Cardiology update Clinical Decision Seminar: Difficult ECG Interpretations February 13th, 2013 Lars Eckardt Firat Duru Corinna Brunckhorst
|
|
|
- Emory McCormick
- 6 years ago
- Views:
Transcription
1 Cardiology update Clinical Decision Seminar: Difficult ECG Interpretations February 13th, 2013 Lars Eckardt Firat Duru Corinna Brunckhorst
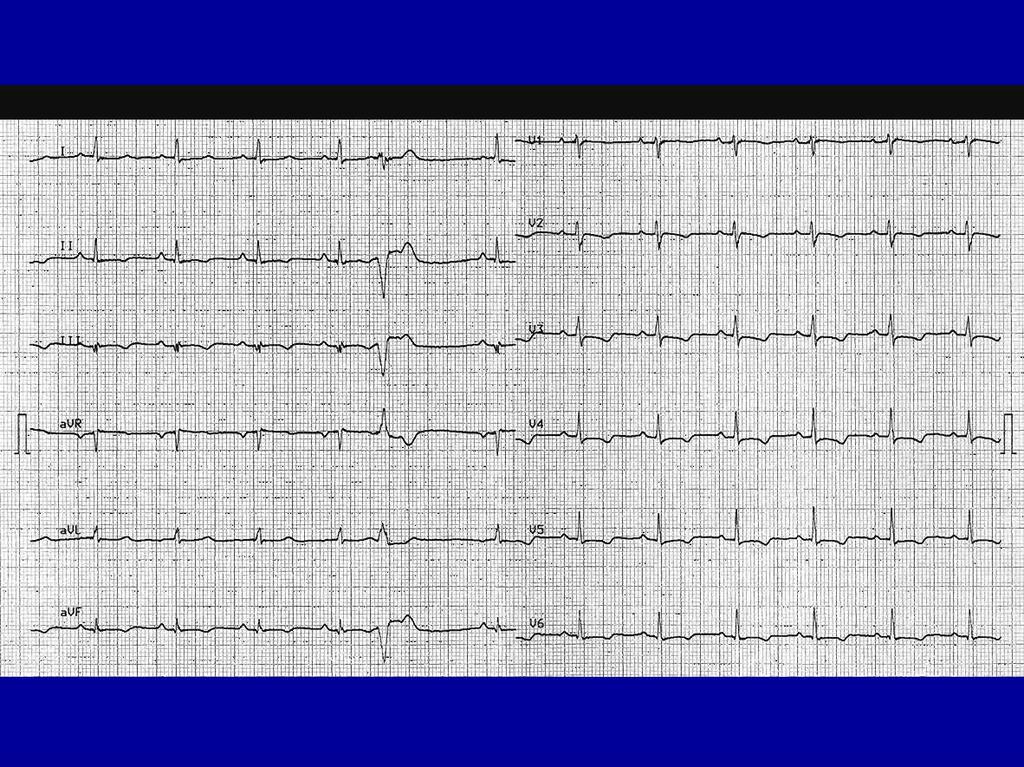
2 1. Patient K.P., male, 68 years Fatigue Exercise intolerance for one year Echo: globally reduced LV Function: EF 30%

3

4 1. Atrial Tachycardia 1a. What is the diagnosis? 2. Permanent junctional reciprocating tachycardia 3. Atrial flutter 4. AVNRT 5. AVRT 6. Can be anything of the above

5
6 1. Atrial Tachycardia 1b. What is the diagnosis? 2. Permanent junctional reciprocating tachycardia 3. Atrial flutter 4. AVNRT 5. AVRT 6. Can be anything of the above
7 RA Atrial Flutter FO CSO TA VCI inferiorer Isthmus


8
9 RA Typical Atrial Flutter Type I FO CSO TA VCI inferiorer Isthmus


10 RA Typical Atrial Flutter Type II FO CSO TA VCI inferiorer Isthmus

11 Atrial Flutter

12

13
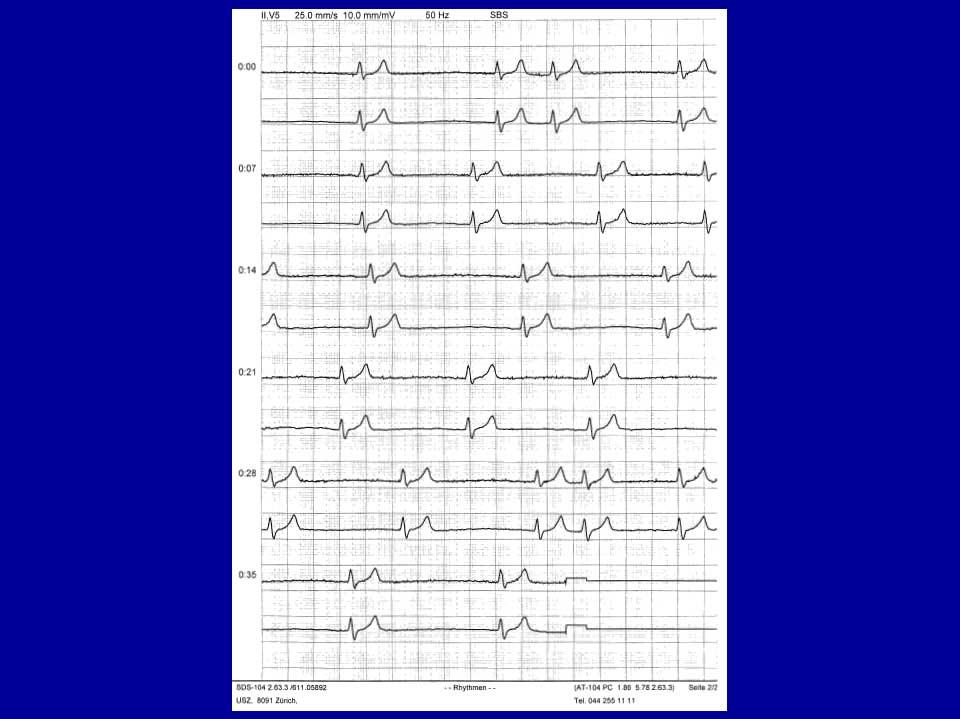
14 Patient K.P., male, 68 years Check-up 3 months after ablation: Symptoms resolved Back to normal activity Echo: LV Function recovered: EF 55%
15 2. Patient S.K., male, 52 years Palpitations SOB Palpitations during Skitour which did not terminate by itself

16

17 2. Diagnosis 1. Polymorphic VT 2. Monomorphic VT and Sinustach 3. SVT with and without aberrancy 4. VT and SVT 5. Sinus Tach with BBB 6. SVT with and without linking 7. Don t know

18
19 Treatment EP study: AVNRT Slow pathway modification
20 3. Patient E.H, male, 24 years Unresponsive at night on street Smell of alcohol


21
22 3a. What does this patient need? 1. Calcium 2. Magnesium 3. Potassium 4. Slight cooling 5. Core warming 6. Glucose-Insuline
23 3b. What is the name of these waves? 1. Epsilon Wave 2. Delta Wave 3. Alpha wave 4. J wave 5. Osborne wave 6. 4 and 5
24 Typical ECG Features of Hypothermia 1. Sinus Bradycardia 2. P waves widened 3. QRS widened 4. Osborn waves (J waves): Concave elevation at end of QRS-Beginning of ST 5. Prolonged QT
25 Complications Myocardial damage (reversible) Hypotension AF VF Pulmonary Hematologic Renal

26 Prominent J deflection attributed to hypothermia first reported in 1938 by Tomaszewski. J waves described in 1953 by John J. Osborn 1917 and named after him ( American Journal of Physiology on experimental hypothermia)
27 4. Patient P.G, male, 54 years Prolonged URI Chest pain Otherwise healthy







28
29 4a. Diagnosis 1. SA Block 2. AV Block I 3. AV Block II Type Wenckebach 4. AV Block II Type Mobitz 5. AV Block III 6. Don t know (indeterminate block)
30 Indeterminate Block
31 4b. What do we do? 1. Implant a pace-maker 2. Implant an event recorder 3. Reassure and send home 4. Exercise test 5. EP Study
32 5. Patient R.P., female, 57 years No previous medical history
33 Presenting complaint acute onset of palpitations, dizziness, presyncope, nausea spontaneous recovery recurrence of the same symptoms during afternoon walk 3h later

34
35 5a. Diagnosis of this WCT? 1. SVT with Aberrency? 2. Ventricular tachycardia? 3. WPW with antidromic AV Tachycardia?
36 SVT-VT Differential Diagnosis AV-Dissociation? no no RS in precordial leads? no yes yes VT VT R-S >100 ms in one precordial lead? no yes morphology criteria for V1 and V6 are met? VT no yes VT SVT with Aberration Brugada, Circulation 1991;83(5):
37 SVT-VT Differential Diagnosis AV-Dissociation? no no RS in precordial leads? no yes yes VT VT R-S >100 ms in one precordial lead? no yes morphology criteria for V1 and V6 are met? VT no yes VT SVT with Aberration Brugada, Circulation 1991;83(5):
38 5b. Origin of this VT 1. LV base 2. LV apex 3. RV base 4. RV apex 5. Can t tell
39
40 Major criteria ARVC Severe structural abnormalities of the RV Fibrofatty replacement of myocardial tissue Epsilon waves at right precordium (V1-V3) Familial disease (necropsy or surgery) Task Force Criteria, Mc Kenna, 2010
41 Minor criteria ARVC Mild structural abnormalities of the RV Inverted T waves at right precordium (V2, V3) Late potentials (SAECG) LBBB type VT or frequent VES (>1000/d) Family hx of SCD or ARVD Task Force Criteria, Mc Kenna, 2010
42 ARVC Program Zurich Founded in June 2011 National and international collaboration: Research and clinical of according subspecialties
43 6. Patient H.F., male, 67 years «Not feeling well» for one month Fever UTI Now: nausea, insomnia

44

45
46

47 6. What is the diagnosis? 1. Ischemia 2. Myocardial Infarction 3. Hypertrophy 4. Hypertensive crisis 5. Hyperkalemia 6. Hypokalemia
48 Hyperkalemia 2% of Potassium extracellular Ratio: K(intra) : K(extra) determines Membranepotential Hyperkalemia: Ratio: K(intra) : K(extra) decreases Hyperkalemia decreases Membranepotential Moderate Hyperkalemia: Depolarisation, increased exitability (Nernstequation) Severe Hyperkalemia: Depolarisation Sodium System stays inactivated
49 Hyperkalemia Cave: Arrhythmias (sinusoidal, VT, Asystolie) Pacing Threshold increases! Negativ inotrope Negativ dromotrope Principle of cardioplegic solution
50 Hyperkalemia mmol/l: Peaked T-Waves QRS Widening PQ-Prolongation, AV Block >7.0 mmol/l: no P-Waves Extremely wide QRS VT ( sinusoidal ) Asystolie
51 K 6.8 mmol/l K 7.5 mmol/l K 8.5 mmol/l K 4.8 mmol/l
52 K 6.8 mmol/l K 7.5 mmol/l K 8.5 mmol/l K 4.8 mmol/l
53 K 6.8 mmol/l K 7.5 mmol/l K 8.5 mmol/l K 4.8 mmol/l
54 K 6.8 mmol/l K 7.5 mmol/l K 8.5 mmol/l K 4.8 mmol/l
55 K 6.8 mmol/l K 7.5 mmol/l K 8.5 mmol/l K 4.8 mmol/l


56 68 y/o malepatient CAD St. p. CABG barely responsive
57 K 6.8 mmol/l K 7.5 mmol/l K 8.5 mmol/l K 4.8 mmol/l
58
59 Patient M.L., female, 38 years AV Block III congenital Very active lifestyle Exercise Intolerance

60

61

62

63

64

65

66

67

68

69

70

71

72 Intrinsic ECG

73
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
PAEDIATRIC ECG Dimosthenis Avramidis, MD.
 PAEDIATRIC ECG Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece S. Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece 5 y/o with sinus tach Background ECG changes
PAEDIATRIC ECG Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece S. Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece 5 y/o with sinus tach Background ECG changes
Office ECG Interpretation
 Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient October 4, 2007
 Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
ECG S: A CASE-BASED APPROACH December 6,
 ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
ECG Interactive Session
 SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient September 25, 2009
 Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Supraventricular Arrhythmias. Reading Assignment. Chapter 5 (p17-30)
") Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
Return to Basics. Normal Intervals & Axes. ECG Rate and Rhythm
 Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Appendix D Output Code and Interpretation of Analysis
 Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
ECGs on the acute admission ward. - Cardiology Update -
 ECGs on the acute admission ward - Cardiology Update - Dr Simon Fynn Consultant Cardiologist Papworth Hospital, Cambridge RCP London Oct 2017 ECG 1 1. AF with BBB 2. Pre-excited AF 3. SVT with BBB 4.
ECGs on the acute admission ward - Cardiology Update - Dr Simon Fynn Consultant Cardiologist Papworth Hospital, Cambridge RCP London Oct 2017 ECG 1 1. AF with BBB 2. Pre-excited AF 3. SVT with BBB 4.
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
You Don t Want to Miss This One! Focus on can t miss EKG tracings
 You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
WPW syndrome and AVRT
 WPW syndrome and AVRT Myung-Yong Lee, MD, PhD Division of Cardiology Department of Internal Medicine School of Medicine Dankook University, Cheonan, Korea Supraventricular tachycardia (SVT) Paroxysmal
WPW syndrome and AVRT Myung-Yong Lee, MD, PhD Division of Cardiology Department of Internal Medicine School of Medicine Dankook University, Cheonan, Korea Supraventricular tachycardia (SVT) Paroxysmal
InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions
 InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions The Clinical Revisions provide details of changes to InterQual Clinical Criteria. They do not provide information on changes made to CareEnhance
InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions The Clinical Revisions provide details of changes to InterQual Clinical Criteria. They do not provide information on changes made to CareEnhance
Blocks & Dissociations. Reading Assignment (p47-52 in Outline )
") Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block:
Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block:
MICS OF MYOCARDIAL ISCHEMIA AND INFARCTION REVISED FOR LAS VEGAS
 ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
FLB s What Are Those Funny-Looking Beats?
 FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD
 Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
APPROACH TO TACHYARRYTHMIAS
 APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)
 PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)") 1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
December 2018 Tracings
 Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Family Medicine for English language students of Medical University of Lodz ECG. Jakub Dorożyński
 Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Acute Coronary Syndromes Unstable Angina Non ST segment Elevation MI (NSTEMI) ST segment Elevation MI (STEMI)
 ST segment Elevation MI (STEMI)") Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Section V. Objectives
 Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Antony French Consultant Cardiologist & Electrophysiologist
 Antony French Consultant Cardiologist & Electrophysiologist Palpitations Unpleasant awareness of rapid or forceful heart beat Not all tachycardias cause palpitations, and not all palpitations are due to
Antony French Consultant Cardiologist & Electrophysiologist Palpitations Unpleasant awareness of rapid or forceful heart beat Not all tachycardias cause palpitations, and not all palpitations are due to
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Electrical System Overview Electrocardiograms Action Potentials 12-Lead Positioning Values To Memorize Calculating Rates
 Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
ECGs: Everything a finalist needs to know. Dr Amy Coulden As part of the Simply Finals series
 ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
Antiarrhythmic Drugs
 Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
ECG Workshop. Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care
 ECG Workshop Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care ECG workshop case study1 44 Year old male. Reports SOB, Lethargy, tiredness. PMH: Hypertension, nil else. What tests? What treatment?
ECG Workshop Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care ECG workshop case study1 44 Year old male. Reports SOB, Lethargy, tiredness. PMH: Hypertension, nil else. What tests? What treatment?
Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG?
 Objectives What s in an ECG?") Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG? The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic
Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG? The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic
a lecture series by SWESEMJR
 Arrhythmias Automaticity- the ability to depolarize spontaneously. Pacemakers: Sinoatrial node: 70 bpm AV-nodal area: 40 bpm His-Purkinje: 20-40 bpm it Mechanisms of arrhythmias 1. Increased automaticity
Arrhythmias Automaticity- the ability to depolarize spontaneously. Pacemakers: Sinoatrial node: 70 bpm AV-nodal area: 40 bpm His-Purkinje: 20-40 bpm it Mechanisms of arrhythmias 1. Increased automaticity
Miscellaneous Stuff Keep reading the Outline
 Miscellaneous Stuff Keep reading the Outline Welcome to the 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic measurements:
Miscellaneous Stuff Keep reading the Outline Welcome to the 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic measurements:
THE ELECTROCARDIOGRAM A UBIQUITOUS AND COST-EFFECTIVE DIAGNOSTIC TOOL FOR THE FAMILY MEDICINE REFRESHER COURSE MARCH 8, 2019
 THE ELECTROCARDIOGRAM A UBIQUITOUS AND COST-EFFECTIVE DIAGNOSTIC TOOL FOR THE FAMILY MEDICINE REFRESHER COURSE MARCH 8, 2019 Major Clinical Disorders Pulmonary Embolism 69 y/o woman with dyspnea and an
THE ELECTROCARDIOGRAM A UBIQUITOUS AND COST-EFFECTIVE DIAGNOSTIC TOOL FOR THE FAMILY MEDICINE REFRESHER COURSE MARCH 8, 2019 Major Clinical Disorders Pulmonary Embolism 69 y/o woman with dyspnea and an
Management of Arrhythmias The General Practitioners role
 Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Solutions for Every Day Problems Cardiologists and the ECG: Are We Really That Good at It? Part II Daniel José Piñeiro Profesor Titular de Medicina,
 Solutions for Every Day Problems Cardiologists and the ECG: Are We Really That Good at It? Part II Daniel José Piñeiro Profesor Titular de Medicina, Universidad de Buenos Aires, Argentina Member, Membership
Solutions for Every Day Problems Cardiologists and the ECG: Are We Really That Good at It? Part II Daniel José Piñeiro Profesor Titular de Medicina, Universidad de Buenos Aires, Argentina Member, Membership
Update on Palpitations and AF February 28 th 2018
 Update on Palpitations and AF February 28 th 2018 Dr Mrinal Andrew Saha MA(Cantab) MBBS FRCP PhD Consultant Interventional Cardiologist GHNHSFT Dr Mrinal Saha Appointed 2010 Special interests: Angioplasty,
Update on Palpitations and AF February 28 th 2018 Dr Mrinal Andrew Saha MA(Cantab) MBBS FRCP PhD Consultant Interventional Cardiologist GHNHSFT Dr Mrinal Saha Appointed 2010 Special interests: Angioplasty,
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
Tachycardias II. Štěpán Havránek
 Tachycardias II Štěpán Havránek Summary 1) Supraventricular (supraventricular rhythms) Atrial fibrillation and flutter Atrial ectopic tachycardia / extrabeats AV nodal reentrant a AV reentrant tachycardia
Tachycardias II Štěpán Havránek Summary 1) Supraventricular (supraventricular rhythms) Atrial fibrillation and flutter Atrial ectopic tachycardia / extrabeats AV nodal reentrant a AV reentrant tachycardia
a lecture series by SWESEMJR
 Electrolyte disturbances Hypokalaemia Decreased extracellular potassium increases excitability in the myocardial cells and consequently the effect of very severe hypokalaemia is ventricular arrhythmia.
Electrolyte disturbances Hypokalaemia Decreased extracellular potassium increases excitability in the myocardial cells and consequently the effect of very severe hypokalaemia is ventricular arrhythmia.
Bryan Heart. Unknown ECGs for the Clinician. Disclaimer 9/2/2015
 Bryan Heart Unknown ECGs for the Clinician 2015 Bryan Heart Fall Cardiology Conference Andrew Merliss, MD, FACC, CDRS, FHRS Director of Cardiac Arrhythmia Service Bryan Heart Disclaimer Advisory Board
Bryan Heart Unknown ECGs for the Clinician 2015 Bryan Heart Fall Cardiology Conference Andrew Merliss, MD, FACC, CDRS, FHRS Director of Cardiac Arrhythmia Service Bryan Heart Disclaimer Advisory Board
Hatim Al Lawati. MD, FRCPC, DABIM(CV), FACC
, FACC") Hatim Al Lawati. MD, FRCPC, DABIM(CV), FACC Consultant Interventional Cardiology & Structural Heart Disease Department of Medicine Sultan Qaboos University Hospital hatim.al.lawati@gmail.com April 2017
Hatim Al Lawati. MD, FRCPC, DABIM(CV), FACC Consultant Interventional Cardiology & Structural Heart Disease Department of Medicine Sultan Qaboos University Hospital hatim.al.lawati@gmail.com April 2017
Paediatric ECG Interpretation
 Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
2017 EKG Workshop Advanced. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천
 The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천 Differentiation Supraventricular Origin from Ventricular Origin on ECG. QRS-Complex Width. 1. Narrow QRS-Complex Tachycardia (
The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천 Differentiation Supraventricular Origin from Ventricular Origin on ECG. QRS-Complex Width. 1. Narrow QRS-Complex Tachycardia (
ARRHYTHMIAS IN THE ICU
 ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
Myocardial Infarction. Reading Assignment (p66-78 in Outline )
") Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
15 16 September Seminar W10O. ECG for General Practice
 15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
Ablation Update and Case Studies. Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group
 Ablation Update and Case Studies Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group Disclosures No financial relationships to disclose Objectives At the conclusion of this activity,
Ablation Update and Case Studies Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group Disclosures No financial relationships to disclose Objectives At the conclusion of this activity,
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Ventricular tachycardia Ventricular fibrillation and ICD
 EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
EKG Practice. Homan Wai
 EKG Practice Homan Wai Objectives Learn EKG by Examples Learn by repetition Learn by repetition Learn by repetition Learn by repetition Learn by repetition Learn by repetition Learn by repetition Details
EKG Practice Homan Wai Objectives Learn EKG by Examples Learn by repetition Learn by repetition Learn by repetition Learn by repetition Learn by repetition Learn by repetition Learn by repetition Details
KNOW YOUR ECG. G. Somasekhar MD DM FEp Consultant Electro physiologist, Aayush Hospital, Vijayawada
 KNOW YOUR ECG G. Somasekhar MD DM FEp Consultant Electro physiologist, Aayush Hospital, Vijayawada CASE DETAILS A 48-year-old female non hypertensive, non diabetic presented with history of shortness of
KNOW YOUR ECG G. Somasekhar MD DM FEp Consultant Electro physiologist, Aayush Hospital, Vijayawada CASE DETAILS A 48-year-old female non hypertensive, non diabetic presented with history of shortness of
Advanced ECG Interpretation Pt. II
 Advanced ECG Interpretation Pt. II Dysrhythmias Amal Mattu, MD, FAAEM Professor and Vice Chair Director, Emergency Cardiology Fellowship Department of Emergency Medicine University of Maryland School of
Advanced ECG Interpretation Pt. II Dysrhythmias Amal Mattu, MD, FAAEM Professor and Vice Chair Director, Emergency Cardiology Fellowship Department of Emergency Medicine University of Maryland School of
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
BSH Heart Failure Nurse and Healthcare Professional Study Day 2017
 BSH Heart Failure Nurse and Healthcare Professional Study Day 2017 Presentation title: Malignant Arrhythmias Speaker: Derek Connelly Conflicts of interest: Speakers fees / advisory boards: Boehringer Ingelheim,
BSH Heart Failure Nurse and Healthcare Professional Study Day 2017 Presentation title: Malignant Arrhythmias Speaker: Derek Connelly Conflicts of interest: Speakers fees / advisory boards: Boehringer Ingelheim,
Case-Based Practical ECG Interpretation for the Generalist
 Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด
 Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
Other 12-Lead ECG Findings
 Other 12-Lead ECG Findings Left Atrial Enlargement Left atrial enlargement is illustrated by increased P wave duration in lead II, top ECG, and by the prominent negative P terminal force in lead V1, bottom
Other 12-Lead ECG Findings Left Atrial Enlargement Left atrial enlargement is illustrated by increased P wave duration in lead II, top ECG, and by the prominent negative P terminal force in lead V1, bottom
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
Paroxysmal Supraventricular Tachycardia PSVT.
 Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
The most common. hospitalized patients. hypotension due to. filling time Rate control in ICU patients may be difficult as many drugs cause hypotension
 Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Masqueraders of STEMI
 Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs
 EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important step for
EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important step for
Tachycardia Devices Indications and Basic Trouble Shooting
 Tachycardia Devices Indications and Basic Trouble Shooting Peter A. Brady, MD., FRCP Cardiology Review Course London, March 6 th, 2014 2011 MFMER 3134946-1 Tachycardia Devices ICD Indications Primary and
Tachycardia Devices Indications and Basic Trouble Shooting Peter A. Brady, MD., FRCP Cardiology Review Course London, March 6 th, 2014 2011 MFMER 3134946-1 Tachycardia Devices ICD Indications Primary and
Treatment of Arrhythmias in the Emergency Setting
 Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Ben Taylor, PhD, PA-C
 Ben Taylor, PhD, PA-C The patient is a 23-year-old white male with a history of polysubstance abuse who was found unresponsive, last seen the day before. Classic signs of systemic hypothermia with prominent
Ben Taylor, PhD, PA-C The patient is a 23-year-old white male with a history of polysubstance abuse who was found unresponsive, last seen the day before. Classic signs of systemic hypothermia with prominent
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
An Approach to the Patient with Syncope. Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva
 An Approach to the Patient with Syncope Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva Case presentation A 23 y.o. man presented with 2 episodes of syncope One during exercise,one at rest
An Approach to the Patient with Syncope Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva Case presentation A 23 y.o. man presented with 2 episodes of syncope One during exercise,one at rest
Arrhythmias (II) Ventricular Arrhythmias. Disclosures
 Ventricular Arrhythmias. Disclosures") Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
Dr. Schroeder has no financial relationships to disclose
 Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
Degrees AV blocks in athletes
 Degrees AV blocks in athletes Name: BCA Age: 22yo Sex: Male Race: Black Weight: 82 kg Height: 1.96m Biotype: Athletic rofession: professional basketball player Date: 2/09/2001 Clinical diagnosis: athlete
Degrees AV blocks in athletes Name: BCA Age: 22yo Sex: Male Race: Black Weight: 82 kg Height: 1.96m Biotype: Athletic rofession: professional basketball player Date: 2/09/2001 Clinical diagnosis: athlete
INTERESTING ECGS. Wide-complex tachycardias 11/13/ yr male with acute ant wall MI, S/P primary PTCA
 INTERESTING ECGS V S Prakash Prof, & Head Dept. of Cardiology M S Ramaiah Hospitals 50 yr male with acute ant wall MI, S/P primary PTCA Pt. underwent successful PAMI An hour later,in the CCU Ventricular
INTERESTING ECGS V S Prakash Prof, & Head Dept. of Cardiology M S Ramaiah Hospitals 50 yr male with acute ant wall MI, S/P primary PTCA Pt. underwent successful PAMI An hour later,in the CCU Ventricular
EPS Case presentation Looks like VT but it isn t!
 EPS Case presentation Looks like VT but it isn t! E. Συμεωνίδου, MD, PhD Β Παν Καρδιολογική κλινική, Νοσ Aττικόν Σεμινάρια Ομάδων Εργασίας ΕΚΕ 2016 Ιωάννινα Disclosures I have no conflict of interest to
EPS Case presentation Looks like VT but it isn t! E. Συμεωνίδου, MD, PhD Β Παν Καρδιολογική κλινική, Νοσ Aττικόν Σεμινάρια Ομάδων Εργασίας ΕΚΕ 2016 Ιωάννινα Disclosures I have no conflict of interest to
ECG in modern medicine: Yesterday or Forever young?
 ECG in modern medicine: Yesterday or Forever young? Valentin A. Kokorin, MD PhD, HFEFIM, Assoc. prof. Hospital therapy 1 department Pirogov Russian National Research Medical University Moscow, Russia 25th
ECG in modern medicine: Yesterday or Forever young? Valentin A. Kokorin, MD PhD, HFEFIM, Assoc. prof. Hospital therapy 1 department Pirogov Russian National Research Medical University Moscow, Russia 25th
Dr.Binoy Skaria 13/07/15
 Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
How To Think About Rhythms and Conduction
 How To Think About Rhythms and Conduction Frank Yanowitz, MD Professor of Medicine (Cardiology) University of Utah School of Medicine Medical Director, IHC ECG Services Intermountain Healthcare http://ecg.utah.edu
How To Think About Rhythms and Conduction Frank Yanowitz, MD Professor of Medicine (Cardiology) University of Utah School of Medicine Medical Director, IHC ECG Services Intermountain Healthcare http://ecg.utah.edu
Section 3 and 4. Objectives. Bundle Branches 10/9/2018. LBBB, RBBB Bifascicular, Trifascicular Block
 Section 3 and 4 LBBB, RBBB Bifascicular, Trifascicular Block Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation
Section 3 and 4 LBBB, RBBB Bifascicular, Trifascicular Block Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation
Arrhythmias on the AMU
 Arrhythmias on the AMU Dr Andrew R. Houghton United Lincolnshire Hospitals NHS Trust @arh_cardio An arrhythmia is present in 10% of admissions to the AMU Case history AMU referral to cardiology 25 yr 2-3
Arrhythmias on the AMU Dr Andrew R. Houghton United Lincolnshire Hospitals NHS Trust @arh_cardio An arrhythmia is present in 10% of admissions to the AMU Case history AMU referral to cardiology 25 yr 2-3
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
Tachycardia-induced heart failure - Does it exist?
 Tachycardia-induced heart failure - Does it exist? PD Dr Etienne Delacrétaz Clinique Cecil et Hôpital de Fribourg SSC Cardiology meeting 2015 Zürich Rapid atrial fibrillation is a common cause of heart
Tachycardia-induced heart failure - Does it exist? PD Dr Etienne Delacrétaz Clinique Cecil et Hôpital de Fribourg SSC Cardiology meeting 2015 Zürich Rapid atrial fibrillation is a common cause of heart
2/7/ LEAD ECG CASE STUDIES Lisa Riggs MSN, RN, ACNS-BC, CCRN-K CASE #1 WHAT ELSE WOULD YOU ASSESS? WHAT S YOUR DIAGNOSIS?
 12 LEAD ECG CASE STUDIES Lisa Riggs MSN, RN, ACNS-BC, CCRN-K CASE #1 31 y/o male is a direct admit from the physician s office with c/o chest pain and SOA WHAT ELSE WOULD YOU ASSESS? WHAT S YOUR DIAGNOSIS?
12 LEAD ECG CASE STUDIES Lisa Riggs MSN, RN, ACNS-BC, CCRN-K CASE #1 31 y/o male is a direct admit from the physician s office with c/o chest pain and SOA WHAT ELSE WOULD YOU ASSESS? WHAT S YOUR DIAGNOSIS?
ECG Interpretation. Introduction to Cardiac Telemetry. Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services
 ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
Conduction disorders
 Conduction disorders L.V. Bogun, N.I. Yabluchansky, F.M. Abdueva, O.Y. Bichkova, A.N. Fomich, P.A. Garkavyi, A.L. Kulik, N.V. Lysenko, N.V. Makienko, L.A. Martimyanova, I.V. Soldatenko, E.E. Tomina Department
Conduction disorders L.V. Bogun, N.I. Yabluchansky, F.M. Abdueva, O.Y. Bichkova, A.N. Fomich, P.A. Garkavyi, A.L. Kulik, N.V. Lysenko, N.V. Makienko, L.A. Martimyanova, I.V. Soldatenko, E.E. Tomina Department
ECG Workshop. Jared W Magnani, MD, MSc University of Pittsburgh UPMC Heart and Vascular Institute Pittsburgh, PA March 24, 2017
 ECG Workshop Jared W Magnani, MD, MSc University of Pittsburgh UPMC Heart and Vascular Institute Pittsburgh, PA March 24, 2017 Overview and Objectives Review a differential for supraventricular tachycardia
ECG Workshop Jared W Magnani, MD, MSc University of Pittsburgh UPMC Heart and Vascular Institute Pittsburgh, PA March 24, 2017 Overview and Objectives Review a differential for supraventricular tachycardia