How to Reduce Residual Risk in Primary Prevention
|
|
|
- Augustine Chase
- 6 years ago
- Views:
Transcription


1 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA
 AFCAPS (1998) LIPID (1998) HPS (2002) ASCOT-LLA (2003) TNT, 10 (2005) TNT, 80 (2005) 5 0 210 190 170 150 130 110 90 70 Closed symbols = statin group; open symbols = placebo group Mean LDL-C")
2 Patients with CHD Event (%) Lower Is Better : Statin Therapy Provides Benefits Even in Patients with Lower LDL-C 30 Secondary prevention Primary prevention S (1994) WOSCOPS (1995) CARE (1996) AFCAPS (1998) LIPID (1998) HPS (2002) ASCOT-LLA (2003) TNT, 10 (2005) TNT, 80 (2005) Closed symbols = statin group; open symbols = placebo group Mean LDL-C Level at Follow-up (mg/dl) Adapted from Kastelein JJP. Atherosclerosis. 1999;143(suppl 1):S17-S21. Sever PS, et al. Lancet. 2003;361: HPS. Lancet. 2002;360:7-22. LaRosa JC, et al. N Engl J Med. 2005;352:1-11.

3 LDL cholesterol 3.36mmol/L 4.14mmol/L
 16% RR (P = 0.")
 5 0 0 3 6 9 12 15 18 21 24 27 30 Ridker PM et al.")
4 30 25 PROVE IT - TIMI 22: All-Cause Death or Major CV Events in All Randomized Subjects Pravastatin 40mg (26.3%) 16% RR (P = 0.005) % with Event Atorvastatin 80mg (22.4%) Mean LDL 62mg/dL(1.6mmol/L) Ridker PM et al. N Engl J Med 2005;352: Months of Follow-up
5 The Need to Go Beyond LDL-cholesterol Reduction Many patients with adequately controlled LDL-C still experience a CVD event. Disorders that contribute to CVD risk other than LDL-C are common among those with CAD, even those with LDL-C<100mg/dL. There are effective therapies to treat other CVD risk factors, and new therapies are under development.




6 How Can We Improve Our Ability to Predict CHD Risk? Arterial imaging/ function Biomarkers Metabolic syndrome Family history Framingham risk score/score(esc) Adapted from Kullo IJ, et al. Mayo Clin Proc. 2005;80:
7 Age-adjusted Prevalence (%) Age- and Sex Adjusted Risk (%) Family History: Both Sibling and Parental History Can Affect CV Risk Prevalence of CAC 100 by Family History of Premature CHD No Family History Parental Family History Sibling Family History Both year Risk for CVD in Middle-aged Adults No Sibling CVD Sibling CVD No RF 1 RF 2 RF 3 RF Entire Population Cohort with Both Parents in FHS CAC = coronary artery calcification; RF = risk factor Nasir K, et al. Circulation. 2004;110: Murabito MJ, et al. JAMA. 2005;294:
8 NHANES III Metabolic Syndrome At least 3 metabolic abnormalities: Abdominal obesity (waist): Men >102 cm (>40 in) Women >88 cm (>35 in) FBG 110 mg/dl* TG 150 mg/dl HDL-C NCEP Criteria Men <40 mg/dl Women <50 mg/dl (1.69 mmol/l) BP 130/85 mm Hg or on antihypertensive medication Abdominal Obesity Hypertriglyceridemia Low HDL-C HTN/on Medication High Blood Glucose/on Medication 3 Components US Population (%) *Fasting plasma glucose; NHLBI/AHA now recommends >100 mg/dl Expert Panel. JAMA. 2001;285: Ford ES, et al. JAMA. 2002;287: Grundy SM, et al. Circulation. 2004;109:
 Time (months) 20%, No Metabolic Syndrome >20%, No Metabolic Syndrome 20%, Metabolic Syndrome >20%, Metabolic Syndrome MACE = major")
9 Cumulative Incidence (%) Metabolic Syndrome May Increase Risk for MACE Regardless of Framingham Estimated Risk AFCAPS 4S Time (months) Time (months) 20%, No Metabolic Syndrome >20%, No Metabolic Syndrome 20%, Metabolic Syndrome >20%, Metabolic Syndrome MACE = major adverse coronary events; AFCAPS/TexCAPS = Air Force/Texas Coronary Atherosclerosis Prevention Study; 4S = Scandinavian Simvastatin Survival Study Girman CJ, et al. Am J Cardiol. 2004;93:
 <0.5 0.5-1 1-3 3-10 >10 Ridker PM, et al. Circulation. 2004;109:2818-2825.")
10 hscrp Modified Global CHD Risk Low High Biomarkers May Improve Prediction of CV Events Beyond Framingham Scores <5 Calculated Framingham 10-y Risk (%) < >10 Ridker PM, et al. Circulation. 2004;109:
11 Ridker P, et al NEJM Nov ,939 healthy women 1.00 Probability of Event Free Survival hscrp<2mg/l, LDL<130mg/dL (3.36mmol/L) hscrp<2, LDL>130 hscrp>2, LDL< hscrp>2, LDL> Years of follow up Event free survival according to baseline hs-crp quintile
12
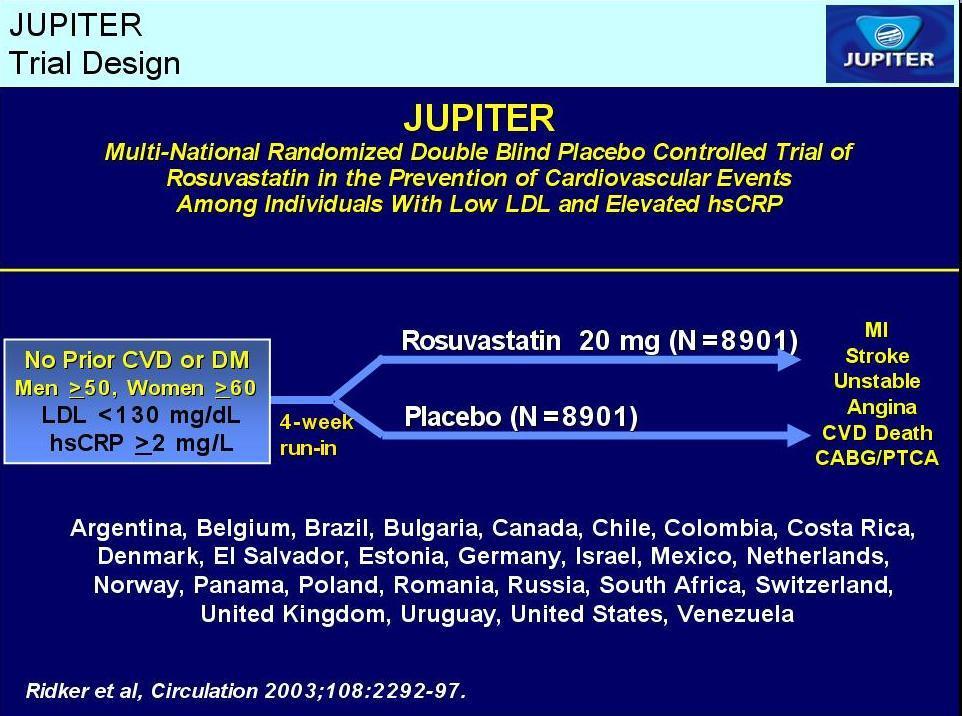
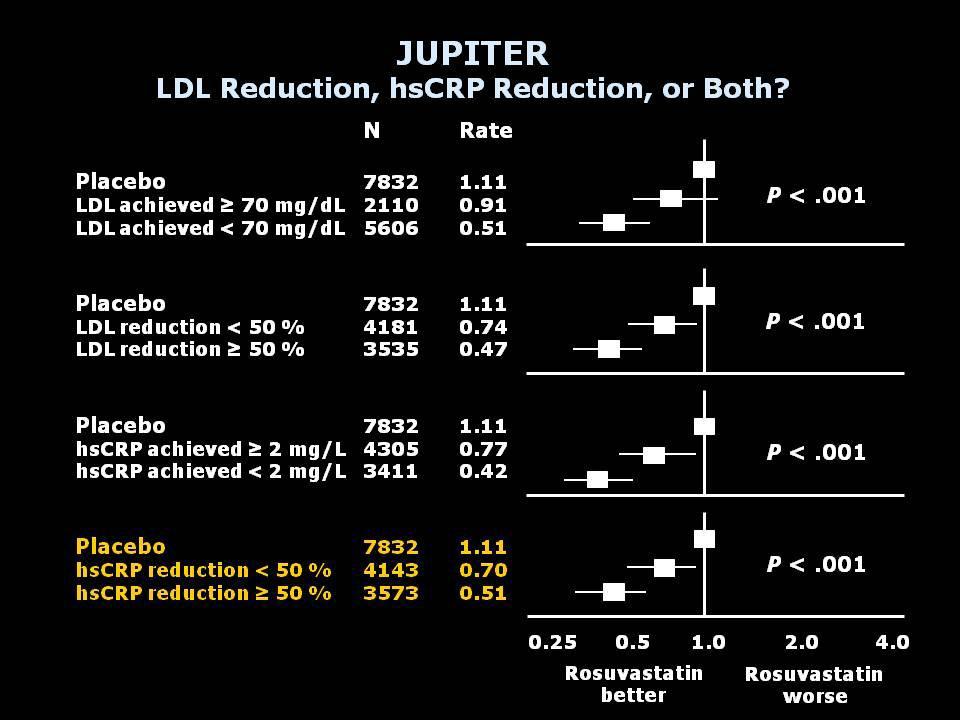
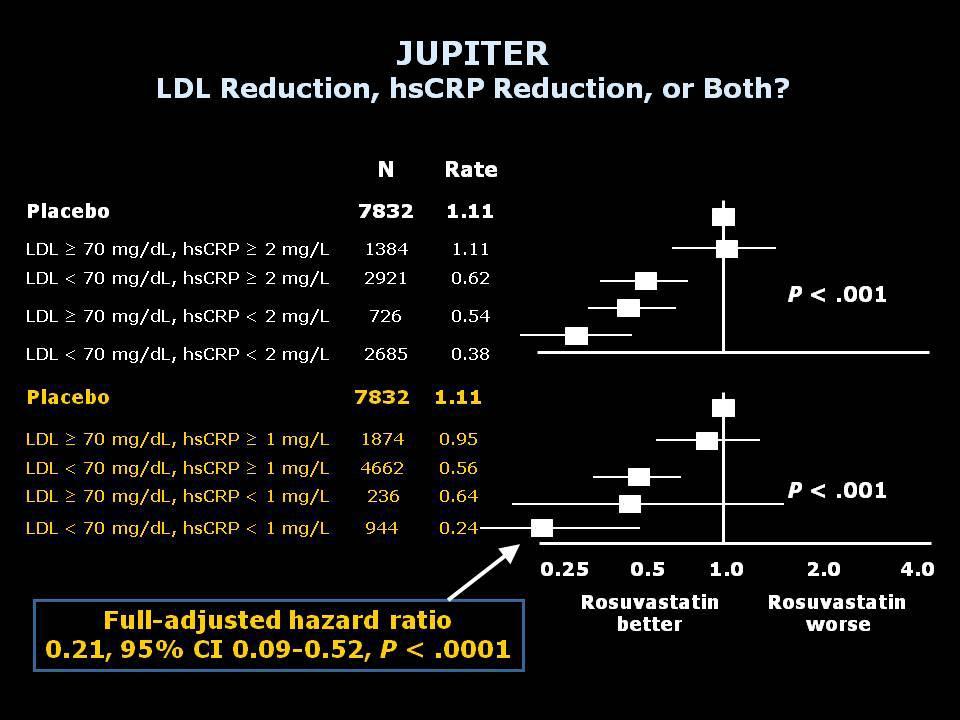
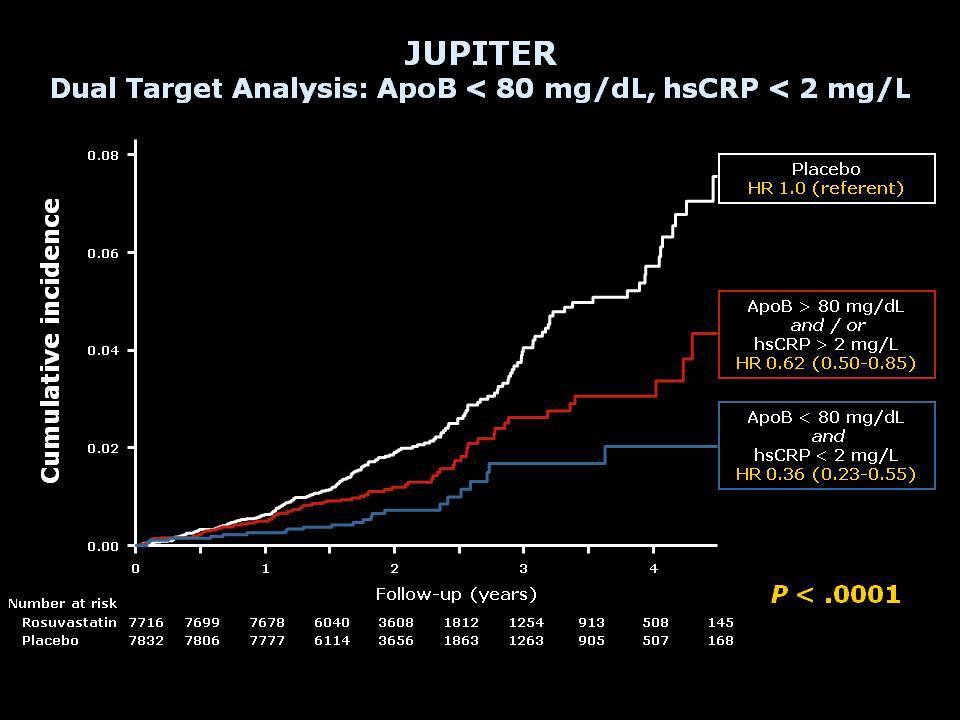
13 JUPITER Achieved LDLC, Achieved hscrp, or Both? Objectives: To compare clinical outcomes among JUPITER trial participants according to achieved levels of LDLC and hscrp, after adjustment for all available baseline clinical characteristics, including entry levels of LDLC, HDL-C, and hscrp. To evaluate whether clinical outcomes according to achieved lipid and hscrp levels are altered by substituting ApoB or the ApoB:ApoA ratio for LDLC. Ridker, PM et al. ACC 2009

14 Ridker P et al. N Eng J Med 2008;359:

15 Ridker P et al. N Eng J Med 2008;359:
 450 400 350 300 250 200 150 100 50 0")
16 JUPITER 5-Year NNT Values for Primary Prevention of CVD Number Needed to Treat (5 years)
17 JUPITER
18
19
20 hscrp: Conclusions LDL-C and hscrp are strong independent predictors of future CVD events. Statins lower LDL-C and hscrp Lower is better for both LDL-C and hscrp Consider Dual Target of LDL-C<70mg/dL and hs CRP<2mg/L.
21 How has JUPITER affected the guidelines? ATP IV ?hsCRP US FDA has approved the JUPITER indication for rosuvastatin Canadian 2009 Guidelines recommending the use of CRP to determine statin eligibility among patients considered "intermediate risk." (10-year Framingham risk between 10% and 20%). ESC-have not granted the JUPITER indication but endorsed use of rosuvastatin in patients with a Framingham risk score over 20% or a SCORE [risk model used in Europe] over 5%
22 Clinical Predictors of Plaque Progression Despite Very Low Levels of Low-Density Lipoprotein Cholesterol Pooled Data from 7 prospective atherosclerosis progression/regression IVUS trials. Total of 3437 patient with CAD underwent serial IVUS examinations. Patients who achieved on treatment LDL-C<70mg/dL (n=951) were stratified as progressors -defined as >5% increase in percent atheroma volume (PAV)-(n=200) and nonprogressors (n=751) and compared. Bayturan et al. J Am Coll Cardiol 2010;55: Copyright 2008 American College of Cardiology Foundation. Restrictions may apply.
23 Results Compared to patients with on treatment LDL-C >70mg/dL, those with LDL-C<70mg/dL demonstrated less progression of PAV. Despite achieving LDL-C<70mg/dL, >20% of patients continued to progress. Progressors had higher baseline levels of glucose and triglycerides. Independently associated risk factors of progression in patients with LDL-C<70mg/dL: 1. diabetes mellitus 2. increase in systolic blood pressure 3. less increase in HDL-cholesterol 4. smaller decrease in apob levels (Not changes in c-reactive protein) Bayturan et al. J Am Coll Cardiol 2010;55:

24 Coronary Artery Calcium Scoring For image on left (LAD), calcium score is 60. For image on right (RCA), calcium score is 16. For these two slices, score would be 76. Total calcium score is the sum of all individual calcium scores for the entire epicardial coronary artery system.
25 The St. Francis Heart Study Coronary Artery Calcium Scores Predict CV Events Event Rate (%) Relative Risk RR= RR= % (n=63) RR=1 RR= % (n=38) 0.54% 1% (n=20) (n=8) 0 1 to to Coronary Artery Calcium Score Arad Y, et al. J Am Coll Cardiol. 2005;46:
26 Imaging to Detect Subclinical Atherosclerosis to Predict Future CVD Events Individualizes risk assessment beyond the use of age. Identifies individuals at risk beyond established risk factors. Offers an integrated assessment of the exposure to risk factors. Detection of subclinical atherosclerosis can guide therapy based on plaque burden. NCEP ATP III and ESC suggest additional tests to better assess intermediate risk for confirmation or reclassification of risk. NCEP ATP III recommends 75 th percentile value based on age and gender, ESC defines high risk as CAC>100 and/or >75 th percentile.
27 Therapeutic Approaches to Reducing Residual Risk Lifestyle modification Mediterranean diets associated with longevity, low CVD mortality and less diabetes Exercise-physical activity can reduce CVD and type II diabetes by up to 50%. Smoking cessation-return to baseline risk after 5 years Intensify statin monotherapy, consider dual target Combination drug therapy Further reduce LDL-C Reduce non-hdl-c in mixed dyslipidemia
28 Niacin and Statins: HDL-Atherosclerosis Treatment Study (HATS) 3-year double-blind trial Simvastatin plus niacin and/or antioxidants vs. placebo 160 patients with CAD, low HDL-C, and normal LDL-C levels Simvastatin plus niacin (sustained- or immediate-release) Reduced LDL-C 42%; TG 36% Increased HDL-C 26% Reduced TC:HDL-C ratio from 6.5 to 3.5 (P <0.001) Regression of stenosis by 0.4% (vs. 3.9% progression in placebo group; P <0.001) 90% reduction in composite end point* (P <0.03 vs. placebo) *Death from coronary causes, confirmed MI or stroke, or revascularization for worsening ischemic symptoms Brown et al. N Engl J Med. 2001;345:1583.
29 Mean Change in Stenosis, % HATS: Angiographic and Clinical Endpoints After 3 Years Placebo S+N S+N+AV Proximal Lesions * % reduction 14.3 Coronary Death, MI, Stroke, or Revascularization HATS = HDL-C-Atherosclerosis Treatment Study; S = simvastatin; N = niacin; AV = antioxidant vitamins. *p<0.001 vs. placebo; p<0.005 vs. placebo; p=0.04 vs. placebo. Adapted from Brown BG et al. N Engl J Med. 2001;345: Composite Event Rate, %
. Follow-up was 14 months. (p = 0.003) -0.0142 Extended-release niacin -0.")
 Change in LDL cholesterol: -10.0 mg/dl vs. - 17.6 mg/dl (p = 0.01), respectively Change in HDL cholesterol: 7.5 mg/dl vs. -2.8 mg/dl (p < 0.001), respectively MACE: 1% vs. 5% (p = 0.")
30 mm ARBITER 6-HALTS Trial design: Patients with CHD (or risk equivalent) on statin therapy and with low HDL cholesterol were randomized to extended-release niacin 2000 mg daily (n = 97) versus ezetimibe 10 mg daily (n = 111). Follow-up was 14 months. (p = 0.003) Extended-release niacin Change in mean carotid IMT at 12 months Ezetimibe Results Change in mean carotid intima-media thickness (IMT): mm with niacin vs mm with ezetimibe (p = 0.003) Change in LDL cholesterol: mg/dl vs mg/dl (p = 0.01), respectively Change in HDL cholesterol: 7.5 mg/dl vs mg/dl (p < 0.001), respectively MACE: 1% vs. 5% (p = 0.04), respectively Conclusions Among CHD patients on statin therapy, with LDL cholesterol <100 mg/dl and HDL cholesterol <50 mg/dl for men or <55 mg/dl for women, the use of extended-release niacin was beneficial Niacin reduced mean carotid IMT and raised HDL cholesterol Taylor AJ, et al. N Engl J Med 2009;Nov 15:[Epub]


31 Fibrates (PPAR- Agonists) and Statins Combination may significantly improve TG, LDL-C, and HDL-C levels Fibrates plus statins associated with increased risk for myopathy and rhabdomyolysis Fenofibrate may have relatively less potential for impairment of statin metabolism DATA: VA-HIT 24%RRR, FIELD 11%RRR Ballantyne CM, et al. Arch Intern Med. 2003;163: Bays H. Am J Cardiol. 2002;90:30K-43K. Bays HE, et al. Expert Opin Pharmacother. 2003;4:
32 Change from Baseline (%) SAFARI Addition of Fenofibrate to Statin Therapy Benefits Patients with Combined Hyperlipidemia Simvastatin 20 mg Simvastatin 20 mg + Fenofibrate 160 mg -20.1% -43.0% * N= % -25.8% -49.1% -31.2% 9.7% TG VLDL-C LDL-C HDL-C SAFARI = Simvastatin Plus Fenofibrate for Combined Hyperlipidemia *P<0.001 vs simvastatin Grundy SM, et al. Am J Cardiol. 2005;95: % Baseline: mg/dl 50 mg/dl mg/dl mg/dl * * *
33 % per year ACCORD Lipid Trial design: Type 2 diabetics treated with a statin were randomized to fenofibrate (n = 2,765) vs. placebo (n = 2,753). Mean follow-up was 4.7 years. (p = 0.32) Fatal or nonfatal CV event Fenofibrate Placebo Results CV mortality, MI, or stroke: 2.2%/year with fenofibrate vs. 2.4%/year with placebo Primary outcome plus revascularization or hospitalization for CHF: 5.4%/year vs. 5.6%/year (p = 0.30), respectively All-cause mortality: 1.5%/year vs. 1.6%/year (p = 0.33), respectively Exploratory analysis: possible benefit in men vs. women (p for interaction = 0.01) Conclusions Among type 2 diabetics treated with a statin, there was no long-term benefit from fenofibrate compared with placebo Composite CV outcomes were similar between the two groups Presented by Dr. Henry Ginsberg at ACC.10/i2 Summit
34 Clinical Concerns About Combination Drug Therapy Limited data on benefit Potential for increased risk of adverse events (AEs) and reduced tolerability Increased cost, complexity, and reduced tolerability may reduce patient adherence McKenney JM. Am J Ther. 2004;11:54-59.
35 INTER-HEART: Risk of acute MI associated Risk factor with risk factors in the overall population ApoB/ApoA-1 (fifth quintile compared with first) Odds ratio adjusted for age, sex, and smoking (99% CI) Yusuf S, Hawken S, Ounpuu S, on behalf of the INTERHEART Study Investigators. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364: Odds ratio adjusted for all (99% CI) 3.87 ( ) 3.25 ( ) Current smoking 2.95 ( ) 2.87 ( ) Diabetes 3.08 ( ) 2.37 ( ) Hypertension 2.48 ( ) 1.91 ( ) Abdominal obesity 2.22 ( ) 1.62 ( ) Psychosocial 2.51 ( ) 2.67 ( ) Vegetable and fruits daily 0.70 ( ) 0.70 ( ) Exercise 0.72 ( ) 0.86 ( ) Alcohol intake 0.79 ( ) 0.91 ( ) All combined ( ) ( )
36 Finnish Diabetes Prevention Study Design 522 middle-aged overweight (BMI 31) 172 men and 350 women Mean duration 3.2 years Intervention Group: Individualized counseling Reducing weight, total intake of fat and saturated fat Increasing uptake of fiber, physical activity Tuomilehto J, et al. N Engl J Med. 2001;344:







37 Diet and Exercise Intervention Controls Goals Weight reduction >5% Fat intake <30% energy Sat fat <10% energy Fiber >15 g/1000 kcal % of subjects P value Exercise >4 hr/wk Tuomilehto J, et al. N Engl J Med. 2001;344:

 diabetes")
 after 4")


38 Benefit of Lifestyle Changes Risk of 23% (17-29CI) diabetes reduced by 58% 11%( 6-15CI) after 4 years Intervention Control % with Diabetes Tuomilehto J et al. N Engl J Med 2001;344:
39 Mortality Rate Changes in Physical Fitness and CVD Mortality: ACLS deaths in 9,777 men 4.9 years between exams Unfit Unfit Unfit Fit Fitness at Two Exams Fit Fit Blair SN et al. JAMA 1995;273:
40 Conclusions We need to think beyond lower is better LDL goals to adequately address residual risk. Consider additional risk assessors including biomarkers (hscrp, ApoB) and imaging (CAC) to better classify risk category and determine intensity of therapy. Consider a dual target of LDL-C and hs-crp goals.
41
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Landmark Clinical Trials.
 Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Dyslipidaemia. Is there any new information? Dr. A.R.M. Saifuddin Ekram
 Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
Hyperlipidemia: Lowering the Bar on the Lipid Limbo. Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH
 Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Lessons from Recent Atherosclerosis Trials
 Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
Qué factores de riesgo lipídicos debemos controlar? En qué medida?
 Qué factores de riesgo lipídicos debemos controlar? En qué medida? Risk category High risk: CHD or CHD risk equivalents (10- year risk >20%) Moderately high risk: two or more risk factors (10-year risk
Qué factores de riesgo lipídicos debemos controlar? En qué medida? Risk category High risk: CHD or CHD risk equivalents (10- year risk >20%) Moderately high risk: two or more risk factors (10-year risk
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Lipid Management: A Case-Based Approach. Overview. Simple Lipid Therapy Approach. Patients have lipid disorders of:
 Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Is it an era for statin for life?
 Is it an era for statin for life? Mohamed Abdel Ghany Professor of Cardiology Cairo University Cardiovascular Disease (CVD) is the leading global cause of death 1 Dyslipidemia as a main Risk Factor for
Is it an era for statin for life? Mohamed Abdel Ghany Professor of Cardiology Cairo University Cardiovascular Disease (CVD) is the leading global cause of death 1 Dyslipidemia as a main Risk Factor for
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Young high risk patients the role of statins Dr. Mohamed Jeilan
 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Should we treat everybody over 60 years with a statin? Comprehensive primary prevention in practice
 Should we treat everybody over 60 years with a statin? Comprehensive primary prevention in practice Pathogenesis of atherosclerosis A decades-long disease course Inflammation Selectins ICAM IL M-CSF CRP
Should we treat everybody over 60 years with a statin? Comprehensive primary prevention in practice Pathogenesis of atherosclerosis A decades-long disease course Inflammation Selectins ICAM IL M-CSF CRP
Advances in Lipid Management
 Advances in Lipid Management Kavita Sharma, MD Assistant Professor of Medicine, Division of Cardiology Clinical Director of the Lipid Management Clinics, The Ohio State University Wexner Medical Center
Advances in Lipid Management Kavita Sharma, MD Assistant Professor of Medicine, Division of Cardiology Clinical Director of the Lipid Management Clinics, The Ohio State University Wexner Medical Center
Cholesterol Treatment Update
 Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Preventing Cardiovascular Disease With Lipid Management: Matching Therapy to Risk
 PREVENTING CARDIOVASCULAR DISEASE WITH LIPID MANAGEMENT : MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict
PREVENTING CARDIOVASCULAR DISEASE WITH LIPID MANAGEMENT : MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict
Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients. Copyright. Not for Sale or Commercial Distribution
 CLINICAL Viewpoint Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients Copyright Not for Sale or Commercial Distribution By Ruth McPherson, MD, PhD, FRCPC Unauthorised
CLINICAL Viewpoint Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients Copyright Not for Sale or Commercial Distribution By Ruth McPherson, MD, PhD, FRCPC Unauthorised
Placebo-Controlled Statin Trials
 PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
Environmental. Vascular / Tissue. Metabolics
 Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
10/15/2012. Lessons Learned from Tim Russert: Investigating Residual Risk. Tim Russert: Residual CV Risk?
 Lessons Learned from Tim Russert: Investigating Residual Risk Peter H. Jones, MD, FACP Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Houston, Texas Tim Russert:
Lessons Learned from Tim Russert: Investigating Residual Risk Peter H. Jones, MD, FACP Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Houston, Texas Tim Russert:
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode Island Cardiology Center
 Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
The TNT Trial Is It Time to Shift Our Goals in Clinical
 The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
The Metabolic Syndrome
 The Metabolic Syndrome Advances in Internal Medicine David D. Waters, MD May 21, 27 UCSF Metabolic Syndrome: Definition abdominal obesity increased waist circumference atherogenic dyslipidemia low HDL-C,
The Metabolic Syndrome Advances in Internal Medicine David D. Waters, MD May 21, 27 UCSF Metabolic Syndrome: Definition abdominal obesity increased waist circumference atherogenic dyslipidemia low HDL-C,
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Inflammation and and Heart Heart Disease in Women Inflammation and Heart Disease
 Inflammation and Heart Disease in Women Inflammation and Heart Disease What is the link between een inflammation and atherosclerotic disease? What is the role of biomarkers in predicting cardiovascular
Inflammation and Heart Disease in Women Inflammation and Heart Disease What is the link between een inflammation and atherosclerotic disease? What is the role of biomarkers in predicting cardiovascular
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Changing lipid-lowering guidelines: whom to treat and how low to go
 European Heart Journal Supplements (2005) 7 (Supplement A), A12 A19 doi:10.1093/eurheartj/sui003 Changing lipid-lowering guidelines: whom to treat and how low to go C.M. Ballantyne Section of Atherosclerosis,
European Heart Journal Supplements (2005) 7 (Supplement A), A12 A19 doi:10.1093/eurheartj/sui003 Changing lipid-lowering guidelines: whom to treat and how low to go C.M. Ballantyne Section of Atherosclerosis,
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation.
 Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist
 1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
Dyslipidemia in women: Who should be treated and how?
 Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP
 Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP Professor of Medicine Medical-Director, Preventive Cardiology John Ochsner Heart and Vascular
Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP Professor of Medicine Medical-Director, Preventive Cardiology John Ochsner Heart and Vascular
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Traitements associés chez l hypertendu: Statines, Aspirine
 Traitements associés chez l hypertendu: Statines, Aspirine Pr Jean-Jacques Mourad CHU Avicenne, Université Paris 13, Bobigny DU HTA, Mars 2012 jean-jacques.mourad@avc.aphp.fr Global Mortality 2000: Impact
Traitements associés chez l hypertendu: Statines, Aspirine Pr Jean-Jacques Mourad CHU Avicenne, Université Paris 13, Bobigny DU HTA, Mars 2012 jean-jacques.mourad@avc.aphp.fr Global Mortality 2000: Impact
RECOGNITION OF THE METABOLIC SYNDROME
 THE METABOLIC SYNDROME IN CLINICAL PRACTICE Michael H. Davidson, MD* ABSTRACT Patients with the metabolic syndrome remain at significantly elevated risk of morbidity and mortality associated with coronary
THE METABOLIC SYNDROME IN CLINICAL PRACTICE Michael H. Davidson, MD* ABSTRACT Patients with the metabolic syndrome remain at significantly elevated risk of morbidity and mortality associated with coronary
Data Alert. Vascular Biology Working Group. Blunting the atherosclerotic process in patients with coronary artery disease.
 1994--4 Vascular Biology Working Group www.vbwg.org c/o Medical Education Consultants, LLC 25 Sylvan Road South, Westport, CT 688 Chairman: Carl J. Pepine, MD Eminent Scholar American Heart Association
1994--4 Vascular Biology Working Group www.vbwg.org c/o Medical Education Consultants, LLC 25 Sylvan Road South, Westport, CT 688 Chairman: Carl J. Pepine, MD Eminent Scholar American Heart Association
Imaging Biomarkers: utilisation for the purposes of registration. EMEA-EFPIA Workshop on Biomarkers 15 December 2006
 Imaging Biomarkers: utilisation for the purposes of registration EMEA-EFPIA Workshop on Biomarkers 15 December 2006 Vascular Imaging Technologies Carotid Ultrasound-IMT IVUS-PAV QCA-% stenosis 2 ICH E
Imaging Biomarkers: utilisation for the purposes of registration EMEA-EFPIA Workshop on Biomarkers 15 December 2006 Vascular Imaging Technologies Carotid Ultrasound-IMT IVUS-PAV QCA-% stenosis 2 ICH E
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Consensus and Controversy in Diabetic Dyslipidemia
 Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
TABLE 1. Cardiovascular Disease Management Guidelines for the Primary Prevention of CAD a Risk category b LDL-C goal (mg/dl) c Moderately high risk (
 c Moderately high risk (") REVIEW PRIMARY PREVENTION OF CAD Intensive Lowering of Low-Density Lipoprotein Cholesterol Levels for Primary Prevention of Coronary Artery Disease DEAN G. KARALIS, MD Coronary artery disease (CAD) is
REVIEW PRIMARY PREVENTION OF CAD Intensive Lowering of Low-Density Lipoprotein Cholesterol Levels for Primary Prevention of Coronary Artery Disease DEAN G. KARALIS, MD Coronary artery disease (CAD) is
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
American Osteopathic College of Occupational and Preventive Medicine 2012 Mid-Year Educational Conference St. Petersburg, Florida
 The 21 st Century Paradigm Shift: Prevention Rather Than Intervention for the Treatment of Stable CHD The Economic Burden of Cardiovascular Diseases Basil Margolis MD, FACC, FRCP Director, Preventive Cardiology
The 21 st Century Paradigm Shift: Prevention Rather Than Intervention for the Treatment of Stable CHD The Economic Burden of Cardiovascular Diseases Basil Margolis MD, FACC, FRCP Director, Preventive Cardiology
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona,
 Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Weintraub, W et al NEJM March Khot, UN et al, JAMA 2003
 Global risk hscrp Should not be included in a Global Cardiovascular Risk Assessment. Jodi Tinkel, MD Assistant Professor Director of Cardiac Rehabilitation Associate Program Director, Cardiovascular Medicine
Global risk hscrp Should not be included in a Global Cardiovascular Risk Assessment. Jodi Tinkel, MD Assistant Professor Director of Cardiac Rehabilitation Associate Program Director, Cardiovascular Medicine
Atherosclerosis Regression An Overview of Recent Findings & Issues
 Atherosclerosis Regression An Overview of Recent Findings & Issues 13th Angioplasty Summit 2008 Cheol Whan Lee, MD University of Ulsan, Asan Medical Center, Seoul, Korea CardioVascular Research Foundation
Atherosclerosis Regression An Overview of Recent Findings & Issues 13th Angioplasty Summit 2008 Cheol Whan Lee, MD University of Ulsan, Asan Medical Center, Seoul, Korea CardioVascular Research Foundation
CVD Risk Assessment. Lipid Management in Women: Lessons Learned. Conflict of Interest Disclosure
 Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Beyond Framingham: Risk Assessment & Treatment for Primary Prevention
 Beyond Framingham: Risk Assessment & Treatment for Primary Prevention Ronald M. Goldenberg, MD, FRCPC, FACE Consultant Endocrinologist, North York General Hospital Medical Co-Director, LMC Endocrinology
Beyond Framingham: Risk Assessment & Treatment for Primary Prevention Ronald M. Goldenberg, MD, FRCPC, FACE Consultant Endocrinologist, North York General Hospital Medical Co-Director, LMC Endocrinology
Treating Lipids for Prevention of CAD in Women: Matching Therapy to Risk
 TREATING LIPIDS FOR PREVENTION OF CAD IN WOMEN: MATCHING THERAPY TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
TREATING LIPIDS FOR PREVENTION OF CAD IN WOMEN: MATCHING THERAPY TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Disclosures. Prevention of Heart Disease: The New Guidelines. Summary of Talk. Four guidelines. No relevant disclosures.
 Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Prof. John Chapman, MD, PhD, DSc
 Prof. John Chapman, MD, PhD, DSc Director of the Dyslipidemia and Atherosclerosis Research Unit of the National Institute for Health and Medical Research (INSERM) at the Pitié-Salpétrière Hospital in Paris
Prof. John Chapman, MD, PhD, DSc Director of the Dyslipidemia and Atherosclerosis Research Unit of the National Institute for Health and Medical Research (INSERM) at the Pitié-Salpétrière Hospital in Paris
Ezetimibe and SimvastatiN in Hypercholesterolemia EnhANces AtherosClerosis REgression (ENHANCE)
") Ezetimibe and SimvastatiN in Hypercholesterolemia EnhANces AtherosClerosis REgression (ENHANCE) Thomas Dayspring, MD, FACP Clinical Assistant Professor of Medicine University of Medicine and Dentistry
Ezetimibe and SimvastatiN in Hypercholesterolemia EnhANces AtherosClerosis REgression (ENHANCE) Thomas Dayspring, MD, FACP Clinical Assistant Professor of Medicine University of Medicine and Dentistry
Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention Center: Rooms 315 & 316
 Ambulatory Care PRN Focus Session New Developments in Hypertension and Dyslipidemia Management Activity No. 0217-0000-11-101-L01-P (Application-Based Activity) Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention
Ambulatory Care PRN Focus Session New Developments in Hypertension and Dyslipidemia Management Activity No. 0217-0000-11-101-L01-P (Application-Based Activity) Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk?
 There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
Cholesterol lowering intervention for cardiovascular prevention in high risk patients with or without LDL cholesterol elevation
 TrialResults-center.org www.trialresultscenter.org Cholesterol lowering intervention for cardiovascular prevention in high risk patients with or without LDL cholesterol elevation A systematic review and
TrialResults-center.org www.trialresultscenter.org Cholesterol lowering intervention for cardiovascular prevention in high risk patients with or without LDL cholesterol elevation A systematic review and
The Atherogenic Dyslipidemia of Diabetes Mellitus- Not just a question of LDL-C
 The Atherogenic Dyslipidemia of Diabetes Mellitus- Not just a question of LDL-C Eun-Jung Rhee Department of Endocrinology and Metabolism Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine
The Atherogenic Dyslipidemia of Diabetes Mellitus- Not just a question of LDL-C Eun-Jung Rhee Department of Endocrinology and Metabolism Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine
Nearly 62 million people in the. ... REPORTS... New Therapeutic Options in the National Cholesterol Education Program Adult Treatment Panel III
 ... REPORTS... New Therapeutic Options in the National Cholesterol Education Program Adult Treatment Panel III Robert L. Talbert, PharmD Abstract Coronary heart disease (CHD) is a common, costly, and undertreated
... REPORTS... New Therapeutic Options in the National Cholesterol Education Program Adult Treatment Panel III Robert L. Talbert, PharmD Abstract Coronary heart disease (CHD) is a common, costly, and undertreated
Hyperlipidemia and Cardiovascular Disease. Kathmandu November 2010 Harold E. Lebovitz, MD, FACE
 Hyperlipidemia and Cardiovascular Disease Kathmandu November 21 Harold E. Lebovitz, MD, FACE Diabetes and Lifetime Risk for CHD Adjusted cummula ative incidence.7.6.5 Men 67% 3%.7.6.5 Women Diabetes No
Hyperlipidemia and Cardiovascular Disease Kathmandu November 21 Harold E. Lebovitz, MD, FACE Diabetes and Lifetime Risk for CHD Adjusted cummula ative incidence.7.6.5 Men 67% 3%.7.6.5 Women Diabetes No
New Insights on Optimal Management of LDL-C in High-risk Populations. Copyright
 New Insights on Optimal Management of LDL-C in High-risk Populations By David Fitchett, MD, FRCPC Division of Cardiology, St. Michael s Hospital, University of Toronto Copyright Low-density lipoprotein
New Insights on Optimal Management of LDL-C in High-risk Populations By David Fitchett, MD, FRCPC Division of Cardiology, St. Michael s Hospital, University of Toronto Copyright Low-density lipoprotein
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
Ten Year Risk for CVD Event by Systolic HTN and CVD Risk Factors (Where s Age?)
") Prevention and Treatment of CVD in Older Patients with Diabetes and Pre Diabetes: Hypertension and Dyslipidemia ASP Workshop on Diabetes Mellitus and Cardiovascular Disease in Older Adults Pentagon City
Prevention and Treatment of CVD in Older Patients with Diabetes and Pre Diabetes: Hypertension and Dyslipidemia ASP Workshop on Diabetes Mellitus and Cardiovascular Disease in Older Adults Pentagon City
Accelerated atherosclerosis begins years prior to the diagnosis of diabetes
 Joslin Diabetes Forum 211: Optimizing Care for the Practicing Clinician Risk for atherosclerosis is 2 4 times greater in patients with diabetes CVD accounts for 65% of diabetic mortality >5% of patients
Joslin Diabetes Forum 211: Optimizing Care for the Practicing Clinician Risk for atherosclerosis is 2 4 times greater in patients with diabetes CVD accounts for 65% of diabetic mortality >5% of patients
Current Cholesterol Guidelines and Treatment of Residual Risk COPYRIGHT. J. Peter Oettgen, MD
 Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Welcome! Mark May 14, Sat!
 Welcome! Mark May 14, Sat! Do We Have All Answers with Statins In Treating Patients with Hyperlipidemia? Kwang Kon Koh, MD, PhD, FACC, FAHA Cardiology, Gil Heart Center, Gachon Medical School, Incheon,
Welcome! Mark May 14, Sat! Do We Have All Answers with Statins In Treating Patients with Hyperlipidemia? Kwang Kon Koh, MD, PhD, FACC, FAHA Cardiology, Gil Heart Center, Gachon Medical School, Incheon,
Dyslipidemia and the Use of Statins. Troy L Randle, DO, FACC, FACOI
 Dyslipidemia and the Use of Statins Troy L Randle, DO, FACC, FACOI Objective: Identify CV risk. Determine what dyslipidemia (dyslipoproteinemia) is Decrease CV risk and optimize lipid levels for your
Dyslipidemia and the Use of Statins Troy L Randle, DO, FACC, FACOI Objective: Identify CV risk. Determine what dyslipidemia (dyslipoproteinemia) is Decrease CV risk and optimize lipid levels for your
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
Low-density lipoprotein as the key factor in atherogenesis too high, too long, or both
 Low-density lipoprotein as the key factor in atherogenesis too high, too long, or both Lluís Masana Vascular Medicine and Metabolism Unit. Sant Joan University Hospital. IISPV. CIBERDEM Rovira i Virgili
Low-density lipoprotein as the key factor in atherogenesis too high, too long, or both Lluís Masana Vascular Medicine and Metabolism Unit. Sant Joan University Hospital. IISPV. CIBERDEM Rovira i Virgili
Pharmaceutical Help to Control Cholesterol
 Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
Effective Treatment Options With Add-on or Combination Therapy. Christie Ballantyne (USA)
") Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Triglyceride as Vascular Risk Factor
 Curriculum Vitae Name : Prof. Dr. dr. Idrus Alwi SpPD, KKV, FINASIM, FACP, FACC, FESC, FAPSIC Current Position : - President of the Indonesian Society of Internal Medicine Medical Student : Faculty of
Curriculum Vitae Name : Prof. Dr. dr. Idrus Alwi SpPD, KKV, FINASIM, FACP, FACC, FESC, FAPSIC Current Position : - President of the Indonesian Society of Internal Medicine Medical Student : Faculty of
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel