Disease Balloons in CHD Initially used in the 80s Learning
Role of Balloons and Stents in Congenital Heart Disease Rui Anjos Lisbon, Portugal No conflict of interest Balloon dilatation in Congenital Heart Disease Balloons in CHD Initially used in the 80s Learning
Debate: Should Ductal Stent Implantation be Considered for All Newborn Infants with Reduced Pulmonary Blood Flow?_Pros
 Debate: Should Ductal Stent Implantation be Considered for All Newborn Infants with Reduced Pulmonary Blood Flow?_Pros Mazeni Alwi Institut Jantung Negara Kuala Lumpur, Malaysia 5 th Asia Pacific Congenital
Debate: Should Ductal Stent Implantation be Considered for All Newborn Infants with Reduced Pulmonary Blood Flow?_Pros Mazeni Alwi Institut Jantung Negara Kuala Lumpur, Malaysia 5 th Asia Pacific Congenital
Preoperative Echocardiographic Assessment of Uni-ventricular Repair
 Preoperative Echocardiographic Assessment of Uni-ventricular Repair Salem Deraz, MD Pediatric Cardiologist, Aswan Heart Centre Magdi Yacoub Heart Foundation Uni-ventricular repair A single or series of
Preoperative Echocardiographic Assessment of Uni-ventricular Repair Salem Deraz, MD Pediatric Cardiologist, Aswan Heart Centre Magdi Yacoub Heart Foundation Uni-ventricular repair A single or series of
ADULT CONGENITAL HEART DISEASE. Stuart Lilley
 ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
Slide 1. Slide 2. Slide 3 CONGENITAL HEART DISEASE. Papworth Hospital NHS Trust INTRODUCTION. Jakub Kadlec/Catherine Sudarshan INTRODUCTION
 Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
CARDIOVASCULAR SURGERY
 Volume 107, Number 4 April 1994 The Journal of THORACIC AND CARDIOVASCULAR SURGERY Cardiac and Pulmonary Transplantation Risk factors for graft failure associated with pulmonary hypertension after pediatric
Volume 107, Number 4 April 1994 The Journal of THORACIC AND CARDIOVASCULAR SURGERY Cardiac and Pulmonary Transplantation Risk factors for graft failure associated with pulmonary hypertension after pediatric
가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY
 가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY PA c IVS (not only pulmonary valve disease) Edwards JE. Pathologic Alteration of the right heart. In: Konstam MA, Isner M, eds.
가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY PA c IVS (not only pulmonary valve disease) Edwards JE. Pathologic Alteration of the right heart. In: Konstam MA, Isner M, eds.
Case Report. Stent Placement in a Neonate with Sano Modification of the Norwood using Semi-Elective Extracorporeal Membrane Oxygenation.
 Stent Placement in a Neonate with Sano Modification of the Norwood using Semi-Elective Extracorporeal Membrane Oxygenation Mustafa Gulgun and Michael Slack Associated Profesor Children National Medical
Stent Placement in a Neonate with Sano Modification of the Norwood using Semi-Elective Extracorporeal Membrane Oxygenation Mustafa Gulgun and Michael Slack Associated Profesor Children National Medical
Transcatheter Pulmonary Valve Replacement Update on progress and outcomes
 Transcatheter Pulmonary Valve Replacement Update on progress and outcomes Barry Love, MD Director, Congenital Cardiac Catheterization Laboratory Mount Sinai Medical Center New York, New York Transcatheter
Transcatheter Pulmonary Valve Replacement Update on progress and outcomes Barry Love, MD Director, Congenital Cardiac Catheterization Laboratory Mount Sinai Medical Center New York, New York Transcatheter
3/14/2011 MANAGEMENT OF NEWBORNS CARDIAC INTENSIVE CARE CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 WITH HEART DEFECTS
 CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
Cardiac surgery Closure of defect of artrioventicular septum using dual prosthesis patches
 CARDIOLOGY / CARDIOTHORACIC SURGERY PROCEDURES PROCEDURE A ( RM 4401 - RM 4800 ) 1 General procedures Replacement of aortic valve (including valvuloplasty) 2 General procedures Replacement of mitral valve
CARDIOLOGY / CARDIOTHORACIC SURGERY PROCEDURES PROCEDURE A ( RM 4401 - RM 4800 ) 1 General procedures Replacement of aortic valve (including valvuloplasty) 2 General procedures Replacement of mitral valve
Percutaneous VSD closure
 Percutaneous VSD closure Gianfranco Butera San Donato Milanese - Italy Patients selection Pts having hemodynamically significant VSD Left ventricular enlargement (left ventricular overload),defined as
Percutaneous VSD closure Gianfranco Butera San Donato Milanese - Italy Patients selection Pts having hemodynamically significant VSD Left ventricular enlargement (left ventricular overload),defined as
Jian Fang 1, Shaobo Xie 2, Lunchao Ma 2, Chao Yang 2. Original Article
 Original Article Anatomic and surgical factors affecting the switch from minimally invasive transthoracic occlusion to open surgery during ventricular septal defect repair Jian Fang 1, Shaobo Xie 2, Lunchao
Original Article Anatomic and surgical factors affecting the switch from minimally invasive transthoracic occlusion to open surgery during ventricular septal defect repair Jian Fang 1, Shaobo Xie 2, Lunchao
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim
 or AoV plasty- Kyung-Hwan Kim") 42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
Adult Congenital Heart Disease T S U N ` A M I!
 Adult Congenital Heart Disease T S U N ` A M I! Erwin Oechslin, MD, FRCPC, FESC Director, Congenital Cardiac Centre for Adults University Health Network Peter Munk Cardiac Centre / Toronto General Hospital
Adult Congenital Heart Disease T S U N ` A M I! Erwin Oechslin, MD, FRCPC, FESC Director, Congenital Cardiac Centre for Adults University Health Network Peter Munk Cardiac Centre / Toronto General Hospital
Debate in Management of native COA; Balloon Versus Surgery
 Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
Native Outflow Tract Transcatheter Pulmonary Valve Replacement
 Native Outflow Tract Transcatheter Pulmonary Valve Replacement John P. Cheatham, MD, FSCAI George H. Dunlap Endowed Chair in Interventional Cardiology Co-Director, The Heart Center, Nationwide Children
Native Outflow Tract Transcatheter Pulmonary Valve Replacement John P. Cheatham, MD, FSCAI George H. Dunlap Endowed Chair in Interventional Cardiology Co-Director, The Heart Center, Nationwide Children
Survival Rates of Children with Congenital Heart Disease continue to improve.
 DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!!
 Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Interventions in Adult Congenital Heart Disease: Role of CV Imaging. Associate Professor. ACHD mortality. Pillutla. Am Heart J 2009;158:874-9
 Interventions in Adult Congenital Heart Disease: Role of CV Imaging Sangeeta Shah MD, FACC, FASE Associate Professor ACHD mortality Pillutla. Am Heart J 2009;158:874-9 Adult Congenital Heart Disease Heterogenity
Interventions in Adult Congenital Heart Disease: Role of CV Imaging Sangeeta Shah MD, FACC, FASE Associate Professor ACHD mortality Pillutla. Am Heart J 2009;158:874-9 Adult Congenital Heart Disease Heterogenity
Type Size AP/PS RP/RS Qp/Qs. Ia Resistive <0.3 < Ib Resistive <0.3 < IIa Resistive <0.5 >2
 Transcatheter closure of VSD using Duct Occluder device Nguyen Lan Hieu, MD, PhD Hanoi Medical University Vietnam Heart Institute Anatomy of VSD 1. Perimembranous VSD: Aneurysm septal membranous(tv or
Transcatheter closure of VSD using Duct Occluder device Nguyen Lan Hieu, MD, PhD Hanoi Medical University Vietnam Heart Institute Anatomy of VSD 1. Perimembranous VSD: Aneurysm septal membranous(tv or
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
The Ohio State University Columbus, Ohio, USA
 8 th National ACHA Conference, June 3 rd, 2017, Orlando, FL Transcatheter Heart Valves A Hybrid Approach Let s Work Together John P. Cheatham, MD, MSCAI George H. Dunlap Endowed Chair in Interventional
8 th National ACHA Conference, June 3 rd, 2017, Orlando, FL Transcatheter Heart Valves A Hybrid Approach Let s Work Together John P. Cheatham, MD, MSCAI George H. Dunlap Endowed Chair in Interventional
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016
 1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
PATENT DUCTUS ARTERIOSUS (PDA)
") PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
"Lecture Index. 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.
 Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.") "Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
"Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
Treatment of congenital aortic valve disease: Neonatal surgical management. Pascal Vouhé - Sick Children Hospital, Paris
 Treatment of congenital aortic valve disease: Neonatal surgical management Pascal Vouhé - Sick Children Hospital, Paris Challenges. valvar lesions. associated lesions. status of left ventricle Valvar lesions.
Treatment of congenital aortic valve disease: Neonatal surgical management Pascal Vouhé - Sick Children Hospital, Paris Challenges. valvar lesions. associated lesions. status of left ventricle Valvar lesions.
Cardiac MRI in ACHD What We. ACHD Patients
 Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
In 1980, Bex and associates 1 first introduced the initial
 Technique of Aortic Translocation for the Management of Transposition of the Great Arteries with a Ventricular Septal Defect and Pulmonary Stenosis Victor O. Morell, MD, and Peter D. Wearden, MD, PhD In
Technique of Aortic Translocation for the Management of Transposition of the Great Arteries with a Ventricular Septal Defect and Pulmonary Stenosis Victor O. Morell, MD, and Peter D. Wearden, MD, PhD In
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
Cardiac Catheterization Cases Primary Cardiac Diagnoses Facility 12 month period from to PRIMARY DIAGNOSES (one per patient)
") PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
Case 47 Clinical Presentation
 93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases
 Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
TRANSCATHETER VALVE IMPLANTATION IN THE RIGHT HEART
 TRANSCATHETER VALVE IMPLANTATION IN THE RIGHT HEART Dr Aphrodite Tzifa, MD(Res), FRCPCH Director, Paediatric and GUCH Cardiologist, Mitera Children's Hospital, Athens, Greece September 10, 2003 FAILURE
TRANSCATHETER VALVE IMPLANTATION IN THE RIGHT HEART Dr Aphrodite Tzifa, MD(Res), FRCPCH Director, Paediatric and GUCH Cardiologist, Mitera Children's Hospital, Athens, Greece September 10, 2003 FAILURE
Data Collected: June 17, Reported: June 30, Survey Dates 05/24/ /07/2010
 Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical)
") September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
Adult Congenital Heart Disease: The New Reality. Disclosures
 Adult Congenital Heart Disease: The New Reality Kathryn Rouine-Rapp, MD Professor of Anesthesia Disclosures I have nothing to disclose 1 Outline Historic perspective Our reality Common lesions Guidelines
Adult Congenital Heart Disease: The New Reality Kathryn Rouine-Rapp, MD Professor of Anesthesia Disclosures I have nothing to disclose 1 Outline Historic perspective Our reality Common lesions Guidelines
Atrial Septal Defect Closure. Stephen Brecker Director, Cardiac Catheterisation Labs
 Stephen Brecker Director, Cardiac Catheterisation Labs ADVANCED ANGIOPLASTY Incorporating The Left Main 5 Plus Course Conflicts of Interest The following companies have supported educational courses held
Stephen Brecker Director, Cardiac Catheterisation Labs ADVANCED ANGIOPLASTY Incorporating The Left Main 5 Plus Course Conflicts of Interest The following companies have supported educational courses held
Management of complex CHD in adults
 Management of complex CHD in adults Victor Tsang Society of Thoracic Surgeons of Thailand 2016 The impact of infant cardiac surgery Over 90 % of infants born with CHD will reach adulthood By 2010, adults
Management of complex CHD in adults Victor Tsang Society of Thoracic Surgeons of Thailand 2016 The impact of infant cardiac surgery Over 90 % of infants born with CHD will reach adulthood By 2010, adults