PATIENT S NAME, DATE/TIME,
|
|
|
- Ashley Lawson
- 6 years ago
- Views:
Transcription

1 ECG and Arrhythmias Dec, 1 st 2014 Doctor Mohammad Jarrah References: - Lecture and Slides - ECG Made Easy - Davidson Principles of Medicine - First Aid Cases for the USMLE Step 1 - Mini-OSCE Archive ECG stands for electrocardiogram; it s a record of the heart s electrical activity. it s a very important tool that can provide evidences to support a specific diagnosis. Remember that most abnormalities in the ECG are amenable to reason. The Basics: The quality of an ECG is determined by the presence of PATIENT S NAME, DATE/TIME, the 12 LEADS and a RYTHEM STRIP at the bottom. The paper moves in a speed of 25mm/s (horizontal).?if faster (50mm/s) it ll give a false impression of slow HR And a caliberation of 1cm or 10mm/mV (vertical).?if >1mm/mv gives a false impression of Left Ventriuclar Hypertrophy 1 small square (Ssq) = 1 mm, 1 large square (Lsq) = 5 Ssq = 5 mm. P: Atria Depolarization (<2.5 mm vertical) QRS: Ventricular Depolarization T: Ventricular Repolarization U: Repolarization of the papillary muscles follows the T wave. (Normal or Abnormal) PR interval: ms (3-5 small squares) >220: Block, <120: accessory pathway QRS complex: 120 ms (3 small squares) 1 min = 60 sec = 60* (5 large squares) = 300 large square Heart Rate= 300 (Lsq)/ R-R interval = 1500 (Ssq)/ R-R interval = # of R per 15 (Lsq) * 20 = ( bpm) normally. Rhythm: - Sinus rhythm if each QRS is preceded by P - Regular rhythm if the distance between the R is constant. 1




2 Normal ECG Positive deflection: If a wave of depolarization passing through the heart is moving toward a surface electrode Negative deflection: If a wave of depolarization passing through the heart is moving away from the electrode. Biphasic wave: If a wave of depolarization passing through the heart is moving perpendicularly to the electrode. The 12-Lead ECG 6 limb leads: I between right arm and left arm. II between right arm and left leg. III between left arm and left leg. avr: right arm, avl: left arm, avf: left leg I, II, avl: Left lateral surface. III, avf: Inferior surface. avr: Right surface. In a normal cardiac axis (about 60 degrees): Lead II and avf have the highest positive deflection. I and II are normally both positively deflected. Lead II is usually the long rhythm strip, with the most obvious P wave. 2

3 6 chest leads: V1 and V2: Parasternal at 4 th intercostals space. V3 is in between V2 and V4. V4, V5 and V6 at the 5 th intercostal space: V4: Midclavicular line V5: Anterior axillary line V6: Middle axillary line. V1, V2, V3, V4: Anteriospetal surface. V5,V6: Lateral surface In a normal cardiac axis (about 60 degrees): - V1: Small R, Deep S - V2: R increases, S decreases - V3/V4: R=S - V5/V6: Large R, S disappears in normal people If the R is poorly enlarging (poor progression R wave sign of ischemia) The Cardiac Axis: Normally, between -30 and +90 Right Axis Deviation/RAD (>+90): Right ventricular hypertrophy Left Axis Deviation/LAD (<-30): Left ventricular hypertrophy, LBBB. Indeterminate Axis (No Man s Land): extreme LAD or extreme RAD, Dextrocardia. -ve Lead I +ve Lead II +ve Lead I -ve Lead II -ve Lead I, II & III 3

 Normal axis (+ve lead I,II and III)")
4 Normal ECG Record: 12 leads with a rhythm strip (II) Good Voltage (2 Lsq or 1cm vertical) HR = 300/5 = 60 bpm Regular Sinus Rhythm: P wave precedes each QRS with good relation between them PR interval is between 3-5 Ssq, P voltage is less than 2.5 Ssq QRS complex is less than 3 Ssq QT isn t prolonged (<450 ms) Normal axis (+ve lead I,II and III) Negative T wave in V1 is normal V1 V6: R increases and S decreases (disappears in V6) 4

 Poor")
 Abnormalities due to")
5 ECG Record with some abnormalities: 12 leads with a rhythm strip (II) Good Voltage (2 Lsq or 1cm vertical) HR > 60 bpm Regular Sinus Rhythm: P wave precedes each QRS with good relation between them PR interval is between 3-5 Ssq, P voltage is less than 2.5 Ssq QRS complex is slightly widened is some leads Left axis deviation (+ve Lead I and ve Lead II) Poor progression R wave Ischemia S wave in V6? Abnormality The abnormally looking complex in avf is just an artefact (not significant) Abnormalities due to machine or human error: Paper speed 12.5 mm/s false rapid heart rate Patient is shivering Remember: ECG must be individualized: Male vs Female, Old vs Young, Chest Pain vs Normal 5

: accessory pathway associated with Delta wave. - Could be normal in rapid heart rate.")
6 The Abnormalities of the waves, complexes and intervals: Absence P Pulmonale: Pointy; >2.5 Ssq vertical in Lead II P wave abnormalities Not Sinus Right Atrial dilatation/hypertrophy due to cor pulmonale/copd/... P Mitral: Bifid in Lead II Left Atrial dilatation/hypertrophy due to Mitral stenosis (MS) or sometimes MR Too short (<3 Ssq) Too long (>1Lsq) PR Interval Abnormalities - Wolf Parkinson White syndrome (WPW): accessory pathway associated with Delta wave. - Could be normal in rapid heart rate. Heart block/av block (1 st, 2 nd and 3 rd degrees) Spot on Arrhythmias: Preexcitation syndromes (WPW Syndrome): Preexcitation is a condition characterized by an accessory pathway of conduction, which allows the heart to depolarize in an atypical sequence. In Wolfe-Parkinson-White (WPW) syndrome, there s a direct atrioventricular connection allows the ventricles to begin depolarization while the standard action potential is still traveling through the AV node. ECG Characteristics of WPW: 1. Short PR interval 2. QRS prolongation 3. Delta Wave 4. Followed by tachycardia 6
: 1 st degree Heart block: - Prolongation of the PR interval, which is constant - All P waves")

: No relationship between P waves")
7 In fact, the PR interval isn t shortened, but it looks so due to the emergence of the delta wave. Heart Block (AV block): 1 st degree Heart block: - Prolongation of the PR interval, which is constant - All P waves are conducted 2 nd degree Heart block (Mobitz 1)/Wenckebach: - Progressive prolongation of the PR interval until a P wave is not conducted. - As the PR interval prolongs, the RR interval actually shortens 2 nd degree Heart block (Mobitz 2): Constant PR interval with intermittent failure to conduct Third degree Heart block (Complete): No relationship between P waves and QRS complexes, Relatively constant PP intervals and RR intervals and Greater number of P waves than QRS complexes 7
 Accepted Q waves: V1, avr and III Pathological Q waves: >25% of subsequent complex and unusual location")
 in V1 and the biggest R wave in V5 or V6 >35mm (> 5Lsq) Left Ventricular Hypertrophy (LVH) If LVH is")
8 QRS complex Abnormalities Generally, if QRS > 0.12 ms Bundle Branch Block (Rt vs Lt) Accepted Q waves: V1, avr and III Pathological Q waves: >25% of subsequent complex and unusual location on leads previous infarction. Sum of the S wave (-ve deflection) in V1 and the biggest R wave in V5 or V6 >35mm (> 5Lsq) Left Ventricular Hypertrophy (LVH) If LVH is presented with ST depression and T inversion on the left leads indicates LVH induced infarction (blood supply isn t enough for the hypertrophied muscle tissue (LVH with Strain) LVH with Strain, Normal sinus rhythm 8
 in V1, V2 and")
 or LAD (Atrial septal defect, severe conducting problem)")
 in V5, V6, I and deep S in V1 - Usually associated with LAD Mnemonic MaRRoW: M")
9 Spot on LBBB and RBBB: Common causes ECG changes Appearance RBBB - Normal variant - Right ventricular hypertrophy or strain - ASD QRS > 3 Ssq RSR (M shaped QRS complex) in V1, V2 and deep S in V6. - May present with RAD (usually) or LAD (Atrial septal defect, severe conducting problem) LBBB - CAD - HTN - Aortic valve disease - Cardiomyopathy QRS > 3 Ssq RSR (M shaped QRS complex) in V5, V6, I and deep S in V1 - Usually associated with LAD Mnemonic MaRRoW: M first letter = M in V1 WiLLiaM: M last letter = M in V6 RBBB with LAD: Bifascicular rhythm s 9

, consider LVH with strain or digoxin toxicity ST elevation - Infarction")
 and axis, ST elevation is V2-V6, and minimally in avl, Q wave")
10 ST segment Abnormalities These are usually in territories eg. anterior/lateral/inferior etc. and will be present in contiguous leads (III,aVF or I,aVL,V5,V6...) ST depression: - Downsloping or horizontal = abnormal - Ischaemia (coronary stenosis): Chest pain association - If lateral (V4-V6), consider LVH with strain or digoxin toxicity ST elevation - Infarction (coronary occlusion) - Pericarditis (widespread) - Prinzmetal spasm - Post ventricular aneurysm - Early embolization Normal rhythm (P wave in II) and axis, ST elevation is V2-V6, and minimally in avl, Q wave also present: Acute MI in the proximal Left Anterior Descending Artery. 10


11 Sinus rhythm ST depression Lead I, avl, ST elevation V5, V6 Lateral MI (acute over chronic) ST elevation in III and avf Inferior MI reciprocal ST depression in V1, V2 Posterior MI InferioPosterioLateral MI Super-dominant Right coronary artery, proximal occlusion. ask for Right ventricular leads Right Ventricular Infarction Cardiogenic Shock Hypotension IV fluids Pericarditis: Sinus tachycardia with Diffuse ST elevation in all leads except: V1: Normal or depression, avr: ST depression 11

 and irregular rhythm, rate = 120, right axis deviation?")

