Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support
|
|
|
- Naomi Jacobs
- 6 years ago
- Views:
Transcription



1 Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support Mahir Elder, MD, FACC,SCAI Medical Direct of PERT program Medical Director of Endovascular medicine Clinical Professor of Medicine Wayne State University-School of Medicine
2 Disclosures Abiomed Speakers Bureau BTG
3 Right Ventricular Failure - Definition Right ventricular chamber overload with contractile abnormalities resulting in compromised ability to deliver blood to the pulmonary circulation Multiple proposed parameters to diagnose RV failure & monitor RV function
4 Right Ventricular Failure - Parameters Parameters suggestive of RV dysfunction in acute PE Right atrial pressure (mean >5) Pulmonary artery pressure (Systolic > 25, Diastolic > 10) Pulmonary vascular resistance (> 1600 dynes-sec cm -5 ) Right Ventricular stroke work index (< 300 mmhg/ml/m 2 ) RA-to-PCWP ratio (>0.63) PAPi (<1)
5 Right Ventricular Failure Assessment, PAPi Pulmonary artery pulsatility index (PAPi) PAPi < 1 associated with in-hospital mortality with Inferior AMI (Sn 88.9%, Sp 98.3%) Catheter Cardiovascular Intervention, 2012 Oct 1;80(4): PAPi studied in LVAD recipients Found that it is an independent predictor of RV failure and the need for RVAD support after LVAD placement J. Heat Lung Transplantation, January 2016 Vol 35, Issue 1, Pages No large randomized trial to study predictive value of PAPi in Acute Pulmonary Embolism
6 Proposed Parameters of Acute RV Failure CT / Echo showing RV/LV Ratio >1 McConnell s Sign Akinesis of mid Free wall and hypercontactile RV apex PA Pressure PA Systolic > 55 mmhg + BNP and/or Troponin Elevated CVP Systemic SBP < 90 PA O2 Saturation

7 Right Ventricular Failure - Mechanisms JACC, Vol. 56, No. 18, 2010
8 Cardiac Dysfunction Cascade
9 Clinical Cases
10 Case # 1 60 yr old man with history of DVT, off anticoagulation Presented to ER Respiratory Distress, swelling in R calf x 2d CT - massive PE : PESI 132 (class V, mortality % in 30 days), Echo shows McConnell s Sign BP 76/30 (lowest recorded)

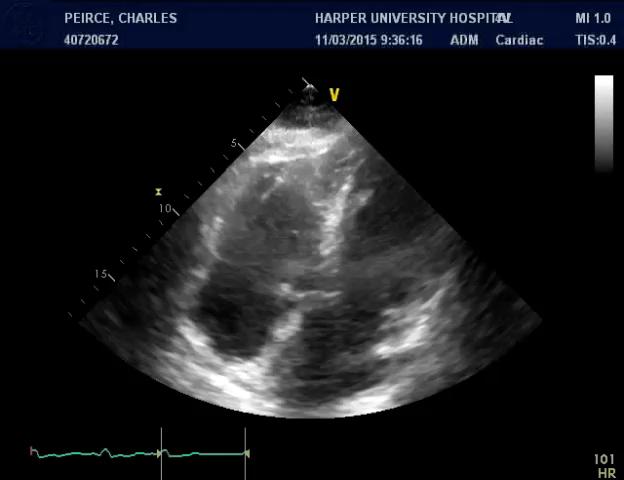
11 Echo


12 CT Scan and Pulmonary angiogram
13 Mean RA 28, PA 65 /38, RV Failure with PaPi score of <1 B/L Ekos for 6 hours (total of 20mg TPA)- PE clot improved RV still in failure and hypotensive despite -IV Pressor Decision was made to support RV with RV impella

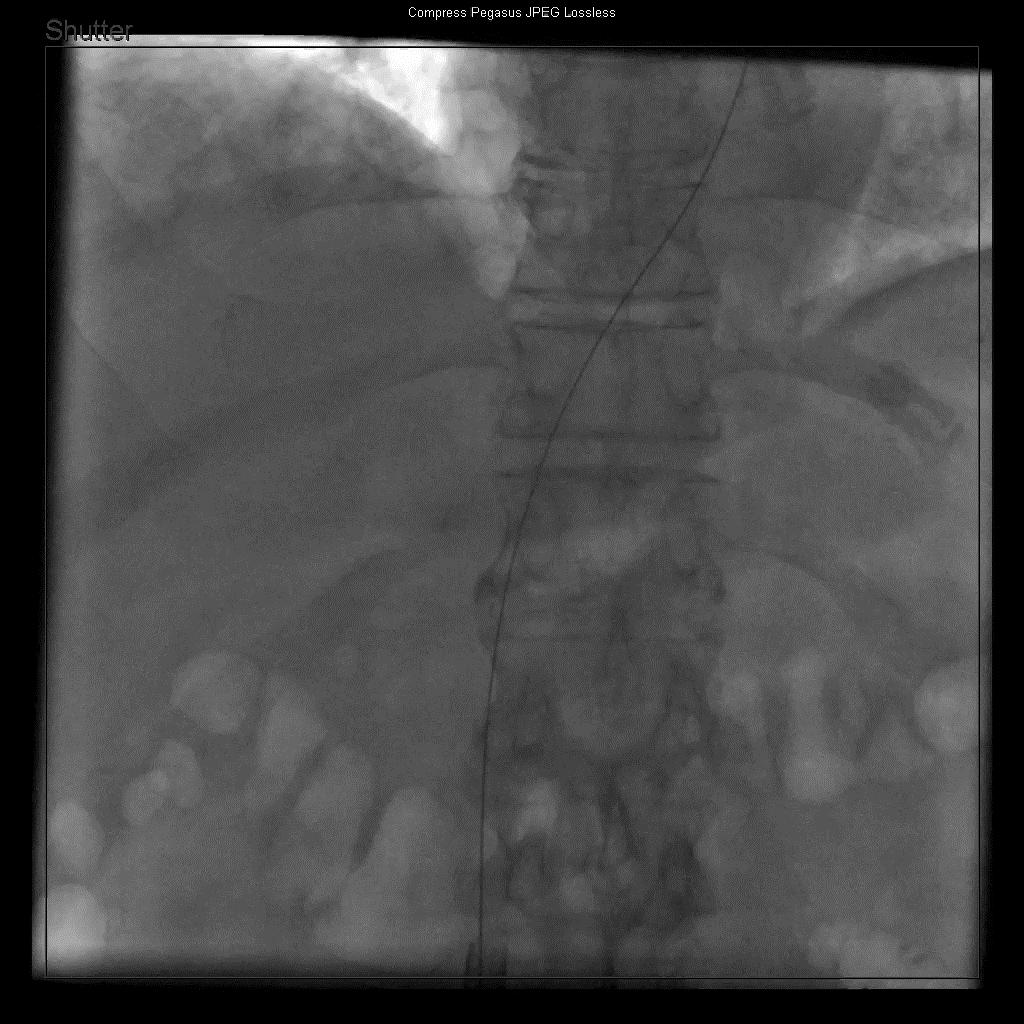
14 Step 1: Advancing Impella Sheath under fluoroscopy
15
16
17
18 Post CDT Oral NOAC Iv fluid RP Impella 2 days at 3.3 L/m on P6 D/C pressor Maintain B/P Recovery of RV function, PaPi Score 3.0 Mean RA 10, PA 40/10 Discharged home 3 month follow up-echo: Mild pulmonary HTN Normal RV/LV ratio and function
19 Case #2 presentation Chief Complaint 52 year old female who presented with exertional dyspnea for 3 days. History of Present Illness Recent admission for lower extremity cellulitis. finished two weeks course of cefipime and bactrim. Physical examination Unremarkable aside of sinus tachycardia.

20 Electrocardiogram + Sinus tachycardia. + Inverted T waves in V1-V3. - Left axis. - Lack of classic S1Q3T3. - No new RBBB.
21 Relevant lab results Creatinine 1.06 mg%, normal electrolytes. Troponin I ng%. Lactic Acid 2.8 mmoles/l. CBC: WBC 7.7 in mm3. Hb 9.5 gr%. PLT 241 in mm3. Risk stratification: PESI 109- moderate range. Modified PESI 8.9% risk of index admission mortality.

22 Computed Tomography Sub massive pulmonary embolism: the main right and left pulmonary arteries. Severe RV enlargement: RV/LV ratio >> 0.9.
23 Right heart cath- First day of admission RA: 16/18/17 mmhg. RV: 40/10/20 mmhg. PA: 39/23/30 mmhg. PAPI: PA pulse pressure / mean RA = Cardiac output: 4.7 L/min. Cardiac index: 2.15 L/min/m2. Catheter mediated thrombolysis- Two EKOS catheter based ultrasonic filaments were placed into the right and left main pulmonary arteries.
24 Hemodynamic deterioration- Third day of admission Systolic blood pressure 86 mmhg. Heart rate 105 min. Reduced urine output. Respiratory rate 36 min. Right heart catheterization: RA: 19/24/23 mmhg. RV: 42/11/26 mmhg. PA: 41/28/33 mmhg. PAPI: PA pulse pressure / mean RA = Impella RP insertion


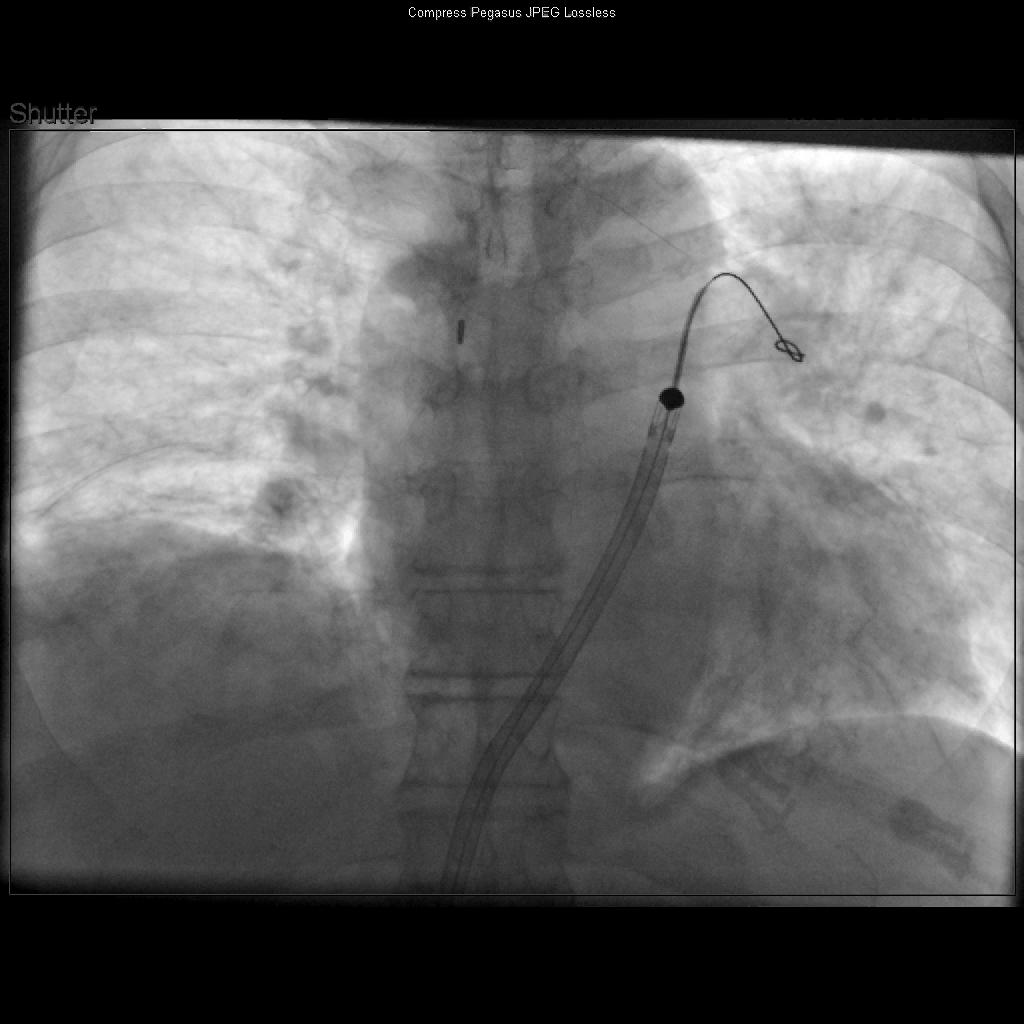
25 Impella RP insertion Impella RP 23 French sheath into the IVC level Platinum plus at the level of the left upper pulmonary vein.


26 Impella RP insertion Impella RP is advanced into the RA level Impella RP is in position
27 Impella RP for 6 days Marked hemodynamic improvement. Right heart catheterization before Impella removal: RA 18/22/21 mmhg. RV 49/14/20 mmhg. PA 48/31/37 mmhg. PAPI: Patient was discharged after 20 days of admission.



28 Echocardiography Before Impella: Severe RV dilatation with reduction in FAC Impella RP day 4: Severe RV dilatation with mild improvement in FAC Post Impella: Severe RV dilatation with significant improvement in FAC

29 ACC-2017 O'Neil 37 discharge 80% survival 100% native heart
 spap-dpap/ra CPO < 0.6 CPO > 0.6 PAPi PAPi 1.5 > 1.")
30 CARDIOGENIC SHOCK FLOW CHART 30 Reassess Hemodynamics via PAC prior to Discharge from the Cath Lab: 1. Cardiac Power Output (CPO) MAP CO/451 W 2. Pulmonary Artery Pulsatility Index (PAPi) spap-dpap/ra CPO < 0.6 CPO > 0.6 PAPi PAPi 1.5 > > 1.5 RV Dysfunction: Right-sided MCS (Impella RP ) RV Preserved: Escalate MCS or consider transfer to LVAD/Transplant Center RV Dysfunction: Right-sided MCS (Impella RP) Persistent Hypoxemia? PaO 2 < 55 on 100% FiO 2 VA or VV-ECMO: Recommend maintaining Impella at low speed for LV decompression Ye s No Admit to ICU to maximize supportive care and to actively assess for myocardial recovery RV Failure as defined by Recover Right 1 : CI < 2.2 L/min/m 2 (despite continuous infusion of 1 high dose inotrope, ie, da/dobutamine 10 µg/kg/min or equivalent) and any of the following: 1. CVP > 15 mmhg, or 2. CVP/PCWP or LAP ratio >0.63, or 3. RV dysfunction on TTE (TAPSE score 14 mm) Anderson MB, et al. J Heart Lung Transplant. 2015;34(12): IMP
31 Impella RP in patients with Massive Pulmonary Embolism N. Blank; A. Kaki; M. Elder; W. Htun; T. Mohamad; T. Schreiber. Detroit Medical Center- Heart hospital
32 Impella RP in a series of 4 patients Four consecutive patients with Massive PE and RV Cardiogenic shock refractory to inotropes treated with RP Impella as bridge to recovery. Prior to Impella RP, all patients treated with EKOS/CDT.
33 Major parameters: Baseline (before Impella RP insertion): Cardiac index = 1.7 l/min/m2 (range ). Mean pulmonary blood pressure = 42 mmhg (range 33-57) Impella RP used an average of 3.75 days (range of 1-6). During Impella RP treatment all patients improved clinically & hemodynamically: Cardiac index increased to 2.5 l/min/m2 (range ), p=0.09 on day 1 Cardiac index increased to 3.1 l/min/m2 (range ), p<0.05 at day 2. Echocardiography in two patients showed marked improvement in RV size and function. The other two patients had persistent severe RV dilation & hypokinesis. No significant change was found in renal function, hemoglobin and platelets level with Impella RP treatment. No patient required transfusion. One patient treated with Impella RP for 6 days had hemoglobin level drop from 13.7 to 7.3 gm/dl.

34 RV assessment by Echo at index day and follow up days 3-4

35 Vital signs and risk stratification. Before and after related to treatment with Impella RP.

36 Right heart catheterization before & after treatment with Impella RP
37 Mechanical RV Circulatory Support Impella RP Tandem Heart-Protek ECMO: V-V


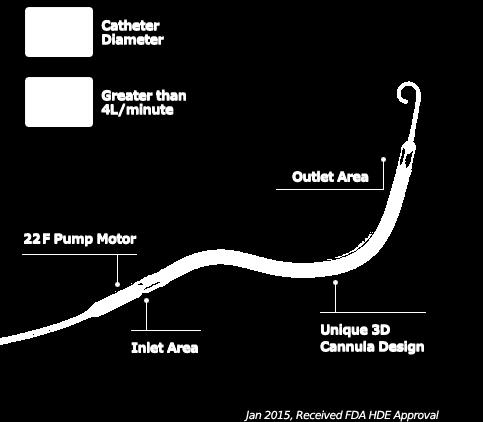
38 Impella RP Indicated for providing circulatory assistance for up to 14 days in patients with a body surface area 1.5 m2 who develop acute right heart failure or decompensation following LVAD, myocardial infarction, heart transplant, or open-heart surgery.



39 TandemHeart Single IJ Access Double Venous Access - IJ/Femoral - Femoral/Femoral Common uses in Acute RV failure - Acute PE - RV infarction - RV dysfunction post-lvad - ARDS Double or Single Venous Access - In-flow from right atrium - Out-flow to pulmonary artery
40 ECMO V-V ECMO Refractory respiratory failure Modest cardiac or hemodynamic effects RV and LV pre- and after-load largely unaffected Potential decrease in RV afterload à improved oxygenation V-A ECMO Heart and Lung support RV pre-load and pulmonary flow LV afterload and arterial pulse pressure

41 Common Veno-Venous ECMO a) Femoral Jugular Cannulation b) Bicaval dual lumen cannulation of right internal jugular c) Femoral Femoral Cannulation. Avalon Cannula Simon J. Finney Eur Respir Rev 2014;23: by European Respiratory Society

42 V-A and V-VA ECMO a) Venoarterial ECMO b) Venovenous Arterial ECMO Simon J. Finney Eur Respir Rev 2014;23: by European Respiratory Society
 Cannula Size 24F Peel away, 9Fr")





43 Impella RP Tandem Heart V-V ECMO (CentriMag) Mechanism Micro-axial Centrifugal Centrifugal Centrifugal V-A ECMO (CentriMag) Cannula Size 24F Peel away, 9Fr catheter 29-31Fr Dual Lumen 31Fr Dual lumen or Fr. Single in/outflow Fr Arterial Fr Venous Insertion Technique Single femoral vein, 9Fr catheter remains in vein Dual lumen IJ IJ dual lumen or fem vein and IJ Peripheral or Central Hemodynamic Support >4 L/min maximum flow Up to 5 L/min Up to 4.5L/ min 5 L/min Implantation Time Device Preparation Time Anticoagulation Post Implant Management Hemolysis Risk Respiratory Support No Yes Yes Yes Risk of Hemolysis Pros Single access site BiVAD possible with escalation Ambulate (neck) Oxygenation -+++ Hemodynamic support Oxygenation +++ Cons No intrinsic oxygenator Long insertion time High Transfusion rates Transseptal (LA-FA bypass) No Hemodynamic support LV Distension Vascular complications, SIRS Transfusion (bleed) 23Fr
44 Conclusion: There are several proposed criteria for assessing RV failure Critical to Recognition of RV failure as an etiology for patient deterioration Time sensitive- implementation of medical & invasive strategies to treat RV failure Several invasive mechanical options are available to offload RV Promote RV recovery and stabilize patients Impella RP provides mechanical circulatory support in PE patients complicated by acute refractory right heart failure despite CDT. Low adverse events rates observed in this small series Tandem Heart ECMO Further study is warranted
Management of Acute Shock and Right Ventricular Failure
 Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Cardiogenic Shock Protocol
 Cardiogenic Shock Protocol Impella Devices Best Practices in AMI Cardiogenic Shock Identify 1-3 SBP < 90 mmhg or on inotropes /pressors Cold, clammy, tachycardia Lactate elevated > 2 mmoi /L Stabilize
Cardiogenic Shock Protocol Impella Devices Best Practices in AMI Cardiogenic Shock Identify 1-3 SBP < 90 mmhg or on inotropes /pressors Cold, clammy, tachycardia Lactate elevated > 2 mmoi /L Stabilize
Mechanics of Cath Lab Support Devices
 Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Chief Medical Officer First Coast Cardiovascular Institute, Jacksonville, FL Professor of Medicine, UCF, Orlando, FL None DISCLOSURE Percutaneous
Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Chief Medical Officer First Coast Cardiovascular Institute, Jacksonville, FL Professor of Medicine, UCF, Orlando, FL None DISCLOSURE Percutaneous
Mechanics of Cath Lab Support Devices
 Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Professor of Medicine Mayo Clinic College of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida DISCLOSURE Presenter:
Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Professor of Medicine Mayo Clinic College of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida DISCLOSURE Presenter:
Management of Cardiogenic Shock. Dr Stephen Pettit, Consultant Cardiologist
 Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Echo assessment of patients with an ECMO device
 Echo assessment of patients with an ECMO device Evangelos Leontiadis Cardiologist 1st Cardiology Dept. Onassis Cardiac Surgery Center Athens, Greece Gibbon HLM 1953 Goldstein DJ et al, NEJM 1998; 339:1522
Echo assessment of patients with an ECMO device Evangelos Leontiadis Cardiologist 1st Cardiology Dept. Onassis Cardiac Surgery Center Athens, Greece Gibbon HLM 1953 Goldstein DJ et al, NEJM 1998; 339:1522
Acute Mechanical Circulatory Support Right Ventricular Support Devices
 Acute Mechanical Circulatory Support Right Ventricular Support Devices Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Acute Mechanical Circulatory Support Right Ventricular Support Devices Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management
 Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management Yoshifumi Naka, MD, PhD Columbia University Medical Center New York, NY Disclosure Abbott/St. Jude Med./Thoratec Consultant
Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management Yoshifumi Naka, MD, PhD Columbia University Medical Center New York, NY Disclosure Abbott/St. Jude Med./Thoratec Consultant
Mechanical Cardiac Support in Acute Heart Failure. Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research
 Mechanical Cardiac Support in Acute Heart Failure Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research Disclosures Research Support and/or Consulting NHLBI Amgen Cytokinetics
Mechanical Cardiac Support in Acute Heart Failure Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research Disclosures Research Support and/or Consulting NHLBI Amgen Cytokinetics
LV Distension and ECLS Lungs
 LV Distension and ECLS Lungs Kevin W. Hatton, MD, FCCM Interim Vice-Chair for Anesthesiology Research Division Chief, Anesthesiology Critical Care Medicine Program Director, Anesthesiology Critical Care
LV Distension and ECLS Lungs Kevin W. Hatton, MD, FCCM Interim Vice-Chair for Anesthesiology Research Division Chief, Anesthesiology Critical Care Medicine Program Director, Anesthesiology Critical Care
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Extra Corporeal Life Support for Acute Heart failure
 Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
The Role of Mechanical Circulatory Support in Cardiogenic Shock: When to Utilize
 The Role of Mechanical Circulatory Support in Cardiogenic Shock: Presented by Nancy Scroggins ACNP, CNS-CC CV Surgery ACNP Bayshore Medical Center The Role of Mechanical Circulatory Support in Cardiogenic
The Role of Mechanical Circulatory Support in Cardiogenic Shock: Presented by Nancy Scroggins ACNP, CNS-CC CV Surgery ACNP Bayshore Medical Center The Role of Mechanical Circulatory Support in Cardiogenic
Bridging With Percutaneous Devices: Tandem Heart and Impella
 Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
ECMO as a bridge to durable LVAD therapy. Jonathan Haft, MD Department of Cardiac Surgery University of Michigan
 ECMO as a bridge to durable LVAD therapy Jonathan Haft, MD Department of Cardiac Surgery University of Michigan Systolic Heart Failure Prevalence 4.8 million U.S. 287,000 deaths per year $39 billion spent
ECMO as a bridge to durable LVAD therapy Jonathan Haft, MD Department of Cardiac Surgery University of Michigan Systolic Heart Failure Prevalence 4.8 million U.S. 287,000 deaths per year $39 billion spent
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012
 Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
Right Ventricular Failure: Prediction, Prevention and Treatment
 Right Ventricular Failure: Prediction, Prevention and Treatment 3 rd European Training Symposium for Heart Failure Cardiologists and Cardiac Surgeons University Hospital Bern June 24-25, 2016 Disclosures:
Right Ventricular Failure: Prediction, Prevention and Treatment 3 rd European Training Symposium for Heart Failure Cardiologists and Cardiac Surgeons University Hospital Bern June 24-25, 2016 Disclosures:
Disclosures. Objectives 10/11/17. Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock. I have no disclosures to report
 Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Case - Advanced HF and Shock (INTERMACS 1)
") Case - Advanced HF and Shock (INTERMACS 1) Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive Director,
Case - Advanced HF and Shock (INTERMACS 1) Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive Director,
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO)
") Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Right Heart Failure in LVAD patients: Prevention and Management.
 Christian Bermudez MD. Associate Professor Director Thoracic Transplantation Division Cardiac Surgery Department of Surgery University of Pennsylvania Right Heart Failure in LVAD patients: Prevention and
Christian Bermudez MD. Associate Professor Director Thoracic Transplantation Division Cardiac Surgery Department of Surgery University of Pennsylvania Right Heart Failure in LVAD patients: Prevention and
Percutaneous Mechanical Circulatory Support Devices
 Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions
 Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions Kush R Desai, MD Assistant Professor of Radiology Northwestern University Feinberg School of Medicine Chicago, IL Disclosures
Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions Kush R Desai, MD Assistant Professor of Radiology Northwestern University Feinberg School of Medicine Chicago, IL Disclosures
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE. Mark Goodwin, MD
 Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
AllinaHealthSystem 1
 : Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
: Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017
 Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Assist Devices in STEMI- Intra-aortic Balloon Pump
 Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Circulatory Support: From IABP to LVAD
 Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference Dubai: October Acute Coronary Syndromes
 8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 OSPEDALE Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 OSPEDALE Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele
IABP to prevent pulmonary edema under VA-ECMO
 IABP to prevent pulmonary edema under VA-ECMO Alain Combes Service de Réanimation ican, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre et Marie Curie,
IABP to prevent pulmonary edema under VA-ECMO Alain Combes Service de Réanimation ican, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre et Marie Curie,
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD
 A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities
 The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Jennifer A. Brown The Cleveland Clinic School of Perfusion Cleveland, Ohio
 Biventricular Heart Failure Advanced Treatment Options at The Cleveland Clinic Jennifer A. Brown The Cleveland Clinic School of Perfusion Cleveland, Ohio I have no disclosures. Examine respiratory and
Biventricular Heart Failure Advanced Treatment Options at The Cleveland Clinic Jennifer A. Brown The Cleveland Clinic School of Perfusion Cleveland, Ohio I have no disclosures. Examine respiratory and
A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD
 A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD SK Singh MD MSc, DK Pujara MBBS, J Anand MD, WE Cohn MD, OH Frazier MD, HR Mallidi MD Division of Transplant & Assist
A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD SK Singh MD MSc, DK Pujara MBBS, J Anand MD, WE Cohn MD, OH Frazier MD, HR Mallidi MD Division of Transplant & Assist
Update on Mechanical Circulatory Support. AATS May 5, 2010 Toronto, ON Canada
 Update on Mechanical Circulatory Support AATS May 5, 2010 Toronto, ON Canada Disclosures NONE Emergency Circulatory Support ECMO Tandem Heart Impella Assessment Cardiac Function Pulmonary function Valvular
Update on Mechanical Circulatory Support AATS May 5, 2010 Toronto, ON Canada Disclosures NONE Emergency Circulatory Support ECMO Tandem Heart Impella Assessment Cardiac Function Pulmonary function Valvular
What is New in Acute Pulmonary Embolism? Interventional Treatment. Prof. Nils Kucher University Hospital Bern Switzerland
 What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis
 Receiving Catheter- Directed Thrombolysis") Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis John A. Phillips, M.D. OhioHealth Heart and Vascular Physicians
Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis John A. Phillips, M.D. OhioHealth Heart and Vascular Physicians
Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California
 High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
Long Term Support for Respiratory Failure: VV ECMO or Oxygenated RVAD?
 Long Term Support for Respiratory Failure: VV ECMO or Oxygenated RVAD? Mechanical Circulatory Support Symposium 2018 (Houston, TX) Charles Hoopes, MD Professor of Surgery University of Alabama (Birmingham)
Long Term Support for Respiratory Failure: VV ECMO or Oxygenated RVAD? Mechanical Circulatory Support Symposium 2018 (Houston, TX) Charles Hoopes, MD Professor of Surgery University of Alabama (Birmingham)
Case. Case. Management of Pulmonary Embolism in the ICU
 Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
ECLS as Bridge to Transplant
 ECLS as Bridge to Transplant Marcelo Cypel MD, MSc Assistant Professor of Surgery Division of Thoracic Surgery Toronto General Hospital University of Toronto Application of ECLS Bridge to lung recovery
ECLS as Bridge to Transplant Marcelo Cypel MD, MSc Assistant Professor of Surgery Division of Thoracic Surgery Toronto General Hospital University of Toronto Application of ECLS Bridge to lung recovery
Epidemiology. Update on Pulmonary Embolism. Keys to PE Management 5/5/2014. Diagnosis. Risk stratification. Treatment
 Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation.
 Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation. Evaluation of RVAD Function. Ioannis A Paraskevaidis Attikon University Hospital Historical Perspective
Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation. Evaluation of RVAD Function. Ioannis A Paraskevaidis Attikon University Hospital Historical Perspective
Ventricular Assisting Devices in the Cathlab. Unrestricted
 Ventricular Assisting Devices in the Cathlab Unrestricted What is a VAD? A single system device that is surgically attached to the left ventricle of the heart and to the aorta for left ventricular support
Ventricular Assisting Devices in the Cathlab Unrestricted What is a VAD? A single system device that is surgically attached to the left ventricle of the heart and to the aorta for left ventricular support
Bilateral Central Pulmonary Embolism and Recent History of Ischemic Stroke
 WHAT WOULD YOU DO? Bilateral Central and Recent History of Ischemic Stroke MODERATOR: KEITH M. STERLING, MD PANEL: JAMES F. BENENATI, MD; NOAH J. JONES, MD, FACC, FSCAI; AND AKHILESH K. SISTA, MD, FSIR
WHAT WOULD YOU DO? Bilateral Central and Recent History of Ischemic Stroke MODERATOR: KEITH M. STERLING, MD PANEL: JAMES F. BENENATI, MD; NOAH J. JONES, MD, FACC, FSCAI; AND AKHILESH K. SISTA, MD, FSIR
Acute Management of Pulmonary Embolism
 Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
 Pulmonary Embolism Response Teams Not So Fast Early Interventions is a House of Cards Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
Pulmonary Embolism Response Teams Not So Fast Early Interventions is a House of Cards Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
Management of Acute Pulmonary Embolism. Judith Hurdman Consultant Respiratory Physician
 Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
Adult Extracorporeal Life Support (ECLS)
") Adult Extracorporeal Life Support (ECLS) Steven Scott, M.D., F.A.C.S. Piedmont Heart Institute Cardiothoracic Surgery Disclosures None ECMO = ECLS A technique of life support that involves a continuous
Adult Extracorporeal Life Support (ECLS) Steven Scott, M.D., F.A.C.S. Piedmont Heart Institute Cardiothoracic Surgery Disclosures None ECMO = ECLS A technique of life support that involves a continuous
PE and DVT. Dr Anzo William Adiga WatsApp or Call Medical Officer/RHEMA MEDICAL GROUP
 PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
เอกราช อร ยะช ยพาณ ชย
 30 July 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Disclosure Speaker, CME service: Merck, Otsuka, Servier Consultant, non-cme service: Novartis, Menarini
30 July 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Disclosure Speaker, CME service: Merck, Otsuka, Servier Consultant, non-cme service: Novartis, Menarini
Rationale for Prophylactic Support During Percutaneous Coronary Intervention
 Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Introduction to Acute Mechanical Circulatory Support
 Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure
 Guidelines for Pediatric Respiratory Failure") Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Physiologic Based Management of Circulatory Shock Kuwait 2018
 Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
MCS for Acute Heart Failure Eric Adler MD Associate Professor of Medicine Medical Director Cardiac Transplant
 MCS for Acute Heart Failure 2016 Eric Adler MD Associate Professor of Medicine Medical Director Cardiac Transplant Why do we decompensate? Which Heart Failure Patients Should Get Palliative Care and Who
MCS for Acute Heart Failure 2016 Eric Adler MD Associate Professor of Medicine Medical Director Cardiac Transplant Why do we decompensate? Which Heart Failure Patients Should Get Palliative Care and Who
Matching Patient and Pump in the New Era of Percutaneous Mechanical Circulatory Support
 Matching Patient and Pump in the New Era of Percutaneous Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced
Matching Patient and Pump in the New Era of Percutaneous Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced
Innovative ECMO Configurations in Adults
 Innovative ECMO Configurations in Adults Practice at a Single Center with Platinum Level ELSO Award for Excellence in Life Support Monika Tukacs, BSN, RN, CCRN Columbia University Irving Medical Center,
Innovative ECMO Configurations in Adults Practice at a Single Center with Platinum Level ELSO Award for Excellence in Life Support Monika Tukacs, BSN, RN, CCRN Columbia University Irving Medical Center,
Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know!
: What Every Pharmacist Needs to Know!") Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know! Matthew A. Wanat, PharmD, BCPS, BCCCP, FCCM Clinical Assistant Professor University of Houston College of Pharmacy Clinical Pharmacy
Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know! Matthew A. Wanat, PharmD, BCPS, BCCCP, FCCM Clinical Assistant Professor University of Houston College of Pharmacy Clinical Pharmacy
Thrombolysis in PE. Outline. Disclosure. Overview on Pulmonary Embolism. Hot Topics in Emergency Medicine 2012 Midyear Clinical Meeting
 Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
DEMYSTIFYING VADs. Nicolle Choquette RN MN Athabasca University
 DEMYSTIFYING VADs Nicolle Choquette RN MN Athabasca University Objectives odefine o Heart Failure o VAD o o o o Post Operative Complications Acute Long Term Nursing Interventions What is Heart Failure?
DEMYSTIFYING VADs Nicolle Choquette RN MN Athabasca University Objectives odefine o Heart Failure o VAD o o o o Post Operative Complications Acute Long Term Nursing Interventions What is Heart Failure?
Disclosures. Objectives
 BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
Andrew Civitello MD, FACC
 Timing the Transition from Short Term to Long Term Mechanical Circulatory Support Andrew Civitello MD, FACC Medical Director, Heart Transplant Program Director, Fellowship Co-Director, Baylor St. Luke's
Timing the Transition from Short Term to Long Term Mechanical Circulatory Support Andrew Civitello MD, FACC Medical Director, Heart Transplant Program Director, Fellowship Co-Director, Baylor St. Luke's
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
I Was Too Late With Device Placement
 SCAI SHOCK 2018 A Team-Based Course On Cardiogenic Shock General Session # 2 Saturday, October 13, 2018 8:39 8:51 AM Boston Park Plaza - Boston, MA I Was Too Late With Device Placement M Chadi Alraies,
SCAI SHOCK 2018 A Team-Based Course On Cardiogenic Shock General Session # 2 Saturday, October 13, 2018 8:39 8:51 AM Boston Park Plaza - Boston, MA I Was Too Late With Device Placement M Chadi Alraies,
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Which mechanical assistance for cardiogenic shock?
 Which mechanical assistance for cardiogenic shock? Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre et Marie Curie Sorbonne
Which mechanical assistance for cardiogenic shock? Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre et Marie Curie Sorbonne
Catheter Directed Interventions for Pulmonary Embolism
 Catheter Directed Interventions for Pulmonary Embolism Rabih A. Chaer, MD, MSc Professor of Surgery, UPMC Residency Program Director Site chief, Presbyterian campus Division of Vascular Surgery Pittsburgh,
Catheter Directed Interventions for Pulmonary Embolism Rabih A. Chaer, MD, MSc Professor of Surgery, UPMC Residency Program Director Site chief, Presbyterian campus Division of Vascular Surgery Pittsburgh,
CENTRAL ECMO WHEN AND HOW? RANJIT JOHN, MD UNIVERSITY OF MINESOTA
 CENTRAL ECMO WHEN AND HOW? RANJIT JOHN, MD UNIVERSITY OF MINESOTA Background How to do Case reports When to do Managing complications Post operative management strategies CASE PRESENTATION 46 year old
CENTRAL ECMO WHEN AND HOW? RANJIT JOHN, MD UNIVERSITY OF MINESOTA Background How to do Case reports When to do Managing complications Post operative management strategies CASE PRESENTATION 46 year old
Hemodynamic Monitoring and Circulatory Assist Devices
 Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Mechanical Cardiac Support and Cardiac Transplant: The Role for Echocardiography
 Mechanical Cardiac Support and Cardiac Transplant: The Role for Echocardiography David Langholz, M.D., F.A.C.C. Co-Director Cardiovascular Imaging Fredrick Meijer Heart and Vascular Institute Spectrum
Mechanical Cardiac Support and Cardiac Transplant: The Role for Echocardiography David Langholz, M.D., F.A.C.C. Co-Director Cardiovascular Imaging Fredrick Meijer Heart and Vascular Institute Spectrum
ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS
 ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS DISCLOSURES No financial disclosures or conflicts of interest OBJECTIVES Define ECMO/ECLS and be able to identify the main types
ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS DISCLOSURES No financial disclosures or conflicts of interest OBJECTIVES Define ECMO/ECLS and be able to identify the main types
The Role of ECMO in Thoracic Surgery. Matthew Hartwig, MD
 The Role of ECMO in Thoracic Surgery Matthew Hartwig, MD Disclosure Slide Consultant for Mallincrodkt and Quark Pharmaceuticals Case #1 28 y.o. female with tracheal mass No previous medical or surgical
The Role of ECMO in Thoracic Surgery Matthew Hartwig, MD Disclosure Slide Consultant for Mallincrodkt and Quark Pharmaceuticals Case #1 28 y.o. female with tracheal mass No previous medical or surgical
Venous Thrombosis. Magnitude of the Problem. DVT 2 Million PE 600,000. Death 60,000. Estimated Cost of VTE Care $1.5 Billion/year.
 Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Mechanical ventilation induced or exacerbated right ventricular failure
 Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
ECLS Registry Form Extracorporeal Life Support Organization (ELSO)
") ECLS Registry Form Extracorporeal Life Support Organization (ELSO) Center ID: Center name: Run No (for this patient) Unique ID: Birth Date/Time Sex: (M, F) Race: (Asian, Black, Hispanic, White, Other)
ECLS Registry Form Extracorporeal Life Support Organization (ELSO) Center ID: Center name: Run No (for this patient) Unique ID: Birth Date/Time Sex: (M, F) Race: (Asian, Black, Hispanic, White, Other)
The right heart: the Cinderella of heart failure
 The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
ST-Elevation Myocardial Infarction & Cardiogenic Shock. - What Should We Do?
 ST-Elevation Myocardial Infarction & Cardiogenic Shock - What Should We Do? Advanced Angioplasty 2008 Dan Blackman Leeds General Infirmary Conflicts of interest Advisory Boards Cordis Boston Scientific
ST-Elevation Myocardial Infarction & Cardiogenic Shock - What Should We Do? Advanced Angioplasty 2008 Dan Blackman Leeds General Infirmary Conflicts of interest Advisory Boards Cordis Boston Scientific
Acute heart failure, beyond conventional treatment: persisting low output
 Acute heart failure, beyond conventional treatment: persisting low output Alexandre Mebazaa, FESC Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts
Acute heart failure, beyond conventional treatment: persisting low output Alexandre Mebazaa, FESC Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts
Complications of VAD therapy - RV failure
 Complications of VAD therapy - RV failure Nana Afari-Armah, MD Advanced heart failure and transplant cardiology Temple University Hospital 3/24/18 Goals Understand the role of the right ventricle in LVAD
Complications of VAD therapy - RV failure Nana Afari-Armah, MD Advanced heart failure and transplant cardiology Temple University Hospital 3/24/18 Goals Understand the role of the right ventricle in LVAD
Medical Management of Acute Heart Failure
 Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Cardiogenic Shock. Dr. JPS Henriques. Academic Medical Center University of Amsterdam The Netherlands
 Cardiogenic Shock Dr. JPS Henriques Academic Medical Center University of Amsterdam The Netherlands Conflict of interest disclosure Research grant Abbott Vascular Research grant Abiomed Inc. Global Impella
Cardiogenic Shock Dr. JPS Henriques Academic Medical Center University of Amsterdam The Netherlands Conflict of interest disclosure Research grant Abbott Vascular Research grant Abiomed Inc. Global Impella
Counterpulsation. John N. Nanas, MD, PhD. Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece
 John N. Nanas, MD, PhD Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece History of counterpulsation 1952 Augmentation of CBF Adrian and Arthur Kantrowitz, Surgery 1952;14:678-87
John N. Nanas, MD, PhD Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece History of counterpulsation 1952 Augmentation of CBF Adrian and Arthur Kantrowitz, Surgery 1952;14:678-87
ECMO Experience from ECMO-ICU, Karolinska
 ECMO Experience from ECMO-ICU, Karolinska X Curso de Ventilacion Mecanica en Anestesia, Cuidados Criticos y Transplantes Madrid 2012 International numbers Totally since 1989; 46500 patients as of July
ECMO Experience from ECMO-ICU, Karolinska X Curso de Ventilacion Mecanica en Anestesia, Cuidados Criticos y Transplantes Madrid 2012 International numbers Totally since 1989; 46500 patients as of July
ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient
 ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient Shaf Keshavjee MD MSc FRCSC FACS Surgeon-in-Chief, University Health Network James Wallace McCutcheon Chair in Surgery Director,
ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient Shaf Keshavjee MD MSc FRCSC FACS Surgeon-in-Chief, University Health Network James Wallace McCutcheon Chair in Surgery Director,
HISTORY. Question: How do you interpret the patient s history? CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: 45-year-old man.
 HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
Revision of 10/27/2017 Form #280 Page 1 of 12 PVDOMICS STUDY Clinical Center Right Heart Catheterization (RHC) Results Form #280
 Results Form #280") Revision of 10/27/2017 Form #280 Page 1 of 12 PVDOMICS STUDY Clinical Center Right Heart Catheterization (RHC) Results Form #280 Instructions: Review PVDOMICS MOP Chapter 100 prior to completing right
Revision of 10/27/2017 Form #280 Page 1 of 12 PVDOMICS STUDY Clinical Center Right Heart Catheterization (RHC) Results Form #280 Instructions: Review PVDOMICS MOP Chapter 100 prior to completing right
Καθετηριασμός δεξιάς κοιλίας. Σ. Χατζημιλτιάδης Καθηγητής Καρδιολογίας ΑΠΘ
 Καθετηριασμός δεξιάς κοιλίας Σ. Χατζημιλτιάδης Καθηγητής Καρδιολογίας ΑΠΘ The increasing interest in pulmonary arterial hypertension (PAH), the increasing interest in implantation of LVADs, and the evolution
Καθετηριασμός δεξιάς κοιλίας Σ. Χατζημιλτιάδης Καθηγητής Καρδιολογίας ΑΠΘ The increasing interest in pulmonary arterial hypertension (PAH), the increasing interest in implantation of LVADs, and the evolution
Disclosure Information : No conflict of interest
 Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year
![Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year](/thumbs/76/74263761.jpg "Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year") PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS.
 RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: Physicians managing adult patients with massive and submassive pulmonary emboli in the
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: Physicians managing adult patients with massive and submassive pulmonary emboli in the
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Cite this article as:
 doi: 10.21037/acs.2018.08.06 Cite this article as: Loforte A, Baiocchi M, Gliozzi G, Coppola G, Di Bartolomeo R, Lorusso R. Percutaneous pulmonary artery venting via jugular vein while on peripheral extracorporeal
doi: 10.21037/acs.2018.08.06 Cite this article as: Loforte A, Baiocchi M, Gliozzi G, Coppola G, Di Bartolomeo R, Lorusso R. Percutaneous pulmonary artery venting via jugular vein while on peripheral extracorporeal