CLASIFICATION OF ACUTE HEART FAILURE
|
|
|
- Willis Craig
- 6 years ago
- Views:
Transcription




1

2

3


4
5 CLASIFICATION OF ACUTE HEART FAILURE CLINICAL STATUS HR SBP mmhg CI L/min/m 2 PCWP mmhg Congestion Killip/Forrester Diuresis Hupoperfusion End-organ hypoperfusion I. Acute decompensated CHF +/ Low normal /High Low normal /High Mild elevation K II/F II + +/ II. Acute HF with hypertension III. Acute HF with pulmonary oedema + IVa. Cardiogenic shock*/low output syndrome + Usually increased High +/ >18 K II-IV/FII-III +/ +/ Low normal Low Elevated KIII/FII + +/ Low normal Low, <2.2 >16 K III-IV/F I-III low + + IVb. Severe cardiogenic shock >90 <90 <1.8 >18 K IV/F IV Very low , with CNS symptoms V. High output HF + +/ + +/ KII/FI-II + VI Acute rightheart failure Usually low Low Low Low F I +/ +/, acute onset +/ Legend:*differentiation of low cardiac output syndrome is subjective; SBP=systolic blood pressure; CI=cardiac index; PCWP=pulmonary capillary wedge pressure; CNS
6 ICU hospitalisations 3400 % of total Mortality rate (%) AHF ,5 9,1% AHF type Prevalence of AHF % Mortality rate I. Acute decompensated CHF II. Acute HF with hypertension III. Acute HF with pulmonary oedema IVb. Severe cardiogenic shock VI. Acute rightheart failure ,2 25 (23,6%) 52 13,3 3 (5,8%) ,3 17 (10,1%) 52 13,3 35 (67,3%) 11 2,8 3(27,3%)
7 Events leading to rapid deterioration Rapid arrhythmia or severe bradycardia/conduction disturbances Acute coronary syndrome Mechanical complication of acute coronary syndrome (rupture of IVS, mitral valve chordal rupture, right ventricular infarction) Acute pulmonary embolism Hypertensive crysis Aortic dissection Surgery and perioperative problems Peripartum cardiomyopathy Events leading to less rapid deterioration Infective endocarditis Anaemia Kidney dyssfunction Non-atherence to diet/drug therapy Iatrogenic causes (drug interactions) Arrhythmia/bradycardia/conduction disturbances Uncontrolled hypertension Hyperthyroidism or hypothyroidism Alcohol and drug abuse
8 The diagnosis of ADHF should be based primarily on signs and symptoms. Strength of Evidence = C When the diagnosis is uncertain, determination of BNP or NT-proBNP concentration is recommended in patients being evaluated for dyspnea who have signs and symptoms compatible with HF. Strength of Evidence = A The natriuretic peptide concentration should not be interpreted in isolation, but in the context of all available clinical data, and with the knowledge of cardiac and noncardiac factors that can raise it s levels.
9 Authors/Task Force Members et al. Eur Heart J 2012;33:
10 Hospital admission is recommended when: Evidence of severely decompensated HF, including: Hypotension Worsening renal failure Altered mentation Dyspnea at rest Typically reflected by resting tachypnea Less commonly reflected by oxygen saturation < 90% Hemodynamically significant arrhythmia Including new onset of rapid atrial fibrillation Acute coronary syndromes Strength of Evidence = C Hospital admission should be considered when: Worsened congestion Signs and symptoms of pulmonary or systemic congestion Major electrolyte disturbance Associated co morbid conditions Pneumonia, pulmonary embolus, diabetic ketoacidosis, symptoms suggestive of TIA or stroke Repeated ICD firings Previously undiagnosed HF with signs and symptoms of systemic or pulmonary congestion Strength of Evidence = C

11 Improve symptoms, especially congestion and low output symptoms Restore normal oxygenation Optimize volume status Identify etiology Identify and address precipitating factors Optimize chronic oral therapy Minimize side effects Identify patients who might benefit from revascularization or device therapy Identify risk of thromboembolism and need for anticoagulant therapy Educate patients concerning medications and self assessment of HF Consider and where possible, initiate a disease management program

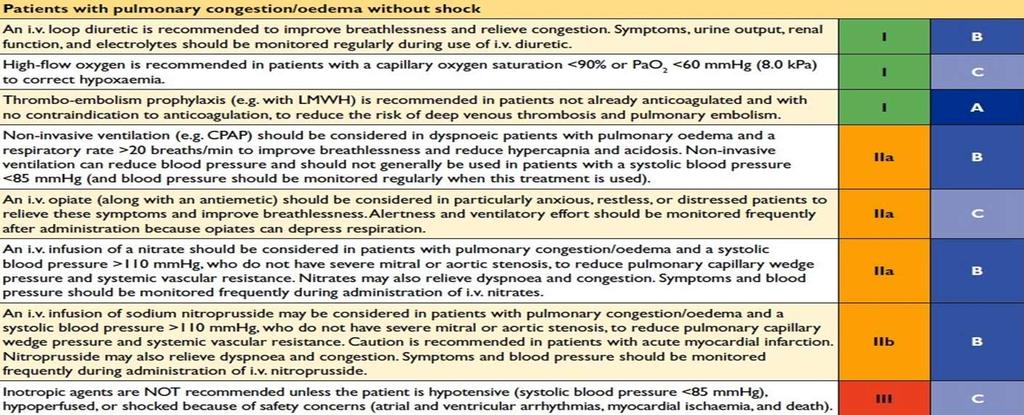
12 Authors/Task Force Members et al. Eur Heart J 2012;33: INITIAL THERAPY: 1. DIURETIC therapy 2. OXYGEN therapy Routine administration of supplemental oxygen: Is recommended in the presence of hypoxia saturation <90% or PAo2 <8,0 kpa Is not recommended in the absence of hypoxia Strength of Evidence = C (NEW in 2010) Use of non-invasive positive pressure ventilation may be considered for severely dyspnoic patients with clinical evidence of pulmonary edema. Strength of Evidence = C 3. MORPHINE mg of plus 10 mg metoclopramide, repeat as needed DEPENDING ON THE RESPONSE: Start an i.v. infusion of DOBUTAMINE 2.5 μg/kg/min, doubling dose every 15 min according to response or tolerability. A dose >20 μg/kg/min is rarely needed. Start i.v. infusion of NTG 10 g/min and doubled every 10 min depending on response and tolerability. Dose> 100 g/min is rarely necessary APPROPRIATE RESPONSE: reducing breathlessness, adequate diuresis (>100 ml/hour urine within the first 2 hours), increased oxygen saturation, improved organ perfusion, reduced HR and respiratory frequency after 1-2 hours of treatment.

13 It is recommended that patients with ADHF and evidence of fluid overload be treated initially with loop diuretics given i.v. (Strength of Evidence=B ) It is recommended diuretics to be administered: (Strength of Evidence=C) at doses needed to produce a rate of diuresis sufficient to achieve optimal volume status with relief of signs and symptoms of congestion (edema, elevated JVP, dyspnea) without inducing an excessively rapid reduction in: intravascular volume (which may result in symptomatic hypotension and/or worsening renal function) or serum electrolytes (which may precipitate arrhythmias or muscle cramps) In patients already on DTh-2,5 higher dose is recommended, to be repeated if necessary Patients should undergo routine laboratory studies and clinical examination Careful observation for development of a side effects (renal dysfunction, electrolyte abnormalities, symptomatic hypotension) is recommended It is recommended that serum potassium and magnesium levels be monitored at least daily and maintained in the normal range. Careful observation for the development of renal dysfunction is recommended in patients treated with diuretics. Patients with moderate to severe renal dysfunction and evidence of fluid retention should continue to be treated with diuretics, because in the presence of severe fluid overload, renal dysfunction may improve with diuresis. B Thyazides are not recomended if estimated GFR is <30 ml/min, except when prescribed synergistically with loop diuretics. C Indapamide is a non-thiazide sulfonamide. D A mineralocorticoid antagonist (MRA) spironolactone/eplerenone
 2.")
14 Authors/Task Force Members et al. Eur Heart J 2012;33: Doubling the dose of loop diuretic furosemide 500 mg equivalent (doses of 250 mg and higher should be given in the form of infusion over 4 h) 2. In the absence of a response start IV infusion of dopamine 2,5 g/kg/min. Higher doses are not recommended to enhance diuresis 3. In the absence of adequate diuresis in a patient who remains in pulmonary edema, veno-venous ultrafiltration Other alternatives: Strength of Evidence = C Continuous infusion of a loop diuretic Addition of a second type of diuretic orally (metolazone or spironolactone) or intravenously (chlorothiazide) Restricting sodium and fluid DEPENDING ON THE RESPONSE: Unappropriate response: <100 ml/h diuresis more than 1-2 hours is inadequate initial response IV diuretic In patients with: persistently low blood pressure / shock, think about alternative diagnoses, pulmonary arterial catheterization in order to identify inappropriate leftventricular filling pressure and adjustment of vasoactive therapy Absence/low diuresis:strength of Evidence = C
 Particularly if these patients: Have marginal systolic blood pressure (<90 mm Hg), Have symptomatic hypotension despite adequate filling pressure, Or are")
15 Intravenous inotropes (milrinone or dobutamine) may be considered to relieve symptoms and improve end-organ function in patients with: LV dilation Reduced LVEF And diminished peripheral perfusion or endorgan dysfunction (low output syndrome) Particularly if these patients: Have marginal systolic blood pressure (<90 mm Hg), Have symptomatic hypotension despite adequate filling pressure, Or are unresponsive to, or intolerant of, intravenous vasodilators. Intravenous inotropes (milrinone or dobutamine) are not recommended unless left heart filling pressures are known to be elevated or cardiac index is severely impaired based on direct measurement or clear clinical signs. It is recommended that administration of intravenous inotropes (milrinone or dobutamine) in the setting of ADHF be accompanied by continuous or frequent blood pressure monitoring and continuous monitoring of cardiac rhythm. If symptomatic hypotension or worsening tachyarrhythmias develop during administration of these agents, discontinuation or dose reduction should be considered.

16 In the absence of symptomatic hypotension, i.v. nitroglycerin, nitroprusside or nesiritide may be considered as an addition to diuretic therapy for rapid improvement of congestive symptoms in patients admitted with ADHF. Strength of Evidence = B Frequent blood pressure monitoring is recommended with these agents. Strength of Evidence = B These agents should be decreased in dosage or discontinued if symptomatic hypotension or worsening renal function develops. Strength of Evidence =B Reintroduction in increasing doses may be considered once symptomatic hypotension is resolved. Strength of Evidence=C IV vasodilators (intravenous nitroglycerin or nitroprusside) and diuretics are recommended for rapid symptom relief in patients with acute pulmonary edema or severe hypertension. Strength of Evidence=C Intravenous vasodilators may be considered in patients with ADHF who have persistent severe HF despite aggressive treatment with diuretics and standard oral therapies. Nitroprusside Strength of Evidence=B Nitroglycerine, nesiritide Strength of Evidence=C
17 Frequency Value Specifics At least daily Weight Determine after voiding in the morning Account for possible increased food intake due to improved appetite At least daily Fluid intake and output Monitoring of daily weights, intake, and output is recommended to assess clinical efficacy of diuretic therapy. Routine use of a Foley catheter is not recommended for monitoring volume status. However, placement of a catheter is recommended when close monitoring of urine output is needed or if a bladder outlet obstruction is suspected of contributing to worsening renal function. More than daily Vital signs Orthostatic blood pressure, if indicated Oxygen saturation daily until stable At least daily Signs Edema, ascites, pulmonary rales, hepatomegaly, increased jugular venous pressure, hepatojugular reflux, liver tenderness At least daily Symptoms Orthopnea, paroxysmal nocturnal dyspnea or cough, nocturnal cough, dyspnea, fatigue, lightheadedness At least daily Electrolytes Potassium, sodium At least daily Renal function BUN, serum creatinine
18 The routine use of invasive hemodynamic monitoring in patients with ADHF is not recommended. Strength of Evidence = A Invasive hemodynamic monitoring should be considered in a patient: Who is refractory to initial therapy Whose volume status and cardiac filling pressures are unclear Who has clinically significant hypotension (typically SBP < 80 mm Hg) or worsening renal function during therapy Or who is being considered for cardiac transplant and needs assessment of degree and reversability of pulmonary hypertension Or in whom documentation of an adequate hemodynamic response to the inotropic agent is necessary when chronic outpatient infusion is being considered Strength of Evidence = C
19 (NEW in 2010) Venous thromboembolism prophylaxis with low dose unfractionated heparin, low molecular weight heparin or fondaparinux to prevent proximal deep venous thrombosis and pulmonary embolism is recommended for patients who are admitted to hospital with ADHF and who are not already anticoagulated and have no contraindication to anticoagulation. Strength of Evidence = B Venous thromboembolism prophylaxis with a mechanical device (intermittent pneumatic compression devices or graded compression stockings ) to prevent proximal deep venous thrombosis and pulmonary embolism should be considered for patients who are admitted to the hospital with ADHF, who are not already anticoagulated, and who have a contraindication to anticoagulation. Strength of Evidence = C
20 FLUID RESTRICTION (<2 L/daily): Is recommended in patients with moderate hyponatremia (serum sodium < 130 meq/l) Should be considered to assist in treatment of fluid overload in other patients. Strength of Evidence = C In patients with severe (serum sodium < 125 meq/l) or worsening hyponatremia, stricter fluid restriction may be considered. Strength of Evidence = C SODIUM RESTRICTION A low sodium diet (2 g daily) is recommended for most hospitalized patients. Strength of Evidence = C In patients with recurrent or refractory volume overload, stricter sodium restriction may be considered. Strength of Evidence = C
21

22

23
24
25 Recommended for all HF patients Strength of Evidence = C Should be considered for patients with advanced HF or recurrent admissions for HF Strength of Evidence = C Exacerbating factors addressed Near optimal volume status observed Transition from intravenous to oral diuretic successfully completed Patient and family education completed, including clear discharge instructions Near optimal pharmacologic therapy achieved, including ACEI and BB (for patients with reduced LVEF) or intolerance documented Follow-up clinic visit scheduled, usually for 7-10 days Oral medication regimen stable for 24 hours No intravenous vasodilator or inotropic agent for 24 hours Ambulation prior to discharge to assess functional capacity after therapy Plans for post-discharge management (scale present in home, visiting nurse or telephone follow up generally no longer than 3 days after discharge) Referral for disease management, if available
26 It is recommended that every effort be made to utilize the hospital stay for assessment and improvement of patient adherence via patient and family education and social support services. Strength of Evidence = B DISCHARGE PLANNING is recommended as part of the management of patients with ADHF. Discharge planning should address the following issues: Details regarding medication, dietary sodium restriction and recommended activity level Follow-up by phone or clinic visit early after discharge to reassess volume status Medication and dietary compliance Alcohol moderation and smoking cessation Monitoring of body weight, electrolytes and renal function Consideration of referral for formal disease management Strength of Evidence = C
27 QUESTIONS/ DISSCUSION
Medical Management of Acute Heart Failure
 Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Section 12: Evaluation and Management of Patients With Acute Decompensated Heart Failure
 Journal of Cardiac Failure Vol. 12 No. 1 2006 Section 12: Evaluation and Management of Patients With Acute Decompensated Heart Failure Overview Acute decompensated heart failure (ADHF) has emerged as a
Journal of Cardiac Failure Vol. 12 No. 1 2006 Section 12: Evaluation and Management of Patients With Acute Decompensated Heart Failure Overview Acute decompensated heart failure (ADHF) has emerged as a
Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year
![Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year](/thumbs/76/74263761.jpg "Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year") PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
Integrating Current Knowledge into Consensus Guidelines for Acute Decompensated Heart Failure
 Integrating Current Knowledge into Consensus Guidelines for Acute Decompensated Heart Failure J. Herbert Patterson, Pharm.D., FCCP One of Four Continuing Education Programs in the Series, Acute Decompensated
Integrating Current Knowledge into Consensus Guidelines for Acute Decompensated Heart Failure J. Herbert Patterson, Pharm.D., FCCP One of Four Continuing Education Programs in the Series, Acute Decompensated
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%
 with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%") Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
Management of Acute Heart Failure
 Management of Acute Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu ADHF Treatments Goals.2 Improve symptoms.
Management of Acute Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu ADHF Treatments Goals.2 Improve symptoms.
Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes?
 Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor
Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance
 Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
Heart Failure: Guideline-Directed Management and Therapy
 Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Management of acute decompensated heart failure and cardiogenic shock. Arintaya Phrommintikul Department of Medicine CMU
 Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Medical Management of Acutely Decompensated Heart Failure. William T. Abraham, MD Director, Division of Cardiovascular Medicine
 Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
ACUTE HEART FAILURE. Julie Gorchynski MD, MSc, FACEP, FAAEM. Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014
 ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
Diagnosis & Management of Heart Failure. Abena A. Osei-Wusu, M.D. Medical Fiesta
 Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
CASE STUDIES IN ADVANCED HEART FAILURE
 CASE STUDIES IN ADVANCED HEART FAILURE Navin Rajagopalan, MD Director, Congestive Heart Failure Medical Director, Cardiac Transplantation Gill Heart Institute, Cardiovascular Medicine DISCLOSURES NOTHING
CASE STUDIES IN ADVANCED HEART FAILURE Navin Rajagopalan, MD Director, Congestive Heart Failure Medical Director, Cardiac Transplantation Gill Heart Institute, Cardiovascular Medicine DISCLOSURES NOTHING
CLINICAL PRACTICE GUIDELINE
 CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
Pivotal Role of Renal Function in Acute Heart failure
 Pivotal Role of Renal Function in Acute Heart failure Doron Aronson MD, FESC Department of Cardiology RAMBAM Health Care Campus Haifa, Israel Classification and definitions of cardiorenal syndromes CRS
Pivotal Role of Renal Function in Acute Heart failure Doron Aronson MD, FESC Department of Cardiology RAMBAM Health Care Campus Haifa, Israel Classification and definitions of cardiorenal syndromes CRS
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
ACUTE HEART FAILURE in the ED. Pr. Samir Nouira Emergency Department Fattouma Bourguiba University Hospital Monastir Tunisia
 ACUTE HEART FAILURE in the ED Pr. Samir Nouira Emergency Department Fattouma Bourguiba University Hospital Monastir Tunisia ACUTE HEART FAILURE 80% Acute Heart Failure Syndrome Sensitivity Specificity
ACUTE HEART FAILURE in the ED Pr. Samir Nouira Emergency Department Fattouma Bourguiba University Hospital Monastir Tunisia ACUTE HEART FAILURE 80% Acute Heart Failure Syndrome Sensitivity Specificity
Intravenous Inotropic Support an Overview
 Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
They may forget your name, but they will never forget how you made them feel.
 Relax and Learn at the Farm 2013 Presented By DNP, RN, CCNS, CCRN-CMC, CHFN Cardiovascular Nursing Education Associations 1 They may forget your name, but they will never forget how you made them feel.
Relax and Learn at the Farm 2013 Presented By DNP, RN, CCNS, CCRN-CMC, CHFN Cardiovascular Nursing Education Associations 1 They may forget your name, but they will never forget how you made them feel.
The Art and Science of Diuretic therapy
 The Art and Science of Diuretic therapy Dr. Fayez EL Shaer Associate Professour of cardiology Consultant cardiologist MD, MSc, PhD, CBNC, NBE FESC, ACCP, FASNC,HFA KKUH, KFCC Heart failure: fluid overload
The Art and Science of Diuretic therapy Dr. Fayez EL Shaer Associate Professour of cardiology Consultant cardiologist MD, MSc, PhD, CBNC, NBE FESC, ACCP, FASNC,HFA KKUH, KFCC Heart failure: fluid overload
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration
![ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration](/thumbs/77/76069192.jpg "ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration") ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF
 CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
Heart Failure Management Policy and Procedure Phase 1
 1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
Contents DEFINITION. TYPES EPIDEMIOLOGY PATHOPHYSIOLOGY. CLINICAL PRESENTATION. DIAGNOSIS. TREATMENT. EVALUATION OF THERAPEUTIC OUTCOMES.
 Heart Failure Contents DEFINITION. TYPES EPIDEMIOLOGY PATHOPHYSIOLOGY. CLINICAL PRESENTATION. DIAGNOSIS. TREATMENT. EVALUATION OF THERAPEUTIC OUTCOMES. DEFINITION Heart failure (HF) is a progressive clinical
Heart Failure Contents DEFINITION. TYPES EPIDEMIOLOGY PATHOPHYSIOLOGY. CLINICAL PRESENTATION. DIAGNOSIS. TREATMENT. EVALUATION OF THERAPEUTIC OUTCOMES. DEFINITION Heart failure (HF) is a progressive clinical
HEART FAILURE PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
Assessment and Diagnosis of Heart Failure
 Assessment and Diagnosis of Heart Failure Heart failure (HF) is a complex clinical syndrome resulting from any structural or functional impairment of ventricular filling or ejection of blood and is characterized
Assessment and Diagnosis of Heart Failure Heart failure (HF) is a complex clinical syndrome resulting from any structural or functional impairment of ventricular filling or ejection of blood and is characterized
Cardiorenal Syndrome: What the Clinician Needs to Know. William T. Abraham, MD Director, Division of Cardiovascular Medicine
 Cardiorenal Syndrome: What the Clinician Needs to Know William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Renal Hemodynamics in Heart Failure Glomerular
Cardiorenal Syndrome: What the Clinician Needs to Know William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Renal Hemodynamics in Heart Failure Glomerular
Heart Failure. Jay Shavadia
 Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept
 Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Estimated 5.7 million Americans with HF. 915, 000 new HF cases annually, HF incidence approaches
 Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Practical Points in Cardiorenal Syndrome
 Practical Points in Cardiorenal Syndrome Vichai Senthong, MD. Cardiovascular Unit, Faculty of Medicine Khon Kaen university HFCT Annual Scientific Meeting June 16, 2017, Eastin Grand Sathorn Hotel, Bangkok
Practical Points in Cardiorenal Syndrome Vichai Senthong, MD. Cardiovascular Unit, Faculty of Medicine Khon Kaen university HFCT Annual Scientific Meeting June 16, 2017, Eastin Grand Sathorn Hotel, Bangkok
Incidence. 4.8 million in the United States. 400,000 new cases/year. 20 million patients with asymptomatic LV dysfunction
 Heart Failure Diagnosis According to the Working Group in Heart Failure, CHF is a syndrome where the diagnosis has the following essential components: A combination of: Symptoms, typically breathlessness
Heart Failure Diagnosis According to the Working Group in Heart Failure, CHF is a syndrome where the diagnosis has the following essential components: A combination of: Symptoms, typically breathlessness
Heart Failure CTSHP Fall Seminar
 Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe
Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe
Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment
 ESC 2012 27Aug - 3Sep, 2012, Munich, Germany Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment Marco Metra, MD, FESC Cardiology University
ESC 2012 27Aug - 3Sep, 2012, Munich, Germany Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment Marco Metra, MD, FESC Cardiology University
Tri-City Cardiology Consultants FIFTH ANNUAL SYMPOSIUM
 Tri-City Cardiology Consultants FIFTH ANNUAL SYMPOSIUM Faculty Disclosure Banner Baywood Medical Center -Chief of Staff FIFTH ANNUAL SYMPOSIUM NYHA class III-IV symptoms Clinical signs of fluid retention
Tri-City Cardiology Consultants FIFTH ANNUAL SYMPOSIUM Faculty Disclosure Banner Baywood Medical Center -Chief of Staff FIFTH ANNUAL SYMPOSIUM NYHA class III-IV symptoms Clinical signs of fluid retention
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
Nesiritide: Harmful or Harmless?
 Nesiritide: Harmful or Harmless? Michael P. Dorsch, Pharm.D., and Jo Ellen Rodgers, Pharm.D. Nesiritide is the recombinant form of human B-type (brain) natriuretic peptide (BNP), and its amino acid sequence
Nesiritide: Harmful or Harmless? Michael P. Dorsch, Pharm.D., and Jo Ellen Rodgers, Pharm.D. Nesiritide is the recombinant form of human B-type (brain) natriuretic peptide (BNP), and its amino acid sequence
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 3/2/2014
 3/2/2014") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Acute heart failure, beyond conventional treatment: persisting low output
 Acute heart failure, beyond conventional treatment: persisting low output Alexandre Mebazaa, FESC Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts
Acute heart failure, beyond conventional treatment: persisting low output Alexandre Mebazaa, FESC Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts
Heart Failure. Dr. Alia Shatanawi
 Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Question by Question (QXQ) Instructions for the HCHS/SOL Heart Failure Diagnosis Form (HFD)
 Instructions for the HCHS/SOL Heart Failure Diagnosis Form (HFD)") Question by Question (QXQ) Instructions for the HCHS/SOL Heart Failure Diagnosis Form (HFD) A Heart Failure Diagnosis (HFD) Form is filled out by the reviewer for all case packets that are sent to them
Question by Question (QXQ) Instructions for the HCHS/SOL Heart Failure Diagnosis Form (HFD) A Heart Failure Diagnosis (HFD) Form is filled out by the reviewer for all case packets that are sent to them
Disclosures. Objectives 10/11/17. Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock. I have no disclosures to report
 Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Proposed Health Technology Appraisal. Serelaxin for treating acute decompensation of heart failure
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Proposed Health Technology Appraisal Serelaxin for treating acute decompensation of heart Draft scope (pre-referral) Draft remit/appraisal objective To
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Proposed Health Technology Appraisal Serelaxin for treating acute decompensation of heart Draft scope (pre-referral) Draft remit/appraisal objective To
Drugs Used in Heart Failure. Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia
 Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to
Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
MANAGEMENT OF ACUTE PULMONARY EDEMA. Pr. NOUIRA Semir Emergency Department Fattouma Bourguiba University Hospital
 MANAGEMENT OF ACUTE PULMONARY EDEMA Pr. NOUIRA Semir Emergency Department Fattouma Bourguiba University Hospital ACUTE HEART FAILURE 35% 10% Goals of Acute Management Rapidly improve symptoms while preserving
MANAGEMENT OF ACUTE PULMONARY EDEMA Pr. NOUIRA Semir Emergency Department Fattouma Bourguiba University Hospital ACUTE HEART FAILURE 35% 10% Goals of Acute Management Rapidly improve symptoms while preserving
Professional Development Presents. May 2016 Medication of the Month. Milrinone Drip IN2731
 Med of the Month For any question regarding May 2016 Med of the Month: Milrinone Drip You may contact: Sherr Ann Arabit MSN, RN-BC, CCRN/Professional Development Department Ext 4196 Professional Development
Med of the Month For any question regarding May 2016 Med of the Month: Milrinone Drip You may contact: Sherr Ann Arabit MSN, RN-BC, CCRN/Professional Development Department Ext 4196 Professional Development
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction
 Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction Masahito Shigekiyo, Kenji Harada, Ayumi Okada, Naho Terada, Hiroyoshi Yoshikawa, Akira Hirono,
Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction Masahito Shigekiyo, Kenji Harada, Ayumi Okada, Naho Terada, Hiroyoshi Yoshikawa, Akira Hirono,
Acute heart failure syndromes: clinical challenges. Pathophysiology. ESC Congress August. Paris, France. Marco Metra
 ESC Congress 2011 27-31 August. Paris, France. Acute heart failure syndromes: clinical challenges. Pathophysiology Marco Metra Cardiology, Dept. Of experimental and applied medicine. University of Brescia.
ESC Congress 2011 27-31 August. Paris, France. Acute heart failure syndromes: clinical challenges. Pathophysiology Marco Metra Cardiology, Dept. Of experimental and applied medicine. University of Brescia.
Disclosure Information : No conflict of interest
 Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Management of Advanced Systolic Heart Failure. Robert W. Hull MD FACC Associate Professor of Medicine West Virginia University
 Management of Advanced Systolic Heart Failure Robert W. Hull MD FACC Associate Professor of Medicine West Virginia University American College of Cardiology Foundation (ACCF) American Heart Association
Management of Advanced Systolic Heart Failure Robert W. Hull MD FACC Associate Professor of Medicine West Virginia University American College of Cardiology Foundation (ACCF) American Heart Association
State-of-the-Art Management of Chronic Systolic Heart Failure
 State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency
 Application of ICG in Intensive Care and Emergency") Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
Topic Page: congestive heart failure
 Topic Page: congestive heart failure Definition: congestive heart f ailure from Merriam-Webster's Collegiate(R) Dictionary (1930) : heart failure in which the heart is unable to maintain an adequate circulation
Topic Page: congestive heart failure Definition: congestive heart f ailure from Merriam-Webster's Collegiate(R) Dictionary (1930) : heart failure in which the heart is unable to maintain an adequate circulation
Cor pulmonale. Dr hamid reza javadi
 1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
Case Presentation. This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
 Worsening Renal Function in Heart Failure Patients Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
Worsening Renal Function in Heart Failure Patients Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland
 2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland Disclosures Consultancy fees and speaker s honoraria from: Amgen, Servier, Novartis, Johnson & Johnson, Merck, Berlin Chemie,
2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland Disclosures Consultancy fees and speaker s honoraria from: Amgen, Servier, Novartis, Johnson & Johnson, Merck, Berlin Chemie,
State of the Art: acute heart failure Is it just congestion?
 ESC CONGRESS 2017 Barcelona, 26. 30. August 2017 State of the Art: acute heart failure Is it just congestion? S.B. Felix, FESC Klinik für Innere Medizin B Ernst-Moritz-Arndt-Universität Greifswald 1456
ESC CONGRESS 2017 Barcelona, 26. 30. August 2017 State of the Art: acute heart failure Is it just congestion? S.B. Felix, FESC Klinik für Innere Medizin B Ernst-Moritz-Arndt-Universität Greifswald 1456
Heart Failure and Renal Failure. Gerasimos Filippatos, MD, FESC, FHFA President HFA
 Heart Failure and Renal Failure Gerasimos Filippatos, MD, FESC, FHFA President HFA Definition Epidemiology Pathophysiology Management (?) Recommendations for NHLBI in cardiorenal interactions related to
Heart Failure and Renal Failure Gerasimos Filippatos, MD, FESC, FHFA President HFA Definition Epidemiology Pathophysiology Management (?) Recommendations for NHLBI in cardiorenal interactions related to
Congestive Heart Failure Patient Profile. Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption
 Congestive Heart Failure Patient Profile Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption Chief Complaint - SOB - When asked: Increasing difficulty
Congestive Heart Failure Patient Profile Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption Chief Complaint - SOB - When asked: Increasing difficulty
EHMRG SCORE STUDY version 6.2; date: 11Jul11 PI: Dr. Douglas Lee. Study Background
 EHMRG SCORE STUDY version 6.2; date: 11Jul11 PI: Dr. Douglas Lee Study Background Heart failure (HF) is a leading cause of morbidity and cardiovascular mortality. The burden of HF has increased over time
EHMRG SCORE STUDY version 6.2; date: 11Jul11 PI: Dr. Douglas Lee Study Background Heart failure (HF) is a leading cause of morbidity and cardiovascular mortality. The burden of HF has increased over time
The Treatment Targets in Acute Decompensated Heart Failure
 SUCCESS WITH HEART FAILURE The Treatment Targets in Acute Decompensated Heart Failure Gregg C. Fonarow, MD The Ahmanson-UCLA Cardiomyopathy Center, Division of Cardiology, UCLA School of Medicine, Los
SUCCESS WITH HEART FAILURE The Treatment Targets in Acute Decompensated Heart Failure Gregg C. Fonarow, MD The Ahmanson-UCLA Cardiomyopathy Center, Division of Cardiology, UCLA School of Medicine, Los
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation
 Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
Nitroglycerin and Heparin Drip Interfacility Protocols
 Nitroglycerin and Heparin Drip Interfacility Protocols EMS Protocol This protocol applies to nitroglycerin and Heparin drips that are initiated at the transferring facility prior to transport and are not
Nitroglycerin and Heparin Drip Interfacility Protocols EMS Protocol This protocol applies to nitroglycerin and Heparin drips that are initiated at the transferring facility prior to transport and are not
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Heart failure hospitalizations with preserved or reduced ejection fraction
 Clinical profile and in-hospital outcomes in patients admitted for heart failure with preserved or reduced ejection fraction. EPI-CARDIO prospective registry Tajer, C; Mariani, J; de Abreu, M; Charask,
Clinical profile and in-hospital outcomes in patients admitted for heart failure with preserved or reduced ejection fraction. EPI-CARDIO prospective registry Tajer, C; Mariani, J; de Abreu, M; Charask,
How to define the target population?
 Heart Failure 2011 22-24 May. Gothenburg, Sweden Mortality or morbidity as target in acute heart failure trials How to define the target population? Marco Metra, Brescia The Burden of Acute HF Acute HF
Heart Failure 2011 22-24 May. Gothenburg, Sweden Mortality or morbidity as target in acute heart failure trials How to define the target population? Marco Metra, Brescia The Burden of Acute HF Acute HF
Intravenous Infusions
 Intravenous Infusions 1) An IV insulin infusion can be used for patients: a) with out of control diabetes b) with DKA (Diabetic Ketoacidosis) c) after a heart attack 2) Hyperglycemia is an adaptive response
Intravenous Infusions 1) An IV insulin infusion can be used for patients: a) with out of control diabetes b) with DKA (Diabetic Ketoacidosis) c) after a heart attack 2) Hyperglycemia is an adaptive response
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Hyponatremia in Heart Failure: why it is important and what should we do about it?
 Objectives Hyponatremia in Heart Failure: why it is important and what should we do about it? Pathophysiology of sodium and water retention in heart failure Hyponatremia in heart failure (mechanism and
Objectives Hyponatremia in Heart Failure: why it is important and what should we do about it? Pathophysiology of sodium and water retention in heart failure Hyponatremia in heart failure (mechanism and
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
ACC Heart Failure Guidelines Slide Set
 ACC Heart Failure Guidelines Slide Set Based on the 2009 Focused Update ncorporated nto the ACCF/AHA 2005 guidelines for the Diagnosis and Management of Heart Failure in Adults: A Report of the American
ACC Heart Failure Guidelines Slide Set Based on the 2009 Focused Update ncorporated nto the ACCF/AHA 2005 guidelines for the Diagnosis and Management of Heart Failure in Adults: A Report of the American
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Overcoming the Cardiorenal Syndrome
 Overcoming the Cardiorenal Syndrome October 29, 2016 Randall C Starling MD MPH FACC FESC FHFSA FHFA Professor of Medicine Heart & Vascular Institute Cleveland Clinic Lerner College of Medicine Cleveland
Overcoming the Cardiorenal Syndrome October 29, 2016 Randall C Starling MD MPH FACC FESC FHFSA FHFA Professor of Medicine Heart & Vascular Institute Cleveland Clinic Lerner College of Medicine Cleveland
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure
 New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure Deborah Budge, MD Intermountain Healthcare Heart Failure Cardiologist Objectives: State the updates from the ACC 2013 HF
New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure Deborah Budge, MD Intermountain Healthcare Heart Failure Cardiologist Objectives: State the updates from the ACC 2013 HF
5 Important Things to Know About Heart Failure. Kia Afshar, MD
 5 Important Things to Know About Heart Failure Kia Afshar, MD Disclosures I have no conflicts of interest to disclose I will not be discussing any off label medications and/or devices Objectives 1) Understand
5 Important Things to Know About Heart Failure Kia Afshar, MD Disclosures I have no conflicts of interest to disclose I will not be discussing any off label medications and/or devices Objectives 1) Understand
The right heart: the Cinderella of heart failure
 The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong
 Pol.Col.Dr.Kasem Ratanasumawong") Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong Management of valvular heart disease Accurate diagnosis and disease severity Prevention and treatment
Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong Management of valvular heart disease Accurate diagnosis and disease severity Prevention and treatment
Chapter 10. Learning Objectives. Learning Objectives 9/11/2012. Congestive Heart Failure
 Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
Peripartum Cardiomyopathy. Lavanya Rai Manipal
 Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Meet the experts: Cardiogenic Shock
 Meet the experts: Cardiogenic Shock Inotropes: effects on the heart, the microcirculation and other organs ACCA Masterclass 2017 Alessandro Sionis Director Acute & Intensive Cardiac Care Unit Hospital
Meet the experts: Cardiogenic Shock Inotropes: effects on the heart, the microcirculation and other organs ACCA Masterclass 2017 Alessandro Sionis Director Acute & Intensive Cardiac Care Unit Hospital