12 T wave Abnormalities Peaked hyperkalaemia or normal young man Inverted/biphasic ischaemia, previous infarct Small hypokalaemia What is the rate, rhythm and axis for these patients, and is there any other abnormalities? Not sinus (ectopic) and irregular rhythm, rate = 120, right axis deviation?, LVH due to deep S and huge R, T inversion can be seen laterally. LVH Right atrial abnormality and fibrillation P wave present, Sinus tachycardia and LVH (what s the rate?) 12
 Recall that the NORMAL SINUS RHYTHM shows Regular")


13 P wave present, Sinus bradychardia (what s the rate?) Recall that the NORMAL SINUS RHYTHM shows Regular narrow-complex rhythm Rate bpm, Each QRS complex is proceeded by a P wave P wave is upright in lead II & downgoing in lead avr Bradycardia, and obvious delta wave in V1 WPW Syndrome ST elevation in inferior leads and No relation between P and QRS complete Heart Block 13
 Atrial and Ventricular Arrythmias? Supraventricular means SA, AV or Atrial origin.")
14 QT interval must be corrected because it s affected by the HR: QT interval Abnormalities Long QT (>450ms) can be genetic (long QT syndrome) or secondary due to drugs (amiodarone, sotalol) Associated with risk of sudden death due to Torsades de Pointes (check page 16) Atrial and Ventricular Arrythmias? Supraventricular means SA, AV or Atrial origin. Most Important Arrythmias to be familiar with: SVT (Supraventricular Tachycardia): Narrow QRS, Rate >150, regular RR complexes, P wave may be superimposed on T wave or hidden inside the QRS complex: Atrial Flutter: Biphasic sawtooth flutter waves at a rate of >250/min Flutter waves have constant amplitude, duration, and morphology through the cardiac cycle. There is usually either a 2:1 or 4:1 block at the AV node, resulting in ventricular rates of either 150 or 75 bpm Adenosine is used to unmask an unclear record (SVT or Flutter?) by showing the saw-tooth appearance. 14


15 Atrial Fibrillation Atrial fibrillation is caused by numerous wavelets of depolarization spreading throughout the atria simultaneously, leading to an absence of coordinated atrial contraction. AF is important because it can lead to: Hemodynamic compromise, Systemic embolization and other Symptoms On ECG: Absent P waves, Presence of fine fibrillatory waves which vary in amplitude and morphology, Irregularly irregular ventricular response. Ventricular Tachychardia: (usually follows MI) - Broad bizzare QRS complex - Regular RR waves - Rate >120 (less than the SVT) - P waves are present, fused with T or on top of ascending QRS complexes - Treat with lignocaine or DC shock. Some times a normal QRS is present within the tachycardia: Capture beat. 15


? 1. Is the rate slow (<60 bpm) or fast (>100 bpm)?")
16 Torsade de Pointe: usually with prolonged QT interval The QRS complexes spin around the baseline, changing their axis and amplitude Ectopic Beats Abnormal early beat whether atrial or ventricular within a normal ECG In ventricular extrasystole/ectopic beat : QRS would look broad and bizarre, not preceeded by P and followed by opposing ST-T changes and by a compnesatory pause. In Atrial extrasystole/ectopic beat: QRS would look normal, abnormally looking P wave and with a compnesatory pause. Unknown Arrhythmia (not discussed)? 1. Is the rate slow (<60 bpm) or fast (>100 bpm)? Slow Suggests sinus bradycardia, sinus arrest, or conduction block Fast Suggets increased/abnormal automaticity or reentry 16
17 2. Is the rhythm irregular? Irregular Suggests atrial fibrillation, 2 nd degree AV block, multifocal atrial tachycardia, or atrial flutter with variable AV block 3. Is the QRS complex narrow or wide? Narrow Rhythm must originate from the AV node or above Wide Rhythm may originate from anywhere 4. Are there P waves? Absent P waves Suggests atrial fibrillation, ventricular tachycardia, or rhythms originating from the AV node 5. What is the relationship between the P waves and QRS complexes? More P waves than QRS complexes Suggests 2 nd or 3 rd degree AV block More QRS complexes than P waves Suggests an accelerated junctional or ventricular rhythm 6. Is the onset/termination of the rhythm abrupt or gradual? Abrupt Suggests reentrant rhythm Gradual Suggests altered automaticity When the variations in PP interval occur in phase with respiration, this is considered to be a normal variant, called sinus arrhythmia: What is the Sick Sinus Syndrome (SSS)? Characterized by a collection of symptoms and ECG findings due to chronic dysfunction of the sinoatrial (SA) node: Chronic and severe sinus bradycardia 17

18 Sinus pauses Sinus arrhythmia Complete sinus arrest Progressive development of atrial arrhythmias (a-flutter, a-fib, atrial tachycardia) Patients are usually elderly and present with lightheadedness and/or syncope, but it can also manifest as angina, dyspnea, and palpitations. Tachycardia-Bradycharida Variant: (needs pacemaker and medication for the AV) Etiologies: Sinus node firbosis, Atherosclerosis of the SA artery, Congenital heart disease, Excessive vagal tone, Familial, Pericarditis, Hypothyrodism. Multifocal Atrial Tachycardia: Discrete P waves with at least 3 different morphologies. Atrial rate > 100 bpm. The PP, PR, and RR intervals all vary. It s very common with COPD and Lung fibrosis patients. 18
 Hypokalemia: (U wave)")
 Interpret this ECG case, before checking its")
19 Abnormalities due to electrolyte disturbance: Hyperkalemia: (peaked T) Hypokalemia: (U wave) Hypercalcemia: (QT Shortening) Hypocalcemia: (QT Elongation) Interpret this ECG case, before checking its answer beneath it: RBBB 19

20 First Aid Cases? 20

21 Past-Years Mini-OSCE Question: A 68 year old male presents with hx of frequent palpitations. What is your diagnosis? Answer: AF Note: Arrythmias were discussed in 10 minutes out of 2 hours, this sheet provide the most important ones according to what the doctor came through and what Davidson emphasized on. Make an effort to differentiate Normal from Abnormal ECG, and diagnose MI, Angina, Bundle Branch Blocks, AV Blocks, Tachycardia, Bradycardia, Axis deviation, Atrial and Ventricular hypertrophy, and Abnormal/ectopic/SV rhythms in general. Good Luck. Melad 21
22 Reminders 8 REMINDERS WHAT TO LOOK FOR 1. The rhythm and conduction: sinus rhythm or some early arrhythmias evidence of first, second or third degeree block evidence of bundle branch block. 2. P wave abnormalities: peaked, tall right atrial hypertrophy notched, broad left atrial hypertrophy. 3. The cardiac axis: right axis deviation QRS complex predominantly downward in lead I left axis deviation QRS complex predominantly downward in leads II and III. 4. The QRS complex: width: if wide, ventricular origin, bundle branch block or the WPW syndrome height: tall R waves in lead V 1 in right ventricular hypertrophy tall R waves in lead V 6 in left ventricular hypertrophy transition point: R and S waves are equal in the chest leads over the interventricular septum (normally lead V 3 or V 4 ) clockwise rotation (persistent S wave in lead V 6 ) indicates chronic lung disease. Q waves:? septal? infarction. 5. The ST segment: raised in acute myocardial infarction and in pericarditis depressed in ischaemia and with digoxin. 6. T waves: peaked in hyperkalaemia flat, prolonged, in hypokalaemia inverted: normal in some leads ischaemia infarction left or right ventricular hypertrophy pulmonary embolism bundle branch block. 7. U waves: can be normal hypokalaemia. 175
23 Now test yourself REMINDERS CONDUCTION PROBLEMS First degree block One P wave per QRS complex. PR interval greater than 200 ms. Second degree block Wenckebach (Mobitz type 1): progressive PR lengthening then a nonconducted P wave, and then repetition of the cycle. Mobitz type 2: occasional nonconducted beats. 2:1 (or 3:1) block: two (or three) P waves per QRS complex, with a normal P wave rate. Third degree (complete) block No relationship between P waves and QRS complexes. Usually, wide QRS complexes. Usual QRS complex rate less than 50/min. Sometimes, narrow QRS complexes, rate 50 60/min. Right bundle branch block QRS complex duration greater than 120 ms. RSR 1 pattern. Usually, dominant R 1 wave in lead V 1. Inverted T waves in lead V 1, and sometimes in leads V 2 V 3. Deep and wide S waves in lead V 6. Left anterior hemiblock Marked left axis deviation deep S waves in leads II and III, usually with a slightly wide QRS complex. Left bundle branch block QRS complex duration greater than 120 ms. M pattern in lead V 6, and sometimes in leads V 4 V 5. No septal Q waves. Inverted T waves in leads I, VL, V 5 V 6 and, sometimes, V 4. Bifascicular block Left anterior hemiblock and right bundle branch block (see above). 176
24 Reminders 8 REMINDERS CAUSES OF AXIS DEVIATION Right axis deviation Normal variant tall thin people. Right ventricular hypertrophy. Lateral myocardial infarction (peri-infarction block). Dextrocardia or right/left arm lead switch. The Wolff Parkinson White (WPW) syndrome. Left posterior fascicular block. Left axis deviation Left anterior hemiblock. The WPW syndrome. Inferior myocardial infarction (peri-infarction block). Ventricular tachycardia. REMINDERS POSSIBLE IMPLICATIONS OF ECG PATTERNS P:QRS apparently not 1:1 If you cannot see one P wave per QRS complex, consider the following: If the P wave is actually present but not easily visible, look particularly at leads II and V 1. If the QRS complexes are irregular, the rhythm is probably atrial fibrillation, and what seem to be P waves actually are not. If the QRS complex rate is rapid and there are no P waves, a wide QRS complex indicates ventricular tachycardia, and a narrow QRS complex indicates atrioventricular nodal (junctional or AV nodal) re-entry tachycardia. If the QRS complex rate is low, it is probably an escape rhythm. P:QRS more than 1:1 If you can see more P waves than QRS complexes, consider the following: If the P wave rate is 300/min, the rhythm is atrial flutter. If the P wave rate is /min and there are two P waves per QRS complex, the rhythm is atrial tachycardia with block. If the P wave rate is normal (i.e /min) and there is 2:1 conduction, the rhythm is sinus with second degree block. If the PR interval appears to be different with each beat, complete (third degree) heart block is probably present. continued 177
25 Now test yourself REMINDERS POSSIBLE IMPLICATIONS OF ECG PATTERNS continued Wide QRS complexes (greater than 120 ms) Wide QRS complexes are characteristic of: Sinus rhythm with bundle branch block Sinus rhythm with the WPW syndrome Ventricular extrasystoles Ventricular tachycardia Complete heart block. Q waves Small (septal) Q waves are normal in leads I, VL and V 6. A Q wave in lead III but not in VF is a normal variant. Q waves probably indicate infarction if present in more than one lead, are longer than 40 ms in duration and are deeper than 2 mm. Q waves in lead III but not in VF, plus right axis deviation, may indicate pulmonary embolism. The leads showing Q waves indicate the site of an infarction. ST segment depression Digoxin: ST segment slopes downwards. Ischaemia: flat ST segment depression. T wave inversion Normal in leads III, VR and V 1 ; and in V 2 V 3 in black people. Ventricular rhythms. Bundle branch block. Myocardial infarction. Right or left ventricular hypertrophy. The WPW syndrome. 178
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECGs: Everything a finalist needs to know. Dr Amy Coulden As part of the Simply Finals series
 ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Paediatric ECG Interpretation
 Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
ECG CONVENTIONS AND INTERVALS
 1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Appendix D Output Code and Interpretation of Analysis
 Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
Blocks & Dissociations. Reading Assignment (p47-52 in Outline )
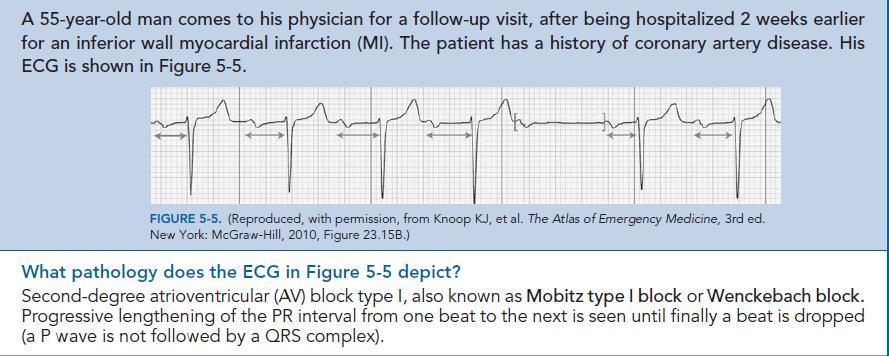
") Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block:
Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block:
Cardiology Flash Cards
 Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Family Medicine for English language students of Medical University of Lodz ECG. Jakub Dorożyński
 Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Conduction Problems / Arrhythmias. Conduction
 Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Ekg pra pr c a tice D.HAMMOUDI.MD
 Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Supraventricular Arrhythmias. Reading Assignment. Chapter 5 (p17-30)
") Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
402 Index. B β-blockers, 4, 5 Bradyarrhythmias, 76 77
 Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
DR QAZI IMTIAZ RASOOL OBJECTIVES
 PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology)
") ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
12 Lead ECG. Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept.
 12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)
 PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)") 1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1
 usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1") If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1 mm depth and 3 mm width( most specific) Since Mitral
If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1 mm depth and 3 mm width( most specific) Since Mitral
Electrocardiography Abnormalities (Arrhythmias) 7. Faisal I. Mohammed, MD, PhD
 7. Faisal I. Mohammed, MD, PhD") Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
Electrical System Overview Electrocardiograms Action Potentials 12-Lead Positioning Values To Memorize Calculating Rates
 Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
2017 EKG Workshop Advanced. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
The Electrocardiogram part II. Dr. Adelina Vlad, MD PhD
 The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG
 By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
This presentation will deal with the basics of ECG description as well as the physiological basics of
 Snímka 1 Electrocardiography basics This presentation will deal with the basics of ECG description as well as the physiological basics of Snímka 2 Lecture overview 1. Cardiac conduction system functional
Snímka 1 Electrocardiography basics This presentation will deal with the basics of ECG description as well as the physiological basics of Snímka 2 Lecture overview 1. Cardiac conduction system functional
Introduction to Electrocardiography
 Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
Section V. Objectives
 Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
15 16 September Seminar W10O. ECG for General Practice
 15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
Introduction to ECG Gary Martin, M.D.
 Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
General Introduction to ECG. Reading Assignment (p2-16 in PDF Outline )
") General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
ELECTROCARDIOGRAPH. General. Heart Rate. Starship Children s Health Clinical Guideline
 General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
12 Lead ECG Skills: Building Confidence for Clinical Practice. Presented By: Cynthia Webner, BSN, RN, CCRN-CMC. Karen Marzlin, BSN, RN,CCRN-CMC
 12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
Electrocardiogram ECG. Hilal Al Saffar FRCP FACC College of medicine,baghdad University
 Electrocardiogram ECG Hilal Al Saffar FRCP FACC College of medicine,baghdad University Tuesday 29 October 2013 ECG introduction Wednesday 30 October 2013 Abnormal ECG ( ischemia, chamber hypertrophy, heart
Electrocardiogram ECG Hilal Al Saffar FRCP FACC College of medicine,baghdad University Tuesday 29 October 2013 ECG introduction Wednesday 30 October 2013 Abnormal ECG ( ischemia, chamber hypertrophy, heart
Miscellaneous Stuff Keep reading the Outline
 Miscellaneous Stuff Keep reading the Outline Welcome to the 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic measurements:
Miscellaneous Stuff Keep reading the Outline Welcome to the 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic measurements:
Myocardial Infarction. Reading Assignment (p66-78 in Outline )
") Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
ECG Practice Strips Discussion part 1:
 ECG Practice Strips Discussion part 1: The first 20 strips are for teaching various abnormalities of the morphology of the waves of the ECG. Strips 21 and following are for teaching some abnormalities
ECG Practice Strips Discussion part 1: The first 20 strips are for teaching various abnormalities of the morphology of the waves of the ECG. Strips 21 and following are for teaching some abnormalities
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm 2012 Session 2: 12 Lead ECG Fundamentals 101 Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Though for Today Mastery is not something that strikes in an instant, like a thunderbolt,
Relax and Learn At the Farm 2012 Session 2: 12 Lead ECG Fundamentals 101 Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Though for Today Mastery is not something that strikes in an instant, like a thunderbolt,
Pathologic ECG. Adelina Vlad, MD PhD
 Pathologic ECG Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze the morphology and
Pathologic ECG Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze the morphology and
ECG pre-reading manual. Created for the North West Regional EMET training program
 ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
ECG Interactive Session
 SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
Understanding the 12-lead ECG, part II
 Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Chapter 2 Practical Approach
 Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
THE ELECTROCARDIOGRAM A UBIQUITOUS AND COST-EFFECTIVE DIAGNOSTIC TOOL FOR THE FAMILY MEDICINE REFRESHER COURSE MARCH 8, 2019
 THE ELECTROCARDIOGRAM A UBIQUITOUS AND COST-EFFECTIVE DIAGNOSTIC TOOL FOR THE FAMILY MEDICINE REFRESHER COURSE MARCH 8, 2019 Major Clinical Disorders Pulmonary Embolism 69 y/o woman with dyspnea and an
THE ELECTROCARDIOGRAM A UBIQUITOUS AND COST-EFFECTIVE DIAGNOSTIC TOOL FOR THE FAMILY MEDICINE REFRESHER COURSE MARCH 8, 2019 Major Clinical Disorders Pulmonary Embolism 69 y/o woman with dyspnea and an
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
Appendix. Table 1: Causes for abnormal axis deviation Left axis deviation
 Appendix Table 1: Causes for abnormal axis deviation Left axis deviation Normal variant (2 5%) Left anterior fascicular block Left ventricular hypertrophy Inferior wall myocardial infarction Primum atrial
Appendix Table 1: Causes for abnormal axis deviation Left axis deviation Normal variant (2 5%) Left anterior fascicular block Left ventricular hypertrophy Inferior wall myocardial infarction Primum atrial
PAEDIATRIC ECG Dimosthenis Avramidis, MD.
 PAEDIATRIC ECG Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece S. Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece 5 y/o with sinus tach Background ECG changes
PAEDIATRIC ECG Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece S. Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece 5 y/o with sinus tach Background ECG changes
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University. OBHG Education Subcommittee
 -RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
ECG. Prepared by: Dr.Fatima Daoud Reference: Guyton and Hall Textbook of Medical Physiology,12 th edition Chapters: 11,12,13
 ECG Prepared by: Dr.Fatima Daoud Reference: Guyton and Hall Textbook of Medical Physiology,12 th edition Chapters: 11,12,13 The Concept When the cardiac impulse passes through the heart, electrical current
ECG Prepared by: Dr.Fatima Daoud Reference: Guyton and Hall Textbook of Medical Physiology,12 th edition Chapters: 11,12,13 The Concept When the cardiac impulse passes through the heart, electrical current
ECG Interpretation. Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction
 * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction") ECG to save Babies ECG Interpretation Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction Electrical Activity in the heart 5 events
ECG to save Babies ECG Interpretation Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction Electrical Activity in the heart 5 events
EKG. Danil Hammoudi.MD
 EKG Danil Hammoudi.MD What is an EKG? The electrocardiogram (EKG) is a representation of the electrical events of the cardiac cycle. Each event has a distinctive waveform, the study of which can lead to
EKG Danil Hammoudi.MD What is an EKG? The electrocardiogram (EKG) is a representation of the electrical events of the cardiac cycle. Each event has a distinctive waveform, the study of which can lead to
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient September 25, 2009
 Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Electrocardiography for Healthcare Professionals. Chapter 14 Basic 12-Lead ECG Interpretation
 Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
at least 4 8 hours per week
 ECG IN ATHLETS An athlete is defined as an individual who engages in regular exercise or training for sport or general fitness, typically with a premium on performance, and often engaged in individual
ECG IN ATHLETS An athlete is defined as an individual who engages in regular exercise or training for sport or general fitness, typically with a premium on performance, and often engaged in individual
FLB s What Are Those Funny-Looking Beats?
 FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
ECG (MCQs) In the fundamental rules of the ECG all the following are right EXCEP:
 In the fundamental rules of the ECG all the following are right EXCEP:") ECG (MCQs) 2010 1- In the fundamental rules of the ECG all the following are right EXCEP: a- It is a biphasic record of myocardial action potential fluctuations. b- Deflection record occurs only during
ECG (MCQs) 2010 1- In the fundamental rules of the ECG all the following are right EXCEP: a- It is a biphasic record of myocardial action potential fluctuations. b- Deflection record occurs only during
ECG interpretation basics
 ECG interpretation basics Michał Walczewski, MD Krzysztof Ozierański, MD 21.03.18 Electrical conduction system of the heart Limb leads Precordial leads 21.03.18 Precordial leads Precordial leads 21.03.18
ECG interpretation basics Michał Walczewski, MD Krzysztof Ozierański, MD 21.03.18 Electrical conduction system of the heart Limb leads Precordial leads 21.03.18 Precordial leads Precordial leads 21.03.18
also aid the clinician in recognizing both the obvious and subtle abnormalities that may help guide therapy.
 Karen Lieberman, MS, CRNP f the many diagnostic tools used to screen for and evaluate cardiac abnormalities, the 12-lead electrocardiogram (ECG) is among the most basic. This inexpensive and noninvasive
Karen Lieberman, MS, CRNP f the many diagnostic tools used to screen for and evaluate cardiac abnormalities, the 12-lead electrocardiogram (ECG) is among the most basic. This inexpensive and noninvasive
12 Lead ECG Interpretation
 12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
Case 1. Case 2. Case 3
 Case 1 The correct answer is D. Occasionally, the Brugada syndrome can present similar morphologies to A and also change depending on the lead position but in the Brugada pattern the r is wider and ST
Case 1 The correct answer is D. Occasionally, the Brugada syndrome can present similar morphologies to A and also change depending on the lead position but in the Brugada pattern the r is wider and ST
Skin supplied by T1-4 (medial upper arm and neck) T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio
 T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio") Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Return to Basics. Normal Intervals & Axes. ECG Rate and Rhythm
 Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
12 LEAD EKG BASICS. By: Steven Jones, NREMT P CLEMC
 12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
1/22/2007 Fernald Medical Monitoring Program Sort Code EKG coding
 1/22/2007 Fernald Medical Monitoring Program Sort Code EKG coding PLEASE NOTE THAT ALL EKG CODES MUST RANGE FROM 500-599 OR FROM 900-999. PLEASE DO NOT ASSIGN NUMBERS OUTSIDE THAT RANGE FOR EKG CODES.
1/22/2007 Fernald Medical Monitoring Program Sort Code EKG coding PLEASE NOTE THAT ALL EKG CODES MUST RANGE FROM 500-599 OR FROM 900-999. PLEASE DO NOT ASSIGN NUMBERS OUTSIDE THAT RANGE FOR EKG CODES.
Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG?
 Objectives What s in an ECG?") Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG? The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic
Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG? The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic
Course Objectives. Proper Lead Placements. Review the ECG print paper. Review the mechanics of the Myocardium. Review basics of ECG Rhythms
 ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
Acute Coronary Syndromes. Disclosures
 Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient October 4, 2007
 Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
2017 EKG Workshop Basic. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Basic Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part I - Objectives Discuss a systematic approach to EKG interpretation
2017 EKG Workshop Basic Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part I - Objectives Discuss a systematic approach to EKG interpretation
5- The normal electrocardiogram (ECG)
") 5- The (ECG) Introduction Electrocardiography is a process of recording electrical activities of heart muscle at skin surface. The electrical current spreads into the tissues surrounding the heart, a small
5- The (ECG) Introduction Electrocardiography is a process of recording electrical activities of heart muscle at skin surface. The electrical current spreads into the tissues surrounding the heart, a small
Office ECG Interpretation
 Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
ELECTROCARDIOGRAPHY KEVIN REBECK PA-C. For more presentations
 ELECTROCARDIOGRAPHY KEVIN REBECK PA-C For more presentations www.medicalppt.blogspot.com Objectives ECG History Pathophysiology Basics Case Historys Electrical activation of the heart In the heart
ELECTROCARDIOGRAPHY KEVIN REBECK PA-C For more presentations www.medicalppt.blogspot.com Objectives ECG History Pathophysiology Basics Case Historys Electrical activation of the heart In the heart
ABCs of ECGs. Shelby L. Durler
 ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
Ben Taylor, PhD, PA-C
 Ben Taylor, PhD, PA-C The patient is a 23-year-old white male with a history of polysubstance abuse who was found unresponsive, last seen the day before. Classic signs of systemic hypothermia with prominent
Ben Taylor, PhD, PA-C The patient is a 23-year-old white male with a history of polysubstance abuse who was found unresponsive, last seen the day before. Classic signs of systemic hypothermia with prominent
1 st Degree Block Prolonged P-R interval caused by first degree heart block (lead II)
") AV Heart Blocks 1 st degree A condition of a rhythm, not a true rhythm Need to always state underlying rhythm 2 nd degree Type I - Wenckebach Type II Classic dangerous to the patient Can be variable (periodic)
AV Heart Blocks 1 st degree A condition of a rhythm, not a true rhythm Need to always state underlying rhythm 2 nd degree Type I - Wenckebach Type II Classic dangerous to the patient Can be variable (periodic)
A Review of Cardiac Pathophysiology and EKG. Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS
 A Review of Cardiac Pathophysiology and EKG Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS Cardiac Pathophysiology Coronary Artery Disease Congestive Heart Failure Valvular Heart Disease Athletic Heart
A Review of Cardiac Pathophysiology and EKG Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS Cardiac Pathophysiology Coronary Artery Disease Congestive Heart Failure Valvular Heart Disease Athletic Heart
ELECTROCARDIOGRAPHY (III) THE ANALYSIS OF THE ELECTROCARDIOGRAM
 THE ANALYSIS OF THE ELECTROCARDIOGRAM") ELECTROCARDIOGRAPHY (III) THE ANALYSIS OF THE ELECTROCARDIOGRAM Scridon Alina, Șerban Răzvan Constantin Recording and analysis of the 12-lead ECG is part of the basic medical assessment performed for every
ELECTROCARDIOGRAPHY (III) THE ANALYSIS OF THE ELECTROCARDIOGRAM Scridon Alina, Șerban Răzvan Constantin Recording and analysis of the 12-lead ECG is part of the basic medical assessment performed for every
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
12 Lead EKG. The Basics
 12 Lead EKG The Basics Objectives Demonstrate proper 12 EKG lead placement Determine electrical axis Identify ST and T wave changes as they relate to myocardial ischemia Describe possible complications
12 Lead EKG The Basics Objectives Demonstrate proper 12 EKG lead placement Determine electrical axis Identify ST and T wave changes as they relate to myocardial ischemia Describe possible complications
Dr.Binoy Skaria 13/07/15
 Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
Bundle Branch & Fascicular Blocks. Reading Assignment (p53-58 in Outline )
") Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
Case-Based Practical ECG Interpretation for the Generalist
 Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
6/19/2018. Background Athlete s heart. Ultimate question. Applying the International Criteria for ECG
 Applying the International Criteria for ECG Interpretation in Athletes to a preparticipation screening program DAVE SIEBERT, MD, CAQSM ASSISTANT PROFESSOR DEPARTMENT OF FAMILY MEDICINE UNIVERSITY OF WASHINGTON
Applying the International Criteria for ECG Interpretation in Athletes to a preparticipation screening program DAVE SIEBERT, MD, CAQSM ASSISTANT PROFESSOR DEPARTMENT OF FAMILY MEDICINE UNIVERSITY OF WASHINGTON
Understanding basics of EKG
 Understanding basics of EKG By Alula A.(R III) www.le.ac.uk Topic for discussion Understanding of cellular electrophysiology Basics Rate Rhythm Axis Intervals P wave QRS ST/T wave Abnormal EKGs Understanding
Understanding basics of EKG By Alula A.(R III) www.le.ac.uk Topic for discussion Understanding of cellular electrophysiology Basics Rate Rhythm Axis Intervals P wave QRS ST/T wave Abnormal EKGs Understanding