Clinical Applications of The Pleth. Variability Index (PVI):
|
|
|
- Chad Hoover
- 6 years ago
- Views:
Transcription
: A non")

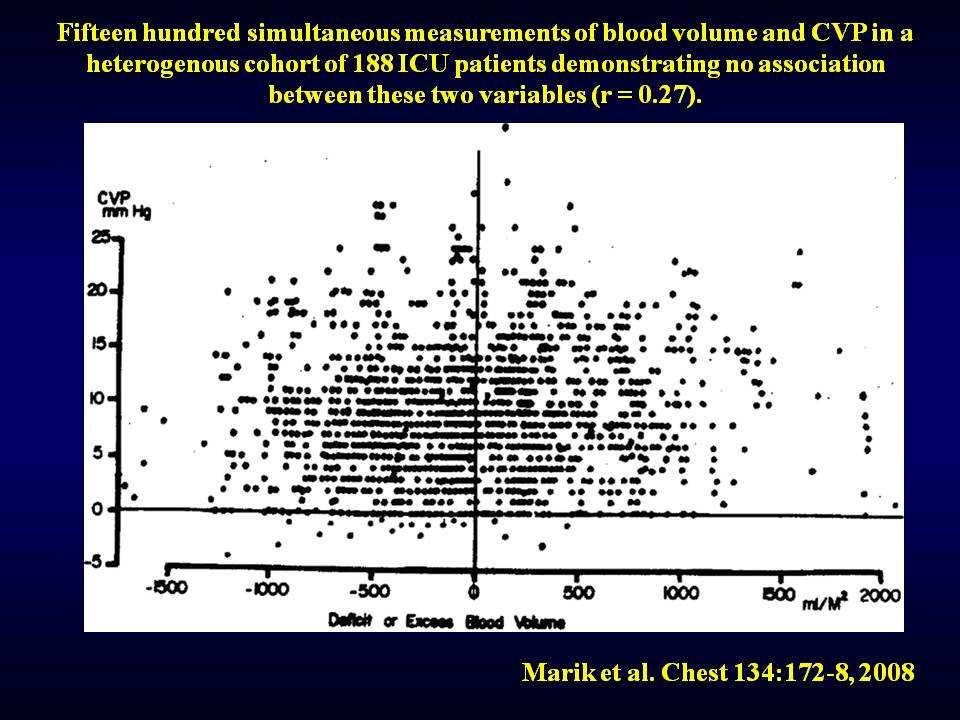
1 Clinical Applications of The Pleth. Variability Index (PVI): A non invasive and continuous monitoring of fluid responsiveness J.PIRSON, MD 26 nov. 2011

2 Preoperative hypovolemia after an overnight fasting period does not occur regularly in all patients. Fluid reloading is unjustified, at least in cardiovascular healthy patients before low-invasive surgery Fluid loss from insensible perspiration is overestimated in many patients, a loss of only 1 ml/kg per hour occurs even when the abdominal cavity is opened 2

3 Where is the «Third Space»? «Eradicating this notion from our minds could be a further key to achieving perioperative fluid optimisation» Jacob et al

4 Starling Law = Glycocalyx 4

: 1458-61.")
5 Atrial Natriuretic Peptide Induces Shedding of Endothelial Glycocalyx Am J Physiol 2005; 289: H1999. J Clin Invest 2005; 115(6): Basic Res Cardiol 2011; Jul 19. 5


6 Intravascular Volume Effect of IV Fluids Jacob et al. 2007; Lancet 369: Crystalloids vs Colloids: only if glyococalyxis intact The Context Sensitivity of Colloidal Volume Effects 6
7 7
8 Strategies for Volume Replacement Strunden et al. Annals of Intensive Care 2011; 1: 2-8 «Restrictive» strategies were compared with «permissive» or «liberal»ones. Ann Surg 2003; 238: Ann Surg 2004; 240: Anesth Analg 2005; 100: Anesthesiology 2005; 103: Etc But: Commonly accepted definition of «restrictive»or «liberal»fluid strategies do not exist, making those studies not comparable Endpoints varied from PONV to pain, tissue oxygenation or bowel recovery time, which de facto rules out a comparison All those studies have in common that no hemodynamic goal were set which is in contrast with «goal-directed-therapy approaches» 8
9 Goals & Strategies for Volume Replacement Strunden et al. Annals of Intensive Care 2011; 1: 2-8 The primary goal of the cardiovascular system is to supply adequate amount of oxygen to the body and match its metabolic demand. Hypovolemia as well as hypervolemia decreases tissue perfusion. Intensive Care Med 2011; 37: Even supplemental oxygendoes not improve oxygenation in hypoperfused tissue Crit Care 1988; 16: AnesthAnalg 2005; 100: AnesthesiolReanim 1999; 24: Br J Anaesth 2002; 89: Crit Care Med 2008; 36: S Is tissue oxygenation adequate? Because representative tissue oxygenation is not measurable directly, mixed venous oxygen saturation, central venous oxygenation and serum lactate are used as surrogates. None of them is able to detect tissue oxygen debt definetely. Intensive Care Med 2011; 37: Crit Care Clin 2010; 26: Ned TijdschrGeneeskd 2000; 144: Curr Opin Crit care 2006; 12: Peri-and post-operative studies in surgical patients show an improvement in patients outcome by CO guided fluid management. Int J Clin Pract 2008; 62: Br J Surg 2006; 93: Intensiv Care Med 2007; 33: AnesthAnalg Br J Anaesth 2009; 103: How can cardiac output (CO) as the main determinate of oxygen delivery, be improved? 9

10 Endpoint of Volume Expansion? Preload-responsiveness = CO can be improved by VE If Preload is optimal, one can assume that no ANP is released The impact of fluidtherapy on microcirculation and tissue oxygenation in hypovolemic patients: a review. Bold et al. Intensive Care Med (2010) 36: Cardiac Output (CO): ΔCO = Heart Rate xδstroke Volume HR in beats/min SV = ml/beat Normal CO: 4-6 L/min Cardiac Index = CO/BSA Normal CI: L/min/M 2 SV = EDV ESV SVI = SV/BSA EF = SV/EDV x 100 Normal EF: 40-60%
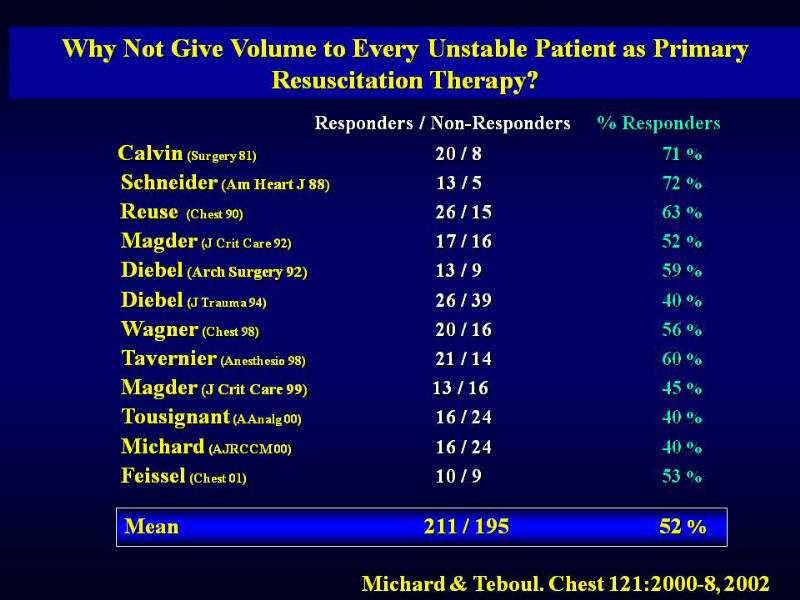
11 11
12 12
13 13
14 The Magnitude of the Change in Stroke Volume/Pulse Pressure Due to Positive Airway Pressure is an Indicator of Bi-ventricular Preload Dependency
")
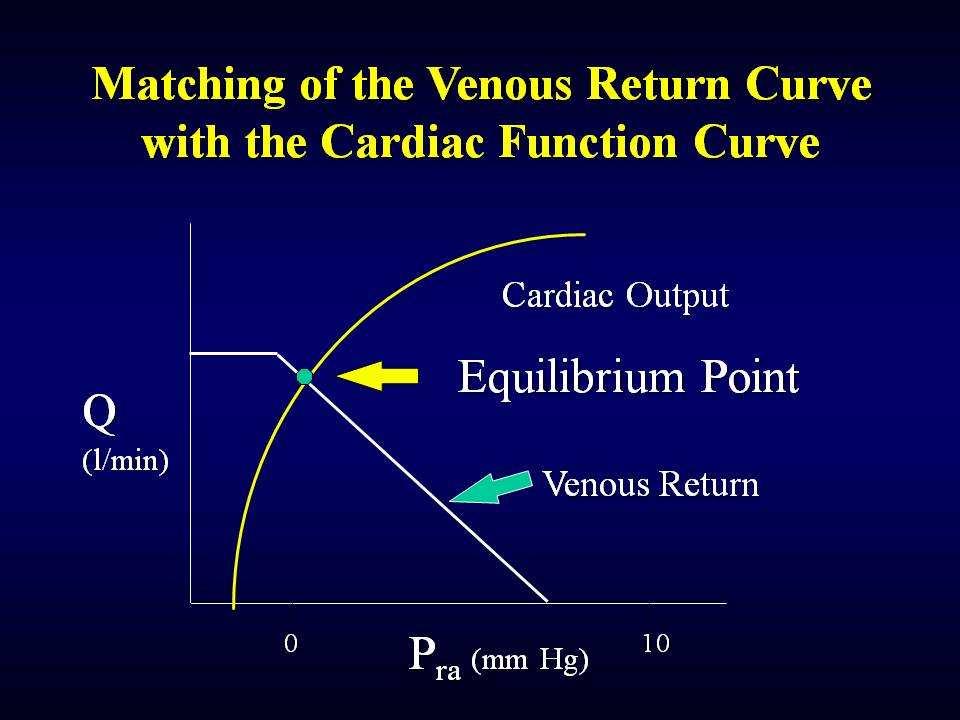
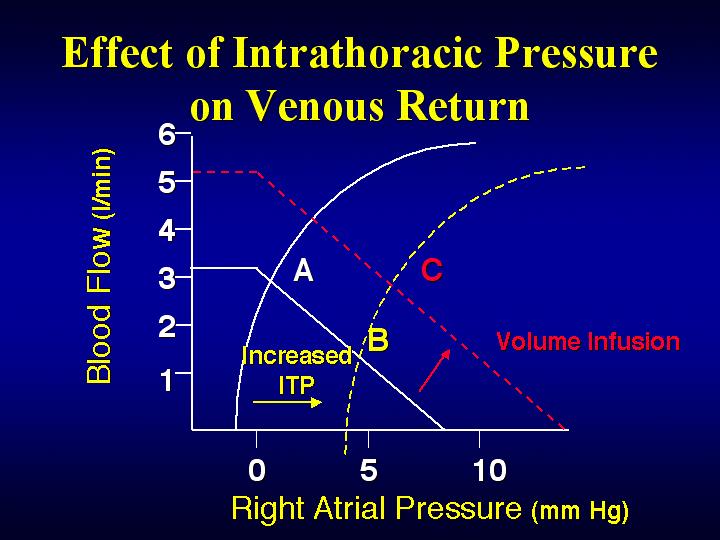
15 Stroke Volume Variation During Mechanical Ventilation The Heart is a Pressure Chamber within a Pressure Chamber Guyton (Am J Physiol 1957) 15
")
16 Guyton (Am J Physiol 1957) 16
17 17
18 18
19 Right Heart Left Heart Rise of pleural pressure impedes venous return to the RA Decreased in RV stroke volume (occurs immediately: one heart beat) Transit time in pulmonary vessels = 3,6 heart beats Decreased LV preload Decrease in LV stroke volume De Backer et al. Anesthesiology 2009;110: (Increase in ITP decrease LV afterload) Pinsky et al. Am J Physiol 1983; 154:
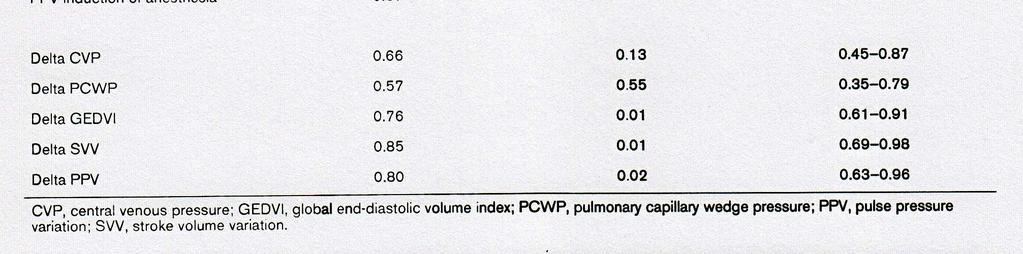
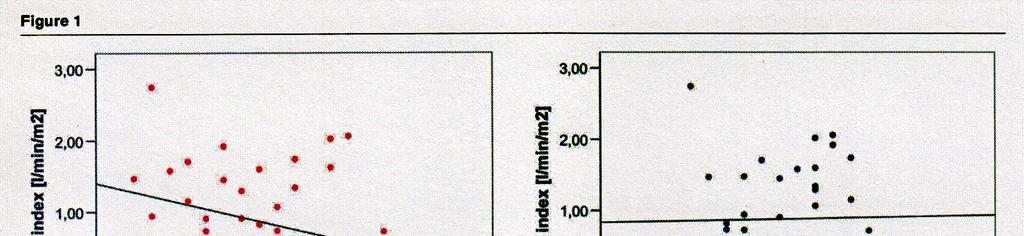
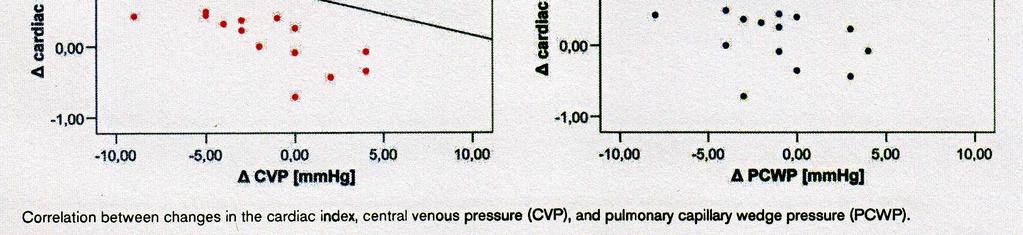
20 ΔPP & ΔSP are Surrogate Measures of ΔSV Michard et al. Am J Crit Care Med 162, 134-8; 2000 ΔSV = resp. change in stroke volume ΔPP = resp. change in (PP max PP min)/(pp mean) ΔSP = resp. change in systolic pressure Endpoint: ΔCI > 15% ΔPP best; ΔPP > 13% is 94% sensit. and 96% spec. to detect VE responsiveness ΔPP reflects changes in stroke volume better than ΔSP because transmural pressure (pleural pressure) affects both systolic and diastolic pressures 20
21 Relation between Respiratory Change in Pulse Pressure and Fluid Responsiveness in Septic Patients with acute Circulatory Failure Michard et al. Am J Crit Care Med 162, 134-8;
22 22

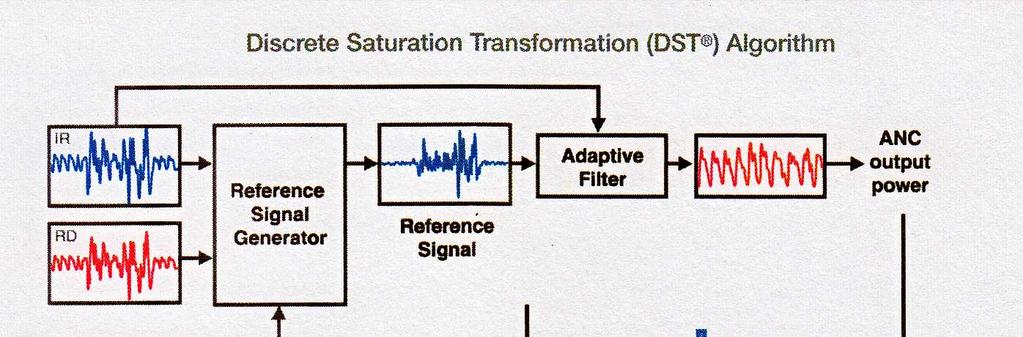
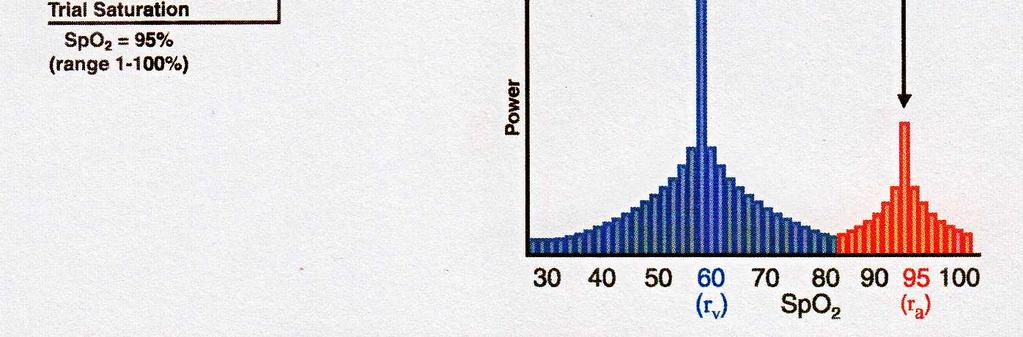
23 Perfusion Index (PI) PlethVariability Index (PVI) 23
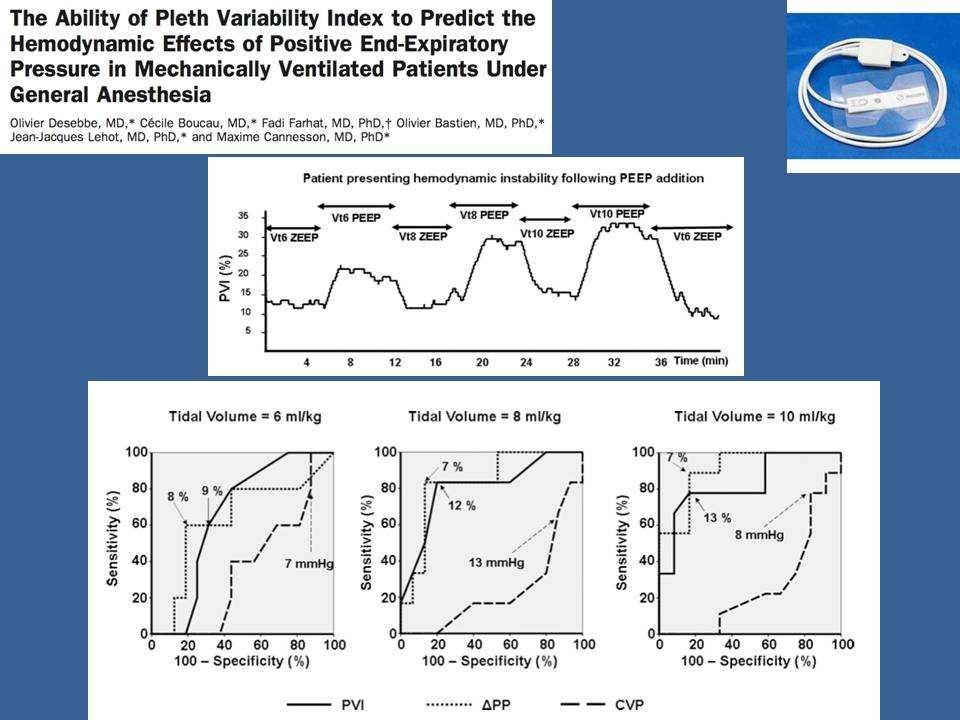
24 PVI (ΔPI) is a Surrogate Measure of ΔPP Cannesson et al, Crit care 2005 Natalini et al, Anesthesiology 2006 Solus et al, B J Anaesth 2006 Zimmermann et al, Eur J Anaesthesiol 2010 Cannesson et al, B J Anaesth 2008 PVI > 13 predicts fluid responsiveness 24
25 Pleth Variability Index 25
 De Backer et al.")
26 Pleth. Variability Index (PVI) How to do it? Volume expansion if PVI > 13 VE until PVI Preload responsiveness at PVI >13 with 100% Sens. & 81% Specif. But About Ventilation: Requires positive-pressure ventilation Keep RF at 12 or less (nextslide) De Backer et al. Anethesiology 2009;110: If thorax is open, PVI is influenced by pre-load but not by ventilation Sander et al. Crit Care 2007; 11: R 121 A high PEEP will influence CO 26
27 Influence of RR on LeftSV Variations As the circulation is pulsatile, Pulmonary transit time is dependent on the HR (3,6 beats) not the RR In high RR, R SV variations are preserved but not L SV variations: the influence of positive ventilation pressure is blured during pulmonary transit time HR/RR < 3,6 RR should be 12/min. or less De Backer et al. Anesthesiology 2009;110:
28 PlethVariability Index (PVI) But About Value of the Signal, Software Calculations: Requires +2 minutes (calculation of mean PVI on n resp. cycles) Requires more time to have a stable value when starting to measure Requires PI > 0,5 cf: PVI does not reflect ventilation related variability of PI if low perfusion in the periphery. Accuracy of PVI is influenced by the quality of PI (4% or more are best) Broch et al. Acta AnethesiolScand 2011; 55(6):
29 PlethVariability Index (PVI) But About Adult vs. Small and BigChildren: Not for children, why? In infants, the cardiac muscle is immature and there is a very low reserve of contractility. The most efficient way to increase CO is to increase the heart rate. The very young heart is chronotropicdependent and afterloaddependent. The intravascular compliance is higher in kids than in adults (diastolic arterial pressure tends to be lower while diastolic pressure tends to be higher, best to use mean art.pressure). The few studies in children demonstrate that SVV is a strong predictor of fluidresponsiveness (with a threshold of 10-15%), while peripheralparameters such as PPV or PVI fail to predict fluidresponsiveness. The most convincing explanation is that SVV is absorbed by the high arterial compliance. Durand et al. Intensive Care Med. 2008; 34: Pereira de Souza Neto et al. British Journal of Anaesthesia. 2011; 106(6):
30 PlethVariability Index (PVI) But About Cardiovascular Status of the patient: Requires regular (sinusal) HR (atrial fibrillation, frequent PVC) A failing right or left heart can be preload independent Not if severe valvular disease 30

31 SUMMARY Goal Directed Therapy: Volume Expansion (VE) CO Atrial filling optimal (not overstretched) means no release of ANP & no iatrogenic destruction of glycocalyx CO = SV x HR Stroke Volume: High = VE CO It gives information on where the patient is on Starling curve In: Adult patients Positive pressure ventilation No high PEEP Sinusal HR No severe valve disease Not in low perfusion SV PI = PVI Optimal Fluid Status for PVI: 10 13%

32 PVI >13% = VE will increase CO VE or NO VE depending on clinical context Hard to be more simple, less invasive (and cheaper) 32
33 Pulsus Paradoxus Clinical occurrence of PP Lowintrathoracic pressure during spontaneous inspiration Cardiac tamponade Chronic obstructive airway disease Pulmonary embolism Severe asthma, etc. 33
34 34
35 Clinical Applications of Pulse Pressure Variability Colorectal (Haifang et al, Chin Med J 2002) Pheo (Mallat et al, C J Anesth 2003) CABG (Cannesson et al, Anesth Analg 2008) PO CABG (Rex et al, B J Anaesth 2004) Hepatectomy (Solus et al, B J Anaesth 2006) High-risk (Lopes et al, Crit Care 2007) 35
36 36
37 Prediction of volume responseunderopen-chest conditions during CABG. Sander et al. Crit Care 2007, 11: R121 37







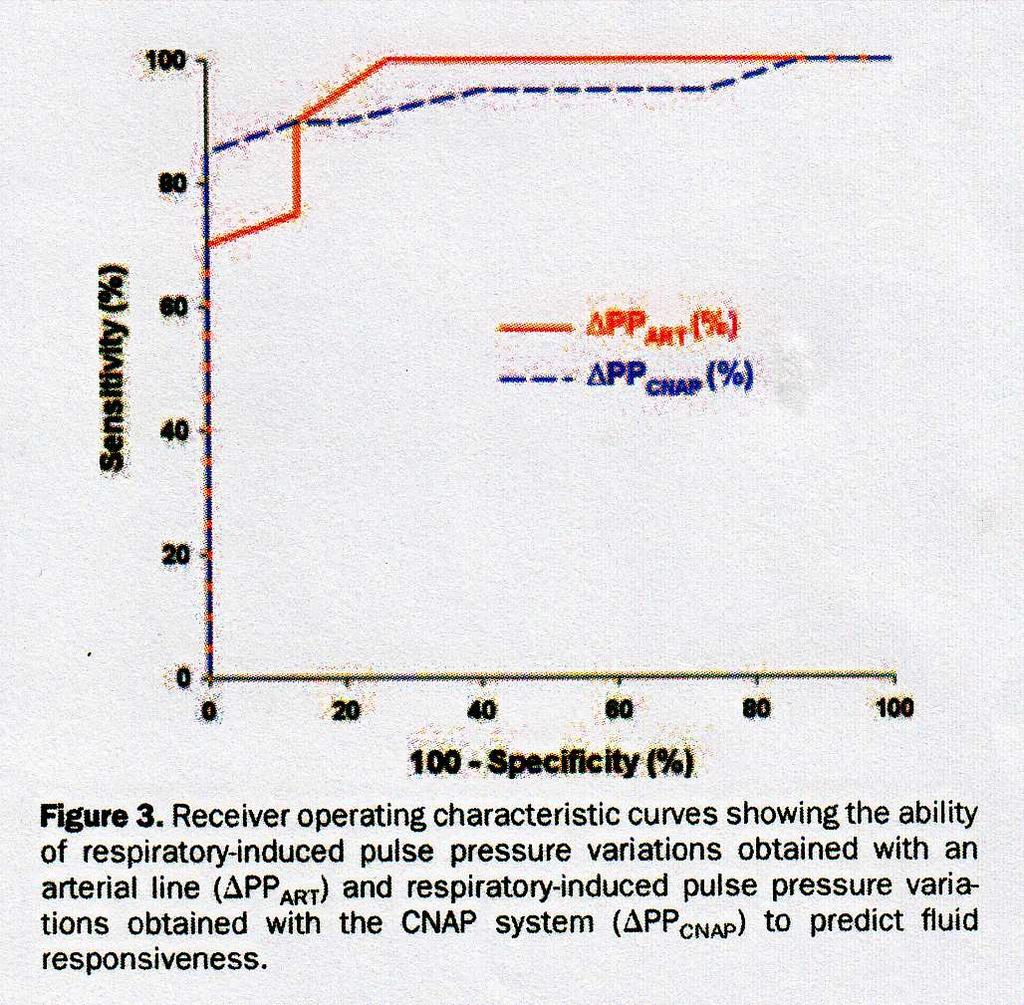
38 CNAP CNAP Invasive Arterial Pressure Blood volume in a finger is kept constant by applying corresponding pressure. The constantly changing external pressure needed to keep the volume constant cooresponds to the arterial pressure. 38
39 39
Fluid responsiveness Monitoring in Surgical and Critically Ill Patients
 Fluid responsiveness Monitoring in Surgical and Critically Ill Patients Impact clinique de la Goal-directed-therapy Patrice FORGET, M.D Cliniques universitaires Saint Luc Université catholique de Louvain,
Fluid responsiveness Monitoring in Surgical and Critically Ill Patients Impact clinique de la Goal-directed-therapy Patrice FORGET, M.D Cliniques universitaires Saint Luc Université catholique de Louvain,
The Use of Dynamic Parameters in Perioperative Fluid Management
 The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
Review Article. Interactive Physiology in Critical Illness : Pulmonary and Cardiovascular Systems. Introduction
 310 Indian Deepak J Physiol Shrivastava Pharmacol 2016; 60(4) : 310 314 Indian J Physiol Pharmacol 2016; 60(4) Review Article Interactive Physiology in Critical Illness : Pulmonary and Cardiovascular Systems
310 Indian Deepak J Physiol Shrivastava Pharmacol 2016; 60(4) : 310 314 Indian J Physiol Pharmacol 2016; 60(4) Review Article Interactive Physiology in Critical Illness : Pulmonary and Cardiovascular Systems
Fluid management. Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center
 Fluid management Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center Disclosure Consultant and research funding Edwards Lifesciences Goals of fluid therapy 1. Maintain
Fluid management Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center Disclosure Consultant and research funding Edwards Lifesciences Goals of fluid therapy 1. Maintain
Jan M. Headley, R.N. BS
 Fluid First: Using PLR & SVV to Optimize Volume Jan M. Headley, R.N. BS Disclosure Director, Clinical Marketing & Professional Education Edwards Lifesciences Does this Patient NEED Fluid?? WE Have a Problem
Fluid First: Using PLR & SVV to Optimize Volume Jan M. Headley, R.N. BS Disclosure Director, Clinical Marketing & Professional Education Edwards Lifesciences Does this Patient NEED Fluid?? WE Have a Problem
The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter
 1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter for continuous central venous oximetry (ScvO2) 3
1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter for continuous central venous oximetry (ScvO2) 3
Using Functional Hemodynamic Indicators to Guide Fluid Therapy
 CE 2.6 HOURS Continuing Education Using Functional Hemodynamic Indicators to Guide Fluid Therapy A more accurate and less invasive way to gauge responsiveness to iv volume replacement. OVERVIEW: Hemodynamic
CE 2.6 HOURS Continuing Education Using Functional Hemodynamic Indicators to Guide Fluid Therapy A more accurate and less invasive way to gauge responsiveness to iv volume replacement. OVERVIEW: Hemodynamic
The cornerstone of treating patients with hypotension,
 Does the Central Venous Pressure Predict Fluid Responsiveness? An Updated Meta-Analysis and a Plea for Some Common Sense* Paul E. Marik, MD, FCCM 1 ; Rodrigo Cavallazzi, MD 2 Background: Aim: Data Sources:
Does the Central Venous Pressure Predict Fluid Responsiveness? An Updated Meta-Analysis and a Plea for Some Common Sense* Paul E. Marik, MD, FCCM 1 ; Rodrigo Cavallazzi, MD 2 Background: Aim: Data Sources:
Actualités sur le remplissage peropératoire. Philippe Van der Linden MD, PhD
 Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
PulsioFlex Patient focused flexibility
 PulsioFlex Patient focused flexibility Modular platform with intelligent visualisation for advanced patient Minimally invasive perioperative cardiac output trend with ProAQT Enables calibrated cardiac
PulsioFlex Patient focused flexibility Modular platform with intelligent visualisation for advanced patient Minimally invasive perioperative cardiac output trend with ProAQT Enables calibrated cardiac
Perioperative Fluid Management in ERPs
 Perioperative Fluid Management in ERPs Robert H. Thiele, M.D. Assistant Professor University of Virginia First Do No Harm Intravenous fluids should be considered a pharmacotherapeutic agent Just like all
Perioperative Fluid Management in ERPs Robert H. Thiele, M.D. Assistant Professor University of Virginia First Do No Harm Intravenous fluids should be considered a pharmacotherapeutic agent Just like all
Les solutés de remplissage. Philippe Van der Linden MD, PhD
 Les solutés de remplissage Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Fluid Resuscitation Morbidity Procedure Co-morbidities
Les solutés de remplissage Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Fluid Resuscitation Morbidity Procedure Co-morbidities
Goal-directed vs Flow-guidedresponsive
 Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
PiCCO based algorithms
 European Society of Anaesthesiologists Annual Meeting 12.-15. June 2010, Helsinki, Finland PiCCO based algorithms Berthold Bein, MD, PhD, DEAA Department of Anaesthesiology and Intensive Care Medicine
European Society of Anaesthesiologists Annual Meeting 12.-15. June 2010, Helsinki, Finland PiCCO based algorithms Berthold Bein, MD, PhD, DEAA Department of Anaesthesiology and Intensive Care Medicine
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Topics to be Covered. Cardiac Measurements. Distribution of Blood Volume. Distribution of Pulmonary Ventilation & Blood Flow
 Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL. Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium
 FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium Why do we want to administer fluids? To correct hypovolemia? To increase
FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium Why do we want to administer fluids? To correct hypovolemia? To increase
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency
 Application of ICG in Intensive Care and Emergency") Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Assessing Preload Responsiveness Using Arterial Pressure Based Technologies. Patricia A. Meehan, RN, MS Education Consultant Edwards Lifesciences, LLC
 Assessing Preload Responsiveness Using Arterial Pressure Based Technologies Patricia A. Meehan, RN, MS Education Consultant Edwards Lifesciences, LLC Content Description : Fluid administration is a first
Assessing Preload Responsiveness Using Arterial Pressure Based Technologies Patricia A. Meehan, RN, MS Education Consultant Edwards Lifesciences, LLC Content Description : Fluid administration is a first
Impedance Cardiography (ICG) Method, Technology and Validity
 Method, Technology and Validity") Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
Principles of Biomedical Systems & Devices. Lecture 8: Cardiovascular Dynamics Dr. Maria Tahamont
 Principles of Biomedical Systems & Devices Lecture 8: Cardiovascular Dynamics Dr. Maria Tahamont Review of Cardiac Anatomy Four chambers Two atria-receive blood from the vena cave and pulmonary veins Two
Principles of Biomedical Systems & Devices Lecture 8: Cardiovascular Dynamics Dr. Maria Tahamont Review of Cardiac Anatomy Four chambers Two atria-receive blood from the vena cave and pulmonary veins Two
NONINVASIVE/MINIMALLY INVASIVE HEMODYNAMIC MONITORING
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Chapter 9, Part 2. Cardiocirculatory Adjustments to Exercise
 Chapter 9, Part 2 Cardiocirculatory Adjustments to Exercise Electrical Activity of the Heart Contraction of the heart depends on electrical stimulation of the myocardium Impulse is initiated in the right
Chapter 9, Part 2 Cardiocirculatory Adjustments to Exercise Electrical Activity of the Heart Contraction of the heart depends on electrical stimulation of the myocardium Impulse is initiated in the right
Perioperative Goal- Protocol Summary
 Perioperative Goal- Directed Therapy Protocol Summary Evidence-based, perioperative Goal-Directed Therapy (GDT) protocols. Several single centre randomized controlled trials, meta-analysis and quality
Perioperative Goal- Directed Therapy Protocol Summary Evidence-based, perioperative Goal-Directed Therapy (GDT) protocols. Several single centre randomized controlled trials, meta-analysis and quality
PCV and PAOP Old habits die hard!
 PCV and PAOP Old habits die hard! F Javier Belda MD, PhD Head of Department Associate Professor Anaesthesia and Critical Care Hospital Clínico Universitario Valencia (SPAIN) An old example TOBACO SMOKING
PCV and PAOP Old habits die hard! F Javier Belda MD, PhD Head of Department Associate Professor Anaesthesia and Critical Care Hospital Clínico Universitario Valencia (SPAIN) An old example TOBACO SMOKING
Effects of mechanical ventilation on organ function. Masterclass ICU nurses
 Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Perioperative Goal- Protocol Summary
 Perioperative Goal- Directed Therapy Protocol Summary Evidence-based, perioperative Goal-Directed Therapy (GDT) protocols. Several single centre randomized controlled trials, meta-analysis and quality
Perioperative Goal- Directed Therapy Protocol Summary Evidence-based, perioperative Goal-Directed Therapy (GDT) protocols. Several single centre randomized controlled trials, meta-analysis and quality
Hemodynamic Monitoring To Guide Volume Resuscitation
 Hemodynamic Monitoring To Guide Volume Resuscitation Nick Johnson, MD Acting Assistant Professor Division of Emergency Medicine Attending Physician, Medical & Neuro-Intensive Care Units Harborview Medical
Hemodynamic Monitoring To Guide Volume Resuscitation Nick Johnson, MD Acting Assistant Professor Division of Emergency Medicine Attending Physician, Medical & Neuro-Intensive Care Units Harborview Medical
Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS
 Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS a mismatch between tissue perfusion and metabolic demands the heart, the vasculature
Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS a mismatch between tissue perfusion and metabolic demands the heart, the vasculature
Intra-operative Echocardiography: When to Go Back on Pump
 Intra-operative Echocardiography: When to Go Back on Pump GREGORIO G. ROGELIO, MD., F.P.C.C. OUTLINE A. Indications for Intraoperative Echocardiography B. Role of Intraoperative Echocardiography C. Criteria
Intra-operative Echocardiography: When to Go Back on Pump GREGORIO G. ROGELIO, MD., F.P.C.C. OUTLINE A. Indications for Intraoperative Echocardiography B. Role of Intraoperative Echocardiography C. Criteria
Nurse Driven Fluid Optimization Using Dynamic Assessments
 Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
The Hemodynamic Puzzle
 The Hemodynamic Puzzle SVV NIRS O 2 ER Lactate Energy Metabolism (Oxygen Consumption) (Ml/min/m 2 ) Oxygen Debt: To Pay or Not to Pay? Full Recovery Possible Delayed Repayment of O 2 Debt Oxygen Deficit
The Hemodynamic Puzzle SVV NIRS O 2 ER Lactate Energy Metabolism (Oxygen Consumption) (Ml/min/m 2 ) Oxygen Debt: To Pay or Not to Pay? Full Recovery Possible Delayed Repayment of O 2 Debt Oxygen Deficit
Cardiorespiratory Interactions:
 Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
ICU Volume 12 - Issue 4 - Winter 2012/ Matrix Features
 ICU Volume 12 - Issue 4 - Winter 2012/2013 - Matrix Features Fluid Management in Critically Ill Patients: A Guided Approach Prof. Antonio Artigas, MD, PhD ICU Management & Practice Editorial Board Member
ICU Volume 12 - Issue 4 - Winter 2012/2013 - Matrix Features Fluid Management in Critically Ill Patients: A Guided Approach Prof. Antonio Artigas, MD, PhD ICU Management & Practice Editorial Board Member
Sepsis Wave II Webinar Series. Sepsis Reassessment
 Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
UPMC Critical Care
 UPMC Critical Care www.ccm.pitt.edu Cardiovascular insufficiency with Initiation and Withdrawal of Mechanical Ventilation Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of
UPMC Critical Care www.ccm.pitt.edu Cardiovascular insufficiency with Initiation and Withdrawal of Mechanical Ventilation Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of
Heart Pump and Cardiac Cycle. Faisal I. Mohammed, MD, PhD
 Heart Pump and Cardiac Cycle Faisal I. Mohammed, MD, PhD 1 Objectives To understand the volume, mechanical, pressure and electrical changes during the cardiac cycle To understand the inter-relationship
Heart Pump and Cardiac Cycle Faisal I. Mohammed, MD, PhD 1 Objectives To understand the volume, mechanical, pressure and electrical changes during the cardiac cycle To understand the inter-relationship
Swan Ganz catheter: Does it still have a role? Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium
 Swan Ganz catheter: Does it still have a role? Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium How can cardiac output be measured? Thermodilution Arterial waveform
Swan Ganz catheter: Does it still have a role? Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium How can cardiac output be measured? Thermodilution Arterial waveform
haemodynamic monitoring
 haemodynamic monitoring Mostcare Up is the only monitor able to follow, in real time and from beat to beat, even the slightest haemodynamic variations in the patient. The patented algorithm based on the
haemodynamic monitoring Mostcare Up is the only monitor able to follow, in real time and from beat to beat, even the slightest haemodynamic variations in the patient. The patented algorithm based on the
Functional Hemodynamic Monitoring and Management A practical Approach
 Functional Hemodynamic Monitoring and Management A practical Approach Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf University Hospital Hamburg, Germany Euronaesthesia
Functional Hemodynamic Monitoring and Management A practical Approach Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf University Hospital Hamburg, Germany Euronaesthesia
Goal-directed resuscitation in sepsis; a case-based approach
 Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
Cardiac output and Venous Return. Faisal I. Mohammed, MD, PhD
 Cardiac output and Venous Return Faisal I. Mohammed, MD, PhD 1 Objectives Define cardiac output and venous return Describe the methods of measurement of CO Outline the factors that regulate cardiac output
Cardiac output and Venous Return Faisal I. Mohammed, MD, PhD 1 Objectives Define cardiac output and venous return Describe the methods of measurement of CO Outline the factors that regulate cardiac output
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Hemodynamic monitoring beyond cardiac output
 Hemodynamic monitoring beyond cardiac output Prof Xavier MONNET Medical Intensive Care Unit Bicêtre Hospital Assistance publique Hôpitaux de Paris FRANCE Conflicts of interest Lilly GlaxoSmithKline Pulsion
Hemodynamic monitoring beyond cardiac output Prof Xavier MONNET Medical Intensive Care Unit Bicêtre Hospital Assistance publique Hôpitaux de Paris FRANCE Conflicts of interest Lilly GlaxoSmithKline Pulsion
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
TOPIC : Cardiogenic Shock
 University of Ferrara Department of Morphology, Surgery and Experimental Medicine. Section of Anaesthesia and Intensive Care Medicine TOPIC : Cardiogenic Shock What is shock? Shock is a condition of inadequate
University of Ferrara Department of Morphology, Surgery and Experimental Medicine. Section of Anaesthesia and Intensive Care Medicine TOPIC : Cardiogenic Shock What is shock? Shock is a condition of inadequate
Fluid Responsiveness Monitoring In Surgical and Critically Ill Patients
 Fluid Responsiveness Monitoring In Surgical and Critically Ill Patients Clinical Impact of Goal-Directed Therapy Release Date: September 1, 2010 Expiration Date: September 30, 2011 Needs Statement Volume
Fluid Responsiveness Monitoring In Surgical and Critically Ill Patients Clinical Impact of Goal-Directed Therapy Release Date: September 1, 2010 Expiration Date: September 30, 2011 Needs Statement Volume
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL
 FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children?
 Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia (Spain) Pulsion MAB
 Pulsion MAB") State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
Index. K Knobology, TTE artifact, image resolution, ultrasound, 14
 A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
How can the PiCCO improve protocolized care?
 How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART
 FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
Hemodynamic Monitoring in Critically ill Patients in Arthur Simonnet, interne Tuteur : Pr. Raphaël Favory
 Hemodynamic Monitoring in Critically ill Patients in 2017 Arthur Simonnet, interne Tuteur : Pr. Raphaël Favory Rationale for Hemodynamic Monitoring Identify the presence of hemodynamic instability Identify
Hemodynamic Monitoring in Critically ill Patients in 2017 Arthur Simonnet, interne Tuteur : Pr. Raphaël Favory Rationale for Hemodynamic Monitoring Identify the presence of hemodynamic instability Identify
Invasive Cardiac Output Monitoring and Pulse Contour Analysis. Harshad B. Ranchod Paediatric Intensivist Chris Hani Baragwanath Hospital COPICON 2011
 Invasive Cardiac Output Monitoring and Pulse Contour Analysis Harshad B. Ranchod Paediatric Intensivist Chris Hani Baragwanath Hospital COPICON 2011 Introduction The primary goal of haemodynamic monitoring
Invasive Cardiac Output Monitoring and Pulse Contour Analysis Harshad B. Ranchod Paediatric Intensivist Chris Hani Baragwanath Hospital COPICON 2011 Introduction The primary goal of haemodynamic monitoring
During exercise the heart rate is 190 bpm and the stroke volume is 115 ml/beat. What is the cardiac output?
 The Cardiovascular System Part III: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Be able to calculate cardiac output (CO) be able to define heart rate
The Cardiovascular System Part III: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Be able to calculate cardiac output (CO) be able to define heart rate
Preload optimisation in severe sepsis and septic shock
 Preload optimisation in severe sepsis and septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris South France Conflicts of interest Member of themedical Advisory Board ofpulsion
Preload optimisation in severe sepsis and septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris South France Conflicts of interest Member of themedical Advisory Board ofpulsion
Perioperative Goal Directed Therapy Improving the Quality of Care for Our Surgical Patients
 Perioperative Goal Directed Therapy Improving the Quality of Care for Our Surgical Patients DESIRÉE CHAPPELL, CRNA ERAS TEAM LEAD NORTON AUDUBON HOSPITAL, LOUISVILLE, KY Disclosure Edwards Lifesciences,
Perioperative Goal Directed Therapy Improving the Quality of Care for Our Surgical Patients DESIRÉE CHAPPELL, CRNA ERAS TEAM LEAD NORTON AUDUBON HOSPITAL, LOUISVILLE, KY Disclosure Edwards Lifesciences,
Edwards Critical Care Education. Perioperative Goal-Directed Therapy Protocol Summary
 Edwards Critical Care Education Perioperative Goal-Directed Therapy Protocol Summary Issue Date: November 2014 Evidence-based, Perioperative Goal-Directed Therapy (PGDT) protocols Note: This protocol summary
Edwards Critical Care Education Perioperative Goal-Directed Therapy Protocol Summary Issue Date: November 2014 Evidence-based, Perioperative Goal-Directed Therapy (PGDT) protocols Note: This protocol summary
Respiratory Physiology and the Impact of Different Modes of Ventilation on the Photoplethysmographic Waveform
 Sensors 2012, 12, 2236-2254; doi:10.3390/s120202236 Review OPEN ACCESS sensors ISSN 1424-8220 www.mdpi.com/journal/sensors Respiratory Physiology and the Impact of Different Modes of Ventilation on the
Sensors 2012, 12, 2236-2254; doi:10.3390/s120202236 Review OPEN ACCESS sensors ISSN 1424-8220 www.mdpi.com/journal/sensors Respiratory Physiology and the Impact of Different Modes of Ventilation on the
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
SIKLUS JANTUNG. Rahmatina B. Herman
 SIKLUS JANTUNG Rahmatina B. Herman The Cardiac Cycle Definition: The cardiac events that occur from the beginning of one heartbeat to the beginning of the next The cardiac cycle consists of: - Diastole
SIKLUS JANTUNG Rahmatina B. Herman The Cardiac Cycle Definition: The cardiac events that occur from the beginning of one heartbeat to the beginning of the next The cardiac cycle consists of: - Diastole
Pre-operative usage of IABP for patients for by pass surgery
 Pre-operative usage of IABP for patients for by pass surgery Mitrev Z, Anguseva T, Hristov N Special hospital for surgery Filip Vtori Skopje - Macedonija Oktomvri, 2008 IABP Background Preload Afterload
Pre-operative usage of IABP for patients for by pass surgery Mitrev Z, Anguseva T, Hristov N Special hospital for surgery Filip Vtori Skopje - Macedonija Oktomvri, 2008 IABP Background Preload Afterload
Alterações na Pressão Arterial durante Ventilação Mecânica. Rafael Lisboa de Souza Especialista em Medicina Intensiva pela UFSC e AMIB
 Alterações na Pressão Arterial durante Ventilação Mecânica Rafael Lisboa de Souza Especialista em Medicina Intensiva pela UFSC e AMIB Changes in Arterial Pressure during Mechanical Ven4la4on. Michard,
Alterações na Pressão Arterial durante Ventilação Mecânica Rafael Lisboa de Souza Especialista em Medicina Intensiva pela UFSC e AMIB Changes in Arterial Pressure during Mechanical Ven4la4on. Michard,
Sepsis and septic shock Practical hemodynamic consequences. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
The circulatory system
 Introduction to Physiology (Course # 72336) 1 הלב עקרונות בסיסיים (הכנה למעבדת לב) Adi Mizrahi mizrahia@cc.huji.ac.il Textbook Chapter 12 2 The circulatory system To the heart Away from the heart 3 L 2.5
Introduction to Physiology (Course # 72336) 1 הלב עקרונות בסיסיים (הכנה למעבדת לב) Adi Mizrahi mizrahia@cc.huji.ac.il Textbook Chapter 12 2 The circulatory system To the heart Away from the heart 3 L 2.5
Hemodynamics: Cardiac and Vascular Jeff Davis, RRT, RCIS
 Hemodynamics: Cardiac and Vascular Jeff Davis, RRT, RCIS Program Director, Cardiovascular Technology Florida SouthWestern State College Fort Myers, FL Disclosures Speaker s Bureau: None Stockholder: None
Hemodynamics: Cardiac and Vascular Jeff Davis, RRT, RCIS Program Director, Cardiovascular Technology Florida SouthWestern State College Fort Myers, FL Disclosures Speaker s Bureau: None Stockholder: None
From PV loop to Starling curve. S Magder Division of Critical Care, McGill University Health Centre
 From PV loop to Starling curve S Magder Division of Critical Care, McGill University Health Centre Otto Frank 1890 s Frank-Starling Relationship ( The Law of the Heart ) The greater the initial stretch
From PV loop to Starling curve S Magder Division of Critical Care, McGill University Health Centre Otto Frank 1890 s Frank-Starling Relationship ( The Law of the Heart ) The greater the initial stretch
Cardiac Output Monitoring - 6
 Cardiac Output Monitoring - 6 How to use Wrexham s Cardiac Output Monitors. Wrexham Maelor Critical Care Version 02.05.16 Introduction Types of Devices: NICOM - Cheetah Oesophageal Doppler +/- Pulse Contour
Cardiac Output Monitoring - 6 How to use Wrexham s Cardiac Output Monitors. Wrexham Maelor Critical Care Version 02.05.16 Introduction Types of Devices: NICOM - Cheetah Oesophageal Doppler +/- Pulse Contour
Introduction to Physiology (Course # 72336) 1. Adi Mizrahi Textbook Chapter 12
 1. Adi Mizrahi Textbook Chapter 12") Introduction to Physiology (Course # 72336) 1 עקרונות בסיסיים (הכנה למעבדת לב) הלב Adi Mizrahi mizrahia@cc.huji.ac.il Textbook Chapter 12 2 The circulatory system To the heart Away from the heart 3 L 2.5
Introduction to Physiology (Course # 72336) 1 עקרונות בסיסיים (הכנה למעבדת לב) הלב Adi Mizrahi mizrahia@cc.huji.ac.il Textbook Chapter 12 2 The circulatory system To the heart Away from the heart 3 L 2.5
Edwards Critical Care Education. Perioperative Goal-Directed Therapy Protocol Summary
 Edwards Critical Care Education Perioperative Goal-Directed Therapy Protocol Summary Issue Date: March 2013 Evidence-based, Perioperative Goal-Directed Therapy (PGDT) protocols Note: This protocol summary
Edwards Critical Care Education Perioperative Goal-Directed Therapy Protocol Summary Issue Date: March 2013 Evidence-based, Perioperative Goal-Directed Therapy (PGDT) protocols Note: This protocol summary
Age-related changes in cardiovascular system. Dr. Rehab Gwada
 Age-related changes in cardiovascular system Dr. Rehab Gwada Objectives explain the main structural and functional changes in cardiovascular system associated with normal aging Introduction aging results
Age-related changes in cardiovascular system Dr. Rehab Gwada Objectives explain the main structural and functional changes in cardiovascular system associated with normal aging Introduction aging results
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
3/14/2017. Disclosures. None. Outline. Fluid Management and Hemodynamic Assessment Paul Marik, MD, FCCP, FCCM
 Fluid Management and Hemodynamic Assessment Paul Marik, MD, FCCP, FCCM Disclosures Stocks Advisory boards Grants Speakers Bureau None Outline Hemodynamic Goals Fluid Resuscitation Historical Perspective
Fluid Management and Hemodynamic Assessment Paul Marik, MD, FCCP, FCCM Disclosures Stocks Advisory boards Grants Speakers Bureau None Outline Hemodynamic Goals Fluid Resuscitation Historical Perspective
Cardiac Output (C.O.) Regulation of Cardiac Output
 Regulation of Cardiac Output") Cardiac Output (C.O.) Is the volume of the blood pumped by each ventricle per minute (5 Litre) Stroke volume: Is the volume of the blood pumped by each ventricle per beat. Stroke volume = End diastolic
Cardiac Output (C.O.) Is the volume of the blood pumped by each ventricle per minute (5 Litre) Stroke volume: Is the volume of the blood pumped by each ventricle per beat. Stroke volume = End diastolic
Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy
 Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy antonio.pesenti@unimi.it CCCF 2017 Is it useful? YES: CVP It is an important diagnostic element! Your best guess CVP
Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy antonio.pesenti@unimi.it CCCF 2017 Is it useful? YES: CVP It is an important diagnostic element! Your best guess CVP
Hemodynamic Monitoring
 Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
UPMC Critical Care
 UPMC Critical Care www.ccm.pitt.edu Shock and Monitoring Samuel A. Tisherman, MD, FACS, FCCM Professor Departments of CCM and Surgery University of Pittsburgh Shock Anaerobic metabolism Lactic acidosis
UPMC Critical Care www.ccm.pitt.edu Shock and Monitoring Samuel A. Tisherman, MD, FACS, FCCM Professor Departments of CCM and Surgery University of Pittsburgh Shock Anaerobic metabolism Lactic acidosis
Norepinephrine in septic shock
 Norepinephrine in septic shock Prof. Zsolt Molnár zsoltmolna@gmail.com Department of Anaesthesia and Intensive Therapy University of Szeged, Hungary A few months ago should we give it earlier? (Courtesy
Norepinephrine in septic shock Prof. Zsolt Molnár zsoltmolna@gmail.com Department of Anaesthesia and Intensive Therapy University of Szeged, Hungary A few months ago should we give it earlier? (Courtesy
Continuous and noninvasive arterial blood pressure monitoring
 Continuous and noninvasive arterial blood pressure monitoring Pr. Jean-Luc Fellahi fellahi-jl@chu-caen.fr Pôle Réanimations-Anesthésie-SAMU, CHU de Caen UFR de Médecine, EA4650, Université de Caen Basse-Normandie
Continuous and noninvasive arterial blood pressure monitoring Pr. Jean-Luc Fellahi fellahi-jl@chu-caen.fr Pôle Réanimations-Anesthésie-SAMU, CHU de Caen UFR de Médecine, EA4650, Université de Caen Basse-Normandie
Evolutionary origins of the right ventricle. S Magder Department of Critical Care, McGill University Health Centre
 Evolutionary origins of the right ventricle S Magder Department of Critical Care, McGill University Health Centre Fully separated four chamber heart only evolved in birds and mammals What are the evolutionary
Evolutionary origins of the right ventricle S Magder Department of Critical Care, McGill University Health Centre Fully separated four chamber heart only evolved in birds and mammals What are the evolutionary
Edwards Critical Care Education. Perioperative Goal-Directed Therapy Protocol Summary
 Edwards Critical Care Education Perioperative Goal-Directed Therapy Protocol Summary Issue Date: March 2013 Evidence-based, Perioperative Goal-Directed Therapy (PGDT) protocols Note: This protocol summary
Edwards Critical Care Education Perioperative Goal-Directed Therapy Protocol Summary Issue Date: March 2013 Evidence-based, Perioperative Goal-Directed Therapy (PGDT) protocols Note: This protocol summary
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
DESCRIBE THE FACTORS AFFECTING CARDIAC OUTPUT.
 DESCRIBE THE FACTORS AFFECTING CARDIAC OUTPUT. BY: DISHA PRAKASH I MBBS, ROLL NO: 16M069 OBJECTIVES OF LEARNING Terminology and conceptual understanding of Cardiac Output. Factors regulating Cardiac Output.
DESCRIBE THE FACTORS AFFECTING CARDIAC OUTPUT. BY: DISHA PRAKASH I MBBS, ROLL NO: 16M069 OBJECTIVES OF LEARNING Terminology and conceptual understanding of Cardiac Output. Factors regulating Cardiac Output.
Making the Case For Less Invasive Flow Based Parameters: APCO + SVV. Patricia A. Meehan, RN, MS, CCRN (a) Education Consultant Edwards Lifesciences
 Education Consultant Edwards Lifesciences") Making the Case For Less Invasive Flow Based Parameters: APCO + SVV Patricia A. Meehan, RN, MS, CCRN (a) Education Consultant Edwards Lifesciences A New Gold Standard? How does the system work? Sensor
Making the Case For Less Invasive Flow Based Parameters: APCO + SVV Patricia A. Meehan, RN, MS, CCRN (a) Education Consultant Edwards Lifesciences A New Gold Standard? How does the system work? Sensor
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
Mechanical ventilation induced or exacerbated right ventricular failure
 Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Fluid responsiveness and extravascular lung water
 Fluid responsiveness and extravascular lung water Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Conflicts of interest Member of the Medical Advisory Board of Maquet/Pulsion
Fluid responsiveness and extravascular lung water Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Conflicts of interest Member of the Medical Advisory Board of Maquet/Pulsion
BME 5742 Bio-Systems Modeling and Control. Lecture 41 Heart & Blood Circulation Heart Function Basics
 BME 5742 Bio-Systems Modeling and Control Lecture 41 Heart & Blood Circulation Heart Function Basics Dr. Zvi Roth (FAU) 1 Pumps A pump is a device that accepts fluid at a low pressure P 1 and outputs the
BME 5742 Bio-Systems Modeling and Control Lecture 41 Heart & Blood Circulation Heart Function Basics Dr. Zvi Roth (FAU) 1 Pumps A pump is a device that accepts fluid at a low pressure P 1 and outputs the
Obligatory joke. The case for why it matters. Sepsis: More is more. Goal-Directed Fluid Resuscitation 6/1/2013
 Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR
 IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR The ability to evaluate and manage a critically ill patient is one of the most important skills any intensivist
IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR The ability to evaluate and manage a critically ill patient is one of the most important skills any intensivist
Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University
 Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University of Texas Health Science Center, Department of Emergency
Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University of Texas Health Science Center, Department of Emergency
Cardiac filling pressures are not appropriate to predict hemodynamic response to volume challenge*
 Cardiac filling pressures are not appropriate to predict hemodynamic response to volume challenge* David Osman, MD; Christophe Ridel, MD; Patrick Ray, MD; Xavier Monnet, MD, PhD; Nadia Anguel, MD; Christian
Cardiac filling pressures are not appropriate to predict hemodynamic response to volume challenge* David Osman, MD; Christophe Ridel, MD; Patrick Ray, MD; Xavier Monnet, MD, PhD; Nadia Anguel, MD; Christian
PA Catheters - Useful or Not
 PA Catheters - Useful or Not Perioperative in Liver Transplantation ILTS/ASA, San Francisco, 2003 Claus U. Niemann, MD Department of Anesthesia and Perioperative Division of Liver Transplantation University
PA Catheters - Useful or Not Perioperative in Liver Transplantation ILTS/ASA, San Francisco, 2003 Claus U. Niemann, MD Department of Anesthesia and Perioperative Division of Liver Transplantation University
-12. -Ensherah Mokheemer - ABDULLAH ZREQAT. -Faisal Mohammad. 1 P a g e
 -12 -Ensherah Mokheemer - ABDULLAH ZREQAT -Faisal Mohammad 1 P a g e In the previous lecture we talked about: - cardiac index: we use the cardiac index to compare the cardiac output between different individuals,
-12 -Ensherah Mokheemer - ABDULLAH ZREQAT -Faisal Mohammad 1 P a g e In the previous lecture we talked about: - cardiac index: we use the cardiac index to compare the cardiac output between different individuals,
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT.
 HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT