RESUSCITATION IN TRAUMA. Important things I have learnt
|
|
|
- Lizbeth Marsh
- 6 years ago
- Views:
Transcription


1 RESUSCITATION IN TRAUMA Important things I have learnt
2

3 Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now
4 1977

5 Fluids Summary Dogs subjected to arterial hemorrhage and infused with 3:l volumes of lactated Ringer s solution became progressively hypovolemic, to the point of frank shock. Stability and normovolemia were restored only after additional fluid delivery, in a net ratio of 8:l. These were the mathematically predicted values that satisfied Starling s hypothesis American Journal of Surgery 1979:129;

6 Fluids More is better Resuscitate to the point of pulmonary oedema then use PPV Adhere to the 3:1 rule (or more)

7 MAST The "G-suit," a device for combating hypovolemic shock with external pneumatic counterpressure, represents an application of an old idea to a relatively common medical problem. Its simplicity of use and quick therapeutic effect buys time for the patient with hypovolemic shock, whether the suit is applied in the prehospital or emergency department setting.

8 MAST First line treatment for haemorrhagic shock Enhanced venous pressure and allowed easier line placement Useful for stabilisation of pelvic fractures

9 Emergency Department Thoracotomy Urgent thoracotomy in the emergency center environment is an adjunct to resuscitation and allows control of reversible intrathoracic injuries. Journal of the American College of Emergency Physicians 1974:1;13-14

10 Goals of ED Thoracotomy Stopping bleeding Release of tamponade Cardiac massage Cross clamp aorta Preventing air embolism

11 Emergency Department Thoracotomy Worth a try in most circumstances Occasional survivors Justified for resident training even when survival improbable

12 DPL The American Journal of Surgery 1978:136;

13 DPL Virtually mandatory in unassessable patients with blunt abdominal trauma Eyeball test used more often than formal evaluation Low false negative rate but high rate of non-therapeutic laparotomy
14 1987
15 MAST

16 MAST We discovered when you put on MAST, you increase the chance the patient would die, you increase their length of stay in the hospital, you increase their cost of hospitalization, increase their complications and it didn t save their life at all,
17 Crystalloids vs colloids
18 Crystalloids vs colloids The resuscitation times were almost always shorter with a regimen of about one-fourth colloids than with crystalloids only. This is consistent with the observations of greater increases in hemodynamic and oxygen transport variables after albumin than after lactated Ringer's solution when the latter was given in either 2 or 4 times the volume.
19 Crystalloids vs colloids In this study meta-analysis was used to pool mortality data from reports of eight previously published, randomized, clinical trials, in which the efficacy of crystalloid and colloid fluid resuscitation was compared. The overall treatment effect when the data from all the clinical trails were pooled showed a 5.7% relative difference in mortality rate in favor of crystalloid therapy

20 Crystalloids vs colloids When the data from only those studies using trauma patients were pooled, the overall treatment effect showed a 12.3% difference in mortality rate in favor of crystalloid therapy.
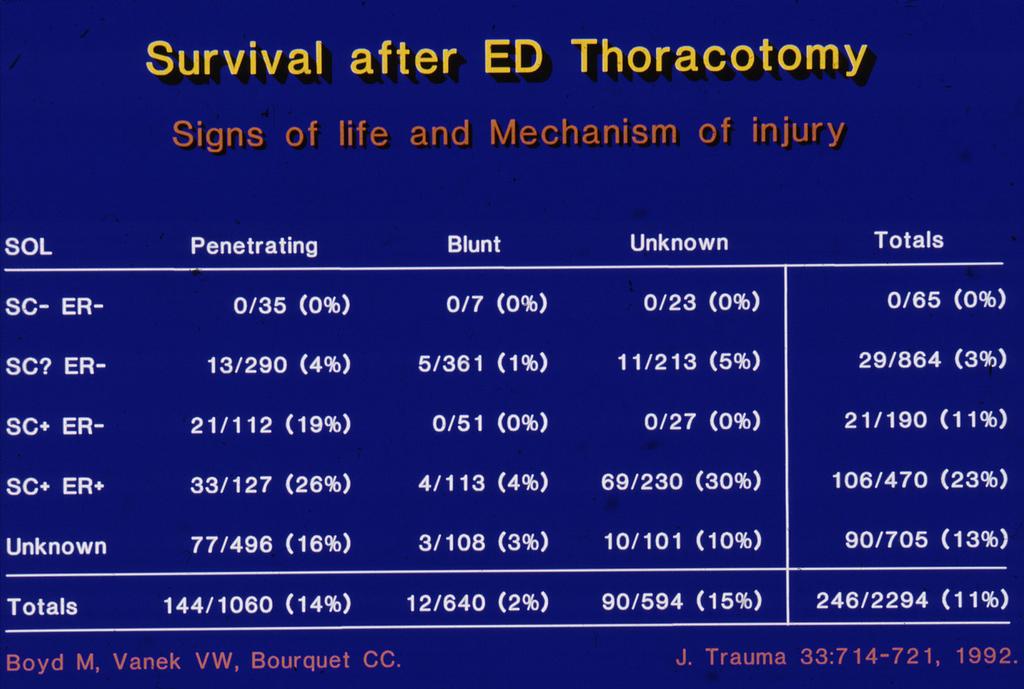
21 ED Thoracotomy

22 ED Thoracotomy Of very limited utility in blunt trauma Unless signs of life are present at least shortly before admission to ED unlikely to be successful even in penetrating trauma In the post-hiv period significant risks to staff recognised Cost of procedure recognised as an important issue where true success uncommon


23 Damage control

24 Damage control
25 Damage Control PART I OR control of hemorrhage control of contamination abbreviation/packing temporary closure PART III OR definitive reconstruction PART II ICU restoration of physiology Rotondo et al, Journal of Trauma 1993
26 The US surgeons response a technique that is the procedure of choice with the threat of exsanguination from a coagulopathy Pachter 1992 it requires more sound cognitive judgement to terminate an operation Mattox 1993 it s judgement, not genital insufficiency that leads one to pack a patient Richardson 1993
27 Fluids out (a bit)
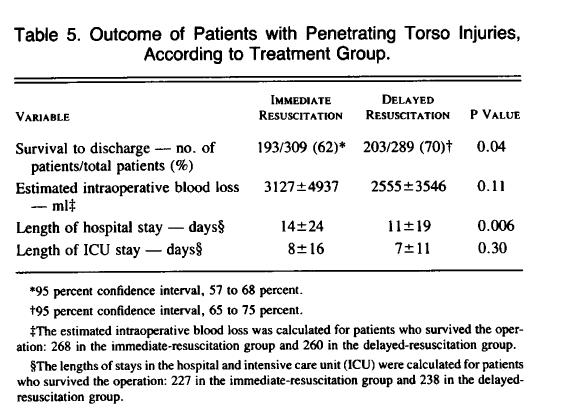
28 Fluid resuscitation

29

30 DPL

31 DPL

32 2007

33 Fluids out more
34

35 Fluids out more

36 Damage control resuscitation

37 Records of 467 MT patients transferred to Level 1 Trauma Centers in Records were analysed for products used in resuscitation ISS and outcome correlated


38 Damage control surgery

39 DPL out During a 30-month period ending July 1997, 2,576 patients had abdominal US in the evaluation of BAT and were entered into our trauma US database. This database was analyzed to determine the utility of US in the evaluation of BAT. J Trauma. 2001;50:
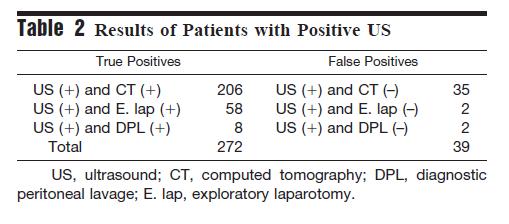
40 DPL out
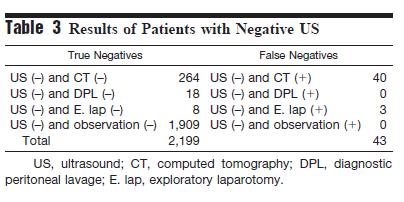
41 DPL out
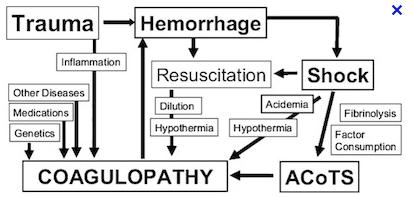
42 Traumatic coagulopathy
43 Monitoring of coagulopathy Traditional tests (INR, fibrinogen) too slow and unproven Thromboelastography Improved outcome in CABG, Liver Tx, Trauma Gold standard is the presence of non surgical bleeding
44
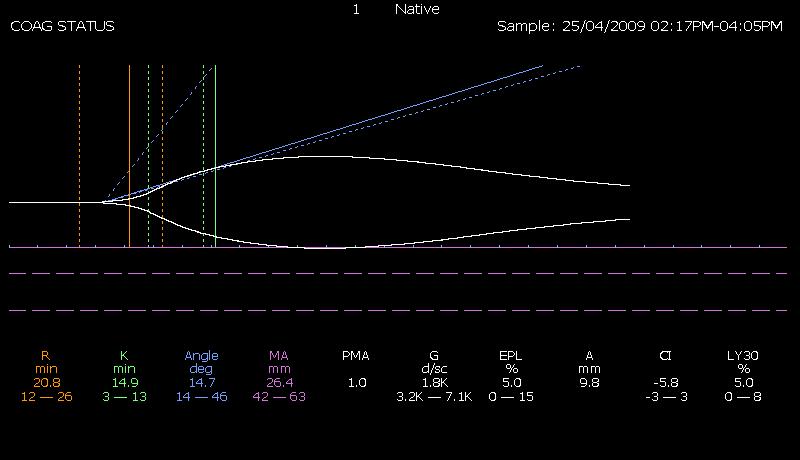
45 TEG
46

47 The place of TEG? Johannon Vox Sanguinis

48 What about Massive Transfusion Protocols?



49 Timing is everything
50 Stanford before and after MTP introduction study Always had a good ratio of plasma to RBCs 40 activated of MTP in each arm (8 months) J Am Coll Surg 2009;209:


51 J Am Coll Surg 2009;209: Level 1 Trauma Center In 2004 changed to a MTP with 1:1.5 ratio FFP:PRBC 40 patients before and 37 after change Transfusion ratios 1:1.8 same before and after
52

53
54 OBJECTIVE To relate inhospital mortality to early transfusion of plasma and/or platelets and to time-varying plasma:red blood cell (RBC) and platelet:rbc ratios. DESIGN Prospective cohort study documenting the timing of transfusions during active resuscitation and patient outcomes SETTING Ten US level I trauma centers. PATIENTS Adult trauma patients surviving for 30 minutes after admission who received a transfusion of at least 1 unit of RBCs within 6 hours of admission (n = 1245, the original study group) and at least 3 total units (of RBCs, plasma, or platelets) within 24 hours (n = 905, the analysis group). MAIN OUTCOME MEASURE In-hospital mortality
55 RESULTS Plasma:RBC and platelet:rbc ratios were not constant during the first 24 hours Increased ratios of plasma:rbcs (adjusted hazard ratio = 0.31; 95% CI, ) and platelets:rbcs (adjusted hazard ratio = 0.55; 95% CI, ) were independently associated with decreased 6-hour mortality, when hemorrhagic death predominated. In the first 6 hours, patients with ratios less than 1:2 were 3 to 4 times more likely to die than patients with ratios of 1:1 or higher. After 24 hours, plasma and platelet ratios were unassociated with mortality, when competing risks from nonhemorrhagic causes prevailed
56 CONCLUSIONS Higher plasma and platelet ratios early in resuscitation were associated with decreased mortality in patients who received transfusions of at least 3 units of blood products during the first 24 hours after admission.

57 Tranexamic Acid


58

59 What s confusing? What is this group of patients and is 16% mortality OK? Who should we give it to here? Where is its place with an MTP?
60

61 What about interventional radiology (IR) in trauma resuscitation? Bleeding anywhere! Pelvic fractures Abdominal solid organ injury Specific vascular injury Aortic/arch vessel rupture Peripheral vascular trauma

62 IR for stopping bleeding and treating injuries

63

64 IR for stopping bleeding and treating injuries Head and neck Chest Abdomen Pelvis Extremities
65 Abdominal solid organ injury AE has a well established role in abdominal trauma Haemodynamically unstable patients with a positive FAST or relevant clinical signs should still undergo urgent laparotomy However, more stable patients can be imaged with MD-CT Patients with solid organ injuries may have CT features that indicate a high risk of re-bleeding. AE should be considered in these cases: High grade injury Contrast extravasation Pseudoaneurysm Arteriovenous fistula
66 Timing Retrospective TNDB study involving 635 patients In unstable trauma patients undergoing therapeutic IR, delay beyond 60 minutes was associated with a twofold increase in mortality. For each additional hour, risk of mortality increased 47%
67 Timing
68 Timing

69 Therapeutic angioembolisation Efficacy rate %
70 Embolisation for pelvic fractures Angiography and TAE represent effective acute interventions for arterial haemorrhage control Drawbacks are delays, time consuming and requirement for specialised personnel and appropriate equipment. Robust evidence of a comparative analysis between TAE and emergency pelvic stabilisation and pelvic tamponade are currently lacking

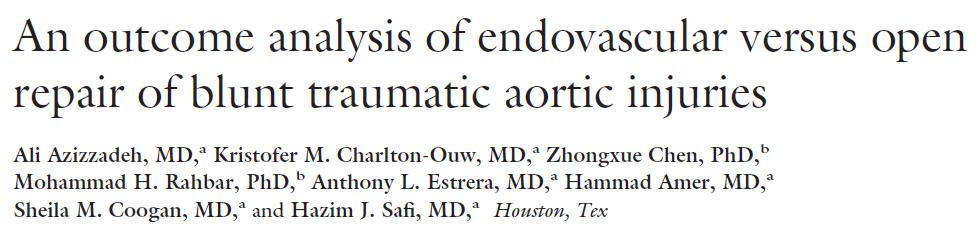
71 Aortic rupture High prehospital mortality Associated with severe multiple injuries Traditional surgery associated with risks of bleeding, paraplegia, stroke, pulmonary insufficiency, renal failure etc

72 A paradigm shift Move to stent graft repair throughout 2000s, becoming almost universal after 2005
73


74 The changing approach to blunt aortic injury at ACH

75 What do you need to make this work? Good collaboration Between IR and trauma team Between IR and vasc surg Between vasc surg and trauma
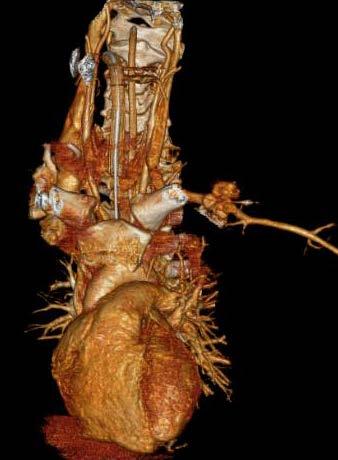
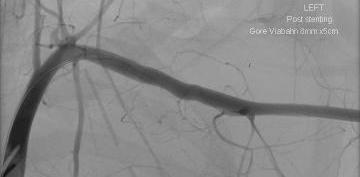
76 IR for other arterial injuries Traumatic injuries of the subclavian or axillary artery are associated with high morbidity and mortality rates. The management of these injuries has traditionally required morbid operative surgical intervention, with surgical exposures that can prove challenging.

77

78
79

80 Resuscitation in trauma important things I have learnt Knowledge is a relative thing Always study what you are doing Never assume what you are doing now is the best way to treat patients Timing is critical

81

82
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Hemostatic Resuscitation in Trauma. Joanna Davidson, MD 6/6/2012
 Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA)
") The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA) Disclosure Speaker name: Ren Wei, Li Zhui, Li Fenghe, Zhao Yu Department of Vascular Surgery, The First Affiliated Hospital of
The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA) Disclosure Speaker name: Ren Wei, Li Zhui, Li Fenghe, Zhao Yu Department of Vascular Surgery, The First Affiliated Hospital of
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD
 ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors. THOR Collaboration
 Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Initial Management of Pelvic Injuries
 Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
Guidelines and Protocols
 TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Unrestricted. Dr ppooransari fellowship of perenatalogy
 Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
TEVAR FOR! THORACIC AORTIC TRAUMA"
 10th HKL Vascular Surgery Conference and Workshop" TEVAR FOR! THORACIC AORTIC TRAUMA" Dr Hanif Hussein" Vascular and General Surgeon" Department of Surgery" Hospital Kuala Lumpur" Source: MIROS! Thoracic
10th HKL Vascular Surgery Conference and Workshop" TEVAR FOR! THORACIC AORTIC TRAUMA" Dr Hanif Hussein" Vascular and General Surgeon" Department of Surgery" Hospital Kuala Lumpur" Source: MIROS! Thoracic
Transfusion 2004: Current Practice Standards. Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service
 SBB SWMC Transfusion Service") Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
May Clinical Director, Peninsula Trauma Network (Edited for PTN)
") Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a
Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Kay Barrera MD. Surgery Grand Rounds June 19, 2014 SUNY Downstate
 Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Outline Why are we talking about this SCORE expectations When do we use
Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Outline Why are we talking about this SCORE expectations When do we use
Advances in Treatment of Traumatic Aortic Transection
 Advances in Treatment of Traumatic Aortic Transection Himanshu J. Patel MD University of Michigan Medical Center Author Disclosures Consulting fees from WL Gore Inc. There is no disease more conducive
Advances in Treatment of Traumatic Aortic Transection Himanshu J. Patel MD University of Michigan Medical Center Author Disclosures Consulting fees from WL Gore Inc. There is no disease more conducive
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out?
 and Tranexamic acid (TXA): Is the Jury Still Out?") Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
ICU treatment of the trauma patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
Management of the Open Abdomen
 Management of the Open Abdomen Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Associate Professor of Surgery Denver Health Medical Center / University of Colorado The Open Abdomen
Management of the Open Abdomen Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Associate Professor of Surgery Denver Health Medical Center / University of Colorado The Open Abdomen
5/30/2013. I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow. Trauma = #1 cause of death persons <40 yo 1
 I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow Trauma = #1 cause of death persons
I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow Trauma = #1 cause of death persons
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
TRAUMA RESUSCITATION. Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital
 TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
3/16/15. Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation. Obligatory Traumatologist Slide
 Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury
 TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury Megan Brenner MD MS RPVI FACS Associate Professor of Surgery Division of Trauma/Surgical Critical Care, RA Cowley
TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury Megan Brenner MD MS RPVI FACS Associate Professor of Surgery Division of Trauma/Surgical Critical Care, RA Cowley
Massive Transfusion in Pediatric Trauma: Analysis of the National Trauma Databank
 Massive Transfusion in Pediatric Trauma: Analysis of the National Trauma Databank Michelle Shroyer, MPH, Russell Griffin, PhD, Vincent Mortellaro, MD, and Rob Russell MD, MPH Introduction Hemorrhage is
Massive Transfusion in Pediatric Trauma: Analysis of the National Trauma Databank Michelle Shroyer, MPH, Russell Griffin, PhD, Vincent Mortellaro, MD, and Rob Russell MD, MPH Introduction Hemorrhage is
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
REBOA new snake in the grass?
 REBOA new snake in the grass? Does it have a place in South Africa and other LMICs? Tim Hardcastle Trauma Surgeon IALCH/UKZN Controversies in Surgery 2016 History nothing new under the sun (Solomon = Ecclesiates)
REBOA new snake in the grass? Does it have a place in South Africa and other LMICs? Tim Hardcastle Trauma Surgeon IALCH/UKZN Controversies in Surgery 2016 History nothing new under the sun (Solomon = Ecclesiates)
Open Repair of RAAA is always possible -is it always better? No disclosures!! Lazar B. Davidovic MD, PhD, FETCS
 Open Repair of RAAA is always possible -is it always better? Lazar B. Davidovic MD, PhD, FETCS Professor of Surgery School of Medicine, University of Belgrade Head of the Clinic for Vascular and Endovascular
Open Repair of RAAA is always possible -is it always better? Lazar B. Davidovic MD, PhD, FETCS Professor of Surgery School of Medicine, University of Belgrade Head of the Clinic for Vascular and Endovascular
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
Surgical Resuscitation Management in Poly-Trauma Patients
 Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University
 PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
Thoracic aortic trauma A.T.O.ABDOOL-CARRIM ACADEMIC HEAD VASCULAR SURGERY DEPARTMENT OF SURGERY UNIVERSITY OF WITWATERSRAND
 Thoracic aortic trauma A.T.O.ABDOOL-CARRIM ACADEMIC HEAD VASCULAR SURGERY DEPARTMENT OF SURGERY UNIVERSITY OF WITWATERSRAND Thoracic Aortic Trauma In USA and CANADA 7500-8000 die of blunt thoracic aortic
Thoracic aortic trauma A.T.O.ABDOOL-CARRIM ACADEMIC HEAD VASCULAR SURGERY DEPARTMENT OF SURGERY UNIVERSITY OF WITWATERSRAND Thoracic Aortic Trauma In USA and CANADA 7500-8000 die of blunt thoracic aortic
Thicker than Water. Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago
 Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
6. Endovascular aneurysm repair
 Introduction The standard treatment for aortic aneurysm, open repair, involves a large abdominal incision and cross-clamping of the aorta. In recent years, a minimally invasive technique, endovascular
Introduction The standard treatment for aortic aneurysm, open repair, involves a large abdominal incision and cross-clamping of the aorta. In recent years, a minimally invasive technique, endovascular
Massive transfusion: Recent advances, guidelines & strategies. Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad
 Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY
 MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application
 Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application Authors Alan A Garner Retrieval consultant CareFlight Northmead,
Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application Authors Alan A Garner Retrieval consultant CareFlight Northmead,
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
10/4/2018. Nothing to Disclose. Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO
 Nothing to Disclose Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO History of IV Resuscitation Review of Data for Fluid Strategies Historical Examples of IV
Nothing to Disclose Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO History of IV Resuscitation Review of Data for Fluid Strategies Historical Examples of IV
How to select ruptured AAA for EVAR or open repair?
 How to select ruptured AAA for EVAR or open repair? Dr. Skyi Pang Associate Consultant Division of Vascular Surgery Department of Surgery Pamela Youde Nethersole Eastern Hospital Hong Kong SAR, China Disclosure
How to select ruptured AAA for EVAR or open repair? Dr. Skyi Pang Associate Consultant Division of Vascular Surgery Department of Surgery Pamela Youde Nethersole Eastern Hospital Hong Kong SAR, China Disclosure
M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH
 Unrestricted M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH Patients at imminent risk of exsanguination Manual aortic compression Resuscitative endovascular balloon occlusion of the aorta Uterine tourniquet
Unrestricted M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH Patients at imminent risk of exsanguination Manual aortic compression Resuscitative endovascular balloon occlusion of the aorta Uterine tourniquet
Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference
 Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference John A. Aucar, MD, MSHI, FACS, CPE EmCare Acute Care Surgery Del Sol Medical Center Associate Professor, University
Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference John A. Aucar, MD, MSHI, FACS, CPE EmCare Acute Care Surgery Del Sol Medical Center Associate Professor, University
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Adult Trauma Advances in Pediatrics. (sometimes they are little adults) FAST examination. Who is bleeding? How much and what kind of TXA volume?
 FAST examination. Who is bleeding? How much and what kind of TXA volume?") Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Groupe d Intérêt en Hémostase Périopératoire
 How do I treat massive bleeding? Red blood cell / plasma / platelet ratio and massive transfusion protocols Anne GODIER Service d Anesthésie-Réanimation Hopital Cochin Paris Groupe d Intérêt en Hémostase
How do I treat massive bleeding? Red blood cell / plasma / platelet ratio and massive transfusion protocols Anne GODIER Service d Anesthésie-Réanimation Hopital Cochin Paris Groupe d Intérêt en Hémostase
Tasopoulou KM 1, Argyriou C 1, Mantatzis M 2, Kantartzi K 3, Passadakis P 3, Georgiadis GS 1
 Tasopoulou KM 1, Argyriou C 1, Mantatzis M 2, Kantartzi K 3, Passadakis P 3, Georgiadis GS 1 1 Department of Vascular Surgery, 2 Department of Radiology/Interventional Radiology Unit and 3 Department of
Tasopoulou KM 1, Argyriou C 1, Mantatzis M 2, Kantartzi K 3, Passadakis P 3, Georgiadis GS 1 1 Department of Vascular Surgery, 2 Department of Radiology/Interventional Radiology Unit and 3 Department of
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
Abdominal Aortic Aneurysms. A Surgeons Perspective Dr. Derek D. Muehrcke
 Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Pediatric emergencies. Emergent Neuroimaging Acute chest (non-trauma) Acute abdomen (non-trauma) Sports injuries (trauma) Highlights/Trends Polytrauma
 Acute abdomen (non-trauma) Sports injuries (trauma) Highlights/Trends Polytrauma") Department of Clinical Radiology, Munich University Hospital Pediatric emergencies Emergent Neuroimaging Acute chest (non-trauma) Acute abdomen (non-trauma) Sports injuries (trauma) Highlights/Trends Polytrauma
Department of Clinical Radiology, Munich University Hospital Pediatric emergencies Emergent Neuroimaging Acute chest (non-trauma) Acute abdomen (non-trauma) Sports injuries (trauma) Highlights/Trends Polytrauma
Chapter 3 MAKING THE DECISION TO TRANSFUSE
 Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
University of Florida Department of Surgery. CardioThoracic Surgery VA Learning Objectives
 University of Florida Department of Surgery CardioThoracic Surgery VA Learning Objectives This service performs coronary revascularization, valve replacement and lung cancer resections. There are 2 faculty
University of Florida Department of Surgery CardioThoracic Surgery VA Learning Objectives This service performs coronary revascularization, valve replacement and lung cancer resections. There are 2 faculty
Hydroxyethyl starch and bleeding
 Hydroxyethyl starch and bleeding Anders Perner Dept. of Intensive Care, Rigshospitalet University of Copenhagen Scandinavian Critical Care Trials Group Intensive Care Medicine COIs Ferring, LFB - Honoraria
Hydroxyethyl starch and bleeding Anders Perner Dept. of Intensive Care, Rigshospitalet University of Copenhagen Scandinavian Critical Care Trials Group Intensive Care Medicine COIs Ferring, LFB - Honoraria
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway
 MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Pelvic Fractures. AOCP National Course Belfast City Hospital. 11 th June D Swain BSc; FRCSI; FRCS (Orth.)
") Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
2012, Görlinger Klaus
 Gerinnungsmanagement der Gegenwart - wie gehen wir heute vor? 25. Allander Gerinnungsrunde am 15. März 2012 Klaus Görlinger Universitätsklinikum Essen klaus@goerlinger.net CSL Behring GmbH Octapharma AG
Gerinnungsmanagement der Gegenwart - wie gehen wir heute vor? 25. Allander Gerinnungsrunde am 15. März 2012 Klaus Görlinger Universitätsklinikum Essen klaus@goerlinger.net CSL Behring GmbH Octapharma AG
Abdominal Aortic Aneurysm - Part 1. Learning Objectives. Disclosure. University of Toronto Division of Vascular Surgery
 University of Toronto Division of Vascular Surgery Abdominal Aortic Aneurysm - Part 1 Dr Mark Wheatcroft & Dr Elisa Greco Vascular Surgeon, St Michael s Hospital, Toronto & University of Toronto Disclosure
University of Toronto Division of Vascular Surgery Abdominal Aortic Aneurysm - Part 1 Dr Mark Wheatcroft & Dr Elisa Greco Vascular Surgeon, St Michael s Hospital, Toronto & University of Toronto Disclosure
SHOCK and the Trauma Victim. JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital.
 SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
ED Thoracotomy Left chest opened and extended across sternum with 1000mL blood drained Pericardium opened with 100mL blood drained 1cm laceration in t
 Case Report 39yM stabbed in the left upper chest by wife with kitchen knife. Intubated in the field. Loss of vitals on arrival to hospital while in ambulance. In ED, (-) palpable pulse and (+) organized
Case Report 39yM stabbed in the left upper chest by wife with kitchen knife. Intubated in the field. Loss of vitals on arrival to hospital while in ambulance. In ED, (-) palpable pulse and (+) organized
THE INITIAL MANAGEMENT OF PELVIC AND ACETABULAR TRAUMA LOUIS LEBLOND MD FRCSC DEPT OF ORTHOPAEDICS THE MONCTON HOSPITAL - L HÔPITAL DE MONCTON
 THE INITIAL MANAGEMENT OF PELVIC AND ACETABULAR TRAUMA LOUIS LEBLOND MD FRCSC DEPT OF ORTHOPAEDICS THE MONCTON HOSPITAL - L HÔPITAL DE MONCTON DISCLOSURES + BACKGROUND No. Centre de formation médicale
THE INITIAL MANAGEMENT OF PELVIC AND ACETABULAR TRAUMA LOUIS LEBLOND MD FRCSC DEPT OF ORTHOPAEDICS THE MONCTON HOSPITAL - L HÔPITAL DE MONCTON DISCLOSURES + BACKGROUND No. Centre de formation médicale
Priorities in Penetrating Chest Trauma
 Priorities in Penetrating Chest Trauma K. Inaba, MD FRCSC FACS Division of Trauma Surgery & Critical Care LAC+USC Medical Center University of Southern California ü None. DISCLOSURES OBJECTIVES ü Practical
Priorities in Penetrating Chest Trauma K. Inaba, MD FRCSC FACS Division of Trauma Surgery & Critical Care LAC+USC Medical Center University of Southern California ü None. DISCLOSURES OBJECTIVES ü Practical
account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die
 account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die within the first month if aorta not repaired 30-90% overall
account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die within the first month if aorta not repaired 30-90% overall
Clinical Module. Pelvic Injury Trauma. Princess Alexandra Hospital Emergency Department. 1 Introduction
 Princess Alexandra Hospital Emergency Department Clinical Module Trauma Review Officers: Katherine Isoardi / Glenn Ryan Version no: 2 Review date: Aug 2015 Key Words: Pelvic Trauma, Pelvic Injury, Pelvic
Princess Alexandra Hospital Emergency Department Clinical Module Trauma Review Officers: Katherine Isoardi / Glenn Ryan Version no: 2 Review date: Aug 2015 Key Words: Pelvic Trauma, Pelvic Injury, Pelvic
Role of the Radiologist
 Diagnosis and Treatment of Blunt Cerebrovascular Injuries NORDTER Consensus Conference October 22-24, 2007 Clint W. Sliker, M.D. University of Maryland Medical Center R Adams Cowley Shock Trauma Center
Diagnosis and Treatment of Blunt Cerebrovascular Injuries NORDTER Consensus Conference October 22-24, 2007 Clint W. Sliker, M.D. University of Maryland Medical Center R Adams Cowley Shock Trauma Center
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury. Conflict of Interest. Hypotensive shock 5/5/2014. none
 EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
Complications of ECLS. Rajasekhar Malyala, MD Assistant Professor, Surgery University of Kentucky
 Complications of ECLS Rajasekhar Malyala, MD Assistant Professor, Surgery University of Kentucky Faculty Disclosure No financial Disclosures Education Need/Practice Gap Recommendations and guidelines regarding
Complications of ECLS Rajasekhar Malyala, MD Assistant Professor, Surgery University of Kentucky Faculty Disclosure No financial Disclosures Education Need/Practice Gap Recommendations and guidelines regarding
Disclosure. I do not have any potential conflict of interest
 Endovascular repair of ruptured abdominal aortic aneurysms is superior to open repair in risk stratified patients: a look at the United States experience through the SVS Vascular Quality Initiative 2003
Endovascular repair of ruptured abdominal aortic aneurysms is superior to open repair in risk stratified patients: a look at the United States experience through the SVS Vascular Quality Initiative 2003
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
Traumatic Posterior Tibial Pseudoaneursym: A rare late complication repaired conventionally
 Volume 2 Issue 3 Article 3 2016 Traumatic Posterior Tibial Pseudoaneursym: A rare late complication repaired conventionally Farzad Amiri, MD; Zachary Sanford; and Constantinous Constantinou, MD Follow
Volume 2 Issue 3 Article 3 2016 Traumatic Posterior Tibial Pseudoaneursym: A rare late complication repaired conventionally Farzad Amiri, MD; Zachary Sanford; and Constantinous Constantinou, MD Follow
Hemorrhage Control. Chapter 6
 Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Hemostatic Resuscitation
 Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley
 Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley British Journal of Surgery 2013; 100: 1045 1049 The risk of 30 day mortality
Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley British Journal of Surgery 2013; 100: 1045 1049 The risk of 30 day mortality
Gunshot Wounds to the Abdomen: From Bullet to Incision. Patrick M Reilly MD FACS
 Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
The principle of 1:1:1 blood product use in the resuscitation of trauma victims. K. D. Boffard
 The principle of 1:1:1 blood product use in the resuscitation of trauma victims K. D. Boffard Milpark Hospital Department of Surgery University of the Witwatersrand Johannesburg, South Africa Annual Controversies
The principle of 1:1:1 blood product use in the resuscitation of trauma victims K. D. Boffard Milpark Hospital Department of Surgery University of the Witwatersrand Johannesburg, South Africa Annual Controversies
Clinical Overview of Coagulation Testing Issues
 Clinical Overview of Coagulation Testing Issues Adam M. Vogel, MD Assistant Professor, Division of Pediatric Surgery Washington University in St. Louis School of Medicine September 19, 2014 Disclosure
Clinical Overview of Coagulation Testing Issues Adam M. Vogel, MD Assistant Professor, Division of Pediatric Surgery Washington University in St. Louis School of Medicine September 19, 2014 Disclosure
Experience of endovascular procedures on abdominal and thoracic aorta in CA region
 Experience of endovascular procedures on abdominal and thoracic aorta in CA region May 14-15, 2015, Dubai Dr. Viktor Zemlyanskiy National Research Center of Emergency Care Astana, Kazakhstan Region Characteristics
Experience of endovascular procedures on abdominal and thoracic aorta in CA region May 14-15, 2015, Dubai Dr. Viktor Zemlyanskiy National Research Center of Emergency Care Astana, Kazakhstan Region Characteristics
Bundeswehrkrankenhaus Ulm Abteilung HNO Kopf-Halschirurgie
 Kai Johannes Lorenz and Klaus Effinger Department of Otorhinolaryngology, Head and Neck Surgery Department of Radiology and interventional Radiology German Armed Forces Hospital Incidence of hemorrhage
Kai Johannes Lorenz and Klaus Effinger Department of Otorhinolaryngology, Head and Neck Surgery Department of Radiology and interventional Radiology German Armed Forces Hospital Incidence of hemorrhage
Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy
 ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
journal ORIGINAL RESEARCH
 texas orthopaedic journal ORIGINAL RESEARCH Mortality with Circumferential Pelvic Compression for Pelvic Ring Disruption in Polytraumatized Patients: A Retrospective Analysis of 1,639 Pelvic Ring Injuries
texas orthopaedic journal ORIGINAL RESEARCH Mortality with Circumferential Pelvic Compression for Pelvic Ring Disruption in Polytraumatized Patients: A Retrospective Analysis of 1,639 Pelvic Ring Injuries
Transcatheter Aortic Valve Implantation Procedure (TAVI)
") Page 1 of 5 Procedure (TAVI) Introduction Aortic stenosis (AS) is a common heart valve problem associated with heart failure and death. Surgical valve repair or replacement is recommended if AS patients
Page 1 of 5 Procedure (TAVI) Introduction Aortic stenosis (AS) is a common heart valve problem associated with heart failure and death. Surgical valve repair or replacement is recommended if AS patients
Traumatic Cardiac Arrest Protocol
 Traumatic Cardiac Arrest Protocol Background: Major Trauma continues to be the leading worldwide cause of death in young adults. Mortality remains high but there are reports of good neurological outcomes
Traumatic Cardiac Arrest Protocol Background: Major Trauma continues to be the leading worldwide cause of death in young adults. Mortality remains high but there are reports of good neurological outcomes
TXA. Things Change. Tranexamic Acid TXA. Resuscitation 2017 TXA In The ED March 31, MAST Trousers. High Flow IV Fluids.
 Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Haemodynamically unstable patient with chest trauma
 HR J Clinical Case - Test Yourself Interventional Haemodynamically unstable patient with chest trauma Dimitrios Tomais, Theodoros Kratimenos, Dimosthenis Farsaris Interventional Radiology Unit, Radiology
HR J Clinical Case - Test Yourself Interventional Haemodynamically unstable patient with chest trauma Dimitrios Tomais, Theodoros Kratimenos, Dimosthenis Farsaris Interventional Radiology Unit, Radiology
OPCAB IS NOT BETTER THAN CONVENTIONAL CABG
 OPCAB IS NOT BETTER THAN CONVENTIONAL CABG Harold L. Lazar, M.D. Harold L. Lazar, M.D. Professor of Cardiothoracic Surgery Boston Medical Center and the Boston University School of Medicine Boston, MA
OPCAB IS NOT BETTER THAN CONVENTIONAL CABG Harold L. Lazar, M.D. Harold L. Lazar, M.D. Professor of Cardiothoracic Surgery Boston Medical Center and the Boston University School of Medicine Boston, MA
Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED. Surgical Grand Rounds
 Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED Surgical Grand Rounds ALBUMIN Most abundant plasma protein 1/3 intravascular 50% of interstitial SKIN Synthesized in hepatocytes Transcapillary escape rate COP
Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED Surgical Grand Rounds ALBUMIN Most abundant plasma protein 1/3 intravascular 50% of interstitial SKIN Synthesized in hepatocytes Transcapillary escape rate COP
British Society of Gastroenterology. St. Elsewhere's Hospital. National Comparative Audit of Blood Transfusion
 British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
Prehospital Hemorrhage Control
 Prehospital Hemorrhage Control LCOL Edward Tan, MD PhD Military Traumasurgeon Radboud University Medical center, LCOL Edward C.T.H. Tan, MD PhD Nijmegen, The Netherlands Military traumasurgeon Radboud
Prehospital Hemorrhage Control LCOL Edward Tan, MD PhD Military Traumasurgeon Radboud University Medical center, LCOL Edward C.T.H. Tan, MD PhD Nijmegen, The Netherlands Military traumasurgeon Radboud
Abdominal Trauma. Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital
 Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation