Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
|
|
|
- Jocelyn Day
- 6 years ago
- Views:
Transcription
1 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
2 I have nothing to disclose.

3 Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection Fraction: Reduced vs Preserved Symptoms Correlate Poorly With Ventricular Function
4 Aortic Stenosis in Patients With Heart Failure And Reduced Ventricular Function TAVI or Surgery?
5 TAVI vs Surgery Heart Failure + LV Dysfunction What Are The Goals? 1. Lowest Mortality 2. Lowest Morbidity 3. Recovery of LV Function 4. Good Valve Hemodynamics 5. Persistent Long Term Outcomes
6 Predictors of Mortality After Surgery Aortic Stenosis With Heart Failure and Reduced Ventricular Function
7 Results of Surgery in Severe Aortic Stenosis Ejection Fraction < 35% Mortality 30 d: 4-12% Survival 5 Years: 65-70% Predictors of Mortality: LVESVI, CardioThoracic Index Coronary Artery Disease Mean Gradient Ejection Fraction (Late Mortality) Connoly,, Circulation 1997 Vaquette, Heart 2005 Chukwuemeka, EJTCS, 2006 Pai Ann ThoracSurg, 2008 Ding, Eur Heart J 2009 Halkos, Ann Thorac Surg 2009 Chikwe, Am J Cariol, 2009

8 Functional Results of Surgery Aortic Stenosis With Ejection Fraction < 35% NYHA II NYHA III IV 20 0 Pre Op Post Op Connoly Circulation 1997 Vaquette Heart 2005 Pai Ann ThoracSurg 2008 Ding Eur Hear J 2009
9 NYHA III-IV + EF 30% N = Day Mortality : 12% Independent Predictor : CardioThoracic Ratio 0.6

 > 10 EF Units c <")
10 Change in Ejection Fraction 80% Have Improved EF c N = 55 (44%) > 10 EF Units c < 10 EF Units

11 Survival Depends on Recovery of Ejection Fraction Predictors of EF >10% 1/ CardioThoracicRatio 2/ Mean Gradient

12 PPM: AVA <0.85cm2/m2 J Thorac Cardiovasc Surg 2006;131:
13 TAVI & Heart Failure / LV Dysfunction What Do We Know?


14 N = 147 EF<50% vs EF 50%
15 No Mortality Difference (But Higher MACCE)
16 No Survival Difference With Matched SAVR

17 Circ Cardiovasc Interv.2012; 5: LVEF N 30d Mortality 1 Year Survival 35% 50 10% 69% >35% 334 3% 87% Predictors of Late Mortality: 1. Congestive Heart failure 2. Log EuroSCORE 3. Moderate-Severe PeriValvular Leak P=0.01 p<0.001
18 3195 patients FRANCE 2 Registry Log EuroSCORE 21.9±14.3% STS score 14.4±12.0% At 1 year Stroke 4.1% Periprosthetic Aortic Regurgitation 64.5%. Independent predictors of 1-year mortality o Increased logistic EuroSCORE, o NYHA functional class III or IV otransapical approach operiprosthetic regurgitation grade 2 or more N Engl J Med 2012;366:
19 FRANCE 2 Registry N Engl J Med 2012;366:
20 What Is The Impact of Coronary Artery Disease?

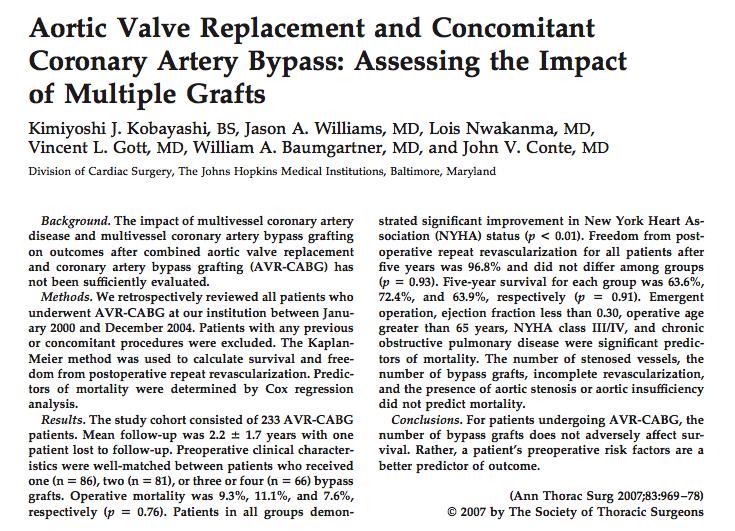
21 Associated CABG pdf/ndb2010/1stharvestexecutivesummary%5b1%5d.pdf.

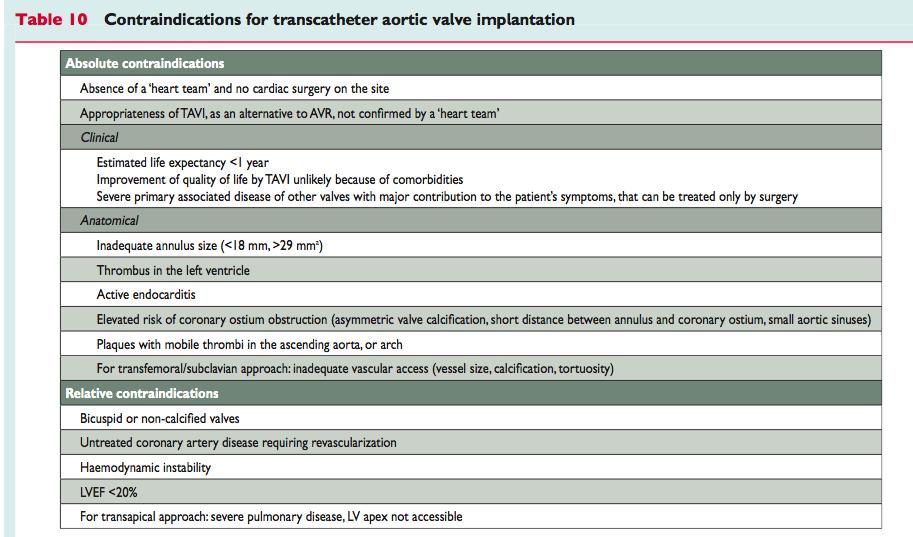
22 What About TAVI + Coronary Disease? RCTs Excluded Patients Requiring Revascularization Extent of CAD Impacts Safety AND Long Term Durability EF=30% + NYHA IV + 3 Vessel Disease: Is TAVI Safe?
23 PCI in Severe Aortic Stenosis
24 Low Flow Low Gradient and Reduced Ejection Fraction
25


26
27 Prognostic Impact of Low Gradient and/or Reduced EF After TAVI Reduced EF, Low Gradient Preserved EF, High Gradient
28 Decompensated Heart Failure & Aortic Stenosis
29 Role of Balloon Valvuloplasty Recovery High Risk TAVI


30 Decompensated Heart Failure J Thorac Cardiovasc Surg 2012;143: EF 10%-25% N = 21 Log EuroScore 66% 30 D Mortality: 4.8% No Neuro Events Post Op EF 38% 1 y Survival 76%
31 TAVI vs SAVR in Severe AS and Reduced LV Function

, absence of atrial fibrillation (P 0.")
, and complete or no need for coronary revascularization")
32 TAVI EF 50% SAVR N On multivariable analysis, the predictors of absolute change in LVEF after the procedure were female gender (P 0.004), absence of atrial fibrillation (P 0.01), baseline LVEF (P 0.005), TAVI (P 0.007), AVA (P 0.01), and complete or no need for coronary revascularization (P 0.01) Mortality 30d 19% 13% EF >50% 1 Y 58% 20% A Regurgitation 37% 5%
33 Change in Ejection Fraction Predictors of absolute change in LVEF: Whole Cohort -Female gender -Absence of atrial fibrillation -Baseline LVEF -TAVI -Greater Increase AVA -Complete or no need for coronary EF < 35% revascularization Circulation. 2010;122:
34 How Do We Decide? TAVI or Surgery?
35 TAVI vs Surgery in Heart Failure Gaps in Knowledge Limitations of The Evidence No Randomized Studies Different Cut Offs for Ejection Fraction Aortic Stenosis as Continuum: High Gradient Low Ejection Fraction Low Gradient Low Ejection Fraction: Few Patients Selection Bias Publication Bias: Learning Curve Results UnderReported


36 N Engl J Med 2012;366:

37 Circulation. 2012;126: LBBB=34% Multivariate Cox Regression All-Cause Mortality Female Sex Creatinine COPD LVEF<50% TAVI Induced LBBB


38 Consequences of Pace Maker Induced Dyssynchrony? European Journal of Heart Failure (2010) 12,

39 Risk Assessment Conditions Requiring Individual Approach Low Flow Low Gradient AS Conditions Likely To Be Associated With Insufficient Validation Requiring Further Study LV Dilatation, Diastolic Dysfunction, RV Dysfunction
40 The Heart Team Risk Assessment No Decision Without MultiDisciplinary Clinical Judgement SURGEON CARDIOLOGISTS Imaging specialists (Echo, CT, MRI) Surgery Or TAVI? Anesthesiologist Gerontologist
41 What Do Guidelines Say?
42 If mean gradient is >40 mmhg, there is theoretically no lower EF limit for aortic valve replacement in symptomatic patients with severe aortic stenosis.
43 In patients not medically fit for surgery transcatheter aortic valve replacement should be considered
44

45
46
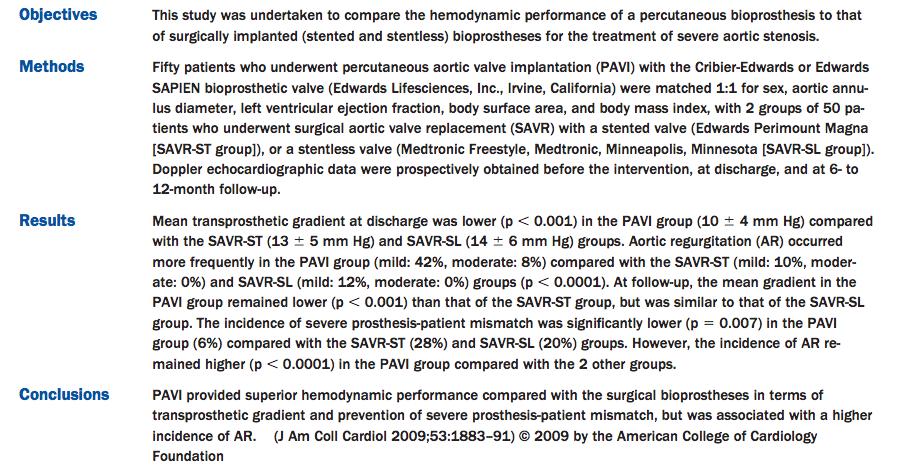
47 Take Home Messages (1) 1. Advanced Heart Failure and/or Reduced Ejection Fraction Increases the Risk of Early and Late Death After AVR But Also After TAVI 2. Risk Is Higher in Patients With Low Flow Low Gradient AS, No Contractile Reserve, Coronary Disease, Large Ventricles and NYHA III/IV 3. TAVI Provides Better Hemodynamic Than SAVR But More Aortic Regurgitation and Pace Makers 4. Surgical AVR is A Safe, Effective and Durable Option Which Should Not Be Denied to Patients On The Basis of Low LVEF Alone
48 Take Home Messages (2) 5. Avoid Patient Prosthesis Mismatch Since Depressed LV Systolic Function Patients Are Most Vulnerable to Residual LV Afterload Associated With PPM 6. TAVI May Provide a Good Alternative to Surgical AVR in patients with severe AS and Depressed Left Ventricular Systolic Function At High or Prohibitive Surgical Risk, Due to Severe Comorbidities, Small Aortic Root, and/or Lack of Myocardial Contractile Reserve. 7. Heart Team Based Approach Foundational Requirement for Risk Assessment, Decision Making, and Patient Information
49 Thank You for Your Attention

50 J Am Coll Cardiol 2012;59: As TAVI becomes more routine and widely available, operators may be tempted to implant the device in younger patients with less comorbidities. Uncertainties about the long-term durability, in addition to the unresolved issues of paravalvular aortic regurgitation and conduction abnormalities, should be cautiously weighed against the immediate benefits being widely reported.
51
 0 40 50 60 70 80 Age yr Angina Syncope Failure 0 2 4 6 Average survival (yr) Average age death (male) Ross J, Braunwald E. Aortic stenosis. Circulation.")
52 Survival % Natural history of symptomatic Aortic Stenosis is very bad without treatment TAVI vs AVR Onset of severe symptoms Latent period (increasing obstruction, myocardial overload) Age yr Angina Syncope Failure Average survival (yr) Average age death (male) Ross J, Braunwald E. Aortic stenosis. Circulation.1968; 38 [Suppl 5]:61-7

53 LV End Systolic Volume Index


54 N = 254 EF 30% 5.4% EF > 30% 1.2% 30 D Mortality p <0.01 STS 10% 10.4% STS < 10 0% <0.01 <
55 Surgical Aortic Valve Replacement Does Ejection Fraction Influence Mortality? Rahimtoola Eur Heart J 2008;;29:1783

56 Current Risk Scores Do Not Provide Reliable Estimate of Operative Mortality Specific Risk Models Should Be Developed for TAVI Future Risk Scores Should Include: Cognitive Status Functional Capacity, Nutritional Status

57 Cathet Cardiovasc Interv 2012;79:
58 TAVI in Low-Flow, Low Gradient Aortic Stenosis Low Flow Low Gradient (N=15) 33% No LF/LG (N=152) 13% Mortality (6 Months) P < Ejection Fraction Survivors N=10 Cathet Cardiovasc Interv 2012;79:


59

60 Low Flow Low Gradient Aortic Stenosis 5 Year Survival All patients N = 81 SAVR Medical p 54% 13% <0.001 Propensity Matched 65% 11% <0.02 despite a high operative mortality of 22%
61 No Contractile Reserve Influence of Mean Gradient and Coronary Disease JACC 2009;53:
62
63 Predictors of mortality after aortic valve replacement. Tjang Y S et al. Eur J Cardiothorac Surg 2007;32:
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Spotlight on Valvular Heart Disease Guidelines
 Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Severe left ventricular dysfunction and valvular heart disease: should we operate?
 Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Aortic Stenosis in the Elderly: Difficulties for the Clinician. Are Symptoms Due to Aortic Stenosis?
 Aortic Stenosis in the Elderly: Difficulties for the Clinician Are Symptoms Due to Aortic Stenosis? Raphael Rosenhek Department of Cardiology Medical University of Vienna No disclosure European Society
Aortic Stenosis in the Elderly: Difficulties for the Clinician Are Symptoms Due to Aortic Stenosis? Raphael Rosenhek Department of Cardiology Medical University of Vienna No disclosure European Society
Paris, August 28 th Gian Paolo Ussia on behalf of the CoreValve Italian Registry Investigators
 Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
Aortic Stenosis: Background
 Transcatheter Aortic Valve Replacement in Low Surgical Risk Patients Barry George, MD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Aortic Stenosis: Background Severe Symptomatic
Transcatheter Aortic Valve Replacement in Low Surgical Risk Patients Barry George, MD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Aortic Stenosis: Background Severe Symptomatic
Aortic Stenosis Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan
 Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France
 Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France Faculty disclosure Bernard Iung I disclose the following financial relationships: Consultant
Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France Faculty disclosure Bernard Iung I disclose the following financial relationships: Consultant
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer
 «Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial
 in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial") Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
Natural History and Echo Evaluation of Aortic Stenosis
 Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation
 Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation Ömer Aktug 1, MD; Guido Dohmen 2, MD; Kathrin Brehmer 1, MD; Verena Deserno 1 ; Ralf Herpertz 1 ; Rüdiger
Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation Ömer Aktug 1, MD; Guido Dohmen 2, MD; Kathrin Brehmer 1, MD; Verena Deserno 1 ; Ralf Herpertz 1 ; Rüdiger
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor
 Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes
 Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes Kostis Raisakis General Hospital of Athens «G. Gennimatas» Severe Aortic Stenosis Peak Velocity 4 m/s Up to 40%
Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes Kostis Raisakis General Hospital of Athens «G. Gennimatas» Severe Aortic Stenosis Peak Velocity 4 m/s Up to 40%
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con
 TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
When is it too late to perform transcatheter mitral valve repair? Alec Vahanian, FESC,FRCP(Edin.) Bichat hospital University Paris VII
 Bichat hospital University Paris VII") When is it too late to perform transcatheter mitral valve repair? Alec Vahanian, FESC,FRCP(Edin.) Bichat hospital University Paris VII I, (Alec Vahanian) DO have a financial interest/arrangement or affiliation
When is it too late to perform transcatheter mitral valve repair? Alec Vahanian, FESC,FRCP(Edin.) Bichat hospital University Paris VII I, (Alec Vahanian) DO have a financial interest/arrangement or affiliation
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Load and Function - Valvular Heart Disease. Tom Marwick, Cardiovascular Imaging Cleveland Clinic
 Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Transcatheter Aortic Valve Implantation. SSVQ November 23, 2012 Centre Mont-Royal 15:40
 Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives. Bernard Iung Bichat Hospital, Paris
 Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
The Role of TAVI in high-risk and normal-risk Patients
 The Role of TAVI in high-risk and normal-risk Patients Joachim Schofer Hamburg University Cardiovascular Center and Department for percutaneous treatment of structural heart disease Albertinen Heart Center
The Role of TAVI in high-risk and normal-risk Patients Joachim Schofer Hamburg University Cardiovascular Center and Department for percutaneous treatment of structural heart disease Albertinen Heart Center
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis
 Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
TAVI in Korea, How to Avoid Conduction
 TAVI in Korea, How to Avoid Conduction Disturbance after CoreValve Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine, Heart Institute, Asan Medical Center, Seoul,
TAVI in Korea, How to Avoid Conduction Disturbance after CoreValve Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine, Heart Institute, Asan Medical Center, Seoul,
Low Gradient Severe? AS
 Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
1-YEAR OUTCOMES FROM JOHN WEBB, MD
 1-YEAR OUTCOMES FROM JOHN WEBB, MD ON BEHALF OF THE SAPIEN 3 INVESTIGATORS UNIVERSITY OF BRITISH COLUMBIA VANCOUVER, CANADA Potential conflicts of interest Speaker's name: John Webb I have the following
1-YEAR OUTCOMES FROM JOHN WEBB, MD ON BEHALF OF THE SAPIEN 3 INVESTIGATORS UNIVERSITY OF BRITISH COLUMBIA VANCOUVER, CANADA Potential conflicts of interest Speaker's name: John Webb I have the following
LOW RISK TAVR. WHAT THE FUTURE HOLDS
 LOW RISK TAVR. WHAT THE FUTURE HOLDS Michael J. Reardon, M.D. Professor of Cardiothoracic Surgery Allison Family Distinguish Chair of Cardiovascular Research Houston Methodist DeBakey Heart & Vascular
LOW RISK TAVR. WHAT THE FUTURE HOLDS Michael J. Reardon, M.D. Professor of Cardiothoracic Surgery Allison Family Distinguish Chair of Cardiovascular Research Houston Methodist DeBakey Heart & Vascular
Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes
 Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes A/ Professor Darren Walters On behalf of the ANZ Source Investigators Director of Cardiology Brisbane, Australia ANZ
Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes A/ Professor Darren Walters On behalf of the ANZ Source Investigators Director of Cardiology Brisbane, Australia ANZ
TAVR in patients with. End-Stage CKD or in Renal Replacement Therapy:
 TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH
 TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
Mitral Valve Disease, When to Intervene
 Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy
 TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
RANDOMISED TRIALS TAVI WITH SAVR STEPHAN WINDECKER AORTIC VALVE DISEASE COMPARING
 AORTIC VALVE DISEASE RANDOMISED TRIALS COMPARING TAVI WITH SAVR STEPHAN WINDECKER DEPARTMENT OF CARDIOLOGY SWISS CARDIOVASCULAR CENTER AND CLINICAL TRIALS UNIT BERN BERN UNIVERSITY HOSPITAL, SWITZERLAND
AORTIC VALVE DISEASE RANDOMISED TRIALS COMPARING TAVI WITH SAVR STEPHAN WINDECKER DEPARTMENT OF CARDIOLOGY SWISS CARDIOVASCULAR CENTER AND CLINICAL TRIALS UNIT BERN BERN UNIVERSITY HOSPITAL, SWITZERLAND
Assessment and Preparation of Patients with TAVI. Rob Tanzola Associate Professor, Queen s University
 Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
TAVI in Rabin Medical Center -
 Long-Term Outcomes of 560 Consecutive Patients treated with TAVI and Propensity Score Matched- Analysis of Early Versus New Generation Valves Amos Levi, MD, Uri Landes, MD, Abid R Assali, MD, Katia Orvin,
Long-Term Outcomes of 560 Consecutive Patients treated with TAVI and Propensity Score Matched- Analysis of Early Versus New Generation Valves Amos Levi, MD, Uri Landes, MD, Abid R Assali, MD, Katia Orvin,
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Transcatheter Aortic Valve Replacement
 Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment
 Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment Stefanos Karagiannis MD PhD Cardiologist Director Echocardiology Dpt Athens Medical Center ESC 2017
Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment Stefanos Karagiannis MD PhD Cardiologist Director Echocardiology Dpt Athens Medical Center ESC 2017
Transcatheter aortic valve implantation and pre-procedural risk assesment
 Transcatheter aortic valve implantation and pre-procedural risk assesment Alec Vahanian,FESC, FRCP(Edin.) Bichat Hospital University Paris VII, Paris, France Disclosures Relationship with companies who
Transcatheter aortic valve implantation and pre-procedural risk assesment Alec Vahanian,FESC, FRCP(Edin.) Bichat Hospital University Paris VII, Paris, France Disclosures Relationship with companies who
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Aortic valve implantation using the femoral and apical access: a single center experience.
 Aortic valve implantation using the femoral and apical access: a single center experience. R. Hoffmann, K. Brehmer, R. Koos, R. Autschbach, N. Marx, G. Dohmen Rainer Hoffmann, University Aachen, Germany
Aortic valve implantation using the femoral and apical access: a single center experience. R. Hoffmann, K. Brehmer, R. Koos, R. Autschbach, N. Marx, G. Dohmen Rainer Hoffmann, University Aachen, Germany
Clinical Outcome in Patients with Aortic Stenosis
 Clinical Outcome in Patients with Aortic Stenosis Is the Prognosis Worse in Patients with Low-Gradient Severe Aortic Stenosis? Yoel Angel BSc, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc,
Clinical Outcome in Patients with Aortic Stenosis Is the Prognosis Worse in Patients with Low-Gradient Severe Aortic Stenosis? Yoel Angel BSc, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc,
Peri-operative results and complications in 15,964 transcatheter aortic valve implantations from the German Aortic valve RegistrY (GARY)
") Peri-operative results and complications in 15,964 transcatheter aortic valve implantations from the German Aortic valve RegistrY (GARY) Thomas Walther, Christian W. Hamm, Gerhard Schuler, Alexander Berkowitsch,
Peri-operative results and complications in 15,964 transcatheter aortic valve implantations from the German Aortic valve RegistrY (GARY) Thomas Walther, Christian W. Hamm, Gerhard Schuler, Alexander Berkowitsch,
On-Pump vs. Off-Pump CABG: The Controversy Continues. Miguel Sousa Uva Immediate Past President European Association for Cardiothoracic Surgery
 On-Pump vs. Off-Pump CABG: The Controversy Continues Miguel Sousa Uva Immediate Past President European Association for Cardiothoracic Surgery On-pump vs. Off-Pump CABG: The Controversy Continues Conflict
On-Pump vs. Off-Pump CABG: The Controversy Continues Miguel Sousa Uva Immediate Past President European Association for Cardiothoracic Surgery On-pump vs. Off-Pump CABG: The Controversy Continues Conflict
Results of Transfemoral Transcatheter Aortic Valve Implantation
 Results of Transfemoral Transcatheter Aortic Valve Implantation Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Results of Transfemoral Transcatheter Aortic Valve Implantation Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
2/28/2010. Speakers s name: Paul Chiam. I have the following potential conflicts of interest to report: NONE. Antegrade transvenous transseptal route
 Transcatheter Aortic Valve Implantation Asian perspective Speakers s name: Paul Chiam Paul TL Chiam MBBS, MRCP, FACC I have the following potential conflicts of interest to report: NONE Consultant National
Transcatheter Aortic Valve Implantation Asian perspective Speakers s name: Paul Chiam Paul TL Chiam MBBS, MRCP, FACC I have the following potential conflicts of interest to report: NONE Consultant National
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO
 AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
Incidence, Predictors, and Outcomes of Prosthesis-Patient Mismatch in 62,125 TAVR Patients. An STS/ACC TVT Registry Report
 Incidence, Predictors, and Outcomes of Prosthesis-Patient Mismatch in 62,125 TAVR Patients An STS/ACC TVT Registry Report Howard C. Herrmann, MD University of Pennsylvania Philadelphia Howard C. Herrmann
Incidence, Predictors, and Outcomes of Prosthesis-Patient Mismatch in 62,125 TAVR Patients An STS/ACC TVT Registry Report Howard C. Herrmann, MD University of Pennsylvania Philadelphia Howard C. Herrmann
Reverse left atrium and left ventricle remodeling after aortic valve interventions
 Reverse left atrium and left ventricle remodeling after aortic valve interventions Alexandra Gonçalves, Cristina Gavina, Carlos Almeria, Pedro Marcos-Alberca, Gisela Feltes, Rosanna Hernández-Antolín,
Reverse left atrium and left ventricle remodeling after aortic valve interventions Alexandra Gonçalves, Cristina Gavina, Carlos Almeria, Pedro Marcos-Alberca, Gisela Feltes, Rosanna Hernández-Antolín,
Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute
 Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute Despite a 33 fold growth in the first five years, there is still tremendous variability among penetration in different countries
Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute Despite a 33 fold growth in the first five years, there is still tremendous variability among penetration in different countries
Vinod H. Thourani, MD, FACC, FACS
 Considering SAVR in the TAVR era: Surgical Implications of TAVR Vinod H. Thourani, MD, FACC, FACS Professor of Cardiothoracic Surgery and Medicine Chief of Cardiothoracic Surgery, Emory Hospital Midtown
Considering SAVR in the TAVR era: Surgical Implications of TAVR Vinod H. Thourani, MD, FACC, FACS Professor of Cardiothoracic Surgery and Medicine Chief of Cardiothoracic Surgery, Emory Hospital Midtown
Interventional procedures guidance Published: 26 July 2017 nice.org.uk/guidance/ipg586
 Transcatheter aortic valve implantation for aortic stenosis Interventional procedures guidance Published: 26 July 17 nice.org.uk/guidance/ipg586 Your responsibility This guidance represents the view of
Transcatheter aortic valve implantation for aortic stenosis Interventional procedures guidance Published: 26 July 17 nice.org.uk/guidance/ipg586 Your responsibility This guidance represents the view of
Percutaneous Management of Severe AS in Octagenarians. Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington
 Percutaneous Management of Severe AS in Octagenarians Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington May 2017 Outline Aetiology of AS Natural History of AS Assessment
Percutaneous Management of Severe AS in Octagenarians Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington May 2017 Outline Aetiology of AS Natural History of AS Assessment
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives. Martin B. Leon, MD
 The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval?
 Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval? Update from PARTNER EU and SOURCE Registries T. Lefèvre Disclosure Statement Cardiologist Interventional cardiologist 1 st PABV in
Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval? Update from PARTNER EU and SOURCE Registries T. Lefèvre Disclosure Statement Cardiologist Interventional cardiologist 1 st PABV in
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI)
") Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504
 Transcatheter valve-in-valve e implantation for aortic bioprosthetic valve dysfunction Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504 Your responsibility This
Transcatheter valve-in-valve e implantation for aortic bioprosthetic valve dysfunction Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504 Your responsibility This
ΔΙΑΔΕΡΜΙΚΗ ΑΝΣΙΚΑΣΑΣΑΗ ΑΟΡΣΙΚΗ ΒΑΛΒΙΔΑ αντιμετώπιση επιπλοκών ΠΕΣΡΟ. ΔΑΡΔΑ, MD, FESC IICE 2012
 ΔΙΑΔΕΡΜΙΚΗ ΑΝΣΙΚΑΣΑΣΑΗ ΑΟΡΣΙΚΗ ΒΑΛΒΙΔΑ αντιμετώπιση επιπλοκών ΠΕΣΡΟ. ΔΑΡΔΑ, MD, FESC IICE 2012 TAVR Technologies Current Generation Devices ~ 50,000 patients treated thru 2011 in > 500 interventional centers
ΔΙΑΔΕΡΜΙΚΗ ΑΝΣΙΚΑΣΑΣΑΗ ΑΟΡΣΙΚΗ ΒΑΛΒΙΔΑ αντιμετώπιση επιπλοκών ΠΕΣΡΟ. ΔΑΡΔΑ, MD, FESC IICE 2012 TAVR Technologies Current Generation Devices ~ 50,000 patients treated thru 2011 in > 500 interventional centers
Understanding the guidelines for Interventions in MR. Ali AlMasood
 Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Is TAVR the treatment of choice for high risk diabetic patients with aortic stenosis? Insights from the FRANCE2 Registry
 Is TAVR the treatment of choice for high risk diabetic patients with aortic stenosis? Insights from the FRANCE2 Registry E Van Belle, E Teiger, F Juthier, A Vincentelli, B Iung, H Eltchaninoff, J Fajadet,
Is TAVR the treatment of choice for high risk diabetic patients with aortic stenosis? Insights from the FRANCE2 Registry E Van Belle, E Teiger, F Juthier, A Vincentelli, B Iung, H Eltchaninoff, J Fajadet,
Valvular Intervention
 Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Asymptomatic Valvular Disease:
 Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Role of Stress Echo in Valvular Heart Disease. Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
 Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC
 Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
First Transfemoral Aortic Valve Implantation In Bulgaria - Crossing The Valve With The Device Is Not Always
 ISPUB.COM The Internet Journal of Cardiology Volume 9 Number 2 First Transfemoral Aortic Valve Implantation In Bulgaria - Crossing The Valve With The Device Is Not T D, J P. Citation T D, J P.. First Transfemoral
ISPUB.COM The Internet Journal of Cardiology Volume 9 Number 2 First Transfemoral Aortic Valve Implantation In Bulgaria - Crossing The Valve With The Device Is Not T D, J P. Citation T D, J P.. First Transfemoral
How to Avoid Prosthesis-Patient Mismatch
 How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
Saudi Heart Association. Raising Standards through Education and Training
 Saudi Heart Association Raising Standards through Education and Training 25th Annual Meeting EACTS Lisbon, Oc ctober 2011 WWW EA WWW. ACTS ORG ACTS.ORG Clinical decision making in case of Aortic valve
Saudi Heart Association Raising Standards through Education and Training 25th Annual Meeting EACTS Lisbon, Oc ctober 2011 WWW EA WWW. ACTS ORG ACTS.ORG Clinical decision making in case of Aortic valve
Coronary interventions
 Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Alec Vahanian,FESC, FRCP (Edin.) Bichat Hospital University Paris VII, Paris, France
 Bichat Hospital University Paris VII, Paris, France") Future Percutaneous Therapies for Mitral Valve Disease (Mitraclip,percutaneous annuloplasty and transcatheter valve implantation) Will they reach the TAVI s success? Alec Vahanian,FESC, FRCP (Edin.) Bichat
Future Percutaneous Therapies for Mitral Valve Disease (Mitraclip,percutaneous annuloplasty and transcatheter valve implantation) Will they reach the TAVI s success? Alec Vahanian,FESC, FRCP (Edin.) Bichat
Managing the Low Output Low Gradient Aortic Stenosis Patient
 Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Percutaneous aortic valve replacement should NOT be preferred therapy for aortic stenosis
 Percutaneous aortic valve replacement should NOT be preferred therapy for aortic stenosis James Bartholomew McClurken, MD FACC, FCCP, FACS, FESC Professor & Vice-Chair of Surgery, Temple University Hosp.,
Percutaneous aortic valve replacement should NOT be preferred therapy for aortic stenosis James Bartholomew McClurken, MD FACC, FCCP, FACS, FESC Professor & Vice-Chair of Surgery, Temple University Hosp.,
Patient referral for elective coronary angiography: challenging the current strategy
 Patient referral for elective coronary angiography: challenging the current strategy M. Santos, A. Ferreira, A. P. Sousa, J. Brito, R. Calé, L. Raposo, P. Gonçalves, R. Teles, M. Almeida, M. Mendes Cardiology
Patient referral for elective coronary angiography: challenging the current strategy M. Santos, A. Ferreira, A. P. Sousa, J. Brito, R. Calé, L. Raposo, P. Gonçalves, R. Teles, M. Almeida, M. Mendes Cardiology
TAVR y Enfermedad Coronaria. Mauricio G. Cohen, MD, FACC, FSCAI Director, Cardiac Catheterization Lab Associate Professor of Medicine
 TAVR y Enfermedad Coronaria Mauricio G. Cohen, MD, FACC, FSCAI Director, Cardiac Catheterization Lab Associate Professor of Medicine CAD and AS Similar Pathological Processes CAD in TAVR Patients (n=390)
TAVR y Enfermedad Coronaria Mauricio G. Cohen, MD, FACC, FSCAI Director, Cardiac Catheterization Lab Associate Professor of Medicine CAD and AS Similar Pathological Processes CAD in TAVR Patients (n=390)
Indication, Timing, Assessment and Update on TAVI
 Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Maurizio D Amico M.D.
 TAVI BEST CANDIDATE AND OPTIMIZED LONG TERM FOLLOW-UP Maurizio D Amico M.D. Dipartimento Cardiovascolare e Toracico Città della Salute e della Scienza, Turin Italy Regional Guidelines for TAVI implantation
TAVI BEST CANDIDATE AND OPTIMIZED LONG TERM FOLLOW-UP Maurizio D Amico M.D. Dipartimento Cardiovascolare e Toracico Città della Salute e della Scienza, Turin Italy Regional Guidelines for TAVI implantation
TAVI: 10 Years After the First Case Low-Risk and High-Risk Patients What are the Limits? Dr Bernard Prendergast DM FRCP FESC John Radcliffe Hospital
 TAVI: 10 Years After the First Case Low-Risk and High-Risk Patients What are the Limits? Dr Bernard Prendergast DM FRCP FESC John Radcliffe Hospital Oxford I have financial relationships to disclose Honoraria
TAVI: 10 Years After the First Case Low-Risk and High-Risk Patients What are the Limits? Dr Bernard Prendergast DM FRCP FESC John Radcliffe Hospital Oxford I have financial relationships to disclose Honoraria
Aortic Stenosis Background and Breakthroughs in Treatment: TAVR Update
 Aortic Stenosis Background and Breakthroughs in Treatment: TAVR Update Howard J Broder MD Interventional Cardiology DaVita Medical Group/ Healthcare Partners Cardiology Disclosures for Howard J Broder
Aortic Stenosis Background and Breakthroughs in Treatment: TAVR Update Howard J Broder MD Interventional Cardiology DaVita Medical Group/ Healthcare Partners Cardiology Disclosures for Howard J Broder
Supplementary Online Content
 Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
 Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Dr.ssa Loredana Iannetta. Centro Cardiologico Monzino
 Dr.ssa Loredana Iannetta Centro Cardiologico Monzino Bicuspid aortic valve BAV is the most common congenital cardiac anomaly. Estimated incidence is 2% in general population. 4:1 male predominance. Frequency
Dr.ssa Loredana Iannetta Centro Cardiologico Monzino Bicuspid aortic valve BAV is the most common congenital cardiac anomaly. Estimated incidence is 2% in general population. 4:1 male predominance. Frequency
Incidence and Management of Early Implant Failure after Transcatheter Aortic Valve Implantation
 ESC Congress 2010 28 Aug 2010-01 Sep 2010 Stockholm - Sweden Incidence and Management of Early Implant Failure after Transcatheter Aortic Valve Implantation Gian Paolo Ussia, MD Director of Interventional
ESC Congress 2010 28 Aug 2010-01 Sep 2010 Stockholm - Sweden Incidence and Management of Early Implant Failure after Transcatheter Aortic Valve Implantation Gian Paolo Ussia, MD Director of Interventional
Rapid deployment aortic valve replacement for the treatment of severe aortic stenosis in high risk patients. Β. Κόλλιας, Σ. Ματιάτου, Δ. Αγγουράς.
 Rapid deployment aortic valve replacement for the treatment of severe aortic stenosis in high risk patients. Οι βιοπροσθετικές αορτικές βαλβίδες ταχείας έκπτυξης στην αντιµετώπιση της σοβαρής αορτικής
Rapid deployment aortic valve replacement for the treatment of severe aortic stenosis in high risk patients. Οι βιοπροσθετικές αορτικές βαλβίδες ταχείας έκπτυξης στην αντιµετώπιση της σοβαρής αορτικής
Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS
 Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T H E P A R T N E R T R
Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T H E P A R T N E R T R
Severity of AS Degree of AV calcification (? Bicuspid AV), annulus size, & aortic root
, annulus size, & aortic root") The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
What the Cardiologist needs to know from Medical Images
 What the Cardiologist needs to know from Medical Images Gerald Maurer Department of Cardiology Medical University of Vienna What kinds of Cardiologists Plumbers Electricians Photographers And then there
What the Cardiologist needs to know from Medical Images Gerald Maurer Department of Cardiology Medical University of Vienna What kinds of Cardiologists Plumbers Electricians Photographers And then there
Low Gradient AS Normal LVEF
 Low Gradient AS Normal LVEF Shahbudin H. Rahimtoola MB, FRCP, MACP, MACC, FESC, D.Sc.(Hon) Distinguished Professor University of Southern California Griffith Professor of Cardiology Professor of Medicine
Low Gradient AS Normal LVEF Shahbudin H. Rahimtoola MB, FRCP, MACP, MACC, FESC, D.Sc.(Hon) Distinguished Professor University of Southern California Griffith Professor of Cardiology Professor of Medicine
PARTNER 2A & SAPIEN 3: TAVI for intermediate risk patients
 O P E N A C C E S S Department of Cardiology, Aswan Heart Centre *Email: ahmed.elguindy@aswanheartcentre.com Lessons from the trials PARTNER 2A & SAPIEN 3: TAVI for intermediate risk patients Ahmed ElGuindy*
O P E N A C C E S S Department of Cardiology, Aswan Heart Centre *Email: ahmed.elguindy@aswanheartcentre.com Lessons from the trials PARTNER 2A & SAPIEN 3: TAVI for intermediate risk patients Ahmed ElGuindy*
Welcome 17 Michigan TAVR Participating Hospitals!
 Welcome 17 Michigan TAVR Participating Hospitals! 1 MICHIGAN TAVR BRIEF OVERVIEW HOW AND WHY PRE-TAVR IMAGING EVALUATION AND THE TVT Michael Grossman, MD Co-Director, BMC2 Coordinating Center Why Michigan
Welcome 17 Michigan TAVR Participating Hospitals! 1 MICHIGAN TAVR BRIEF OVERVIEW HOW AND WHY PRE-TAVR IMAGING EVALUATION AND THE TVT Michael Grossman, MD Co-Director, BMC2 Coordinating Center Why Michigan
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR
 TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
2/15/2018 DISCLOSURES OBJECTIVES. Consultant for BioSense Webster, a J&J Co. Aortic stenosis background. Short history of TAVR
 TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO!
 ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,